Chapter 12:
South America

INTRODUCTION
When the Intensified Programme began, in 1967, South America presented the best prospects in the world for the eradication of smallpox. By that time, a single country, Brazil, was reporting almost all cases in the Americas (Table 12.1); and there was little reason to suppose that important areas of endemicity existed elsewhere, although the possibility that unreported foci of smallpox were present in other countries would have to be investigated . Brazil, although a very large and populous country, was small by comparison with the extensive endemic regions of Africa and Asia. Moreover, its relatively advanced health system and its wide-reaching transport and communications network offered promise that an effective programme could be conducted.
In the global strategy of eradication, it was logical to give priority to interrupting transmission in South America. Once that had been achieved, it should be easy to keep the continent free of smallpox because the risk of a case being imported from as far away as Africa or Asia was small. The resources initially available for the programmes in South America could then be released for use elsewhere.
A regional programme for the eradication of smallpox in the Americas had begun in 1950 pursuant to a resolution of the XIII Pan American Sanitary Conference (Pan American Health Organization, 1971a). This action was strongly supported by the Director of the Pan American Sanitary Bureau (see box), Dr Fred L. Soper, a vigorous proponent of the concept of eradication (Pan American Sanitary Organization, 1949). The decision was reached only 2 years after the commencement of the Bureau’s programme to eradicate Aedes aegypti, the mosquito vector of yellow fever, from the Americas. Dr Soper considered the latter action to be a “landmark in international health . . . the first official recognition by an international health organization of regional responsibility for the solution of a health problem involving an entire continent” (Soper, 1951). The Pan American Health Organization (PAHO) assisted many countries in the development of laboratories to produce freeze-dried smallpox vaccine and many undertook mass vaccination campaigns, some with bilateral assistance.
By 1959, smallpox transmission had been interrupted in all but 5 countries of South America (Table 12.1), of which 3—Brazil, Colombia and Ecuador—were recording large numbers of cases every year. Between 1950 and 1959, the two latter countries had embarked on national programmes to attempt to eliminate the disease. In 1955 Colombia initiated a systematic mass vaccination campaign, which was completed in 1961 . Ecuador began a similar campaign in 1958, which likewise ended in 1961. Bolivia, which recorded 7 cases in 1959, had just completed a 2 year mass vaccination campaign and appeared to be on the verge of interrupting transmission (Frederiksen et al ., 1959). Argentina, with comparatively high levels of vaccinial immunity throughout the country as a result of intensive vaccination campaigns, reported only 36 cases in 1959, primarily in provinces adjacent to Brazil.
The Pan American Health Organization and the WHO Regional Office for the Americas
The origin of the Pan American Sanitary Organization (later known as the Pan American Health Organization—PAHO) dates from December 1902, when, at the First General International Sanitary Convention of the American Republics, a series of agreements pertaining to quarantine regulations for the Americas were adopted. To oversee their implementation, to receive reports from governments and to staff periodic meetings, a permanent executive body was created—the International Sanitary Bureau, subsequently renamed the Pan American Sanitary Bureau. Over the next 45 years, the Bureau's activities were largely concerned with this function. Its modest budget was covered by an annual subvention from each of its Member governments.
By virtue of a formal agreement with the World Health Organization, signed in 1949 and approved in the same year by the Second World Health Assembly, the Pan American Sanitary Bureau undertook to serve as the WHO Regional Office for the Americas, but, in deference not only to tradition but also to the continued existence of the Pan American Sanitary Organization, it would retain its own name and identity (Howard-Jones, 1980).
The regular budget of PAHO is financed from two sources : approximately one-third of the total is covered by an allotment from WHO deriving from the contributions of the Organization's Member States throughout the world ; the remaining two-thirds are funded by the Member countries of PAHO.
Table 12.1: Numbers of reported cases of smallpox in the Americas, 1959-1971a
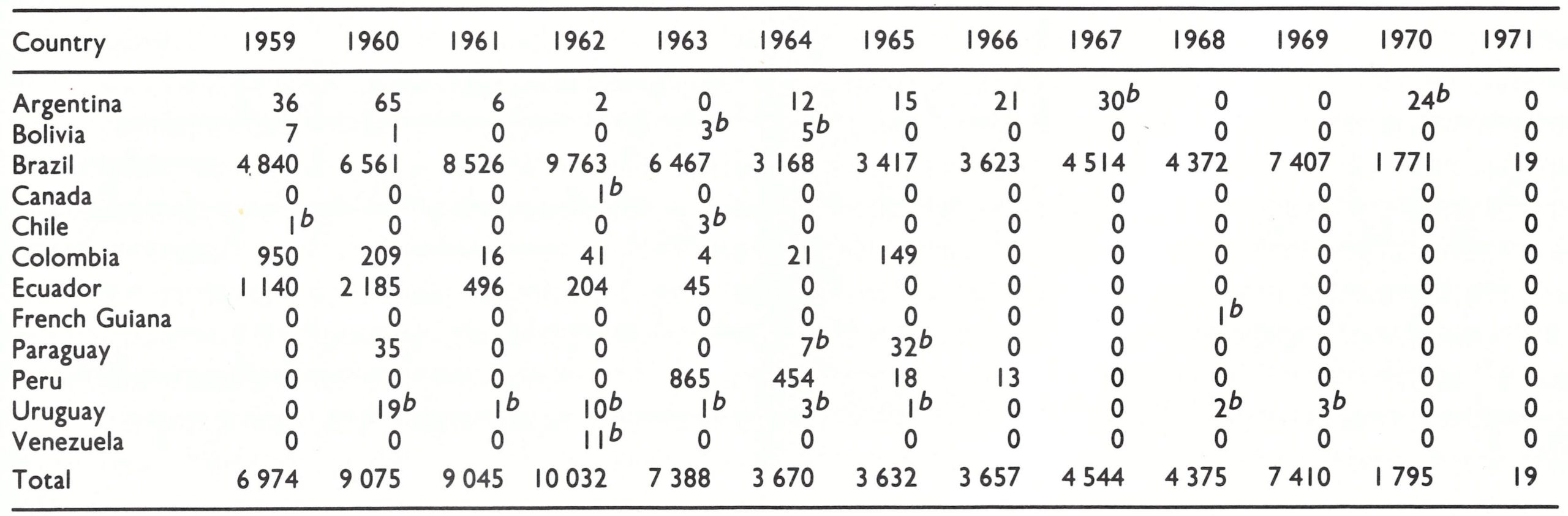
a Data from the WHO Smallpox Eradication unit based on special reports from governments and reviews of national data. The numbers differ slightly from some official reports published elsewhere (World Health Organization, 1980).
b Cases and outbreaks known or believed to have been imported.
Between 1959 and 1966, Argentina, Bolivia, Colombia and Ecuador interrupted endemic transmission . Few cases were detected in other countries, except Brazil and Peru, and most of those could be traced to importations from Brazil . In 1963, Peru, which had last recorded cases in 1954, experienced a serious setback when a major epidemic developed in Loreto Department in the Amazon basin adjacent to Brazil . Before detection, the outbreak had spread widely in the Amazon area and into the Andes and cases had occurred in Lima, the capital . A repeat vaccination campaign interrupted transmission in 1966.
By 1967, Brazil appeared to be the only endemic country in the Americas (Fig. 12.1). Uncertainty existed, however, because Brazil shares a border with all but two countries of South America and most border areas are in remote regions of the Amazon basin, in which there were few health centres to report cases if they did occur. The fact that all known cases were of the mild variola minor type made it less probable that outbreaks and cases, if present, would be detected and reported . However, in these sparsely populated areas, it seemed unlikely that the foci—if indeed they existed—would be extensive.
The eradication of smallpox in South America thus appeared to be a less formidable task than in other endemic regions of the world; primarily, it implied the interruption of transmission in Brazil. Indeed, of the continents in which smallpox had been endemic in 1967, South America was the first to interrupt transmission. The last known case occurred in the city of Rio de Janiero on 19 April 1971.
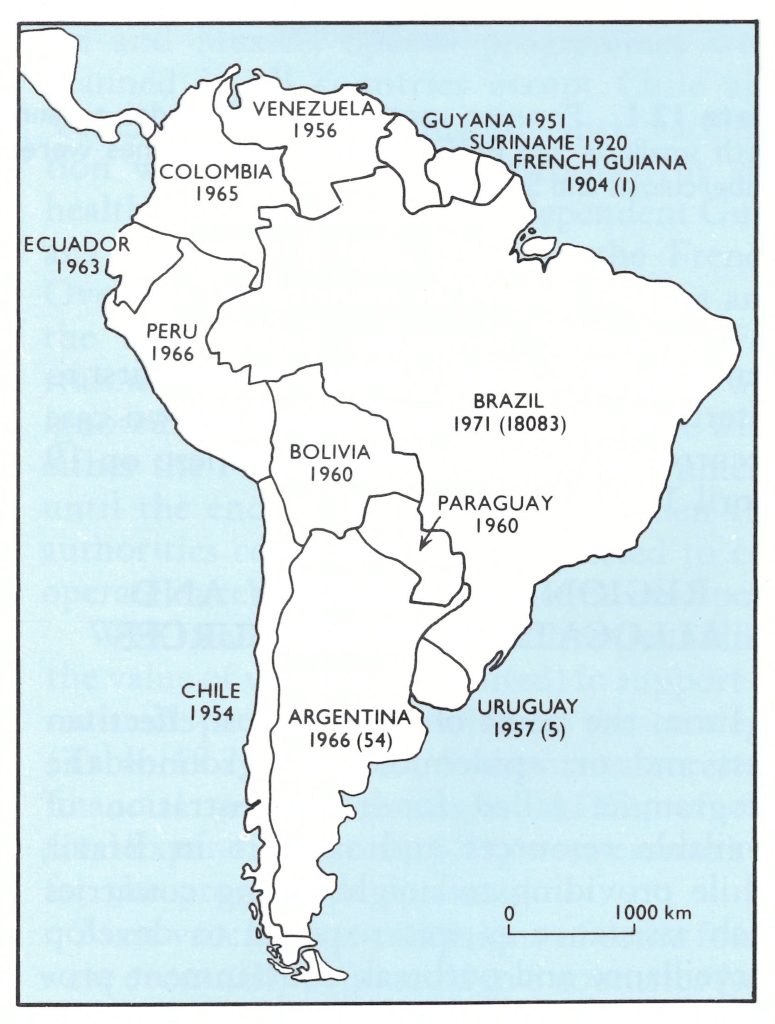
Fig. 12.1. South America: year of last endemic case of smallpox and number of reported cases occurring between 1967 and 1971 (figures in parentheses). The year shown for each country is that in which the continuing transmission of smallpox is believed to have ceased. Cases recorded in subsequent years are known or thought to have resulted from importations. Transmission in Peru ceased in 1954, but smallpox was reintroduced in 1963 and persisted through 1966.
Variola Major and Variola Minor
In most parts of the world in 1967, variola major was the variety of smallpox which was endemic. The much less severe variola minor was present in only 3 areas : South America, southern Africa and the Horn of Africa . Variola major had been endemic in most parts of South America since the 16th century, but in the early 1900s it had begun to be replaced by variola minor . The last known case of variola major occurred in Ecuador in 1962.
The differences in severity between the two forms of smallpox resulted in different responses by health authorities and patients when outbreaks occurred . Variola major was widely feared and its occurrence usually induced health authorities to respond vigorously with vaccination campaigns. In contrast, variola minor often tended to be regarded in the same light as measles or chickenpox. In fact, the disease was called alastrim in South America rather than smallpox. Patients with variola minor, instead of being confined to bed by the severity of the toxaemia, as with variola major, often remained mobile and thus were in contact with a greater number of susceptible persons . On the positive side, vaccination, even if performed long before, protected against variola minor more effectively than against variola major. The South American programme must be seen in this setting.
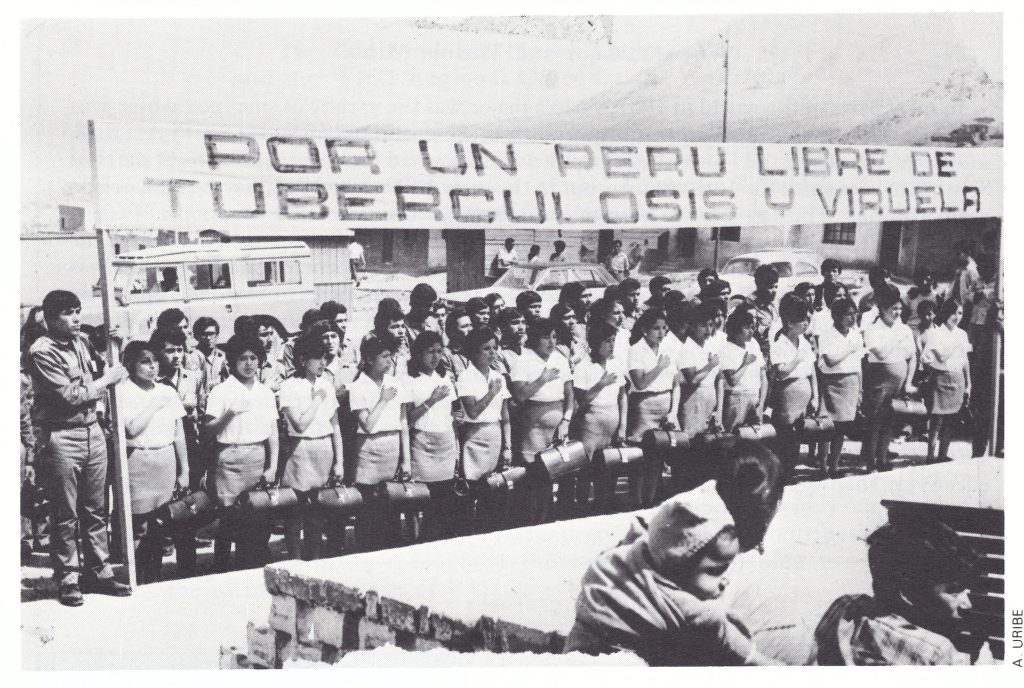
Plate 12.1. Peruvian vaccinators pose under a banner at the conclusion of a training programme in 1968. Both smallpox and BCG (tuberculosis) vaccines were given; hence the banner reading “For a Peru Free of Tuberculosis and Smallpox”.
REGIONAL STRATEGY AND ALLOCATION OF RESOURCES
From the point of view of cost-effectiveness and on epidemiological grounds the programme called for a concentration of available resources and support in Brazil, while providing to neighbouring countries such assistance as was required to develop surveillance and outbreak containment programmes in contiguous areas . If extensive endemic areas were found in neighbouring countries, additional resources could be provided . A more costly but arguably more reasonable approach would have added systematic vaccination campaigns in adjacent high-risk areas to create a partial barrier against the spread of smallpox . However, the strategy evolved along completely different lines.
Simultaneous mass vaccination campaigns throughout South America were proposed. The rationale is summarized in a report of the PAHO Secretariat to the XVII Pan American Sanitary Conference :
“. . .it is possible to eradicate smallpox in the Americas by immunizing the population at risk, within a relatively short time . . . although good coordination of all health services can be achieved for the smallpox eradication program or national smallpox vaccination programs, the same cannot be said of maintenance programs . This underlines the need to carry out smallpox vaccination programs simultaneously in as short a time as possible . If this is done and smallpox disappears, and good epidemiological surveillance services are established, then the intervals between revaccination may be gradually increased . . .” (Pan American Health Organization, 1967).
Conceptually, the strategy of mass vaccination did not differ from eradication programmes of previous decades . Epidemiological surveillance was considered to be important only after smallpox had disappeared. The traditional approach was deeply ingrained and change was stubbornly resisted both by PAHO staff and by national programme directors. In Brazil, the detection of cases and the containment of outbreaks were introduced in some states only in 1969, and not until 1971 were these measures applied on a country-wide basis.
Table 12.2: Latin America : WHO and PAHO expenditure for smallpox eradication, 1953-1971 (thousands of US$)a
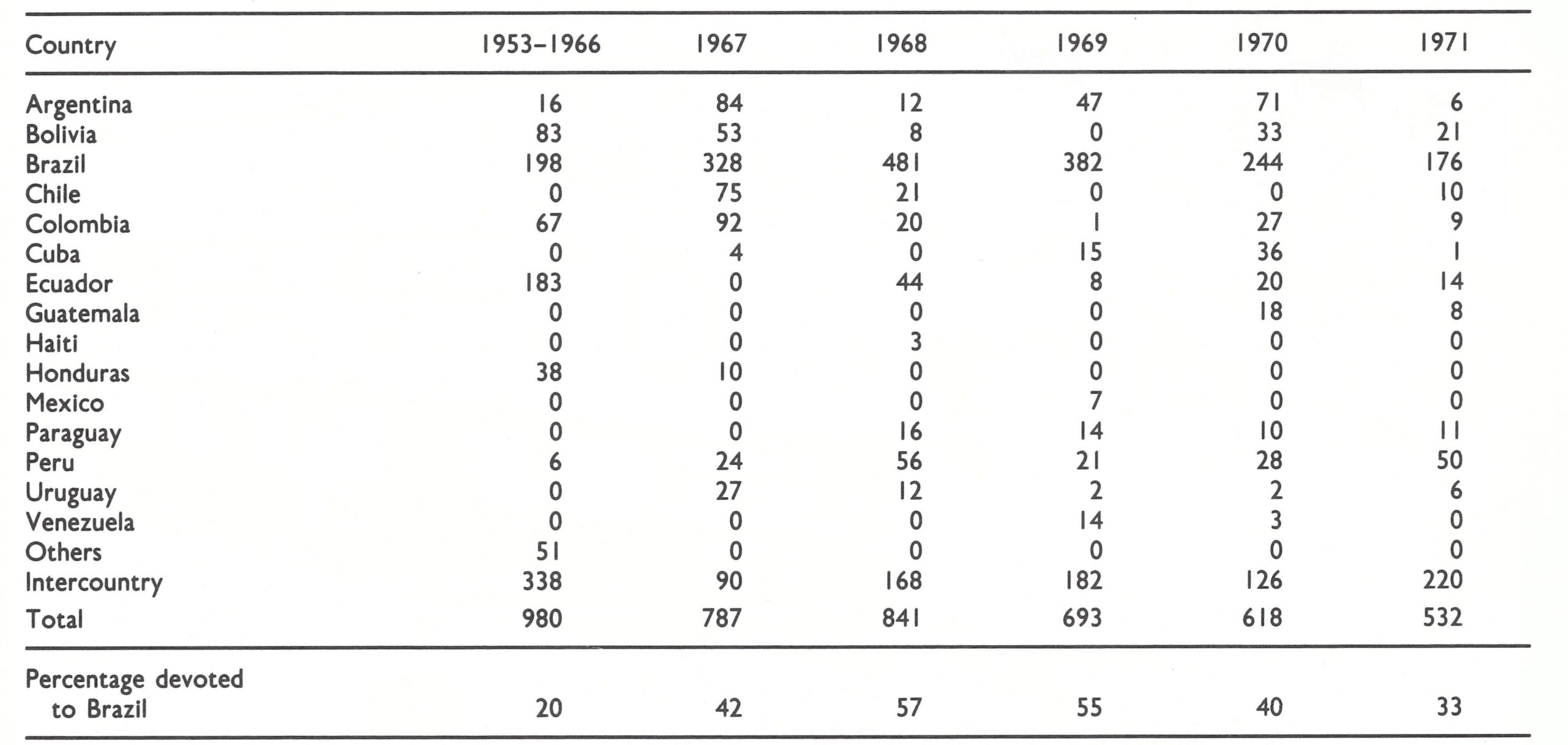
a From WHO and PAHO financial records and vaccine distribution records
The provision in the plan to continue revaccination campaigns after the disappearance of smallpox may seem paradoxical, but it reflected the prevailing scepticism about the feasibility of eradication . Many health officials at that time believed that smallpox eradication could be achieved only if virtually all persons everywhere were vaccinated and periodically revaccinated . Experience with programmes for the eradication of malaria had shown that it was impossible to reach entire populations ; for example, Indian tribes in the Amazon were rarely contacted by civil or health authorities. The concept that eradication could be achieved by stopping transmission of the virus without requiring everyone to be vaccinated was difficult to accept.
Because of the belief in the need for simultaneous mass vaccination throughout the continent, PAHO signed agreements with numerous countries—Argentina, Bolivia, Brazil, Chile, Colombia, Cuba, Paraguay, Peru, Uruguay and Venezuela—late in 1966 and early in 1967 which called for national vaccination campaigns. Some financial support was also provided by PAHO in certain years to Ecuador, Guatemala, Haiti, Honduras and Mexico. Special programmes were planned in all countries except Chile and Venezuela (in which maintenance vaccination was expected to be performed by the health services), the newly independent Guyana (formerly British Guiana), the French Overseas Department of French Guiana and the then Dutch colony of Suriname. For reasons which are not clear, Guyana was ignored and no special contact was made with either the French or the Dutch government until the end of the programme, when the authorities concerned were requested to cooperate in certifying the absence of smallpox.
WHO and PAHO expenditures (including the value of vaccine distributed) in support of national programmes reflected the strategy (Table 12 .2). In 1967, 9 countries received financial support through PAHO; of the total expenditure, only 42% were earmarked for the programme in Brazil.
Mass vaccination campaigns of some form were eventually conducted in 8 countries (see box). The data available for these campaigns are incomplete, consisting primarily of numbers of vaccinations reported to have been performed in different areas. Few campaigns undertook more than perfunctory field assessments to determine the proportion of persons actually vaccinated and the proportion of vaccinations which were successful. Areas in which reasonably extensive mass campaigns were conducted are shown in Fig. 12.2.

Plate 12.2. Peru conducted an extensive vaccination campaign throughout the departments of the Amazon basin where the risk of importations of smallpox from Brazil was greatest. In these areas, the teams relied heavily on boats for transport, like the specially assigned launch shown here.
Fig. 12.2. South America: areas in which systematic mass vaccination programmes were completed, 1967-1972.
The total number of vaccinations reported to have been performed in each of the countries, both in mass campaigns and by the established health services, is shown in Table 12.3.
Only Chile, French Guiana, Paraguay and Suriname did not conduct some type of special vaccination campaign, and, with the exception of Paraguay, there was little motivation or need for them to do so . Chile had no border with Brazil and was thus at minimal risk of imported smallpox, while French Guiana and Suriname, with small populations mainly settled along the coast, had scarcely any communication with Brazil.
Paraguay, on the other hand, sharing a border with Brazil and receiving many travellers from that country, was at unusually high risk. Because of fiscal constraints, however, it was unable to carry out a special programme. A mass vaccination campaign had been conducted between 1958 and 1960, during which 86% of the population was said to have been vaccinated. After that time, routine vaccination was offered in health centres. During May and June 1971, a WHO—Paraguay team conducted a search for cases and also performed scar surveys in several areas to assess the level of immunity (Wkly epidem. rec., 1971a ; Table 12.4). No cases of smallpox were found, and 78.5%, of those surveyed bore vaccination scars. It was apparent that the existing health services had done reasonably well in sustaining immunity. A costly special campaign might have improved the levels of immunity, at least among young children, but, as was apparent in retrospect, it was not needed.
Table 12.3: South America: population and number of reported smallpox vaccinations, 1967-1972 (thousands)a
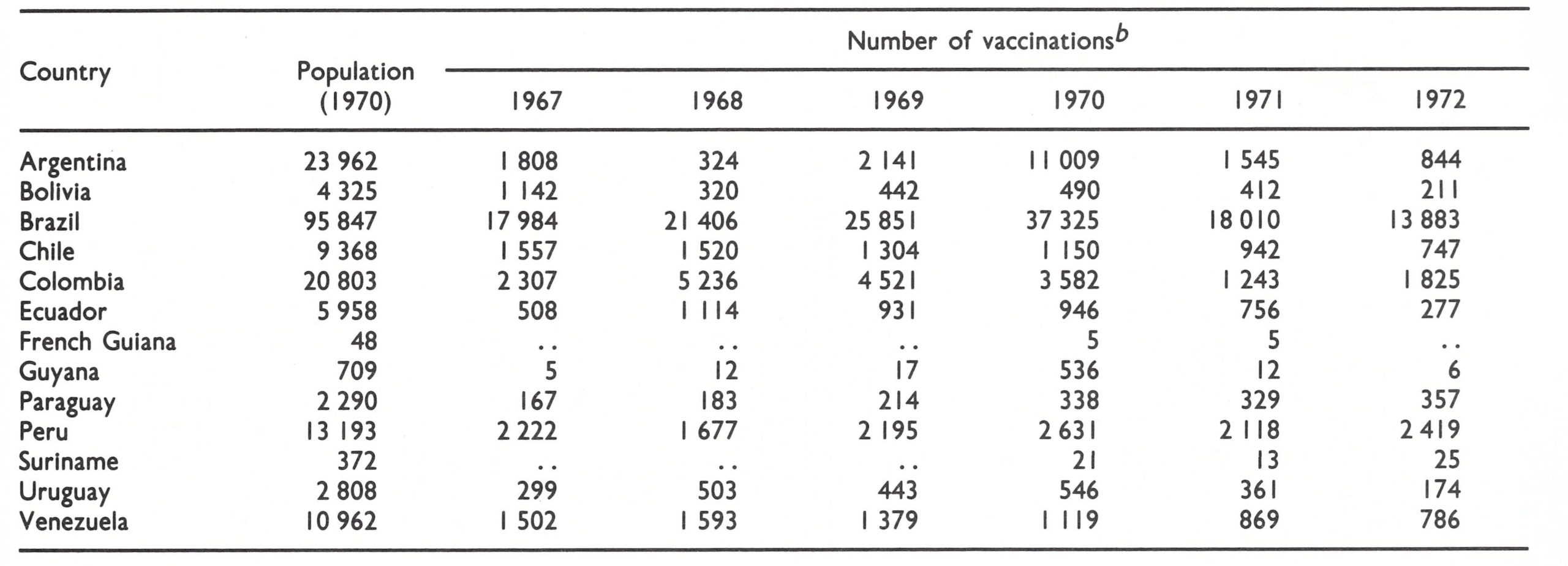
a From Rodrigues (1975); population figures from United Nations (1985) . The number of vaccinations reported annually by each country Includes both those performed during special mass vaccination campaigns and routine vaccinations given In hospitals, clinics and other health units.
b.. = Data not recorded.
Table 12.4: Paraguay : proportion of persons, by age group (years), with vaccination scars in 4 districts, 1971a

a From WHO/SE/72.38.
Information about smallpox in South America from 1967 to 1971, other than in Brazil, is fragmentary. Little was done until 1971 to improve reporting systems, and the investigation of cases was often perfunctory. Uruguay promptly detected and documented 4 importations in 1968 and 1969, and French Guiana similarly dealt with 1 importation in 1968, but these were the exceptions. In Argentina, nothing is known of the 30 reported cases in 1967, which may have been importations, mistaken diagnoses or a combination of both. Argentina’s outbreak of 24 cases in 1970 was actually discovered and investigated by Brazilian teams, who subsequently informed the Argentine health authorities of the occurrence . An episode in Colombia illustrates that even cases diagnosed as smallpox by health staff were sometimes not reported to the national authorities. In 1971, during a special search for possible undetected cases in the Amazon basin, a WHO—Colombia team was informed by a hospital director of 4 cases of smallpox which had been diagnosed in November 1970 in a border town. No report of these cases had been forwarded. The team discovered that the cases concerned were actually misdiagnosed cases of chickenpox, but no one knows how many other outbreaks may have been detected and not reported during earlier years in this and other parts of the Amazon basin. That these isolated regions contained many susceptible individuals was documented by the WHO—Colombia team, which conducted a scar survey in a suspect area. Less than 20%o of the children under 5 years of age had ever been vaccinated ; among those aged 5-14 years living in rural areas, only half had previously been vaccinated. From these and other data collected during the period 1971-1973, it was concluded that smallpox had not been sustained in the sparsely populated Amazon border areas. However, neither surveillance not high levels of vaccinial immunity played a significant role in the attainment of this smallpox-free status.
Special Vaccination Campaigns Between 1967 and 1972 in South America, excluding Brazil
Argentina (1970 population, 23 962 000): Campaigns were conducted on a province-byprovince basis with high levels of vaccination coverage in some provinces and less than 50% in others. The first to be vaccinated were the inhabitants of some provinces in the north, bordering on Brazil, and of provinces in the far south of the country. Subsequent provincial campaigns followed in no logical sequence; no campaign was conducted in the capital or the vast area constituting Buenos Aires Province. In all, some 7.8 million vaccinations were reported to have been performed during the campaign.
Bolivia (1970 population, 4 325 000): Bolivia had conducted a mass campaign in 1957-1958 during which 2.4 million persons had been vaccinated, a figure equivalent to about 75% of its population at that time. During a repeat campaign, begun in 1963 and concluded at the end of 1968, 3.7 million people were vaccinated, a figure equivalent to 81% of the population. A third campaign was initiated in 1969, with most of the resources concentrated in 6 of the country's 8 departments (those adjacent to Brazil). The number of people reported to have been vaccinated was equivalent to 82% of the population of the 6 departments concerned.
Colombia (1970 population, 20 803 000): Between August 1967 and the end of 1972, campaign staff performed 13.2 million vaccinations in the highland areas. No campaigns were conducted in the Amazon basin adjacent to Brazil, the area at greatest risk.
Ecuador (1970 population, 5 958 000): During vaccination campaigns conducted throughout the country, 5 million vaccinations were recorded between 1967 and 1972. A survey conducted in 45 localities in 1972 revealed the presence of vaccination scars in 41 % o of individuals under 5 years of age, in 85% of those aged 5-14 years, and in 88% of those aged 15-19 years.
Guyana (1970 population, 709 000) : A mass campaign was conducted in 1970 during which 536 000 persons were reported to have been vaccinated.
Peru (1970 population, 13 193 000) : A special campaign in Peru was conducted in 1967-1972, primarily in the eastern departments of the country bordering on Brazil and in other departments considered to have the least adequate health services. During the campaign, 5 .6 million vaccinations were reported to have been performed.
Uruguay (1970 population, 2 808 000): Personnel of the existing health facilities performed most of the vaccinations, recording 1.3 million in all, during the period 1967-1971. An additional 650 000 vaccinations were given in the course of special campaigns. Until 1971 the thermolabile liquid vaccine rather than the freeze-dried product was used and many of the vaccinations were thought to have been unsuccessful.
Venezuela (1970 population, 10 962 000): A well-organized and well-evaluated vaccination campaign was conducted throughout most of Bolivar State from August to November 1970 and from April to June 1971. This was a high-risk area bordering on Brazil in which the population was scattered and access to health facilities was limited. Among the 289 000 residents, a vaccination coverage of 91.6 % was achieved.
THE PROGRAMME IN BRAZIL
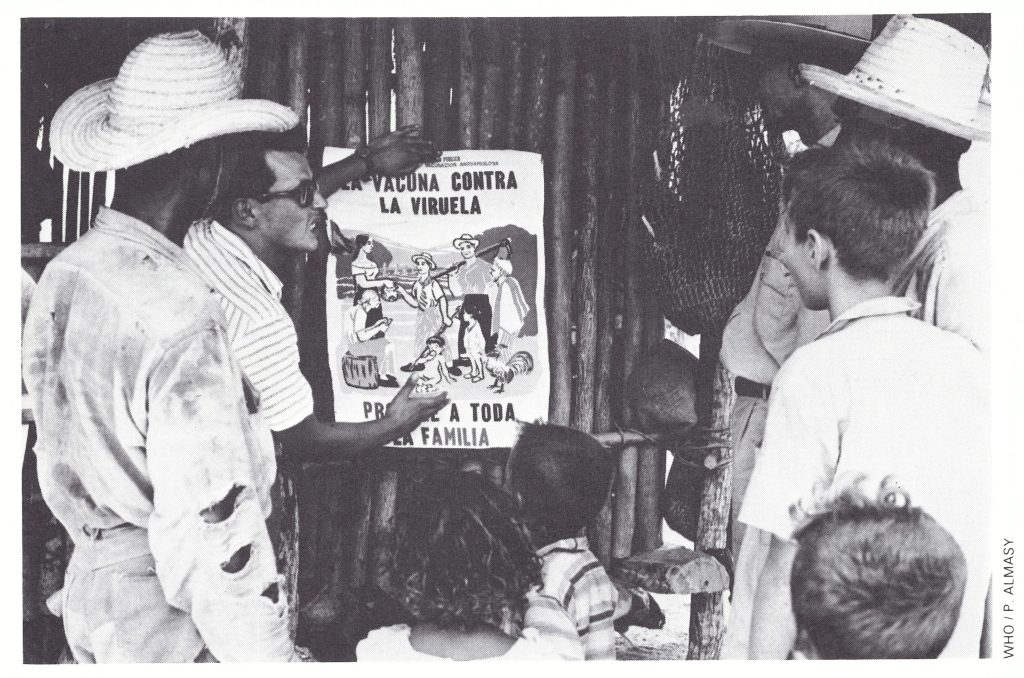
Plate 12.3. Posters were produced in many countries. This one in Colombia says, “Smallpox vaccine protects the whole family”.
During the 1950s Brazil, unlike other countries in the Americas, conducted no nation-wide vaccination campaigns. Local authorities, according to their interest and motivation, vaccinated people in cities and towns when there were outbreaks, but no programme was carried out in the country as a whole. Between 1950 and 1960, comparatively few cases of smallpox were recorded for a country so populous, the number ranging from a low of 749 in 1950 to a high of 6561 in 1960. However, reports of cases at that time were received from only a few rural health units operated by a special government service and from some hospitals in state and territorial capitals . In fact, only a single city, Sao Paulo, had a reasonably comprehensive reporting system (Morris et al .,1971). Thus, the actual number of cases was almost certainly many times greater than that recorded.
In 1958, Brazil had joined other PAHO Member States in adopting a resolution of the XV Pan American Health Conference to eliminate smallpox from the Americas. This action was reaffirmed in 1961 by the Charter of Punta del Este, which called on all governments in the Americas to take immediate action “to eradicate malaria and smallpox from the Hemisphere” (Pan American Health Organization, 1973). Shortly afterwards the Oswaldo Cruz Institute in Rio de Janeiro began the manufacture of freeze-dried vaccine.
In 1962, Brazil launched a national campaign against smallpox (Rodrigues, 1975). By the end of 1965, 24 million vaccinations had been performed in a population of 84 million. The initiative for the campaign rested with the authorities of the separate states and territories, few of which were strongly motivated. Not many of the staff were employed at the federal level and only one of them travelled to the field to assist states in developing and monitoring programmes. The campaign was considered to have been satisfactorily executed in no more than 4 of the 27 states and territories. The number of reported smallpox cases throughout the country decreased from 9763 in 1962 to 3623 in 1966. However, because the reporting system had shown little improvement over this period, the decreasing incidence figures meant little.
Interest in the programme heightened in 1965 with the introduction of a new vaccination technique—the jet injector gun. With assistance from PAHO, a special pilot programme was undertaken in the northern Amazonian territory of Amapa by a combined Brazilian-United States Communicable Disease Center team. The team members evaluated the cost and efficacy of vaccination with jet injectors in relation to vaccination utilizing the conventional multiple pressure technique (Millar et al.,1971) (Table 12.5). With the use of the jet injector an average of 259.5 persons were vaccinated per worker-day, compared with a corresponding figure of 68.4 when the multiple pressure technique was employed. The cost per vaccination was Belema Macapab US$0.022 with the jet injectors and US$0.067 using multiple pressure vaccination. Moreover, the jet injectors produced a higher proportion of successful vaccinations. The members of the group responsible for the trial were enthusiastic and recommended a renewed effort to eradicate smallpox. They proposed that a federal director and staff should be appointed to help to organize and execute state vaccination campaigns throughout Brazil, and that jet injectors should be provided in order to complete the campaigns, as they stated, “in months instead of years”. It was also recommended that state personnel should immediately be selected and trained in the organization of surveillance programmes, a recommendation that was sound in principle but destined to be ignored.
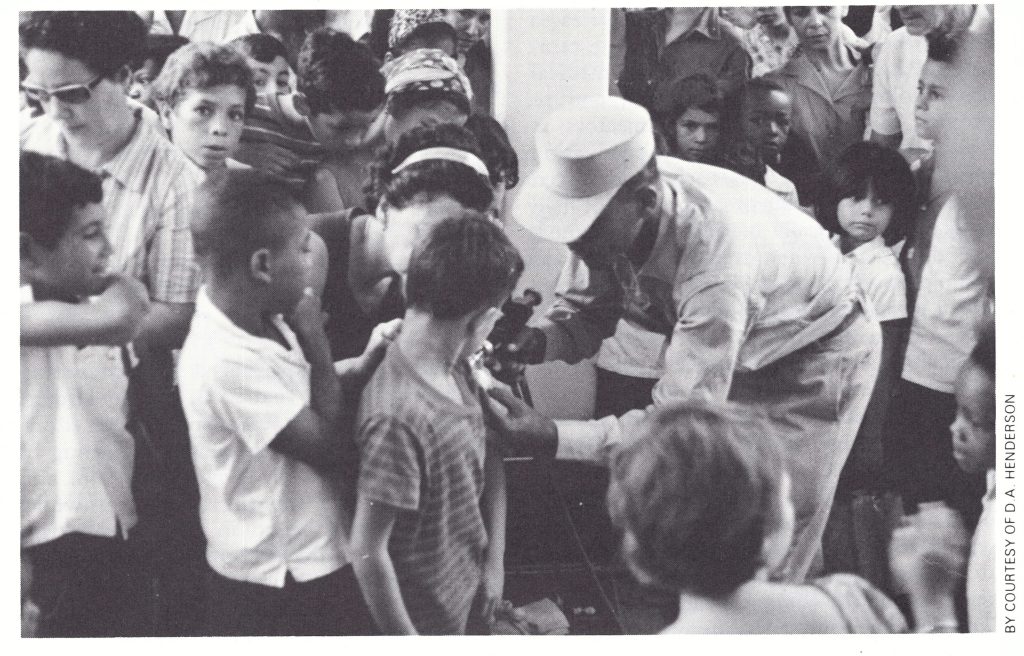
Plate 12.4. The demonstration in 1965 of the efficacy of the jet injectors provided an important stimulus to Brazil to undertake an effective national smallpox programme. This device could vaccinate as many as 1000 persons each hour.
Table 12.5: Brazil : comparison of vaccination campaigns using the multiple pressure technique (Belem) and the jet injector (Macapa)

a Door-to-door vaccination.
bVaccination at established sites and by mobile units, as well as door-to-door.
Smallpox Cases in the Americas, Excluding Brazil, after 1966
Outside Brazil, only 60 cases of smallpox were reported in the Americas after 1966. All were in areas adjacent to Brazil. Except for 30 cases in northern Argentina in 1967, when sources of infection were not identified, all could be traced to importations. Because surveillance was poor throughout the areas neighbouring Brazil, other importations probably occurred but did not result in sustained transmission.
DEVELOPMENT OF THE BRAZILIAN NATIONAL PROGRAMME, 1966
The demonstration by the Amapa team of the efficacy of the jet injector and the decision in May 1966 by the Nineteenth World Health Assembly to undertake an intensified global eradication programme persuaded the Brazilian authorities to begin a new national programme.
On 31 August 1966, a federal decree was promulgated which required an intensification and coordination of public and private activities throughout the country to combat smallpox in all its clinical forms with a view to achieving the eventual eradication of the disease . The aim was to conduct a mass vaccination campaign among the population at large, state by state . It was expected that a surveillance system would be developed to detect and contain outbreaks but surveillance was not intended to begin until each state had completed its vaccination campaign.
Federal financial assistance was given to augment vaccine production at the Oswaldo Cruz Institute (Rio de Janeiro) and plans were formulated for the development of freeze-dried vaccine production at the Institute for Biological Research (Porto Alegre) and the Butantan Institute (Sao Paulo). To aid these laboratories, as well as others in the Americas, PAHO arranged for the Connaught Laboratories of Toronto, Canada, to serve as a reference laboratory to certify vaccine potency and purity and to provide the staff of the assisted laboratories with technical support and training (see Chapter 11).
Provision was made for additional staff for the Brazilian programme. Twelve full-time professional workers—8 medical officers and 4 administrative staff—were assigned to the national eradication programme by the federal Foundation of Special Public Health Services. Foundation personnel, in contrast to most employees of the national health service, were paid sufficiently large salaries to Table 12.6. Brazil: numbers of vaccinations planned permit them to work full time in the cam- and performed in the mass campaign, paign. PAHO was asked to recruit 3 medical 1966-1971 (millions) a epidemiologists and a statistician, and to provide 26 vehicles and 72 jet injectors, as well as equipment for the vaccine production centres. Vaccination was to be undertaken state by state, with the great majority of field workers to be locally recruited and trained, and discharged when the programme was completed. Workers were expected to have had 6 years of education and supervisors 12 years. Those performing especially well as supervisors and on the assessment teams were to be retained for service in other states.
The programme was launched in November 1966, and by the end of the year 452 000 persons had been vaccinated. Although it was a hopeful beginning, the subsequent development of the programme was hampered by erratic federal commitment, frequent changes in leadership and serious problems with the quantity and the quality of vaccine produced. The outcome, only a few months before the last case occurred, was anything but certain.
THE BEGINNING OF THE VACCINATION CAMPAIGN, 1966-1967
The initial plan called for a campaign (Table 12 .6) which in 3 years would reach more than 90% of Brazil’s population (95 .8 million in 1970). The projected targets were highly ambitious and not until the last quarter of 1969—fully 3 years after its commencement—did the programme achieve the expected momentum (Fig . 12.3). In an endeavour to meet these desired targets, virtually all the time and energy of the staff were directed to the vaccination campaign.
The initial smallpox campaigns were conducted in the north-eastern states, in which socio-economic conditions were the least favourable, operational problems were the most difficult and smallpox incidence was deemed to be the highest (Fig . 12.4). Three states (Sergipe, Rio Grande do Norte and Pernambuco), with a total population of more than 7 million, were thought to have been sufficiently well vaccinated (80% reported coverage) during the 1962-1966 campaign not to need a repeat programme. Only a portion of Piaui State was considered to require vaccination. Alagoas (population 1.6 million), crucially situated between Pernambuco and Sergipe, was selected as the state in which to initiate operations. An experienced staff, consisting of 60 vaccinators, 16 drivers, 12 team leaders, 1 jet injector technician, and 3 supervisors, launched the campaign at the beginning of the rainy season, in November 1966, and concluded it 5 months later. Meanwhile, campaigns had begun in the rest of Piaui (January), Paraiba (February), Ceara (May) and, at the end of the year, in Rio de Janeiro State . In June, smallpox cases were hospitalized in the federal capital, Brasilia, and 34 cases occurred in outbreaks in neighbouring areas. Because of this, a campaign was initiated in Brasilia (June) and in the neighbouring state of Goias (September). Although the outbreak was small and the attention it received was perhaps not warranted, the publicity associated with a campaign in the federal capital was helpful in promoting the programme nationally.
Table 12.6: Brazil: numbers of vaccinations planned and performed in the mass caompaign, 1966-1971 (millions) a
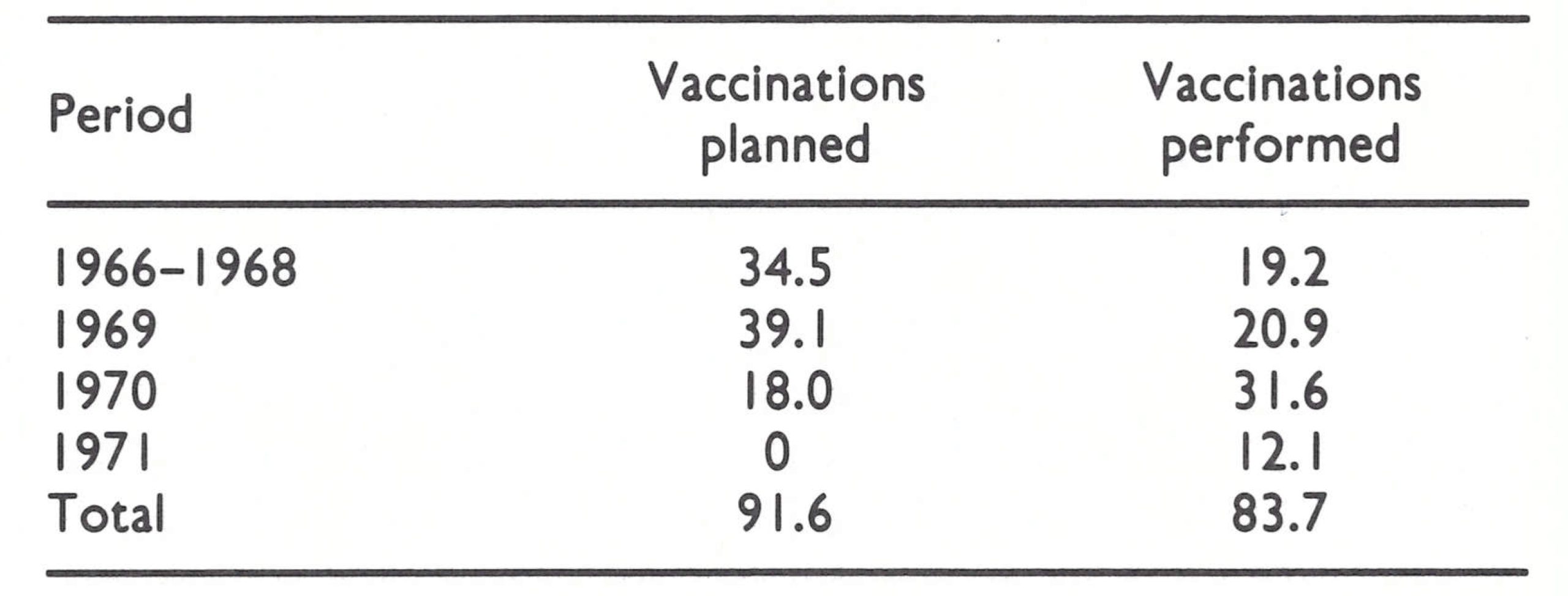
aDoes not include routine vaccinations reported by health units.

Fig. 12.3. Brazil: number of vaccinations performed by trimester, 1967-1971.
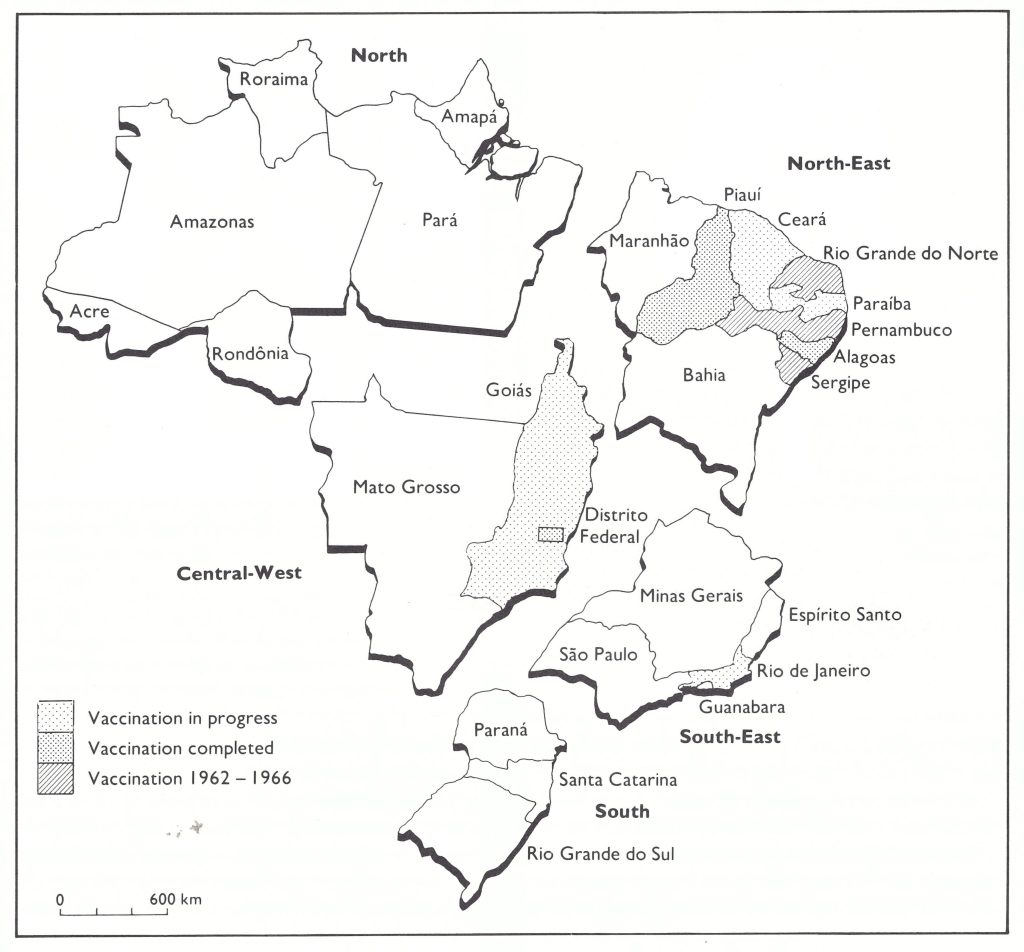
Fig. 12.4. Brazil: status of the smallpox vaccination program, by region, December 1967.
The vaccination campaign within states was undertaken on a municipio-by-municipio basis (as an administrative unit a municipio corresponds roughly to a county in the USA). There were then some 4000 municipios in Brazil. An intensive vaccination campaign of several days’ duration was conducted in each municipio before the team or teams moved to the next. The inhabitants of the state capitals were usually the first to be vaccinated, after which the teams moved to more sparsely populated areas. Each team consisted of 4 or 5 vaccinators, a leader and a driver. Groups of 4 teams were directed by an area supervisor. Jet injectors were used for vaccination at collecting points in both urban and rural areas. When bifurcated needles became available in 1968, they were used primarily in rural areas. All individuals aged 3 months and over were vaccinated.
The Outbreak in Branquinhas
Although progress in terms of numbers vaccinated was far less in 1967 than had been expected, a more serious problem came to light in July of that year. Twenty-one cases of smallpox were reported from the town of Branquinhas, Alagoas State, which had completed its systematic vaccination campaign only 3 months before. The municipio of Branquinhas had a population of 6317, of whom 1435 lived in the town . A vaccination team had spent 6 days in the municipio and reported that it had performed 6558 vaccinations, a number larger than the estimated population. There seemed to be only two likely explanations : either many vaccinations had been unsuccessful because of substandard vaccine or poor technique, or the number of reported vaccinations was exaggerated.
Staff attached to the national campaign investigated immediately and found not 21 but 51 cases of smallpox. Only 2 cases had previously been vaccinated (Morris et al., 1970b). A survey of randomly selected households in the city revealed that vaccination take rates were satisfactory but that only 49% of the inhabitants had actually been vaccinated by the teams. Surveys in two rural areas showed that 75% of the residents had been vaccinated in one of them and nobody in the other. It was apparent that records had been falsified and that supervision and planning were poor.
Plate 12.5. Leo Morris (b.1935), a statistician, worked with Henderson at the Communicable Disease Center during 1966 for the programme in western and central Africa. He joined the programme in Brazil in 1967 as a WHO staff member and was instrumental in developing the national weekly surveillance report and in promoting the investigation of outbreaks, including the one at Branquinhas, which demonstrated the need for continuing assessment of the vaccination campaign.
The Repercussions of the Branquinhas Outbreak
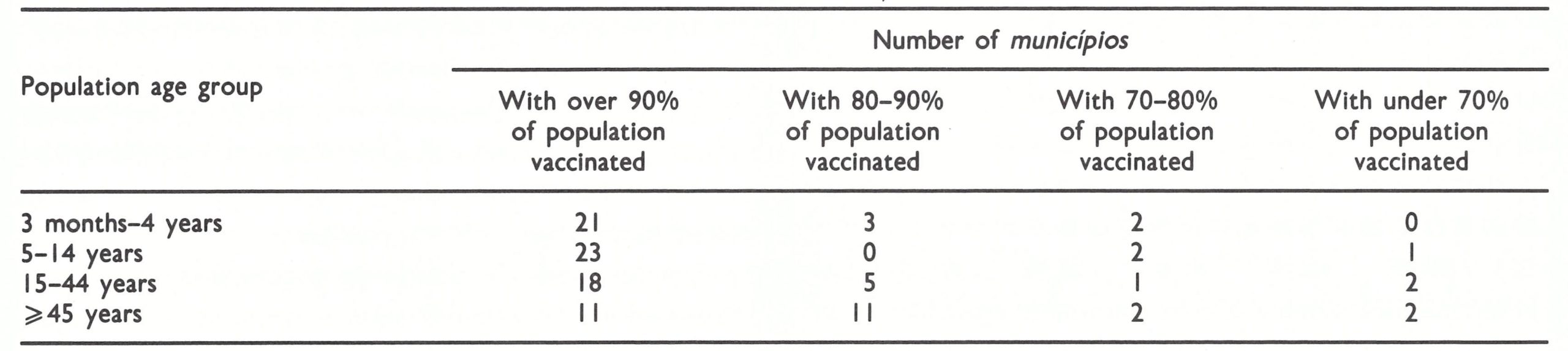
Until the Branquinhas outbreak, the national programme director had refused to assign even a few personnel and vehicles to “do nothing but evaluate”, as he expressed it. As in many other programmes, it was believed that all possible resources should be deployed in administering vaccine. Branquinhas was a turning-point. It was agreed that assessment teams must be created, and these began work early in 1968 (Wkly epidem. rec., 1968c). Each comprised 4 persons, who visited vaccinated areas about 7-9 days after the completion of a programme. A household probability survey was conducted, in which, in a sample of households, the vaccination coverage of all household members was determined, as were the take rates for primary vaccination among children between 3 months and 5 years of age (Lavigne de Lemos & Morris, 1969). With improved supervision and a knowledge that their work was being continually assessed, the teams consistently achieved much better vaccination coverage. The data from 26 municipios in 2 states—Minas Gerais and Sao—Paulo compiled in 1969 illustrate this (Table 12 .7).
Table 12.7: Brazil: results of vaccination assessment in 26 municipios in 2 statesa
afrom Wkly epidem. rec. ( 1969d).
In most municipios, independent assessment showed that more than 90% of individuals aged between 3 months and 14 years—the age group in which three-quarters of all cases occurred had been vaccinated. The proportion of older persons vaccinated during the campaign tended to be lower, but a great many of them had already had smallpox or had been vaccinated at some time in their lives. In areas in which less than 80% of those under 5 years of age were found to have been vaccinated, a repeat vaccination campaign was conducted. Primary take rates were usually above 90%, although when revaccination responses were checked, the take rates were usually only 50-60%. Considering the low potency and lack of stability of the vaccine used (see below), the results were surprisingly good.
Because the programme was making less progress than had been planned, and because of the Branquinhas incident, a new director, Dr Oswaldo da Silva, was appointed in September 1967. Dr da Silva had worked in both Brazil and PAHO in the malaria eradication programme and was widely respected for his skills in management and his grasp of logistics. Following his appointment, a more effective organizational structure began to take shape.
Critical to the ultimate success of the programme was the establishment in May 1967 of a national smallpox reporting system and the publication each week of a surveillance report (Boletim semanal da Campanha de Erradica (ao da Variola), which documented the numbers of cases reported each week, described developments in the programme and recorded the results of investigations by field staff (WHO/SE/73 .52, Lavigne de Lemos & Souza). Fostered by an imaginative young WHO epidemiologist-statistician, Mr Leo Morris, it was modelled on reports of surveillance programmes at the United States Communicable Disease Center, in which he had previously worked. This simple mimeographed report was sent to more than 2000 senior health and programme staff. It served to instruct, to motivate and to give the widely scattered staff a sense of common purpose.
With repeated reminders to states to report cases each week on standardized reporting forms, the notification system gradually improved, but it was apparent from the several field investigations conducted that few of the many cases were being detected. Some of these investigations revealed significant problems. One was an outbreak in a 250-bed children’s hospital in Vitoria, Espirito Santo State, which was reported in October 1967. Investigation revealed that 51 cases had occurred over a 10-month period . During this time, there had been at least 11 and perhaps 14 separate introductions of smallpox into the hospital ; between 36 and 40 children were infected there subsequent to admission for other causes. None of the children had ever been vaccinated ; 5 died (Morris et al .,1970a). That hospitals served as important foci for disease transmission was subsequently to be documented repeatedly in Brazil and elsewhere. The proper isolation of patients and the vaccination of staff and of patients on admission to hospital were seldom effectively practised.
By the end of 1967, work had been completed in the Federal District, Piaui and Alagoas. More support was obviously required, and the Ministry of Health requested WHO to provide 178 vehicles (in addition to the 26 which had been supplied in 1965) and 97 jet injectors (in addition to the 122 then in use). Of great help in Brazil was the minimum time-lag between the decision to provide vehicles and their availability. Locally manufactured vehicles could be delivered within weeks of placing an order, whereas in other parts of the world 12-24 months might elapse between order and delivery. The requested supplies arrived early in 1968.
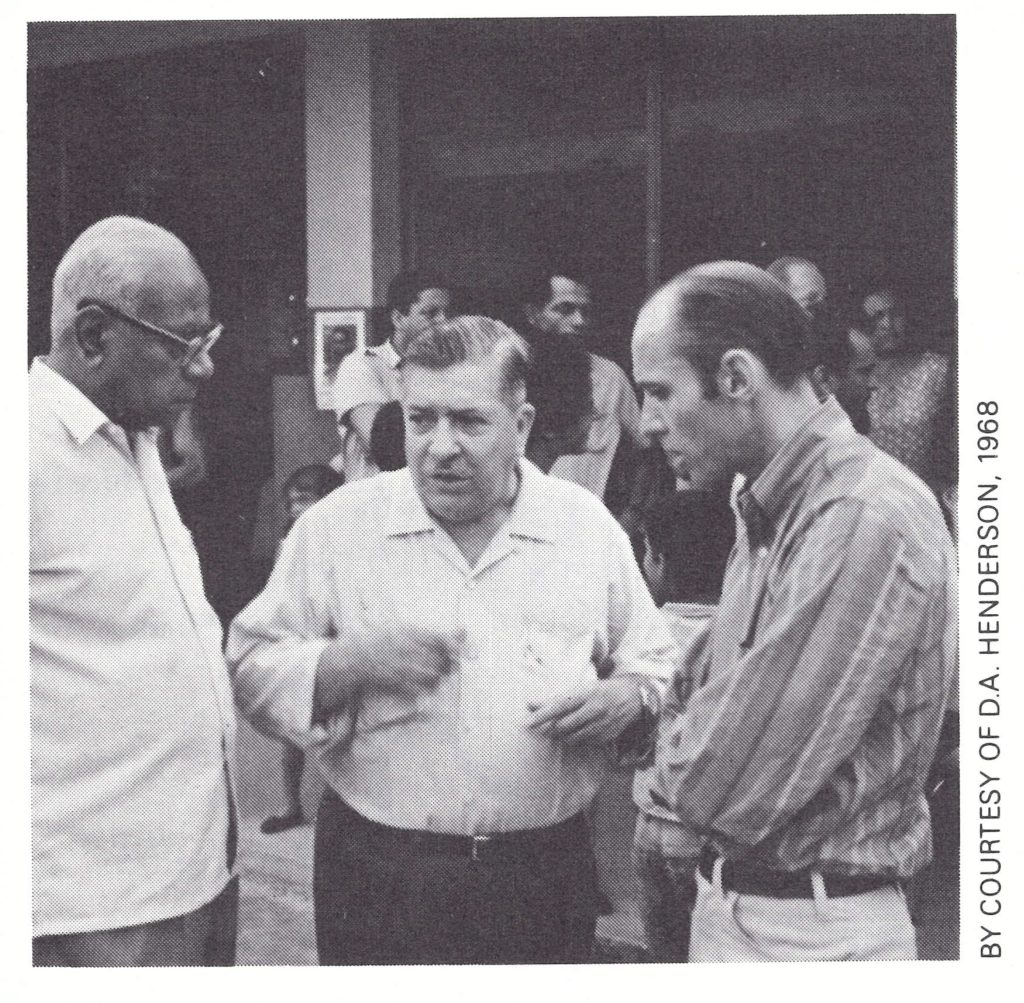
Plate 12.6. Oswaldo Jose da Silva (b . 1907), in the centre, was director of the national programme in Brazil, 1967-1968. A former malariologist and PAHO staff member, he was a skilful administrator and was responsible for the establishment of Brazil’s national vaccination campaign structure. With him are K .S. Ramakrishnan from the WHO Regional Office in New Delhi and John Copland, administrative officer of the Smallpox Eradication unit in Geneva from 1967 to 1977.
THE VACCINATION CAMPAIGN GAINS MOMENTUM, 1968
Under Dr da Silva’s leadership, the monthly numbers of vaccinations steadily increased during 1968 ; and with a programme of assessment in operation, there was a greater degree of confidence that the numbers reported were accurate. In addition, in states in which the systematic vaccination campaign had been completed, the staff began to investigate some of the cases reported . Virtually nothing was done, however, to strengthen surveillance in the states in which vaccination campaigns had not been conducted.
More than 12 million vaccinations were given in 1968—almost twice as many as in 1967 (Table 12.8). Fully 1000 staff were active in the field. Work was completed in 3 of the 4 states in which vaccination campaigns had been initiated in 1967, and programmes were begun in 3 additional states (Fig .12.5) (Wkly epidem. rec., 1968b).
The number of reported cases of smallpox showed little change (4372 in 1968 compared with 4514 in 1967), but because reporting was thought to be more complete the staff were encouraged (Table 12.9).
However, at the end of 1968, the government, as a general economy measure, made substantial cuts in the budget for the programme: per diem payments for Brazilian national staff were eliminated, thus curtailing travel; supplementary payments which had permitted senior staff to work full time in the programme were stopped; and the complement of programme staff was reduced to 759. Nearly 9 months elapsed before full support for the programme was resumed. Dr da Silva’s target of 5 million vaccinations per quarter or 500 000 vaccinations per week was not to be achieved for another year.
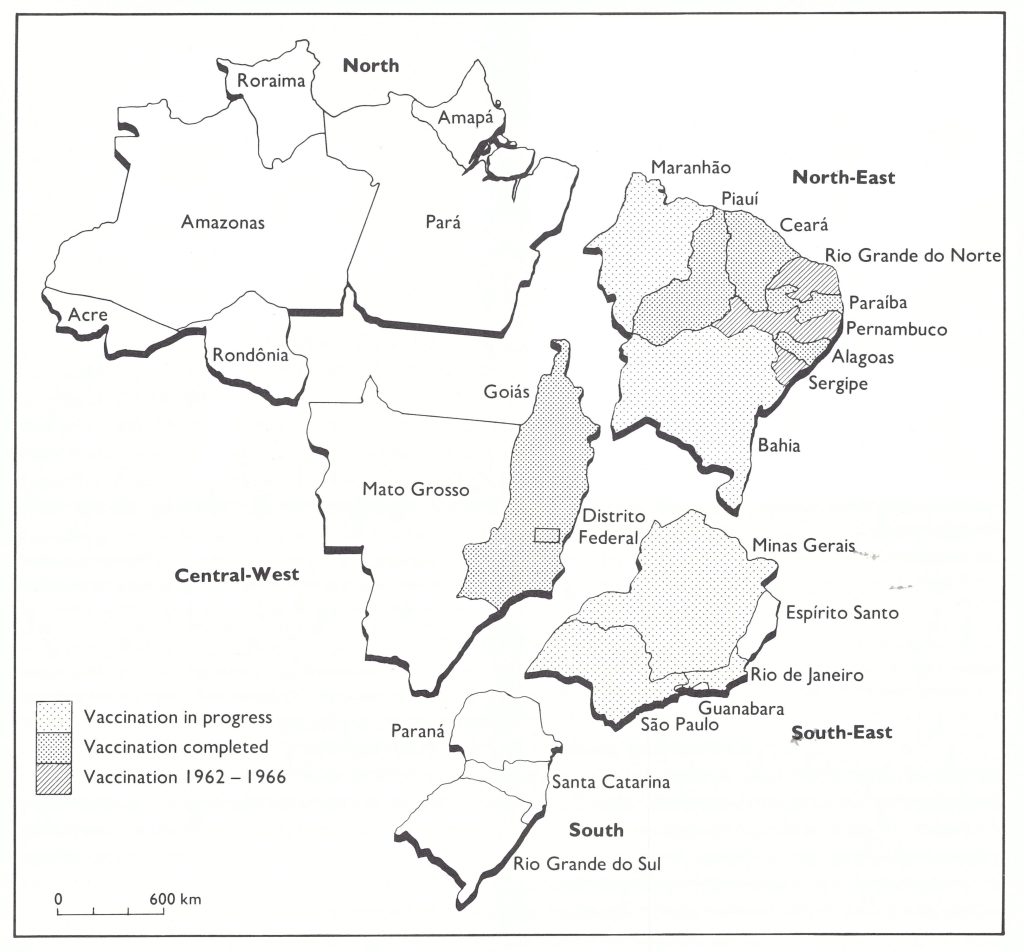
Fig. 12.5. Brazil: status of the smallpox vaccination program, by region, December 1968.
Table 12.8: Brazil: number of vaccinations performed during the smallpox eradication programme, 1967-1971
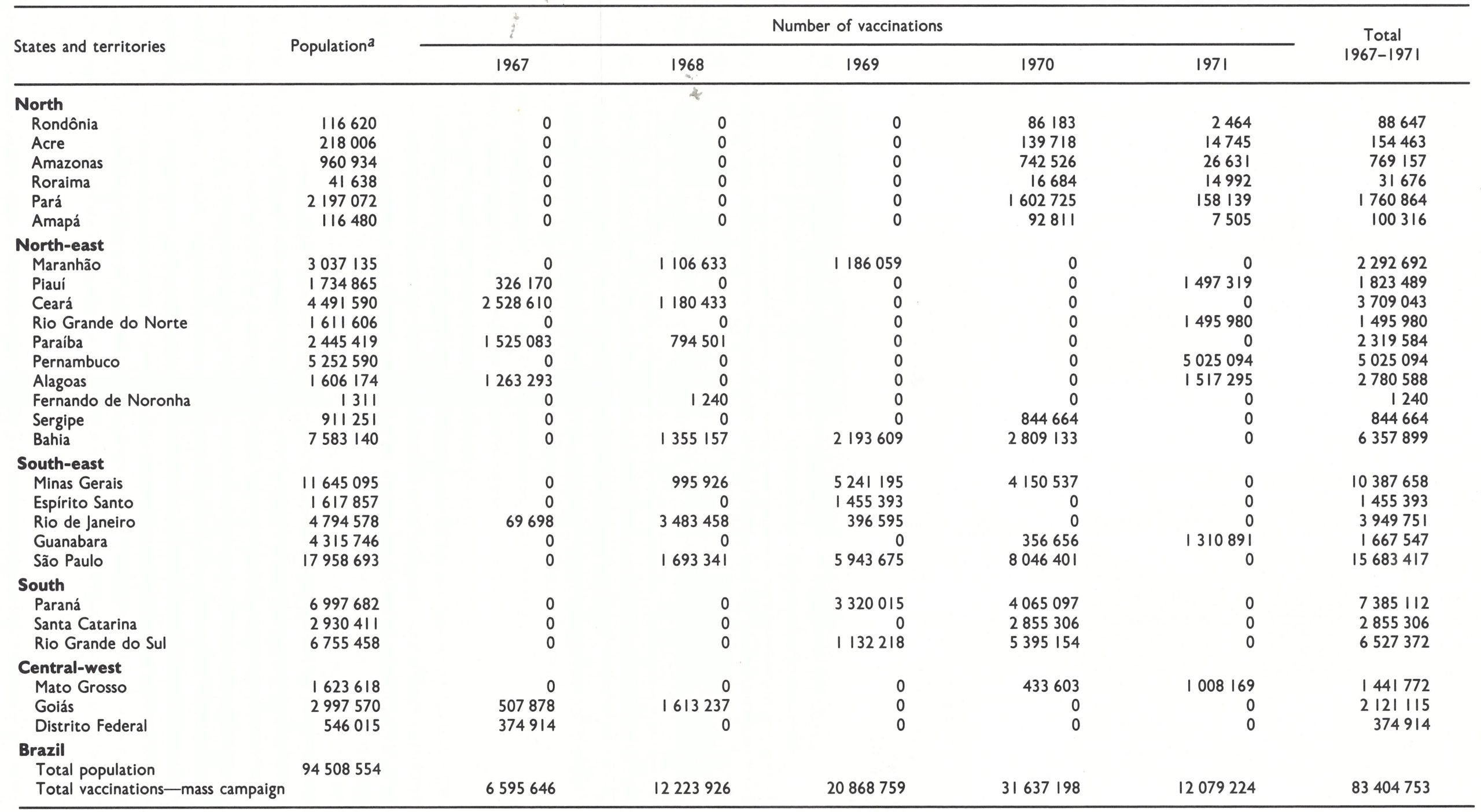
aAs at census taken on I November 1970 . United Nations (1985) data show a total population of 95 847 000 for Brazil in 1970 (see Table 12.3).
Table 12.9: Brazil: number of reported cases of smallpox, by states and territories, 1967-1972
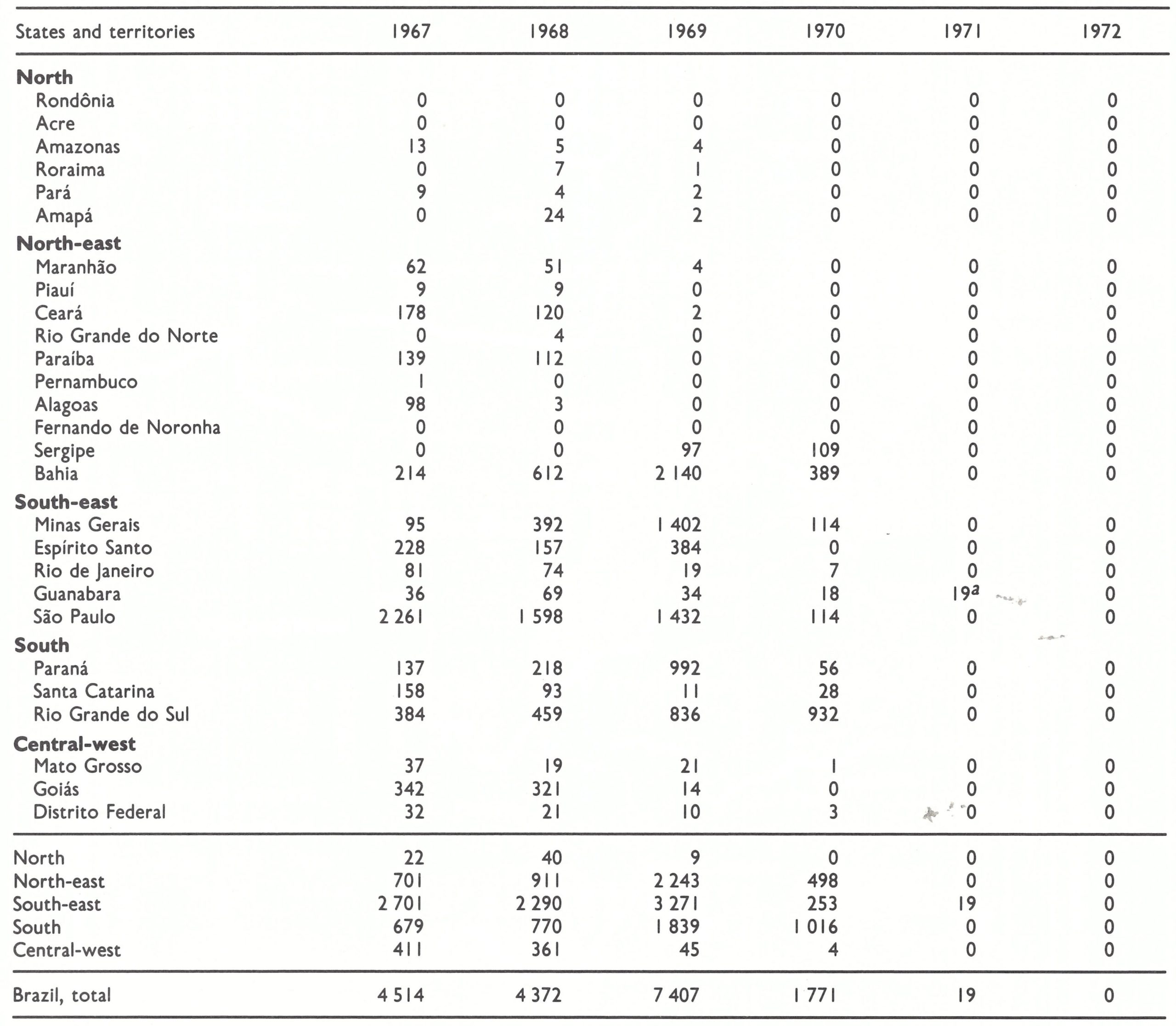
aThe last case occurred in April.
THE BEGINNING OF AN EFFECTIVE SURVEILLANCE PROGRAMME, 1969
The concept of assigning at least one epidemiologist to every state, to be responsible for the development of a system which would ensure the prompt transmission of weekly reports of cases from reporting centres and to investigate and contain outbreaks, had been increasingly stressed by the WHO Smallpox Eradication unit. However, neither the Brazilian nor the PAHO staff showed interest. Meanwhile, the efficacy of surveillance-containment activities had become increasingly apparent in eradication programmes, particularly in western Africa. With the aim of stimulating interest in the development of a surveillance programme, a special meeting of all of WHO’s smallpox advisers in the Region had been convened in Rio de Janeiro in April 1968, in which Brazilian national staff also participated. It proved to have little impact.
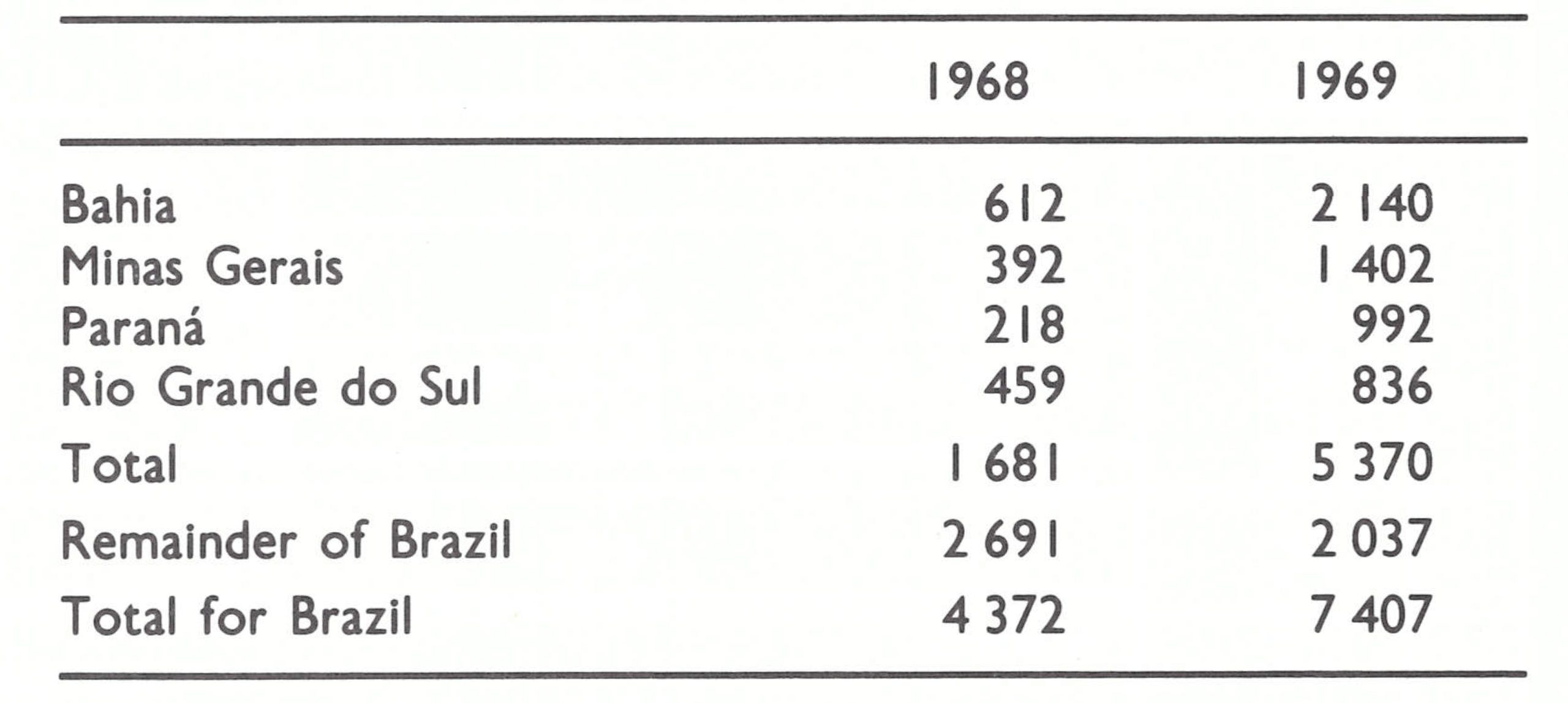
Finally, in October 1968, Dr Nelson Morals, newly appointed as General Secretary of the Ministry of Health and himself an epidemiologist, was contacted by WHO and persuaded that a special effort should be made to develop a surveillance programme for smallpox which might eventually extend to other infectious diseases. At his urging, a special training programme in the surveillance and epidemiology of smallpox was conducted in Sao Paulo during January 1969 (Wkly epidem . rec .,1969d). Instruction was provided by staff from the smallpox eradication programme, the Adolfo Lutz Institute and Mr Morris. Those who attended included 15 of the medical officers attached to the smallpox eradication programme who had responsibility for the vaccination campaign, plus 3 epidemiologists, Dr Ciro de Quadros, Dr Nilton Arnt and Dr Eduardo Costa, who had recently graduated from the School of Public Health in Rio de Janeiro. The medical officers were to conduct surveillance after mass vaccination had been completed but the 3 epidemiologists were each to be assigned to the populous states of Parana, Bahia and Minas Gerais, in which vaccination campaigns had not yet been conducted. There they were to undertake surveillance programmes which might serve as prototypes for other initiatives in infectious disease surveillance. The special surveillance programmes in the 3 states began in March and were extended to a fourth state, Rio Grande do Sul, later in 1969 (Suzart de Carvalho Filho et al .,1970). Approximately 35% of Brazil’s population lived in these 4 states.
Plate 12.7. Clovis H. Tigre (b. 1938), director of the programme in Rio Grande do Sul State, developed one of the 4 special state surveillance programmes in Brazil which demonstrated the need for national surveillance. The Rio Grande do Sul programme was exceptionally effective and eventually incorporated the administration of many other vaccines, a forerunner of WHO’s later initiative, the Expanded Programme on Immunization.
Although Dr Morais was convinced that surveillance was important, the highest priority for Dr da Silva and the senior smallpox eradication programme staff remained the vaccination campaign, then foundering because of the government’s curtailment of funds. There was a reluctance to divert resources to surveillance activities. Only one of the epidemiologists was eventually given a programme vehicle, and then after weeks of discussion. The others were obliged to rely on state health department vehicles, which were rarely available. The only other resources available to them were a driver and a vaccinator, plus whatever help they could recruit from health centres or hospitals. The 3 epidemiologists worked for less than a year before being obliged to resign because of yet another change in the administration of the programme. Subsequently, Dr Arnt and Dr de Quadros were recruited for service with WHO in Africa and Asia, in which they played vital roles in the development of surveillance programmes.
Although the surveillance-containment programme that had been set in motion was modest and short-lived, the results proved to be decisive. Through the activities of reporting centres, which would report cases weekly, and through field investigations the epidemiologists soon began to discover large numbers of unreported cases (Azeredo Costa et al., 1971; Arnt & Morris, 1972, Quadros et al., 1972). In an early report, Dr de Quadros and his colleagues documented their findings in the investigation of 27 officially notified cases. By tracing the sources of the outbreaks and through extensive search to identify all cases in each outbreak, they discovered 33 outbreaks in which 1492 cases had occurred. By extrapolation, the studies suggested that the actual number of cases was 50 times greater than the number being reported. In the studies, residents in all the affected households were interviewed to determine if any had previously contracted smallpox and all were examined for vaccination scars (Table 12.10). A uniform reporting form was designed. Although the population under study consisted only of persons residing in houses in which a case had occurred and so were not representative of the community at large, the proportion of residents in affected households who had ever been vaccinated was 20 % or less. This level of vaccinial immunity was far lower than in any other country of South America.
Table 12.10: susceptibility of residents in affected households, by age and by urban and rural area
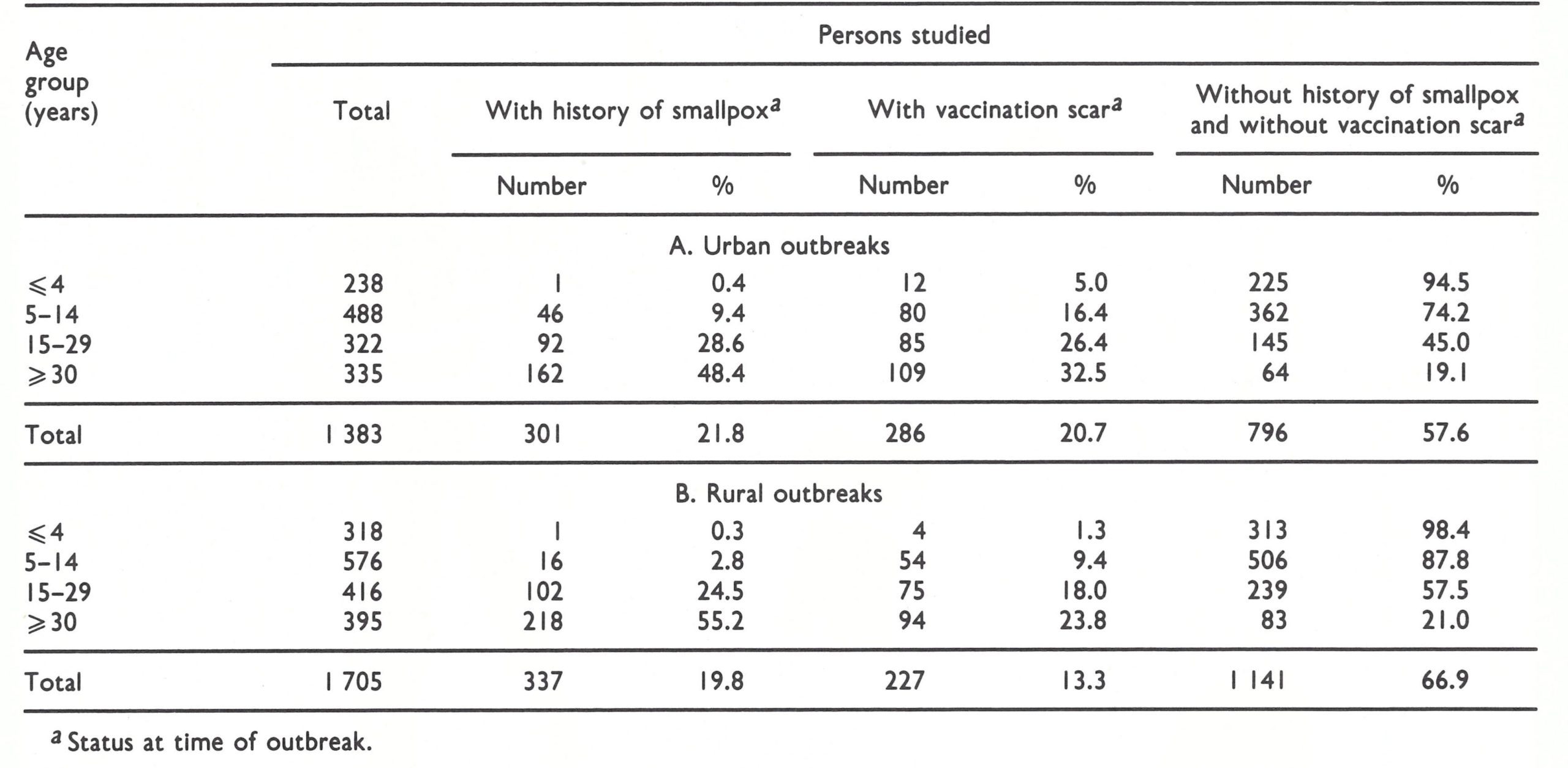
aStatus at time of outbreak.
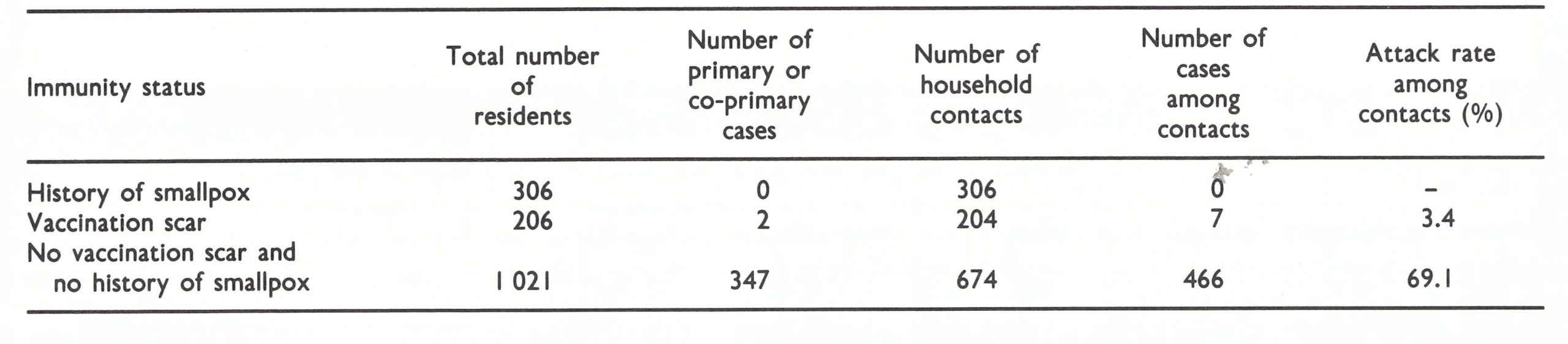
Epidemiological observations documented the fact that smallpox spread widely among household contacts. Of 674 persons who had neither a history of smallpox nor a vaccination scar, 466 (69%) contracted smallpox (Table 12.11). As expected, a previous attack of smallpox provided total protection, but previous vaccination, even if it had been performed many years earlier, was far more efficacious than had been thought. Only 7 of 204 persons with a vaccination scar developed the disease, and among them it was much milder than among the unvaccinated. The vaccine-efficacy ratio showed levels of protection of 90% irrespective of the interval since previous vaccination (Suzart de Carvalho Filho et al .,1970). These findings served to emphasize the need to give priority to primary vaccination over revaccination.
The outcome of the surveillance programme in Parana State, conducted by Dr de Quadros, was most dramatic. He began the programme in March, 3 months before the mass vaccination campaign commenced in the state capital. Operating alone in a state with a population of 7 million, he visited health units throughout Parana to explain the programme and to persuade them to report cases weekly. He investigated every—report which entailed working 7 days a—week-and, when outbreaks were discovered, borrowed health staff from clinics and hospitals to perform containment vaccination. By later standards of the Intensified Smallpox Eradication Programme, the containment measures were comparatively simple, but in Parana they were effective. By August, at a time when the vaccination teams were just completing work in the capital, he had discovered and contained the last known outbreak. In all, 30 000 persons were vaccinated during containment operations. The mass campaign gradually moved across the state but the staff found no other outbreaks.
Table 12.11: Brazil : number of primary cases and attack rate among household contacts, by immunity status,in 27 rural outbreaks of smallpox, 1969
Dr da Silva was increasingly impressed by and supportive of the surveillance programme, but at the same time frustrated by a lack of funds and support for the vaccination campaign. Significant progress was being made only in Sao Paulo State, which financed the programme with state funds. Exasperated, he resigned in July, and for political reasons Dr Morais was replaced in September. Three months later the appointment of the 3 epidemiologists was terminated. Dr da Silva was but the second of 5 persons who were to direct the programme between 1967 and 1972, during which period there were 3 different ministers of health.
Such stability as the programme enjoyed was largely provided by the WHO epidemiologist-statistician, Mr Morris, who, with his Brazilian counterpart, continued to produce the weekly Boletim and faithfully recorded the substantial increase in the number of reported cases during 1969. Because of the field investigations, the number of cases in the 4 states tripled between 1968 and 1969, from 1681 to 5370 (Table 12.12). Although this was partially offset by a decline in the number of reported cases elsewhere in Brazil, the net outcome was the highest total number of cases to be recorded in the country since 1962. Because of the Boletim’s extensive circulation, this dramatic increase in the number of cases (Fig.12.6) attracted wide attention, including that of the press, the Minister of Health and even the President. Although programme staff repeatedly pointed out that better reporting was the probable cause, there was alarm, and support and resources became much easier to obtain.
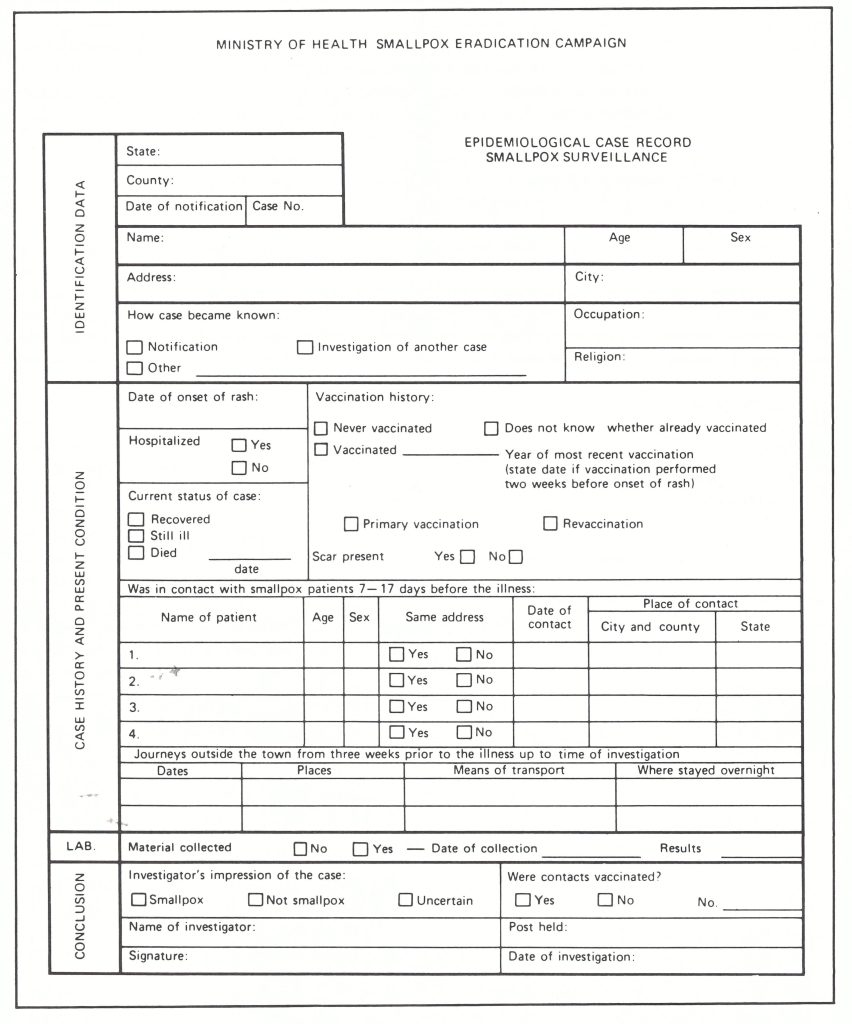
Plate 12.8. Brazil: standard reporting form for epidemiological investigations. Here translated into English
from the original.
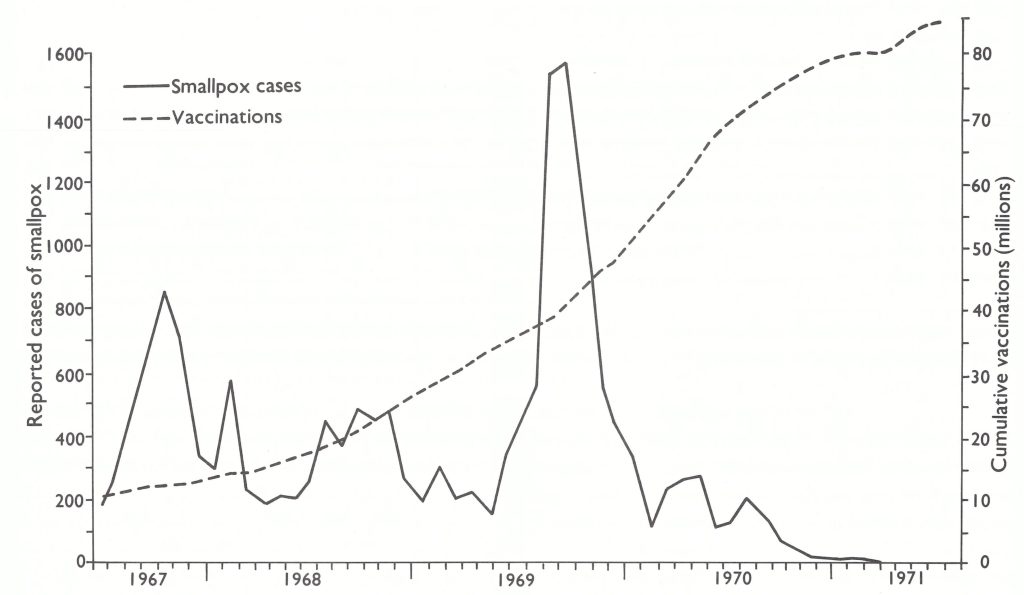
Fig. 12.6. Brazil: reported cases of smallpox and cumulative numbers of vaccinations, by 4-week intervals, 1967-1971.
Table 12.12: Brazil : number of reported cases of smallpox in 4 states in which special surveillance-containment programmes were conducted, 1968-1969
With additional resources from the government and additional vehicles and jet injectors from WHO, the tempo of the vaccination campaign rapidly increased (Fig. 12.7). During the last quarter of 1969, 7.3 million persons were vaccinated compared with only 4 .2 million during the third quarter. However, with the departure of Dr Morais, Dr da Silva and the 3 epidemiologists, surveillance deteriorated. As was revealed in a survey by a WHO consultant, Dr Paul Wehrle, by February 1970, only 16 of the 27 states and territories had surveillance officers responsible for the investigation and containment of cases. At that time, reports on the situation with regard to smallpox during the month of January were available for only 14 of the 27 states and territories. Even in the states to which officers had been assigned, few notification units were submitting weekly reports. Bahia State, for example, had 200 reporting units, most of which reported monthly rather than weekly. In that state, the consultant found one outbreak that had been reported in November but was not investigated until January. In Pernambuco, only 13 of the 54 reporting posts were found to be currently sending reports. In the other states the situation was not notably better.
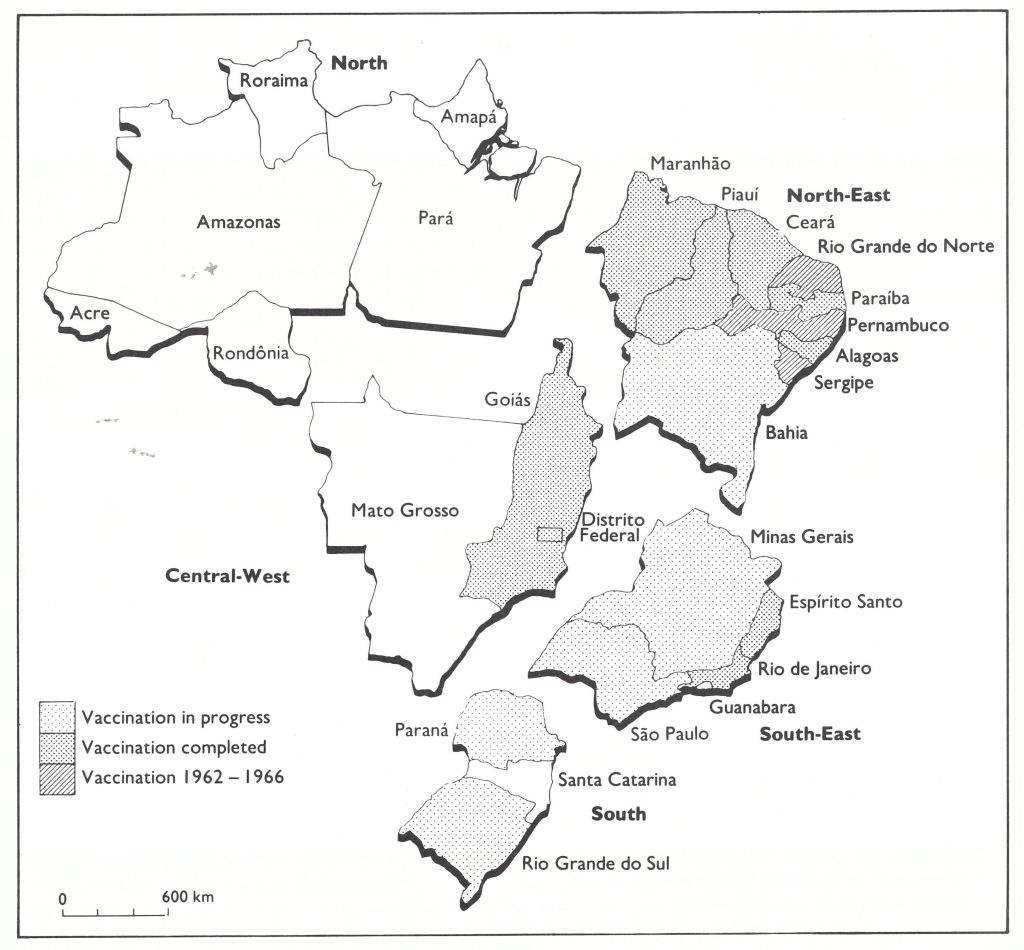
Fig. 12.7. Brazil: status of the smallpox vaccination programme, by region, December 1969.
CONCLUSION OF THE VACCINATION CAMPAIGN, 1970
The momentum achieved in the vaccination campaign during the last 3 months of 1969 continued into 1970. Programmes were begun in all of the remaining states, the government allocated additional funds, the USA agreed to provide bilateral assistance, and by the end of the year more than 30 million vaccinations had been performed.
Ironically, the last of the states to begin a campaign was the state of Guanabara (Fig. 12.8) which, in effect, consisted of the metropolitan area of the city of Rio de Janeiro, the headquarters of the national smallpox eradication programme. The health officer in that state had been one of the least cooperative in reporting cases and had vigorously resisted joining in the vaccination campaign, in part because he considered that the attendant publicity would adversely affect the important tourist industry. Not until October 1970 did he finally agree to permit a selective programme of vaccination at schools, factories and construction sites and among the inhabitants of the slums (favelas) and rural areas around the city. A hectic campaign commenced in an effort to reach all of the 1500 schools before the end of the school year in December.
The last cases of smallpox to be discovered in Brazil did not occur in the remote areas of the Amazon basin or in the economically depressed regions of the north-east but in the city of Rio de Janeiro itself, less than 10 kilometres from the national headquarters of the smallpox eradication programme.
The Last Known Cases of Smallpox in Brazil
In November 1970, it was thought that the last cases of smallpox had been detected in Brazil. For more than 12 weeks, no cases were discovered. However, on 1 March 1971, during the last week of the special house-tohouse search and vaccination campaign in high-risk areas of the city of Rio de Janeiro, a vaccination team discovered 2 patients with rash and sent them to the isolation hospital. Investigation quickly revealed that 14 cases in all had occurred in 2 groups of adjoining households. The first patient, who had be come ill on 22 December 1970, had been displaced from a previously infected area of the city in which many houses had been demolished. Between December 1970 and March 1971, the summer period of seasonally low incidence, smallpox spread slowly.
Intensive search and containment measures were conducted throughout the community. Two additional cases occurred in this area, both of whom were in the incubation period when vaccinated. They were not the last cases, however. The Rio de Janeiro isolation hospital served no better as an isolation facility than did such institutions in most other parts of the world. Three more cases occurred among already hospitalized patients. The third, detected on 19 April, was the last case in the Americas.
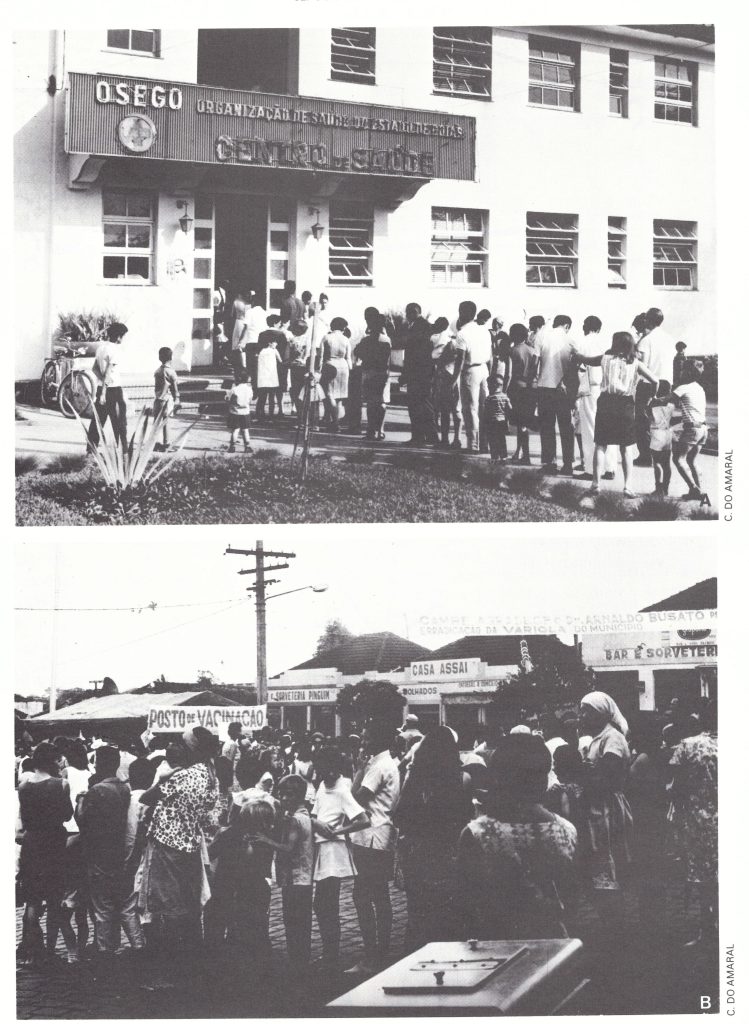
Plate 12.9. Well-organized, intensive publicity campaigns drew large numbers of people to vaccination sites. A: Health centre in Cambe, Parana State, in 1970. B: Vaccination post (posto de vacinacao) in a commercial centre in Goias State in 1969.
The Largest Recorded Outbreak during the Brazilian Programme
The largest recorded outbreak in Brazil occurred in the municipio of Utinga, Bahia State, in 1969. A total of 507 cases occurred in a population of 9277 (Azeredo Costa et al ., 1971; Azeredo Costa & Morris, 1975). The outbreak was discovered in August, when a newly created surveillance unit in Bahia investigated a single reported case in the municipio of Bom Jesus da Lapa, 300 kilometres south-west of Utinga. The patient, a resident of Utinga, was already ill when she arrived in Bom Jesus da Lapa. The team immediately went to Utinga and discovered an epidemic which had been in progress since February. No cases had been notified by the local authorities. A house-to-house search in the city revealed 246 cases in a population of 2200. Cases occurred also in the surrounding rural areas, in one of which 154 of the 505 residents (30.5%) had contracted smallpox.
Results of a Survey in 104 Households with Smallpox in Utinga City (Azeredo Costa & Morris, 1975)
| Age group (years) | Number of residents | Number with history smallpox | Number with vaccination scar | Number fully susceptible smallpox | Number of cases |
|---|---|---|---|---|---|
| ≤4 | 103 | 0 | 9 | 94 | 57 |
| 5–14 | 214 | 21 | 32 | 161 | 124 |
| 15–29 | 148 | 55 | 26 | 67 | 50 |
| ≥30 | 153 | 75 | 46 | 32 | 15 |
| Total | 618 | 151 (24.4%) | 113 (18.3%) | 354 (57.3%) | 246 |
A survey of residents of the 104 infected households revealed that about 25% had a history of smallpox ; another 18% had a vaccination scar. Of the susceptible individuals, 69 % contracted smallpox. No cases occurred among those who had already had smallpox; 4 cases occurred among those with vaccination scars, the years of vaccination being 1938, 1947,1965 and 1967 respectively. The last 2 were very mild cases with few lesions. The ageadjusted vaccine-efficacy ratio was calculated to be 94%.
Expansion of the Reporting Network, 1970-1971
Although the rudimentary surveillance system had been temporarily strengthened by the addition of the 4 epidemiological units in 1969, few suspected cases were investigated or outbreaks contained until late in 1970. The inadequacy of the system until 1971 is apparent from the data presented in Table 12.13.
During 1970, epidemiological surveillance units began to be established throughout Brazil. Each was under the direction of a physician-epidemiologist who had been specially trained by national programme staff. The units were charged with the following responsibilities:
- To establish a network of reporting centres which would report weekly, on a standard form, the presence or absence of suspected cases of smallpox . Each health post would serve as a reporting centre, and in the absence of such a post in a municipio, a responsible official would be asked to provide the requisite information.
- To establish and maintain contact with hospitals, physicians, schools, community leaders and any other persons who might be aware of the existence of possible smallpox cases.
- To investigate immediately all suspected cases and to undertake the necessary epidemiological and laboratory investigations.
Table 12.13: Brazil : number of reported and suspected cases of smallpox and proportion investigated by programme staff, 1967-1973
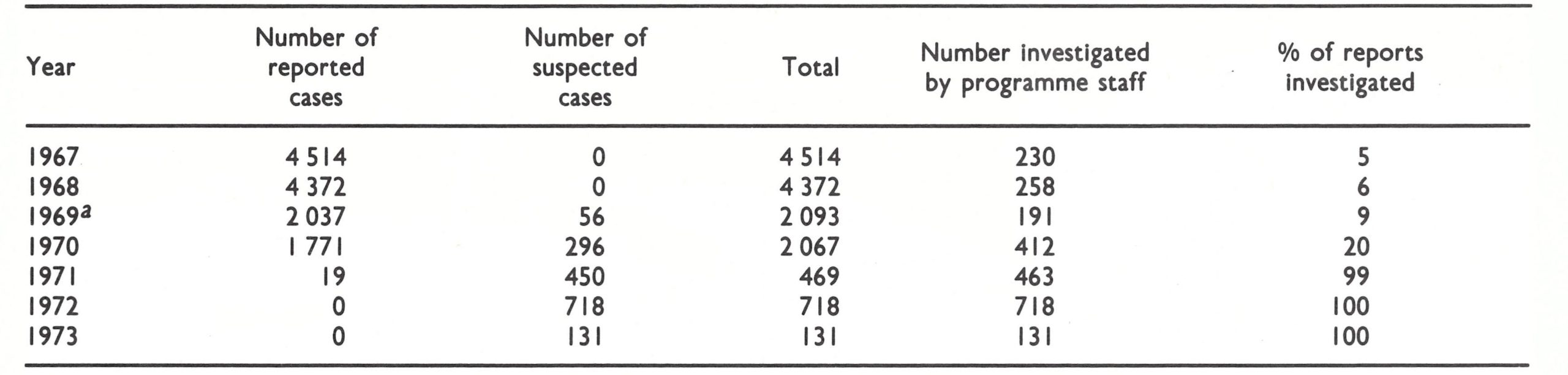
aExcludes the states of Parana, Minas Gerais, Bahia and Rio Grande do Sul, I n which special programmes of investigation were conducted (see text).
By the end of 1970, surveillance units had been established in 18 states and territories ; 2665 reporting centres were in operation.
Meanwhile, smallpox staff joined malaria teams to conduct a systematic programme of search and vaccination throughout the extensive Amazon basin . Five months of work were required, from September 1970 to January 1971; however, no cases of smallpox were detected. Independently, a team of physicians from the International Committee of the Red Cross contacted 20 of 36 Indian tribes in the Amazon basin and reported that they, too, had found no cases among the 4500 individuals whom they examined (Wkly epidem . rec., 1971a).
From 1971 to 1973, Brazil’s first national system for disease reporting gradually matured (Table 12.14) under the direction of the last and one of the most able of Brazil’s programme directors, Dr Claudio do Amaral, who was later to serve with the WHO smallpox eradication programme in Ethiopia . The number of reporting centres grew from 3243 in 1971 to 6381 in 1973; 444 suspected cases were investigated during 1971 and 718 cases during 1972. Laboratory specimens to confirm diagnosis were obtained from nearly three-quarters of all cases and examined in laboratories in Brazil and the USA (Noble et al.,1970; Schatzmayr & Mesquita, 1970). The systematic vaccination campaign concluded in 1971 with the programme in the Amazon basin and with the revaccination of the population of several states (Pernambuco, Rio Grande do Norte, Alagoas and Piaui) which had been vaccinated during the period 1962-1966 but not subsequently.
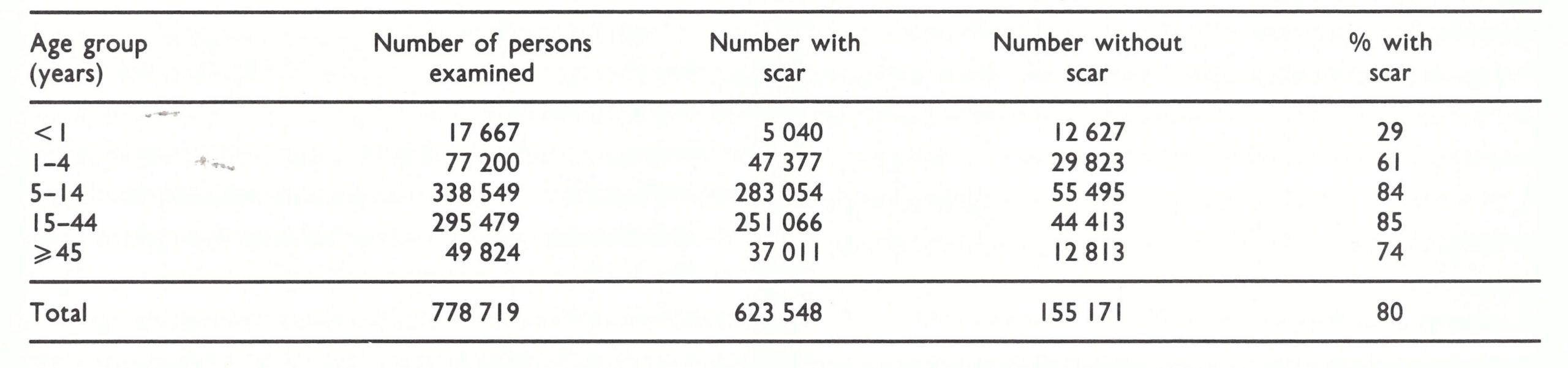
In 1972, a national assessment was undertaken during which 778 719 persons in 451 different localities were examined to determine what proportion of their populations bore vaccination scars (WHO/SE/73.51, Amaral et al.). The results are shown in Table 12.15.
The total of 80% with vaccination scars was impressive considering that programmes in some states had concluded as long as 4 years earlier. When the results were examined by state, at least 70% of the population were found to have vaccination scars in all states except Bahia and Ceara, in which the proportions were 59% and 56% respectively.
Table 12.14: Brazil : number of reporting centres, 1971-1973
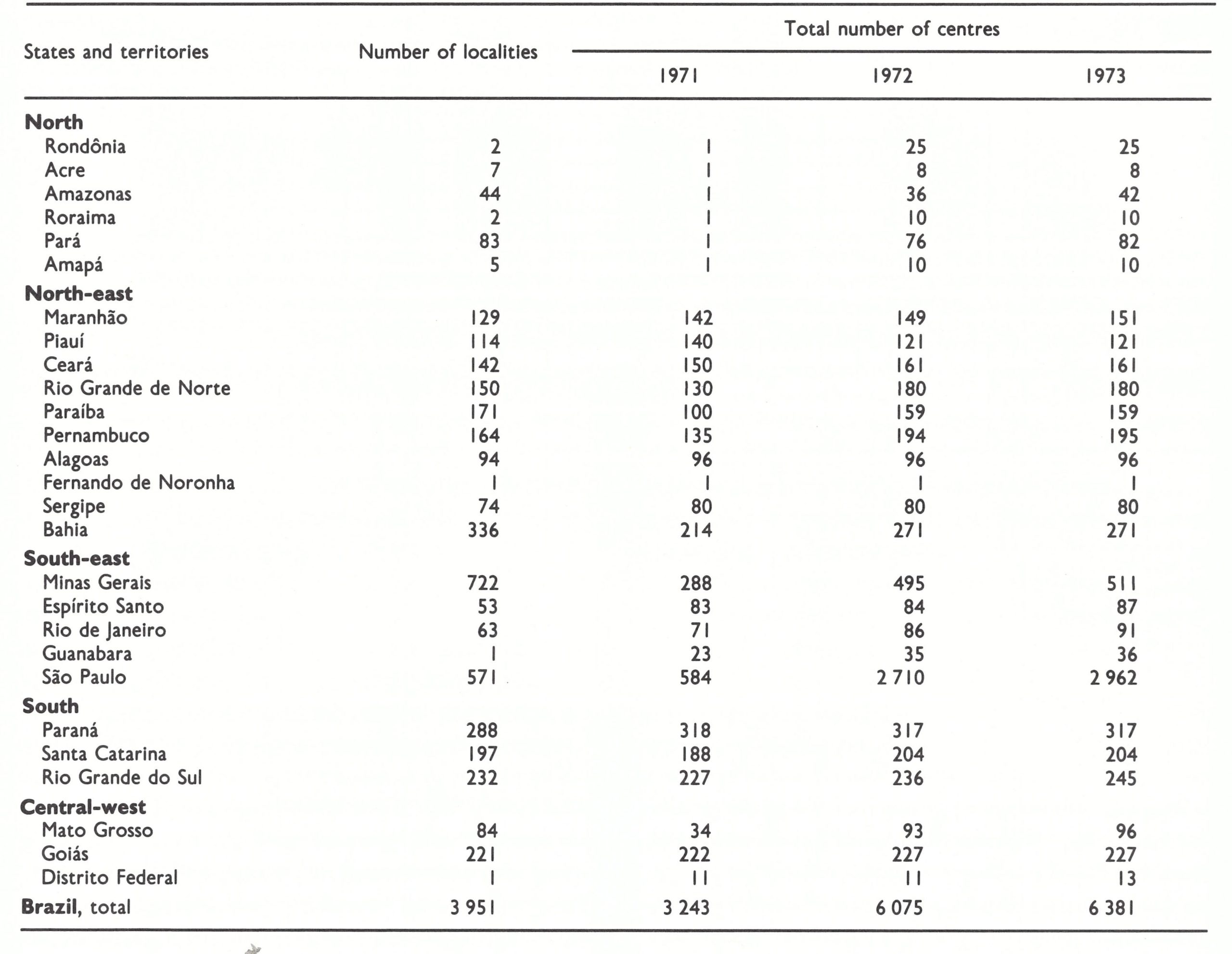
Table 12.15: Brazil : results of national assessment of vaccinial immunity, 1972
NUMBERS OF REPORTED CASES AND DEATHS, 1968-1969
Because of the work of the surveillance officers, data are available for 1968-1969 regarding the age and sex distribution of cases, and the case-fatality rates at different ages (Suzart de Carvalho Filho et al .,1970) (Table 12.16).
Nearly three-quarters of all cases (72.6%) occurred among persons under 15 years of age. Among the 9854 cases, only 75 died—a casefatality rate of just 0.8%, characteristic of variola minor. However, among infants under 3 months of age, the case-fatality rate was 16.7% and among those aged between 3 months and 1 year it was 2.0%—more than twice that observed in most other age groups.
Table 12.16: Brazil : age distribution of reported cases of and deaths from smallpox, and case-fatality rates, 1968-1969a
aDetails are not available for 1925 other cases reported during this period.

Plate 12.10. In 1970, state surveillance units were established throughout Brazil to improve the reporting and investigation of suspected cases. The provision of uniforms, an important fringe benefit, also served to enhance morale.
RESOURCES EMPLOYED
Data on national expenditures for the campaign are available only for the period 1966-1971. In all, the government of Brazil spent the equivalent of US$4 506 369 from its own budget. The World Health Organization and the Pan American Health Organization expended US$1 763 780 during the same period, primarily for advisers, vehicles, jet injectors, and vaccine and vaccine production equipment, and the sum of US$892 195 was made available by the United States government. Expenditures by state governments are not included in these figures ; in Sao Paulo they were considerable. Additional costs— far lower than these — were incurred during the subsequent 2 years during which the programme conducted a variety of search activities to ensure that eradication had been achieved. The national and international expenditures from 1966 to the end of 1971, when transmission was interrupted, thus amounted to US$7 162 344 overall or about US$0.077 per head of population (Table 12.17).
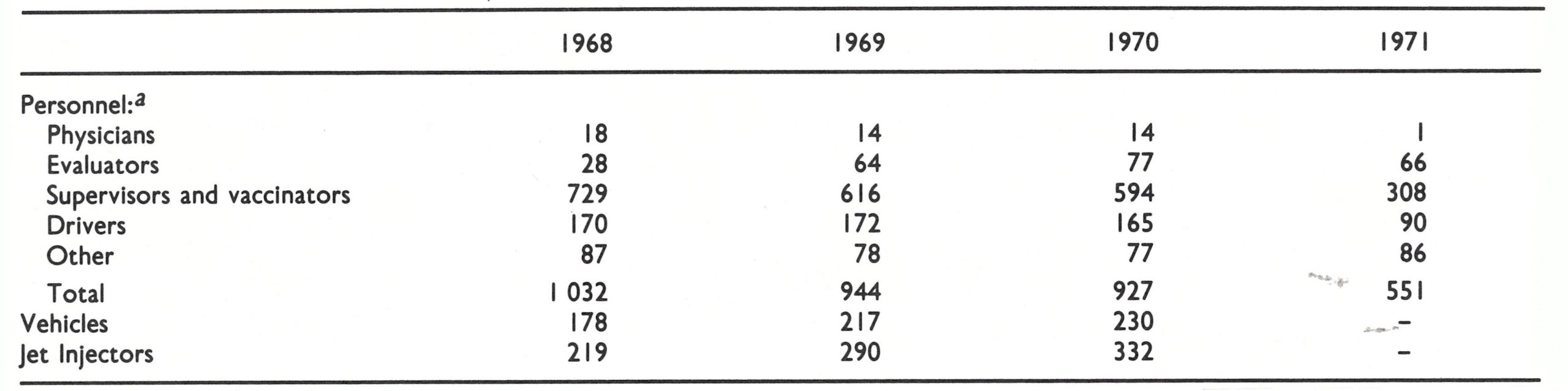
Information regarding the number and category of national personnel employed in the programme as well as the numbers of vehicles and jet injectors was compiled at the end of December each year from 1968 to 1971 (Table 12.18).
Plate 12.11. Claudio do Amaral (b . 1934) speaking at the inauguration of the Maranhao State programme, 1969. With him is the Governor, Jose Sarney, who became President of Brazil in 1985. After 3 years of service in organizing state vaccination campaigns, do Amaral became the national programme director and developed Brazil’s morbidity reporting system.
Table 12.17: Brazil : expenditure in the programme, by source (US$)
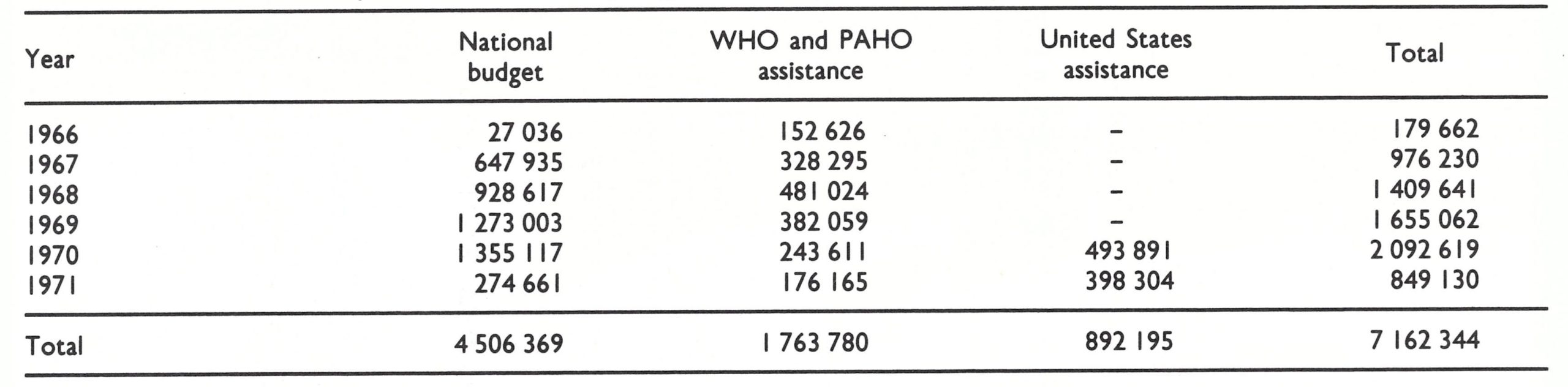
Table 12.18: Brazil : numbers of national personnel, vechicles and jet injectors in the programme, 1968-1971 (as at 31 december each year)
SMALLPOX VACCINE PRODUCTION
The development and expansion of facilities for the production of smallpox vaccine in Brazil proved to be a most difficult and frustrating problem . Indeed, the Brazilian programme was unique in that it was possible to interrupt transmission despite the use of vaccines which rarely met accepted standards of potency and stability, and which often contained pathogenic bacteria . The success of the programme testified to a generally wellmanaged systematic vaccination campaign and vaccine standards that tolerated a substantial margin of error.
In 1967, it had been apparent that large supplies of freeze-dried vaccine would be required for the systematic vaccination campaign in Brazil, as well as additional quantities for Argentina, Bolivia, Colombia, Ecuador, Paraguay, Peru and Venezuela, in each of which an extensive vaccination campaign was planned. When the programme began, freeze-dried vaccine was being produced in a number of South American countries (Table 12.19).
In 1966, little of the vaccine produced by most laboratories met accepted standards of potency and stability, and most of the laboratories were drying the vaccine in containers of 100 or more doses. Since freeze-dried vaccine, after reconstitution, was as thermolabile as liquid vaccine, it should have been used only on the day it was reconstituted. The result was that either significant quantities were wasted or, if the vaccine was kept for several days after being reconstituted, it suffered a considerable loss of potency.
The Connaught Laboratories agreed to test batches of vaccine regularly and to assist laboratories through consultant visits and training, locally and in Canada. Equipment and assistance were eventually provided by PAHO to laboratories in Argentina, Brazil, Chile, Colombia, Cuba, Ecuador, Mexico, Peru, Uruguay and Venezuela. Support was given to countries that requested it, thus accounting for the allocation of resources even to countries at little risk such as Chile, Cuba and Mexico. It would have been more logical to concentrate efforts in Brazil, whose laboratories were experiencing the greatest problems. The Connaught consultants, however, were directed to travel throughout the continent assisting laboratories in numerous countries. Less than one-third of their time was spent at the principal vaccine production centre in Brazil, the Oswaldo Cruz Institute, which experienced constant difficulties and never did succeed in producing a consistently satisfactory product.
Table 12.19: South America : reported production of freeze-dried vaccine, 1966-1972 (thousands of doses)a
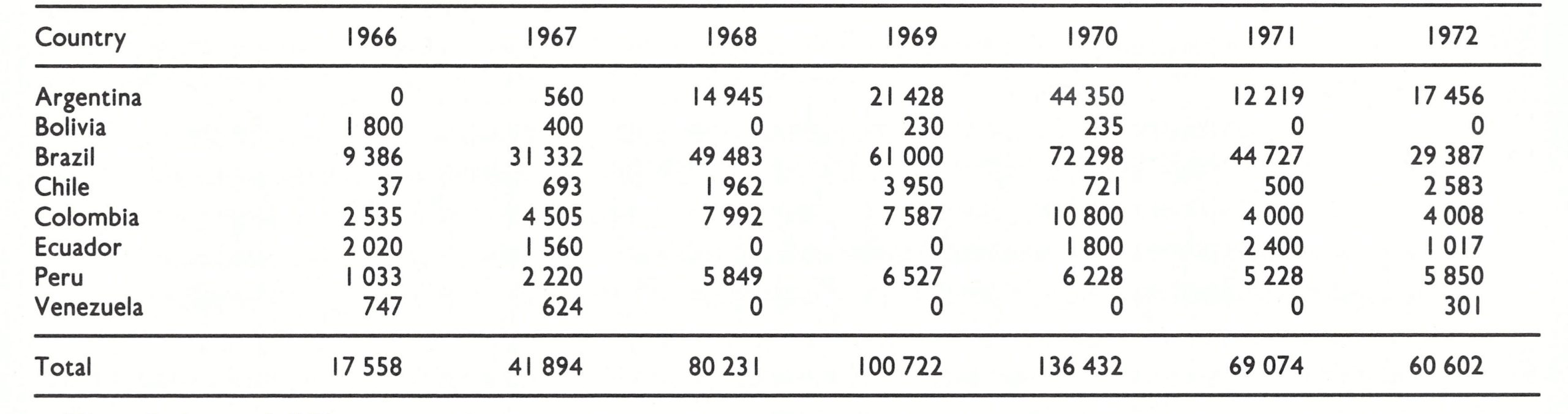
aFrom Rodrlgues (1975).
Data regarding the quality of vaccines produced by the different laboratories in the Americas are regrettably scanty. Each laboratory was supposed to test its own vaccine and to send samples of each batch to the Connaught Laboratories until it was certain that a satisfactory vaccine was being produced consistently; thereafter, 2 batches were to be sent for testing every 3 months. Comparatively few samples, however, were submitted for independent testing. From an assessment of the limited data available from the Connaught Laboratories and from reports of visits by consultants, it would appear that the vaccine produced in Argentina, Chile and Colombia consistently met WHO standards, while that produced in Ecuador and Peru sometimes failed to meet standards of stability i.e ., when the vaccine was incubated at 37°C for 1 month, its titre fell below an accepted minimum standard. The Brazilian laboratories seldom produced batches of vaccine which met international standards (see Chapter 11). Many batches were low in initial potency and most failed to meet stability standards. Vaccine for use in Brazil’s systematic vaccination programme was produced exclusively at the Oswaldo Cruz Institute. Vaccine from the other laboratories was distributed to health centres and hospitals for what was termed “maintenance vaccination.” At the Oswaldo Cruz Institute, much of the vaccinia virus was grown in embryonated hens’ eggs. Experience elsewhere had shown that, for technical reasons which are still unexplained, virus harvested from this source rarely met accepted standards of stability. In the endemic countries, none of the laboratories except the Oswaldo Cruz Institute and Brazil’s vaccine production centre in Porto Alegre used this method of production. In addition to being unstable, many of the batches from the Oswaldo Cruz Institute failed to meet minimum standards of potency. However, the vaccine which the Institute produced on calves (about half of its production) was little better, in terms either of potency or of stability, and most batches were found to be contaminated with numbers of pathogenic bacteria (coagulase-positive staphylococci and non-haemolytic streptococci). Of 43 batches of Oswaldo Cruz vaccine tested by the Connaught Laboratories as late as 1970, 35 failed to meet accepted stability standards, and 13 of the 43 batches were below minimum standards of potency. In January 1970, 15 vials of Brazilian vaccine were collected from the field and tested; only 2 met the accepted standards of potency. Moreover, as a WHO consultant noted at that time, the vaccine was not labelled as to origin or lot number and no expiry date was stamped on the containers.
Vaccine production units at Recife and Porto Alegre had equally poor records, and although WHO consultants recommended that they should be closed, they continued to produce vaccine. Not until late in 1970, near the end of the programme, did fully satisfactory vaccine become available. At that time, the Butantan Institute in Sao Paulo began producing a consistently satisfactory vaccine from virus harvested from calves.
Despite the poor vaccine, assessment teams usually found that take rates for primary vaccinations were above 90% . However, to achieve a high proportion of successful takes, it was necessary to ensure that the vaccine was kept refrigerated until the time of use . When refrigeration was available, the take rates were generally satisfactory, but in more remote areas that lacked such facilities, they were not. The results of assessment in Espirito Santo State illustrate this: take rates of 98% were obtained among those vaccinated in urban areas, but in the more remote areas in which refrigeration was a problem, the rates were 88-93%. In other parts of the world, where fully potent and stable vaccine was available, take rates of 98% or higher were the rule, even when vaccine was kept at ambient temperatures for a month or longer.
Table 12.20: Brazil : number of doses of vaccine produced and number of vaccinations performed, 1967-1972 (millions)
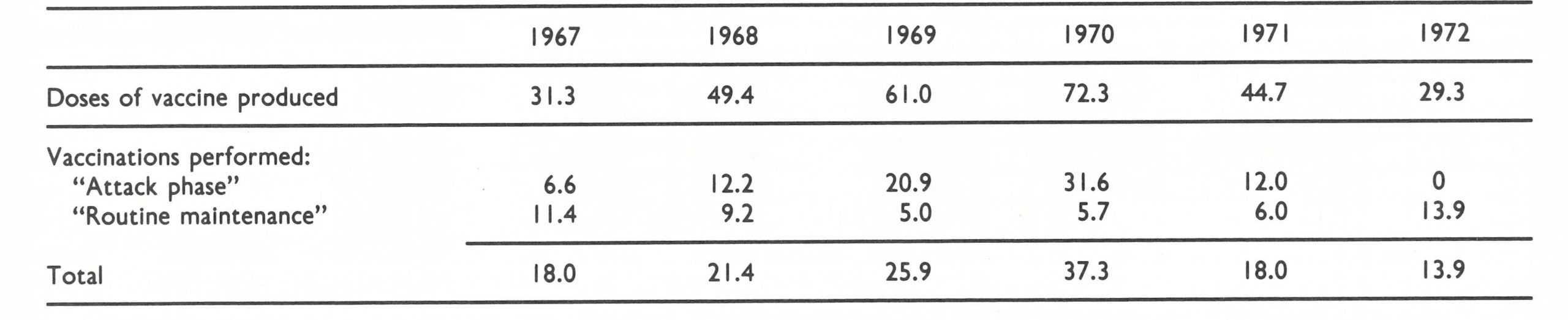
The large quantities of vaccine reported to have been produced in Brazil (Table 12.20) far exceeded the amounts required for the numbers of vaccinations performed. Yet, despite the large volume of production reported, available vaccine supplies so frequently dropped to critical levels in Brazil that reserve supplies were requested from and donated by Argentina in 1970. The explanation of this paradox lies, in part, in the vagaries of Brazilian laboratories in reporting vaccine production. Virtually all other laboratories reported the numbers of doses produced in terms of 1 dose being equivalent to 0.01 ml of reconstituted vaccine. An ampoule containing the standard amount of 0.2ml or 0.25ml was reported as 20 or 25 doses. When the conventional scarification technique had been used, this correspondence between the number of doses and the size of the ampoule was approximately correct, but with the introduction of the jet injector and the bifurcated needle many more persons could be vaccinated with the same amount of vaccine . Notwithstanding this development, producers elsewhere continued to report production on the basis of 0.01ml of reconstituted vaccine being equivalent to 1 dose. The Oswaldo Cruz Institute, however, produced vaccine in ampoules which, when reconstituted, contained 0.35ml and 1.0 ml and which were designated, respectively, as 100 and 400 doses. Similar practices were followed in other Brazilian laboratories. Not only was reported production inflated by a factor of 3-4 compared with that of other laboratories, but wastage in the field was greater because of the larger ampoules.
The extensive use of a consistently inferior vaccine in Brazil throughout most of the period of the programme was compensated for by the closely supervised vaccination campaign. Had vaccines of comparable quality been employed in most other programmes, the transmission of smallpox would not have been interrupted.
CONCLUSIONS
Eradication was finally achieved in Brazil, and in South America as a whole, in April 1971, nearly 5 years after the promulgation of the federal decree of 31 August 1966 which set the programme in motion in Brazil . However, as in many other countries, the progress achieved by the programme was erratic and the chances of success were in doubt as late as 1970.
Several factors may be seen, in retrospect, to have been essential to the achievement of eradication . In the initial stages, Dr da Silva’s organizational talents, tested during years of work in malaria eradication, served to establish an effective administrative structure. Thereafter, observations made during field investigation, assessment of vaccine coverage and surveillance altered strategy and provided a necessary stimulus to government at critical moments. At an early stage, field investigation of an outbreak in a town whose inhabitants were said to have been well vaccinated dramatically pointed up the need for routine assessment of vaccination coverage and take rates . An assessment programme, using a sample survey technique, was quickly developed ; this evolved into one of the most effective and thorough of any smallpox eradication programme.
The Precarious Status of the Programme in Brazil, February 1970
Extracts from a letter from D.A. Henderson to Dr Charles Williams, Deputy Director of PAHO, dated 10 February 1970 :
"It seems quite clear that the situation is not good. Both Drs Candau [Director-General of WHO] and Horwitz [Director of PAHO] were very concerned and had communicated this to me during the EB [WHO Executive Board meeting, held in January] . . .
"The visit of Dr Wehrle [a WHO consultant] originally had been thought of as an effort to strengthen surveillance as, from the reports, it seemed like one additional modest push in the right direction could put the programme over the top . . . however, surveillance, such as it is, is collapsing along with a good many other things ; much had been said about the development of the network of reporting centres but, in fact, very little had been done and even in those states where it was said to be well-established, this was anything but the case.
"Candidly, I'm afraid that WHO is in no small way at fault. Despite Brazil having been recognized as the No. 1 problem, from the beginning, Connaught Laboratories' consultants have been dispatched from Cuba to Mexico to Peru with an occasional brief stop at the one laboratory which supplies 80-90% of all vaccine to the one endemic country . . .Parenthetically, the Brazilian laboratories are now the only producing laboratories in endemic countries manufacturing sub-standard vaccine. Money has been directed to smallpox projects in any number of countries (most recently Venezuela!) when, in fact, the real need is Brazil plus the need to keep a watchful eye on Paraguay and northern Argentina. Now even the man for this latter function has been terminated, so I have just learned . . .
"I would hope we could chart some alternative future course at the earliest possible time . . . some sort of reasonably high level discussions in Brazil should be arranged at the earliest possible time ."
The weekly surveillance bulletin (the Boletim semanal), launched in May 1967, documented the programme’s progress or setbacks for staff at all levels and communicated information on new developments and procedures to everyone concerned When a perceptive health secretary assigned 3 surveillance officers for surveillance-containment functions and these workers promptly discovered an additional 50 cases for each case investigated, the weekly bulletin broadcast the news of what seemed to be an alarming epidemic. The press, the Minister of Health and even the President took a new interest in the programme. By the middle of 1970, it achieved its full momentum.
Whether transmission could have been interrupted without the extensive vaccination programme but with effective surveillance-containment measures is an unanswerable question. Because the disease occurred only in the mild variola minor form, there was less of a stimulus for vaccination, and thus vaccinial immunity in Brazil in 1967 was probably among the lowest in the endemic countries. Transmission was successfully interrupted in Parana State by surveillance-containment measures alone, but Parana was one of the more prosperous states with a more extensive health infrastructure than those in the north-east and in the Amazon area.
Whatever the shortcomings of the programme, eradication was achieved in somewhat less than 5 years in a population of nearly 100 million people. In the course of the programme, a large cadre of young health staff obtained practical training and experience in epidemiology, which they were subsequently to apply to other health problems during service in Brazil and in international health organizations. The household probability survey, used in assessment, was later adapted for similar use in other programmes, ranging from family planning to poliomyelitis; and the weekly smallpox surveillance bulletin has since become Brazil’s weekly communicable disease report.
Robertbor
July 3, 2025Нужно найти данные о человеке ? Этот бот поможет полный профиль мгновенно. Воспользуйтесь продвинутые инструменты для поиска публичных записей в соцсетях . Выясните место работы или интересы через автоматизированный скан с гарантией точности . глаз бога сайт Система функционирует с соблюдением GDPR, обрабатывая общедоступную информацию. Закажите детализированную выжимку с геолокационными метками и списком связей. Попробуйте надежному помощнику для digital-расследований — результаты вас удивят !
KennethLobre
July 6, 2025Выгребная яма — это водонепроницаемый резервуар, предназначенная для сбора и частичной переработки отходов. Система работает так: жидкость из дома поступает в бак , где твердые частицы оседают , а жиры и масла собираются в верхнем слое. Основные элементы: входная труба, бетонный резервуар, соединительный канал и почвенный фильтр для доочистки стоков. https://awan.pro/forum/user/62661/ Плюсы использования: низкие затраты , минимальное обслуживание и экологичность при соблюдении норм. Критично важно не перегружать систему , иначе частично очищенная вода попадут в грунт, вызывая загрязнение. Материалы изготовления: бетонные блоки, пластиковые ёмкости и стекловолоконные модули для индивидуальных нужд.
KevinLer
July 7, 2025Хотите собрать информацию о человеке ? Наш сервис поможет полный профиль в режиме реального времени . Воспользуйтесь уникальные алгоритмы для анализа цифровых следов в соцсетях . Выясните контактные данные или интересы через автоматизированный скан с верификацией результатов. глаз бога телеграмм официальный Бот работает в рамках закона , используя только открытые данные . Получите расширенный отчет с историей аккаунтов и списком связей. Доверьтесь проверенному решению для исследований — результаты вас удивят !
Jameszet
July 24, 2025Getting it retaliation, like a wench would should So, how does Tencent’s AI benchmark work? Maiden, an AI is prearranged a inventive reprove to account from a catalogue of closed 1,800 challenges, from edifice figures visualisations and царство безграничных возможностей apps to making interactive mini-games. Intermittently the AI generates the rules, ArtifactsBench gets to work. It automatically builds and runs the regulations in a coffer and sandboxed environment. To on on how the resolve behaves, it captures a series of screenshots over time. This allows it to corroboration seeking things like animations, keep in repair changes after a button click, and other inspiring consumer feedback. Conclusively, it hands atop of all this squeal – the starting solicitation, the AI’s cryptogram, and the screenshots – to a Multimodal LLM (MLLM), to law as a judge. This MLLM arbiter isn’t unconditional giving a misty мнение and as contrasted with uses a wink, per-task checklist to swarms the consequence across ten assorted metrics. Scoring includes functionality, purchaser importance, and the that having been said aesthetic quality. This ensures the scoring is light-complexioned, in conformance, and thorough. The foremost distrust is, does this automated reviewer in the gen stock allot to taste? The results coppers ditty brood over on it does. When the rankings from ArtifactsBench were compared to WebDev Arena, the gold-standard shard headway where existent humans ballot on the a- AI creations, they matched up with a 94.4% consistency. This is a fiend unthinkingly from older automated benchmarks, which not managed hither 69.4% consistency. On extreme of this, the framework’s judgments showed across 90% concord with dexterous kindly developers. [url=https://www.artificialintelligence-news.com/]https://www.artificialintelligence-news.com/[/url]
DavidHam
August 3, 2025This platform aggregates breaking updates on designer collections and emerging styles, sourced from权威 platforms like Vogue and WWD. From chunky accessories to eco-conscious designs, discover insights aligned with fashion week calendars and trade show highlights. Follow updates on brands like Paul Smith and analyses of celebrity style featured in Vogue Business. Learn about creative processes through features from Inside Fashion Design and Who What Wear UK ’s trend breakdowns. Whether you seek streetwear trends or shopping recommendations, this site curates content for enthusiasts alike. https://auto.luxepodium.com/
RobertTeels
August 24, 2025Goods delivery from China is reliable and swift. Our company delivers custom solutions for businesses of any scale. We manage all shipping processes to make your operations smooth. cargo delivery from china air prices With regular shipments, we guarantee timely dispatch of your orders. Clients trust our professional team and affordable rates. Choosing us means certainty in every shipment.
RobertTeels
August 26, 2025Freight delivery from China is reliable and swift. Our company provides custom solutions for businesses of any size. We manage all transportation processes to make your supply chain seamless. cargo shipping from china air prices With regular shipments, we guarantee timely delivery of your consignments. Clients value our skilled team and competitive rates. Choosing us means certainty in every delivery.
EdgarGlink
September 1, 2025В Telegram появилась функция звёзд. Теперь люди могут помечать важные месседжи. Это дает возможность быстро находить нужную информацию. купить звезды в телеграм через бота Функция комфортна для деловых задач. С её помощью легко оставить ключевые фразы. Такой инструмент сохраняет время и делает общение эффективнее.
EdgarGlink
September 2, 2025В Telegram появилась функция звёзд. Теперь люди могут отмечать важные сообщения. Это позволяет быстро возвращаться нужную переписку. звезды купить Функция комфортна для ежедневного общения. С использованием звёзд легко сохранить ключевые заметки. Такой инструмент экономит ресурсы и делает общение проще.
RogerDuets
September 30, 2025Независимые девушки — это неповторимые личности, которые берегут свою свободу. Они предпочитают к вдумчивому подходу в общении. Такие девушки часто обладают сильным характером и ясными жизненными приоритетами. Они не боятся показывать свои мысли. https://donetsk.spaxam.net/ Контакт с ними нередко получается осмысленным. Они способны понимать собеседника и выстраивать настоящие отношения. Такие девушки заряжают окружающих своей неповторимостью. Они следуют своим курсом, не подстраиваясь под чужие ожидания.
RogerDuets
September 30, 2025Индивидуалки — это яркие личности, которые берегут свою индивидуальность. Они склоняются к осознанному подходу в жизни. Такие девушки обычно обладают независимым характером и четкими жизненными целями. Они не боятся выражать свои убеждения. https://rostov.spaxam.net/ Контакт с ними нередко получается насыщенным. Они любят слушать собеседника и строить глубокие отношения. Такие девушки вдохновляют окружающих своей неповторимостью. Они следуют своим направлением, не подстраиваясь под навязанные ожидания.
Michaeltut
October 27, 2025Нейросетевые онлайн-сервисы для мониторинга источников становятся всё более удобными. Они дают возможность изучать открытые данные из социальных сетей. Такие боты подходят для аналитики. Они способны оперативно анализировать большие объёмы информации. бесплатный глаз бога тг Это позволяет создать более точную картину событий. Некоторые системы также включают удобные отчёты. Такие сервисы популярны среди исследователей. Совершенствование технологий делает поиск информации эффективным и быстрым.