Chapter 9:
Development of the global smallpox eradication programme,1958-1966

THE COMMITMENT TO GLOBAL SMALLPOX ERADICATION, 1958-1959
The decision by the Twelfth World Health Assembly, in May 1959, to undertake the global eradication of smallpox marked the beginning of a programme which, some 18 years later, would witness the last naturally occurring case. The Health Assembly’s policy, which made the global eradication of a disease one of WHO’S goals, was not without precedent, a similar decision with regard to malaria having been taken 4 years before.
The commitment to smallpox eradication in 1959 represented, for the Health Assembly, an abrupt reversal of its views regarding the disease. The problem of smallpox and its control had been the subject of discussions in the Health Assembly in 1950,1953,1954 and 1955. An eradication programme had been proposed, in fact, by the first DirectorGeneral, Dr Brock Chisholm, to the Sixth World Health Assembly in 1953. However, after 2 years of study and debate, the Eighth World Health Assembly, in May 1955, rejected the concept as unrealistic, and the terse resolution which was adopted (WHA8.38) simply urged “that health administrations conduct, wherever necessary, campaigns against smallpox as an integral part of their public-health programmes” (World Health Organization, 1973a).
From 1955 to 1958, the issue of smallpox eradication lay dormant but, at the Eleventh World Health Assembly, Professor Viktor Zhdanov, Deputy Minister of Health of the USSR and a delegate to the Health Assembly, presented a formal, lengthy report which argued that the problem of smallpox was an important one for endemic and non-endemic countries alike, that eradication was theoretically feasible and that national programmes had demonstrated it to be a practicable possibility (World Health Organization, 1958a). The report concluded: “AS regards its complete eradication throughout the world, we think that this can be achieved within the next ten years.” No reference was made to an 8-year-old regional programme for smallpox eradication in the Americas nor to the Health Assembly’s earlier discussions on smallpox. The USSR had not participated in those discussions, however, having withdrawn from active participation in WHO from 1948 to 1957.
The new initiative originated with Professor Zhdanov himself. From 1951, when he had first assumed responsibility for communicable disease control in the USSR, as Chief of the Department of Sanitary and Epidemiological Services, he had taken an active interest in the concept of disease eradication. His interest was stimulated, in part, by the successful interruption of smallpox transmission throughout the USSR in 1936, and by the elimination of dracunculiasis from the Central Asian republics of the USSR following a 10-year campaign that ended in 1932 (Isaev, 1956; Litvinov, 1970). These successes led him to initiate a study of infectious diseases in the Soviet Union for the purpose of identifying others which might similarly be eliminated (Zhdanov & Timakov, 1952). By assigning more resources in the short term to disease elimination, longer-term savings could be anticipated. Smallpox remained a problem, however, particularly in the Central Asian republics, because of importations from Afghanistan and Iran, 537 cases being recorded between 1950 and 1957 (Burgasov, 1968). Professor Zhdanov’s report to the Health Assembly pointed out that the danger which endemic countries posed to others caused “the countries which are free from smallpox…to make considerable efforts and spend large sums on vaccinating and revaccinating the population in order to provide constant strong immunity against this disease”. Smallpox, as he saw it, would be much easier to eradicate than any of the other infectious diseases, as indicated by the success of the programme in the USSR. Despite the diverse problems presented by a country so large and abundantly populated, transmission had been stopped by means of a programme of compulsory vaccination (Vasil’ev & Vasil’ev, 1982). For other countries to do likewise seemed both logical and feasible and the USSR was willing to offer its assistance to support such efforts. In addition to offering 25 million doses of vaccine to WHO, it informed the Director-General at the twenty-third session of the Executive Board that it had sent offers of assistance to Burma, Cambodia (later Democratic Kampuchea), Ghana, Guinea, India, Indonesia, Iraq and Pakistan (World Health Organization, 1959a).
Plate 9.1. Viktor M. Zhdanov (b. 1914). Academician and Deputy Minister of Health of the USSR, 1955-1960, proposed to the World Health Assembly in 1958 that WHO should undertake the global eradication of smallpox. Many epidemiologists whom he trained while Director of the Ivanovsky Institute served as WHO staff and consultants for the eradication of smallpox.
The Eleventh World Health Assembly was held in Minneapolis, Minnesota (USA), and, with this venue in mind, Professor Zhdanov introduced his report with a quotation : “AS early as 1806, the President of the United States of America Thomas Jefferson… said in his letter to Jennet: ‘It is owing to your discovery…that in the future the peoples of the world will learn about this disgusting smallpox disease only from ancient traditions.’’The Zhdanov report proposed that vaccination and revaccination campaigns should be conducted throughout the endemic areas of the world, commencing in 1959. It recommended that vaccination should be made compulsory and that freeze-dried vaccine should be used. It also suggested that the programme could be accelerated if the Leicester system were introduced as well. This system, as noted in the report, was used for outbreak control, mainly in England (see Chapter 6), and resembled what eventually came to be called surveillance-containment activities—nanamely, “prompt identification of the disease, special notification, isolation, quarantine, disinfection measures”—although it included the “eradication of flies” as well (Fraser, 1980).
The draft resolution introduced by the USSR in 1958 for consideration by the Health Assembly differed from the report in suggesting that eradication in 4-5 years was possible in accordance with the following timetable: (1) preparation of the necessary amount of vaccine in 1958-1960 and the training of vaccinators; (2) vaccination during 1959- 1960 of the populations in which principal endemic foci existed; and (3) completion of eradication in 1961-1962 by additional vaccination and revaccination. Nothing was said of the Leicester system in the resolution.
The concept of global eradication was broadly endorsed by virtually all the delegates who spoke, although a number believed that the timetable was too optimistic and some wondered whether there might not be insuperable technical and administrative problems. Accordingly, the resolution was altered to request “the Director-General to study and report to the Executive Board … on the financial, administrative and technical implications of a programme having as its objective the eradication of smallpox” (see box).
Immediately after the Health Assembly, the Executive Board met and formally accepted the gift of freeze-dried vaccine from the USSR, as well as 2 million doses of glycerolated vaccine offered by Cuba. The Board noted in resolution EB22.Rl2 that the Director-General would establish a special account for smallpox eradication, which would “be credited with the value, as reported by the governments concerned, of these gifts of vaccine and of any gifts for the same purpose which may be accepted by the Board or the Health Assembly in the future” (World Health Organization, 1973a). The resolution included an important provision: “REQUESTS the Director-General to ensure, in accordance with the normal practice of the Organization, that any vaccine accepted for the anti-smallpox programme is of acceptable quality.” Aware that standards for the potency and purity of vaccines of all types were not uniform throughout the world, and even nonexistent in some countries, Mr Milton P. Siegel, an Assistant Director-General of WHO, had drafted this cautionary proviso. As the Director-General noted: “…there were no international standards for vaccines. It was hoped that the Expert Committee on Biological Standardization would establish such standards soon” (World Health Organization, 1958b). This was done, in fact, in November 1958 and formalized in resolution EB23.R40 at the next session of the Executive Board (World Health Organization, 1959a). The stipulation with regard to vaccine quality was to prove most important, and after 1967 it was interpreted by WHO smallpox eradication staff as applying to all vaccines supplied to WHO-supported smallpox eradication programmes, whether or not they were provided through contributions to WHO (see Chapter 11). The Director-General, as requested, submitted to the Executive Board in January 1959, and later to the Twelfth World Health Assembly, a lengthy report concerning the financial, administrative and technical implications of a smallpox eradication programme (World Health Organization, 1959b). It was based in part on replies to questionnaires received from 20 countries. The report noted that “it is generally agreed that eradication of smallpox from an endemic area can be accomplished by successfully vaccinating or revaccinating 80 per cent of the population within a period of four to five years”. The global programme, as envisaged by WHO, would require national mass vaccination campaigns operated by a smallpox eradication service which would be “integrated with the general public health services” but “directed, or at least co-ordinated, centrally”. Freeze-dried vaccine was recommended for use in tropical and remote rural areas and glycerolated vaccine where refrigerated storage and transport were available. The plan proposed that the Organization’s Headquarters’ budget should make provision for the recruitment of a fulltime medical officer, epidemiological consultants (12 man-months per year) and laboratory consultants (6 man-months per year), as well as for the funding of an international conference and 2 training courses on vaccine production, and for the cost of distributing vaccine supplies. WHO regional office budgets would include provision for fellowships and consultants.
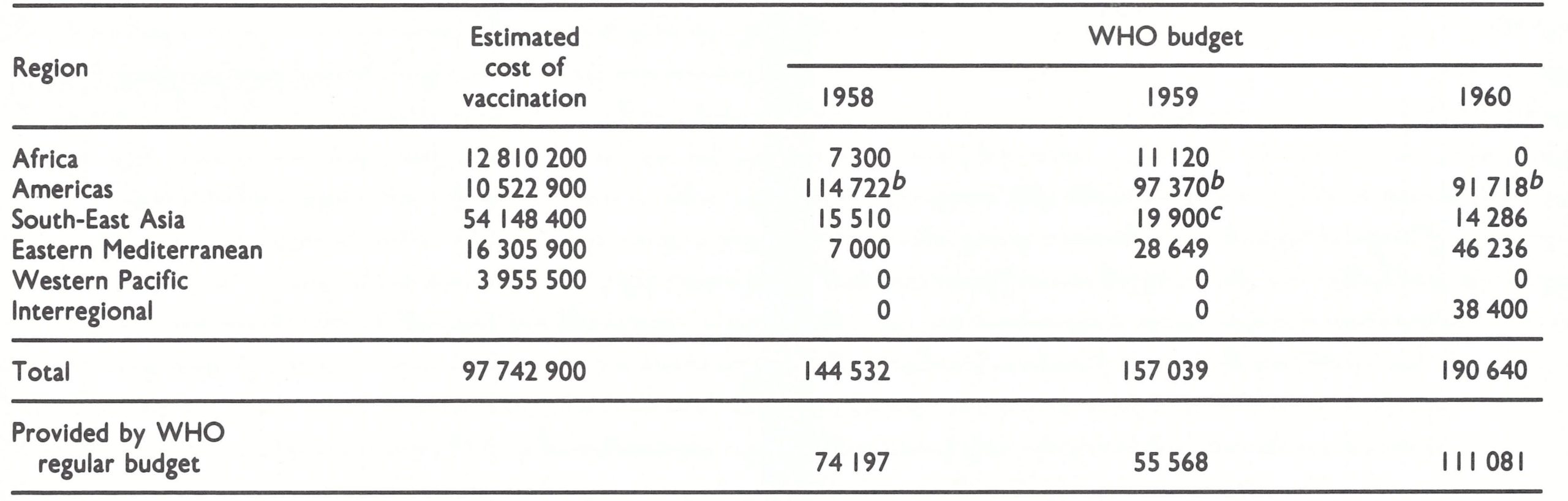
The Director-General’s report estimated that approximately 977 million people then lived in endemic areas and, if all were to be vaccinated, the cost, calculated at US$0.10 per person, would amount to about US$97.7 million (World Health Organization, 1959b). No mention was made in the report of the People’s Republic of China, which was not then a Member of WHO. The report pointed out that all countries were already spending considerable sums for the control of smallpox but speculated that the total costs, as estimated for each country, would be “appreciably higher than their present authorized budget provision for this purpose”. The WHO budget for smallpox control was noted by the Director-General to have been negligible in previous years except in the Americas, where US075 000 had been authorized in 1952 for this purpose, and US$l44 089 in 1954. Although the report pointed out that “large sums are again set aside for the years 1958-1960 to continue the work” (Table 9.1), it also stated that even larger sums would be required in future years.
Table 9.1: Estimated cost of smallpox eradication as at 1959, and budget for smallpox programmes, 1958-1960 (US$)a
 Source: World Health Organization (1959b).
Source: World Health Organization (1959b).
a The estimated costs of vaccination were calculated on the assumption that all persons in countries then Infected would be vaccinated at a cost of US$0.10 each. The People’s Republic of China, not then a Member State of WHO, was not mentioned in the report, nor were the costs for a programme there included In the estimates.
b Includes both WHO and PAHO funds, most of which were allocated to a yaws-smallpox eradication programme in Haitl.
c Includes US$ I6 000 from UNICEF.
The report was discussed both at the Executive Board and subsequently at the Twelfth World Health Assembly (1959), although few substantive comments were made. At the conclusion of the debate, the delegates voted unanimously in favour of the programme. Nothing was said about the wide discrepancy between the identified need and the proposed WHO budget, nor was a request made for additional resources to be provided through voluntary contributions. Indeed, the only doubt about the feasibility of global eradication was expressed by a delegate from South Africa, who indicated that, without knowing the exact position in all other countries, he could not say whether worldwide smallpox eradication was a practical proposition; nevertheless, he supported the resolution. Other delegates presented encouraging reports on their own successes in undertaking smallpox vaccination campaigns and in producing vaccine. The operative paragraphs of the resolution adopted (see box) were as significant for what was omitted as for what was said. No reference was made in them to the reporting of cases, the containment of outbreaks, or a timetable for the achievement of eradication, whether within a 10-year period, as suggested in the report presented by Professor Zhdanov, or in 5 years, as suggested in the resolution adopted by the Eleventh World Health Assembly.
Although the resources budgeted for the programme were modest indeed, Professor Zhdanov’s ambitious proposal had been accepted, at least in principle, and the programme for the global eradication of smallpox formally began.
Resolution WHA12.54, adopted at the Twelfth World Health Assembly in 1959
“Having considered the report of the Director-General on smallpox eradication [ Oficial “Noting : Records the World Health Organization, 95, Annex 181, "Nothing:
- That although great progress has been made in the eradication of the disease in some areas of the world, important endemic foci of smallpox still remain in other areas, especially in South-East Asia and Africa, from which the disease can be exported to countries already free of it;
- That eradication of smallpox from an endemic area can be accomplished by successfully vaccinating or revaccinating 80% of the population within a period of four to five years, as has been demonstrated in several countries;
- That sufficient scientific and technical information is available on the production of a suitable smallpox vaccine; and
- That although an eradication programme may require, for four or five years, an increase in the national efforts and financial obligations for the intensified campaign against smallpox, the heavy annual burden of continuing expenditure incurred for this purpose may be considerably lightened by increasing the interval between vaccinations once eradication may be considered to have been accomplished.
1. Emphasizes the urgency of achieving world-wide eradication;
2. Recommends to the health administrations of those countries where the disease is still present that they organize and conduct, as soon as possible, eradication programmes, making provision for the availability of a potent stable vaccine;
3. Requests the Director-General:
- To urge health administrations of those countries where the disease is still present to develop eradication programmes and to offer them any necessary technical guidance and advice;
- To provide for the necessary activities to further smallpox eradication programmes and for the assistance requested by national health administrations for this purpose, in his programme and budget for future years; and
- To collect from the countries concerned information on the organization and progress of their respective eradication programmes and to report further to the Thirteenth World Health Assembly.
HISTORY OF THE CONCEPT OF ERADICATION
Introduction
The acceptance, as public health policy, of a planned programme designed to eradicate a disease over a large geographical area is a comparatively recent development, and the extension of such a policy to encompass the entire world is an even more recent one (Andrews & Langmuir, 1963). Even in 1958, and indeed for nearly two decades afterwards, the feasibility of global eradication of any disease was by no means universally accepted by the scientific community. However, smallpox was not the first disease to be considered seriously as a target for eradication, nor was the programme the first global campaign to be mounted. Because the personalities, attitudes and practices in previous programmes played an important role in the development and evolution of the smallpox eradication programme, it is important to consider briefly its historical antecedents.
Some would take issue with the assertion that smallpox was not the first disease to be considered for eradication, and in argument cite Jenner (1 800) who wrote: “. . . Cow Pox, an antidote that is capable of extirpating from the earth a disease which is every hour devouring its victims: a disease that has been considered as the severest scourge of the human race!” Others at this time (Carl, 1802) echoed this belief, but the views were more expressions of hope than expectations for the implementation of a broadly conceived international programme.
Following Jennet’s discovery, compulsory vaccination in several European countries resulted in the absence of the disease from a number of them over many years; also, in some small island states and isolated countries, smallpox occurred only sporadically, as a result of importations. However, government authorities, recognizing that smallpox could readily be reintroduced at any time, never spoke in terms of its eradication. The idea was not voiced again until 1949, at which time the Director of the Pan American Sanitary Bureau (the headquarters and secretariat of the Pan American Sanitary (later Health) Organization and WHO Regional Office for the Americas) proposed that such a programme should be undertaken throughout the Western Hemisphere. Meanwhile, efforts to control many other diseases, both animal and human, were being actively pursued.
The possibility of eradicating a disease or its vector emerged as a concept in the late 1800s with the improving scientific understanding of the causation and mechanism of transmission of various diseases and the discovery of methods for preventing them. As applied to a definitive policy, the term eradication appears to have first been used in 1884 in reference to a programme in the USA for the control of an animal disease, bovine contagious pleuropneumonia. Only 4 years later, however, Dr Charles Chapin (quoted in Soper, 1965) was to observe that preventive measures for any disease, if diligently applied, could potentially lead to eradication. He boldly asserted that any disease which could be prevented in part could be prevented in its entirety, and suggested that this might apply specifically to tuberculosis. Gradually, the term eradication came into wider use and, over the years, it was given a variety of definitions. Some authorities asserted that the term should be applied only when a disease pathogen had become extinct throughout the world, while others argued that it could mean simply the reduction in the incidence of a disease to the point where it ceased to be a public health problem (Cockburn, 1963).
In this publication, the term eradication is used in a narrower sense as suggested by its Latin derivation—eradicare, literally “to root out” or “to tear out by the roots”. Most eradication programmes, as such, have been concerned with communicable diseases, although diseases induced by toxic substances could certainly be eradicated by eliminating the offending substances. However, to use the term eradication with regard to programmes directed towards preventing traffic accidents or hunger, as some have done, is obviously inappropriate. For communicable disease programmes, Andrews & Langmuir (1963) provide the most widely accepted distinction between control and eradication: “Control is the purposeful reduction of specific disease prevalence to relatively low levels of occurrence, though transmission occurs frequently enough to prevent its permanent disappearance.” Eradication, however, as they state, proceeds “to the point of continued absence of transmission within a specified area”. While recognizing that the unqualified use of the word eradication signifies the world-wide extermination of a biological species, they accept the use of the word when applied to a specified geographical area—in effect, “area eradication”.
The question of how large a specified area must be in order to apply usefully the term eradication has frequently been a contentious issue. Measles illustrates the quandary as to what the lower limits should be. The eradication of measles in a household or district in a city means little, since transmission periodically ceases in such small areas without the application of control measures, and reinfection regularly occurs. But should one speak of eradication of measles from a state or province, for example, or should the notion apply only to a continent or even larger area? Views differ on this question but most epidemiologists now prefer to use the term eradication only when the area covered is sufficiently large and geographically delimited and the characteristics of the disease or vector are such that reinfection or reinfestation is unlikely. Previous successful programmes, which are described below, are by these criteria properly called area eradication programmes.
Eradication of Animal Diseases
For a number of reasons, national programmes to eradicate animal diseases or pests antedate the first human disease eradication programmes and have been more consistently and vigorously pursued over the past century. To begin with, the measurable economic consequences of animal diseases have usually made it easier to obtain support for animal disease control programmes than for those for human diseases, whose economic consequences are often more difficult to quantify. Moreover, in dealing with animal diseases, useful strategies are available which cannot be employed in controlling human disease, the most important being the ability to apply rigid quarantine measures and to slaughter entire flocks or herds found to be infected. Finally, those concerned with animal husbandry have focused their attention more on the prevention of diseases than on their treatment.
It is not surprising, therefore, that the first planned programme whose stated objective was eradication was one intended to eliminate a disease of cows—bovine contagious pleuropneumonia (Hinman, 1966). This highly fatal disease had been brought from Europe to the USA (New York State) in 1843. Gradually, it spread to the large midwestern cattle-raising areas, and other countries eventually began to embargo imports of livestock from the USA. To deal with the problem, the United States Congress, in 1884, created the Bureau of Animal Industry, whose specific responsibility was to eradicate bovine pleuropneumonia. During a 5-year campaign the disease was eliminated, and the precedent and mechanisms for attacking other animal disease problems were established. Subsequent area-wide eradication programmes, again defined as such, were successfully conducted in the USA against a number of other animal diseases, including glanders (a disease of horses and mules), piroplasmosis (Texas fever) of cattle, and dourine (a sexually transmitted disease of horses) (Hagan, 1958). Rinderpest and sheep pox were eradicated from most countries in Europe late in the 19th century, and early in the present century eradication was accepted as the standard procedure for dealing with importations of serious exotic diseases of livestock into the industrialized countries of Europe, North America and Oceania.
The strategy differed from disease to disease, the approaches adopted depending on the mode of spread of the disease and the most effective point in the cycle of transmission at which to intervene in order to stop dissemination, whether by the isolation and slaughter of infected herds or the killing of vectors. Specific characteristics of the diseases in question were vital to the success of these efforts, among the most important being that the diseases had been introduced comparatively recently into the target areas from other countries and that they tended to be geographically circumscribed. Moreover, it was usually possible to diagnose them easily, subclinical infections and carriers were rare, and none had become enzootic in wild animals. Success in solving the diverse problems involved suggested that there might be a number of microorganisms which clung so tenuously to an ecological niche that simple measures could be found to upset the balance of nature. Intensive, albeit costly, short-term programmes in these instances could be more productive and ultimately less expensive than long-term control efforts and the acceptance of continuing damage to livestock.
Thus, planned programmes for disease eradication on a national scale were a familiar concept to workers in veterinary medicine but the achievements of such programmes were largely unknown to those concerned with human disease. For human diseases such as smallpox, cholera, plague and yellow fever, quarantine regulations were adopted to prevent their introduction into a country, and, in the case of smallpox, intensive vaccination campaigns were conducted when the disease was imported into smallpox-free areas. Until the present century, however, the term eradication, in the sense of a planned programme whose stated aim was the elimination of a human disease throughout a defined geographical area, was not used.
The First Eradication Programmes for Human Diseases—Hookworm and Yellow Fever
Hookworm was the first disease to be considered seriously as a candidate for global eradication, and the first for which a programme was actually mounted. That programme, begun in 1909, was soon followed by a global programme for the eradication of yellow fever. Since the operational methods and styles of leadership adopted in subsequent eradication programmes had their roots in these two campaigns, their history is of interest.
From what is now known of the biology of the two diseases, neither was a reasonable candidate for eradication, but, when the programmes began, inadequate scientific knowledge, coupled with a visionary outlook and excessive optimism, made them appear suitable. The extensive campaigns which ensued left an important legacy in the development of public health services and education in many countries. But, as the programmes progressed and more was learned about these and other diseases, it became increasingly apparent that the causative organisms were remarkably well adapted to their ecological niches and had more intricate and complex relationships with the human and natural environments than had been appreciated. Gradually, it became apparent that disease eradication was a formidable, perhaps even an unattainable, goal (Smith, 1934; Burnet, 1940; Dubos, 1959, 1965).
Hookworm eradication
Early this century, a United States public health official, Dr Charles Wardell Stiles, had the vision of totally interrupting the spread of hookworm in the southern states of his country by a systematic campaign in which infected persons would be identified by stool examination and their infections eliminated by drug therapy. The construction of sanitary privies during this period would prevent faecal contamination of the soil and thus break the transmission cycle, in which hookworm larvae enter the human body through the skin of the feet, migrate to the intestinal mucosa where they feed on blood in the capillaries, and shed eggs that are passed in the faeces to the soil and there develop into larvae. Advisers to Mr John D. Rockefeller, then increasing his support to philanthropic projects, studied the proposition and pronounced it sound. The Rockefeller Sanitary Commission for the Eradication of Hookworm in the United States was established in 1909, and a sum of US$1 million was pledged to be spent over 5 years. Dr Wickliffe Rose, a professor of philosophy, was appointed director of the programme.
Over the first 5 years of the hookworm eradication programme in the USA, extensive operations were carried out in 11 states. By 1914, the Commission reported having screened more than 2 million persons, of whom 500 000 were treated in mobile dispensaries; more than 250 000 rural homes were inspected by sanitary personnel. This undertaking, involving thousands of workers, was the largest and most complex community-wide health programme ever to be carried out in the USA up to that time.
With the establishment in 1913 of the Rockefeller Foundation, Dr Rose was made Director of its International Health Commission, into which the Sanitary Commission was incorporated. The Foundation made a policy decision to “confine itself to projects of an important character, too large to be undertaken, or otherwise unlikely to be undertaken, by other agencies” and to “go to the root of individual or social ill-being and misery” (Fosdick, 1952). Hookworm eradication clearly satisfied these criteria. Thus, as its first initiative, the Foundation’s trustees decided “to extend to other countries and people the work of eradicating hookworm disease as opportunity offers, and so far, as practicable to follow up the treatment and cure of the disease with the establishment of public sanitation and the spread of scientific medicine”. In the following years, cooperative programmes were extended to 52 countries on 6 continents and to 29 island groups.
Not for a number of years were careful field studies conducted to determine whether, given effective execution of the prescribed strategy and tactics, the parasite had actually been eradicated. When such studies were finally conducted, they showed that, even with an effective programme, infection rates did not significantly diminish, although those infected had fewer worms and therefore less illness due to the disease (Smillie, 1922). It was apparent that the biology of hookworm was far more complex than had been appreciated, and that the methods of attacking it were inadequate. Dr William Cort, then the leading authority on hookworm disease, pleaded for more research in both areas but, in doing so, studiously avoided using the word “eradication” (Cort, 1921); the Foundation, at least so far as hookworm was concerned, eventually followed suit. The control programme was remarkably successful in establishing a network of 4-person county health departments (health officer, sanitary engineer, public health nurse and secretary) in the southern USA, and many other countries created similar structures, but hookworm has remained a problem in most developing countries.
Yellow fever eradication
Success in the control of yellow fever in Cuba and Panama laid the groundwork for yet another, apparently more plausible, programme for disease eradication for which the Rockefeller Foundation was also to provide leadership and substantial support. Recurrent severe epidemics of yellow fever had plagued cities in the USA since the 17th century, but the disease had never become endemic. By the end of the 19th century, it was believed that most of these epidemics were the consequence of importations of the disease from Cuba (Strode, 1951). Thus, when Cuba was occupied by United States forces in 1898, during the Spanish-American War, yellow fever control was of special interest to the authorities.
In 1900, a government Yellow Fever Commission, directed by Major Walter Reed, was charged with the responsibility for ascertaining the cause and mode of spread of the disease and for finding methods for its control. A series of brilliant studies rapidly provided the critical insights into the epidemiological behaviour of the disease that permitted an effective control programme to be implemented. Building on the belief of the Cuban scientist, Dr Carlos Finlay, that a mosquito vector was involved, the Commission demonstrated conclusively that the vector was the mosquito Stegomyia fasciata (Aedes aegyptz), which bred almost exclusively in and around houses. Moreover, drawing on observations by Dr Henry Carter, the Commission showed that there was an interval of 9-16 days between the time at which a mosquito took a blood-meal and the time at which it could transmit infection, and that person-to-person spread via excreta or fomites never occurred (Reed et al., 1900). If mosquito control measures were to be introduced and patients isolated in screened quarters, the prospects for yellow fever control looked hopeful.
The Chief Sanitary Officer for Cuba, Dr William Gorgas, then a major in the United States Army Medical Corps, assumed responsibility for the programme. Patients were isolated in screened quarters, and breeding sites for the mosquitos were eliminated by the removal of discarded cans and bottles, in which they bred; in addition, cisterns were coveted with netting and kerosene was applied to water surfaces which could not be otherwise treated (Gorgas, 1911b). The programme was a quasi-military operation, which began on 4 February 1901 and in which teams of 3 inspectors were assigned responsibility for groups of 1000 houses, to be inspected at the rate of 30 houses per day. On 28 September 1901, the last case of yellow fever occurred in the city of Havana proper, only 8 months after the programme had begun-indeed, some 2 weeks before Reed & Carroll (1902) discovered that the disease was caused by a filterable virus. Shortly thereafter, the disease was discovered in a suburb of Havana, but similar operations there promptly terminated transmission and yellow fever vanished from Cuba. Dr Gorgas, in his report of 12 July 1902 to Brigadier General Leonard Wood (Gorgas, 1911a), stated: “I look forward in the future to a time when yellow fever will have entirely disappeared as a disease to which man is subject, for I believe that when the yellow fever parasite has become extinct it can no more return than the dodo or any other species of animal that has disappeared from the earth.”
The efficacy of the measures taken was soon confirmed in Panama. In June 1904, Dr Gorgas was named Chief Sanitary Officer for the Isthmus of Panama, where the Panama Canal was then under construction. After an epic 16-month effort, Panama also became free of yellow fever (McCullough, 1977). Success was achieved even though the campaigns were restricted to urban areas, and the vector was substantially reduced in numbers but not eliminated. In 1908, Dr Oswaldo Cruz added independent confirmation of the efficacy of Dr Gorgas’s methods by eliminating yellow fever from Rio de Janeiro. On the basis of these experiences, Dr Gorgas concluded that the transmission of yellow fever could be sustained only in the more densely populated urban areas and that eradication could be achieved by short-term campaigns against A. aegypti in a few key endemic urban centres (Gorgas, 1908).
Some 6 years later, in 1914, the desirability of testing this hypothesis on a wider scale was suggested to Dr Rose during a visit to Asia. Throughout Asia, he found health officials to be profoundly concerned that yellow fever might be imported as a consequence of the opening of the Panama Canal in that year and the resulting increase in maritime traffic. Although yellow fever did not then occur in Asia (nor is it known to have occurred since that time), the potential mosquito vectors were widely prevalent. If the disease were introduced, massive epidemics could be expected. Dr Rose consulted Dr Gorgas, then Surgeon-General of the United States Army, who expressed the opinion that yellow fever could be “eradicated from the face of the earth within a reasonable time and at a reasonable cost” (Fosdick, 1952). On 26 May 1915, definitive action was taken by the International Health Commission to set such a programme in motion, by its adoption of the following resolution :
“Whereas, yellow fever has been endemic in tropical and subtropical America for centuries, constituting a serious menace in the infected areas and a perennial source from which epidemics have spread to more remote regions both in America and Europe, involving great loss of life and interrupting industry and trade over vast areas, and
“Whereas it has been shown by the work done in Havana and Panama under the direction of Dr William C. Gorgas and in Rio de Janeiro under the direction of Dr Oswaldo Cruz that the infection can be eradicated even in communities where it is endemic, and
“Whereas, the opening of the Panama Canal and the changing of trade relations resulting therefrom have given rise to widespread apprehension that yellow fever may be introduced into the Orient; and that once endemic in these densely populated regions it would become a permanent menace to the rest of the world; therefore “Be it resolved, that the International Health Commission is prepared to give aid in the eradication of this disease in those areas where the infection is endemic and where conditions would seem to invite cooperation for its control.” (Strode, 1951.)
Plate 9.2. William Crawford Gorgas (I 854 – 1920). after successfully freeing Cuba and Panama of yellow fever, encouraged the Rockefeller Foundation to support a global effort to eradicate the disease. Launched in I9 18. with Gorgas as director, this work was the first serious attempt to eradicate a human disease. Its principal technology, vector control, became the basis of subsequent efforts to eradicate the mosquito vectors of malaria and other diseases.
It was anticipated that eradication in the Americas would require perhaps 5 years; further study would be needed to determine a timetable for Africa, the only other endemic area. Soon afterwards, a resolution calling for the eradication of yellow fever from the Americas was approved by the I1 Pan American Scientific Congress (1915-1916) (Duffy, 1977). Between 1916 and 1949, the Rockefeller Foundation was to spend USSl3.8 million on yellow fever control (Strode, 1951).
With the new yellow fever eradication programme and a continuing campaign against hookworm, a critical need arose for skilled physicians trained in organization and management and having a scientific understanding of these diseases. Partly to meet this need, Dr Rose proposed in 1916 that schools of public health should be founded with support from the Rockefeller Foundation. The first of these was established at The Johns Hopkins University. Over the succeeding decade, 23 other schools based on this model were established and supported in 20 different countries in North and South America, Europe and Asia.
The start of the yellow fever eradication campaign was delayed by the First World War, but in 191 8 programmes supported by the Rockefeller Foundation were launched in Guayaquil, Ecuador, and in towns on the Pacific coast of South America at risk of infection from Guayaquil. They were soon extended to other known or suspected foci in the Central American countries, Mexico and Peru. The campaign was predicated on the belief that there was no animal reservoir and that yellow fever was unable to persist as an endemic disease in urban populations of less than 50 000. Campaigns to interrupt transmission were thus conducted only in the cities and larger towns but were extended to smaller towns to control outbreaks when they occurred. Transmission appeared to cease when breeding sites of A. aegypti were found in only 5%”, or fewer of the houses, and thus control, not eradication, of the vector constituted the basic strategy. At first it was dramatically successful. Transmission ceased in Guayaquil after only 6 months, in Peru in 1921 and in Central America in 1924.
Brazil organized its own programme in 191 9 but halted it in 1922 when the “disease had disappeared from the statistics” (Soper, 1965). Yellow fever reappeared in 1923, however, and the Rockefeller Foundation was requested to provide support. Again, rapid progress was made, and from April 1927 to March 1928 no cases were reported from anywhere in the Americas. Meanwhile, in preparation for programmes in Africa, the Rockefeller Foundation established laboratories there to undertake special studies of the disease.
In March 1928, however, cases of yellow fever were again detected in north-east Brazil and, in May, cases appeared in the capital, Rio de Janeiro—the first cases there since Dr Cruz’s campaign 20 years before. From Rio, cases spread rapidly and widely throughout the country, the first such spread of yellow fever from a key urban centre since the programme had begun. At the same time, outbreaks whose sources could not be identified occurred also in Colombia and Venezuela. Many people began to express doubts about the feasibility of yellow fever eradication, and the Rockefeller Foundation, simultaneously faced with a failing anti-hookworm campaign, began to be criticized for its support of disease eradication (Soper, 1965).
The crisis of the Rio de Janeiro epidemic precipitated a series of changes which, in turn, altered the administrative structure of the programme and eventually led to a redirection of its goals. At the same time, it established precedents for centralized, independent programme operations which were to characterize subsequent malaria eradication programmes. Field activities, previously directed by a combination of national and state authorities and Foundation staff, were integrated over a 3-year period into a single National Yellow Fever Service under the direction of Dr F. L. Soper, a Foundation staff member who had worked in the anti-hookworm campaign in Brazil since 1920. No national disease control programme of such magnitude had been undertaken before this time. It was supported in part by the Brazilian government and in part by the Foundation.
The 1928-1929 outbreaks, some of which occurred outside urban areas, dramatized the need for disease surveillance. Information as to where yellow fever was occurring was vital but until 1930, there was no organized system for detecting and reporting cases. Because programme staff had assumed that endemic disease could persist only in urban areas with populations of 50 000 or more, and because the disease was severe and often fatal, they believed that the presence of yellow fever would inevitably become known without much delay. In fact, few hospitals or health units outside urban areas regularly reported suspected cases, and from most areas there were no reports at all. Not until 1930 was it appreciated that the absence of reports did not necessarily mean the absence of cases. To obtain accurate reports, however, was difficult because, clinically, yellow fever resembled other illnesses with fever and jaundice. Neither virology nor immunology was then sufficiently advanced for satisfactory diagnostic methods to have been developed, but, fortunately, the liver pathology of patients with yellow fever was characteristic of the disease. Thus, pathological diagnosis was employed to determine the etiology in fatal cases. To obtain the necessary specimens, the Brazilian government ordered that a specimen of liver should be obtained from all patients who had died within 11 days of the onset of a febrile illness (Soper et al.,1934). A viscerotome was devised (Rickard, 1931) that was simple enough to be used by a layman after brief training. A field organization of viscerotomists was set up, a small payment being made for each specimen provided. It soon became apparent that there was widespread endemic disease in rural areas of the north-east (Soper et al., 1933), and in 1932 the first definitive evidence was obtained that wild animals constituted a jungle reservoir of the disease (Soper, 1936), a fact soon confirmed in other countries.
Aedes aegypti Eradication
With the discovery of the existence of a virus reservoir in wild animals, the eradication of yellow fever was no longer realistic. However, in the course of reorganizing the yellow fever programme, Dr Soper had established a rigidly disciplined and meticulously organized vector control programme in coastal cities throughout north-east Brazil. It soon became apparent that in urban areas, the peri-domestic A. aegypti mosquito could be entirely eliminated through the removal or destruction of breeding sites around human habitations. Reintroduction occurred, however, unless suburban areas were similarly controlled, and this implied that eventually programmes would be required in the interior of the country as well. A programme for the eradication of a mosquito species was an entirely different proposition from one designed only to reduce it to low levels. It required a far more intensive and disciplined effort over a far wider area and for a much longer time than that needed for the Gorgastype yellow fever eradication programme in Havana. However, in view of the already considerable investments of the Brazilian government and of the Rockefeller Foundation and the existence of a highly disciplined organization in the field, Dr Soper in 1934 proposed a new objective-the eradication of A. aegypti, the urban vector of the disease. This was the strategy that he subsequently pursued, although it did not become the declared policy of the Brazilian National Yellow Fever Service until 1942.
With the eradication of yellow fever no longer feasible and that of A. aegypti a more costly and less certain proposition, the Rockefeller Foundation decided to withdraw its support but, because of Dr Soper’s position, this was diplomatically difficult. Dr William Sawyer, of the Foundation, wrote to him on 24 September 1935 stating: “The yellow fever service has grown to such a size that you have practically become a Government official in charge of a large division of the Health Department…it is hardly consistent with our general policies” (Duffy, 1977). The decision to withdraw support was postponed on several occasions at the request of the Brazilian government, but finally, at the end of 1939, support ceased and responsibility for the programme in Brazil was transferred from the Foundation to the government. Dr Soper, however, remained on the staff of the Foundation.
Eradication of Another Mosquito Vector-Anopheles gambiae
Because of the failure to eradicate yellow fever, the concept of eradication might well have been more thoroughly discredited had it not been for the unexpected discovery and the subsequent elimination of a focus of the mosquito Anopheles gambiae, near Natal in north-east Brazil (Duffy, 1977). This African mosquito, an exceptionally efficient vector of malaria, was apparently imported into Brazil in about 1930, soon after the establishment of a rapid mail service between Dakar (Senegal) and Natal (Soper & Wilson, 1943). Epidemic malaria occurred that year within an area of a few square kilometres in which the mosquito was first found. Although the vector was quickly eliminated from Natal, it spread inland, and in 1938 severe epidemics began to occur over large areas of 2 states. In all, 31 000 square kilometres were found to be affected (Fosdick, 1952). Dr Soper proposed that an A. gambiae eradication programme should be started immediately. He rightly portrayedin the most dire terms the implications of a continent-wide spread of the mosquito, but support was not immediately forthcoming from either the Rockefeller Foundation or the Brazilian government. To some, it was seen as little more than an excuse to prolong the life and extend the scope of the vector control services. However, in January 1939, with reluctant financial support from the Foundation as well as substantial government funds, an anti-malaria service was established by presidential decree, its direction being entrusted to the Foundation and to Dr Soper. The problem was a major one, more than 100 000 cases of malaria being detected in 51ay 1939 alone, but the strategy required was entirely different from that used to eliminate Aedes aegypti. Anopheles gambiae bred widely in shallow pools of residual rain-water which were exposed to the sun and without vegetation. It did not usually lay eggs in deep or running water or water which was salty or shaded. During the 4-month rainy season in the area concerned, breeding took place in any small depression in the ground, such as wheel tracks and hoofprints, which could retain water for 8~ 9 days. With the advent of the dry season, however, the tropical sun and low humidity restricted breeding essentially to isolated pools in the beds of large rivers.
The approach which was adopted required a staff of about 4000. The boundaries of the infested area were determined and posts established at which all vehicles and boats leaving the area were fumigated. In the infested areas, vector control staff carried out regular inspections, applying Paris green to all possible breeding sites and spraying houses with pyrethrum (Duffy, 197’7’). They were able to do little more than control breeding during the rainy season, but when the dry season came and breeding sites were few, large areas could rapidly be cleared of the vector. A rigorously disciplined and closely supervised vector control staff, organized with the meticulous attention to detail which had characterized the Aedes aegypti programme, succeeded in these efforts, the last focus of Anopheles gambiae being discovered in November 1940, less than 2 years after the campaign had begun.
Although A. gambiae was a recently introduced rector and less well established in Brazil than in its native African habitat, its eradication from Brazil was nevertheless a dramatic achievement which, at the outset of the programme, had been considered by most to be hopelessly unrealistic. From the experience of this campaign, as well as those against A. aegypti and the Mediterranean fruit fly in Florida (USA), Dr Soper concluded that “selective species eradication”, not only of A.gambiae but of other vectors as well, was in many instances a sound and ultimately less expensive approach than the control of the vector and of the disease (Soper & Wilson, 1943). The belief was reinforced when, in July 1944, he assumed direction of an A. gambiae eradication programme in Egypt, into which the vector had apparently been introduced in about 1942, causing major epidemics of malaria. An estimated 120 000 deaths had already occurred when the Egyptian government requested the help of the Rockefeller Foundation and Dr Soper (Duffy, 1977). Employing the same manual and methods as had been used in Brazil, an effective campaign quickly took shape and, in February 1945, the last focus was eliminated.
Plate 9.3. Fred Lowe Soper (I 893 – 1977) was the most ardent proponent of the policy of disease eradication. While on the staff of the Rockefeller Foundation, he directed the yellow fever eradication programme in Brazil in the 1930s. a programme he transformed into one designed to eradicate the principal mosquito vector (Aedes aegypti). Subsequently, he directed programmes to eradicate infestations of Anopheles gornbiaein Brazil and Egypt. As the Director of the Pan American Sanitary Bureau, I947 – 1959, he was instrumental in persuading the Pan American Sanitary Organization to embark on regional programmes for the eradication of A. aegypti. smallpox, yaws and malaria.
As Dr Soper saw it, success lay in “vigorous and effective action rather than refined measurement of the problem” (Duffy, 1977). He had no malariologists on his staff and saw no need for them. He quoted Dr Ronald Ross (Ross, 1911) on the need for “learning by doing”:
“Amateurs are fond of advising that all practical measures should be postponed pending carrying out detailed researches… In my opinion this is a fundamental mistake…In practical life we observe that the best practical discoveries are obtained during the execution of practical work and that long academical discussions are apt to lead to nothing but academical profit.” (Soper & Wilson, 1943.)
Dr Soper’s advocacy of, and belief in, the principle of eradication was a major factor in later decisions to undertake other eradication programmes. The major constraints, he believed, lay primarily in the lack of vision of health administrators rather than in the lack of appropriate technology. With a meticulously executed field programme directed by dedicated and imaginative staff, the inconceivable became possible.
As early as 1934, Dr Soper had been convinced of the feasibility of eradicating A. aegypti from the Western Hemisphere. His opportunity to pursue the matter came in 1947 when he was elected Director of the Pan American Sanitary Bureau (PASB). He was a forceful and imaginative administrator, who extended and reoriented PASB’s activities, converting it from a body which dealt principally with matters of international quarantine and was staffed entirely by officers seconded from the United States Public Health Service, into the secretariat of a fully fledged international organization, the Pan American Sanitary (later Health) Organization (PASO, later PAHO). One of the first acts of the Directing Council of PASO, in September 1947, was to adopt a resolution:
- “ To entrust to the Pan American Sanitary Bureau the solution of the continental problem of urban yellow fever, based fundamentally on the eradication of Aedes aegypti…
- “To develop the program under the auspices of the Pan American Sanitary Bureau, which . . . shall take the necessary measures to solve such problems as may emerge … whether they be sanitary, economic or legal.” (Pan American Health Organization, 1971a).
As Dr Soper noted, “For the first time the governments of an entire region committed themselves to the continental solution of a common health problem”(Soper, 1965). Ironically, the goal was never achieved. At one time or another A. aegypti eradication was certified in all the countries of the Americas except Colombia, the USA, Venezuela and some of the Caribbean islands. However, reinfestations repeatedly occurred and a USf54 million programme in the USA, which was not begun until 1964, was terminated in 1968, its failure resulting to a large extent from the fact that there were substantially more breeding sites than had been anticipated and that vector control staff could not legally be given the unrestricted right of entry to all premises to look for them (Fontaine et al., 1965).
Programmes for the Eradication of Malaria, Yaws and Other Human Diseases
Dr Soper’s advocacy served to encourage acceptance of the principle of eradication as the defined objective of disease control programmes. Resolutions were adopted uncritically supporting the eradication of other diseases, only limited consideration being given to the technical feasibility, the available resources or the strategy to be used. The XIII Pan American Sanitary Conference (1950) committed PASB to regional programmes for the eradication of yaws, malaria and smallpox. Later, the World Health Assembly committed WHO to global eradication programmes for malaria (1955) and smallpox (1959). Events leading to the decision to undertake the eradication of smallpox are described in a subsequent section, but a brief description of the other initiatives and their outcomes is pertinent.
The malaria programme
Of all the eradication programmes, that for malaria represented by far the largest commitment, in terms both of the number of countries involved and of the resources deployed. It was, moreover, the only global disease eradication programme other than that for smallpox to be approved by the World Health Assembly. Because malaria eradication activities antedated those of the smallpox eradication programme and continued through much of its course, they are of special interest. The successes and failures of its policies provided guidance in formulating smallpox eradication strategy, and its continuing operations competed both for resources and for the attention of national and international authorities until the mid-l 970s.
Malaria was and is one of the most serious of the health problems of tropical and subtropical countries throughout the world. Until the Second World War, the principal control methods available were costly ones—drug therapy for the disease and mosquito control through environmental management and the application of chemicals to destroy larvae and adult mosquitos. Where these measures were diligently applied, especially in areas in which mosquitos did not breed throughout the year, reasonable control could be achieved; such cases as did occur could be treated, usually successfully, with drugs. In few of the non-industrialized countries, however, was it possible to achieve such control measures outside urban centres.
However difficult the control of malaria, the idea that eradication was possible was raised as early as 1916 (Hoffman, 1916) and actually adopted, in part, in a resolution of the II Pan American Scientific Congress in January of that year, which urged “…that all American countries inaugurate a well considered plan of malaria eradication and control” (Jeffery, 1976). Little was achieved, but in the early 1940s the discovery of the insecticide DDT radically changed the situation. DDT, it was found, had a remarkable property in that it retained its toxicity for mosquitos over many months when applied to surfaces (Soper et al.,1947). Most malaria-bearing anophelines, after taking a blood-meal, rested on a nearby surface. If this was a wall coated with DDT, they died before they could transmit the disease.
As increasing quantities of inexpensive DDT became available, it was used in many malaria control programmes in different parts of the world. The effect on malaria morbidity and mortality was dramatic. In Venezuela, for example, in states with an accurate death registration system, mortality rates plummeted from median of 173 per 100000 population in 1941-1945 to 2 per 100 000 in 1949 (Gabaldbn, 1951). Similar results were observed in countries as distant and disparate in character as Ceylon (Sri Lanka) and China (Province of Taiwan). The complete disappearance of malaria from infected areas in Greece and Italy, as well as from the whole of Sardinia, was even more dramatic (Logan, 1953). Of particular interest was the discovery in Greece that even when DDT spraying was temporarily stopped owing to a shortage of the insecticide, the disease did not return (Pampana, 1963). A DDT-based malaria era-cation programme throughout infected areas of the USA (Andrews, 1951) also appeared to have stopped transmission towards the end of the 194Os, although surveillance data collected at a later stage revealed that the campaign had actually begun some time after transmission had effectively been stopped by traditional measures (Langmuir, 1963).
These successes, real or imagined, spurred the imagination of the eradicationists. Thus, in 1948, Dr E. J. Pampana proposed that global malaria eradication should be undertaken (Pampana, 1948). This proposal was translated into policy 2 years later, in 1950, when the XI11 Pan American Sanitary Conference, encouraged by Dr Soper, recommended that PASB should “collaborate with the malarious nations of the Americas in national malaria eradication programmes” (Pan American Health Organization, 1971a). Little note was taken of the fact that malaria transmission had so far been interrupted only in the more developed areas of the world or where the mosquito vector was able to breed for only part of the year.
Plate 9.4. Emilio J. Pampana (I 895 – I973), a distinguished Italian malariologist. in I948 proposed the global eradication of malaria, a commitment adopted by the World Health Assembly in 1955. He was on the WHO staff from I947 to 1958, first as chief of the malaria section, later as the first Director of the Division of Malaria Eradication.
The financial and personnel resources of PASB were limited, and, as Dr Soper was to observe: “The action of the conference on malaria eradication proved to be ahead of its time; the PASB itself was not sufficiently developed to give adequate leadership” (Soper, 1965). During the succeeding 4 years, the successful use of DDT was reported from other countries but further progress in malaria eradication in the Americas was limited. Although United States bilateral assistance for malaria control in the Americas amounted to US$60 million between 1942 and 1957 (International Cooperation Administration, Expert Panel on Malaria, 1962), this was far too little to tackle the problem seriously.
Greater international support was required. The key to obtaining that support was provided by the first scattered reports, in 1951, of mosquito resistance to DDT—the insecticide on which the whole programme of malaria control depended (Pampana, 1963)—thus raising the spectre of widespread vector resistance that would render DDT useless as a means of control. It was argued that, in view of this situation, the only workable strategy was to carry out an intensive global programme to eradicate malaria before the problem of resistance became widespread. When confronted with this scenario, the XIV Pan American Sanitary Conference, in October 1954, declared regional malaria eradication to be an emergency need and authorized a special fund of US$100000 for administrative expenses (Pan American Health Organization, 1971a). Immediately thereafter, UNICEF also agreed to provide support (Soper, 1960).
By no means were all scientists convinced that eradication was a feasible objective, given the tools available (Farid, 1980; Downs, 1981). For Dr Soper, however, the answer, as with his Aedes aegypti and Anopheles gambiae campaigns, lay in an aggressive approach, in meticulous organization, and in tackling the problems as they emerged. As he was to point out later, the eradication programme for A. aegypti had required no new technical or administrative methods—merely the careful supervision and checking of work and the standardization of operating procedures. He believed that there was an “essential identity of the malaria program with that of yellow fever” (Soper, 1960). To subscribe to the objective of malaria eradication required an act of faith. To those who doubted, Dr Soper quoted the pessimistic 1945 Presidential Address of the sceptical Dr Henry Johnson, President of the National Malaria Society in the USA: “I feel this [malaria eradication in the USA] is an untenable concept as we do not yet know in sufficient detail just where and under what conditions the disease occurs” Uohnson, 1946). It became apparent only a few years later that malaria eradication in the USA was imminent, if not already achieved, even as Dr Johnson spoke.
In May 1955, less than a year after the Pan American Sanitary Conference decided on an emergency programme for the eradication of malaria from the Americas, the Eighth World Health Assembly endorsed this as a worldwide policy, and WHO was committed to its first global eradication programme. In the words of resolution WHA8.30, the Health Assembly :
“Considering that the ultimate goal of malaria-control programmes should be the eradication of the disease,
1.1. REQUESTS governments to intensify plans of nation-wide malaria control so that malaria eradication may be achieved and the regular insecticide-spraying campaigns safely terminated before the potential danger of a development of resistance to insecticides in anopheline vector species materializes.” (World Health Organization, 1973a.)
A Malaria Eradication Special Account for voluntary contributions was created and programmes began throughout much of the world, although not in sub-Saharan Africa.
The WHO Expert Committee on Malaria, which met a year later, was extremely cautious, however, when it discussed the feasibility of malaria eradication. In its report, it noted only that eradication “has been accomplished and has shown that it can withstand the test of time in a number of areas in the Mediterranean countries and the Americas” and that “malaria eradication might have still remained an exceptional aim if events had not made it a preferable one to mere control” (WHO Expert Committee on Malaria, 1957). Nothing was said, or could be said, about the prospects for eradication in sub—Saharan Africa in particular. No successful national programmes had been carried out there, most of the countries concerned were at an early stage of development and there was year round breeding of the vectors in many areas. Given these and other problems, there was good reason to believe that eradication could not be achieved (Macdonald, 1957). Little mention was made by WHO thereafter of the fact that “Africa south of the Sahara was at present excluded from the eradication programme, for physical, economic and developmental reasons complicated by high endemicity and prolonged transmission factors” (World Health Organization, 1957). The visionary goal of the global eradication of a disease as serious as malaria was enthusiastically welcomed by politicians and agencies around the world, as well as by those concerned with public health. The programme was foreseen to be a costly one but it was supported by multilateral and bilateral agencies as no previous international health undertaking had ever been. At the same time, participation by countries in a fully fledged eradication effort was encouraged by the policy of providing funds only to countries which agreed to accept the objective and strategies of eradication. By 1958, 63 countries had either started malaria eradication programmes or had converted their control programmes to eradication campaigns; 700 million people, 65% of the population in malarious areas, lived in these countries (Yekutiel, 1981).
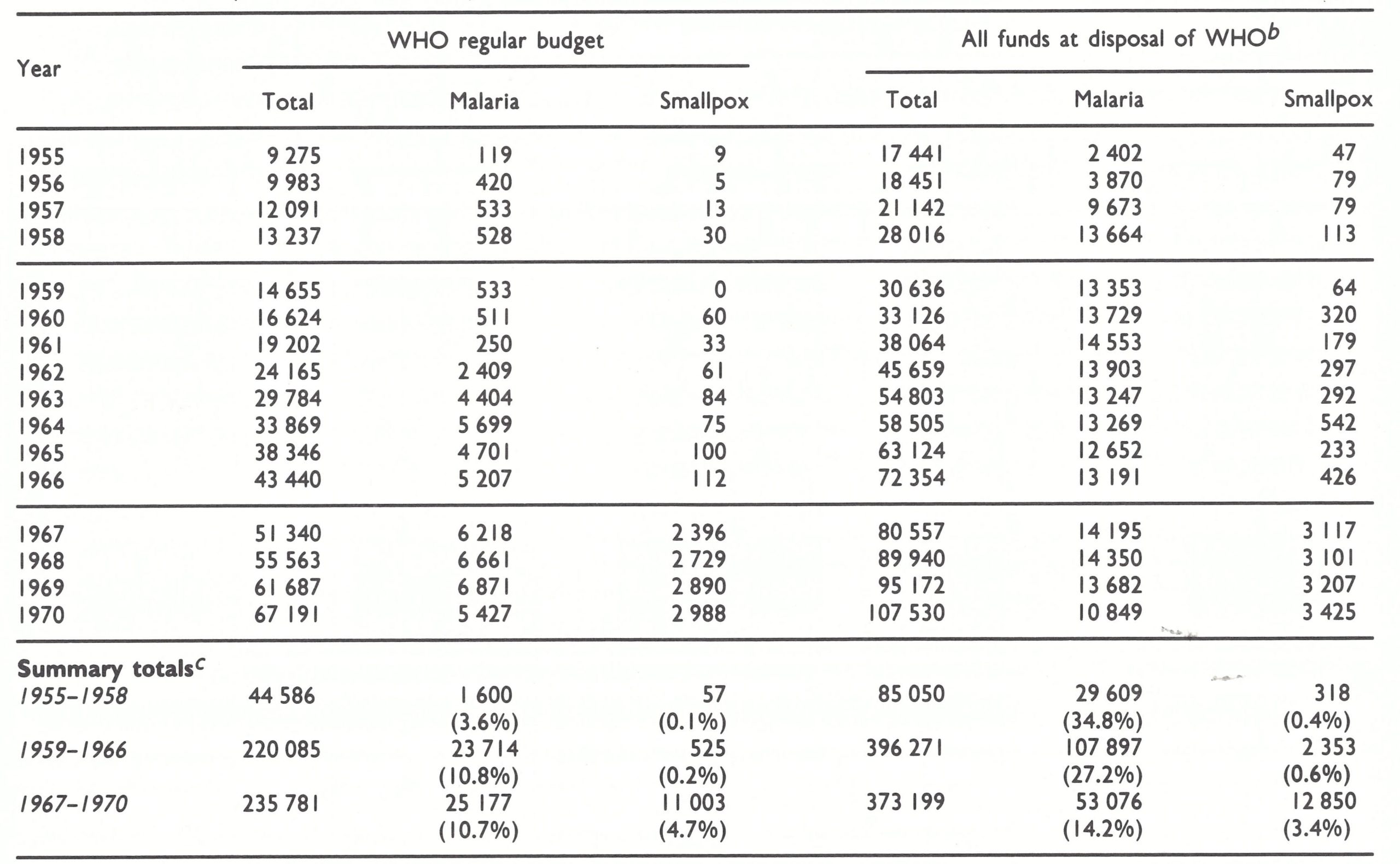
Increased expenditures from the WHO regular budget were substantially augmented by voluntary contributions to the WHO Malaria Eradication Special Account, and supported by other funds administered by WHO, including those provided by UNICEF and the United Nations Expanded Programme of Technical Assistance (later named the United Nations Development Programme) (Table 9.2). The malaria eradication programme quickly became WHO’s most important activity and in 1962, when contributions to the Special Account diminished, funds from WHO’s regular budget, although originally intended for other purposes, were transferred to the Special Account. Expenditures from funds administered by WHO increased from US$2.4 million in 1955 to US$13.7 million in 1958; the number of staff posts likewise increased, from 84 in 1955 to 259 in 1958 and to 577 in 1960. From 1955 to 1958, the malaria eradication programme accounted for 3.6% of WHO’S regular budget and 34.8% of all funds and its disposal (Table 9.3). Between 1959 and 1966, obligations for malaria eradication increased substantially, accounting for 10.8%, of WHO’s regular budget and 27.2% of all funds placed at the Organization’s disposal. In comparison, smallpox control received little support and, after the global eradication programme began in 1959, expenditure remained below 1.0% until 1967. Bilateral contributions to national programmes were also greatly augmented and national government budgets were vastly increased. An estimated US$1400 million were expended from all sources for malaria eradication between 1957 and 1967, and US$1OOO-1200 million over the succeeding 8 years (United States Agency for International Development, 1983).
Table 9.2: Number of WHO staff posts and estimated expenditure for malaria eradication from the WHO regular budget and from funds provided to WHO through the Malaria Eradication Special Account and by other international agencies, 1955-1970a
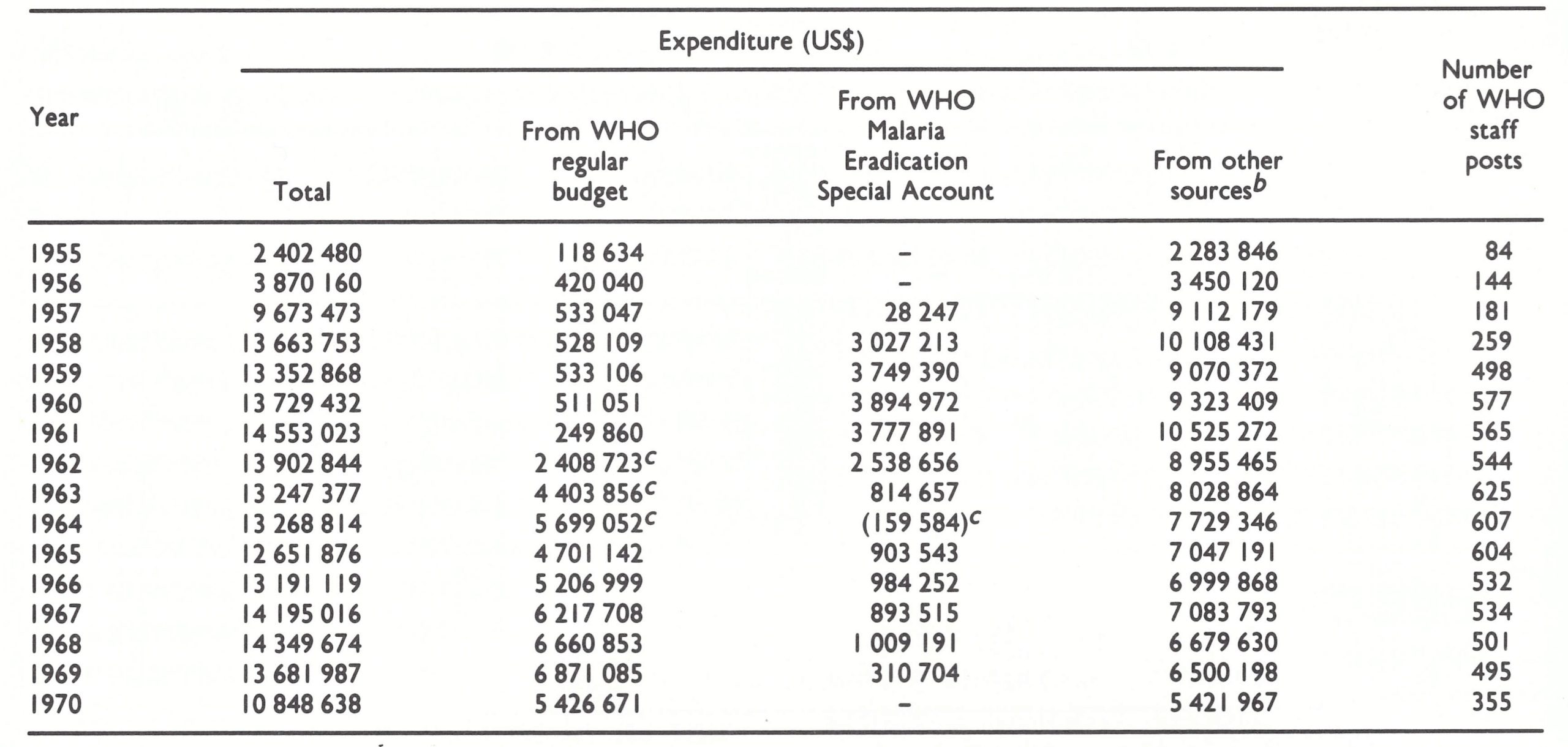 a Estimates derived from WHO financial reports, WHO proposed programme and budget volumes and reports to the Director Council of PAHO.
a Estimates derived from WHO financial reports, WHO proposed programme and budget volumes and reports to the Director Council of PAHO.
b United Nations Expanded Programme of Technical Assistance, UNICEF, PAHO regular budget and PAHO special malaria fund.
c ln 1962, 1963 and 1964, WHO regular budget funds were transferred to the Malaria Eradication Special Account In amounts, respectively, of USS2 million, USS4 million and US$5 363 000 (World Health Organization, 1963a, 1964a, 1965a). These expenditures are shown in the table as regular budget expenditure, which accounts for an apparently negative expenditure figure from the WHO Special Account In 1964.
Table 9.3: Expenditurea of funds placed a t the disposal of WHO from all sources, for all purposes, for malaria eradication, 1955-1970; for smallpox control, 1955-1958; and for smallpox eradication, 1959-1970 (thousands of US$)
 a Source: see Table 9.2.
a Source: see Table 9.2.
b Identified in the Official Records of the World Health Organization as the “integrated international health programme”. This includes disbursements under the regular effective working budget, the technical assistance component of UNDP, the Voluntary Fund for Health Promotion and other funds administered by WHO, including funds in trust, Revolving Sales Fund, Real Estate Fund, etc. It does not include bilateral aid.
c 1955 was the first year of the global malaria eradication programme; 1959 was the first year of the global smallpox eradication programme; 1967 was the first year of the Intensified Smallpox Eradication Programme.
In its organization and relationship to other public health activities, the malaria eradication programme resembled the Aedes aegypti eradication programme in Brazil, as it called for a distinct and separate malaria eradication service which would have no other duties. In most countries, the malaria programmes were by design entirely independent of the health authorities, reporting only to a national council and thence to the head of state. The WHO Expert Committee on Malaria (1 957) saw the malaria eradication staff as serving eventually as a nucleus for other public health programmes, but believed that it should not merge with other activities until success had been achieved. There were some grounds for this view, because the nature of the field work—namely personnel of all other government health programmes combined.
In addition, malaria eradication staff were generally of higher calibre than other comparably trained health workers and their pay scales were almost always higher. It was inevitable, therefore, that the all but autonomous, independent malaria eradication services, with their more highly paid and better supported staff, would be resented by those in the health services-and they were. As a consequence of this programme, there gradually arose a belief, held with almost ideological fervour, that a “vertical” programme—i.e., virtually any organized programme in which staff were responsible for attaining objectives specific to a particular disease—was a heresy. Later efforts to develop smallpox eradication programmes, even though as an integral part of the health service structure, were often met with hostility; the assistance or even passive cooperation of the malaria eradication services was obtained only with the greatest difficulty, or not at all.
The systematic application of DDT to the walls of all houses and buildings was the principal element in the strategy, although this was supplemented in the later phases of each campaign with the treatment of cases with drugs. Traditional methods of mosquito control, such as the drainage and larviciding of breeding sites, were rarely used; nor was the need foreseen for research to identify alternative control measures. It was believed that the tools needed for eradication were available; the problem was the administrative one of applying them properly. Thus, for each country, a highly elaborate plan of operations was developed which included the use of standardized and detailed manuals. National plans varied little from country to country. They called for preparatory, attack, consolidation and maintenance phases—terms which many persons were later to apply to stages of the smallpox eradication programme.
Unacceptable Doubts about Malaria Eradication—Reflections of Dr Wilbur Downs
“In the early 1950s, when malaria eradication became the cause, Dr. Soper came to Mexico to persuade Mexico to get aboard the band wagon. Since I was in Mexico and had been there for 6 years, I was summoned to be with Soper in the office of the Ministry of Health, where multimillion dollar issues were being discussed. My own program budget at the time was less then $50,000 per annum. As I sat in the Minister’s ofice, I heard some amazing things being said, things quite opposite to my own experience, and spoke up saying that there was evidence to indicate very serious problems in the way of eradication in Mexico. Some problems related to the unreconstructed habits of the principal vectors, Anopheles pseudopunctipennis and Anopheles albimanus. Some problems related to the absorption and accelerated decomposition of DDT by the clays found in the mud of adobe walls. Soper strode over to me, put both hands around my neck and shook me vigorously, saying at the same time that it was this kind of talk which was impeding the malaria eradication effort around the world. Not long after that episode, I was advised by my organizational superiors that my malaria study project in Mexico was superfluous and would be terminated.” (Downs, 1981.)
In summary, during the preparatory phase, information was collected on malaria prevalence and vector bionomics, detailed maps were prepared of all structures to be sprayed, houses were numbered, supplies were procured and personnel were recruited and trained. During the attack phase, lasting 3-5 years, insecticide spraying teams sprayed the interior walls of all buildings semi-annually with DDT, working block by block and house by house. Late in this phase, case detection was begun by surveillance agents, who visited each house at monthly intervals to take diagnostic blood samples from anyone who had had fever during the preceding month. Presumptive drug treatment was given and additional spraying conducted when infected foci were detected. When the malaria rate fell below 1 case per 1000 persons, the consolidation phase began, during which routine spraying was halted and intensive surveillance was conducted to detect the few remaining cases, who were then treated, while any residual foci were eliminated by further spraying. The maintenance phase commenced when there had been no evidence of malaria transmission for 3 years. Only in this final phase, expected to be reached within 6-10 years, would the established health services of the country play a role. So detailed and specific were the plans that special manuals were prepared to define explicitly the terminology to be used.
Until 1966, the malaria campaign made steady progress, at least when viewed from a global perspective (Fig. 9.1; Scholtens et al.,1972). Of the total population living in malarious areas in 1959, 26%, lived in maintenance or consolidation-phase areas ; by 1966, this proportion had risen to 59%. Most of the progress, however, was made in countries in which rapid economic development was taking place or in which year-round vector breeding did not occur. In other areas, progress was generally less than anticipated, and the financial resources required to sustain unexpectedly protracted attack and consolidation phases of the campaign were far greater than had been foreseen.
By 1966, government authorities and donors alike had become increasingly concerned about the programme’s progress and apprehensive about its future. The WHO Expert Committee on Malaria, in its thirteenth report, did not dispel these anxieties. In an analysis of 42 programmes, the Expert Committee reported that in 12, satisfactory progress was being made ; in 22, progress was slow and corrective measures had been delayed or were inadequate; and in 8, such measures had been ineffective or had not been taken at all (WHO Expert Committee on Malaria, 1967).
In 1967, the Director-General was requested by the Twentieth World Health Assembly in resolution WHA20.14 to study how best to re-examine the global strategy and to report back. His report in 1969 documented a litany of operational, technical, planning and budgetary problems and concluded that:
“The present methods of eradication . . . are still laborious and often too expensive for the limited resources of developing countries. Unless the present methodology is further simplified, global malaria eradication, though theoretically possible, will continue to be beyond reach for many years to come.” (World Health Organization, 1969b.)
A revised strategy called for malaria control where and when eradication could not be achieved quickly. Global eradication remained the ultimate goal, however, and the responsible division in WHO continued to be called the Division of Malaria Eradication. The principal donors, UNICEF and the United States Agency for International Development (AID), viewed the situation otherwise, and between 1970 and 1973, phased out their support. Dr Perez Yekutiel identifies 1973 as the year that marked the end of the global malaria eradication programme (Yekutiel, 1981). A fundamental weakness in the strategy had been its almost total reliance on the use of residual DDT within the framework of a rigidly defined, meticulously executed programme. However, as Dr Scholtens and his colleagues (1972) pointed out: “There is now wide recognition and acceptance of the limitations of short-term national malaria eradication efforts based on residual insecticides . . . The use of diverse anti-malarial measures has been strongly recommended, but the development of these has been inhibited for a decade because of high expectations from the eradication effort . . . These developments are further complicated by the diminishing number of ‘malariologists’ and proliferation of ‘eradicationists’.”
In brief, research on alternative strategies had been seriously neglected (Farid, 1980). Jeffery (1 976) pointedly observed :
“The science of malaria control, developed slowly and painfully from the beginning of the century to a relatively high state of sophistication, was almost overnight converted to the rather simplistic technology of malaria eradication, which basically 386 SMALLPOX AND ITS ERADICATION required that one know how to deliver 2 grams of something to every square meter of a sometimes elusive interior wall, and to manage a hopefully ever-diminishing Kardex file of cases.”
As many individuals wryly noted, the programme was far more successful in eradicating malariologists than malaria (McGregor, 1984).
As is apparent from this brief account, the proposal by the USSR in 1958 for a global smallpox eradication programme coincided with the initial thrust in the development of the global malaria eradication programme. Substantial resources for that programme continued to be both needed and provided throughout the early 1970s. During this period, interest in, and support for, yet another eradication programme was understandably less than enthusiastic. During the mid-to late 1960s, as the increasing difficulties in executing the malaria programme became evident, confidence in the technical judgement and administrative competence of WHO steadily eroded. Not surprisingly, this was reflected in attitudes towards, and support for, smallpox eradication on the part of potential donor agencies, both international and national, as well as those in the endemic countries. Although some of the people concerned with malaria eradication were later to attribute the demise of that programme to the diversion of attention and resources to smallpox eradication in 1967 (Farid, 1980), it is apparent that the malaria eradication effort was by then already in serious difficulty.
Nevertheless, the malaria eradication programme indirectly made major contributions to the development of the successful Intensified Smallpox Eradication Programme by demonstrating the fallacy of two premises. The first was that, given a highly effective control measure, the problem was simply to apply it correctly. For this reason, and contrary to the practice in malaria eradication, WHO smallpox eradication programme staff actively promoted a gamut of research activities which indeed proved crucial to its success. The second premise was that rigidly standardized procedures, uniformly applied throughout all the countries concerned, could be successful. Thus, in the smallpox eradication programme, principles, rather than a detailed methodology, were stressed, and programme staff were encouraged to adapt their programmes to local conditions, to learn from experience and continually to modify their methods. Not surprisingly, programmes in the different countries varied significantly from one another, and a cadre of experienced smallpox epidemiologists proliferated and matured. The malaria eradication services themselves, with spraymen and surveillance agents regularly visiting every house, might well have contributed significantly to smallpox eradication through their participation in case detection and vaccination. However, as described in later chapters dealing with field operations, in all but a few countries these services refused to undertake any activities except those concerned with malaria. Indeed, in Ethiopia, malaria staff successfully blocked the development of the smallpox eradication programme until 1971.
The yaws programme
Apart from the global programme for malaria eradication and the Aedes aegyptz eradication programme in the Americas, the only other commitment to disease eradication by an international organization before 1959 pertained to yaws. A resolution committing the Pan American Sanitary Bureau to yaws eradication followed successful yaws control field trials in 1948-1949 in Haiti, long a highly endemic area. This stemmed from the discovery that a single injection of longacting penicillin provided a cure for this disease, which primarily affects people living under crowded, poverty-ridden conditions in the rural tropics of Asia, Africa and South America. It is caused by a spirochaete, Treponema pertenue, which is transmitted by direct, non-sexual contact from person to person, and produces chronic, deforming, and incapacitating lesions. In 1948, UNICEF and WHO began to provide support for mass treatment programmes for syphilis and other treponematoses such as yaws (Guthe, 1960), and over the succeeding decade supplies and equipment worth more than US09 million were made available to 61 countries and territories. In the yaws eradication programmes, individual patients were diagnosed by inspection and given penicillin, or, where the disease was widespread, the entire population was treated. The results were immediate and dramatic, but the elimination of the disease from an entire area required repeated visits to ensure that all cases had been cured. If any remained after the campaign had ended, the disease resumed its spread. Occasional latent infections and patients who subsequently relapsed were especially troublesome.
Although a commitment to global eradication was never made by the World Health Assembly, the WHO Expert Committee on Venereal Infections and Treponematoses (1960) recommended that “there should be no delay by health administrations in extending the campaign for the world-wide eradication of yaws and endemic syphilis which is a feasible undertaking from a technical point of view”. Programmes designed to achieve country-wide eradication were launched in the mid-1950s in 49 countries and were remarkably successful in controlling yaws; however, the disease was eliminated in only a few of the smaller countries (Yekutiel, 1981). Evaluations revealed far more low-level persistent infection and transmission than had been originally supposed and by 1966-1967 the term eradication was no longer applied. Even in the Americas, in which regional eradication was the stated objective, the programme was not vigorously supported and Haiti itself never became completely free of yaws.
Programmes for the eradication of other diseases
The possibility of eradicating a number of human diseases was actively debated in many different forums from 1947 onwards. Such discussions, however, effectively ended in 1966, at about the time that the Intensified Smallpox Eradication Programme was established, and simultaneously with an increasing awareness that none of WHO’S regional or global programmes offered much hope of success. In the USA, the term eradication and the concept were examined and discussed with regard to several other diseases. In 1961, the Surgeon General of the United States Public Health Service established a special task force “to evaluate present efforts to control syphilis and to recommend principles and methods that will make it possible to establish a timetable leading to the eradication of syphilis as a public health problem” (Hinman, 1966). The task force, more circumspect, recommended a programme to “eliminate syphilis as a public health hazard in the United States”, but little came of this. The idea of eradicating tuberculosis was more forcefully pursued, first with Dr J. E. Perkins (1959) and then with Dr Soper (1962) arguing that a global programme should be undertaken. Dr Soper took the same view about tuberculosis as he had about other diseases-namely, that the problem was fundamentally one of political commitment and public health administration. The Surgeon General, in 1963, established a task force to examine this problem as well, but its report provided no blueprint for eradication (Hinman, 1966).
During the 1960s, the basic concept of eradication increasingly fell into disrepute. One of the last of the papers to advocate it was that by Dr Soper entitled “Rehabilitation of the eradication concept in prevention of communicable diseases” (Soper, 1965). Most persons accepted the views of the widely read Dr Rene Dubos, who eloquently described for layman and scientist alike the intricate adaptive relationships, evolved over time, between man and microorganisms. One of his books, Man Adapting, published just before the advent of the Intensified Smallpox Eradication Programme, concludes that eradication programmes “will eventually become a curiosity item on library shelves, just as have all social utopias”.
Following the success of the smallpox eradication programme, however, the concept of eradication again came under examination, and although some scientists waxed enthusiastic about the prospects of eradicating other human diseases (Stetten, 1980)—notably, poliomyelitis, measles (Hopkins et al., 1982), yaws (Hopkins, 1976) and dracunculiasis (Hopkins, 1983b)—others, who had themselves been intimately involved with earlier eradication programmes, concluded that there were no suitable candidate diseases for global eradication in the immediate future (Henderson, 1981 ;Yekutiel, 1981). Nevertheless, in view of the unexpectedly rapid progress that had been made in the control of poliomyelitis in the Americas, the Directing Council of the Pan American Health Organization accepted in 1985 a “proposal for action” for the eradication of poliomyelitis from the Americas by 1990. The following year, in 1986, the Twenty-ninth World Health Assembly endorsed efforts to eliminate dracunculiasis “country by country, in association with the International Water Supply and Sanitation Decade” (World Health Organization, 1987). The resolution (WHA39.21) of the Health Assembly refers to “eliminating” the disease, but it is difficult to distinguish this from the notion of eradication (see Chapter 31).
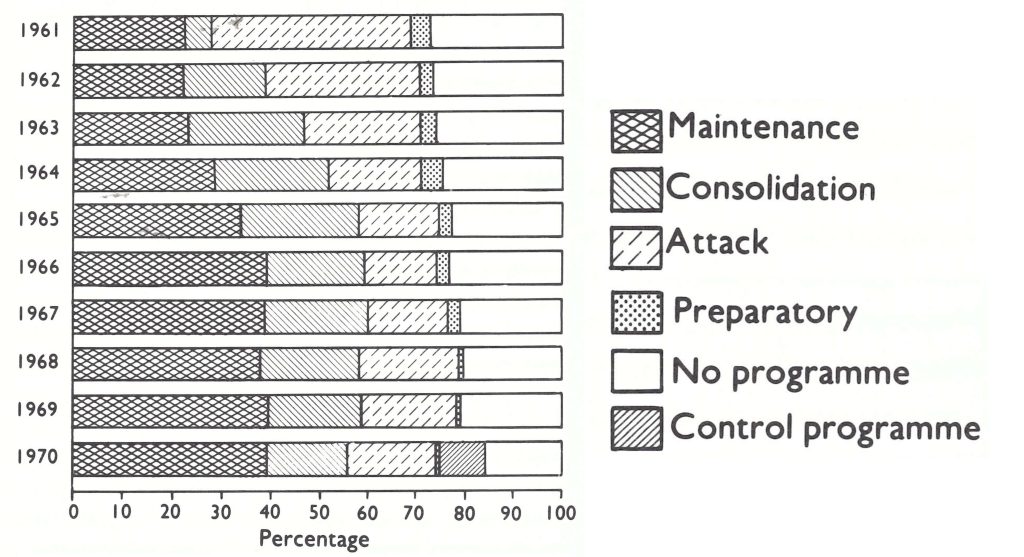
Fig. 9.1. Percentage of population in malarious areas, by phase of campaign, 1961-1970. In 1970. the total population of the malarious areas was 1801 63 1000. (Source: Scholtens et at.. 1972. and WHO data.)
Eradication as Viewed by a Distinguished Scientist
“Eradication in its most exacting sense, namely as applied to the whole world, is not merely an armchair game of epidemiologists; it has become the official policy of several national and international organizations.
“At first sight, the decision to eradicate certain microbial diseases appears to constitute but one more step forward in the development of the control policies initiated by the great sanitarians of the nineteenth century, which have been greatly expanded since the beginning of the microbiological era. In reality, however, eradication involves a new biological philosophy. It implies that it is possible and desirable to get rid of certain disease problems of infection by eliminating completely the etiological agents, once and for all . . .
“In all cases the problems posed by the biological and epidemiological peculiarities of each type of infection are still further complicated by financial, administrative and political uncertainties. Even if genuine eradication of a pathogen or vector on a worldwide scale were theoretically and practically possible, the enormous effort required for reaching the goal would probably make the attempt economically and humanly unwise . . .
The popular appeal and fervid ring of the word eradication is no substitute for a searching analysis of the manner in which limited supplies of resources and technical skills can best be applied for the greatest social good . . .
“Social considerations, in fact, make it probably useless to discuss the theoretical flaws and technical difficulties of eradication programs, because more earthy factors will certainly, bring them soon to a gentle and silent death. Certain unpleasant but universal human traits will put impassable stumbling blocks on the road to eradication. For example, it is easy to write laws for compulsory vaccination against smallpox, but in most parts of the world people would much rather buy the vaccination certificate than take the vaccine; and they shall always find physicians willing to satisfy their request for a small fee . . .
“Public health administrators, like social planners, have to compromise with the limitations of human nature. For this reason, and many others, eradication programs will eventually become a curiosity item on library shelves, just as have all social utopias.” (From Man Adapting, by Dr Rent Dubos, 1965.)
WHO SMALLPOX CONTROL AND ERADICATION ACTIVITIES, 1946-1 958
Introduction
Prior to 1959, when the Twelfth World Health Assembly decided to undertake smallpox eradication, the only cooperative international effort to control smallpox was a WHO regional programme to eradicate it in the Americas. That programme, begun in 1950, was not vigorously promoted and, by 1959, was progressing far more slowly than had been hoped (Pan American Health Organization, 1959).
It may seem curious that smallpox was not identified by WHO as the initial target for eradication, if indeed the objective of disease eradication was to be pursued at all. Smallpox, after all, could easily be prevented by vaccination, and many industrialized countries as well as some developing ones had demonstrated the feasibility of interrupting transmission over large areas encompassing several countries. Because of the frequency of importations, the disease was of concern to all countries and vaccination was extensively practised. Even as late as the 1970s, smallpox vaccine was the only vaccine widely used throughout the world. For tropical areas, a heat-stable freeze-dried preparation was available, although not widely used (see Chapter 7). It was recognized that the disease was spread through close personal contact and that there was no known animal reservoir. Transmission by insect vectors, if it occurred at all, was of no significance.
The control and eventual eradication of smallpox depended in large part on the effective vaccination of large numbers of people. This was a much simpler operation than the more complex and costly vector control measures needed, for example, for the eradication of yellow fever or malaria, and was much easier than trying to treat all cases of a disease—the basic strategy employed in yaws and hookworm eradication programmes.
As has been noted, however, the historical roots of human disease eradication programmes go back to Dr Gorgas’ successful elimination of yellow fever from Cuba and Panama—basically a vector control programme—followed by the Rockefeller Foundation’s yellow fever eradication programme. When this was unsuccessful, the objective of Aedes aegypti eradication was pursued throughout Brazil and subsequently other Latin American countries. During this time, too, recently introduced infestations of Anopheles gambiae in Brazil and Egypt were eliminated. All these activities involved the allocation of large resources to vector control. The question of eradicating smallpox did not arise, perhaps in part because most of those concerned with the eradication concept worked in Brazil and the USA, in which the mild form of the disease, variola minor, prevailed—an illness of marginal public health importance; and perhaps in part because smallpox was then so widespread.
During and immediately after the Second World War, the all but miraculous effect of DDT in destroying insect vectors of disease promised an ultimate solution to the serious problem of malaria. Senior staff of WHO and of the national health services in many countries had been initiated into public health work either in pre-war vector control programmes (principally in the Americas) or in post-war malaria control programmes, and this was where their interest lay. The promise of DDT was still to be explored—a new and exciting venture, incomparably more attractive than endeavouring to apply more widely a vaccine that had been in use for 150 years in the control of a disease that, owing to importations, continued to recur everywhere.
The decision, in 1959, to commit WHO to the global eradication of smallpox represented for the World Health Assembly a marked departure in its attitude towards this disease. Before this time, the Health Assembly resolutions had cautiously urged only improved programmes for smallpox control; for example, in 1954, in resolution WHA7.5, it had requested the Director-General “to provide within budgetary limitations the assistance requested by national administrations to further their smallpox control programmes” (World Health Organization, 1973a). During this period, the Organization’s activities pertaining to smallpox had been concerned primarily with the implementation of the International Sanitary Regulations, the technology required for the preparation of a suitable freeze-dried vaccine, and the development of vaccine standards which might be adopted internationally (see Chapter 7).
Smallpox Eradication in the Region of the Americas
In the Region of the Americas, WHO’S interest in smallpox had been greater than in its five other regions. The countries of that region, on the recommendation of the Regional Director, Dr Soper, had unanimously agreed in 1950, at the XIII Pan American Sanitary Conference, to undertake a regional programme for the eradication of smallpox, a disease which was described in the Director’s report as being widespread throughout the Americas at that time. In Fig. 9.2, which identifies administrative subdivisions in the region that reported 1 case or more during a 3-year period, the problem appears to be far more extensive than it really was. In the USA, for example, cases were almost all of the mild variola minor type; no state reported more than a few cases, and almost none of them was confirmed as smallpox by the state health authorities. Whatever the true extent of the problem, the delegates were sufficiently persuaded to decide on a regional eradication programme, and in 1952 they voted to allocate US$75 000 to the programme; an additional subvention of US$144 000 was made available in 1954.
The ability and inclination of the Region of the Americas to adopt policies dissimilar to those of the Organization as a whole is partly explained by the fact that this region historically had a somewhat different relationship to WHO from that of the other regions, being rather more independent and having additional financial resources. When, in 1946, an International Health Conference had drawn up the WHO Constitution, it had been envisaged that regional organizations then in existence would become an integral part of WHO and, specifically, that the Pan American Sanitary Bureau (PASB) would be integrated as soon as possible. PASB, then only a small organization with few staff, had been in existence, under one name or another, since 1902 (see Chapter 12). Its primary concern, like that of several other regional health bodies, had been to formulate agreements relating to the quarantinable diseases and to oversee their implementation (HowardJones, 1980). However, in January 1947, at the XII Pan American Sanitary Conference, the delegates emphasized the separate identity of PASB by constituting the Pan American Sanitary Organization (PASO; the name was changed in 1958 to the Pan American Health Organization, or PAHO) with PASB as its headquarters and secretariat. Nine months later, at the first meeting of its Directing Council, it authorized its Executive Committee to negotiate with WHO on condition that “the Pan American Sanitary Organization should continue to function as an independent entity for the solution of problems of a continental character” (Pan American Sanitary Organization, 1950a). In April 1949, Dr Brock Chisholm, Director-General of WHO, and Dr Soper, the Director of PASB, signed a formal agreement which recognized PASO as an “independent entity” which could carry out and finance its own programmes in the Western Hemisphere provided that they were “compatible with the policy and programmes” of WHO (Howard—Jones, 1980). PASB was funded thereafter from two sources: funds provided through WHO from the assessed contributions of its Member States and additional funds contributed by Member countries of PASO, the largest contributor being the USA. With proportionately more funds than WHO and with a forceful director committed to the concept of eradication, PASO embarked on a regional smallpox eradication programme in 1950, in addition to the other eradication programmes already described.
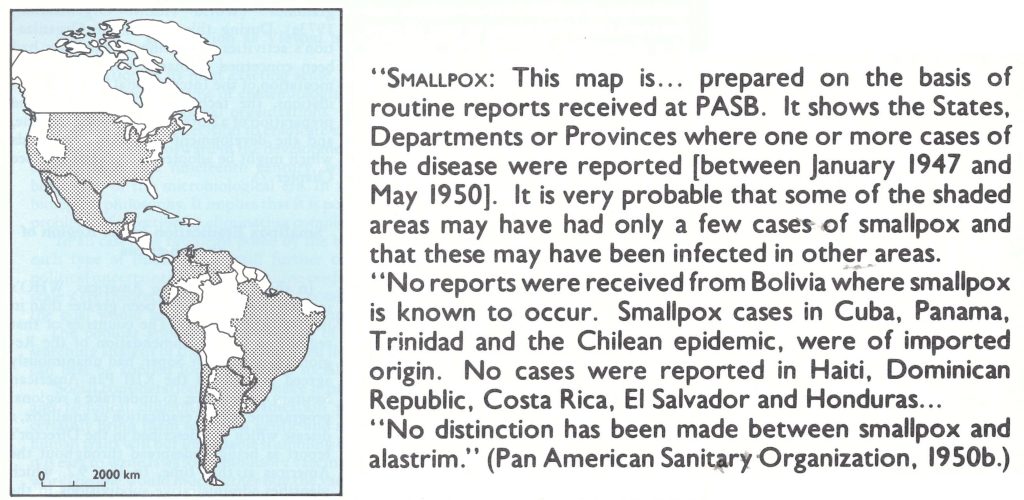
Fig. 9.2. States, departments or provinces of countries in the Americas that reported smallpox cases to the Pan American Sanitary Bureau, January I947 to May 1950.
Until 1947, Dr Soper had personally exhibited little interest in smallpox (Soper, 1965). That year an outbreak of 9 cases occurred in New York City, introduced by a visitor arriving by bus from Mexico (Weinstein, 1947). To control the outbreak, an ill-advised, chaotic, month-long mass vaccination campaign had been launched during which 6.3 million persons were vaccinated, 6 of whom died from complications of vaccination (Greenberg, 1948). Dr Soper, learning that thermostable freeze-dried vaccine was being produced in Europe, recognized that such a vaccine might make it possible to eradicate smallpox in the Americas. Moreover, in the light of the recent turmoil of the New York City outbreak, an eradication programme could be seen to be of significant benefit to PASO’s largest contributor, the USA. The programme would also serve to demonstrate the value of PAS0 as an international health agency of relevance to all Member countries in a way that programmes of little significance to the USA, such as those for the eradication of yaws, yellow fever and malaria, would not. As Dr Soper noted: “The point is too often missed by public health administrators that theirs is a selling as well as an administrative job” (Soper, 1965).
dministrative job” (Soper, 1965). Dr Soper sought help from the United States National Institutes of Health in developing the techniques for preparing freezedried smallpox vaccine and was referred to Mr William Gebhardt at the Michigan State Health Department Laboratory. By 1950, studies on a new freeze-dried vaccine, prepared by Mr Gebhardt, commenced in Peru under the direction of a new PASB staff member, Dr Abraham Horwitz, later to become Dr Soper’s successor. The results were excellent and soon thereafter Mr Gebhardt, supported by PASB, assisted laboratories in other countries of the Americas in preparing the vaccine. Arrangements were made to have it tested at a laboratory in Denmark, although this was seldom done (Pan American Health Organization, 1966). PASB offered technical assistance to some countries but, as noted in the Director’s annual report for 1957 (Pan American Sanitary Organization, 1958): “The Bureau did not have the funds nor the appetite for joining in the intensive vaccination campaigns that have so often given temporary relief, but became interested rather in improving the tools and methods through which permanent eradication might be brought about.” Thus, responsibility for the execution of national programmes and for their cost was left essentially to the respective governments. From available records, it would appear that the programmes in the various countries differed widely in quality; vaccinia1 immunity after mass campaigns was seldom assessed and little was done to improve the reporting of smallpox cases. The Director, in his annual report for 1958 (Pan American Health Organization, 1959), characterized the programme “as advancing at a slower rate than had been anticipated” and noted that “the disease is still an important public health problem in the Americas”. Nevertheless, by the end of 1958, smallpox transmission appeared to have been, or to be on the verge of being, interrupted in all the countries of the Americas except Brazil, Colombia and Ecuador (see Chapter 12).
Up to 1966, the amounts spent annually by PAHO on smallpox eradication never exceeded US075 000 (Table 9.4). The investment was modest in relation to the results obtained.
Table 9.4: Expenditure by PAHO for smallpox eradication, 1953-1966 (US$)
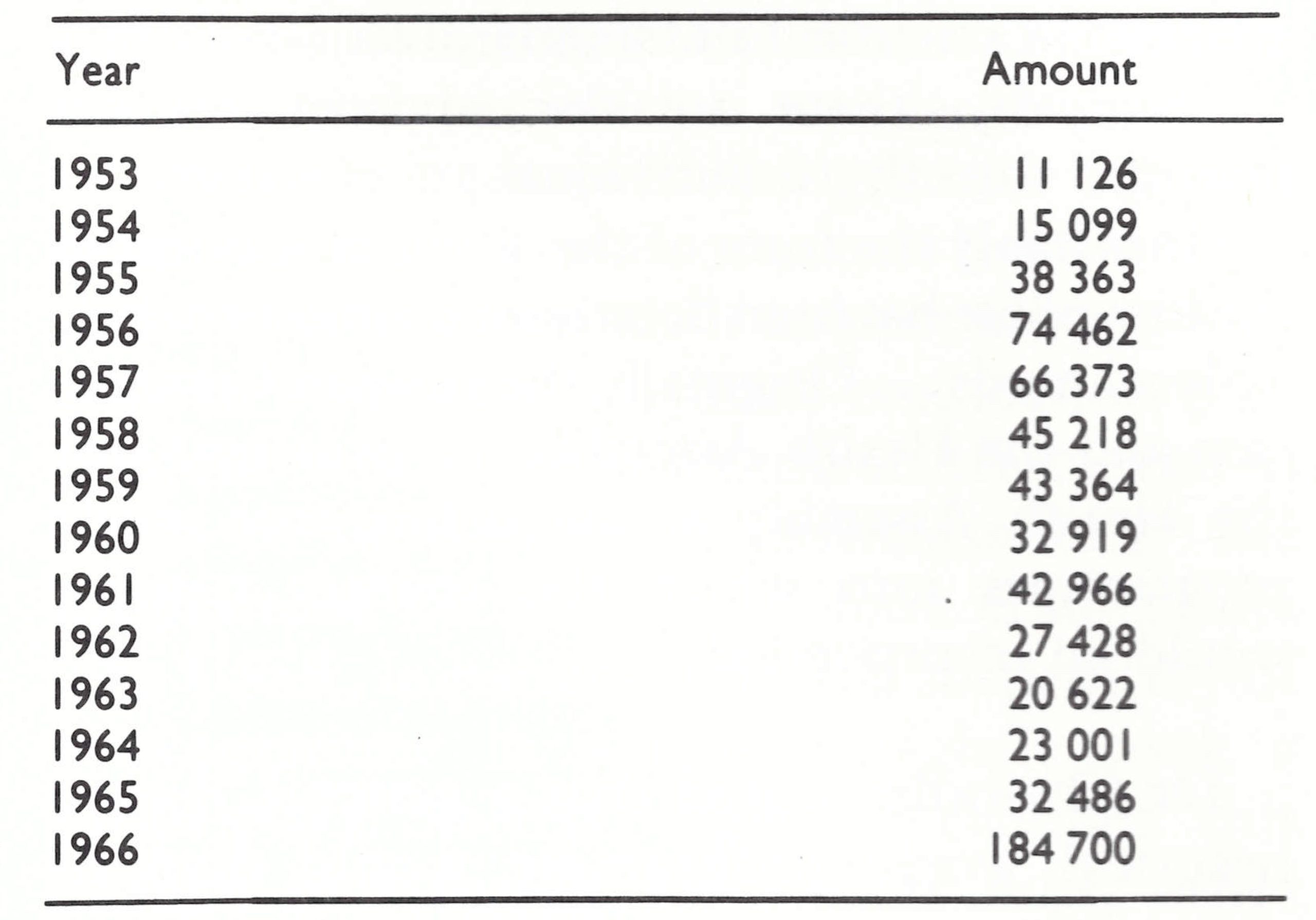 Source: Financial records of PAHO.
Source: Financial records of PAHO.
An Abortive Attempt to Launch a Global Smallpox Eradication Programme, 1953
At the World Health Assembly, the eradication of smallpox was discussed for the first time in 1953. The Constitution of WHO states in Article 2(g) that one of the functions of the Organization is “to stimulate and advance work to eradicate epidemic, endemic and other diseases”. Citing this article, Dr Chisholm, then serving his last year as WHO’S first Director-General, presented a special report entitled “Further action on general world health problems” (document EB11/63 ; unpublished) to the eleventh session of the Executive Board in February 1953 and then to the Sixth World Health Assembly in May. The report states:
“The first four years of work by WHO have shown its programmes developing in practice into two almost distinctive groups. Firstly there are the essential programmes of general international character, many of them traditional…[such as]… quarantine, statistical and standardization of drugs…Secondly, there are the advisory services provided directly to individual governments…“Inevitably the form of the advisory services in the first phase has been determined almost entirely by local needs…Originally the Interim Commission and the Health Assembly…visualized that the Health Assembly would define true world programmes into which the country requests would be incorporated.”
Dr Chisholm noted that a general, direct, practical world programme would demonstrate “the importance WHO has for every Member State” and also its role “not only through the necessary and valuable present form of direct assistance to governments, but also by concerted international action”. He took note of the smallpox eradication programme in the Americas and advanced the argument that an appropriate subject of general concern should be selected for a world-wide campaign—specifically, smallpox eradication. A 5-year budget providing approximately US$131 000 per year was proposed.
The proposal was not enthusiastically received. Delegates from Australia, Belgium, El Salvador, India, Pakistan, South Africa, the United Kingdom, the USA and Venezuela all expressed views to the effect that the problem of smallpox was really a regional or even local one, and that insufficient, knowledge was available. Summarizing, the delegate of the United Kingdom pointed out that the problem was vast and complicated and it did not appear that a world-wide machinery for such a campaign was suitable at this time. He pointed out that, “Such a campaign might prove uneconomical and would not… add to the prestige of the Organization” (World Health Organization, 1953). He put forward a resolution which read, in part:
“In view of the many political, economic and social factors that must be considered,
REQUESTS the Executive Board to further study [the matter] and to report to the Seventh World Health Assembly.”
The delegate of France offered an alternative resolution which stated, inter alia:
“Approves in principle the suggestion of the Director-General that WHO should encourage certain world-wide programmes.”
This was rejected, and a somewhat amended version of the United Kingdom draft was adopted as resolution WHA6.18 (World Health Organization, 1973a).
Each of the regional committees was asked to discuss the proposal but, except in the Americas, none expressed enthusiasm and, at the Seventh World Health Assembly in 1954, the proposal was deferred pending further study. Later that year, the newly elected Director-General, Dr Marcolino Candau, sent a letter to all Member States offering advice and assistance, if required, in the execution of smallpox control programmes and requested replies. In his report (document A8/P&B/7; unpublished) to the Eighth World Health Assembly in 1955 Dr Candau said that the replies received indicated that most countries “do not desire any immediate practical assistance in the control of smallpox. A small number would welcome technical advice and assistance, mainly in connection with the production of reliable [freeze-] dried vaccine. Only two requests were made for consultant services”. The concept of a global programme for smallpox eradication was thereupon quietly buried. In that same year, however, the proposal to adopt a policy of global malaria eradication was advanced and delegates urged that it should be undertaken as a matter of the highest priority. The programme, which was vastly more costly and complex than smallpox eradication and whose feasibility was far more questionable, was adopted virtually without dissent.
Not until the USSR returned to active participation in WHO and Professor Zhdanov presented its proposal was the subject of smallpox eradication again raised. Although the decision in 1959 to embark on a global eradication campaign might appear to have been a logical extension of the regional eradication programme in the Americas, it was not. Professor Zhdanov himself was unaware of the regional initiative and it was not mentioned in debate either at the Executive Board sessions or at the World Health Assemblies of 1958 and 1959, nor was it noted in the Director-General’s reports. It was a regional programme which, by 1958, had been largely forgotten, even by delegates of the countries of the Americas.
THE SMALLPOX ERADICATION PROGRAMME, 1959-1966
Introduction
Seven years had elapsed between the decision of the Twelfth World Health Assembly (1 959) to undertake global smallpox eradication and that of the Nineteenth World Health Assembly (1966) to allocate significant funds from the regular budget of the Organization to enable an intensified campaign to be conducted. Progress during this period was far slower than had been anticipated in the Health Assembly resolution WHA11.54. During the period 1959-1966, malaria eradication was WHO’S largest programme and its principal preoccupation, and this was no less true even for many Member States in which smallpox was endemic, because malaria was also present in most of them. WHO allocated some funds for smallpox eradication, intercountry meetings were held to discuss programme execution and methods of vaccine production, and letters were sent periodically by the Director-General appealing to Member countries for voluntary donations of vaccine. Few such donations were received. The USSR, under bilateral agreements, provided large quantities of vaccine to India, as well as to a number of other countries, and the USA provided bilateral support to several smallpox eradication programmes, including those of Bolivia, India and Iran, but on the whole enthusiasm for smallpox eradication was lacking. Greater interest in the programme began to be shown when a series of events led the USA, in 1965, to commit itself to providing assistance to a regional smallpox eradication programme in western and central Africa, and to begin to support more enthusiastically the programme for global smallpox eradication. The USSR, impatient with the inadequacy of a programme in which it rightly took a proprietary interest, eagerly welcomed this change in attitude. In concert with other delegations, it requested the Director General, in 1965, to prepare a proposed programme and budget for an intensified campaign. In 1966, this was approved together with a designated financial commitment of US$2.4 million from the regular budget. Preparations thereupon started for an Intensified Smallpox Eradication Programme to begin in January 1967.
Status of Smallpox, 1959
In 1959,63 countries or territories officially reported to WHO a total of 77 555 cases of smallpox. When national records were reviewed and revised by WHO in the late 196os, the total for 1959 was increased to 96 571 cases but, whatever the figures, reporting was recognized to be incomplete, though the degree of underreporting was not known. Some countries provided no reports despite the stipulations of the International Sanitary Regulations ; in other countries, including large ones with comparatively well developed health systems, the only cases reported were those hospitalized in the larger cities.
No attempt was made in 1959 to distinguish between countries in which smallpox was endemic and those in which the only cases were imported ones; in preparing this chapter, however, we have tried to determine the probable situation in 1959, based on information now available (Fig. 9.3 and Tables 9.5 and 9.6). To facilitate comparison with the situation in the period 1967-1977, the designations of countries and territories as they existed in 1977 are used. From the records, it is probable that smallpox was endemic in 1959 in 59 countries and territories in Africa, South America and Asia, which then had a total population of 1 734 921 000. Together, these countries constituted a substantial proportion of the land area of the 3 continents concerned and included 59% of the world’s population. It is important to note, however, that in 1959 endemic transmission was on the verge of interruption in a number of Asian countries (Cambodia (Democratic Kampuchea), China, Iraq, Malaysia, Saudi Arabia, Thailand and Viet Nam) and in Africa (Algeria and Angola). Transmission appears to have been interrupted in all these countries over the period 1959-1 962.
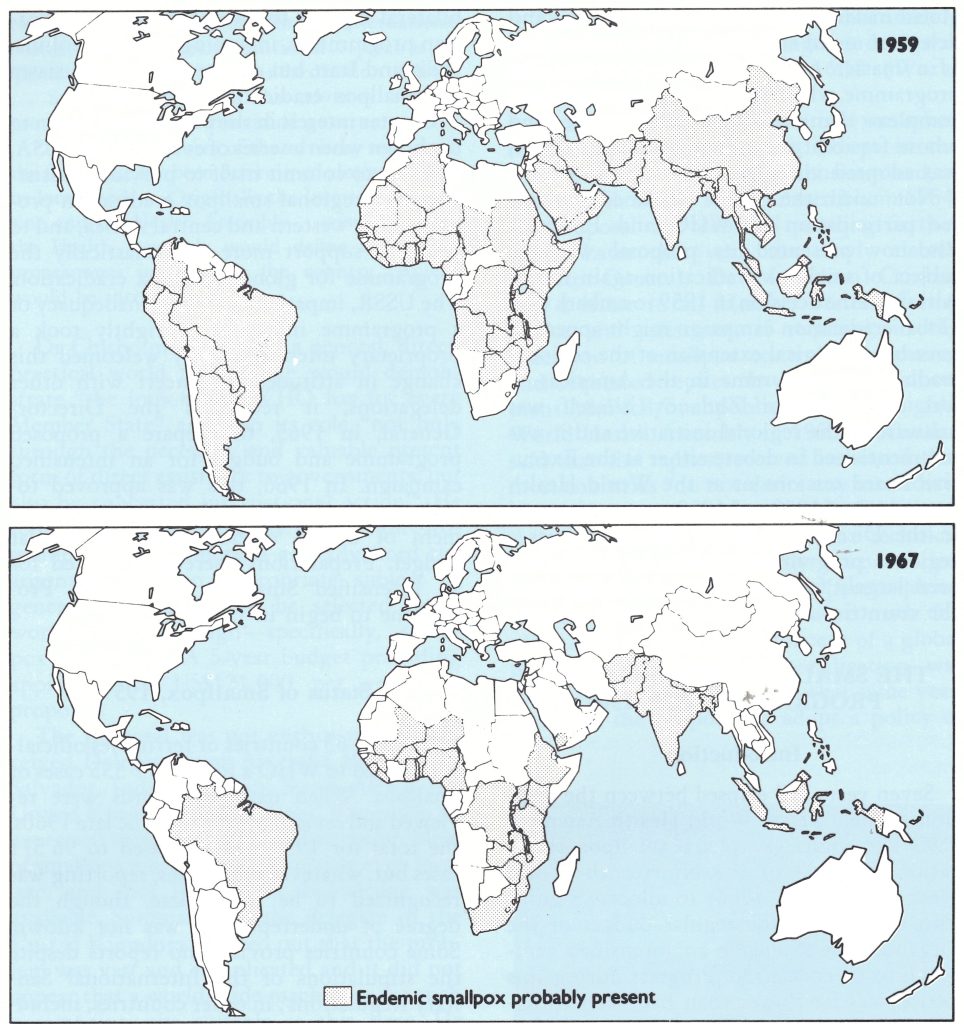
Fig. 9.3. Countries and territories in which smallpox was believed to be endemic, 1959 and 1967.
Table 9.5: Countries and territories believed to have endemic smallpox, 1959 and 1967: summary by continent
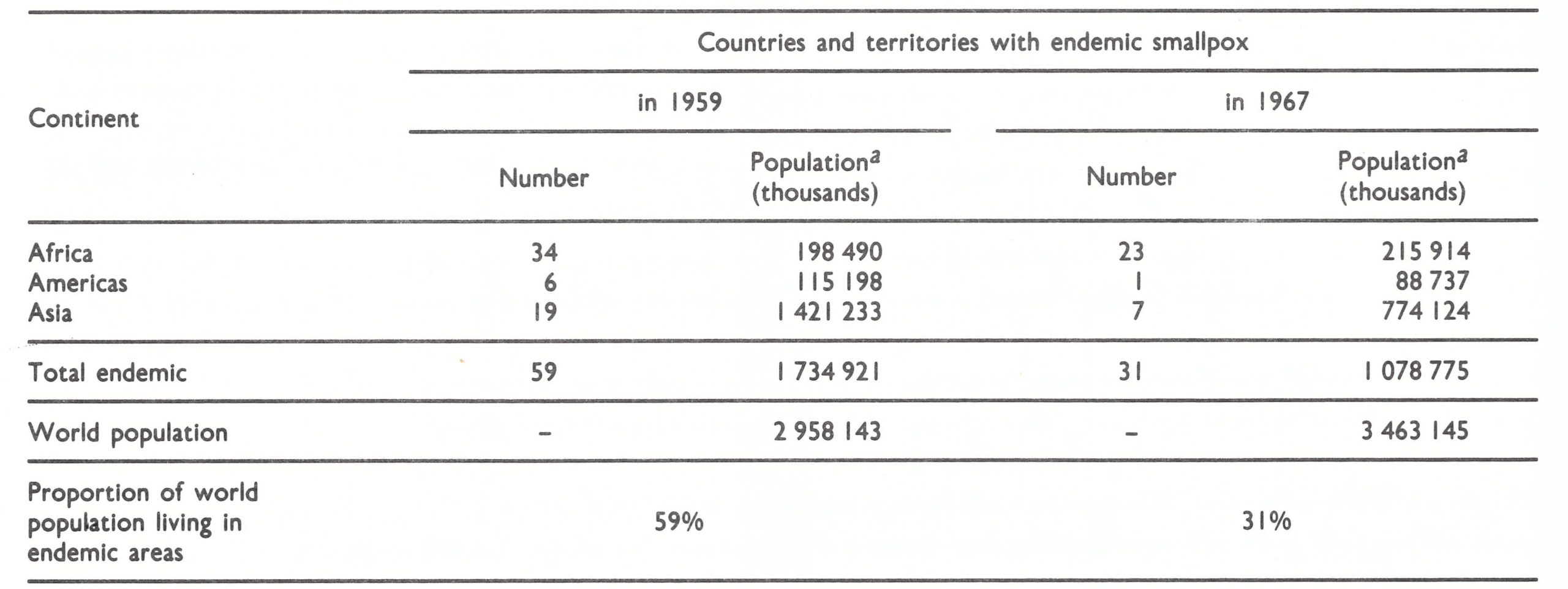 aPopulatlon data from United Natlons (1985).
aPopulatlon data from United Natlons (1985).
Table 9.6: Countries and territories in Africa, the Americas and Asia a believed to have endemic smallpox, 1959 and 1967
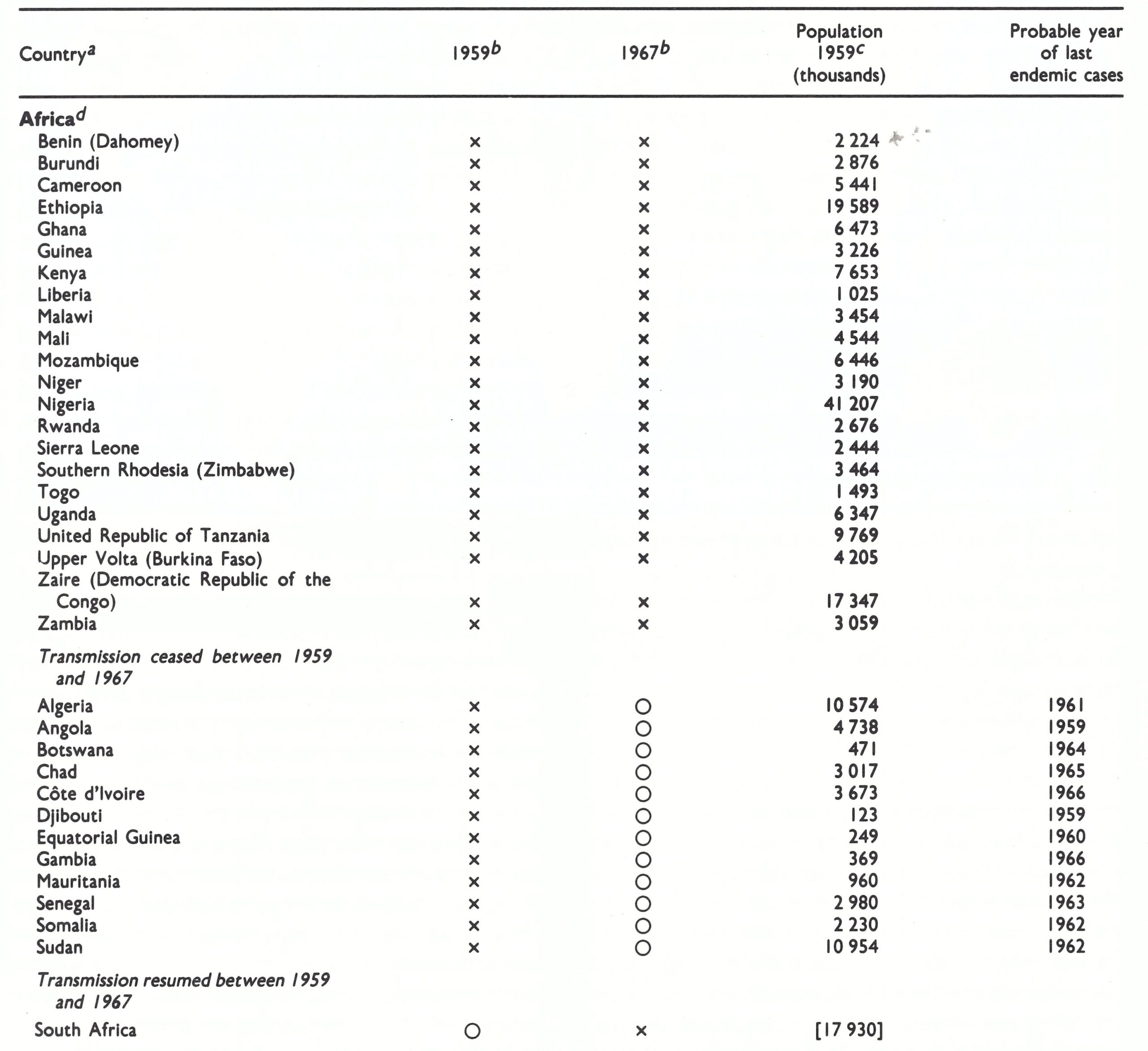
Table 9.6: (cont.)
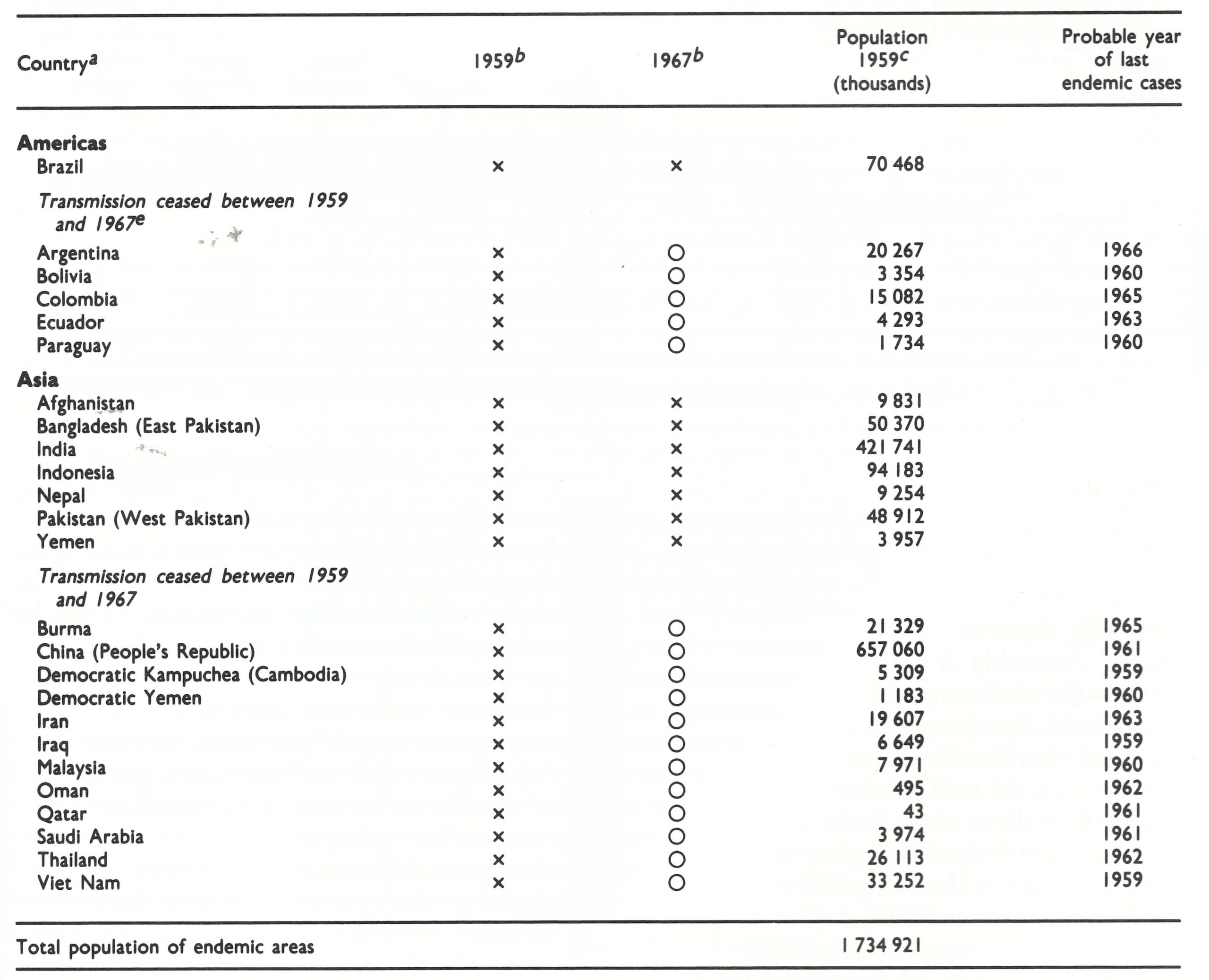 a Designation of countries and territories as in 1977.
a Designation of countries and territories as in 1977.
b x = endemic smallpox present; 0 = probably not endemic for smallpox.
c Population data from United Nations (1985).
d Excluding Lesotho, endemic in 1961-1962, and Swaziland, endemic in 1963-1966.
e ln Peru, endemic transmission ceased in 1954 but resumed In the years 1963-1966.
The Global Eradication Programme Begins, 1959
The Director-General’s proposed programme, as presented to the Twelfth World Health Assembly in 1959, envisaged national campaigns in which at least 80% of the population of each country would be vaccinated or revaccinated. Responsibility would rest primarily with individual governments, which would be expected to bear the major burden of programme administration and execution as well as of cost (World Health Organization, 1959b). WHO would be responsible primarily for providing technical assistance when requested and fellowships for the training of staff, as well as for assisting in the development of vaccine production. Little was said about a leadership role for WHO in overall planning or in coordinating the campaign. Since delegates to the 1954 Health Assembly and most regional committees had so forcefully argued the case that smallpox was a local or regional matter, this approach was understandable. Moreover, malaria eradication then commanded whatever discretionary resources were available.
Budgetary Provision for the Programme
The annual expenditure of funds for smallpox eradication between 1959 and 1966 by WHO, PAHO and the United Nations Expanded Programme of Technical Assistance is shown in Table 9.7. Between 1960 and 1965, the annual expenditure by WHO and PAHO ranged from US976 118 to US$188 351, increasing in 1966 to US$374 544, primarily because of a large disbursement of funds by PAHO for supplies for Brazil. Donations of vaccine averaged US$120 000 per year from 1960 to 1966, and UNICEF provided almost US$250000 during this period for vaccine production equipment. Overall, however, the expenditure for smallpox eradication amounted to only 0.6% of the total expenditure of funds placed at the disposal of WHO between 1960 and 1966 and to 0.2% of the regular budget in the same period (see Table 9.3).
Every year the Director-General reported to the Health Assembly that progress in the smallpox eradication programme was slow, the principal obstacle being identified as the lack of funds for vehicles, supplies and equipment. The Health Assembly regularly urged that a larger budget should be provided for smallpox eradication and, when this was not done, finally requested the Director-General, in resolution WHA17.43 in 1964, to provide “under the future regular programme and budget of the Organization—if necessary at the expense of lower-priority activities—for making good the shortfall of the vaccine required, and of other essential supplies and equipment.. .” (World Health Organization,1973a). Apparently, there were few activities of lower priority because the DirectorGeneral’s proposed budget for 1966 provided for less than US$200 000.
Table 9.7: Expenditure for smallpox eradication by WHO and PAHO, 1959-1966 (US$)a
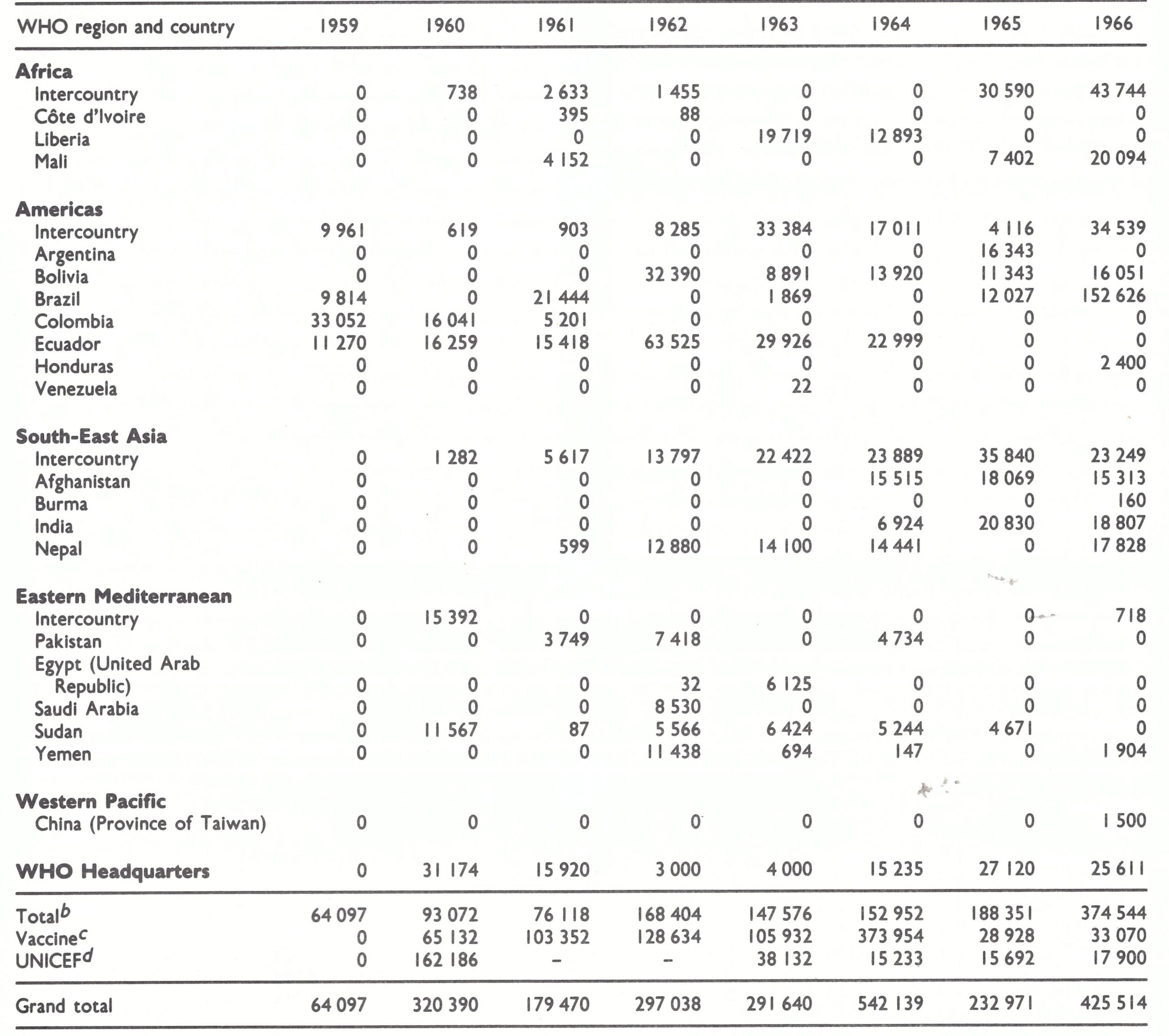 a Source: see Table 9.2.
a Source: see Table 9.2.
b Total includes funds from the regular budgets of WHO and PAHO, the Special Account for Smallpox Eradication (except vaccine) and support provided by the United Nations Expanded Programme of Technical Assistance.
c Value of vaccine contributed through the Special Account for Smallpox Eradication.
d Costs of vaccine production equipment provided to Burma, Guinea, India, Indonesia, Kenya and Pakistan (East).
Programme Activities, 1959-1962
Responsibility for coordinating the programme was assigned to a newly recruited medical officer, with a secretary, who were for several years WHO’S only full-time employees working on smallpox eradication. The medical officer worked as one of several in the Virus Diseases unit of the Division of Communicable Diseases. For comparison, there were 5 professional staff at Headquarters in the Leprosy unit and 28 in the Division of Malaria Eradication. There were no staff members in any of the WHO regional offices solely responsible for smallpox eradication and, until 1966, only 5 full-time WHO Programme Activities, 1959-1962 Responsibility for coordinating the programme was assigned to a newly recruited medical officer, with a secretary, who were for several years WHO’S only full-time employees working on smallpox eradication. The medical officer worked as one of several in the Virus Diseases unit of the Division of Communicable Diseases. For comparison, there were 5 professional staff at Headquarters in the Leprosy unit and 28 in the Division of Malaria Eradication. There were no staff members in any of the WHO regional offices solely responsible for smallpox eradication and, until 1966, only 5 full-time WHO smallpox eradication advisers were assigned to field programmes—in Liberia, from 1962; Bolivia, from 1963; Afghanistan, from 1964; and Kenya and Mali, from 1965. A WHO adviser served in a part-time capacity in Nepal from 1962. The total population of these countries was less than 40 million. None of the programmes made significant progress, although Bolivia, in which there were no cases of smallpox when the adviser was assigned, remained free of the disease.
Soon after the programme began, interregional conferences were held in Africa (1959) and in Asia (1960) to discuss methods of conducting smallpox eradication programmes, and training courses in the techniques of producing freeze-dried vaccine were held in Nigeria (1960) and Thailand (1961). The medical officer from WHO Headquarters visited a number of countries, on request, to discuss the possible implementation of programmes, but it was apparent that few countries were in a position to do much unless additional resources could be made available.
From 1959 onwards, the Director-General, at the request of the World Health Assembly, presented each year a formal report on the programme for discussion by the delegates. Beginning in 1961, the tenor of the discussions and the resolutions reflected increasing impatience. At the Fourteenth World Health Assembly (February 1961), the comments of a delegate of the USSR, Dr V. N. Butrov, were reported as follows :
“It seemed…that WHO and its regional offices were not giving the problem all the attention that it deserved…[In] the Annual Report for 1960, for example, the chapter on the Eastern Mediterranean Region was the only one where the matter was dealt with at all seriously. The chapter on SouthEast Asia…and the chapters on Africa and the Americas did not contain any reference to smallpox.” (World Health Organization, 1961.)
A delegate of Peru, Dr Carlos Quirbs, was no less concerned; he noted that “the proposed programme and budget estimates failed to show any specific allocation for that work [smallpox eradication]”. At that time, the budget document, as presented to the delegates, identified project budgets in each country and region, but the amount to be spent by WHO Headquarters on smallpox eradication was not specified as such nor was a table provided to summarize expenditures by categorical programmes. Dr Quir6s introduced a resolution calling for a specific budget allocation, arguing that “WHO should not merely give assistance to governments for smallpox eradication but should give it as part of a well-defined global eradication programme like the programme that existed in the case of malaria”. The Director-General discouraged such a move, explaining that he did not see what purpose it would serve. The resolution ultimately passed (WHA14.40) stated only that “…it is urgent to speed up the activities of the programme…” but, for the first time, the Health Assembly specifically called for “voluntary contributions in cash or in kind” from Member States, an appeal which was thereafter renewed annually.
During the first few months of 1962, 13 imported outbreaks occurred in Europe, a fact pointedly reported to the Fifteenth World Health Assembly by the Director-General. Despite the obvious problem which smallpox constituted for non-endemic countries, he observed that the Organization had received to date only 34 million doses of vaccine, of which 25 million were from the USSR. His report acknowledged that progress was poor, and he estimated that only US$610 million in external assistance should suffice to achieve eradication. A delegate of the USSR, Dr S. S. Marennikova, renewed the appeal for smallpox eradication to be given a special allocation in the budget and expressed regret that the Organization had “not availed itself of all the offers made by the Soviet Union to provide specialists—in vaccination, research, etc.” In reply, Dr P. M. Kaul, an Assistant Director-General, observed that there was not so much a lack of expert knowledge“…the real difficulty was in providing sufficient vaccinators and in the organization of campaigns, an administrative point in which there was not a marked need for experts” (World Health Organization, 1962). In fact, WHO then had little notion of what was really needed, a point stressed by several delegates and reflected in the resolution adopted (WHA15.53), which called on the Director-General to compile for all countries their “requirements and firm estimates of costs for their smallpox eradication programmes”.
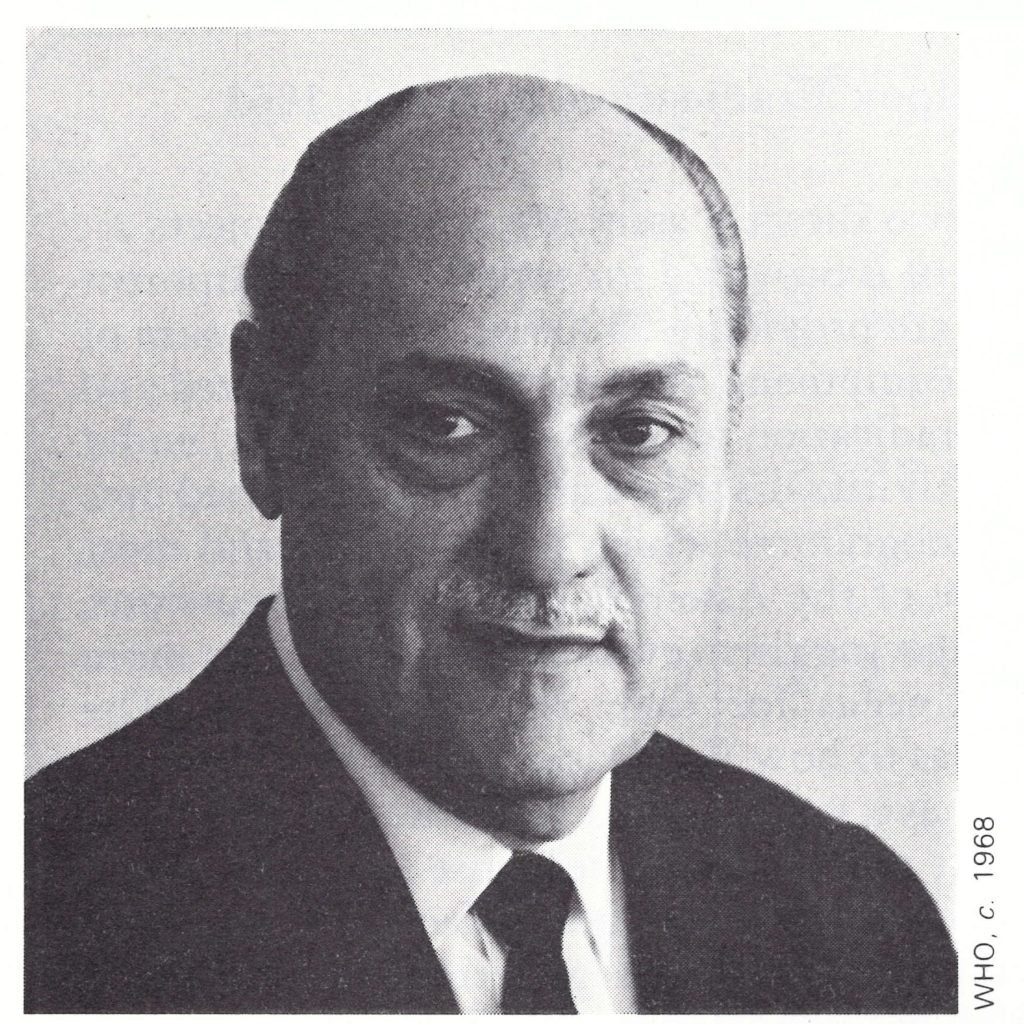
Plate 9.6. Marcolino G. Candau (1911-1983), the second Director-General of WHO, 1953-1973. was largely preoccupied with the difficult and costly task of the global eradication of malaria throughout his tenure. The programme, started in 1955, began to experience serious problems in the mid-1960s and was transformed into a control programme in the early 1970s. The global smallpox eradication programme began and was intensified during his period of office.
Proposed Provision of Support through the WHO Regular Budget, 1963
By the time the Sixteenth World Health Assembly was convened, in May 1963, 4 years had elapsed since WHO had committed itself to global smallpox eradication, but there was still little progress to report and little substantive information available that would permit a better estimate to be made of total needs. With prodding from Professor Zhdanor at the preceding Executive Board session, WHO made its first attempt to define which countries were endemic and which were not. The Director-General’s report (World Health Organization, 1963b) concluded that there were then thought to be 44 endemic countries, of which 14 were conducting eradication programmes, 22 had programmes on paper but were not yet implementing them, and 8 had so far done nothing at all. As Professor Zhdanov pointed out, “WHO was far from having done everything possible” and urgently requested that priority should be given to the programme. “It was, perhaps, the only programme that could really be completed, and in the foreseeable future” (World Health Organization, 1963c). A summary table showing the proposed allocations for smallpox eradication was presented for the first time, but, as a delegate of the USA, Dr C. L. Williams, observed, this amounted to a mere US$227 100 for the whole of 1964. Reasoning that if only US$10 million were required in external assistance, and this over a 5-year period, he expressed the belief that funding should be provided from the regular budget so as not to have to wait for voluntary contributions. This position was supported by a number of other delegates. Dr Kaul, responding on behalf of the Director-General, argued that “the Organization was giving as much encouragement as possible; the reasons for slow progress were mainly to be found at the national level where administrative difficulties and grave material shortages had to be overcome”. He added that “further [voluntary] contributions had been received recently and it was hoped that it would be possible to meet all the requirements for vaccine from that source” (World Health Organization, 1963c).
Support for a special budget, financed through assessments of Member States, was growing, but the Director-General resisted the idea. The malaria eradication programme was already recognized to be in trouble, thus endangering WHO’S credibility. The provision of a special budget for smallpox eradication implied that WHO was taking primary responsibility for promoting and coordinating yet a second eradication effort. In his view, the prospects for its success were not good. It was then believed, as stated in reports prepared by WHO staff, that eradication could be achieved only if at least 80% of the population were vaccinated. From Dr Candau’s own experience in working in Brazil, he knew this to be impossible in the vast Amazon region, and there were unquestionably other areas in other parts of the world in which similar difficulties would arise.
Dr Kaul’s optimistic statement to the Health Assembly in 1963 regarding contributions was surprising, since, in fact, few voluntary contributions were then being received. India, at the time of the Sixteenth World Health Assembly, was desperately short of vaccine. The country had embarked on an ambitious national mass vaccination programme, with substantial support in national currency from the USA and a bilateral gift of approximately 100 million doses of vaccine per annum from the USSR. Nevertheless, the quantity of vaccine available was far from sufficient. Indeed, shortly after the Health Assembly concluded, the Director General made emergency appeals for vaccine for India to help to meet a projected deficit of 50-100 million doses a year. Few countries, however, had the laboratory capacity to make more than token contributions even if they were so inclined.
Problems of WHO Support for Smallpox Eradication in India, 1963
“At present in this Region, there are only two directly assisted smallpox projects... Except for a nominal amount of $1 00, no amount is provided for supplies and equipment for the Nepal project... [For Afghanistan] we are providing $5000 in 1963 and a sum of $12 000 for...1964 and 1965 for supplies and equipment. We are certainly prepared and anxious to give further assistance in smallpox eradication in our Region. However, under the existing budget provisions only marginal activities described above can be carried out.
“This brings me to the case of the Indian programme which is the largest and most important in the whole world ...In pursuance of the Assembly and Board discussions, SEARO has been promising the government in giving them every help in procuring more supplies of dry vaccine to meet their total needs for their mass programme. The government now wants to know very cogently as to how WHO is going to help them...
“In your memorandum of 13 March you have explained to me how the Director- General’s circular letter of 31 July has brought practically no response for free gifts of vaccine, vehicles and other equipment. For WHO this is a very unsatisfactory position.... One thing is certain and that is this— having once pushed a government into a vast programme of this size and a programme which has importance globally much more than nationally, any failure of this magnificent national effort would fall substantially at the door of the WHO, if not legally, at least morally.”
(Extracts from a letter from the Director of the WHO Regional Office for South-East Asia to Dr P. M. Kaul, WHO Assistant Director-General, dated 4 April 1963.)
Voluntary Contributions
Although letters asking for contributions to the programme were sent each year by the Director-General to all countries and to UNICEF, few responded (Table 9.8). UNICEF had provided substantial support for malaria eradication and was not prepared to support another eradication programme. Mr Maurice Pate, the Executive Director, in a letter of 11 July 1962 to Dr Candau stated: “AS a general policy, UNICEF has not been prepared to give assistance to a separate mass campaign for smallpox vaccination but we are quite willing to contribute to countries who wish to incorporate smallpox vaccination as a function of their public health services.” As a consequence, UNICEF’s contributions to the programme remained small and were intended primarily for the purchase of equipment for the production of vaccine.
Up to the end of 1963, only US$7880 in cash had been contributed to the Special Account for Smallpox Eradication and 32 million doses of freeze-dried vaccine of which 25 million came from the USSR and 2 million from the Netherlands. An additional 3 million doses of liquid vaccine were contributed by Jordan and 2 million by Mexico. Twenty-eight million doses had been distributed, but this was much less than what was needed. The problem was, in part, administrative (see Chapter 11). Samples from each lot of vaccine proposed for donation had first to be examined in a WHO reference laboratory to ensure that the lot met the requisite standards of potency and purity. Within WHO, the receipt and dispatch of samples were the duty of the unit dealing with biological standards, a small unit which was not otherwise concerned with the smallpox eradication programme. The reference laboratory, in turn, tested the specimens only when a sufficient number had accumulated to make it worth while. As a result, it was not uncommon for there to be a delay of 6-18 months between the receipt of samples and the notification of results. Even when the results were found to be satisfactory, further delays occurred, often of many weeks’ duration, because of problems in arranging for the shipment of the vaccine. The delays in testing were sometimes so long that the production laboratory sent the lots concerned to other consumers and the whole process had to be repeated.
In response to the Director-General’s emergency appeal of June 1963, a number of pledges of vaccine were made, the status of which in February 1965 (Table 9.9) illustrates some of the problems of vaccine supply at that time.
A total of 15 countries had pledged some 15 million doses of vaccine but 18 months later, as Table 9.9 shows, only about 6.6 million doses from 4 countries had been accepted, far short of the anticipated requirement of 50 million doses for India alone for 1 year.
Table 9.8: Voluntary contributions in cash or in kind (value of vaccine donations) to the WHO Special Account for Smallpox Eradication, 1958-1966 (US$)
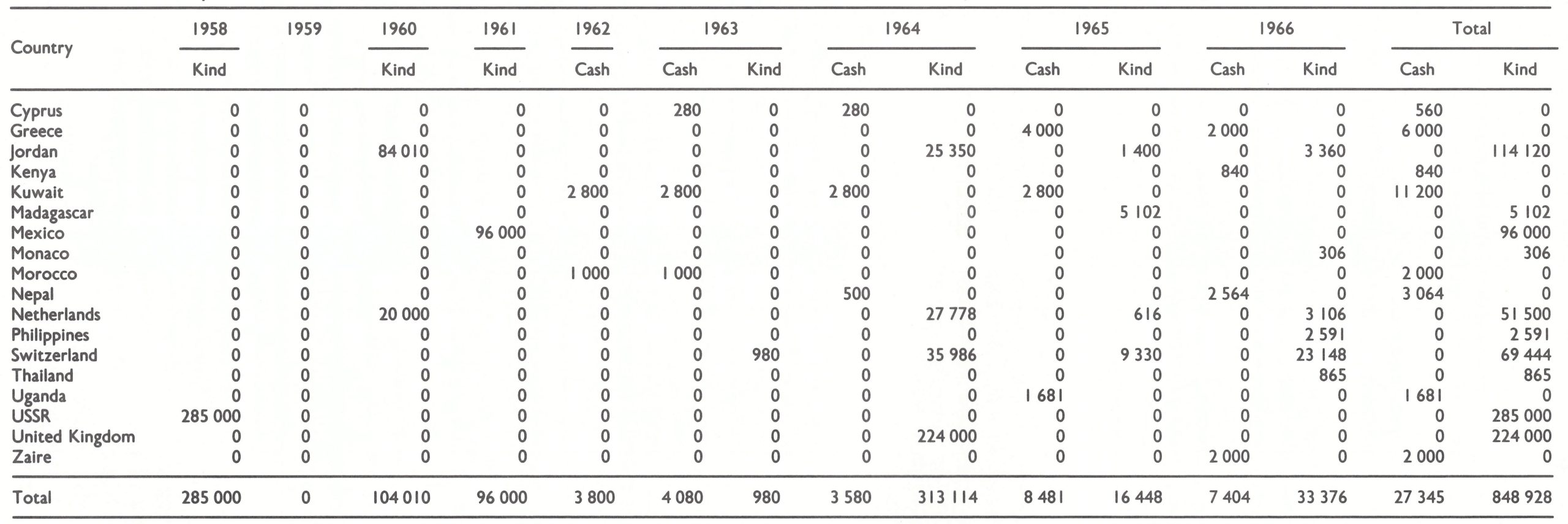
Table 9.9: Status in February I965 of vaccine contributions pledged in response to the emergency appeal of June 1963
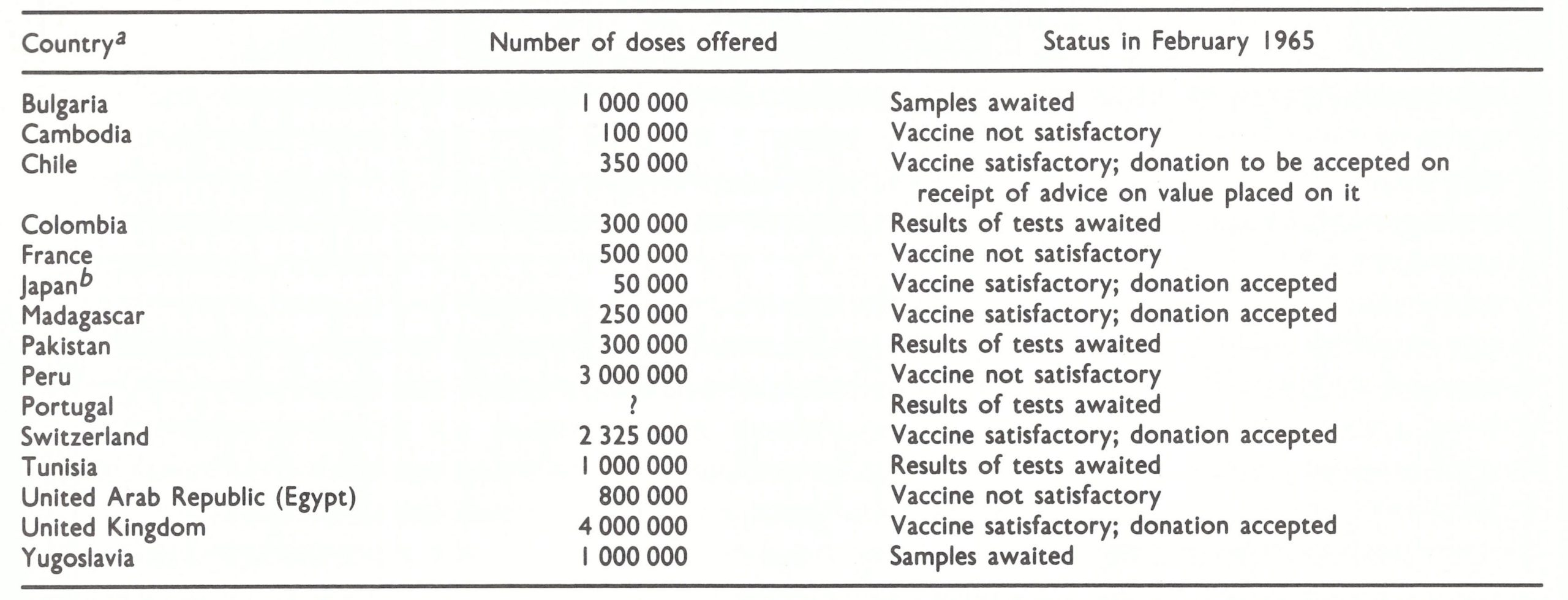 a Designation of countries used at the time.
a Designation of countries used at the time.
b Although the Japanese donation was accepted, its receipt Is not recorded in WHO documents; its value has therefore not been shown in Table 9.8.
The First WHO Expert Committee on Smallpox, 1964
Whatever the urgency conveyed in resolutions adopted by the Health Assembly, WHO took no additional measures to strengthen the smallpox eradication programme. The medical officer originally assigned to work on smallpox left the Organization in June 1963 and his responsibilities were transferred to another staff member, who dealt with smallpox only on a part-time basis.
In January 1964, WHO decided to convene an Expert Committee on Smallpox to discuss the problem. The Committee, in its report (WHO Expert Committee on Smallpox, 1964), carefully noted that the DirectorGeneral had been requested in 1959 “to prepare a programme of advice and help to countries on the basis that campaigns would be primarily the responsibility of national governments”. Nothing is said in the report of the progress or lack of progress made. Although the Committee viewed the eradication of smallpox as feasible, its recommendations did not propose a substantially more responsible role for WHO, as is evident from its report:
“The success of the smallpox eradication programme within a reasonable period of time is directly linked on the one hand with the amount of practical assistance in the form of technical advice and the supply of vaccine and other essentials which the smallpox-free countries are prepared to give to the endemic countries, and on the other with the efforts which the endemic countries are prepared to put into the setting-up of effective programmes on a national or regional basis.
“The Committee’s principal recommendation is that WHO should take all steps in its power to increase the international co-operation so that the success of the programme will be ensured in the shortest possible time.”
The Committee’s report discussed at length various aspects of the virology and immunology of smallpox and vaccinia, the steps to be taken in the conduct of a mass vaccination campaign, and other technical matters. In the execution of programmes, preparatory, attack, and control phases were described which resembled, in both terminology and strategy, those of malaria eradication. Following the preparatory phase, the entire population would be vaccinated during the attack phase, not unlike the corresponding phase in malaria eradication, during which all buildings were sprayed with DDT. After the completion of this phase, the control phase would begin, during which cases and outbreaks would be investigated and contained. The Committee placed its main emphasis on mass vaccination. It stated that vaccination of 80%, or more of the estimated population had been found to be unsatisfactory in some cases and that “the target must be to cover 100%of the population”. What the Committee had in mind was the situation in India, in which smallpox continued to occur in certain areas even though the number of vaccinations recorded was greater than 80% of the estimated population. The statement was made by the Committee despite the fact that assessment in India had already shown that unsuccessful vaccinations, repeat vaccinations of the same individuals and the falsification of reports on numbers of vaccinations performed meant that levels of vaccinia1 immunity were far lower than the reported 80% (see Chapter 15). Nevertheless, the Committee asserted that if success was to be achieved, the target must now be vaccination of the entire population. This conclusion only served to reinforce the Director-General’s doubts about the feasibility of smallpox eradication.
The Committee said little about the reporting of smallpox, except to deplore its unreliability at that time and to urge that “countries in which notification of cases and deaths is defective should make an effort to effect improvements”. No reference was made to the need for developing reporting systems or to surveillance and containment measures—both key factors in the post-1967 strategy.
The Seventeenth World Health Assembly, 1964
At the Seventeenth World Health Assembly (1964), Dr Kaul introduced the subject of smallpox eradication on behalf of the Director-General by stating: “The Expert Committee considered that the Organization’s eradication programme had been well conceived and soundly based” (World Health Organization, 1964b), an opinion which was not expressed in the Committee’s report. The principal problem, as seen by the Organization, was that of providing adequate quantities of freeze-dried vaccine. Dr Kaul pointed out that an emergency appeal for 30 million doses of vaccine, made immediately after the previous Health Assembly, had resulted in the receipt of only 7 million doses, all of which had been used.
Whatever the Expert Committee may have thought about the programme, delegates continued to express displeasure. Several pointed out that there had been no reduction in the number of reported cases between 1959 and 1963, that programmes were proceeding too slowly, and that it was time for WHO to assign priorities to its programmes and to prepare a definitive plan for the smallpox eradication programme, including provision for an adequate central and regional staff, estimates of needs and a specific time schedule (World Health Organization, 1964b). A resolution to this effect was submitted by the delegations of Australia, Chile, India, Liberia, the USSR and the USA, which, with some amendments, was adopted (resolution WHA17.43).

Plate 9.7. A display prepared for the WHO Regional Committee for South-East Asia in 1964. The strategy at that time focused wholly on vaccination and on achieving “100% coverage”. No mention was made of the reporting of cases or the containment of outbreaks.
A Retrospective View of Progress in Smallpox Eradication, 1959-1964
Although the Director-General, in his reports to the Health Assembly, had repeatedly observed that progress was slow and unsatisfactory, the information available to WHO regarding smallpox eradication programmes and on the numbers of cases throughout the world was fragmentary at best, and little effort had been made to obtain better information. Official telegraphic reports of cases were received by WHO in conformity with the International Sanitary Regulations, and a few countries provided descriptions of the programmes which they were undertaking. Reports on national programmes varied widely in quality, from highly optimistic ones containing few data to a very small number which described in detail where, and how many, vaccinations were being performed. Notifications, as the WHO Expert Committee had noted, were “frequently unreliable” and “not accurate”. Indeed, when reporting first began to be emphasized, WHO smallpox eradication staff estimated that not more than 504 of all cases were then being reported; later, it became apparent that the figure was closer to 1%.
Yet, more was achieved during the period 1959-1964 than was appreciated. The most significant progress was made in eastern Asia, notably the elimination of smallpox from China in 1961 or thereabouts. Had this achievement been known and properly documented, it might have provided encouragement both to WHO and to the endemic countries. The People’s Republic of China, however, did not become a Member of the Organization until 1973 and provided little information about either smallpox or its programme until 5 years later. From the incomplete reports available and the observations of visitors, it was believed that China had effectively brought smallpox under control, but not until 1978, when a WHO team visited the country, were data made available confirming that transmission had been interrupted in the early 1960s. Also, in 1959, Cambodia (Democratic Kampuchea) and Viet Nam appear to have recorded their last endemic cases although, because of the increasingly intense fighting throughout the area, their true status was also uncertain for many years. Malaysia, in 1960, and Thailand, in 1962, also succeeded in interrupting transmission following intensive, well-executed vaccination campaigns. Thus, in the period between the beginning of the global programme in 1959 and 1964, 5 large countries in eastern Asia became free of smallpox.
In western Asia also, a contiguous group of countries eliminated endemic smallpox following special vaccination campaigns conducted with varying degrees of diligence: Iraq in 1959, Democratic Yemen in 1960, Saudi Arabia in 1961, and Iran in 1963. Smallpox was, however, periodically reintroduced into these countries and others bordering the Gulf by pilgrims and migrant workers from southern Asia.
In the Americas, the regional programme of eradication begun in 1950 was continued. Although it was neither vigorously promoted nor substantially supported by WHO, Bolivia and Paraguay interrupted transmission in 1960 and Ecuador in 1963. A set-back occurred in 1963, however, when Peru was reinfected by the spread of smallpox from the Amazon region of Brazil.
Throughout much of Africa, the status of smallpox between 1959 and 1964 was less certain than in other parts of the world. Many countries were then becoming independent, civil strife was common and newly established governments were preoccupied with other matters. Health problems were but one of many concerns, and, among the specific diseases, smallpox was usually given little attention except when epidemics occurred. In northern Africa, smallpox was probably not endemic in 1959 except in Algeria, in which a protracted civil war had been in progress. Algeria’s last endemic cases, however, were recorded in 1961. South of the countries bordering the Mediterranean, endemic transmission ceased or diminished to low levels in a number of the former French colonies, in which freeze-dried vaccine produced in France had been extensively employed. As became apparent during the Intensified Programme (see Chapters 17, 19 and 20), a thermostable vaccine, when reasonably widely applied in sparsely populated African countries, often served to interrupt transmission even where coverage was not uniformly high and surveillance was poor. Of the former French colonies, the Central African Republic, the Congo and Gabon appear to have become smallpox-free in 1955,1954 and 1956, respectively ; Mauritania interrupted transmission in 1962 and Senegal in 1963. The Gambia recorded its last endemic cases in 1966. In the sparsely populated countries of Djibouti and Somalia, endemic transmission ceased in 1959 and 1962 respectively, without special programmes. In Angola and the Sudan, freeze-dried vaccine was used in intensive vaccination campaigns, and those countries became free of smallpox in 1959 and 1962 respectively. However, because of the long, open borders between African countries and the generally inadequate health infrastructures, endemic smallpox recurred in Africa as a consequence of importations. Thus 3 contiguous countries—the Central African Republic, the Congo and Gabon—began again to experience epidemics of smallpox in 1961-1962, as did Lesotho, South Africa and Swaziland in 1960-1963.
Meanwhile, other countries, including Burma, Colombia, India, Pakistan and Peru, conducted major vaccination campaigns which were reported in generally optimistic terms.
When the situation is viewed in retrospect, it is evident that much was achieved by a number of countries during this period, despite the lack of external resources and despite inadequate health care structures in many of them and the use of the thermolabile liquid vaccine by most. These achievements were, however, largely unknown to WHO Headquarters staff, so that the DirectorGeneral’s reports were perhaps more pessimistic than was warranted.
Events Leading to the Introduction of an Intensified Global Programme, 1965
Interest in a more important role for WHO in global smallpox eradication began to increase within the WHO Secretariat in 1964 following the appointment of Dr Karel Raska as Director of the Division of Communicable Diseases. Dr Raska, a distinguished and determined epidemiologist from Czechoslovakia, believed that smallpox eradication was an attainable objective. As he wrote: “The increased expenditure on the smallpox eradication programme in developed countries would pay itself back within three years after the achievement of eradication” (Raska, 1966). Even this estimate, as it was later found, was conservative, but using this and other arguments, he was able to persuade the Director-General of the need to create a separate Smallpox Eradication unit. This was established early in 1965, although only one medical officer, Arita, and a secretary were provided to staff it.
Meanwhile, two developments in the USA provided impetus to establishing an intensified eradication programme: the development and demonstration of the jet injector for administering smallpox vaccine; and a commitment by the USA to provide technical and material support to the smallpox eradication programme. These events are summarized below and described in greater detail in Chapter 17.

Plate 9.8. Karel Raska (b. 1909). a distinguished Czechoslovak epidemiologist, served as Director of the Division of Communicable Diseases in WHO Headquarters from 1963 to 1970. He was a staunch advocate within the Organization of global smallpox eradication and played an important role in launching the Intensified Programme in 1967. He had previously been Director of the Institute of Epidemiology and Microbiology, in Prague, which contributed a number of the epidemiologists, including Jezek. Who worked for the Intensified Programme.
Development of the jet injector
During 1964-1965, pilot field studies using the jet injector showed that it had potential in facilitating mass vaccination campaigns. The device had been developed during the 1950s for administering vaccines and other biologicals by percutaneous inoculation. A piston propelled a measured quantity of vaccine through a narrow orifice under high pressure sufficient to penetrate the skin and enter the subcutaneous tissue (Hingson et al.,1963). The fitting of a reservoir of vaccine to the injector made it possible for 500 or more vaccinations to be performed before replenishment was necessary; as many as 1000 persons per hour could be vaccinated by this means. For mass vaccination campaigns, it offered unique advantages, but before it could be used with smallpox vaccine two basic problems had to be solved: to be effective, smallpox vaccine had to be inoculated intradermally rather than subcutaneously; and the only jet injector in the 1950s which was sufficiently sturdy for large-scale use was powered by electricity and therefore unsuitable for use in the field. In 1962, Mr Aaron Ismach of the United States Army Medical Equipment Research and Development Laboratories (Millar et al., 1969) developed a special nozzle which made it possible to inoculate vaccince intradermally, and, subsequently, staff of the Communicable Disease Center (CDC) in the USA demonstrated that the technique was safe and produced as high a proportion of successful vaccinations as that obtained by conventional techniques. The problem of the power supply was also solved when Mr Ismach developed a pedal-operated, hydraulically powered model. Early in 1965, Dr Millar and his colleagues in CDC (Millar et al., 1971), serving as PAHO consultants, demonstrated in a pilot study in Brazil that a vaccination campaign using the jet injector required far less manpower than, and cost only one-third as much as, a campaign in which conventional techniques were used (see Chapters 11 and 12). Although this instrument eventually proved less useful than was initially expected, its advent stimulated the undertaking of mass vaccination campaigns.
The commitment of the USA
Further impetus was given to global smallpox eradication when, in 1965, the USA, WHO’S largest contributor, began actively to support the eradication concept and in November of that year offered to provide technical and material assistance for smallpox eradication and measles control programmes in 18 (eventually 20) contiguous western and central African countries (Gelfand & Henderson, 1966). The background to this initiative is of interest. Support by the USA for largescale health programmes, other than those for malaria eradication and family planning, was a departure from its bilateral assistance policy at that time. The commitment to smallpox eradication emerged as a consequence of two unrelated factors: the need for a United States initiative as a demonstration of support for International Cooperation Year, a celebration of the 20th anniversary of the United Nations; and a developing regional programme, supported by the USA, for measles vaccination in western and central Africa.
United States involvement in providing measles vaccine to countries in western and central Africa began in 1961, when staff of the National Institutes of Health (Meyer et al., 1964a) demonstrated in a small study in Upper Volta (now Burkina Faso) that the new attenuated Edmonston strain of measles virus was both safe and efficacious. This was followed, at Upper Volta’s request, by a country-wide measles vaccination campaign and, subsequently, by programmes supported by the United States Agency for International Development (AID) in other countries in the area (Henderson, 1967). The programme proved to be popular and, by 1965, at the request of governments in western and central Africa, AID had agreed to provide assistance to 11 of them. In the same year, CDC was approached and asked to provide the requisite technical assistance.
To Henderson, then on the staff of CDC, and his colleagues, the measles control programme made little sense, since it would inevitably be too difficult and costly for the countries concerned to sustain when bilateral assistance ceased. A regional programme for the eradication of smallpox, however, appeared to be feasible and to offer the possibility of achieving permanence. However, the control of smallpox, let alone its eradication, had not previously been considered by AID staff. Meanwhile, in a speech on 10 June 1964, the President of the United States, Lyndon Johnson, took public notice of the vaccination campaign in western Africa when he ‘promised a new initiative in support of International Cooperation Year, stating: “I intend to dedicate this year to finding new techniques for making man’s knowledge serve man’s welfare. . . I intend to expand our efforts to provide protection against disease.” He then alluded to the measles vaccination programme in western Africa and continued: “We will expand our efforts to prevent and to control disease on every continent.”
That the United States commitment might apply to smallpox did not emerge until World Health Day of the following year—7 April 1965. World Health Day, which commemorates the day the WHO Constitution entered into force in 1947, has a different theme each year. In 1965 “Smallpox Alert” had been selected as a result of many smallpox importations into Europe in 1962-1963, the intention being to stress the need for vigilance. Dr Benjamin Blood and Dr James Watt of the United States Public Health Service proposed a special presidential message for that day, committing the USA to supporting global smallpox eradication as an answer to the need for continuing vigilance against importations. Although no action was taken, a second opportunity to obtain a presidential commitment arose a month later in conjunction with the expected debate on smallpox eradication at the Eighteenth World Health Assembly. This time they were successful in persuading the staff of the President of the USA to issue a special press release: “President Johnson announced today that he has instructed the US. Delegation at the World Health Assembly to pledge American support for an international program to eradicate smallpox completely from the earth within the next decade.” United States support was envisaged as the “contribution of technical personnel and other resources to the Pan American Health Organization…” and “assisting in the establishment of laboratory facilities in the developing countries to help meet requirements of vaccine”.
Two months after this press release, CDC proposed to AID that a regional smallpox eradication-measles control programme should be established throughout western and central Africa. This was a far more extensive and costly enterprise than the mote geographically limited measles vaccination campaign envisaged by AID, and quite different from the type of assistance pledged by the delegation of the USA in its statement at the World Health Assembly. The President’s staff, however, on learning of the proposed plan, expressed support and, on 23 November 1965, a press release was issued which began:
“Plans for campaigns to protect 105 million people from smallpox and measles in 18 African countries were announced today by the White House.. .AID and PHS staff are beginning consultations with African and WHO officials on plans for the campaign, its acceptability to African countries and their willingness to contribute to the program.”
What had begun as a field trial of a new measles vaccine in 1961 became a smallpox eradication-measles control effort involving 20 countries of western and central Africa (see Chapter 17, Fig. 17.1); in the process, the USA formally and strongly expressed its support for the global smallpox eradication programme.
The Eighteenth World Health Assembly, 1965
At the request of the Seventeenth World Health Assembly, a comprehensive plan for a global eradication programme was presented by the Director-General at the Eighteenth World Health Assembly in May 1965 (World Health Organization, 1965b). Its preparation had been no easy task for the Secretariat, given the small number of staff assigned to smallpox eradication and the lack of information in Geneva about smallpox and smallpox eradication programmes throughout the world. To prepare the report, WHO recruited two consultants, Dr Frank Grant of Ghana and Dr P. M. La1 of India, to assist Arita. They were asked to review all available information and to visit 4 countries (Afghanistan, Burma, Mali and Nigeria) “to assess the situation and to reach some broad conclusions on the basis of a sample survey”.
In his report (World Health Organization, 1965b), the Director-General expressed the belief that, so far as could be determined, 12 countries had succeeded in eradicating smallpox since 1959, but much more needed to be done. He concluded that:
- In many endemic countries, other health problems were considered to be of greater importance than smallpox.
- There was a need for, and frequent lack of, an adequate administrative and supervisory structure.
- Supplies of heat-stable freeze-dried vaccine in very large amounts and also transport, refrigeration and other equipment were needed, as well as short- and long-term consultants for the planning and execution of the campaigns.
- The maintenance phase (continuing vaccination) was as important as the attack phase if smallpox was to be prevented from recurring.
- Pilot projects were needed to determine strategy.
- Assessment of vaccination success rates by an independent team was vital.
- Contiguous endemic countries should start mass campaigns simultaneously.
The recommendations in the report dealt broadly with each of these points.
Introducing the report at the Health Assembly, Dr Kaul indicated that US$80 million would be needed, an estimate which was based on the assumption that the entire population of the endemic countries would need to be vaccinated, at an average cost of US$0.10 per vaccination (World Health Organization, 1965c). The estimate made no provision for the People’s Republic of China, which, as previously noted, was not then a Member State of WHO. Of the total, US$28 million were thought to be required from international sources—i.e., about US$5 million a year for 6 years, rather than US$10 million, as estimated in 1963.
Dr Kaul noted that a substantial increase in effort and in material support was essential if the eradication programme was to be speeded up and achieve its goal within a reasonable time. To strengthen the argument that additional voluntary contributions should be made by the smallpox-free industrialized countries, he pointedly drew attention to the costs associated with a recent importation into Sweden.
Delegates again indicated their dissatisfaction with the slow pace of progress, but more bluntly than before. A delegate of the USSR, Dr M. A. Akhmeteli, expressed the increasing irritation of his country, declaring:
‘‘Malaria eradication seemed to have been the favourite daughter of WHO, whereas smallpox eradication seemed to have been treated rather as a foster child…criticism might have been averted if concrete measures had been included in the 1966 programme…The delegation of the USSR would support any concrete proposal for speeding up the programme, but it wished for a real programme.” (World Health Organization, 1965c.)
Sir George Godber, of the United Kingdom, echoed these thoughts:
“…the Organization had been engaged in smallpox eradication for some seven years and…the programme had not met with as much success as might have been possible. However, only WHO could get down to the root of the problem. It would be far preferable for WHO to concentrate upon smallpox eradication than to turn to some more ostentatious programme [a world health research centre then under consideration] which would lend only spurious prestige to the Organization…”
Support for a WHO budget specifically for smallpox eradication was growing, but the USA in particular, although a promoter of smallpox eradication, was not in favour of this. Official government policy in the USA held that WHO should provide only technical assistance and advice; material support should be provided through other United Nations agencies and through bilateral and voluntary contributions to WHO. Accordingly, Dr Williams, of the United States delegation, introduced a resolution requesting the Director-General “to seek anew the necessary financial and other resources”. This, of course, was what the Director-General had been asked to do by several preceding World Health Assemblies, and he had done so, but with little success. Potentially, one of the larger contributors was UNICEF, but Sir Herbert Broadley, on behalf of that organization, stated at the Health Assembly that UNICEF “would be unable to participate in a world-wide mass eradication campaign against smallpox, as it had done against malaria”.
Although the resolution adopted at the Eighteenth World Health Assembly (WHA18.38) added little to what had already been said, its first operative paragraph expressed, more clearly than before, the attitude of the delegates:
“DECLARES the world-wide eradication of srnallpox to be one of the major objectives of the Organization” (World Health Organization, 1973a).
A Special Budget for Smallpox Eradication, 1966
The Director-General’s position was a difficult one. If a more effective smallpox eradication programme were to be mounted, additional resources would be required, but it was apparent that voluntary contributions alone would not suffice. At the same time, malaria eradication was experiencing serious difficulties, for which additional resources were also required. However, voluntary contributions for malaria eradication had diminished markedly, thus making substantial additional funds from WHO’s regular budget necessary, if only to sustain the existing level of activities. The Director-General could propose a substantial increase in the Organization’s budget to meet the additional requirements of an intensified smallpox eradication programme but that was certain to be met by strong objections, especially from the industrialized countries, which provided the bulk of the Organization’s funds. The Director-General’s proposed budget was debated each year by the Executive Board and Health Assembly but had regularly been accepted as presented. An unacceptable increase involved the risk that the proposed budget would be rejected and that a divisive debate would follow, an outcome which had so far been avoided.
The problem was resolved by presenting a proposal in two parts. The first was the regular budget allocation, which was increased each year to permit a modest growth in WHO’s activities and to compensate for inflation. The second was for a special allocation of USS2.4 million, which was identified as being explicitly for smallpox eradication; the Health Assembly could consider this separately and decide whether or not it was willing to commit these additional funds in support of the resolutions which it had adopted on smallpox eradication. If it was unwilling to do so, it would be apparent that delegates were less firmly committed to smallpox eradication than the Health Assembly’s resolutions would suggest.
The allocation proposed for smallpox eradication may not now appear very large, but WHO’s total budget at that time was itself not substantial. If both allocations were approved, it would mean an increase in the Organization’s total budget of almost 22% and a comparable increase in the assessments of all Member States. Many countries could be expected to vote against the smallpox eradication budget: most of the industrialized countries, as a matter of policy, were opposed to substantial increases in the budgets of the United Nations specialized agencies; others, faced with difficulties in obtaining adequate amounts of convertible currencies to pay their assessments, would also object; and, finally, the smallpox-free developing countries that would not directly benefit from the programme could not be counted on for support.
Before presenting a new proposal to the Executive Board in January 1966, and then to the Nineteenth World Health Assembly in May of that year, the Director-General decided that another, more comprehensive, report should be prepared which would provide a detailed plan of action and more precise cost estimates. In September 1965, Henderson was asked by WHO to work with Arita, Dr RaSka and Dr W. Charles Cockburn, chief of the Virus Diseases unit, in Geneva to prepare the document. Because accurate information on the status of programmes and the occurrence of smallpox was still largely lacking, this planning exercise was as speculative as earlier ones.
The Director-General’s Report to the Nineteenth World Health Assembly
The document prepared for presentation to the Executive Board in summary form, and to the Health Assembly in full (World Health Organization, 1966b), is of interest in that it sets forth the basic framework within which the Intensified Programme began to function. Conceptually, the programme differed from that for malaria eradication in three important ways: (1) principles for programme execution were provided rather than a highly prescriptive plan, in the belief that programmes would have to differ from country to country depending on resources, local conditions and the epidemiological situation ; (2) a reporting system for cases was to be developed from the inception of the programme to serve as a guide in its execution rather than introducing such a system at the conclusion of an attack phase; and (3) research was to be encouraged in the belief that, whatever might be known about smallpox, more could be discovered which would facilitate its eradication. Projections of needs and proposals for the administrative structure represented a compromise between what Henderson and Arita considered necessary and what was acceptable to the Director-General.
Strategy
A basic strategy calling for systematic vaccination campaigns employing freeze-dried vaccine was retained. A new and important additional component was surveillance-the notification and investigation of cases and their epidemiological characterization. This was an approach developed by Dr Alexander Langmuir at CDC (Langmuir, 1963), with whom Henderson had worked for the preceding decade. It had been applied in other disease control programmes in the USA, but appeared to be equally applicable to smallpox. Since this was the strategy which proved so important in the achievement of eradication, the relevant section of the Director-General’s report is quoted here (World Health Organization, 1966b):
“It is necessary for the eradication programmes to develop a systematic plan for the detection of possible cases and concurrent investigation regarding the source and site of acquisition of the disease, the establishment of vaccination status and the prompt instigation of containment measures. Detailed epidemiological investigation of all cases to establish the reasons for their occurrence and the means by which they are being spread can be one of the most effective instruments to provide continuing guidance and direction in the vaccination programme. In the simplest terms, each case which occurs suggests the possibility of flaws in the programme. An outbreak, however small, demands a full critical review with appropriate revisions of the programme.
“The ultimate measure of any eradication programme is its success in reducing the number of cases to zero. So long as the disease is endemically transmitted, an eradication programme has failed to achieve its goal whatever the proportion of the population apparently successfully vaccinated.
“Even in countries with a limited local health structure, a systematic surveillance plan can and must be developed as an essential component of the eradication programme. The simplest type of approach might consist of a weekly report from each hospital and dispensary noting whether suspect cases of smallpox had or had not been seen. Simple basic information should be requested for each suspect case, consisting of name, age, sex, residence of patient and date of onset of illness. Hospitals or dispensaries failing to submit a report should be contacted promptly to ascertain specifically whether or not cases have been observed.
“This portion of the surveillance activity should be initiated concomitantly with the development of any systematic vaccination programme. Even where cases are comparatively few at the inception of the programme, detailed investigative and containment efforts should be initiated promptly. The discovery of apparent indigenous transmission should be accompanied by a two-or three-day intensive mass programme of vaccination in the immediate area. In highly endemic countries, such detailed field appraisal may not be practical until a vaccination campaign in the immediate areas has been completed. It should not, however, be delayed until a country-wide programme has been completed…
“A regional surveillance programme is an important component part of the eradication scheme. Increasing facilities for travel plus continuing major population migrations across national borders permit ready dissemination of infection from country to country. Strengthening of the advisory staff at regional and national level to assist individual countries in the development of adequate surveillance programmes, able to render assistance promptly both in the field investigation phases and in direct containment operations and serving to Integrate information Obtained from the separate countries, would ensure greater success of the overall programme.
“It should be realized that the surveillance system thus being developed will be utilized not only for smallpox services but also to provide epidemiological services for other communicable diseases.”
Plate 9.9. Alexander Duncan Langmuir (b. 1910), as director of the epidemiology programme at the Communicable Disease Centre, Atlanta, GA. USA, from 1949 to 1970, developed the concept of surveillance and its application to the control of communicable diseases in the USA. This approach was introduced in 1967 in the Intensified Programme.
Status of smallpox
The report defined the endemic countries at the end of 1965 as including 6 in Asia (Afghanistan, Burma, India, Indonesia, Nepal and Pakistan), 3 in South America (Brazil Colombia and Peru) and essentially all African countries south of the Sahara. The cases officially reported to WHO in 1964 numbered Just under 50 000; essentially the same number was reported in 1965, and this was not significantly different in magnitude from the 60 956 cases recorded in 1960. It was pointed out, however, that little credence could be given to these figures.
From what was known in WHO, few programmes were thought to be making substantial progress. Of 8 projects which were being assisted in some manner by WHO in Africa, only those in Cote d’Ivoire and Upper Volta were doing well. Liberia and Mali, which had received more assistance, had succeeded in vaccinating less than one-fifth and one-third of their populations, respectively, in 4 years; combined yaws control and smallpox vaccination projects in Nigeria, Sierra Leone and Togo were progressing very slowly; and a project in the Sudan, begun 2 years earlier, was considered unsatisfactory. In South America, only Peru was then taking effective measures. In Asia, mass vaccination campaigns had begun in Burma, India and Pakistan, but only Burma appeared to be making satisfactory progress. WHO-assisted projects in Afghanistan and Nepal were recognized as being in serious difficulty.
Overall programme
An ambitious and, in retrospect, unduly optimistic programme was proposed which focused on the provision of support in 1967 to programmes already in operation and, in 1968, to the extension of the programmes to all other countries to be covered (Table 9.10); this made a total of 41 countries (as before, the People’s Republic of China was not mentioned). The terms preparatory, attack and maintenance phases were used in the planning document but were later discarded when in practice they were found to be of little use. Plate 9.9. Alexander Duncan Langmuir (b. 1910). Thus, any comparison between projected and as director of the epidemiology programme at the actual achievement is impossible to make. Communicable Disease Center, Atlanta, GA. USA,
It was expected that the programmes would differ from country to country, the vaccination campaigns in some being conducted in concert with other programmes by local health staff, and in others by special teams. Vaccination by means of jet injectors, supplemented by multiple-pressure vaccination, was to be used in South America and Africa, but it was felt that prior evaluation was necessary to determine whether jet injectors were suitable for use in Asia. The planning document stressed the need to ensure better vaccination coverage in the more densely populated areas and among migrants but, wherever vaccination was performed, assessment of the results by independent teams was considered vital.
An “adequately staffed headquarters unit” of 3 medical officers was proposed, as well as the posting of a regional adviser in each of the 4 WHO regions in which endemic smallpox was present. International technical assistance personnel were expected to be required in most countries. Special emphasis was given to the need for regional staff “since the method of operations should be flexible enough to develop reasonably efficient programmes in the different epidemiological situations and health service structures in each country or area”. The need for regional offices to assist in the establishment of regional surveillance systems was also noted in the document. It was proposed that funds should be provided for the development of vaccine production facilities, interregional training courses, consultants, fellowships, and necessary supplies and equipment.
Vaccine
The plan called for 220 million persons to be vaccinated in 1967 (Table 9.11). Assuming, as the report did, that the South American countries and Pakistan produced sufficient vaccine for their own needs, and that the USSR would satisfy the needs of Afghanistan, Burma and India through bilateral assistance, enough vaccine would be available for 180 million persons. Much of the rest of the deficit was expected to be met if the United States programme in western and central Africa was implemented, since that would provide some 30-40 million doses each year.
Table 9.10: Planned phasing of smallpox eradication programmes assisted by WHO, 1967- 1976; extracted from the Director-General’s report to the Nineteenth World Health Assemblya,b
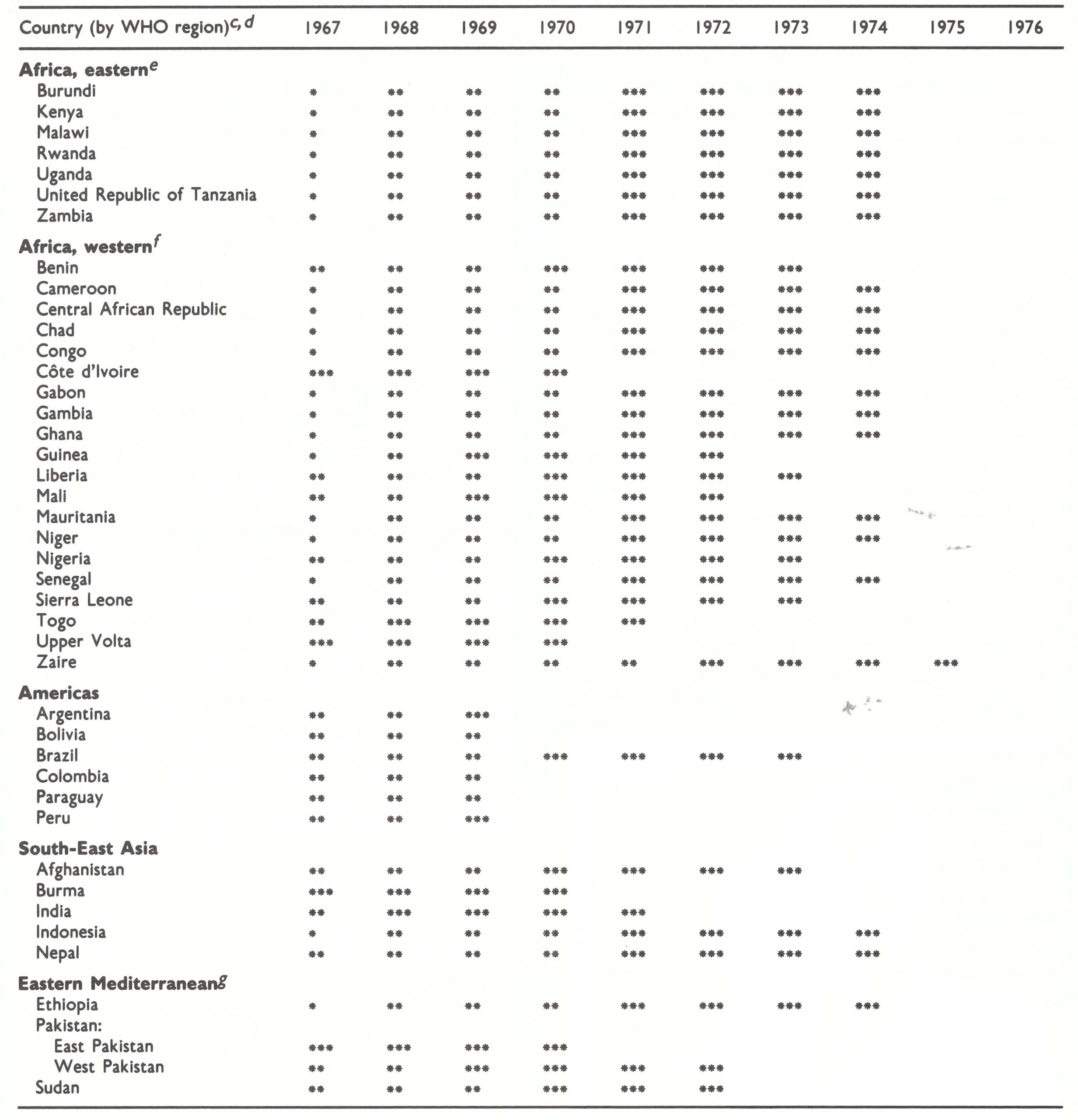 a Source: World Health Organization (1966b).
a Source: World Health Organization (1966b).
b = preparatory stage, or national vaccination campaign in operation; 0s attack phase; *a* = maintenance phase with international assistance.
c Designations of countries as in 1976, except for East Pakistan, which became Bangladesh in 1971.
d Afghanistan formed part of the Eastern Mediterranean Region of Who from 1969. Bangladesh formed part of the South-East Asia Region from 1972. Ethiopia formed part of the African Region from 1977.
e Excluding Angola, Basutoland (Lesotho), Bechuanaland (Botswana), Mozambique, Southern Rhodesia (Zimbabwe), Swaziland and South Africa. It was anticipated that eradication programmes could be carried out in these countries or territories with national finance only.
f Excluding Portuguese Guinea (Guinea-Bissau) and Equatorial Guinea. It was anticipated that eradication programmes could be carried out in these territories with national financing only.
g Smallpox vaccination campaigns were in progress in Saudi Arabia, Somalia and Yemen; however, detailed information was not available at the time the Director-General’s report was prepared.
Table 9.11: Estimated number of smallpox vaccinations to be carried out with international assistance, 1967-1976; extracted from the Director-General’s report to the Nineteenth World Health Assembly
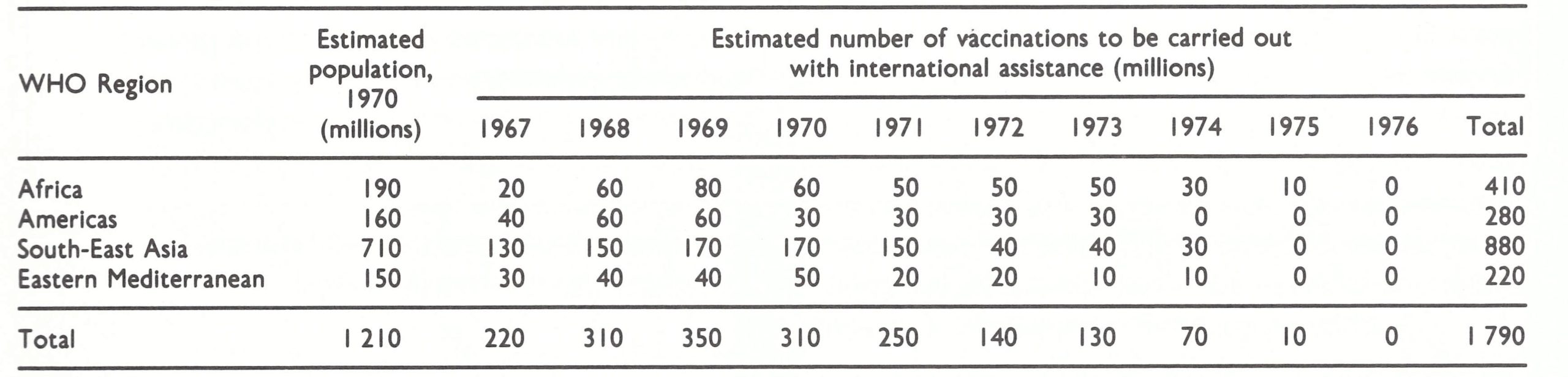 Source: World Health Organization (1966b).
Source: World Health Organization (1966b).
Costs
The overall cost estimates of the programme were based on crude approximations made, as before, by estimating the number to be vaccinated each year and multiplying by US$0.10. The international assistance required was assumed to be about 30% of the total, comprising the costs of external technical assistance (vaccine, transport, supplies and equipment). Overall, an expenditure of US$80 million was anticipated, of which US$48.5 million from international sources would be required (Table 9.12). The totals were substantially greater than those estimated a year before-US$80 million overall, with US$28 million from international sources. For the first year, a WHO budget of US$2.4 million was requested, or 36% of all external assistance required. The balance, it was hoped, would be made up by bilateral support or voluntary contributions. Although the estimates were rough at best and did not take inflation into account, it is worth noting that the international support ultimately provided between 1967 and 1979 (see Chapter 10, Table 10.8) amounted to approximately US$98 million, twice the projected sum.
Research
A statement that there was a need for continuing research on the epidemiology and virology of smallpox was inserted despite the objections of senior WHO staff, who believed, as they had with malaria, that enough was known about smallpox and that the only problems were the mobilization of resources and administration. To obtain agreement to include a section on research, a sentence had to be added: “It is hoped that total or partial financial support for many of these [research] projects will be provided directly to the responsible investigators from national funds.”
Table 9.12: Anticipated expenditure on the Intensified Smallpox Eradication Programme, 1967-1976 (millions of US$); extracted from the Director-General’s report to the Nineteenth World Health Assembly
 Source: World Health Organization (1966b).
Source: World Health Organization (1966b).
Problems With the Plan
The proposed plan was the outcome of a compromise between its authors and senior WHO staff, especially in regard to financial and administrative provisions. Senior WHO staff viewed the problem as being primarily that of providing adequate resources for mass vaccination and saw little need for either technical assistance or international coordination of efforts. Henderson and Arita, believing that the programme and particularly the concept of surveillance would be difficult to implement, saw the problem differently and expressed their concern as follows in a letter of 14 October 1965 to Dr Karel RaSka, Director of the Division of Communicable Diseases (each problem proved to be as great as or greater than they foresaw):
“. . . certain fundamental principles are key...adequate central guidance and direction must be provided which has sufficient authority to express itself through Regional Office levels to the individually responsible countries; adequate financing is mandatory; capable staff at all levels is requisite...The programme, as revised, has a number of inherent weaknesses in each of these major areas:
“(1) Central staff—The proposed staff both at headquarters and at regional levels is...far less than adequate to undertake the job... the general scheme of the proposed programme is different from programmes of the past ; surveillance techniques and their application are unknown in every one of the countries... a substantial amount of training, guidance and assistance will be required from well-trained full-time staff within the Organization... The relationship of the Regional Offices to the programme, central headquarters and country programmes should be carefully examined. Already we sense potential conflicts in policy with AMRO [Regional Office for the Americas], AFRO [Regional Office for Africa] and SEAR0 [Regional Office for South-East Asia].
“(2) Financing—More than half of the anticipated external budget for supplies and equipment must be forthcoming on some sort of volunteer basis from other international organizations or bilateral assistance programmes... Voluntary contributions, however, ...have been negligible...In the light of recent past experience, we question whether this is sound... we are still concerned that a maximum of flexibility in application of funds be maintained both within Regions and between Regions and between budget categories.
“(3) Staff—We gather there are major difficulties at this time in recruitment of competent staff… The necessity of the headquarters and regional WHO smallpox staffs undertaking some responsibility in this regard should be recognized and central staff augmented accordingly…Realistically, we suspect that the programme will be obliged to rely principally on comparatively junior medical officers who can be given intensive training and carefully supervised in their field work… However, intermediate and senior level supervisory people would be requisite. They are not provided for under the revised proposal.”
The Discussions at the Executive Board (January 1966) and at the Nineteenth World Health Assembly (May 1966)
Dr Kaul introduced the Director-General’s report at the Executive Board session in January 1966 and Mr Siegel described the implications of a second appropriation for smallpox eradication. Dr Kaul noted that the Director-General, in his regular budget, had foreseen the need “to provide the impetus, direction, coordination and supervision on a global basis” and, accordingly, had proposed for 1967 the provision of US$200 000 in the regular budget (World Health Organization, 1966a). This included both funds administered by WHO on behalf of the United Nations Expanded Programme of Technical Assistance and PAHO funds. Attention was not drawn to the fact that the amount proposed for smallpox eradication was actually the smallest since 1963. Mr Siege1 introduced the special appropriation for smallpox eradication. WHO’S effective working budget for 1966 had been US$42 442 000; the corresponding figure proposed for 1967 was US$47 242 000, an increase of 11.3% (World Health Organization, 1965d). Two possible figures for the appropriation for smallpox eradication were offered : US$ 1 million and US$2 415 000. If US$1 million extra were provided for smallpox, the increase in the overall budget would be 13.7%; if US$2 415 000 were provided, it would be 17.0%. Tables had been prepared showing the additional assessments for each country for additions to the regular budget of US$1 million and US$2 415 000. If US$2 415 000 were provided, the additional cost for the smallpox programme for the USA, for example, would be US$801 660; for Czechoslovakia, US$25 440; and for the United Kingdom, US$165 210. For purposes of comparison, the estimated annual costs of routine national vaccination activities, as determined at that time by those countries were: USA, US$20 million (later studies revealed the amount to be almost US$150 million), Czechoslovakia, US$1 million, and the United Kingdom, US$650 000. In the course of the debate, however, the fact was noted that the United Kingdom had spent US$3.8 million to control imported outbreaks in 1962-1963.
After prolonged discussion the Executive Board agreed, in principle, to recommend to the Health Assembly the creation of a special appropriation for smallpox eradication in the regular budget, although most Board members expressed the belief that the amount allocated for smallpox eradication should probably be no more than US$1 million, at least for the first year.
At the Nineteenth World Health Assembly (May 1966), the Director-General’s report on smallpox was presented to one of its two principal working committees, the Committee on Programme and Budget. There was, however, only a brief discussion before the Committee was required to resume a suspended debate on a draft resolution on malaria eradication, a resolution which deplored its slow rate of progress and actual regression in several countries. Before the debate could be resumed, the Committee took up the question of the overall WHO budget for 1967, the principal point at issue being the amount, if any, to be added for smallpox eradication.
The total budget figure under consideration by the Health Assembly, including funds for smallpox eradication, was US$ 515 000, an increase, the Director-General said, of 15.8% over the corresponding level for 1966, including the supplementary estimates for that year (World Health Organization, 1966c). For purposes of comparison, it is useful to note what the assessments of certain countries would have been for a budget of this magnitude. The Financial Report for 1967 shows that in that year only 5 countries contributed 5% or more of the budget—USA, US$16.6million; USSR, US$7.1 million; Federal Republic of Germany, US$3.5million; United Kingdom, US$3.4 million; and France, US$2.9 million—while 52 countries contributed the minimum amount, which that year was US$21 320 (World Health Organization, 1968).
The developing countries, the principal recipients of the Organization’s funds, usually argued for large increases in the budget; especially strong support for the smallpox eradication programme was voiced by delegates from the countries of western and central Africa, which had been promised assistance by the USA for a regional smallpox eradication-measles control programme. However, Professor E. J. Aujaleu, an eminent French government official and for many years a delegate of France, expressed a view frequently taken by delegates from most of the industrialized countries—namely, that the Organization’s budget should not, in principle, increase faster than the average annual increase in the gross national product of its major contributors. He suggested that an overall increase in the budget of between 5% and 6% would have been more appropriate; other delegates proposed figures ranging from 4% to 8%. He and other delegates also suggested that the smallpox eradication programme might have an opportunity to become better established if a more modest beginning were to be made in 1967 and the programme expanded later. He proposed an overall budgetary ceiling of US$50 million, with approximately US$1 million earmarked for smallpox eradication. This proposal was supported by Canada, Italy, Turkey and the USSR. A compromise proposal was put forward by the USA, providing for a budgetary ceiling of US$50.4 million, of which US$1.4 million would be set aside for smallpox eradication. This proposal was supported by Australia, Austria, Belgium, the Federal Republic of Germany, Iraq, Japan, the Netherlands and Pakistan. Yugoslavia endorsed the United States proposal for a budgetary ceiling, provided that the full amount of US$2 415 000 was allocated to smallpox eradication. Meanwhile, several countries indicated simply that they could not agree to the budget as proposed (Argentina, Czechoslovakia, Hungary, Poland, Romania and Venezuela); 19 developing countries, plus Finland, Norway, Sweden and Switzerland, spoke in favour of the Director-General’s budget proposal. At the closure of the debate, successive votes were taken on the proposals advanced by France and the USA (Table 9.13), a two-thirds majority of Members present and voting being required for approval of the budget.
Table 9.13: Nineteenth World Health Assembly, May 1966: results of votes on budget proposals
Source: World Health Organization (1966c).
The proposals put forward by France and the USA were defeated, and a larger budget, providing all the requested funds for smallpox eradication, was accepted by a margin of 2 votes—the narrowest margin for the acceptance of a budget in the Organization’s history. In perspective, the sum appropriated for smallpox eradication was not large, considering that programmes were expected to be conducted in 41 countries, thus providing an average allocation of less than US$60 000 per country per year. However, the total sum accounted for 4.7% of WHO’S total budget and was some 10 times greater than the sum allocated in the Organization’s 1966 budget.
When the Committee on Programme and Budget resumed discussion of the proposed smallpox eradication programme, whose budget was now assured, delegates expressed their general support. In the course of the debate, Dr D. Venediktov, a delegate of the USSR, announced that his country would make a contribution of 25 million doses of vaccine each year for 3 years, a contribution which the USSR continued annually throughout the global programme; Dr Blood, a delegate of the USA, briefly described the commitment of the USA to programmes in western and central Africa ; and additional assistance was promised by the League of Red Cross and Red Crescent Societies. The Director-General was requested to seek help from the World Food Programme, UNICEF and UNDP, as well as bilateral agencies. Although bilateral support was to play an important contributory role, relatively little assistance from other international organizations ever materialized.
The programme was thus accepted by the Health Assembly, albeit with less than unanimous conviction and commitment. Privately, many delegates were sceptical about the prospects for global eradication, although all were basically in agreement that better smallpox control would benefit both the countries in which smallpox was endemic and those subject to importations of the disease.
Preparations for Initiating the Intensified Programme, 1966
By January 1966, when the Executive Board decided to recommend a special allocation for an intensified smallpox eradication programme, the global programme had been in progress for more than 6 years, but few WHO personnel had been assigned to it. The smallpox eradication staff consisted of a medical officer and a secretary in Geneva; 2 recently assigned African intercountry advisers, in Kenya and in Liberia; and 3 advisers assigned at country level, in Afghanistan, Bolivia and Mali. With little known about the status of smallpox in the endemic countries or their prospective programmes or needs, major efforts were required to mount a fully fledged global programme capable of effectively utilizing the US$2 415 000 provided in the budget.
In February 1966, immediately after the Executive Board session, the Director-Genera1 sent letters to each of the WHO regions indicating the possibility that additional funds specifically for smallpox eradication might be made available. Each region was requested to develop provisional plans for 1967-1 968, based on a larger budget, and to identify their needs for vaccine, advisory personnel, supplies and equipment. In the Americas, a regional adviser was appointed, who immediately began discussions with the authorities in Brazil as well as with those of Argentina, Colombia, Ecuador and Peru, in which it was thought that programmes would be required.
Meanwhile, at CDC, Henderson was assembling staff, procuring equipment and working out plans with 16 countries of western and central Africa so as to permit programmes to begin there in January 1967 (see Chapter 17).
Late in May 1966, with the Health Assembly’s formal approval of the programme and budget, activities steadily increased. Henderson was rectuited to serve as chief of the Smallpox Eradication unit, a post he was to assume in November; a second medical officer, Dr Stephen Falkland, was temporarily assigned through transfer from another unit in WHO, and an administrative officer was assigned from the malaria programme. One or two consultants were recruited to visit countries in each of the 4 WHO regions in which smallpox was present to encourage them to develop national programmes.
Within the Organization, however, reservations about the wisdom of smallpox eradication were widespread and were reflected in administrative actions. The DirectorGeneral, in a meeting with regional directors immediately after the Health Assembly, privately expressed his doubts about the feasibility of eradication and cautioned them about imposing on countries a special programme like that for malaria eradication. As he saw the situation, the prospects for success depended on progress in the development of each country’s basic health services. It was not surprising, therefore, that a memorandum, dated 10 August 1966, was sent to all regional offices by two Assistant Directors-General, Dr Kaul and Dr John Karefa-Smart, which stated:
“The establishment of permanent basic health services should be given the highest priority since it is a prerequisite for the success of the smallpox eradication programme in any area and you should be prepared to consider providing from the smallpox eradication programme resources, such assistance as may be required for developing and strengthening basic health services in the area where the campaign is launched.”
This policy statement effectively authorized the use of smallpox eradication funds to meet almost any of the all but inexhaustible needs of the basic health services.
In conformity with their belief that the smallpox eradication programme called for little more than the proper distribution of resources, senior WHO staff in July 1966 substantially reduced the Headquarters smallpox eradication budget. Funds for staff travel were reduced from US$6400 to US$2400, then sufficient to permit a total of approximately 3 trips of 21 days each; funds for consultants were cut so as to allow for only 3 man-months instead of 23; and funds for convening a meeting of a scientific group were cancelled. The research budget was reduced from US$30 000 to US$12 000 and responsibility for administering these funds was assigned to the Virus Diseases unit. Dr RaSka vigorously objected to the changes and argued that travel funds should be increased to US$14 000 and that a medical officer and 2 secretaries should be added to the personnel complement to create a unit staff of 7 (3 medical officers, an administrative officer, a technical assistant and 2 secretaries). The funds were eventually restored and the increase in personnel was approved when, in a meeting with the Director-General, Dr Kaul and Dr RaSka, Henderson expressed doubt that he could manage a global programme of such magnitude without the resources stipulated and proposed to withdraw his candidature for the post of unit chief. Although that possibility was considered, Dr RaSka eventually prevailed.
CDC staff, meanwhile, were working intensively to launch the AID-supported programme in western and central Africa. By the end of 1966, agreements had been signed with most of the countries concerned, a staff of 50 had been recruited and trained, operations manuals had been prepared, and supplies and equipment had been procured. The CDC training programme concluded with an address, given by special invitation, by the Director-General of WHO and delivered by telephone on 31 August. His comments are noteworthy for two points. First, he stressed his concern that another special programme like that for malaria eradication might be developed: “You must jointly ensure that the smallpox eradication programme is a coordinated effort within the general health services of the country, and not a separate, isolated activity.” Secondly, he stated : “The programme of eradication is planned over a period of 10 years”, a goal which had been mentioned in the Health Assembly although not stated in the formal resolution. Uncertainty about the eventual outcome of the programme, however, subsequently led to instructions to omit any reference in official documents to the 10-year target date.
The attitudes of the WHO regional directors ranged from the interested, in the Americas (Dr A. Horwitz) and Eastern Mediterranean (Dr A. H. Taba), to the reluctant in the African Region, and to the frankly negative in the South-East Asia Region. In a letter to Dr Kaul (19 July 1966), the Director of the Regional Office for South-East Asia wrote: “In our view, on account of the organizational and administrative weakness of health services and serious socio-economic as well as financial difficulties, smallpox eradication is not likely to be achieved in the countries of this Region in the near future.”
A programme which was rudimentary at best at the beginning of 1966 saw a quantum change in the level of activity by the end of the year. Henderson, Arita and Dr Falkland in the Headquarters unit were joined by Dr G. P. Nikolaevskij, a physician from the USSR, and Mr John Copland from the USA, who was to serve as the unit’s administrative officer over the succeeding decade. Programmes in 16 countries of western Africa were about to commence ; plans of operations had been signed with Brazil and the Democratic Republic of the Congo (Zaire); Dr Ehsan Shafa had been appointed Regional Adviser on Smallpox Eradication for the Eastern Mediterranean Region, and Dr Bichat Rodrigues in the same capacity for the Americas; and discussions had begun with a number of countries in the Eastern Mediterranean and South-East Asia Regions regarding eradication programmes.
Voluntary contributions to the programme during 1966 continued to reflect the general lack of interest among donors. Apart from vaccine donated by Switzerland, contributions in cash and in kind from Greece, Jordan, Kenya, Monaco, Nepal, the Netherlands, the Philippines, Thailand and Zaire were valued at only US4117 632.
As the Intensified Programme commenced operations, however, the areas with endemic smallpox were actually substantially smaller than they had been in 1959 (see Table 9.6). The information now available indicates that in only 31 countries or territories, with a total population of 1 078 775 000, was smallpox endemic in early 1967, compared with 59 in 1959. Nevertheless, the problem remained formidable.
SUMMARY
Since smallpox was such a good candidate for global eradication, it is surprising that the commitment to undertake such a programme was so long delayed and, even after being accepted by the World Health Assembly, so ill-supported both within WHO and by most Member States. In part, this derives from the historical roots of human disease eradication programmes originating, as they did, in vector control programmes, which continued and eventually culminated, in 1955, in the vast and costly global effort to eradicate malaria. Many of the leading figures in international public health during the 1960s had spent their formative years in vector control programmes, and it was with these that they were the most conversant and felt the most comfortable. Among the most important of the experts concerned were clearly Dr Soper, Director of the Pan American Sanitary Bureau for 12 years, and Dr Candau, Director-General of WHO for 20 years. Reluctance to undertake global smallpox eradication may also have originated, in part, from concern about the chances of such a programme being successful in Africa, where, in most areas, the transport, communications and health services infrastructures were poorly developed. Although malaria eradication had been undertaken with alacrity in 1955, and had been referred to as “global” in scope, Africa south of the Sahara had not been included in the programme. Perhaps of equal importance was an unstated acceptance of smallpox as an inevitable, entrenched disease for which vaccination, a permanent feature of public health practice for more than a century, would always be required. Such, at least, was found to be the widely held belief, even after global eradication had been achieved and documented.
The first to call for regional smallpox eradication was the Pan American Sanitary Organization in 1950, and although its programme was reasonably successful as far as it went, it was not actively promoted or diligently pursued. In part, this reflected Dr Soper’s preoccupation with eradication of the Aedes aegypti mosquito and, later, with malaria eradication. The lack of vigour can also be attributed to the fact that the largest endemic country was Brazil, in which the prevailing mild variola minor was not an important public health problem.
The proposal by the USSR in 1958 that a global programme to eradicate smallpox should be undertaken represented a new departure rather than, as some have believed, a logical extension of the regional programme in the Americas. Professor Zhdanov, the author of the proposal, reasoned correctly that smallpox eradication was a far more attainable objective than the eradication of malaria and that such a programme would benefit all countries, including his own, which shared a long border with endemic Asian countries.
Between 1959 and 1966, lack of interest on the part of WHO in smallpox eradication and the perceived lack of progress in the programme must be attributed, in large measure, to WHO’s preoccupation, as well as that of many Member States, with malaria eradication. Over this period, the persistent advocacy of smallpox eradication by the USSR in the World Health Assembly served to sustain interest in such a programme on the part of Member States, even though the Organization assigned few resources to it. Renewed interest in the programme was stimulated by the commitment of the USA in 1965 to support regional smallpox eradication programmes in a contiguous group of countries in western and central Africa, a decision which was less a product of rational policy analysis than a reluctantly accepted byproduct of a regional measles vaccination campaign.
The decision by the World Health Assembly in 1966 to intensify the effort to eradicate smallpox was made with grave reservations. Eradication, as a concept in disease control, had largely been discredited, and the Director-General himself, believing smallpox eradication to be an unachievable objective, viewed the programme as one which could serve only further to undermine the Organization’s credibility. Potential contributors to WHO’s voluntary fund were demonstrably no more enthusiastic, and UNICEF, discouraged by the failure of the costly malaria eradication campaign, refused to support the programme as a matter of policy.
The Intensified Smallpox Eradication Programme was thus conceived in an atmosphere of sanguine rhetoric overshadowed by real doubts abouts its ultimate success.