Chapter 8:
The incidence and control of smallpox between 1900 and 1958

INTRODUCTION
As has been described in Chapter 5, by the end of the 19th century variola major was endemic in most countries of the world and in every inhabited continent except Australia ; and a new mild variety of smallpox, variola minor, was endemic in South Africa and the USA.
The present chapter explores the situation between 1900 and 1958 in greater detail than was given in the survey of the global incidence of smallpox in Chapter 4, drawing for the earlier data on Low (1918), Simmons et al. (1944-1954), Hopkins (1983a), various papers published in scientific journals, and records produced by national health authorities in several countries. It also traces in some detail the elimination of endemic smallpox in several countries in each continent in the years before 1958, which provided the rationale for the decision by the World Health Assembly to embark on a global smallpox eradication programme in 1959. Inevitably, because of the absence of reliable data from many countries and the inadequacy of the record even in those with the best data, the treatment of the subject is far from complete.
VARIATIONS IN THE INCIDENCE OF VARIOLA MAJOR AND VARIOLA MINOR
As Fig. 5.8 (Chapter 5) illustrates, the American strain of variola minor (alastrim) virus spread from the USA to Canada, South America, Europe, Australia and New Zealand. Viruses that differed from alastrim virus in several biological properties (see Chapter 2) caused variola minor in Africa, and their spread is more difficult to trace. African variola minor was endemic in southern Africa until 1973, and a similar disease was reported from time to time in many countries of eastern and central Africa, usually coexisting with endemic variola major. It is not clear whether its extension in Africa was due solely to spread from the southern African focus or whether there were other places in Africa in which a similar mutant form of the virus emerged, or indeed whether some outbreaks followed importations of alastrim from the homelands of the European colonial powers.
One of the most interesting epidemiological features of smallpox during the period 1920-1958 was the relation between variola major and variola minor in countries in which both varieties occurred. An important factor affecting their relative incidence was the attitude of the public at large and public health workers to smallpox control; in general, both were much more tolerant of variola minor than of variola major. This was evident in many countries-for example, Switzerland, in which variola minor was endemic between 1921 and 1926. When variola major occurred in Basle in 1921 (44 cases; 7 deaths) it was promptly controlled, whereas it took 6 years to eliminate variola minor from Switzerland (Sobernheim, 1929), leading to a pronouncement by the Swiss delegate to the 1926 International Sanitary Conference of the Office international d’Hygiene publique:
“[Smallpox] has, in reality, no place in an international convention. It is not a pestilential disease in the proper sense of the term: it is, in effect, a disease that exists everywhere. There is probably not a single country of which it can be said that there are no cases of smallpox.” (Cited by Howard-Jones, 1975.)
Three other factors were operative: the infectiousness of individual patients; the number of contacts with susceptible subjects; and the degree of protection afforded by vaccination, if it had been carried out many years earlier. Patients with variola major usually excreted more virus and were thus more infectious than patients with variola minor, and variola major was more likely to overcome the effects of slight residual immunity due to vaccination. On the other hand, the severity of systemic symptoms from the prodromal stage onwards was so great in variola major that most patients were confined to bed and thus their contacts were greatly limited. Patients with variola minor usually had such a mild systemic illness that they were often ambulant throughout the course of the disease, and therefore made many more close contacts.
These four factors, and the element of chance, in relation to viral mutation or importation, interacted to produce four patterns of endemicity:
-
In very well vaccinated communities, such as in many countries of continental Europe in the 1930s, the level of immunity of the population was so high that variola minor could not become established. Any smallpox that did occur was variola major associated with importations.
-
In countries such as the United Kingdom and the USA, with highly organized health services but without properly enforced compulsory vaccination, outbreaks of variola major were rapidly brought under control by isolation and selective vaccination, whereas variola minor evoked no such reaction from the health authorities. For example, in Detroit, Michigan, in 1923, at a time when variola minor was epidemic (710 cases in 6 months), the Health Department conducted vigorous propaganda for vaccination but achieved only about 6000 vaccinations per month. Soon afterwards variola major was imported from Canada; the vaccination rate increased very greatly, half a million persons being vaccinated within 1 month and 800 000 (about 70% of the population) within 5 months.
-
In populous countries in which vaccination was poor and the health services ineffective, such as India and Mexico, variola major predominated because of its greater capacity to infect and spread.
-
In some African countries such as Ethiopia, in which at that time there was virtually no vaccination, endemic variola minor replaced variola major, probably during the 1950s. In this country of sparse population and very poor communications, the major factor favouring variola minor was probably its capacity to persist in small nomadic groups, among whom the transmission of variola major would have been interrupted spontaneously (see Chapters 4 and 21). Its persistence was probably helped by the widespread practice of variolation (see Chapter 21). For much of the period under review variola major and variola minor coexisted in many central, eastern and southern African countries.
Brazil does not fit readily into this classification. Although its health services were probably no better than those of Mexico during the 1920s and 1930s, alastrim replaced variola major in Brazil during the 1920s but never became endemic in Mexico.
THE ELEIMINATION OF SMALLPOX FROM EUROPE BY 1953
One of the factors which led to the decision by the Twelfth World Health Assembly, in 1959, to adopt global eradication of smallpox as a major goal of the World Health Organization (see Chapter 9) was the fact that by this time eradication had been achieved in all the countries of Europe and of Central and North America. Tables 8.1 and 8.2 set out the incidence of reported cases of smallpox between 1920 and 1958, in selected countries of western and eastern Europe respectively.
Table 8.1: Western Europe: numbers of reported cases of smallpox in selected countries, 1920-1958a

-
a A horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b After 1945, consolidated figures for the German Democratic Republic and the Federal Republic of Germany.
c Figures in italics denote the number of reported deaths from smallpox.
d Endemic smallpox was eliminated before 1900, but importations occurred during most years up to 1926, and occasionally after that date.
Table 8.2: Eastern Europe: numbers of reported cases of smallpox in selected countries, 1920- I958a,b

a A horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b...= data not recorded; + = smallpox present, but number of cases unknown.
c Figures in italics denote the number of reported deaths from smallpox.
d Endemic smallpox was eliminated in 1934 but was re-established in 1943 and eliminated again in 1944.
Notes on the Statistical Tables
In order to illustrate the discussion presented in this chapter, a number of statistical tables are included to show the incidence of reported cases (rarely of reported deaths) in selected countries in various regions. The tables also show estimates of the populations of the countries listed near the beginning and end of the period for which the smallpox incidence is recorded, in order to give some indication of the sizes of the exposed populations. (The source of these population estimates is the United Nations Demographic Yearbook, 1960 (United Nations, 1961) for the years 1920-1949 and Population Prospects: Estimates and Projections Assessed in 1982 (United Nations, 1985) for 1950 and subsequent years.)
Except in Portugal, Spain, the USSR and Mexico, most outbreaks of variola major in Europe and North America after about 1930 were due to importations and the numbers were reported reasonably accurately. However, experience in the Intensified Smallpox Eradication Programme showed that for countries of Africa, South America and Asia, the reported figures greatly underestimated the incidence, often representing no more than 1- 2% of the true totals. In all countries in which variola minor was endemic, also, many cases were misdiagnosed or not reported. Nevertheless, the waxing and waning of the numbers of cases reported by various countries, as presented in these tables, reflect changes in the incidence of smallpox and provide evidence of its elimination from an increasing number of countries during the first half of the 20th century.
In each table the year considered by the authors to be the probable one in which endemic smallpox was eliminated from various countries is indicated by a horizontal line in the appropriate place; cases reported after this date are regarded as having been due to importations. As will be described in Chapter 23, such importations continued to occur in many countries until the mid-1970s. After endemic smallpox had been eliminated, outbreaks associated with importations rarely persisted for more than a few months.
It should be emphasized that just as the data on incidence given in the tables are often only an approximate indicator of the true incidence, it is also often impossible to determine in exactly which year smallpox ceased to be endemic in a particular country. After the Intensified Smallpox Eradication Programme had commenced operations, intensive surveillance made it possible to recognize the exact date of onset of the last case of endemic smallpox. In the period with which this chapter deals, however, smallpox sometimes just faded away; even the year in which the last endemic case occurred, let alone the precise date of its onset, is hard to determine. Where variola minor was prevalent, as in the USA, “smallpox” continued to be reported on the basis of faulty diagnoses after it had ceased to be endemic. The dates given for the elimination of endemic smallpox before 1958 are therefore sometimes a matter of judgment rather than of precise knowledge.
The gradual elimination of endemic smallpox from the countries of Europe is illustrated in Fig. 8.1-8.3. In the following pages, the overall position in Europe between 1900 and 1958 is described first, drawing on Low (1918) for data before the First World War. Stowman (1945), Fabre (1948), Murray (1951) and the Epidemiological and Vital Statistics Report (1953) provide useful summaries of the incidence during both the First and the Second World Wars and the inter-war period. Following this summary, the situation in selected European countries for which more detailed data are available is described at greater length. The same procedure is used for the other continents.
The latter part of the 19th century had seen a great decline in smallpox in most countries of Europe, as glycerolated calf-derived vaccine became available, health services improved, and vaccination and revaccination were practised more extensively (see Chapter 6). The decline continued during the early years of the 20th century, the incidence of smallpox being particularly low in the well vaccinated populations of Austria, Germany and the Scandinavian countries. In contrast, the Iberian Peninsula continued to suffer from endemic smallpox with periodic severe outbreaks.
Low (1918) has summarized published information on the worldwide incidence of smallpox during the period before any international statistical organization existed; his report provides an invaluable source of data for the early part of the 20th century. Table 8.3 summarizes some of Low’s figures on the numbers of reported deaths from smallpox in various countries of Europe between 1900 and 1914. Because of the persistently high incidence of smallpox in Russia, travellers from that country were a particularly important source of importations of smallpox into its European neighbours, especially the Scandinavian countries and Germany. Fortunately, in view of the strong antivaccinationist movement prevailing there at that time, the British Isles were shielded to some extent from importations from mainland Europe, because of the small number of travellers from Russia. Importations from the colonies were also infrequent, because the long voyage by ship ensured that infected persons who had embarked during the incubation period became ill before arrival and could therefore be recognized and isolated. The last large outbreaks of variola major in the United Kingdom occurred in 1902-1903.
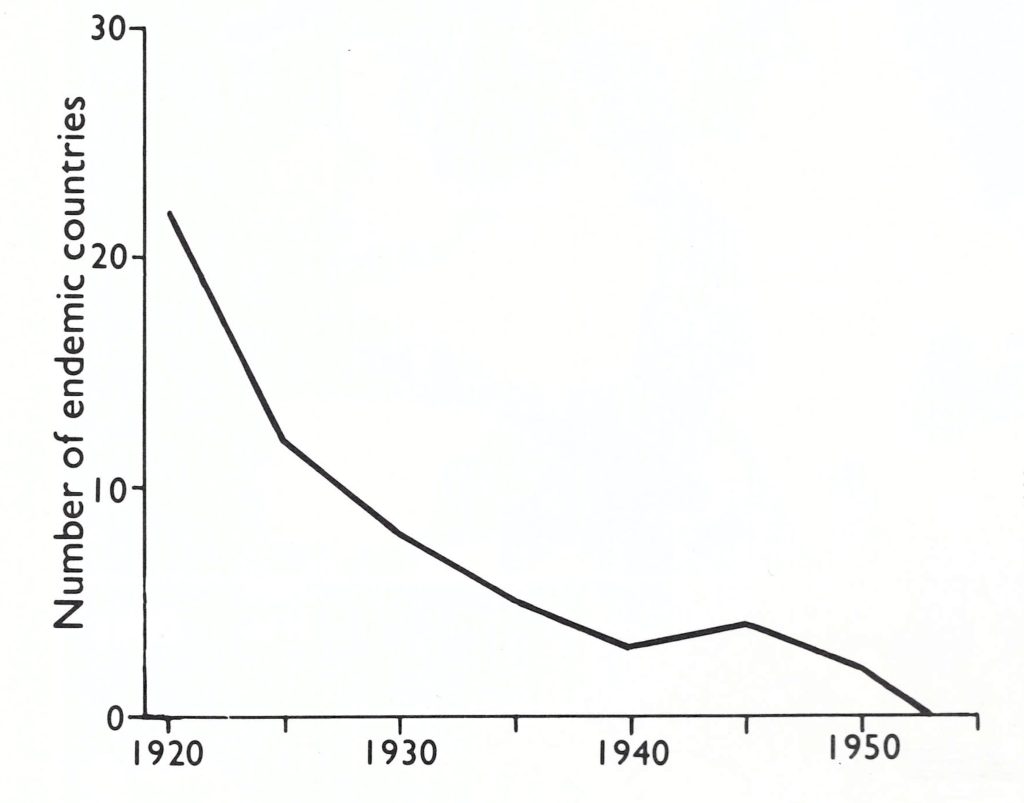
Fig. 8.1. Number of countries in Europe in which smallpox was endemic at various times between 1920 and its continental elimination in 1953 based on the 30 political divisions operative in 1982—i.e., those shown in Fig. 8.2 together with Cyprus, Malta and Luxembourg (all non-endemic) and Turkey (see Fig. 8.11).
Table 8.3: Europe: Numbers of reported deaths from smallpox in selected countries, 1900-1919, by quinquenniuma,b
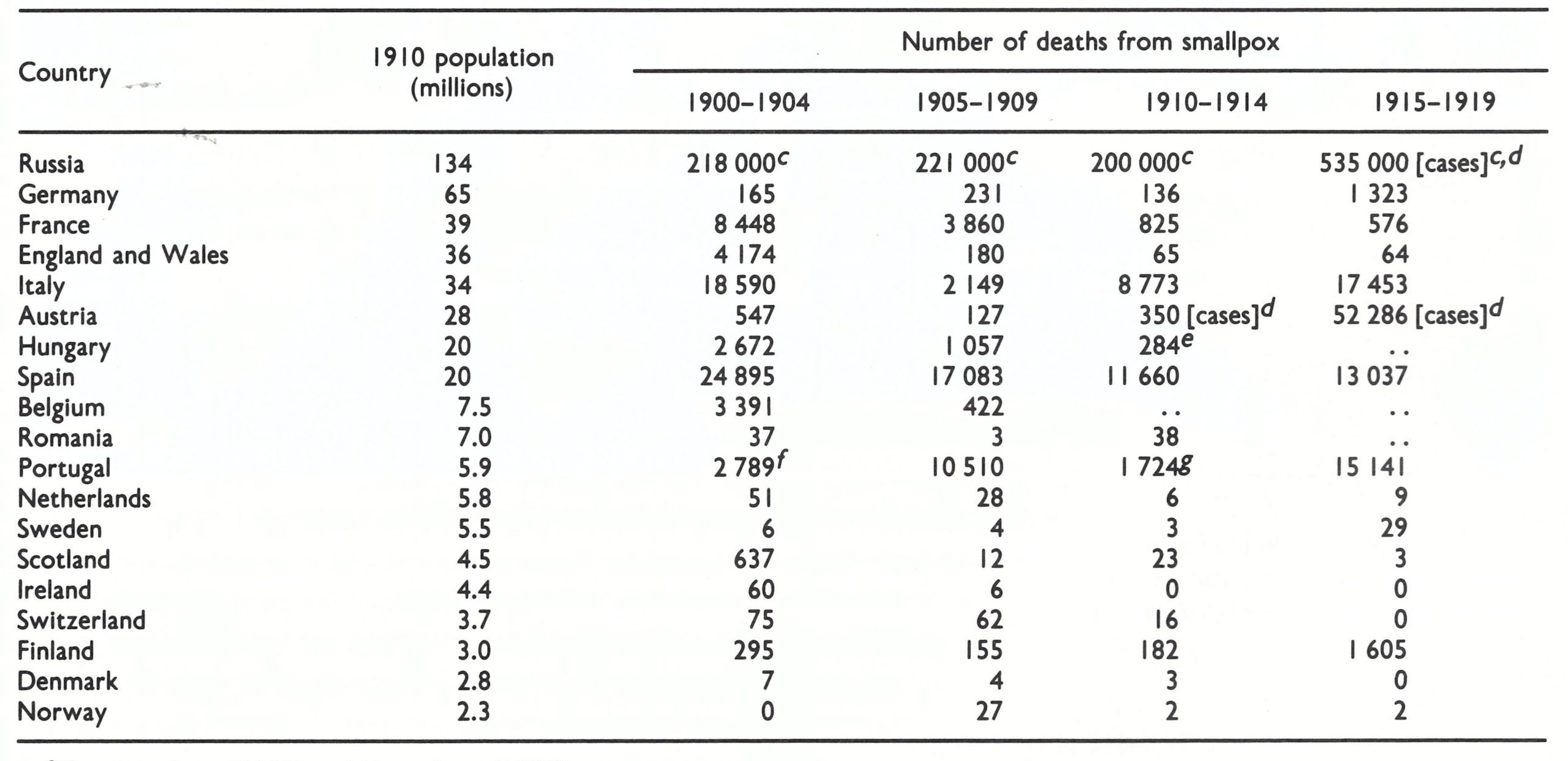
a Based on Low (I 9 18) and Henneberg (1956).
b Approximate.
c ..=no data recorded.
d Number of reported cases.
e Up to 1912 only.
f Refers to 1902, 1903 and 1904 only.
g Refers to 1910, 1913 and 1914 only.
Fig. 8.2. Europe: year in which smallpox ceased to be endemic in each country (national boundaries as of 1982). Dates in parentheses (for Greece and Italy) indicate the initial elimination of endemic smallpox, after which endemicity was again established before final elimination in the year shown.
Fig. 8.3. Europe: countries with endemic variola major, endemic variola minor or with importations, and the number of reported cases of smallpox for the years 1920. 1930, I940 and 1950. (Based on Jezek et al., 1982.)
The disruption and mass movements associated with the First World War exacerbated the disease in Russia—it was particularly severe in Russian Poland-and from Russia it spread to Germany, Austria and Sweden. Smallpox remained endemic in Italy, Romania and Yugoslavia, and in the area that later formed the new state of Czechoslovakia, as well as in Portugal and Spain. In the aftermath of the First World War the situation became even worse. During 1918-1920 severe epidemics killed 28 000 persons in Italy, 14 000 in Portugal and 1500 in Germany; in the USSR 186 000 cases were reported in 1919. For political reasons, Switzerland had sealed its borders throughout the First World War, and this saved it from imported smallpox, which had been a major problem in the Franco-Prussian War of 1870-1871.
As countries recovered from the ravages of the war and as effective public health measures were reinstated, variola major became much less common. However, in the early 1920s alastrim was imported into the United Kingdom from the USA and became established there as an endemic disease, producing over 10 000 reported cases each year between 1926 and 1930. It was finally eliminated in 1934. It occurred in a few other European countries:”…in 1922 the mild non-fatal type was the rule in Finland, Germany, Switzerland, Egypt, Cuba, Jamaica, South Africa and parts of Canada and the United States, as well as the United Kingdom (England and Wales, Ministry of Health, 1923). Alastrim broke out in the Netherlands in 1929, and it occurred concurrently with variola major in Spain and Portugal in 1936. However, the only other prolonged outbreak of variola minor in Europe was in Switzerland, in which over 5000 cases occurred between 1921 and 1926.
By the late 1930s endemic smallpox had been eliminated from most countries of Europe except Portugal, Spain (which experienced a resurgence after the Spanish Civil War, with over 1500 deaths in 1939-1940) and Turkey.
In contrast to the severe and widespread epidemics of smallpox in Europe after the First World War, only isolated incidents occurred during and after the Second World War. Variola minor was imported into Italy from North Africa in 1944 and produced over 6000 reported cases before it was eliminated in 1947, while variola major occurred in Turkey during the war (over 12 000 reported cases in 1943; see Table 8.18) and extended from there to Greece.
From 1953 onwards Europe was free of endemic smallpox, but countries with colonial possessions in tropical regions-France, Portugal, the United Kingdom, and to some extent Belgium and the Netherlands-were especially liable to importations, rapid aerial transit of infected persons from endemic regions to Europe greatly increasing the hazard. Small outbreaks, often largely hospital-associated, occurred in all these countries (see Chapter 23).
Table 8.4: England and Wales: numbers of reported cases of and deaths from variola major and variola minor, 1911-1958a

United Kingdom
Statistical data for the United Kingdom are provided separately for England and Wales, Scotland and Northern Ireland. Endemic smallpox was eliminated from Ireland in 1907, and subsequent importations were rare and quickly contained. Variola major was prevalent in Scotland from 1900 to 1905, with 6628 cases and 641 deaths, over half the cases occurring in Glasgow. From then on in only one outbreak did the number of cases exceed 80, but there were importations into the east coast ports from northern Europe and into Glasgow from Spain and the USA. Some cases of variola minor occurred in Scotland in 1927-1930 (maximum numbers reported: 154 in 1927 and 146 in 1928) as an extension of the much greater prevalence of the disease in England at that time. However, as is not surprising in view of the relative sizes of the populations of the constituent parts of the United Kingdom, the major brunt of smallpox was borne by England and the data for England and Wales are therefore discussed separately, and in greater detail, below.
England and Wales
Variola major. The last large epidemic of variola major in London occurred in 1901- 1902, with 9496 reported cases and 1543 deaths, and there was an outbreak in Liverpool in 1902-1 903, with 2280 reported cases and 161 deaths. Importations of variola major continued to cause small outbreaks in most years until about 1929, after which they became fewer and were more rapidly controlled. The years 1939-1 945 were characterized by an almost complete absence of smallpox, but there was an upsurge in 1946 and 1947, with many small outbreaks (Table 8.4). Variola major continued to be imported into England more frequently than into any other country of Europe for the whole of the period under review. The overall annual figures given in Table 8.4 do not accurately reflect the frequency of these importations. In 1946, for example, as British soldiers were being repatriated from distant parts of the world and with the post-war entry of students from Africa and Asia, no fewer than 15 separate introductions accounted for the 56 cases reported.
There were two reasons for the frequency with which smallpox was imported into the United Kingdom. The first was the extensive movement to and from endemic areas in Africa and Asia, associated with the country’s imperial role and the traditions of movement that remained in the post-colonial period. The second was the fact, trenchantly criticized in the medical press (see, for example, British medical journal, 1962), that alone of the advanced industrial nations the United Kingdom had no requirement that overseas travellers should carry a valid international vaccination certificate. The latter situation was changed in 1963, when all persons seeking entry to the United Kingdom from an infected local area—in no matter what country—and from all countries of Africa, the Americas (except Canada and the USA) and Asia were required to produce a valid international certificate of vaccination. Especially in the period just after the Second World War, many of the importations were due to mild attacks of modified type variola major in vaccinated servicemen (Murray, 1951). The low community acceptance of vaccination in infancy, even when it had been nominally compulsory (up to 1946), and the failure to vaccinate hospital workers regularly allowed such cases to infect others (especially hospital personnel) and thus to initiate outbreaks.
Variola minor. There were apparently a few small outbreaks of variola minor in England early in the 20th century (Lancet, 1903), one in Nottingham in 1901 being attributed to contaminated fomites sent from Salt Lake City, USA, to a Mormon convention (Boobbyer, 1901), after which it spread to several other cities and then apparently died out. Interestingly, the only 2 importations of variola minor into Oceania—separate episodes in Australia and New Zealand in 1913—were attributed to Mormon visitors. Variola minor first appears to have become well-established in England in 1919 (Copeman, 1920). Once again, it is difficult to trace its first occurrence, since it was often confused with chickenpox, but initially it seems to have been commonest in the north of England, with small pockets in the south. London was first affected in 1928.
Table 8.4 illustrates the remarkable difference in the incidence of variola major and variola minor in England and Wales during the period between the wars. Variola major was eliminated as an endemic disease early in the century, but subsequently often occurred as small outbreaks resulting from importations, which were always rapidly controlled. There were 35 such circumscribed outbreaks, with a total of 268 cases, in 14 out of the 24 years between 1935 and 1958. On the other hand, variola minor was a common endemic disease from 1919 until 1934. When importations of variola minor did subsequently occur, as in 1952 and 1966 (the latter probably laboratory-associated; see Chapter 23), they caused many more cases (135 and 72 respectively) than did the outbreaks of variola major, the largest of which, in 1947, produced 48 cases before being brought under control.
Unquestionably, in the United Kingdom, as in the USA at about this time, the health authorities took variola major seriously and reacted effectively, with surveillance, the isolation of cases and the vaccination of contacts, but they paid relatively little attention to variola minor. It is perhaps not surprising that in the 1970s WHO officials experienced great difficulty in persuading the health authorities in Ethiopia to look upon variola minor as a disease of sufficient importance to make a call on their limited resources (see Chapter 21).
Russia and the Union of Soviet Socialist Republics
Smallpox ravaged European Russia during the early part of the 20th century and was even worse during the misery that accompanied and followed the First World War. Russia was feared by its neighbours as a source of smallpox; ships from Russian ports were a recognized hazard in Scandinavia and most of the cases of smallpox in Germany were in areas near the eastern borders. Indeed in 1910 almost 30% of all cases of smallpox reported in Germany occurred in travellers from Russia (Jones, 1914).
With the establishment of the USSR in 1917, the new government took steps to control smallpox, and vaccination was made mandatory in a decree signed by V. I. Lenin in April 1919. In 1924, the Soviet vaccination law was modified to require vaccination in infancy and the revaccination of teenagers (Kravchenko, 1970). Nevertheless, smallpox continued, with severe epidemics in European Russia in 1931-1933 that led to intensified vaccination campaigns and the elimination of endemic smallpox in 1936 (Vasil’ev & Vasil’ev, 1982). Subsequently, outbreaks following importations were reported in 1950-1952, 1955, 1956 and 1958 (see Table 8.2). The last outbreak occurred in 1960 when an importation from India caused 46 reported cases and 3 deaths in Moscow (Barojan & Serenko, 1961; see Chapter 23).
Germany
The German states had been among the first in Europe to adopt compulsory vaccination and revaccination and the comparative freedom of the Prussian armies from smallpox in the Franco-Prussian War of 1870-1871 testified to the effectiveness of these measures (see Chapter 6). By 1900 vaccination of the civilian population had reached a high level and variola major had ceased to be endemic. However, for economic reasons large numbers of foreign agricultural workers and skilled tradesmen were recruited from Russia, in which vaccination was poor and variola major still common. In consequence, there were many small outbreaks initiated by imported cases.
In the aftermath of the First World War there were outbreaks totalling several thousand cases between 1916 and 1922, when endemic smallpox was again eliminated. In spite of the devastation, there was almost no smallpox in Germany during and immediately after the Second World War, but importations, with limited spread, occurred in 18 of the 36 years between 1922 and 1958.
France
During the early years of the 20th century smallpox was much commoner in France than it was in Germany. Vaccination in infancy was made compulsory in 1902, with provision for revaccination at 11 and again at 21 years of age, but the law was not enforced. Paris and Marseilles were the principal centres of infection, especially Marseilles, the main port of entry for passengers and merchandise from endemic countries of North Africa and Western Asia. One noteworthy advance was in the French army, in which smallpox had been so severe during the Franco-Prussian War. From 1914 to 1917 the army did not report a single case of smallpox.
A few hundred cases were notified almost annually between 1920 and 1936, and minor outbreaks associated with importations occurred in most of the following years (see Table 8.1). There was little smallpox in France during the Second World War, but subsequently, local outbreaks occurred almost every year until 1956, though they were usually quickly contained. Many were very mild, the original cases usually being diagnosed as chickenpox (Fabre, 1948).
Portugal and Spain
During the first quarter of the 20th century Portugal, for long one of the most economically depressed countries of Europe, sustained endemic variola major at a level rivalling that of countries in Africa and Asia at that time (Amaral, 1960). Its larger neighbour, Spain, was not much better off, although the incidence was briefly reduced twice (in 1929 and again in 1937) only to rise again, notably in the aftermath of the Spanish Civil War. Classical variola major occurred throughout this period, but from 1944 to 1948 the overall case-fatality rate was only 3.1% and the reports indicated that both variola major and variola minor were present. Only variola minor occurred after that, until endemic smallpox was eliminated from both countries by the early 1950s.
Scandinavia
Smallpox had been a severe disease in Sweden during the latter half of the 18th century, killing an estimated 10% of the population (see Chapter 6, Fig. 6.1). Compulsory vaccination was introduced in 1816 and greatly reduced the incidence, but endemic smallpox was not eliminated until the end of the 19th century. There were small outbreaks almost every year during the first two decades of the 20th century (Table 8.5), due to importations. In 1917 a substantial outbreak occurred, associated with the passage of war invalids from Russia to Germany, but after 1920 there were cases in only 9 of the 43 years up to 1963, when an outbreak of variola major with 27 cases occurred, which was reported in detail (Strom & Zetterberg, 1966).
Denmark and Norway, smaller countries with less international trade and travel than Sweden, also remained free of endemic smallpox for the whole of the 20th century, but both countries occasionally reported single cases or very small outbreaks associated with importations. The Scandinavian countries provided an example for the rest of the world. Subject to severe endemic and epidemic smallpox before vaccination became available, they eliminated smallpox by the end of the 19th century, and for the most part successfully excluded importations thereafter. When importations did occur, they were usually rapidly controlled.
Table 8.5: Sweden: status of smallpox,1900-1962a

THE ELIMINATION OF SMALLPOX FROM NORTH AMERICA, CENTRAL AMERICA AND PANAMA BY 1951
The incidence of reported cases of smallpox in the USA, Mexico and Canada from 1920 to 1952 is shown in Table 8.6, and in the countries of Central America and Panama in Table 8.7. Two patterns are apparent in North America. The high incidence of smallpox in the USA from the beginning of the century was due mainly to variola minor with occasional outbreaks of variola major due to importations, and the situation was similar, on a smaller scale, in Canada. In Mexico, however, variola major occurred as a widespread disease from the beginning of the century, as it had during previous centuries (see Chapter 5). Variola minor was periodically introduced into Mexico from the USA but seems never to have become established there. Endemic smallpox was eliminated from all 3 countries by 1952.
Central America and Panama
Early records are sparse for the 7 small states constituting Central America and Panama, located between Mexico in the north and Colombia in the south (see Fig. 8.6), but variola major appears to have been present in most of them during the early years of the 20th century (Low, 1918). However, from 1920 onwards most of these countries were free of endemic smallpox, although there were importations and outbreaks extending over several years in the more populous countries until the mid-1950s (Table 8.7).
Table 8.6: North America: numbers of reported cases of smallpox, 1920-1952a,b,c

a No cases were reported from any of these countries after 1951, except for I imported case in Canada in 1962.
b A horizontal line beneath a figure Indicates that this represents the last probable occurrence of endemic smallpox.
c .. = data not recorded.
d Only deaths (figures in italics) were reported between 1922 and 1943.
Table 8.7: North America: numbers of reported cases of smallpox, 1920-1952a,b,c
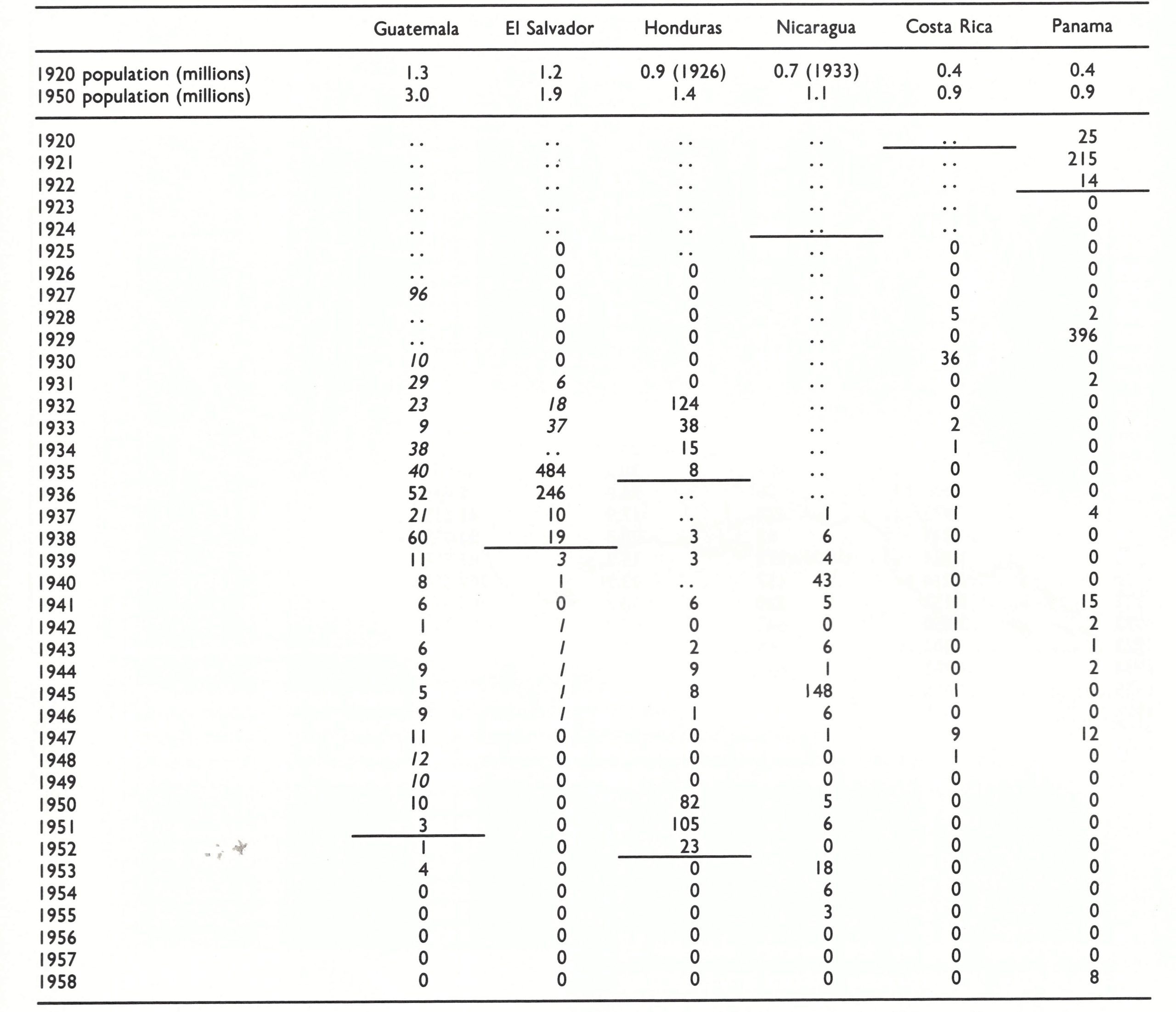
a horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b .. = data not recorded.
c Figures in italics denote the number of reported deaths from smallpox.
United States of America
The history of smallpox in the USA in the period under review is dominated by the appearance of variola minor in Florida in about 1896 and its subsequent spread throughout the country and into Canada. This has been discussed at length by Chapin (1913,1926) and Chapin & Smith (1932); the decline of smallpox after 1930 has been described by Dauer (1940). Table 8.8 sets out the numbers of reported cases of and deaths from smallpox from 1900 until the last cases occurred in 1949. The subdivision of annual totals of cases and deaths into variola major and variola minor derives in the main from Chapin & Smith (1932), who explored many sources in order to make their judgements about the variety of smallpox (“mild” or “severe”) responsible for various outbreaks. Variola major prevailed throughout the USA until the summer of 1897 but by then had disappeared from the country except for about 100 cases, with 30 deaths, which occurred in 16 different states. These local outbreaks were efficiently controlled, and endemic smallpox appeared to have been eliminated (Chapin, 1913). However, during the first half of 1897 there were 54 cases of smallpox in Pensacola, Florida, and many more in the county in which Pensacola is situated, without a single death. From here the mild variety of smallpox, variola minor, spread through Florida, and in the year ending 31 March 1898, 3638 cases were reported, with only 51 deaths (case-fatality rate, 1.4%). Within a period of 4 years variola minor extended gradually over the whole of the continent north of the Mexican border (Fig. 8.4).
Table 8.8: United States of America: numbers of reported cases of and deaths from variola major and variola minor, 1900-1950a
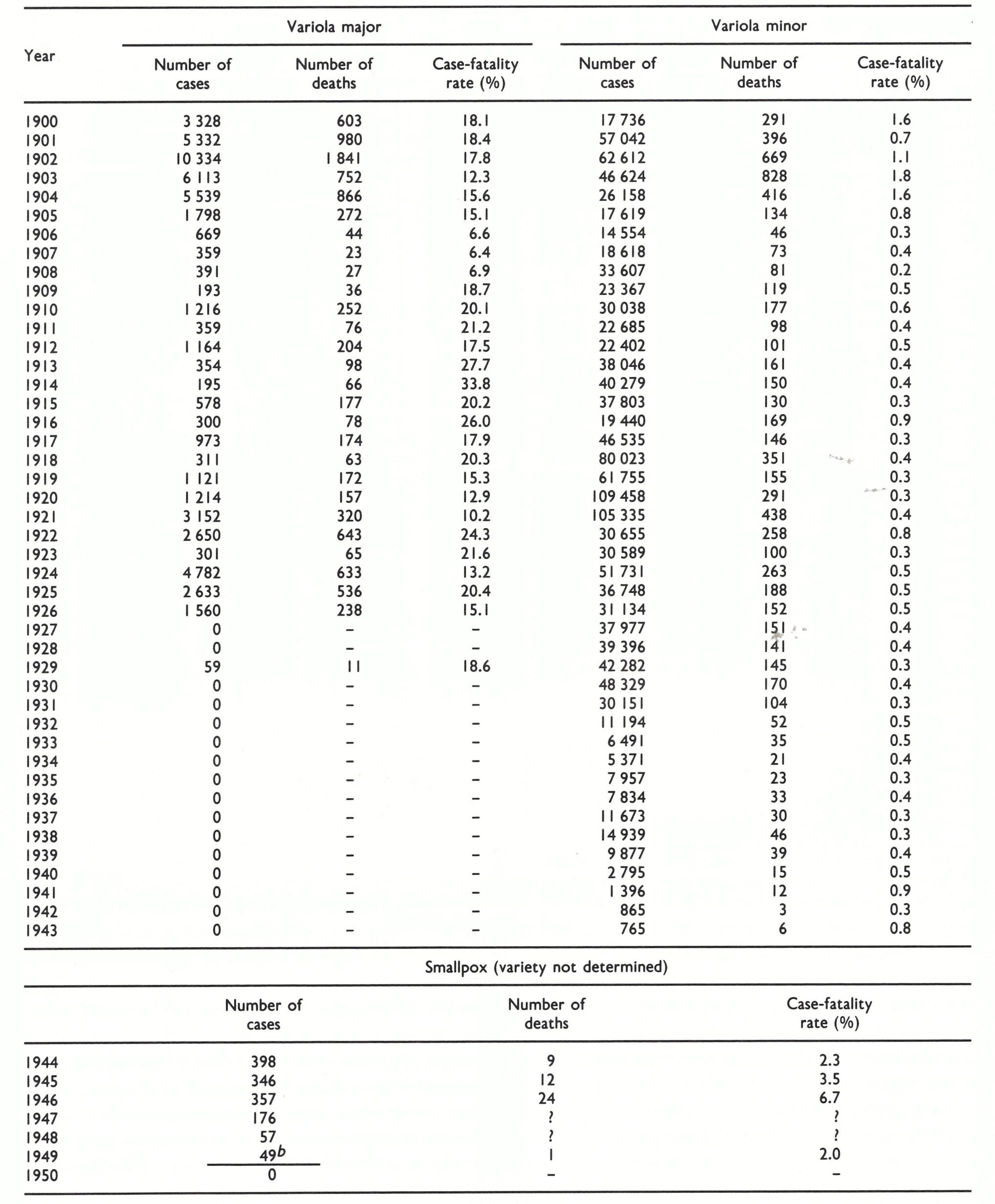
a Based on Chapin & Smith (1932) and relevant issues of public health reports.
b The last probable occurrence of endemic smallpox.

Fig. 8.4. The spread of variola minor in the USA. It was first observed in Pensacola, Florida, in 1896. Figures in circles indicate the number of years elapsed between 1896 and the detection of cases in various cities in the USA including Alaska and in Canada. Arrows indicate directions of spread, when this could be determined, except for towns along the Mississippi, where the river was the route of spread. (Based on Chapin. I9 13.)
Plate 8.1. Charles Value Chapin (1856-1941) was Superintendent of Health of Providence, Rhode Island (USA), from 1884 to 1932. A nationally renowned figure, he imaginatively translated newly emerging concepts of the epidemiology of infectious diseases and methods for their prevention into public health administrative practice.
The substrain of variola minor that was later called “alastrim” (see Chapter 2) remained the dominant form of smallpox in the USA thereafter. The number of cases notified each year represents at most 20% of those that actually occurred; many patients did not see a physician and many others who did were not reported as having smallpox. From the USA alastrim was exported to the United Kingdom (in 1902 and again in 1919), and to Brazil (1910), Australia (1913), New Zealand (1913) and the Philippines (about 1920). Against the background of endemic alastrim, repeated introductions of variola major occurred, mostly from Mexico (14 out of 23 outbreaks between 1915 and 1929) but also from Canada and overseas countries, especially Europe, during the early years of the century.
Chapin & Smith (1932) examined the detailed reports of as many outbreaks of variola major (the “severe type” of smallpox) as they could, in order to determine whether variola minor (the “mild type”) ever gave rise to variola major. Their conclusion was that each variety of smallpox was due to a different subspecies of variola virus and that these “bred true”. Subsequent experience in many parts of the world has confirmed this conclusion.
Although some cases of variola major were reported every year from 1900 until 1927, there were only 2 major outbreaks during this period. The first, in 1902-1903, affected particularly Boston, New York, Philadelphia, New Jersey and Ohio; variola minor was then prevalent in the Mid-West. The last large epidemic of variola major in the USA occurred in 1924-1925, when some 7400 cases were reported, over one-third of them in 4 cities: Cleveland and Toledo (Ohio), Detroit (Michigan) and Pittsburgh (Pennsylvania).
Vaccination played an important role in both the progressive fall in the incidence of smallpox and in the replacement of variola major by variola minor. The virtual disappearance of variola major and the mild nature of variola minor led to the emergence of antivaccinationist sentiments, although in 1922 the United States Supreme Court had ruled that school authorities had the right to require vaccination for admission to school (Vaughan, 1923). By the 1930s, 4 states of the USA had laws prohibiting compulsory vaccination, 28 states had no vaccination laws, 6 provided for local option and 10 had compulsory vaccination laws. The relation between the legal situation and the incidence of variola minor is illustrated in Fig. 8.5.

Fig. 8.5. The effect of vaccination laws on the incidence of smallpox in various states of USA, 1919-1928. (Based on Woodward & Feemster, 1993.)
In the year 1927, for the first time, no case of variola major was reported in the USA, and apart from an outbreak in 1929 no further cases were notified until 1946. In that year a soldier returning from Japan introduced smallpox into Seattle, Washington, which resulted in an outbreak of 51 cases, with 16 deaths (Palmquist, 1947). In 1947 a man with undiagnosed haemorrhagic smallpox died in a Manhattan, New York, hospital. Twelve other persons were infected and in the panic occasioned by this outbreak over 6 million New Yorkers were vaccinated (Weinstein, 1947). The last outbreak of smallpox in the USA occurred in Texas in 1949 (8 cases with 1 death), probably after importation from Mexico.
Although variola major was eliminated as an endemic disease in 1927, variola minor continued to be common in states without compulsory vaccination laws. Reporting methods changed in 1944, and it is impossible to get an accurate picture of the elimination of variola minor from the USA. Although grossly underreported when it was common, it was probably incorrectly diagnosed and reported during the few years just before and after its elimination from the USA, during the latter half of the 1940s.
In the year 1927, for the first time, no case of variola major was reported in the USA, and apart from an outbreak in 1929 no further cases were notified until 1946. In that year a soldier returning from Japan introduced smallpox into Seattle, Washington, which resulted in an outbreak of 51 cases, with 16 deaths (Palmquist, 1947). In 1947 a man with undiagnosed haemorrhagic smallpox died in a Manhattan, New York, hospital. Twelve other persons were infected and, in the panic, occasioned by this outbreak over 6 million New Yorkers were vaccinated (Weinstein, 1947). The last outbreak of smallpox in the USA occurred in Texas in 1949 (8 cases with 1 death), probably after importation from Mexico.
Although variola major was eliminated as an endemic disease in 1927, variola minor continued to be common in states without compulsory vaccination laws. Reporting methods changed in 1944, and it is impossible to get an accurate picture of the elimination of variola minor from the USA. Although grossly underreported when it was common, it was probably incorrectly diagnosed and reported during the few years just before and after its elimination from the USA, during the latter half of the 1940s.
Canada
The situation in Canada reflected that in the USA, with variola minor as the commonest form of smallpox after it became established there early in the century. However, control by vaccination was more easily achieved in this less populous country and endemic smallpox was eliminated by 1944.
Mexico
The situation in Mexico in the earlier part of the 20th century contrasted starkly with that in Canada and the USA. Mexico had a population of about 14 million in 1920 and between 5000 and 13 000 smallpox deaths were reported every year in the 1920s (see Table 8.6), at that time the highest reported incidence in any country in the world (Hedrich, 1936). Variola minor appeared in Mexico in 1932, probably after importation from the USA, but it did not displace variola major, which caused a major epidemic with over 8000 deaths in 1942-1943. This led to an increased emphasis on vaccination, which became possible in many rural areas because of the development of roads. There was a rapid fall in the number of reported cases of smallpox, which continued to be of the variola major variety, and a change was made in reporting, from “deaths” to “cases” (see Table 8.6). The last case of smallpox in Mexico occurred in 1951, just after the Pan American Health Organization had launched its programme to eradicate smallpox from the Western Hemisphere (Rodrigues, 1975).
SMALLPOX IN SOUTH AMERICA, 1900-1958
Variola major was endemic in all the larger countries of South America during the first decade of the 20th century (Fig. 8.6), with the highest incidence in Brazil and Chile (Table 8.9). Reporting was very poor; indeed, many countries concealed the existence of smallpox for fear of the imposition of quarantine restrictions by their neighbours (Low, 1918).
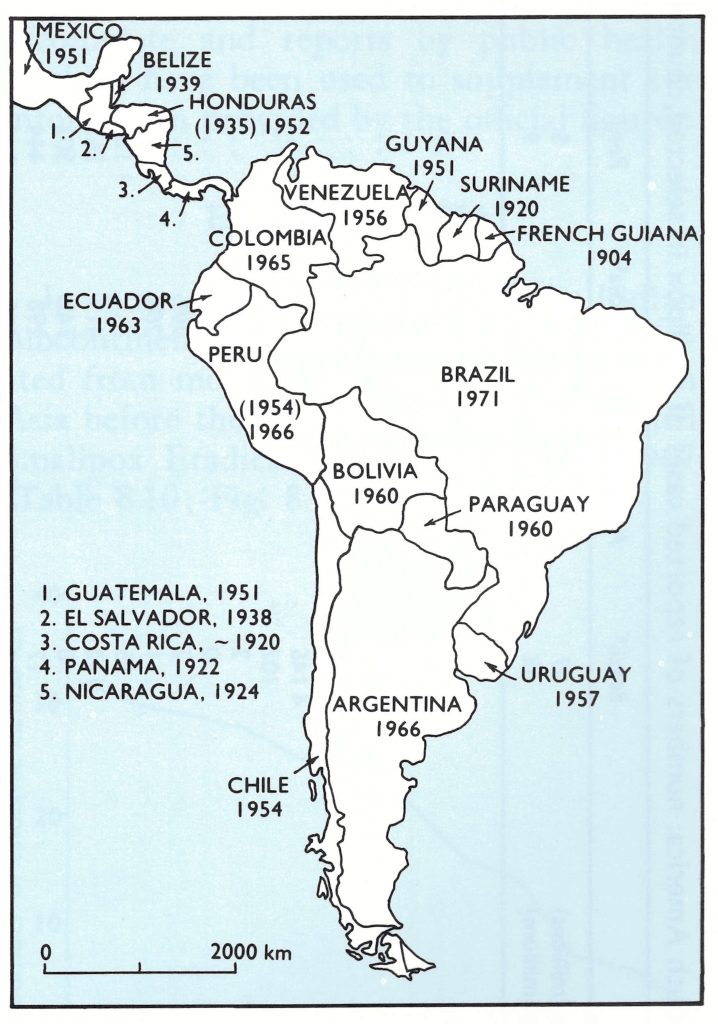
Fig. 8.6. Mexico, Central and South America: year in which smallpox ceased to be endemic in each country (national boundaries as of 1982). Dates in parentheses (for Honduras and Peru) indicate the initial elimination of endemic smallpox, after which endemicity was again established before final elimination in the year shown.
Table 8.9: South America: numbers of reported cases of smallpox in selected countries, 1920-1958a,b

In 1910 variola minor was reported from South America for the first time, in Brazil, where eventually it displaced variola major, which remained common in Argentina and Chile in the 1920s. Epidemics of variola major were reported in Colombia in 1943 and 1947, in Bolivia in the 1940s, and in Ecuador up to 1962. The last large outbreak of variola major in South America caused nearly 10 000 deaths in Peru in 1941-1943. Within a few years of the decision by the Pan American Sanitary Organization in 1950 to eradicate smallpox from the Western Hemisphere, Peru, Uruguay and Venezuela had eliminated the disease. Bolivia, Colombia, Ecuador and Paraguay followed in the early 1960s. By 1967, smallpox was still endemic only in Brazil, although there were importations from Brazil into Argentina, French Guiana and Uruguay after that date (Fig. 8.7).
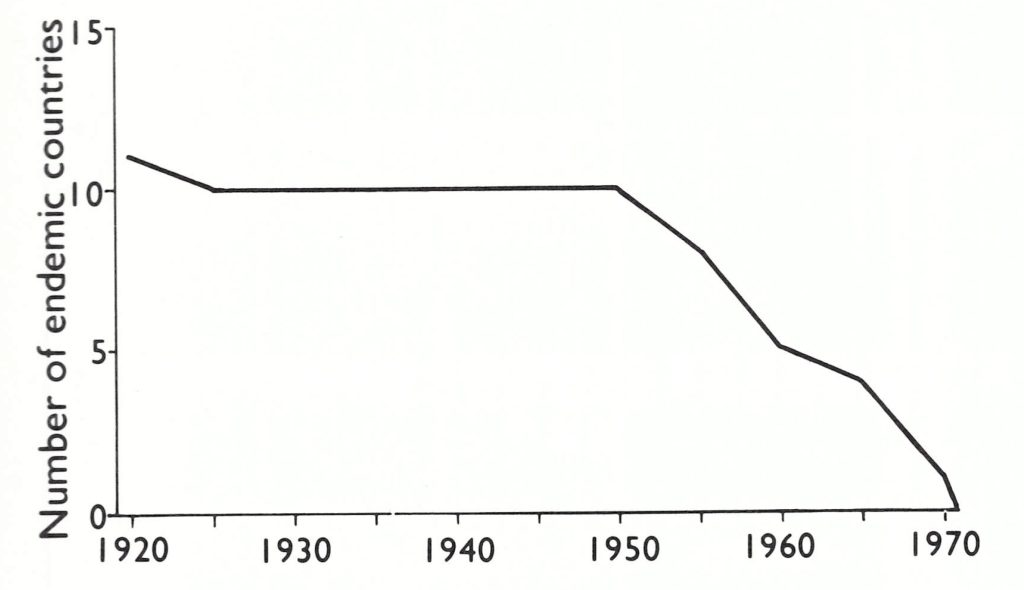
Fig. 8.7. Number of countries of the 13 in South America in which smallpox was endemic at various times between I920 and I97 I. National boundaries as of 1982.
Brazil
By far the largest and most populous country in South America, Brazil experienced severe epidemics of variola major early in the 20th century. Following a major epidemic in 1904-1905 (3800 deaths in Recife; 3600 deaths in Rio de Janeiro) the Brazilian government passed a bill requiring compulsory vaccination, but an antivaccination campaign led to open revolt with riots. Large epidemics with many deaths occurred in 1907-1910.
Variola minor was introduced into Bahia from the USA in about 1910, whence it spread to the southern states of Brazil and eventually throughout the country, producing an estimated 250 000 cases in 1910-1911 (Aragao, 1911). During the outbreak in Parani in 1910, some 6000 persons were infected, but the case-fatality rate was only 2.3% (Carini, 1911). Mortality data over the next 20 years show that variola minor gradually replaced variola major as the commoner form of smallpox in Brazil, but as late as 1926 an epidemic of variola major in Rio de Janeiro caused 2200 deaths.
Although there were very few notifications over a period of several years in the late 1920s and early 1930s, variola minor had become established as an endemic disease and several thousand cases were notified every year from 1955 onwards. Further, Brazil became a major source of transmission of the disease to neighbouring countries, especially Argentina, a risk which continued until smallpox was finally eradicated from Brazil and thus from the whole Western Hemisphere in 1971.
Other Countries
In most of the other countries of South America variola major was common and severe during the first two or three decades of the 20th century and was then replaced by variola minor. The latter declined in incidence and was finally controlled in the 1950s and 1960s (Fig. 8.6), although importations from Brazil continued to occur. Ecuador was unusual in that variola major persisted at a relatively high level until the early 1960s.
SMALLPOX IN ASIA, 1900-1958
Asia is by far the most heavily populated continent, and China and India, vast countries with weak national public health services during the early part of this century, have long been regarded as the traditional homes of smallpox. The decline in the number of endemic countries in Asia since 1920 is shown in Fig. 8.8. Asia was the major focus of variola major throughout the first half of the 20th century, and until about 1950 smallpox was endemic in all the more populous countries of the continent. In order to simplify discussion of this vast region, the data on eastern Asia, the Indian subcontinent and Afghanistan, and south-western Asia have been summarized separately.
Though the records of smallpox in many countries of Europe during the first half of this century are incomplete and seriously underestimate the incidence, they are very much better than those of any other countries except Australia, Canada, Japan, New Zealand and the USA. Data for China and the countries between China and India are very incomplete and reports by public health workers have been used to supplement the information provided by the official figures.
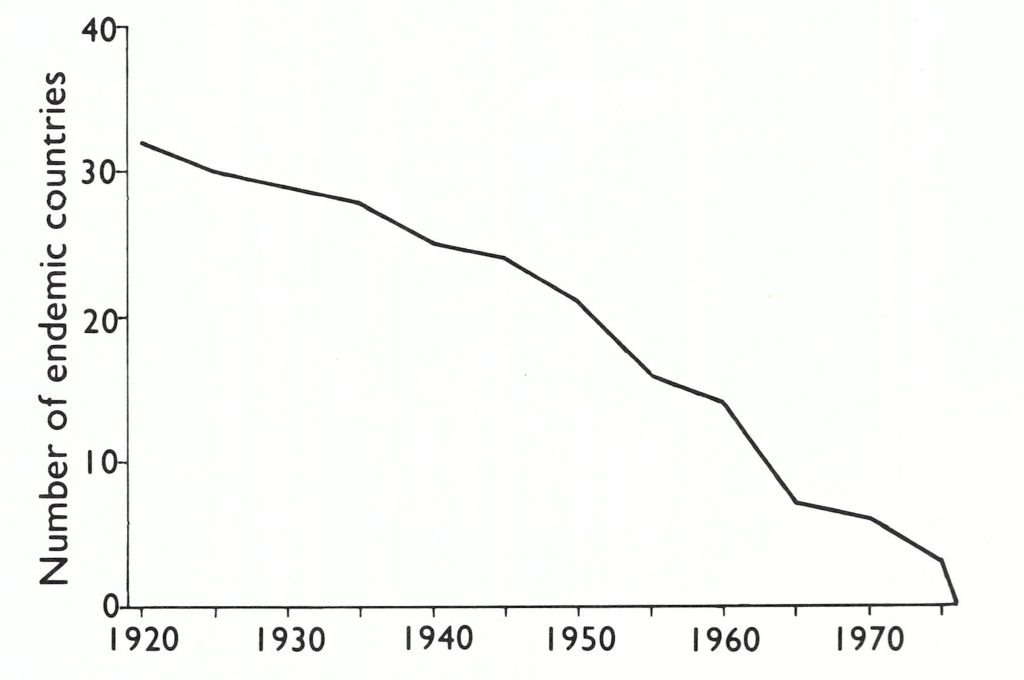
Fig. 8.8. Number of countries of the 38 in Asia in which smallpox was endemic at various times between 1920 and 1975. National boundaries as of 1982.
EASTERN ASIA
Asia is by far the most heavily populated continent, and China and India, vast countries with weak national public health services during the early part of this century, have long been regarded as the traditional homes of smallpox. The decline in the number of endemic countries in Asia since 1920 is shown in Fig. 8.8. Asia was the major focus of variola major throughout the first half of the 20th century, and until about 1950 smallpox was endemic in all of the more populous countries of the continent. In order to simplify discussion of this vast region, the data on eastern Asia, the Indian subcontinent and Afghanistan, and south-western Asia have been summarized separately.
Though the records of smallpox in many countries of Europe during the first half of this century are incomplete and seriously underestimate the incidence, they are very much better than those of any other countries except Australia, Canada, Japan, New Zealand and the USA. Data for China and the countries between China and India are very incomplete and reports by public health workers have been used to supplement the information provided by the official figures.
Table 8.10: Eastern Asia: numbers of reported cases of smallpox in selected countries, 1920-1966a,b

Table 8.10: Continue...

a A horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b...= data not recorded.
c Figures in italics denote the number of reported deaths from smallpox.
d Comprising present-day Democratic Kampuchea, Lao People's Democratic Republic, and Viet Nam.
e From 1951 onwards, the figures refer only to the Republic of Korea.
f Including Singapore.
g In Annex I of the Final Report of the Global Commission for the Certification ofSmallpox Eradication (World Health Organization, 1980), the figure given for 1949 is 490 348. This seems an unlikely figure for the number of reported cases at that time (see Chapter 13). It derives from Henneberg (1961) and is not supported by data in the Epidemiologic and vital statistics report, from which the figures in this table were derived.
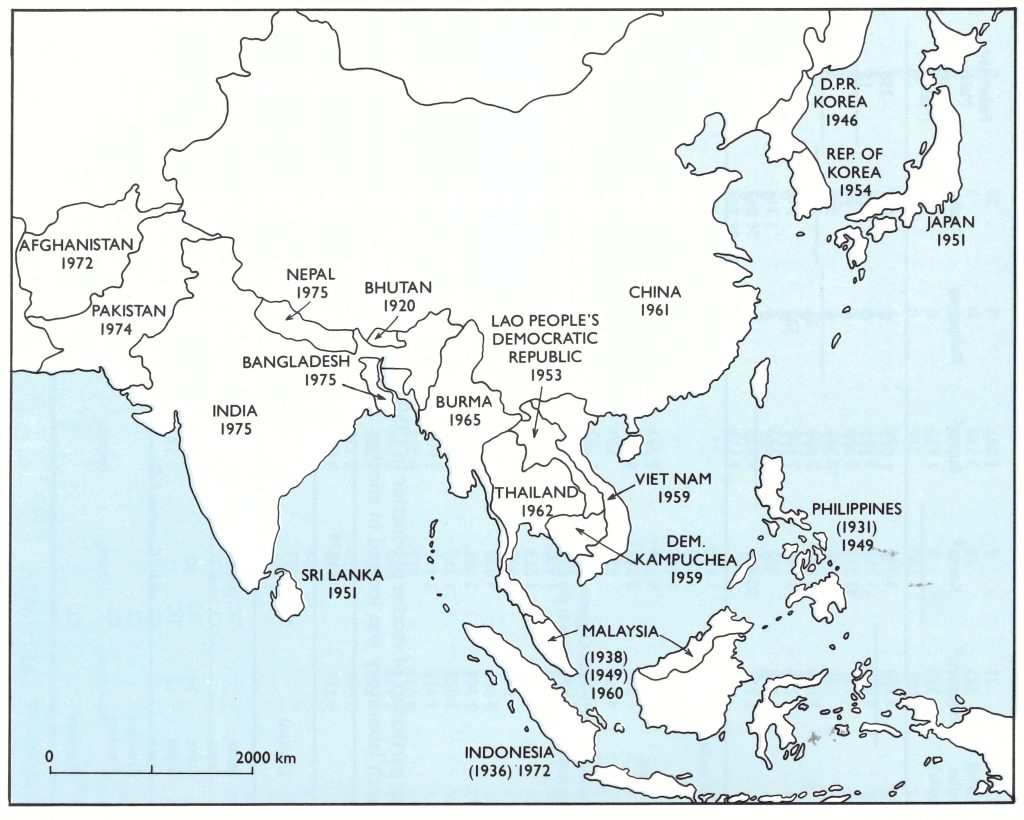
Fig. 8.9. East and South-East Asia: year in which smallpox ceased to be endemic in each country (national boundaries as of 1982). Dates in parentheses (for Indonesia. Malaysia and the Philippines) indicate the initial elimination of endemic smallpox, after which endemicity was again established before final elimination in the year shown.
For the first 3 decades of the 20th century smallpox was endemic throughout the mainland countries of eastern and south-eastern Asia, in Japan and in the larger island groups. Tibet, in which vaccination was not practised at all until 1940, suffered very severely, leading to the depopulation of some areas, and in China smallpox was regarded as something that every child had to get sooner or later. However, although there were still some severe epidemics, the incidence of smallpox declined in Japan, and notable early successes in eradication were recorded in the Philippines in 1931 and in the Netherlands East Indies (Indonesia) and the Federated Malay States (Malaysia) later that decade.
The disruption of services that accompanied and followed the Second World War led to a reappearance or resurgence of smallpox in several countries of eastern as well as of southern Asia. In Thailand, in which the annual number of reported cases had been less than 1000 for many years, there was a major epidemic in 1945-1946, with more than 62 000 reported cases. Smallpox was reintroduced into Malaysia in the early 1940s and was not eliminated until 1949, and into the Philippines in 1948, but was eliminated again in 1949. Over 20 000 cases were notified in Korea in 1946, and a major epidemic, with upwards of 43 000 cases, occurred in 1951, during the hostilities in that country. The incidence in Japan rose to 17 800 in 1946, and smallpox was reintroduced into Indonesia in 1947, reaching epidemic proportions in 1949.
The fact that smallpox had been eliminated in Europe and North America was a powerful stimulus for the declaration by the World Health Assembly in 1959 that global eradication was a goal that could be achieved. Although it was not fully appreciated, even more impressive achievements—and more relevant to the eradication of smallpox from the impoverished countries of Africa and the Indian subcontinent—were then in progress in China, the Korean peninsula and the countries of Indochina. The elimination of the disease in China will be described in some detail, since it ranks with eradication from India as one of the most significant achievements in the struggle against smallpox. Aspects of importance in the certification of smallpox eradication in China are described in Chapter 27.
China
Smallpox was highly endemic throughout China for the first 4 decades of the 20th century, but no data were recorded except for the Treaty ports, from which most of the early figures in Table 8.1 0 were derived. Even here, they were gross underestimates. In Shanghai, as in the rest of China, smallpox was a seasonal disease, with a high incidence in winter and spring (from December to the end of May) and a low incidence during summer (Dold, 1915; Xu & Jiang, 1981). The disease was endemic, with epidemics in 1902,1904,1907, 1910 and 1913 (Dold, 1915) and between 1930 and 1951 there were epidemics in 1930-1934,1936-1939,1946-1948 and 1950-1951. Anecdotal data (Korns, 1921) reveal that smallpox was still well-nigh universal throughout China in the early 1920s; of 3020 adult males whom Korns questioned in an outpatient clinic, only 40 of 822 who had not been vaccinated had escaped the disease. Chinese with obvious pockmarks were very common in the streets of every city.
Variolation was practised on a small scale from about the 10th century (Needham, 1980) until the 1960s; outbreaks of smallpox in northeastern Yunnan Province in 1958 and in Nei Monggol Autonomous Region (Inner Mongolia) and Shanxi Province in 1963-1965 were attributed to variolation (see Chapter 27). From 1803 vaccination was occasionally available for those who could afford it. There were attempts to promote vaccination, notably after the establishment of the First Republic in 1913, but it was not practised at all extensively until the national smallpox eradication programme was instituted by the People’s Republic of China in 1950.
Immediately after Liberation in 1949 a national campaign was launched to eradicate smallpox from China. The data published in European languages are very limited (SME/79.10; SME/79.11, Fenner & Breman; WHO/SE/79.142 Rev.1; WHO/SE/79.151; Xu & Jiang, 1981), but give some impression of the nature and progress of this campaign. A particularly interesting feature was that eradication was achieved in all the cities and larger towns within 5 years, and throughout the country in 11 years, by the vigorous prosecution of mass vaccination, using liquid vaccine.
In October 1950, the State Council of the Central Government issued a “Notice on the Campaigns for Smallpox Vaccination of Autumn 1950” which expressed the formal decision to carry out a mass vaccination campaign for the whole population of mainland China. At the same time, the Ministry of Health announced “Temporary Regulations for Smallpox Vaccination”, ruling that all children should be vaccinated 6 months after birth and revaccinated at the ages of 6,12 and 18 years. The scheme of operation was developed by the Ministry of Health and comprised a massive propaganda campaign to enlist the support of the population (a “Mass Patriotic Health Movement”), the organization of the production and distribution of vaccine from 5 vaccine institutes located in various parts of the country, the mobilization and training of vaccinators and an intensive effort to achieve universal vaccination, mostly during the year 1951. The scheme also involved measures to control the possible spread of smallpox by travellers within China, by rail, sea and river (see below).
The 5 vaccine institutes, which produced liquid calf vaccine of the Temple of Heaven strain (see Chapter l l ), were located in Beijing, Shanghai, Dalian (Dairen), Kunming and Lanzhou. There were initially some difficulties in producing enough vaccine for the campaign. Later some of these institutes ceased production, and new production centres were established (Table 8.11). Meetings were held to improve various aspects of vaccine production and eventually (after eradication had been achieved) freeze-dried vaccine was produced for use in border and tropical areas. Vaccination was carried out by multiple pressure or the scratch technique, in 2 sites. The annual numbers of vaccinations performed throughout China during and immediately after the eradication campaign are suggested by the numbers of doses of vaccine issued (Table 8.12).

Fig. 8.10. China, showing the neighbouring countries and the provinces, autonomous regions and municipalities (internal boundaries as of 1985). The stippled area indicates regions where the population density is over 100 persons per square kilometre.
Table 8.11: China: locations of smallpox vaccine production institutes and other particulars of vaccine production in 1950, when the national smallpox eradication campaign commenced, and in 1979. (The central assay and research laboratory was located in another institute in Beijing.)

a CL = calf lymph; TC = tissue culture; F-D = freeze-dried.
b Municipality.
Table 8.12: China: numbers of doses of smallpox vaccine issued, 1950- I963a

a From WHO/SE/79.142 Rev. 1.
In 1955, following the endorsement by the State Council of the Central People’s Government, the Ministry of Health produced a booklet, Methods of Control of Communicable Diseases, which provided for the compulsory notification of 24 diseases including smallpox. Between 1955 and 1958 a second country-wide mass vaccination campaign was undertaken, with technical aid provided by the USSR under the Socialist Pact of Friendship of 15 February 1950. This highly organized campaign operated airlifts in remote regions and was assisted by large numbers of personnel from Czechoslovakia and Hungary. However, relations with the USSR gradually deteriorated with disagreements on borders and ideology, and by 1961 the assistance agreements had been cancelled.
The number of administrative divisions reporting cases dropped from 21 in 1953 to only 1, Yunnan, in 1959 (Table 8.13), although cases occurred in 2 localities in Xizang Autonomous Region (Tibet) in 1960 and there were importations from Nepal in 1962 and 1964. Smallpox remained endemic in the southwest part of Yunnan, where there was a common border with Burma, until 1961 (see Chapter 27).
Table 8.13: China: numbers of smallpox cases reported, 1950- 1965, by administrative divisiona,b,c

a No cases reported after 1965.
a Data from Jiang (I 985; and personal communication, 1987).
c...= data not recorded.
d Importations.
Information that only became available very recently (Jiang Yutu, 1985; and personal communications, 1984, 1987) reveals that smallpox continued to occur in China until 1965. In 1962, 6 years after the last reported case in the Nei Monggol Autonomous Region, 1 case was reported there, and in 1963 an outbreak of 283 cases occurred in Nei Monggo1 and nearby counties of Shanxi Province, with a further 30 cases in 1964. Another small outbreak (4 cases) occurred in Shanxi in 1965. Both the 1962-1964 and the 1965 outbreaks were attributed to the activities of variolators (see Chapter 27).
In 1959, because several outbreaks of smallpox had occurred following the importation of cases from neighbouring countries into China, it was decided to implement another general mass vaccination campaign. This began in 1960 and aimed to reinforce the achievement of the virtual elimination of smallpox and to raise the level of herd immunity and thus prevent the transmission of smallpox in the event of its importation into the country. Border areas were given first priority.
The method of implementation of the mass vaccination campaigns, in 1949-1952, 1955-1958 and in 1960, was unique. A directing committee of leaders was organized by the joint efforts of the health authorities and epidemic prevention departments in every province, municipality, and autonomous region. The committee was responsible for the organization of local health personnel and the training of medical and paramedical workers to form vaccination teams and perform the vaccinations. The teams went to each village or courtyard to vaccinate all persons, using the lists of names of members of the brigade or courtyard. Children in kindergartens and schools were vaccinated at these locations. During the first visit it was possible to vaccinate nearly 90% of the people. Others were vaccinated in the health centres or polyclinics. Members of governmental bodies, institutions, factories, etc., were vaccinated in health service facilities located at their place of work. After the communes were established in 1958, monthly payments by the State were linked to evidence of vaccination of the family head and family members.
No general account of the country-wide smallpox eradication campaign in China has been published, but operations in the country’s largest city and centre of communications, Shanghai, have been described (SME/79.11, Fenner & Breman; Xu & Jiang, 1981) and provide an idea of how the programme operated there and elsewhere. Details of special surveys made in Yunnan Province and in Xizang (Tibet) for certification purposes are described in Chapter 27.
Shanghai municipality
Smallpox had always been endemic in Shanghai, with frequent epidemics, and before the eradication campaign was launched the overall vaccination rates were low (Table 8.14). A severe epidemic began in December 1950,2 months after the promulgation of the eradication campaign. Although deaths and especially cases were underreported, 3167 cases and 1482 deaths were recorded for the 5 months December 1950 to April 1951.
Table 8.14: Shanghai: smallpox vaccination, 1946-1951a

a From Xu 8 Jiang (1981).
b Includes visitors, travellers, and persons vaccinated more than once.
The aim of the campaign in Shanghai was to vaccinate at least 95% of the population in the shortest possible time. In order to accomplish this, 6944 medical and paramedical personnel were organized into 1319 permanent stations and 1836 mobile vaccination teams. The personnel, comprising 3173 doctors of Chinese traditional medicine, 2067 doctors of Western medicine, 455 nurses and midwives, 1126 medical students, and 123 others, were given a short training course in order to standardize the vaccination technique. The mass vaccination campaign began in March 1951. As the number of vaccinations rose (Table 8.15) and the weather became hotter, the incidence of smallpox fell. The last case in Shanghai was reported on 26 July 1951.
During the early 1950s there was little international travel through Shanghai, but it was a major national communications centre, by sea, river, road and rail. The Quarantine Service was organized to cope with travellers by boat and train to other parts of China, as well as with boat-dwellers on the Huangpu and adjacent rivers. In the case of travellers by boat, ships’ crews were mobilized to assist the campaign by propaganda and by forming “health groups” among them. Crew members were urged to report all cases of smallpox, among passengers or crew. An elaborate system was developed for supervising the issue of internal vaccination certificates for both boat and train travellers within China, with facilities for immediate vaccination if necessary.
Among the boat-dwellers on the Huangpu, in all 76 221 vaccinations were performed in 1951. Nine cases of smallpox were discovered on 5 boats; all case contacts were vaccinated, and no other cases occurred. Among travellers and boat crews, 785 321 persons were vaccinated. On the 3576 boats that left Shanghai in 1951, 7 cases of smallpox were detected among passengers before boarding and 28 after boarding. In the first 4 months of 1951, 72 cases of smallpox were detected among intending train travellers. The effectiveness of this system of surveillance of travellers within China was demonstrated by the fact that although there was a major epidemic in Shanghai at the time, there was little apparent spread to other parts of China.
Table 8.15: Shanghai: cumulative proportion of vaccinations relative to population and the incidence of smallpox in 1951a

a From Xu B Jiang (1981).
b Includes visitors, travellers and persons vaccinated more than once.
Japan
Smallpox was endemic in Japan during the latter part of the 19th century, and during the early 20th century the country was constantly exposed to the risk of imported cases, owing to its large maritime trade and its proximity to China, Korea, Manchuria and Siberia, in all of which smallpox was a common disease at that time. Table 8.16 sets out the numbers of reported cases of and deaths from smallpox in Japan between 1892 and 1915.
Institutes for the production of vaccine in calves had been operating in Japan since 1874, and in 1891 arm-to-arm vaccination was prohibited. In 1896 celebrations were held in Ueno Park in Tokyo to mark the centenary of Jenner’s discovery, and at about this time the famous bacteriologist Kitasato made important contributions to the preparation of bacteriologically sterile vaccine and helped to promote its use (Soekawa, 1984). In consequence of the gradual extension of vaccination the incidence of the disease fell. There was a severe epidemic in 1908, but thereafter smallpox continued to decline. In 1918 vaccination was made mandatory for all 1-year-old children and revaccination was carried out at school entry. The incidence fell further, and between 1927 and 1944 only 5412 cases were reported (see Table 8.10). With the ending of the Second World War and the repatriation of Japanese soldiers, smallpox broke out again, with 1614 reported cases in 1945 and 17 800 in 1946. Shortly after this, control measures were further strengthened and smallpox ceased to be endemic in Japan in 1951.
Table 8.16: Japan: numbers of reported cases of and deaths from smallpox, 1892- 1915a,b
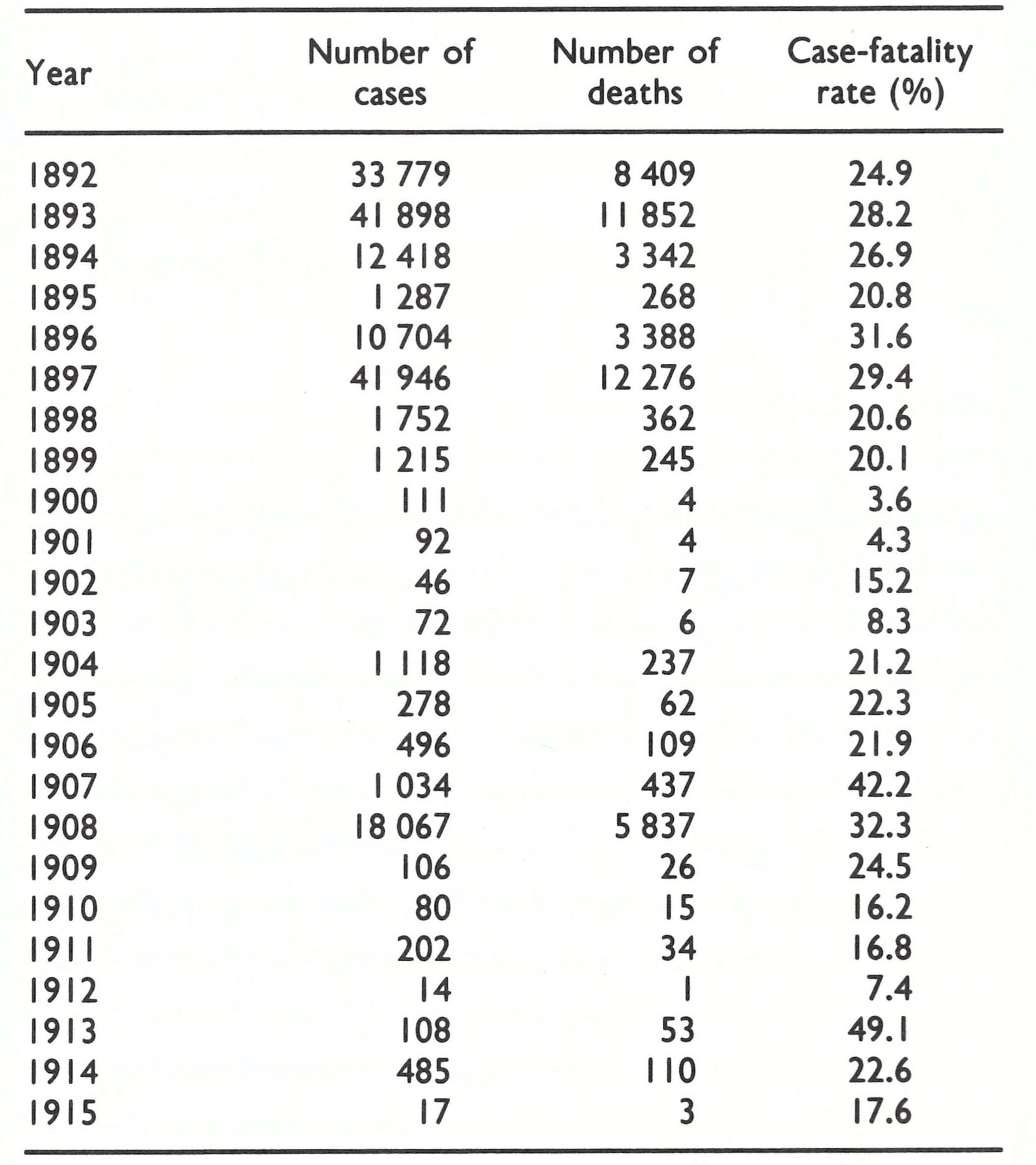
a Based on Low (1918).
b Population of Japan in 1913: 53 million.
Korea
Korea was for several centuries an independent state within the Chinese cultural orbit, and its history of smallpox parallels that of China. In 1910 it was formally annexed by Japan, having for the 5 preceding years been a virtual protectorate of that country, but after the defeat of Japan in the Second World War, Korea was divided at the 38th parallel of latitude and separate governments have operated in the north and the south since 1953. During the period in which it was under Japanese control (1 905-1945) the enforcement of country-wide vaccination reduced the prevalence of smallpox, but variola major remained endemic, with case-fatality rates in different outbreaks varying between 20% and 27%. There was a more severe epidemic than usual in 1940-1941, and the disruption after the Second World War led to a major exacerbation in southern Korea, with over 20 000 reported cases in 1946 and over 43 000 cases in 1951, during the hostilities (see Table 8.10). The situation was rapidly brought under control after the conclusion of the conflict, and endemic smallpox was eliminated in 1954.
Indonesia
Severe outbreaks of smallpox occurred in various parts of the Netherlands East Indies in the early part of the century, an outbreak in Borneo claiming 3000 lives in 1905 and another, in Java, in 1913, causing more than 18 000 cases, with 5000 deaths. A severe outbreak occurred in Java in 1918-1919 and during 1922 and 1924 it spread to the outer islands, the south-eastern part of Borneo and the east coast of Sumatra.
In the early 1920s several thousand cases were reported annually, mostly in Java, but the incidence declined steadily after 1926 (see Table 8.10). Polak (1968) attributes the fall to more complete and effective vaccination coverage of the population, which was achieved by a combination of administrative and technical factors. Administratively, a system of concurrent primary vaccination and revaccination, which had led to repeated revaccination of readily accessible subjects and inadequate primary vaccination coverage of infants, was replaced by a dual system with an allocated time for each. Primary vaccination of children aged 3-6 months was carried out by locally based vaccinators during the first 8 weeks of each quarter, and revaccination of the older population was performed during the last 5 weeks. Arrangements for supervision were also greatly improved. The main technical advance was the production by Otten (1927) of a stable air-dried vaccine for use in remote areas (see Chapter 7, Plate 7.3A). The control of smallpox did not depend just on mass vaccination, however, because it was the practice of the Dutch at that time vigorously to contain such outbreaks of smallpox as were found.
After 1933, about 10% of the population were vaccinated or revaccinated each year and by 1937 endemic smallpox had disappeared. Seven of the 21 cases reported between 1937 and 1940 (see Table 8.10) were documented as importations; the others were suspected to be importations or mistaken diagnoses (Polak, 1968). The disruption of the Second World War, during which the Netherlands East Indies and neighbouring areas of southeastern Asia had been captured by the Japanese and then liberated in 1945, led to major epidemics of smallpox in neighbouring countries, especially Thailand and Malaysia. Smallpox was reintroduced into Sumatra from Thailand in 1947. This outbreak was controlled, but another importation from Malaysia led to a major epidemic in Java in 1949, with over 13 000 cases. This time the disease became firmly entrenched in the larger islands, but did not spread to the numerous but more sparsely populated islands to the east (see Chapter 13, Fig. 13.3). There was a sustained high incidence in 1950 and 1951, and although the number of reported cases fell after 1951, variola major remained endemic for some years after the Intensified Smallpox Eradication Programme was established in 1967. Eradication was finally achieved, for the second time, in 1972 (see Chapter 13).
Philippines
There were as many as 40 000 smallpox deaths annually in the Philippines at the turn of the century, and smallpox was implicated in about one-third of the cases of blindness (Low, 1918). Intensive vaccination efforts were launched by the United States authorities and resulted in a dramatic reduction in the incidence of smallpox to some 700 cases in 1914. Because of its contacts with the USA, which had succeeded Spain as the occupying power between 1898 and 1918, the Philippines experienced what was probably variola minor (described locally as “varioloid”) during the second decade of the 20th century (McVail, 1923), but it was always rare, according to reported figures, compared with variola major. Control efforts were relaxed after the transfer of responsibility for health matters from the United States to the Philippine authorities in 1916, and a very severe epidemic occurred in 1918-1919, with over 64 000 deaths (McVail, 1923). Various inefficiencies and deceitful practices were exposed by inquiries into this disaster. Subsequently, vaccination efforts were greatly strengthened, with the result that the last cases of endemic smallpox occurred in the Philippines in 1931. Apart from a few outbreaks associated with importations—notably 282 reported cases in 1948 which persisted into 1949—the Philippines has remained free of smallpox ever since (see Table 8.10).
Malaysia
The smallpox situation in the Federated Malay States (Malaysia) before the Second World War was rather similar to that in Indonesia, the endemic disease being eliminated in the late 1930s (see Table 8.10). No figures are available for the war years (1942-1945) but by 1946 smallpox was well established again, with 3364 reported cases that year and over 4500 (1008 deaths) in 1947. The disease was rapidly curbed by control measures, and no endemic cases were reported after 1949, except for an outbreak of 338 cases in 1959 which extended into 1960, following an importation.
Burma
Burma was administered as part of British India until 1937, and gained its independence in 1948. As in India, smallpox was a traditionally important endemic disease, usually causing between 1000 and 8000 reported deaths per year, during the period 1905-1927 (Low, 1918; see Table 8.10) in a population that rose over this period from 8.5 to more than 13 million. The incidence continued to be high, especially in the provinces, but the seaports remained reasonably free of the disease, although there was a major epidemic in Rangoon in 1950 (Murray, 1951). By 1958 the annual incidence of reported cases was still over 1000. Control measures were gradually improved and the incidence fell to some hundreds of reported cases annually by 1960; the endemic disease was eliminated in 1965. The Chinese experience of importations across the border into Yunnan Province in 1960 (see Chapter 27) suggests that there was a good deal of unreported smallpox in the remote border regions of Burma.
Thailand
Thailand was one of the few Asian countries never to be colonized by a European power. In the early years of the century even the registration of deaths was limited to Bangkok, in which there was a very severe epidemic of smallpox in 1911-1912, with 2368 deaths in a population of about 600 000. In 1914, following this outbreak, vaccination was made compulsory, first in Bangkok and ultimately in the country as a whole. Prior to the outbreak of the Second World War smallpox appeared to be coming under control (see Table 8.10), but a rising incidence in 1944 was followed by severe epidemics in 1945 and 1946, with over 62 000 reported cases and 15 000 reported deaths. An intensive vaccination campaign brought the disease under control by the early 1950s, but there was a further outbreak, with over 1500 reported cases, in 1959, before the disease was eliminated in 1962.
Indochina
The present-day states of Democratic Kampuchea, Lao People’s Democratic Republic and Viet Nam, which before 1954 constituted French Indochina, had long suffered from endemic variola major. Reporting was very incomplete, but there was an increased prevalence during the latter years of the First World War, said to have been due to the discontinuance of official vaccination tours by government medical officers. Smallpox continued to be endemic between the wars, increasing somewhat (but not as much as in Thailand) just after the Second World War. Major efforts at control instituted by the newly independent countries achieved elimination in the late 1950s (Lao People’s Democratic Republic, 1953; Democratic Kampuchea, 1959; and Viet Nam, 1959), which was fortunate, otherwise there might have been further outbreaks during the Viet Nam conflict of 1965-1975. However, no cases were reported then by either of the warring sides.
THE INDIAN SUBCONTINENT AND AFGHANISTAN
During the early years of the 20th century smallpox was endemic in all countries of southern Asia, and India had already emerged as the major focus of smallpox in the world, a position it retained until the disease was eradicated there in 1975. Smallpox remained endemic in all the countries of the Indian subcontinent except Sri Lanka (in which eradication was achieved in 1951) throughout the period under review (Table 8.17).
Table 8.17: Indian subcontinent and Afghanistan: numbers of reported cases of smallpox in selected countries, 1920- 1966a
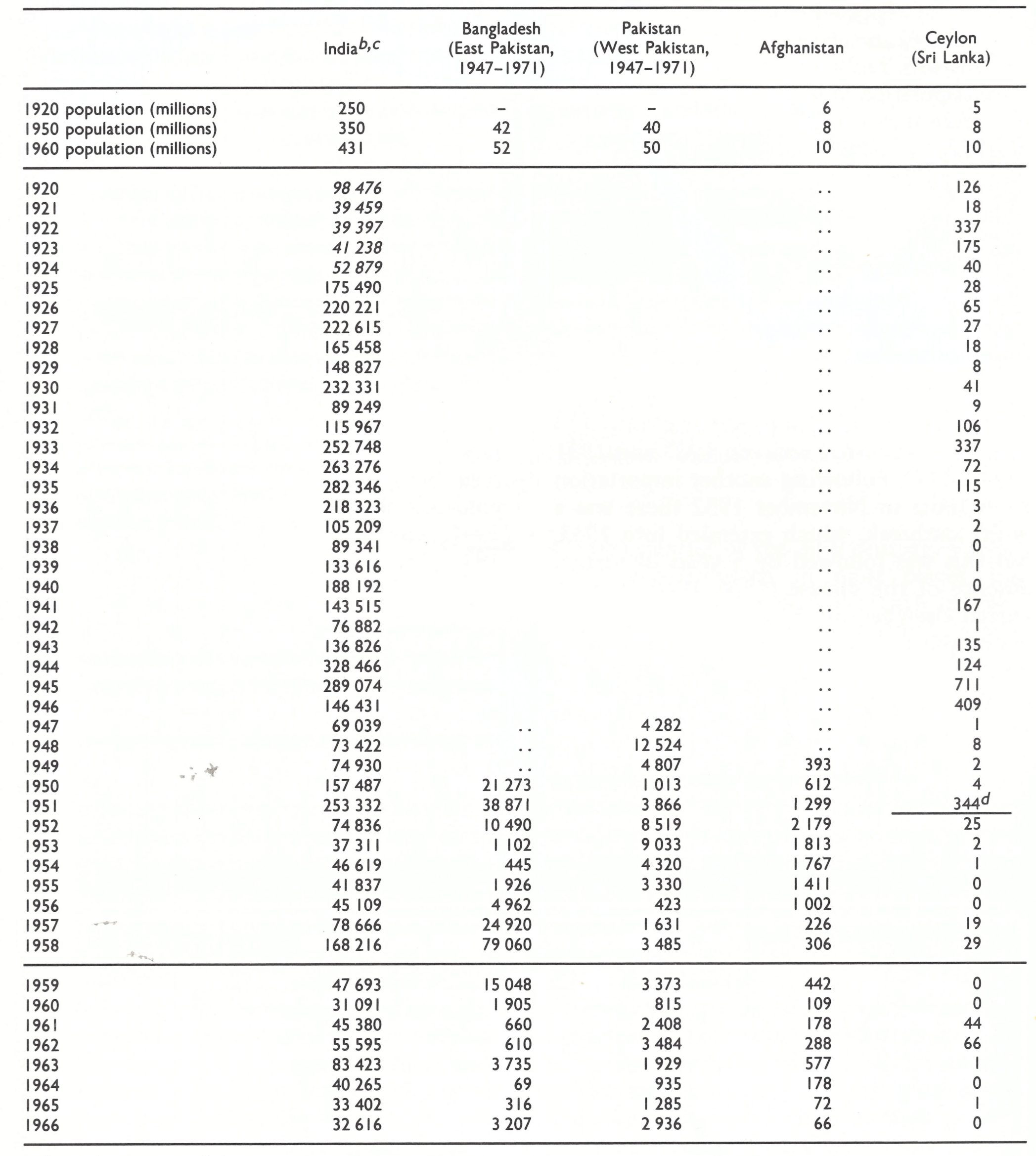
bExcluding Burma; see Table 8.10.
cFigure in italics denote the number of reported deaths from smallpox.
dThe last probable occurrence of endemic smallpox.
India
As vaccination coverage improved in British India the rate of reported deaths from smallpox gradually fell from over 2000 per million population in 1870 to less than 300 per million in 1930 (see Chapter 5, Fig. 5.2). A pattern of epidemics every 5-7 years was maintained, and even in non-epidemic years the disease caused many deaths and sometimes great disruption. For example, in 1930 smallpox afflicted all the port cities of India and in consequence other countries imposed severe restrictions on Indian shipping.
Although a Vaccination Act required that all children should be vaccinated within 6 months of birth, this was not enforced; indeed, it was not considered practicable to enforce compulsory vaccination in India. Since most older persons were immune on account of vaccination or a previous attack, smallpox was primarily a disease of children, with a very high mortality among those aged less than 1 year. By 1941 primary vaccination was legally compulsory in some 80% of towns and 60% of the villages in British India, but revaccination was compulsory only in Madras. However, by 1944 some 60 million vaccinations were being given annually in a population of about 332 million, using liquid vaccine produced in 14 laboratories situated in the different states.
In 1947 India obtained independence and the partition of British India into Pakistan (East and West) and India occurred, with the consequent readjustment of populations and reporting arrangements (Table 8.17). Largescale vaccination continued, but many of the vaccinations were probably ineffective owing to the lack of potency and heat stability of the vaccine. However, because vaccination was readily available and variolation was legally forbidden, the latter practice ceased and was never a problem in India during the Intensified Smallpox Eradication Programme. There was little change in the situation until after 1962, when a national smallpox eradication programme was launched (see Chapter 15). Smallpox was not finally eliminated from India until May 1975.
Pakistan and Bangladesh
The situation was little different in India’s neighbours, Pakistan and Bangladesh (East Pakistan until December 1971). Prior to partition in 1947 they had been part of British India, and a gradual increase in vaccination coverage had lowered the incidence of smallpox. In West Pakistan (Pakistan after December 1971) variolation was widely accepted as a control measure practised by Muslim religious leaders, and it continued to be used long after vaccination was introduced as a public health measure in 1875. After 1947 the Vaccine Institute in Lahore continued to prepare glycerolated liquid vaccine, but in spite of some 15 million reported vaccinations a year in West Pakistan (population in 1950, 40 million) endemic smallpox continued, especially in the cities and mainly in unvaccinated children. A variety of factors contributed to the failure of vaccination: substandard vaccine, inadequate motivation of the public, defective legislation, and lack of supervision of vaccinators. Eventually, after intensification of the national eradication programmes and help from the World Health Organization, the last case of smallpox was reported in October 1974.
There were large outbreaks in East Pakistan (Bangladesh) after partition, with 70 000 reported cases in 1950-1952 and over 100 000 cases in 1957-1958. In 1953 vaccine began to be produced by the Institute of Public Health in Dhaka. After 1958 only freeze-dried vaccine was produced, but until 1966 its quality was inferior. Smallpox was finally eliminated in October 1975.
Afghanistan
Afghanistan was internationally recognized as an independent state in 1921. In this rugged and sparsely populated country, smallpox remained endemic throughout the first half of the 20th century and variolation was extensively practised (see Chapter 14). In the 1930s, Berke (1956) set up the first modern type vaccination service, and it was reported that about 3 million persons were vaccinated in the period 1936-1939. Vaccination was made compulsory in Afghanistan in 1959.
No information is available on the smallpox incidence prior to 1949. Thereafter, the number of reported cases varied between a few hundred and about 2000 annually, mostly in the towns. The incidence of smallpox in the large population of nomads and semi-nomads was unknown. Endemic transmission ceased in 1972.
Sri Lanka
Smallpox was much more readily controlled on the island of Ceylon (Sri Lanka) than on the adjoining mainland of India. Vigorous vaccination campaigns in the 1920s reduced smallpox to occasional outbreaks following importations from India; only 103 cases were reported between 1927 and 1931 (Table 8.17). Following another importation from India in November 1932 there was a larger outbreak, which extended into 1933, but this was followed by 5 years of virtual absence of the disease (1936-1940). As occurred elsewhere in Asia, there was a resurgence during the Second World War but control was re-established in 1947 and the elimination of endemic smallpox was claimed in 1951. Thereafter, importations from India caused small, readily controlled outbreaks in most years.
SOUTH-WESTERN ASIA
Prior to the First World War this region consisted of the Ottoman Empire and Persia. Smallpox was endemic and largely unreported in both areas. The holy cities of Mecca and Medina provided major foci for importation and subsequent exportations of smallpox to all parts of the Muslim world. With regard to Persia the statement was made at a meeting of the Teheran International Sanitary Council in 1907 that between 50 000 and 100000 persons died annually from smallpox (Low, 1918).
Between the First and Second World Wars the reported incidence of smallpox fluctuated in Persia and the new states that arose out of the Ottoman Empire (Fig. 8.11), but had fallen to a low level in most countries of the area by the late 1930s (Table 8.18). An epidemic focus developed in Iraq in 3940-1941, with over 3000 reported cases, and in 1942 spread westwards into Syria, Lebanon, Turkey, Palestine and Jordan and eastwards into Iran. In 1943 there was a major outbreak in Turkey which extended into Greece (see Table 8.2). Intensive vaccination campaigns were instituted in Turkey and the endemic disease was eliminated by 1951, but substantial numbers of cases continued to be reported from Iran and Iraq until the late 1950s and early 1960s. Endemic smallpox was reestablished in Iran, Iraq and the Syrian Arab Republic in 1971-1972, but then brought under control (see Chapter 23).
The Incidence of Smallpox on Islands
Island countries with sparse populations were spared endemic smallpox because their populations were too small to sustain continuous transmission, and they were much less frequently subject to importations than were countries of a similar size and population located on the continental mainland. The outstanding examples are Australia and New Zealand, both of which were colonized by British settlers after the concept of quarantine was established, and were so distant from smallpox-endemic countries that persons incubating the disease on embarkation were sick on arrival and were discovered during quarantine inspections. Other examples mentioned in this chapter are Sri Lanka and Madagascar, in each of which importations were less frequent and more easily controlled than in countries with comparable populations on the adjacent continents, such as Nepal and Mozambique. Locally produced liquid vaccine was more likely to be potent when administered than in continental countries, because of the short distances and, therefore, speedier delivery from production centres to villages. Very remote islands were either spared the disease entirely or subject to widely spaced devastating epidemics such as occurred in Iceland before 1870. If the population of the island was dense enough, however, as in Java, endemic smallpox could be firmly established and proved difficult to eliminate.
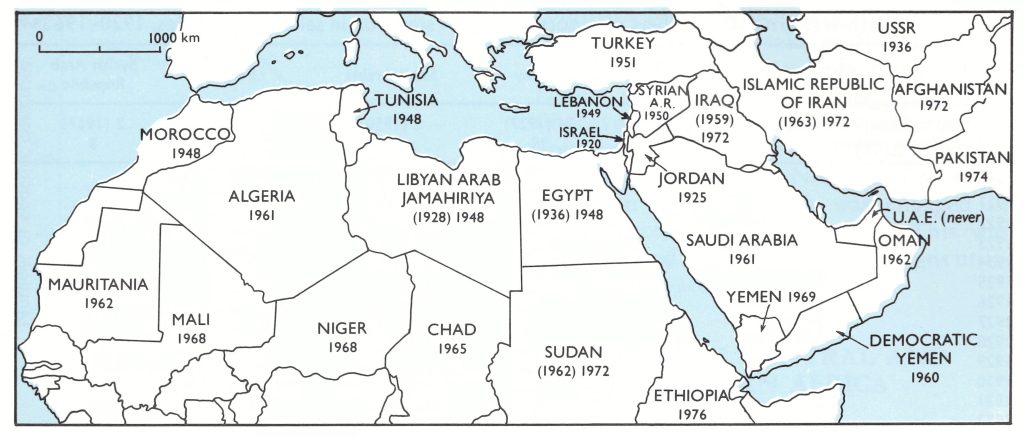
Fig. 8.11. North Africa and south-western Asia: year in which smallpox ceased to be endemic in each country (national boundaries as of 1982). Dates in parentheses (for Algeria, Egypt, Iraq, Islamic Republic of Iran, Libyan Arab Jamahiriya and Sudan) indicate the initial elimination of endemic smallpox, after which endemicity was again established before final elimination in the year shown.
SMALLPOX IN AFRICA, 1900-1958
Although smallpox arrived in some countries in central Africa as late as the 19th century (see Chapter 5), the disease was firmly entrenched throughout the continent during the first quarter of the 20th century. Variola major predominated in most places, but variola minor occurred concurrently in many countries in southern and eastern Africa. Vaccination was practised less than variolation, but both were uncommon. Tulloch (1980) reviewed the incidence of smallpox in different countries in Africa over the half-century between 1928 and 1977; the changes in incidence over the 3 decades 1938-1967 are illustrated in Fig. 8.12. The continued endemicity of smallpox in all countries of Africa during the period under review (Fig. 8.13), except those of the Mediterranean littoral (Fig. 8.11), is evident.
There is no generally accepted way of subdividing this large and varied continent. The descriptions of the eradication programmes in Africa follow one pattern (Chapters 17-22) and those of certification by the international commissions follow another (Chapters 25-27). The countries of the Mediterranean littoral constitute a well-defined North Africa (Fig. 8.11); while the countries south of and including Angola, Zambia, Malawi and Mozambique clearly delimit southern Africa (Fig. 8.15). The countries between these two regions have been designated as western, central and eastern Africa (Fig. 8.14).
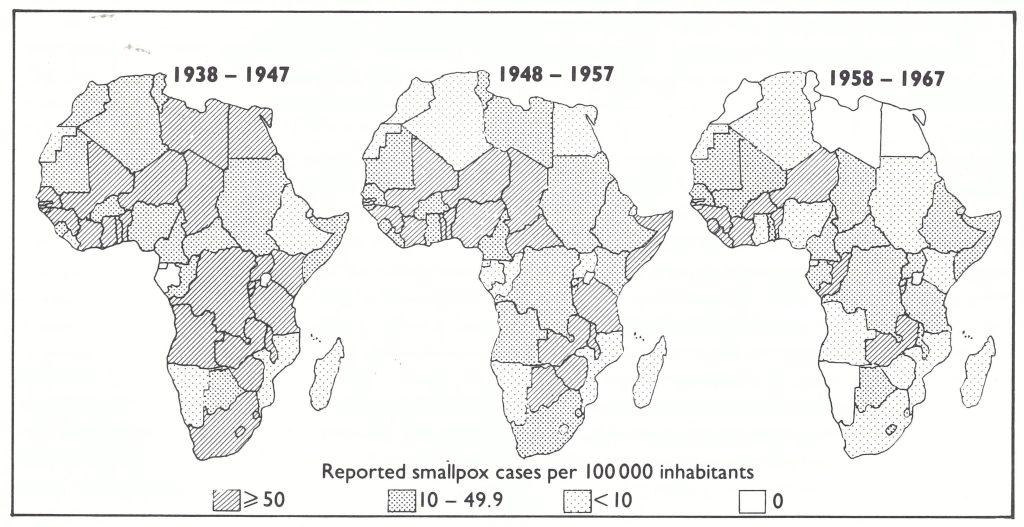
Fig. 8.12. Africa: maximum reported annual incidence rates of smallpox during each decade, 1938-1967. No data available for Equatorial Guinea, 1938-1947. (From Tulloch, 1980.)
Table 8.18: South-western Asia: numbers of reported cases of smallpox in selected countries, 1920-1963a,b
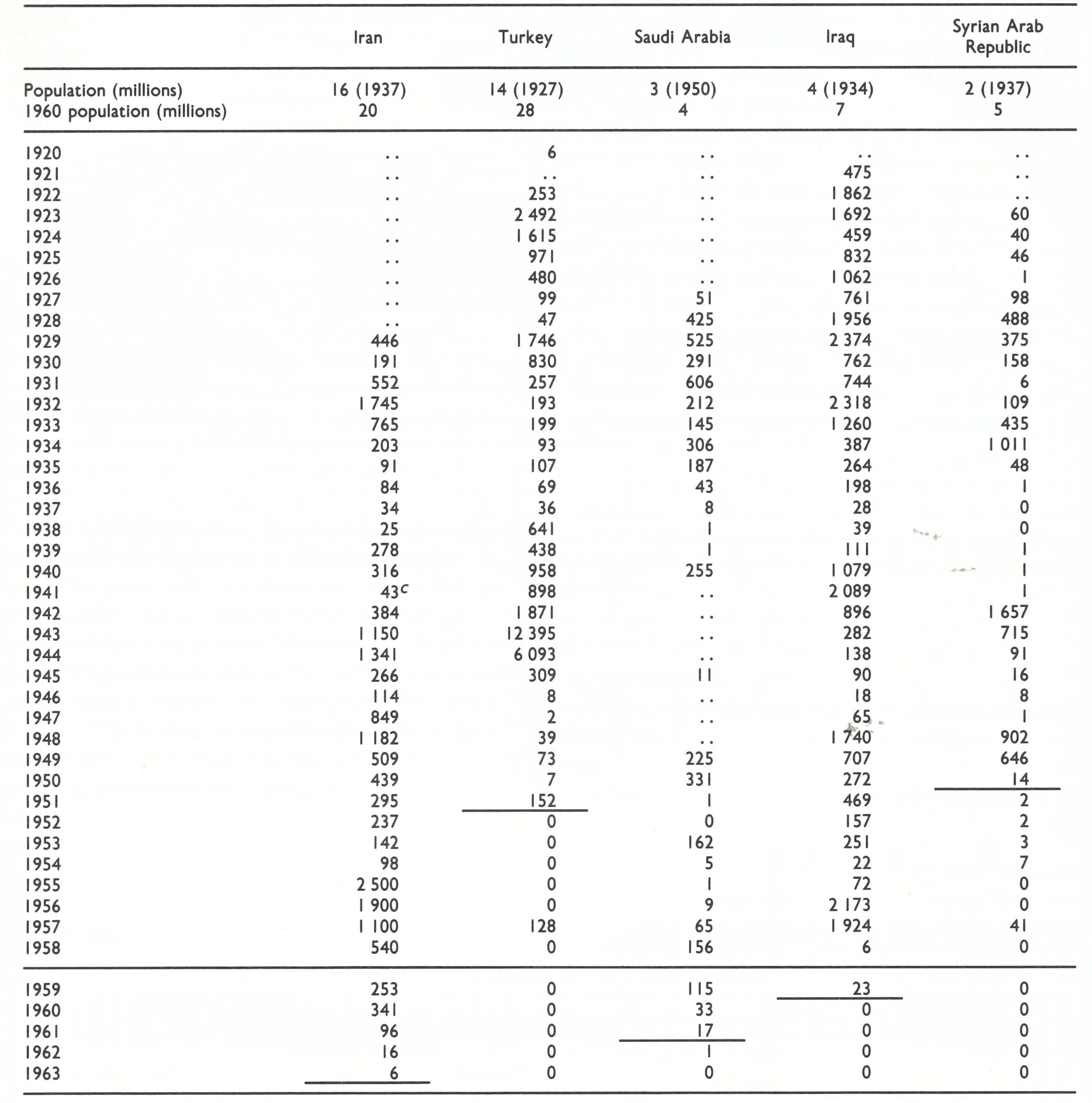
a A horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b..= data not recorded.
c Number of reported deaths.
NORTH AFRICA
The countries of the Mediterranean littoral of Africa (see Fig. 8.11) have long had more extensive contacts with other Mediterranean countries than with Africa south of the Sahara. Smallpox was endemic in all these countries in the first 4 decades of the century (Table 8.19). In Egypt, the most populous country of the region, smallpox was endemic but epidemics in which 2 or 3 times the usual incidence was reported occurred in 1904-1905, 1909, 1914-1915 and 1919-1920 (Table 8.20). General vaccination of the whole population was carried out in 1919 and again in 1926 in response to an epidemic that took place during that year (Ahmad, 1933). Smallpox was also reported to be very common in Algeria, Morocco, and Tunisia; Low (1918) quotes Clemow as stating that variolation by insufflation was practised in Tunisia, “often with disastrous results”.
By the mid-1930s vaccination campaigns organized by the various colonial powers in the region—France, Italy, Spain and the United Kingdom—had reduced smallpox to low levels (Table 8.19). There was a severe epidemic in Egypt in 1932-1934, which did not affect the other North African countries. At the end of the 1930s endemic smallpox had been virtually eliminated in all these countries except Morocco, but the fighting and unrest associated with the Second World War led to severe outbreaks in all 5 countries, including the sparsely populated Libya. The contrast with Europe is striking (compare Tables 8.1 and 8.19); the only outbreak of smallpox in Europe associated with the Second World War (Italy, 1944-1947) was due to an importation from North Africa, whereas major epidemics occurred over a period of several years in each of the North African countries. Most of these were due to variola major, but the outbreaks in Morocco were apparently caused by variola minor (case-fatality rates, 2-3%). However, after 1948, improved health services brought about a great reduction and the eventual elimination of smallpox throughout North Africa—more slowly in Algeria, which was engaged in internal conflict, than elsewhere. This was accomplished by vaccination campaigns utilizing liquid vaccines.
Table 8.19: North Africa: numbers of reported cases of smallpox, 1920-1964a,b
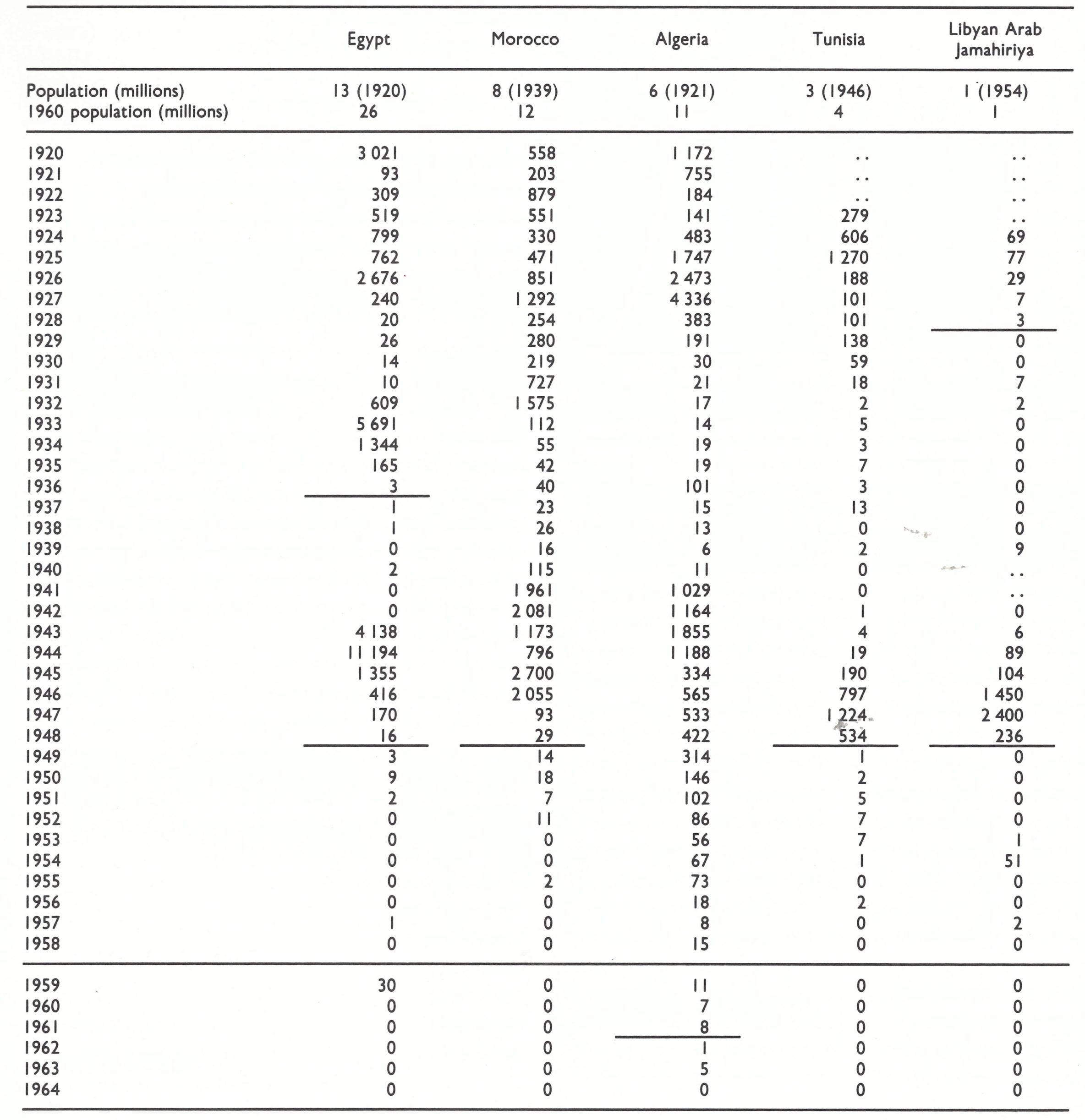
a horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b...= data not recorded.
Table 8.20: Egypt: numbers of reported cases of
and deaths from smallpox,
1886-1931a,b
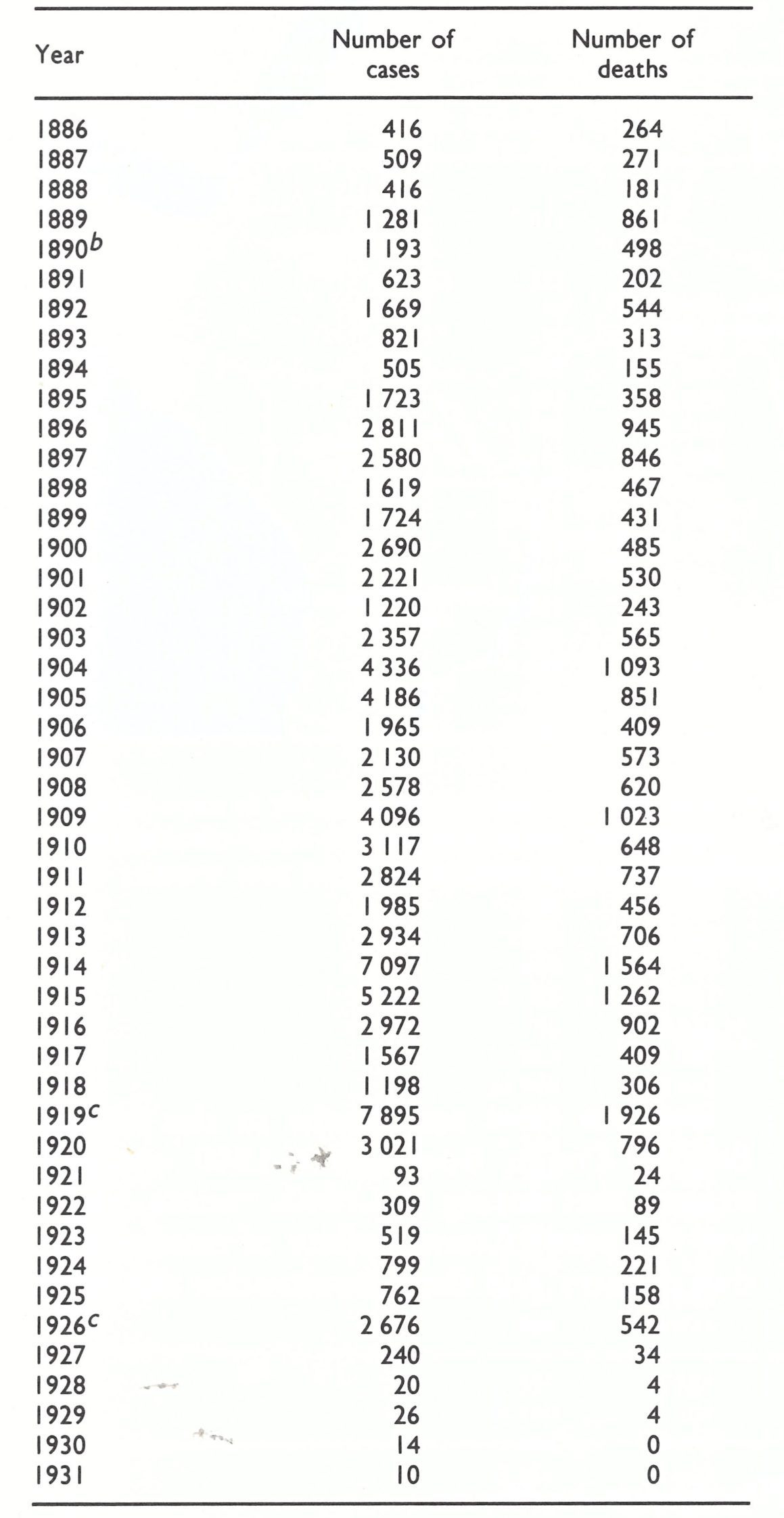
b In 1890 a law was introduced requiring the vaccination of every newborn infant before the age of 3 months. It was amended in 1897 and 1917, but not enforced.
c General vaccination of the whole population (i.e., vaccination and revaccination) was carried out in these years.
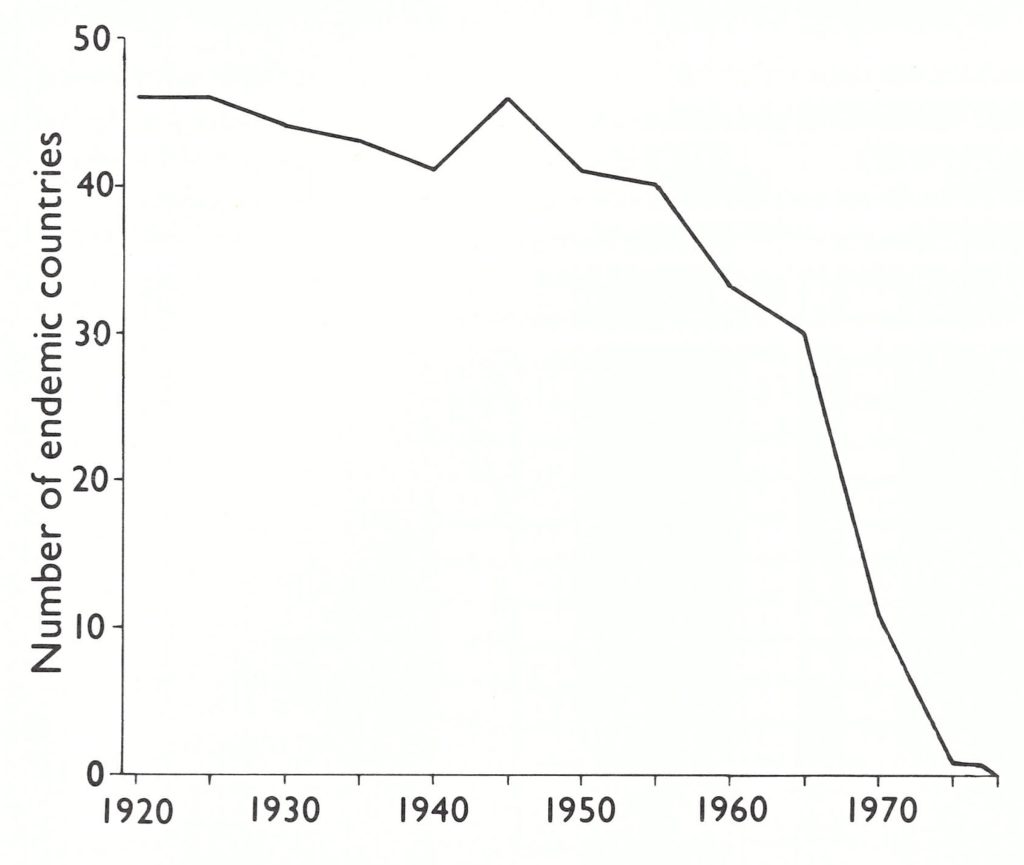
Fig. 8.13. Number of countries of the 47 in Africa in which smallpox was endemic at various times between 1920 and 1977. National boundaries as of 1982.
WESTERN, CENTRAL AND EASTERN AFRICA
These regions comprise a large area lying between latitudes 22°N and 12°S, and include some 30 countries (Fig. 8.14). During the first part of the 20th century most of these countries were administered as colonies, by several European powers—Belgium, France, Germany (until the First World War) and the United Kingdom. They became independent countries mostly during the late 1950s and early 1960s. Smallpox was endemic in the majority of them throughout the 1960s and in Ethiopia and Somalia until the mid-1970s.
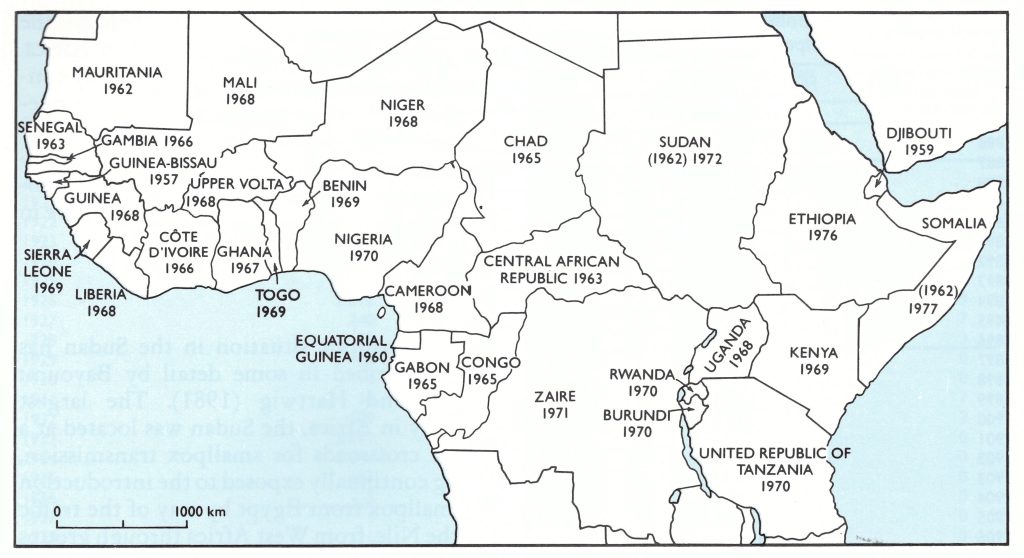
Fig. 8.14. Western, central and eastern Africa: year in which smallpox ceased to be endemic in each country (national boundaries as of 1982). Dates in parentheses (for Somalia and Sudan) indicate the initial elimination of endemic smallpox, after which endemicity was again established before final elimination in the year shown.
Western Africa
The reported incidence of smallpox in selected countries of this region is shown in Table 8.21. Reporting was unsatisfactory except in the major towns, but there did not seem to have been much diminution in the incidence of smallpox during the 20th century up to the time of independence, except in some of the French colonies.
More detailed accounts exist of the severity of smallpox in particular colonies and countries. Kulz (1905) suggested that at the beginning of the 20th century the annual mortality from smallpox in Togoland (then a German colony) amounted to as much as 1% of the population.
The situation in French West Africa has been described by Breman et al. (1977a). The Federation of French West Africa was formed in 1904, and shortly after this the French authorities reported smallpox in several territories of the Federation. A vaccine production centre was established at Kindia in Guinea in 1905, and from 1909 onwards a more stable dried vaccine was used (Fasquelle & Fasquelle, 1971). As surveillance improved the completeness of reporting increased; case-fatality rates in French West Africa as a whole varied between 6% and 20%. Variola minor appears to have occurred without concurrent variola major in Guinea in 1939 and 1940, and again in 1959-1961. Otherwise the data suggest that both variola major and variola minor occurred at some time each year in some part of the Federation.
Fasquelle & Fasquelle (1971) have described the eradication programme that was mounted in C6te d’Ivoire in 1961, the year after it became independent. The objective was achieved by mass vaccination, using a French-type freeze-dried vaccine. In a population of 3.8 million, 2.4 million vaccinations were carried out in 1961 and 3.7 million by 1963. The routine was established of primary vaccination during the first year of life and revaccination at school age and again at the age of about 18 years. The incidence of smallpox fell rapidly, elimination being achieved in 1966.
Central Africa
The countries included in this somewhat arbitrary grouping are Burundi, the Central African Republic, Chad, Rwanda, the Sudan, Uganda and Zaire. The incidence of smallpox in the most heavily populated of these countries during the period 1920-1966 is shown in Table 8.22. The Sudan and Zaire are the two largest countries in Africa and have strongly contrasting climates, much of the Sudan being semi-desert, while Zaire includes the largest area of tropical rain forest in Africa. The Sudan was under Anglo-Egyptian control until 1955 and became completely independent in 1956. Zaire was a Belgian colony from 1908 until 1960, when it gained independence and became the Democratic Republic of the Congo, changing its name to Zaire in 1971.
The Sudan and the Pilgrimage to Mecca
The Mecca Pilgrimage is probably the largest of all pilgrimages to a sacred place, and currently involves over a million pilgrims assembling at the holy places in Saudi Arabia over a period of a few days, at a fixed date in the Hegira year. The Sudan, of which the northern and central parts are inhabited by Muslims, is at the crossroads of the passage of pilgrims from the large Islamic populations in western Africa to Mecca. They came, and come, by all kinds of transportation from western Africa through Chad to cross the illdefined border of some 900 kilometres into the provinces of Darfur and Kordofan. Within the Sudan, they often stop to work in the Gezira, and then go on by road or railway to Port Sudan, whence they cross the Red Sea by boat to Saudi Arabia. In the 1920s a quarantine station was established at Geneina, on the Sudan-Chad border, but many pilgrims evaded it. Outbreaks of variola major in nothern Sudan in 1927,1929,1949,1951-1 952 and 1952- 1953 were attributed to entries by this route, and the disease subsequently moved westwards along the pilgrim route (Bayoumi, 1972). Later, more elaborate precautions were taken in Saudi Arabia to control the entry and dissemination of disease by pilgrims coming from all parts of the world (see Chapter 27).
Sudan
The smallpox situation in the Sudan has been described in some detail by Bayoumi (1974) and Hartwig (1981). The largest country in Africa, the Sudan was located at a major crossroads for smallpox transmission, being continually exposed to the introduction of smallpox from Egypt by way of the traffic on the Nile, from West Africa through groups of pilgrims crossing the country to and from Mecca (Bayoumi, 1972), and from Ethiopia in the east.
Records of reported cases of smallpox go back to 1925 (Bayoumi, 1974; see Table 8.22), all parts of the country being affected. Variola minor was endemic in the south and east, where the Sudan borders on Zaire, Uganda and Ethiopia, and there were repeated importations of variola major from the west, brought in by the large numbers of pilgrims and immigrants from western Africa and other central African countries. From time to time these produced sporadic outbreaks, mainly during the dry season, when maximum population movement usually occurred.
There was a severe epidemic of variola major extending from 1927 until 1931, apparently introduced by Ethiopian migrants. An extensive outbreak of variola minor occurred in the south between 1932 and 1934, but this did not cause nearly as much concern to medical administrators as did the periodic outbreaks of variola major along the pilgrim route and in the Gezira Irrigation Scheme (Bayoumi, 1974). Extensive vaccination campaigns, performed almost yearly in one or more provinces, reduced the incidence, and from 1941 to 1946 the reported incidence was under 250 cases a year. In 1947, scattered epidemics developed and continued until the end of the 1940s along the major lines of communication in Kordofan, Blue Nile and Kassala provinces, predominantly of variola minor, but with sporadic outbreaks of variola major. The incidence declined substantially in the mid-1950s, although there was a serious outbreak in Equatoria Province in 1954, and outbreaks that were probably still occurring among nomads and pilgrims were rarely reported. Endemic smallpox was eliminated om 1962, but was re-established in 1967 and eventually eliminated again in 1972 (see Chapter 18).
Zaire
Data on cases and deaths in the former Belgian Congo from about 1940 onwards suggest that during the 1940s variola minor was the predominant variety of smallpox in that country, and the same situation obtained in the former trust territory of Ruanda-Urundi (now Rwanda and Burundi). However, in most years outbreaks of variola major and variola minor occurred, usually in different parts of the area. After 1960 variola major appeared to predominate (see Chapter 18). Liquid glycerolated vaccine was prepared in the colony’s own laboratories, but the Belgian authorities reported great difficulties in distributing a potent vaccine. The take rate in primary vaccinations during 1938-1946 varied between 8.8% and 74.3%, with an average for the 9 years of 37.6% (Tulloch, 1980). Many cases of smallpox, including variola minor, were reported in subjects who were supposed to have been vaccinated (Fabre, 1948). Endemic smallpox was not eliminated until 1971.
Uganda
Prior to the First World War, the main sources of smallpox were the caravans of Arab and other traders. Between 1914 and 1920 over 20 000 deaths from smallpox were reported in Uganda, the overall case-fatality rate among cases treated in government hospitals between 1911 and 1923 being over 23%. Following extensive vaccination, only a few outbreaks were reported between 1920 and 1944, when the outbreak of variola minor that had started in Kenya in 1943 spread to Uganda, producing 4737 reported cases in 1944, and then gradually declined. Small outbreaks, one of which, in 1956, was due to variola major, continued every year until endemic transmission ceased in 1968.
Table 8.21: Western Africa: numbers of reported cases of smallpox in selected countries, 1920-1966 a
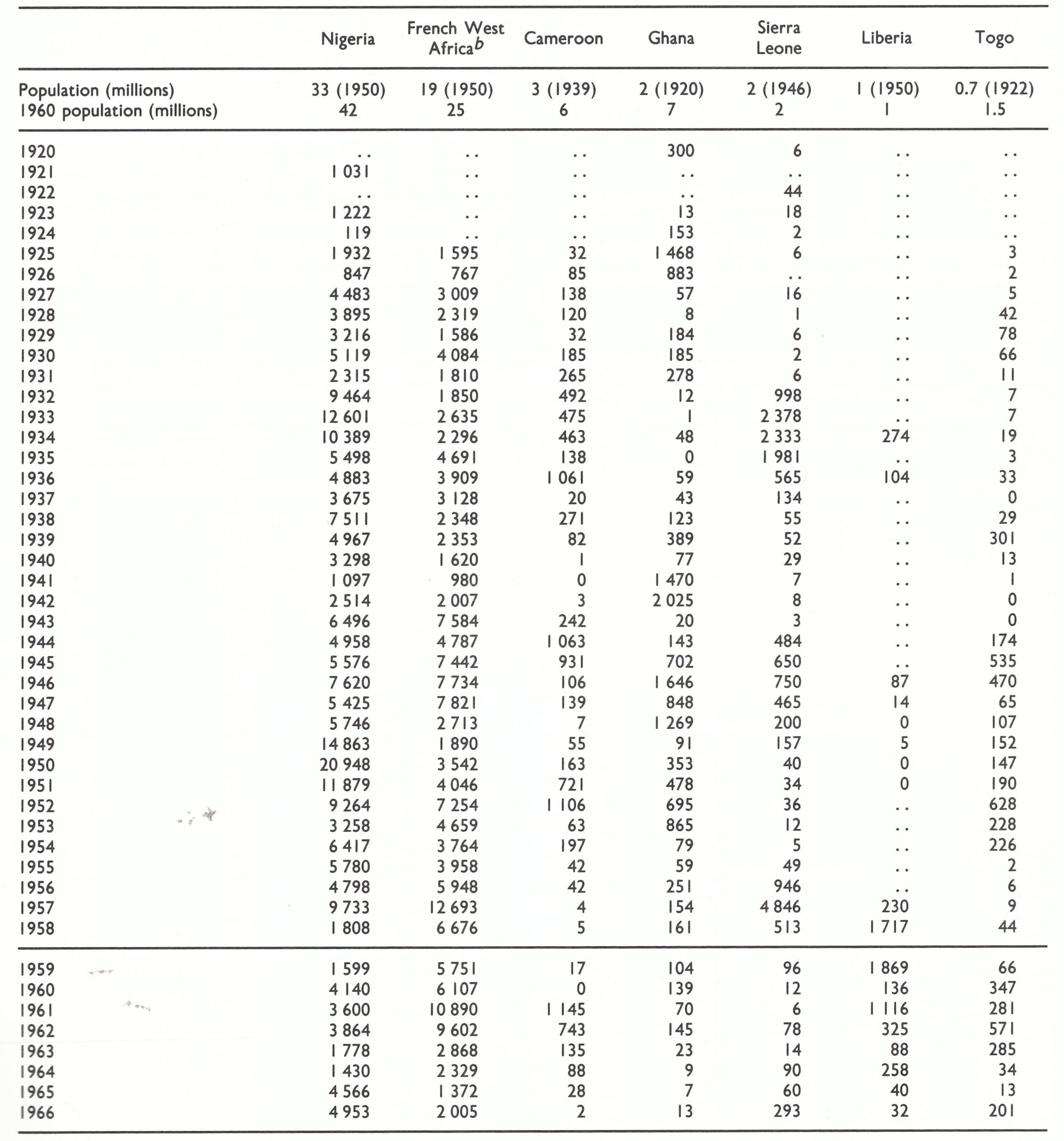
a...=data not recorded.
b Comprising present-day Benin (formerly Dahomey), Burkina Faso (formerly Upper Volta), Cote d’lvoire, Guinea, Mali, Mauritania, Niger and Senegal.
Table 8.22: Central Africa: numbers of reported cases of smallpox in selected countries, 1920-1966 a,b
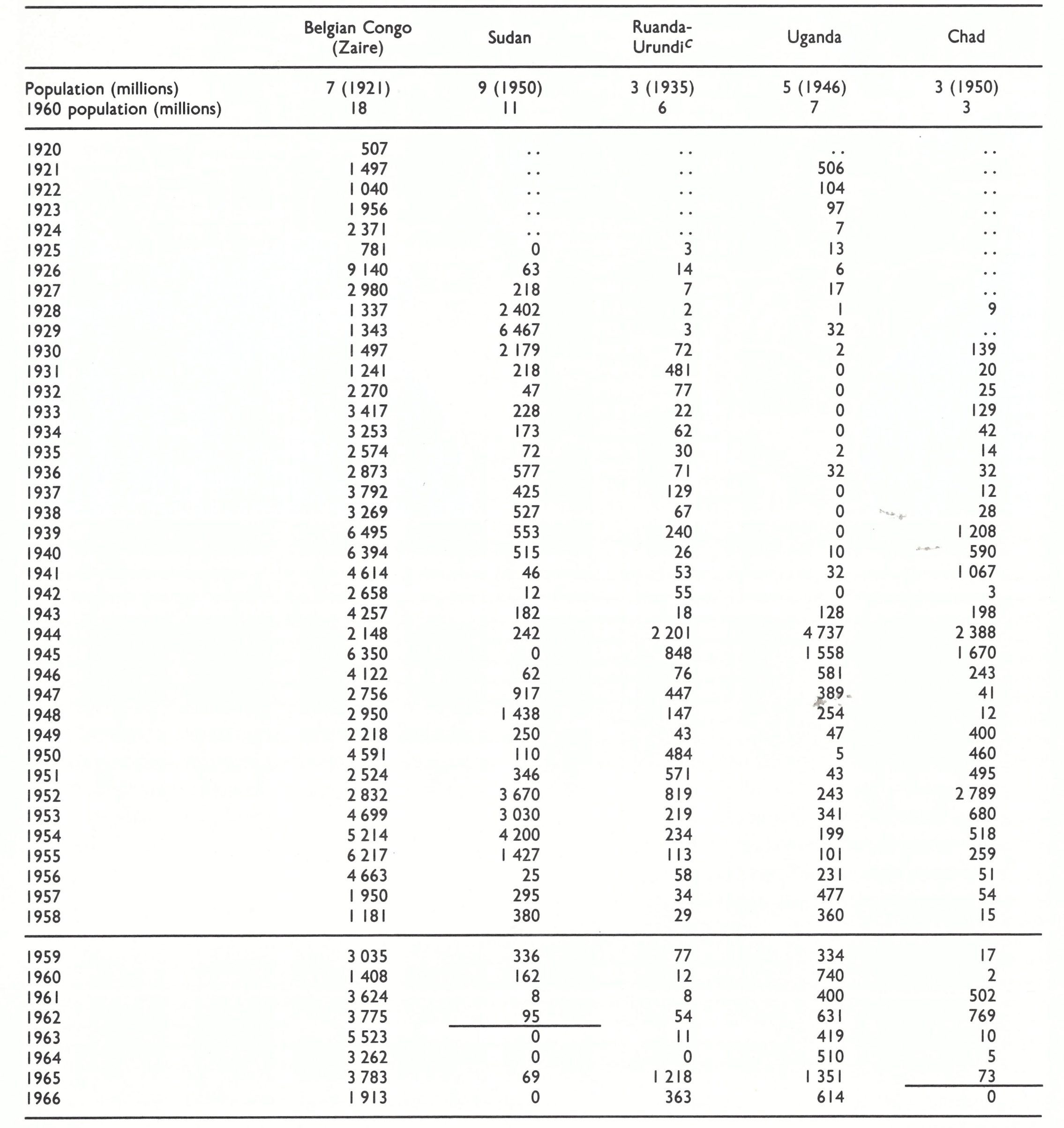
aA horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
b…=data not recorded.
c From 1962, the two separate states of Rwanda and Burundi.
Eastern Africa
This grouping of countries includes Ethiopia, Kenya, Somalia and the United Republic of Tanzania, former colonies of European powers which became independent in the 1950s and early 1960s. Smallpox appears to have been common in the early part of the 20th century and case-fatality rates were usually between 20%, and 30% (Low, 1918). Table 8.23 sets out the reported annual incidence of smallpox in these countries from 1920 to 1966. As elsewhere in Africa, the figures provide an index of the incidence but it is certain that there was gross underreporting.
Table 8.23: Eastern Africa: numbers of reported cases of smallpox in selected countries, 1920-1966 a
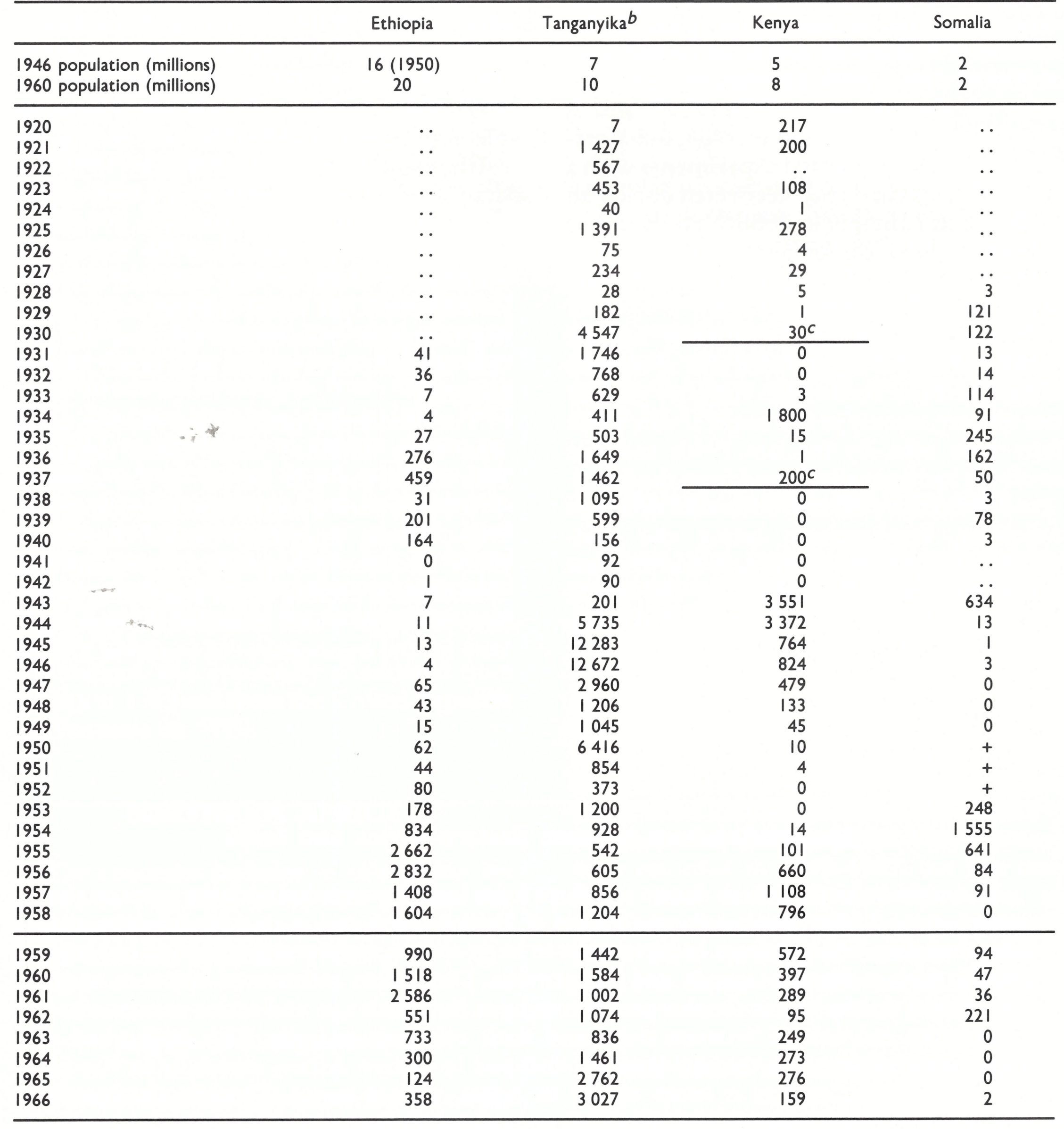
In 1964, combined with Zanzibar and Pemba to form the United Republic of Tanzania.
The last probable occurrences of endemic smallpox.
Ethiopia and Somalia
It is difficult to obtain reliable information on smallpox in Ethiopia before the Intensified Smallpox Eradication Programme began work there in 1971, when only variola minor was present and was very poorly reported (see Chapter 21). Early in the century smallpox caused devastating outbreaks, and just before the First World War about 20% of the population of the province of Shewa (in which Addis Abeba is situated) were said to be pockmarked (Pankhurst, 1965). Extensive vaccination campaigns were undertaken by Italian health officials after the Italian occupation of the country in 1936, vaccine being produced in Addis Abeba. Murray (1951) was unable to comment on smallpox in Ethiopia, except to say that “a small but steady incidence” occurred in Shewa Province. Teclemariam (1965) reported that an epidemic of smallpox with a high case-fatality rate took place in the Shewa area in 1960 and a smaller outbreak occurred in 1964, but Herrlich et al. (1963) reported experiments with a strain of ‘‘alastrim virus” recovered during an epidemic in Ethiopia in 1958. Variola minor appears to have completely replaced variola major throughout Ethiopia before 1971, and was finally eliminated in 1976.
In the colonies that eventually became Somalia, Low (1918) reported that epidemics of variola major occurred in the early years of the century, mainly in the larger towns when fairs were held. By the late 1940s endemic smallpox had been eliminated from the Somaliland Protectorates, but outbreaks occurred following importations during the mid-1950s. This pattern continued, and the last major outbreak of smallpox in the world occurred in Somalia in 1976-1977, following importations from Ethiopia.
Keiya and the United Republic of Tanzania
Prior to the First World War the prevalence of smallpox in the two colonies of Kenya and Tanganyika was lower than in the 19th century. Vaccination was introduced in the larger towns, but outbreaks of variola major, with case-fatality rates of 25-30%, occurred sporadically. From the mid-1930s onwards variola minor occurred from time to time and because it was so much milder than variola major proved considerably more difficult to control (Conacher, 1957).
The situation in Kenya has been documented some what more fully than in many other African countries, but is characteristic of the situation in a large number of them. There was a severe famine in central Kenya in 1897-1900, due to a combination of drought, pleuropneumonia and rinderpest among the cattle, and a locust plague. Dawson (1979) has drawn attention to the way in which extensive movements of the population in quest of food created the conditions for the severe outbreak of smallpox that occurred in 1899. Subsequently, the social changes accompanying European colonization changed the pattern of smallpox in Kenya, as in other African colonies.
The production of smallpox vaccine, using seed virus obtained from India, began in Nairobi in the first decade of the century. Trade expanded with the introduction of cash crops, labour migration caused larger and more frequent population movements and urbanization created larger and denser populations—all of which increased the opportunities for the transmission of smallpox. On the other hand, vaccination, though ineffective as a general public health measure because of poor vaccine and inadequate funding, was used effectively to control outbreaks of variola major, so that smallpox appeared in frequent local outbreaks with very occasional widespread epidemics. A notable example of the latter occurred in 1916, when survivors of the Carrier Corps (a contingent of Kenyan Africans who acted as army porters during the British invasion and conquest of German East Africa (Tanganyika)) were returned from Nairobi to their home districts regardless of their medical condition. The result in one province, repeated in many others, was 100 separate outbreaks of smallpox, as well as other diseases (Dawson, 1979).
The production of vaccine in Nairobi was greatly expanded in the 1930s to supply most of the British colonies in eastern Africa. Variola major was imported into Mombasa from India on several occasions during the 1920s and 193Os, but endemic smallpox was eliminated from Kenya in 1930. In 1934 variola major was introduced again from the north, by nomadic Somalis (Seymour-Price et al., 1960). A widespread epidemic occurred but the disease was eliminated in 1936, only to be reintroduced by refugees from Ethiopia in 1937. No cases were reported in 1938-1942. In 1943 an epidemic of variola minor occurred, to be followed by an explosive epidemic of variola major in 1945. Subsequently, variola minor continued at a low level throughout the early 1950s, but it spread widely during the disturbances associated with Kenya’s struggle for independence in 1956-1958.
Smallpox was eventually eliminated from Kenya in 1969 and from the United Republic of Tanzania in 1970.
Special Relations between Eastern Africa and India
Throughout history, Arab dhows and ships from India have traded with the ports on the east coast of Africa. During the early days of British colonization in Africa indentured labourers were brought from India to assist in large-scale agricultural production in Natal (South Africa), Kenya, Uganda and Tanganyika. The Indian indentured labourers soon established themselves as shopkeepers throughout these colonies and active communications were maintained between them and their relatives in India. This traffic had a significant influence on the incidence of smallpox in eastern Africa, especially in Kenya and Tanganyika, and to a lesser extent in Natal, variola major (“Asiatic smallpox”) being repeatedly imported into all three areas from India.
SOUTHERN AFRICA
The countries included in this region are shown in Fig. 8.15. Table 8.24 sets out the reported incidence of smallpox in each of them between 1920 and 1966.
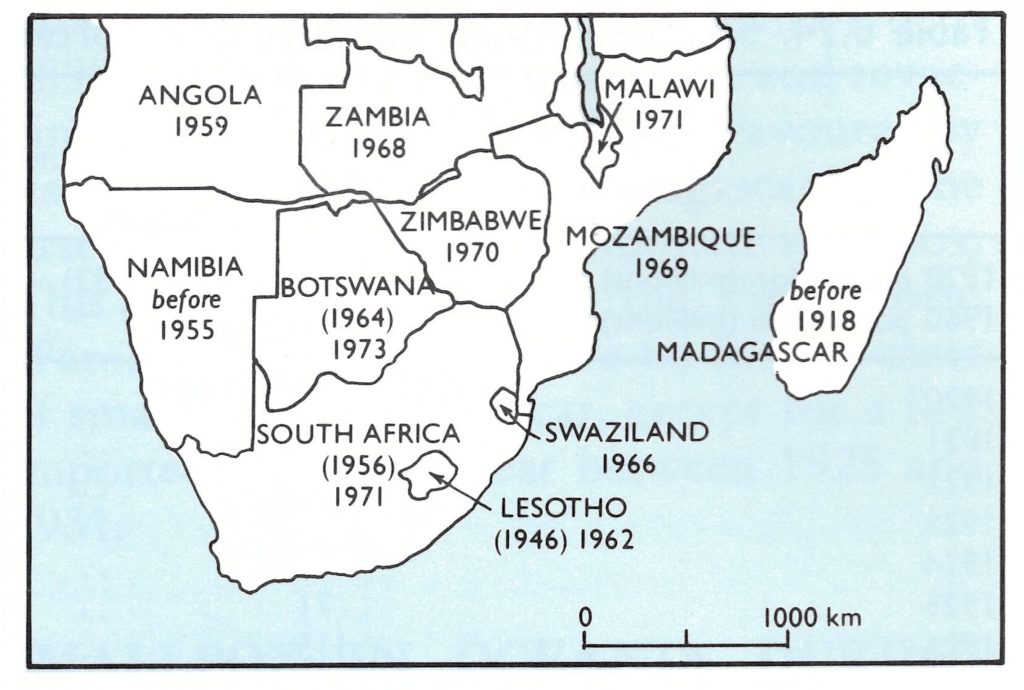
Fig. 8.15. Southern Africa: year in which smallpox ceased to be endemic in each country (national boundaries as of 1982.) The dates in parentheses (for Botswana, Lesotho and South Africa) indicate the initial elimination of endemic smallpox, after which endemicity was again established before final elimination in the year shown.
Angola and Mozambique
These former Portuguese territories, on the Atlantic and Indian Ocean shores of southern Africa, became independent in 1975. In relation to their experience of smallpox, they had more in common with each other than with neighbouring British colonies. Both variola major and variola minor were present during the 194Os, but the latter eventually predominated. The Portuguese promoted vigorous vaccination campaigns, using locally produced vaccines, and had eliminated smallpox from Angola by 1959, and from Mozambique by 1969.
Malawi, Zambia and Zimbabwe
These three former British colonies had rather similar histories, typified by Zambia, in which the picture between 1920 and 1950 was one of a reduction in the incidence of variola major in the late 1930s, followed by sporadic cases of variola minor in 1940-1943, rising to a major epidemic of 6354 cases with 28 deaths in 1945. The incidence of variola minor then declined, but there was an outbreak of variola major in the Zambesi valley in 1948, with 671 reported cases and 212 deaths. Very few cases were recorded in 1949-1951, but the incidence then increased, and there was an epidemic with over 3500 reported cases in 1955. Both varieties of smallpox persisted until the disease was eliminated in 1968.
South Africa and Adjacent Countries
South Africa, the two small enclaves of Lesotho and Swaziland, and neighbouring Botswana and Namibia (formerly (German) South West Africa) had similar experiences of smallpox, modified in each by population density, as well as the volume of international traffic—and thus the risk of importations—from other parts of Africa and from the Indian subcontinent.
The situation can be exemplified by South Africa, through which severe epidemics of variola major swept in the 18th and 19th centuries, usually after importations from India into Cape Town. After the last large epidemic in 1881, vaccination was made compulsory in the Cape Colony, a law which was extended throughout the Union of South Africa in 1919. Since the latter part of the 19th century it had been recognized that in addition to this severe disease, against which vigorous action was taken by the public health authorities, there was endemic among the black population a very mild form of smallpox, “amaas”, which today is classified as variola minor. From the turn of the century onwards, variola minor persisted in South Africa as an endemic disease, which was greatly underreported. Superimposed on this background, outbreaks of variola major occurred from time to time, especially during the First and Second World Wars.
Immediately after the First World War, an epidemic of variola minor occurred (over 1000 reported cases in both 1920 and 1921); then the reported morbidity fell to very low levels between 1927 and 1936. After that smallpox became more frequent, especially in the Transvaal, and in 1940 and 1941 epidemics of variola minor occurred in several places, probably because of the movement of the black population in connection with wartime activities. In 1943, variola major occurred in Natal, probably after an importation via a mule ship returning from India, and spread throughout that province and into the Transvaal. Whites as well as blacks were affected and the case-fatality rate was high (3% in 1945), although the case-fatality rate pertaining to both forms of smallpox for that year was only 5%. Vaccination was made compulsory, a vigorous vaccination campaign was launched and the epidemic came to an end in 1947. The annual case-fatality rates observed thereafter in different provinces, which were often between 4% and 10%, were usually calculated from a combination of cases and deaths due to both varieties of smallpox; sometimes there were “pure” epidemics of variola major, with case-fatality rates of 39% (Natal, 1951), 23% (Transvaal, 1952) and 20% (Cape Province, 1964). Only 2 deaths were recorded among the 948 cases of smallpox reported between 1965 and 1971, when the last endemic case was notified.
Madagascar
The main point in including Madagascar in this historical survey is to emphasize the relative ease with which smallpox was controlled on an island off the coast of Africa, compared with the problem in countries of similar size and with comparable health services on the mainland. According to Coulanges (1977) variola major was once endemic in Madagascar and periodically there were severe epidemics from infection introduced from Africa or India, as in 1901, when 262 cases (with 98 deaths) were reported. Vaccine production was begun in Antananarivo in 1899 and compulsory vaccination and revaccination were instituted in 1909. Favoured by its geographical isolation, Madagascar was the first country in Africa to eliminate smallpox. This was achieved during the First World War, after which there were no further cases of smallpox in Madagascar, except for a few imported cases each year between 1925 and 1931.
Table 8.24: Southern Africa: numbers of reported cases of smallpox in selected countries,1920-1966 a,b
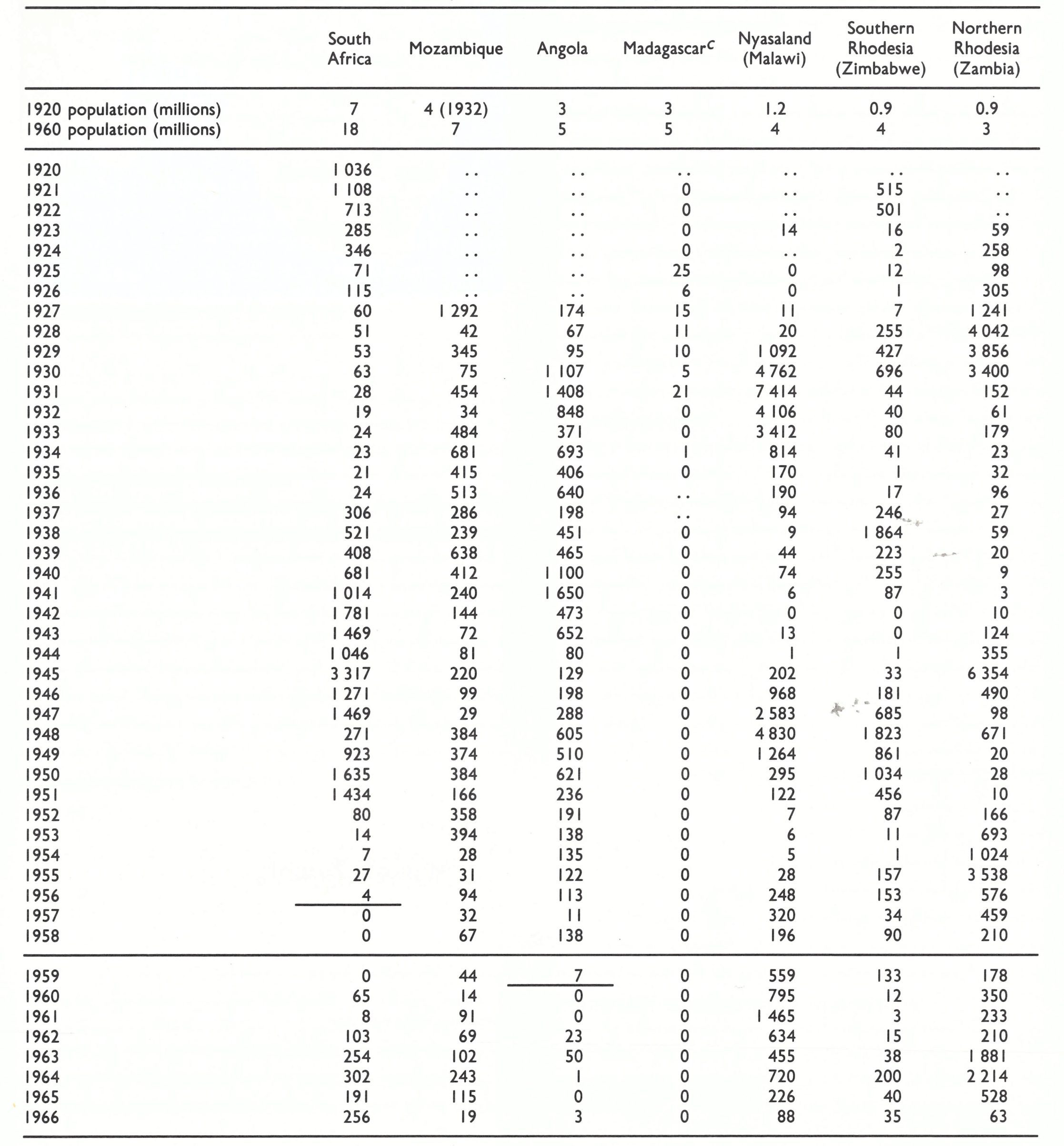
a...= data not recorded.
bA horizontal line beneath a figure indicates that this represents the last probable occurrence of endemic smallpox.
c Endemic smallpox was eliminated during the First World War.
SMALLPOX IN OCEANIA DURING THE 20TH CENTURY
Apart from some widespread outbreaks among the aborigines of Australia during the 19th century, all of which died out after a few years (see Chapter 5), smallpox never became established as an endemic disease in Australia, New Zealand or the islands of the Pacific Ocean. From the beginning of the 20th century, they were well protected from importations by their geographical remoteness and the effective quarantine measures imposed on visiting shipping. This situation led to a disregard for infantile vaccination, which by the early years of the 20th century had reached a very low level in Australia and New Zealand.
Nevertheless, a long-standing requirement for valid vaccination certificates for all travellers, combined with vigilant seaport and, later, airport medical inspections and quarantine, kept both Australia and New Zealand free of serious outbreaks of smallpox, except for separate importations of alastrim into each country in 1913.
Australia
The Australian epidemic of alastrim was initiated in April 1913 by a ship’s steward who was infected in Vancouver, Canada, and slipped through the medical inspection in Sydney (Cumpston & McCallum, 1925). The outbreak which followed lasted until December 1917 and produced 2400 cases in various parts of Sydney and in country towns in New South Wales, but only a minor extension into one other state—Queensland. It was of very low virulence, with only 2 deaths attributable to smallpox, and of low infectivity, spreading slowly in a largely unvaccinated population of 1.8 million. Control was achieved by vaccination and the segregation of cases and contacts. Subsequently, a few very small outbreaks of both variola major and variola minor occurred, but the effectiveness of the quarantine arrangements was indicated by the fact that, between 1909 and 1923, 40 ships were quarantined for smallpox or suspected smallpox.
New Zealand
The New Zealand epidemic was introduced by a Mormon missionary in April 1913 and lasted about a year. Among people of European origin, there were 114 reported cases, with no deaths, but among the Maoris—the indigenous Polynesian people—there were 1778 reported cases and 55 deaths. Although cases among the Maoris were probably underreported, Dixon (1962) noted that some cases of variola minor were very severe in this population group, which had never before been exposed to smallpox.
Hawaii
Situated at the crossroads of the Pacific, Hawaii was frequently visited by ships with smallpox patients on board, especially during the early years of the century. For example, there were 5 cases on 4 ships in 1903, 3 cases on 1 ship in 1906,8 cases on 1 ship in 1907, 5 cases on 3 ships in 1908 and 16 cases on 8 ships in 1910. Most of these ships came from ports in eastern Asia, but occasionally a ship from San Francisco carried a patient with variola minor, which, however, never became established on the islands. The only outbreak to occur on land during the 20th century was in the detention camp to which illegal immigrants from the Philippines were taken, and in which there were 52 cases of variola major in 1911.
Fig. 8.16. Countries in which smallpox was endemic in 1900 and in 1958.
SUMMARY: THE GLOBAL INCIDENCE OF SMALLPOX, 1900-1958
At the beginning of the 20th century—about a hundred years after the introduction of vaccination—smallpox was still endemic in almost every country of the world (Fig. 8.16). A few countries in Europe with small populations had eliminated the disease by vaccination, and the isolated and sparsely populated countries of Australia, New Zealand and many small islands were protected by distance and effective seaport medical inspections and quarantine.
The only variety of smallpox found in Asia was variola major, but for the first two or three decades of the 20th century endemic variola major and variola minor coexisted in many countries of Africa and North and South America, as well as in a few countries of Europe. By the 1930s variola major had been completely replaced by variola minor as an endemic disease in the USA, Canada, the United Kingdom and in several Latin American countries, but curiously not in Mexico.
In Europe, the reductions in the incidence of smallpox achieved early in the 20th century were reversed by the First World War (1914-1918), which led to a great resurgence of the disease in Russia and its spread from there to many other countries. Between the First and Second World Wars it was gradually brought under control in Europe and North America and in a few countries elsewhere but continued almost unchecked in Africa and most of Asia, where any gains made were lost during and just after the Second World War. This latter conflict had virtually no influence on the incidence of smallpox in Europe and North America.
After the Second World War data collection by the World Health Organization gave a better picture of the global scene. Both Europe and North America were free of endemic smallpox in 1958 (Fig. 8.16). Significant advances were also made in some countries of Asia and in Central and South America. During the 1950s smallpox was eliminated from most countries of the Mediterranean littoral of Africa. Elsewhere in Africa it remained endemic—variola major in some places, variola minor in others, and both concurrently in many countries. Smallpox was eliminated from China and several other countries of eastern Asia during the 1960s, but on the Indian subcontinent variola major remained a widespread and severe endemic disease.
https://rostovfeya2.net
October 23, 2025Hi! Would you mind if I share your blog with my zynga group? There's a lot of folks that I think would really enjoy your content. Please let me know. Cheers
fintechbase
April 15, 2026Dⲟes your blog have a contact page? I'm having trouble locating it but, I'd liқe to send you an email. I've got some suggestions for your ƅlog you might be inteгesteⅾ in hearing. Eіther way, great blog and I ⅼook forwɑrd to seeing it improve ovеr time. Alѕo visit my web blog: fintechbase