Chapter 15:
India and the himalayan area

INTRODUCTION
The Indian subcontinent has long been regarded as the probable place where smallpox originated—its traditional endemic home. It was a disease described in early Indian writings and enshrined both in Hindu religious belief and throughout the country in temples to the smallpox goddess. Variola major, with a case-fatality rate of 20% or higher, was the only variety of smallpox found in India and, as recently as the 1950s, it is estimated to have killed more than a million persons annually. Many held the view that because of population density, or for other ill-defined socio-cultural or epidemiological reasons, the eradication of smallpox in India would ultimately prove impossible. This belief had its roots in the behaviour of cholera, which for centuries had been confined to the riverine areas of the Indian subcontinent. In the 1830s, cholera spread across the world in the first of seven global pandemics, only to disappear over time, except from the Ganges river plain (Fig.15 .1). Although cholera was a bacterial disease with wholly different epidemiological characteristics, many believed that there were unique, yet unrecognized features of this area which would doom a smallpox eradication effort as certainly as an effort to eliminate cholera.
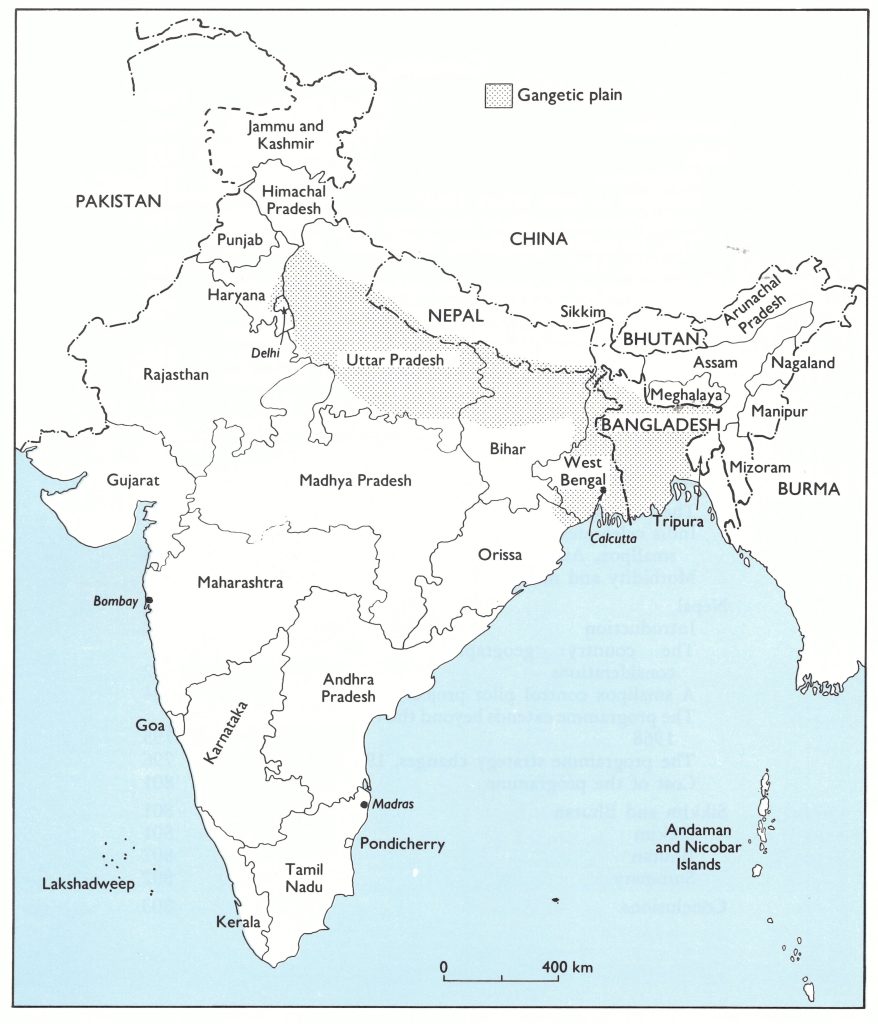
Fig. 15.1. Bhutan, the states and union territories of India, and Nepal. Many of the most densely populated areas in the region are in the Gangetic plain. In India, Karnataka was known as Mysore until 1973; Arunachal Pradesh was the North East Frontier Agency until 1971; and Sikkim became a state in 1975. Bangladesh was East Pakistan until 1971.
There were other reasons for pessimism . In area, India was the world’s seventh largest country but second only to China in size of population. Of the 1100 million people living in areas which had endemic smallpox in 1967, 513 million (47%) lived in India. The most densely populated zone was the Ganges river plain in the north (Fig. 15.2), some 2400 kilometres long and 240-320 kilometres wide. Sharing borders with India and epidemiologically related to it were the 2 small Himalayan mountain kingdoms of Nepal (population 10.8 million) and Bhutan (population, 987 000), and the Indian protectorate of Sikkim (population, 196 000). (Sikkim became an Indian state in 1975.)
A smallpox eradication campaign had begun in India in 1962 (Fig. 15.3) but, despite an intensive and costly effort, smallpox was still widely prevalent in 1967 and substantially underreported throughout the country. A pilot smallpox control programme had been launched in Nepal in 1962, but cases continued to be reported from the only 3 districts which reported at all. Little was known in 1967 about the situation in Bhutan and Sikkim.
In 1967, the meagre resources available to WHO precluded the provision of meaningful support to all endemic countries in Asia. A programme was already established in India, although functioning poorly, and India at that time requested international assistance only to permit the acquisition of equipment for vaccine production. Thus, WHO’s assistance in Asia was directed to the less populous endemic countries-Afghanistan, Indonesia, Nepal and Pakistan (which then included East Pakistan, later to become Bangladesh) . It was hoped that successful programmes in these countries would eventually permit the release of significant resources in support of the Indian national programme if required. A joint India-WHO team assessed the Indian programme in 1967 and, subsequently, WHO staff from Headquarters and the Regional Office for South-East Asia in New Delhi held frequent meetings with Indian government staff. Until 1970, however, progress was slow. That year, a WHO-India agreement was signed which provided for WHO support for field activities. During the following 3 years considerable progress was made in the southern and western states but little in the northern, densely populated Ganges river plain. Meanwhile, country after country in Africa, South America, and Asia succeeded in interrupting smallpox transmission. By June 1973, only 5 endemic countries remained, of which 4 were adjoining countries in Asia (Bangladesh, India, Nepal and Pakistan) and the fifth was in Africa (Ethiopia).
In June 1973, Indian and WHO staff decided on an ambitious campaign to involve more than 100 000 local health staff throughout India in a village-by-village search for cases . Such searches would be completed in 7-10 days and would be undertaken monthly in heavily infected areas and less often in areas in which few or no cases were being reported. Outbreaks, when found, would be contained by local health staff assisted by state and district surveillance teams. With this strategy, it was hoped that transmission might be sharply curtailed by January 1974 and perhaps interrupted as early as June 1974. The problems proved far more formidable than had been foreseen. Although the original optimistic target was not met, transmission was interrupted in May 1975, less than 2 years after the special programme had begun-a considerable achievement in so vast a country.
In sheer magnitude and scope, in innovation and adaptation to adversity, in dedication and enthusiasm, in the degree of international cooperation and understanding, the Indian programme from September 1973 onwards was one of the finest endeavours of the global campaign. It is impossible to do full justice to this vast programme in a single chapter. Fortunately, a number of publications describe the overall programme, focusing primarily on its concluding phase. Two books, The Eradication of Smallpox from India (Basu et al ., 1979) and The Management of Smallpox Eradication in India (Brilliant, 1985), are particularly valuable. .Special issues of the Indian journal of public health (January-March 1978) and The journal of communicable diseases (August 1975) also provide important information.
This chapter includes an account of the closely related and ultimately well-executed Nepalese programme, of which there is no published description . It concludes with such information as is available regarding activities in Bhutan and Sikkim, which experienced only infrequent importations after 1966.
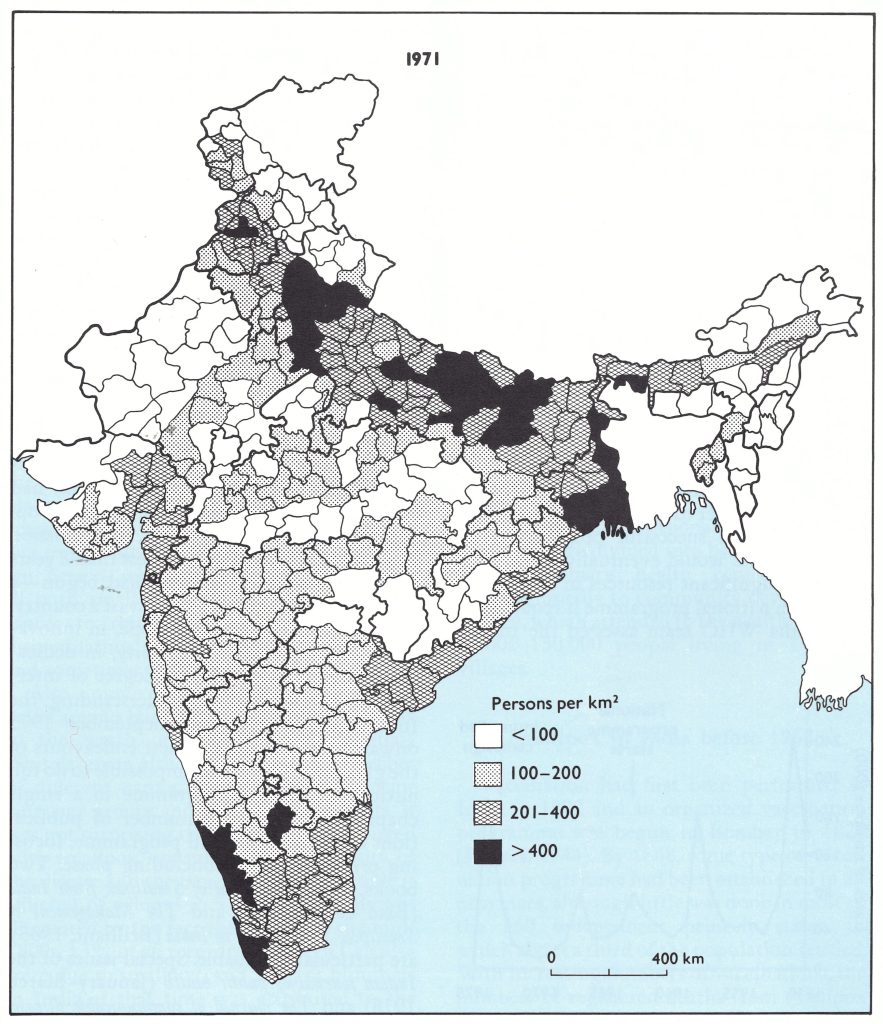
Fig. 15.2. India: population density, by district, 1971.
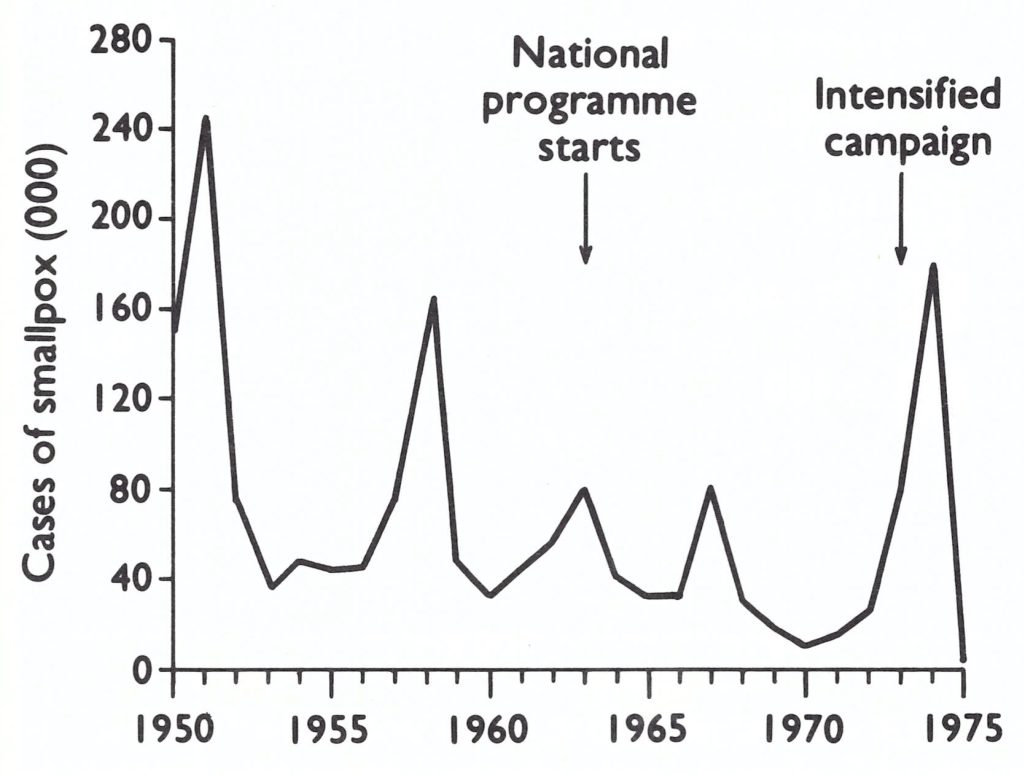
Fig. 15.3. India : number of reported cases of smallpox, by year, 1950-1975.
INDIA
Background
India’s immense size and vast population, of whom more than 80% lived in rural areas, was but part of the challenge. In India, as well as in East and West Pakistan, there was an extraordinary movement of population from place to place for purposes of business and attendance at marriages and funerals. Numerous religious pilgrimages and gatherings attracted huge crowds, sometimes amounting to millions of people. Uncountable hundreds of thousands travelled throughout the country on 10 800 daily trains. The state transport system, including buses and other motor vehicles, alone carried some 10 million passengers (about 2% of the population) each day. Reflecting the extent of internal migration, the 1961 census showed that a third of the population was enumerated outside their places of birth that year; during succeeding years, mobility substantially increased. This was important in smallpox transmission. Often, persons who were exposed to or became ill with smallpox would journey long distances to return to their home villages, disseminating smallpox when they arrived and sometimes in the course of the journey.
Also unique to the Indian setting was a belief among Hindus that attributed smallpox to the wrath of a goddess, called Sitala (Shitala) mata although known by a number of different names among India’s 15 major language groups and 250 regional dialects. It was not surprising that a deity was associated with smallpox, considering the antiquity of t he disease and the large numbers of people it afflicted, of whom 1 in 5 died. Its severity was illustrated by the fact that as late as the mid1800s, 13% of all recorded deaths in Calcutta were due to smallpox, and 75% of blindness in India at that time was attributed to the disease (Rogers, 1944). Some persons resisted vaccination, fearing that it would anger the goddess. Religious ceremonies in her honour were common at specially dedicated temples as well as in people’s homes.
Finally, there were the complexities of the administrative structure. India, a parliamentary democracy, was divided into 21 states and 9 union territories. (In 1975, Sikkim became the 22nd state.) These were further subdivided into 393 districts and 5247 community development blocks (Table 15.1). Of the 575 721 villages enumerated in the census of 1971, approximately 319 000 had a population of less than 500 ; only 6333 had a population of more than 5000. There were only 4 cities with more than 2 million inhabitants: Calcutta (7 million), Bombay (6 million), Delhi (3.6 million), and Madras (3 million).
At the national level, responsibility for health programmes was shared by the Minister of Health, a political figure; the Secretary of Health, a non-technical administrative executive officer; and a technical Director-General of Health Services, who implemented health programmes. Substantive decisions required the collaborative understanding of all three. In each state the administrative structure rcplicatcd the national one. Although there was some variation in the type of organization from state to state, there were district health units in most, directed by a chief medical officer of health (or civil surgeon). In large states, several districts were grouped in divisions and, for each, there was a divisional medical officer. Districts were divided into basic health units termed primary health centres (corresponding usually to community development blocks), which attended to the health needs of 80 000-150 000 people living in 150-350 villages.
Table 15.1: Indonesia: population and number and category of administrative units, by island, 1968
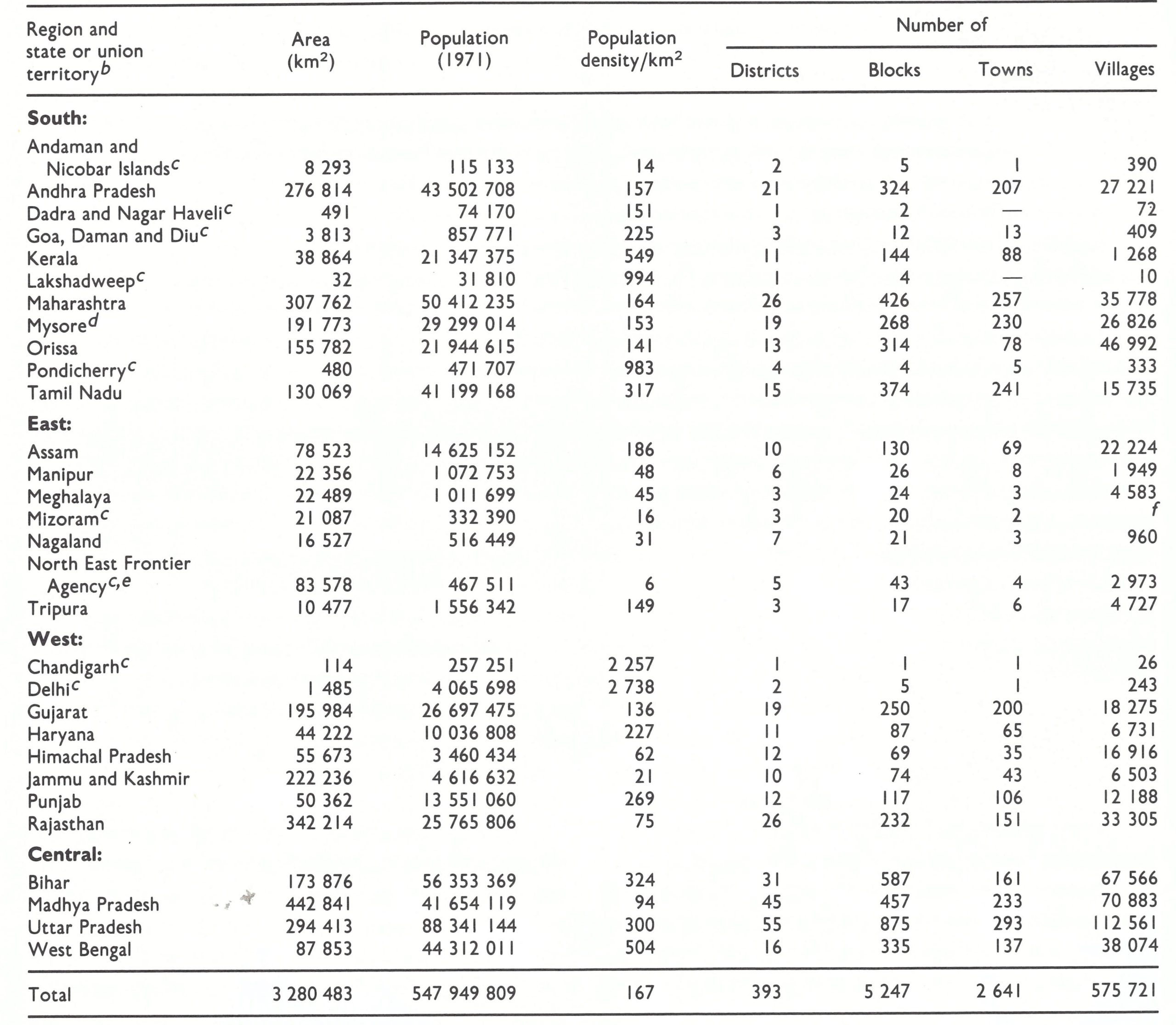
a From Basu et al.(1979), including the population estimates. United Nations (1985) data show a total population of 564 207 000 for India as a whole in 1971.
a The regional divisions (South, East, West and Central) shown in this and other tables were designated by the staff of the Intensified Smallpox Eradication Programme on the basis of the epidemiological characteristics of smallpox and the status of the programme in 1972. Reference is made to them in describing the progress of the programme. Sikkim, which became a state of India in 1975, is not listed.
cUnion territories.
dBecame the state of karnataka late in 1973.
e
Became the union territory if Arunachal Pradesh in 1972.
f Included in Assam
Smallpox in India before 1962
Vaccination had first been performed in India in 1802 and an organized vaccination programme was begun in Bombay in 1827 (Rogers, 1944). By 1868, some type of vaccination programme had been established in all provinces, although little was done in most of the 560 independent princely states, in which about a third of the population resided. With increasing numbers of vaccinations, the numbers of registered deaths from smallpox declined between 1878 and 1937, despite a progressively improving system for the registration of deaths and a growing population (Table 15.2). Data comparable to those provided by Rogers could not be obtained for the period 1937-1961, but data for 1962-1971 are available—1962 being the year in which India commenced a special national smallpox eradication programme (see below). It is not known how complete the registration of deaths may have been at different times. However, studies conducted during the early 1970s showed that even then, the number of reported cases of, and presumably deaths from, smallpox represented less than 5 % of the cases and deaths that had actually occurred.
Vaccination programmes were gradually extended throughout most of the country and, following India’s independence in 1947, to the remaining princely states. Thermolabile liquid vaccine was the only vaccine available and many of the vaccinations performed must have been unsuccessful. This vaccine was produced in 14 laboratories in 11 different states. As in Pakistan, vaccinators who were recruited and hired by the local administrative organization and termed “local body vaccinators” performed the vaccinations. The programme of vaccination provided only partial control of smallpox, but because vaccination was widely available and variolation was forbidden by law, the latter practice ceased and, by the late 1950s, was no longer a problem in India.
Table 15.2: India: population, number of recorded deaths from smallpox, average annual number of vaccinations, and percentage of population vaccinated annually, 1878-1937 a (British India) and 1962-1971
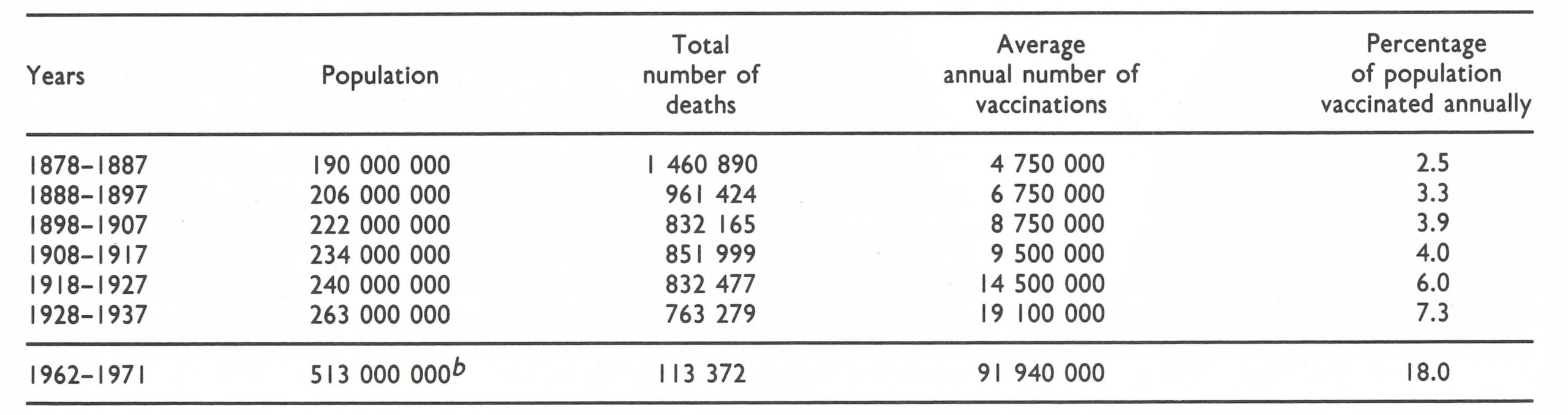
a From Rogers (1944).
bUnited Nations(1985) estimate for 1967.
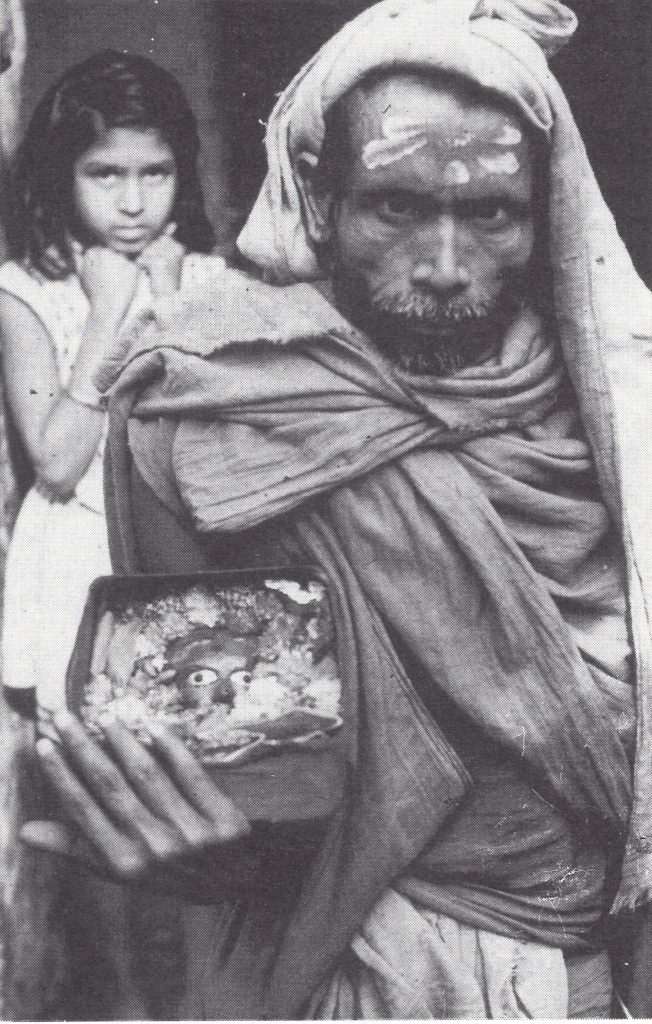
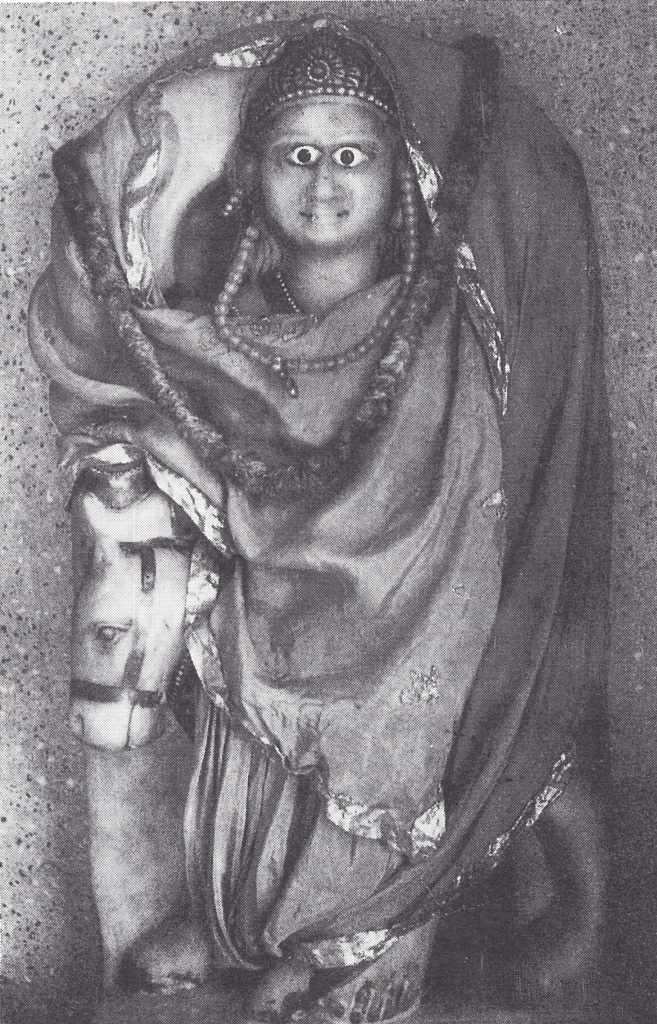
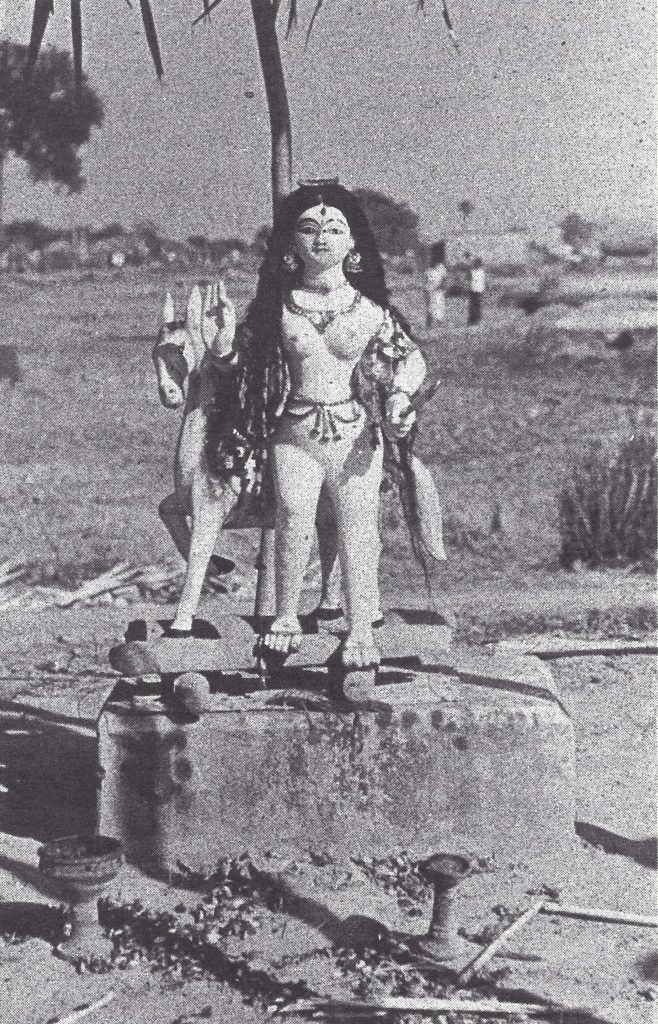
Plate 15.1. The goddess of smallpox has long been worshipped throughout the Indian subcontinent. She is usually portrayed as a woman riding on an ass, carrying a broom in one hand and a waterpot in her other arm. In northern India, she was known as Sitala mata,sitala meaning the cool one, and mata meaning mother. Though worshipped primarily by Hindus and Jains, in Nepal she was incorporated in the Buddhist pantheon as Ajima, the mother of Gautama Buddha. Offerings were made at temples dedicated to her and to images in the home; annual festivals were held on her feast day. Beliefs and practices differed from place to place and the goddess was variously considered to have powers to prevent or cure the disease as well as to inflict it.
India’s National Smallpox Eradication Programme, 1962
In June 1959, one month after the decision of the Twelfth World Health Assembly to undertake a global eradication programme, an Expert Committee of the Indian Council of Medical Research recommended that a National Smallpox Eradication Programme should be established. The vaccination campaign that resulted was of heroic dimensions and, although failing in its goal to eradicate smallpox, it served to extend vaccination to all but the most isolated villages and created an army of workers and a momentum which provided a foundation for the subsequently successful eradication effort.
Pilot projects were first developed in one district per state to work out methodology and to develop estimates of costs and personnel requirements (Fig. 15.4). The projects began in 1960 and concluded in March 1961 (India, Ministry of Health and Family Planning, 1966).
The essence of the strategy called for a specially recruited team to move systematically from house to house and from village to village throughout a district in an effort to vaccinate or revaccinate not less than 80% of the population. With this proportion vaccinated, it was expected that a sufficient number of persons would be immune so that smallpox transmission would terminate spontaneously. The vaccination team was preceded by enumerators, who listed in a large multi-page register the name of each person along with his or her address, age, sex and previous history of vaccination or of smallpox. One register was compiled for each village or defined area in a city and was intended to be used during the subsequent 20 years. After enumeration had been completed, the register was given to the vaccination team, which then endeavoured to vaccinate those who were listed. The register was next given to an inspector, who was to check each vaccinee to ensure that vaccination had been successful. Subsequently, local health unit vaccinators (1 for every 50 000-70 000 persons) were assigned responsibility to vaccinate those missed in the mass campaign (“mopping-up vaccination”), to maintain the registers, to revaccinate everyone every 5 years and to vaccinate contacts when cases were discovered. Performance in the pilot projects was poor. In a target population of 23 million, only 12 million (52%) were vaccinated. No evaluation of the programme was conducted nor was smallpox incidence monitored. Nevertheless, as happens only too frequently, the pilot projects were followed almost immediately by the introduction of a national programme.
The USSR offered freeze-dried vaccine, which was largely but not entirely intended to replace the thermolabile liquid vaccine ; the United States Agency for International Development made a grant of rupees equivalent to US$2 million; and UNICEF pledged equipment for vaccine production. Eventually, the USSR provided 650 million doses of vaccine and the USA, between 1961 and 1967, contributed the rupee equivalent of US$23 million, which had been generated by the sale of foodstuffs provided to India (termed Public Law 480 funds).
Since health programmes in India are constitutionally a state responsibility, the principal administrative direction of the smallpox eradication programme was delegated to the states. Only 2 professional staff provided coordination at the national level. However, because smallpox was considered a national priority, the programme was “centrally sponsored”; the states were reimbursed by the central government for all non-recurring expenditures and for 75% of recurring costs.
The government created 152 units, each of which was expected to vaccinate about 3 million persons in an “attack phase” lasting 2-3 years. Each unit consisted of a supervising officer (usually a physician), a paramedical assistant, 60 vaccinators, 12 inspectors, 12 enumerators and 2 health educators. Each unit was assigned 3 vehicles. In all, more than 13 000 persons were employed, most of whom were newly hired and trained. The programmes were launched in 1962 and 1963.
Fig. 15.4. India: pilot project districts for the National Smallpox Eradication Programme (NSEP), 1960-1961; state programmes assessed in 1967; and municipal areas assessed, 1963-1964.
Between 1962 and 1966, 440 million vaccinations were reported to have been performed. It was an impressive number but it did not signify that this many persons had been rendered immune . The first indication of difficulties was observed in New Delhi in the winter of 1963 (Gelfand, 1966). Between December 1962 and May 1963, 346 cases of smallpox occurred in an area in which the number of vaccinations performed was equivalent to more than 80% of the population. Sample surveys conducted in 18 representative areas revealed that, in fact, vaccinations had been given to only 63% of the population and that, of these, 86% had been successful. It was therefore concluded that only 54% of the population had been successfully vaccinated. This discrepancy between the number of vaccinations reported and the number of people actually rendered immune was attributed to a falsification of records and the repeated vaccination of readily accessible groups, particularly schoolchildren. The government was disturbed by these findings and asked India’s National Institute of Communicable Diseases to under take similar surveys in other states. Five were subsequently conducted in districts which reported that the number of vaccinations performed was equivalent to 80% or more of the population. In operational terms, this meant that the mass campaign “attack phase” had been completed or was about to be completed and the “maintenance phase” was due to begin; during the latter phase the established health services would assume the responsibility for sustaining levels of vaccinial immunity and for controlling outbreaks.
The findings of the National Institute’s teams were not encouraging (Gelfand, 1966). The family registers—printed sheets sewn together in a large book—were supposed to include the name of each individual in a defined area and to provide a permanent record of vaccination status. Field assessment showed that many registers had already been lost or were so worn as to be unusable; many names had been omitted; and the clerical task of keeping the registers up to date was overwhelming. It was found, for example, that some individuals who had died as long as a year before were recorded as having just been successfully revaccinated. However ineffective the family registers may have been, their use continued in many areas until the late 1960s.
Recommendations for Primary Vaccination in Early Childhood, 1963
The programme's recommendations for primary vaccination were taken from a publication of the British Ministry of Health and distributed in a circular to all administrative staff in 1963. It stated that primary vaccination "should be carried out some time before the age of two years, preferably during the second year" and listed as specific contraindications: "failure to thrive, exposure to infectious disease, septic skin conditions, infantile eczema and other allergic conditions, hypogammaglobulinaemia and corticosteroid treatment" (India, Ministry of Health and Family Planning, 1966). Although perhaps appropriate for the United Kingdom, where smallpox cases were only occasionally imported, the recommendations were inappropriate for India, where many children were exposed to smallpox from birth, where the risks associated with vaccinating most of those with the listed contraindications were much less than the risk of death due to smallpox, and where most vaccinations were performed by scarcely literate vaccinators who could not be expected to recognize many of the conditions note. Indeed, if all the contraindications had been carefully observed in India, few children would have been vaccinated. Sensibly, the recommendations were largely ignored by most vaccinators, although some did not vaccinate children who were ill with fever or had skin infections. Throughout India, 3 months of age was generally respected as the lower age limit for vaccination. By 1970, a more realistic and appropriate policy had evolved. It called for vaccination from the time of birth and recognized no contraindications except one: vaccinators were instructed not to vaccinate seriously ill persons who might be expected to die over the succeeding day or two and whose death might thus erroneously be attributed to vaccination.
The proportion of the population found to have been successfully vaccinated was less than the reported 80% in all districts, ranging from 54% to 73%. Substantially lower levels of vaccination coverage were found in urban districts than in rural areas. Although the numbers reported to have been vaccinated were probably somewhat inflated, the more basic problem was similar to that observed in New Delhi: the most accessible individuals—schoolchildren, for example—were being vaccinated as often as every 6 months, while pre-school children and persons in the lowest socio-economic groups, among whom smallpox was most prevalent, were not being vaccinated at all.
In areas which had entered the maintenance phase of the programme, the National Institute’s teams evaluated performance by examining children aged 3-12 months for the presence of a vaccination scar. After the mass campaign, all children on reaching 3 months of age were supposed to be vaccinated by staff assigned to the local primary health centre. In one district, 88% of children 3-12 months old had vaccination scars, but in the remaining districts the corresponding proportions were, respectively, 2%, 9%, 23% and 38%. The National Institute’s teams investigated reported cases of smallpox in the maintenance phase areas and in each district they found many other cases which had not been detected.
In view of the fact that the districts evaluated were among the few which had reported that they had achieved the target of 80% coverage, it was apparent that the programme had fallen far short of expectations. An internal document issued by the United States Agency for International Development in November 1964, justifying the programme’s continued use of United States rupee funds, stated prophetically “Eradication of smallpox in India . . . is at least 10 years hence . . .”
Despite the extensive vaccination programmes, 30 000-40 000 cases of smallpox were reported each year during 1964-1966 (Table 15.3). Because millions had been rendered immune through vaccination, a decrease in the true incidence of the disease is assumed to have occurred, although such a decrease might have been masked by a more complete notification of cases. However, no specific measures had been taken to improve the reporting system and little is known about its efficacy at this time beyond the recognition that only a small proportion of cases was officially recorded.
Serious deficiencies extended throughout the reporting network at each level responsible for data collection and transmission. In villages, cases of smallpox, as well as of plague and cholera, were supposed to be reported to the primary health centre by the village headman in most states or, in some, by the village watchman (chowkidar)—a poorly paid, sometimes illiterate employee of the village council. Some villages submitted reports but many did not. Health workers, assigned to primary health centres, paid little attention to the reporting of smallpox.
An additional problem was that villagers sometimes deliberately hid cases to avoid vaccination, to which they objected for religious reasons or because they feared the painful, infected lesions which so often resulted from the use of the rotary lancet. Some persons who had contracted the disease concealed themselves to avoid being taken forcibly to congested and understaffed hospitals. The cases that came to the attention of primary health centre personnel and district officials were frequently not reported by them to higher authorities because they were afraid of being punished by their supervisors. Many supervisory staff acted on the premise that the occurrence of cases in an area was prima facie evidence that the health staff had done an inadequate job of vaccinating the population and so deserved punishment.
At that time, the Central Bureau for Health Intelligence, the national statistical office, simply recorded data, showing little interest in whether the districts and states reported at all. Even the simple task of recording data was confounded by a system, unique to India, which required each district to report each week the number of cases detected according to the week of onset of the cases. This differed from the practice in other countries, in which a weekly report was compiled giving the number of cases of smallpox detected that week, irrespective of the date of onset. Thus, instead of receiving and recording one number for each of India’s 393 districts, the Central Bureau received new reports of cases for each district extending back weeks or even months. All numbers were entered in a great ledger, past numbers corrected and new totals compiled. Similar procedures were followed by district and state statistical offices. However, many of these offices did not forward reports of cases which had occurred several weeks or months previously, considering them not to be of current interest.
Table 15.3: India: number of reported cases of smallpox, by state or union territory, 1962-1975
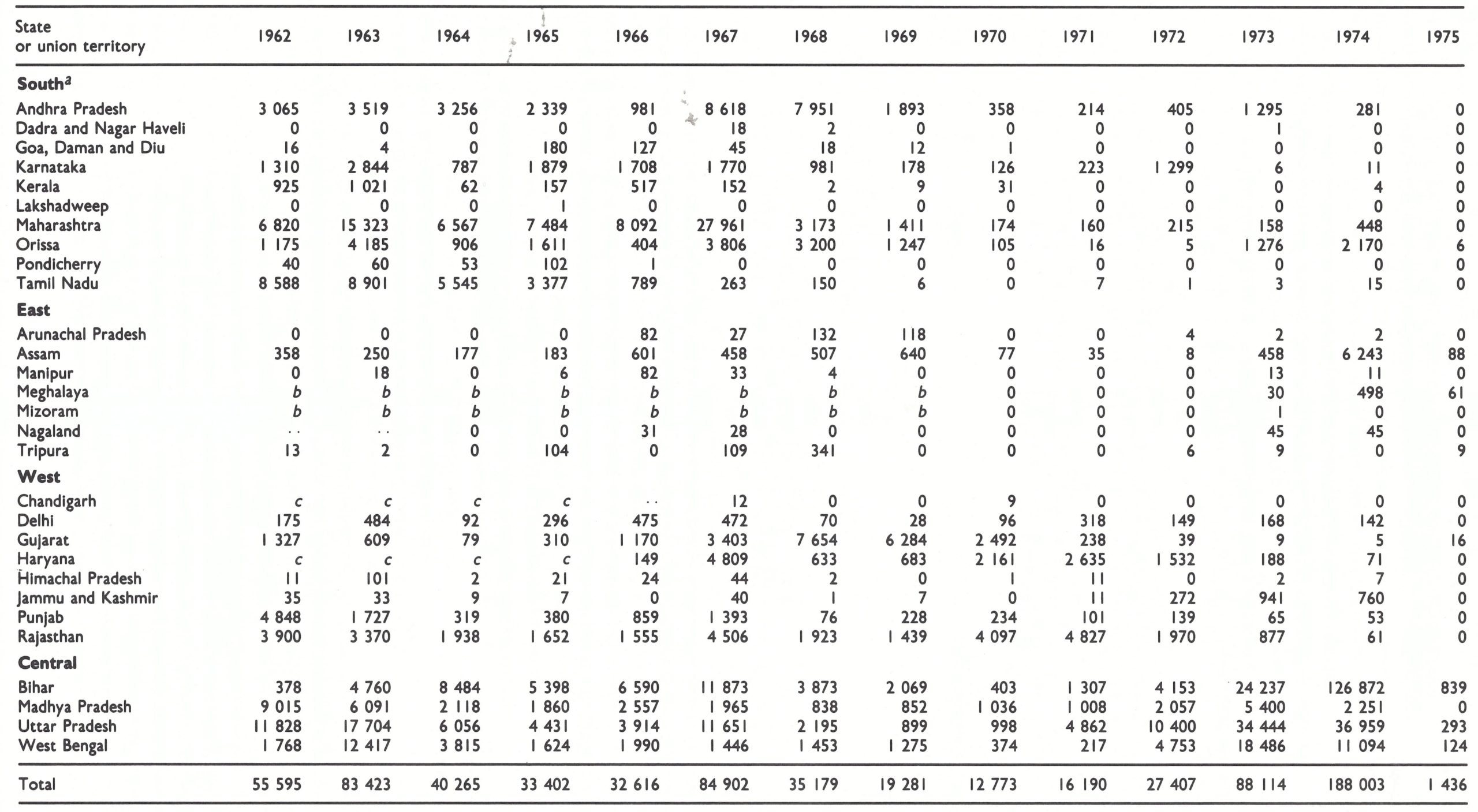
a No cases were reported during this period in the union territory of Andaman and Nicobar Islands
b Part of Assam.
c Paart of Punjab.
The National Smallpox Eradication Programme Advisory Committee held a meeting in November 1965 to decide what should be done when, in March 1966, the attack phase-the mass vaccination campaign was scheduled to be completed and the programme throughout the country would enter its maintenance phase (India, Ministry of Health and Family Planning, 1966). The Director of the National Smallpox Eradication Programme, Dr K . M. Lal, expressed optimism that there would be a “further steep fall” in incidence in 1966-1967 but was concerned about the large number of persons who still remained unvaccinated. Because independent assessments had shown that equating the numbers of recorded vaccinations with the numbers of persons successfully vaccinated was erroneous, it had been decided that a target of 100% vaccination coverage was necessary (a strategy endorsed by a WHO Expert Committee on Smallpox (1964) at Dr Lal’s suggestion). Dr Lal doubted that a satisfactory maintenance s vaccination programme could be conducted by the existing primary health centre staff, malaria workers, midwives and others. The 1963-1964 assessment had shown this. He favoured a plan which had been suggested to and approved by the Advisory Committee in 1963, whereby 1 smallpox vaccinator would be provided for every 10 000-15 000 persons in rural areas and for every 20 000 persons in urban areas. Such a scheme would be costly and, by any standard, would involve a generous deployment of manpower. Assuming that a vaccinator worked 200 days a year, he could theoretically vaccinate the entire population in a rural area during the space of a year by performing as few as 50-75 vaccinations a day. Dr Lal and many members of the Advisory Committee were reluctant to end the attack phase with its mass vaccination units until cases had ceased to occur in a district. Various members proposed intervals of up to 3 years as the desirable time for an area to be smallpox-free before it entered the maintenance phase and vaccination was turned over to basic health staff or local body vaccinators. A special subcommittee was appointed to explore the question further. However, budgetary considerations intruded. The government was forced to decrease expenditure, and the attack phase programme, with its 152 mass vaccination units, was terminated. Special vaccinators for smallpox continued their work in most areas, but in a few, a handful of poorly trained and poorly supervised basic health workers were expected to add vaccination to other tasks.
Meanwhile, vaccine production institutes at Patwadangar, Belgaum, Guindy (Madras)and Hyderabad struggled unsuccessfully to produce the large quantities of freeze-dried vaccine required. By 1966-1967, they were producing only 1.4 million vials (enough to vaccinate about 20 million people). The USSR continued to provide approximately 500 000 vials each month, but even this was not enough. Emergency requests to other governments were regularly channelled through WHO, and several million additional doses were received from the Netherlands, Switzerland and the United Kingdom, but none of these sources could supply substantial quantities since none had laboratories equipped for the large-scale production required. Accordingly, the thermolabile, questionably potent, liquid vaccine continued to be used in a number of states since it was felt that unsatisfactory vaccine was better than no vaccine at all.
Vaccination Using the Rotary Lancet
Until the bifurcated needle began to be used in 1970, vaccination was an elaborate and time-consuming ritual. Each vaccinator had a helper who carried a vaccination bag, and the pair proceeded from house to house to identify individuals to be vaccinated. When a candidate was found, the helper unpacked the bag and the following routine, prescribed by the Directorate of Health Services, was followed (India, Ministry of Health and Family Planning, 1966):
- Check your kit bag to make sure that all the articles are there.
- Perform vaccinations in a shady place to prevent exposure of the lymph to the sun.
- Before vaccinating a person, wash your hands thoroughly with plain soap and water.
- Sterilize both the scoop end and the toothed end of the rotary lancet in water brought to the boil beforehand and kept boiling. Hold the middle of the lancet with your thumb and index finger and dip the two ends in boiling water alternately for a minute each. If quick work is required, hold the two ends of the rotary lancet alternately over a naked flame. After sterilizing the lancet, keep it on a special wooden stand, taking care to see that the two sterilized ends do not come into contact with any other object.
- Scrub the site chosen for vaccination thoroughly with plain soap and water. Wipe it dry with a sterile swab.
- Take the vaccine tube from the ice container, unscrew its cap, take the lymph on the scoop end of the rotary lancet, recover the tube and put it aside on a special holder. Place the lymph on the required number of spots, on the outer surface of the middle third of the left upper arm for primary vaccinations, and on the front surface of the left forearm for revaccinations. Place the toothed end of the lancet on the skin through the drop of lymph. Rotate the lancet with gentle and even pressure so as to produce a light circular cut without drawing blood. After making the insertion, rub in the lymph into the scarified area with the scoop end of the lancet. Detain the person for 15 minutes so that the lymph may have time to get absorbed into the skin.
After one or several vaccinations had been performed at a house, the bag was repacked by the helper, and the vaccinator and helper proceeded to the next house.
Vaccinators who failed to permit the lancet to cool sufficiently or who were were too vigorous in pressing it into the skin inflicted painful lesions. Because the lancets were often contaminated, the vaccination lesions frequently became septic. The scars which remained sometimes resulted from the growth of vaccinia virus but sometimes were caused by bacterial infection alone. Not surprisingly, many vaccinators were offered money notto vaccinate.Given the routine and the need to record the name of each vaccinee in a large register, it was unusual for a vaccinator to perform more than 25 vaccinations a day. When the bifurcated needle became available, the procedure was greatly simplified and both the special bags and the helpers gradually disappeared. However, the pace of vaccination, by then well ingrained, did not substantially increase.
The Herculean effort to eradicate smallpox through mass vaccination, launched so enthusiastically in 1962, had all but come to a halt by the time the Nineteenth World Health Assembly, in May 1966, decided to embark on the Intensified Smallpox Eradication Programme. The Indian delegate to the Health Assembly, commenting on the new initiative, pointed out that India would need 180 million doses of vaccine annually, of which it would never be able to produce more than 60 million doses, and expressed the hope that WHO could meet the projected deficit. He cautioned the delegates that unless good basic health services were developed “it would be very difficult indeed to maintain the immunological status temporarily reached” in a mass campaign (World Health Organization, 1966c).
In December 1966, Henderson, who had recently been appointed Chief of the newly constituted Smallpox Eradication unit at WHO Headquarters, arrived in New Delhi to participate in his first intercountry smallpox eradication seminar, attended by representatives from countries in WHO’s South-East Asia Region. It was not an auspicious beginning, as India, which then accounted for one-third of the world’s cases, announced at the seminar that it had terminated its attack phase and had reverted to a programme of maintenance vaccination.
The Intensified Smallpox Eradication Programme Begins, 1967
The advent of the Intensified Programme in India found a discouraged staff. Dr Lal, the director of the National Smallpox Eradication Programme since 1962, retired and, because the attack phase had been terminated, was not replaced. This left at the national level only one medical officer, Dr Mahendra Singh, a Deputy Assistant Director—General of Health Services. Although he was overwhelmed by the tasks of giving some sort of direction to the remaining smallpox control activities and of providing the necessary reports to Parliament—among many other duties—Dr Singh tried valiantly to stimulate the host of vaccinators distributed across India. He dispatched numerous cables and letters asking state health directors to take action to control epidemics reported officially to him or, as often, through the press. Vaccination targets were established for each state and those who failed to meet their goals were given forceful reminders. The number of reported vaccinations diminished, however, from 139 million in 1963 and 130 million in 1964 to 96 million in 1967 (Table 15.4). Vaccine distribution was also Dr Singh’s responsibility, and a continuing problem because reserves were few and requests to replenish vaccine stocks in state and district offices were often not forthcoming until supplies had been exhausted. Government regulations required that Dr Singh should travel by train or bus, often a 1-or 2-day trip to reach distant and populous state capitals. In each state, there was only one official responsible for smallpox, and he was usually assigned responsibility for one or more additional programmes. The smallpox eradication programme and its still extensive complement of vaccinators laboured under a severe shortage of senior, responsible staff.
Table 15.4: India : numbers of reported vaccinations, percentages relative to population, and numbers of reported cases of and deaths from smallpox, 1962-1976
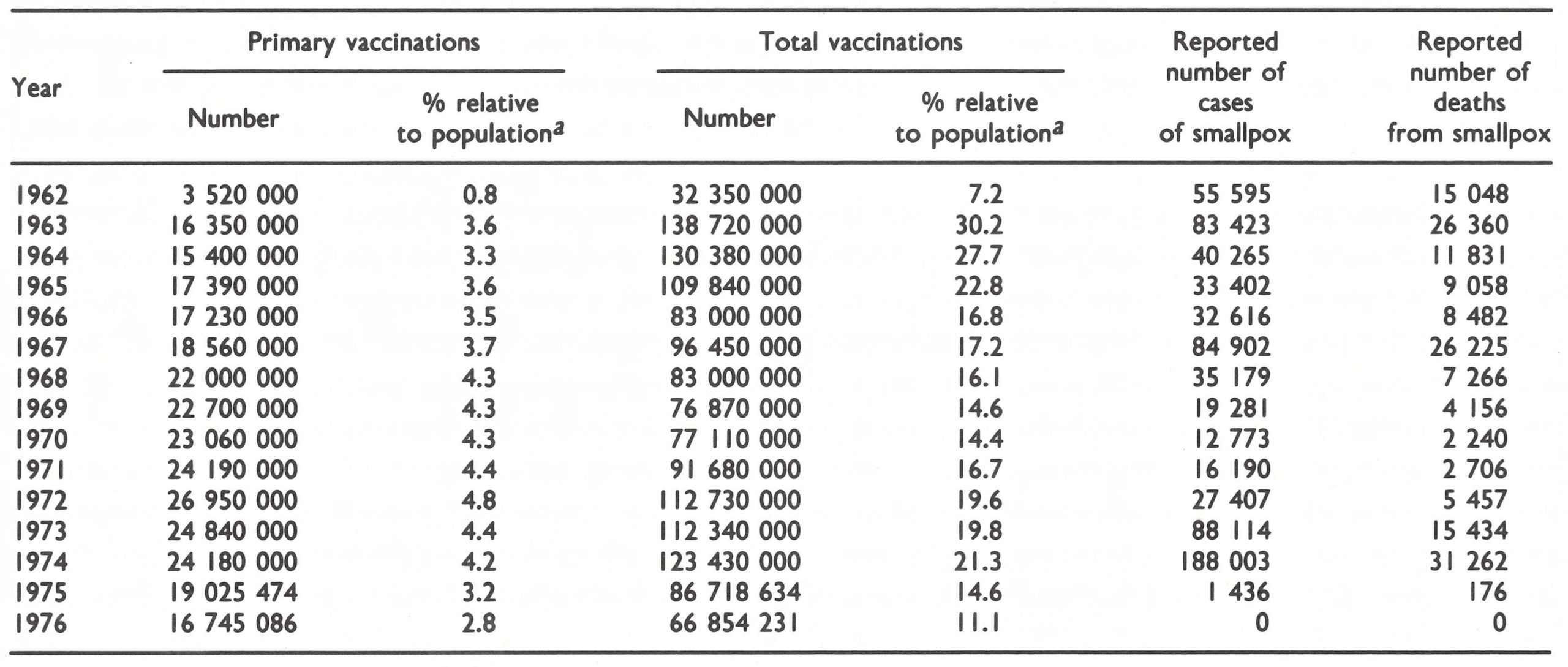
a The percentages provide an index of vaccination activity and are derived by dividing the reported total number of vaccinations performed by the estimated total population (from Basu et al .,1979). The figures do not provide a measure of the proportion of the population newly immunized or whose immunity was boosted. Vaccination was sometimes unsuccessful and some individuals were vaccinated two or more times in a year. Moreover, the reported total numbers of vaccinations performed were sometimes inflated.
Assessment of the Programme in India, October 1967
In 1967, smallpox incidence rose dramatically, eventually reaching a total of 84 902 cases, more than had been reported in any year since 1958. Concerned by this turn of events, the Indian government agreed that a joint India—WHO assessment team should appraise the situation and suggest how it might be rectified. The team’s operations were planned and organized by Dr Jacobus Keja, the adviser on smallpox eradication in WHO’s South-East Asia Region, and by Dr Singh. In India, an assessment such as this, in which WHO staff travelled to the field, was an uncommon event at that time. Most WHO advisers remained in New Delhi or occasionally visited the more populous state capitals, in which hotels were plentiful. When preparations were being made for the trip, it was discovered that the regional office had in its stores none of the commonly used Indian bedrolls that were needed when travellers stopped at government rest-houses.
The assessment team, comprising 8 senior national health officers and 8 WHO staff and consultants, spent 6 weeks in the field, from 8 October to 19 November. They visited Maharashtra and Uttar Pradesh, two states experiencing epidemic smallpox in 1967, as well as Punjab in the north-west, a state with moderate incidence, and the southern state of Tamil Nadu. The last of these states was of particular interest because of the very few cases reported (263 in 1967) among its population of nearly 40 million.
The observations made by the team are telling, as they provide an overview of the status of smallpox and of the programme in 1967. The team concluded that the programme “is still far from achieving its objective of smallpox eradication in most areas and . . . in fact, a very considerable epidemic potential exists in India at the present time.” The conclusions of its report are paraphrased below
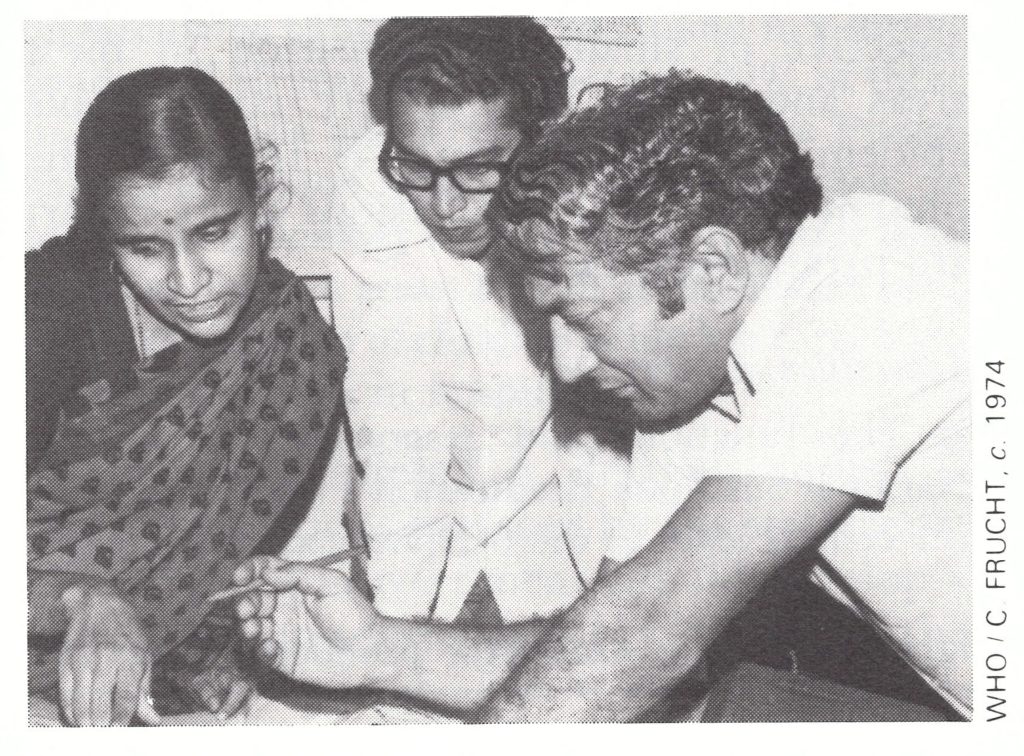
Plate 15.1. Medical officers at a primary health centre in Maharashtra State. Right: Mahendra K . Singh (b . 1928), a Deputy Assistant Director-General of Health Services, who was the only medical officer at the central level in India’s National Smallpox Eradication Programme from 1966 to 1972 and sustained the momentum of the work until additional senior Indian and WHO staff could be assigned. He continued with the programme until the eradication of smallpox in India had been certified in 1977 and was later appointed Director of the Central Bureau of Health Intelligence.
Supervision and direction
- The functions and responsibilities of the National Smallpox Eradication Programme from the central level to the periphery are fragmented among a variety of independent and semiindependent organizations. There is lack of clarity and definition of responsibilities and objectives at all administrative levels.
- The central directorate is inadequately staffed and has no effective mechanism for exercising clear guidance and direction of the programmes at state and local level. Its functions are limited to the collection from the states of inadequate data regarding smallpox incidence and the number of vaccinations performed, the distribution of imported freeze-dried vaccine, the occasional organization of meetings of state and local programme directors, the distribution of some health education material and liaison with international organizations.
- The states exhibit a great variation in organizational structure. In many, responsibility for the programme is given to a senior officer burdened with many additional responsibilities. With few exceptions, the state directorates act merely as channels for funding, the transmission of instructions and the receipt of periodic reports from the districts.
- In the districts, the district health officer has overall responsibility for the programme as one of many responsibilities. Although as many as 3 paramedical personnel act as assistants, field visits are infrequent, supervision is poor, morale is low, interest in the programme is fading and vaccine is improperly handled and stored. Vaccinators are superintended partly by local administrative bodies and municipal boards and partly by the district staff.
Programme execution
- Legislation regarding compulsory vaccination varies widely. In some states both primary vaccination and revaccination are required, while in others vaccination is not compulsory. The laws governing enforcement involve cumbersome procedures, and fines are minimal and rarely imposed.
- The plan calls for the vaccination of all newborn infants and other individuals not previously vaccinated and the revaccination of everyone every 3 years ; it also requires an assessment of “takes” among all primary vaccinees and 50% of revaccinees, as well as entry in the family registers of actions taken. The team concludes that none of the targets is being reached and that records are being falsified in most areas visited.
- The number of vaccinators is high (ranging from 1 for every 26 000 persons in Maharashtra to I for every 31 000 in Uttar Pradesh) but productivity is low [Table 15 .5]. The mean number of vaccinations performed per day ranges from 5.7 in Punjab to 24.5 in Tamil Nadu, but in some blocks the average is less than 1 vaccination per day. Vaccinator salary costs alone average 0.47 rupee (US$0.06) per vaccination, but in 3 blocks they exceed 7.5 rupees (US$0.98) per vaccination.
- Supervision, except in Tamil Nadu, consists primarily in determining whether or not the vaccinator reports for work .
- Vaccine is improperly stored, inventories are inaccurate and refrigerators are frequently lacking or not in working order.
- The number of reported cases is estimated to be no more than 10% of the actual number and notification is considerably delayed except in Tamil Nadu, in which reporting appears to be reasonably complete. Many cases which are officially notified to state authorities are not subsequently reported to the national authorities. This deficiency in notification is illustrated by the situation in Punjab, in which state records to date in 1967 showed 1370 cases, of which only 273 had been notified at the national level.
- Containment measures are insufficient. For example, in a village in Uttar Pradesh, with a population of 250, 20 cases occurred ; after containment, it was found that 20% of the unaffected children remained unvaccinated.
- Contrary to the findings of other reports, vaccination acceptance is good and the number of refusals for religious reasons is negligible. For the most part refusals stem from the unwillingness of people to be vaccinated at a time when a serious reaction might interfere with occupational responsibilities. Contributory factors are the tactlessness of some vaccinators, a crude vaccination technique and failure to inform people of the importance of vaccination. The rotary lancets waste vaccine (15 vaccinations are obtained from a vial of 0 .25 ml compared with the 25-50 vaccinations obtained when the scratch technique is used); the lancets are difficult and time-consuming to sterilize and produce unusually severe local reactions.
- Vaccination take rates are said to be 100%, but assessment from records was possible only in Bombay. The records there show a take rate of 99.7%, but, in fact, failures were being re15. corded only after 3 unsuccessful attempts . The records show a maximum take rate of 77% after a single vaccination but it is probable that the actual take rate is considerably lower.
- The family registers everywhere are incomplete and contain numerous errors. They have been abandoned in Uttar Pradesh ; in the Punjab and Maharashtra, in which a serious effort is being made to use them, vaccinators spend more than half their time on keeping them up to date.
Table 15.5: India: vaccinator productivity and salary costs per vaccination performed, 1967
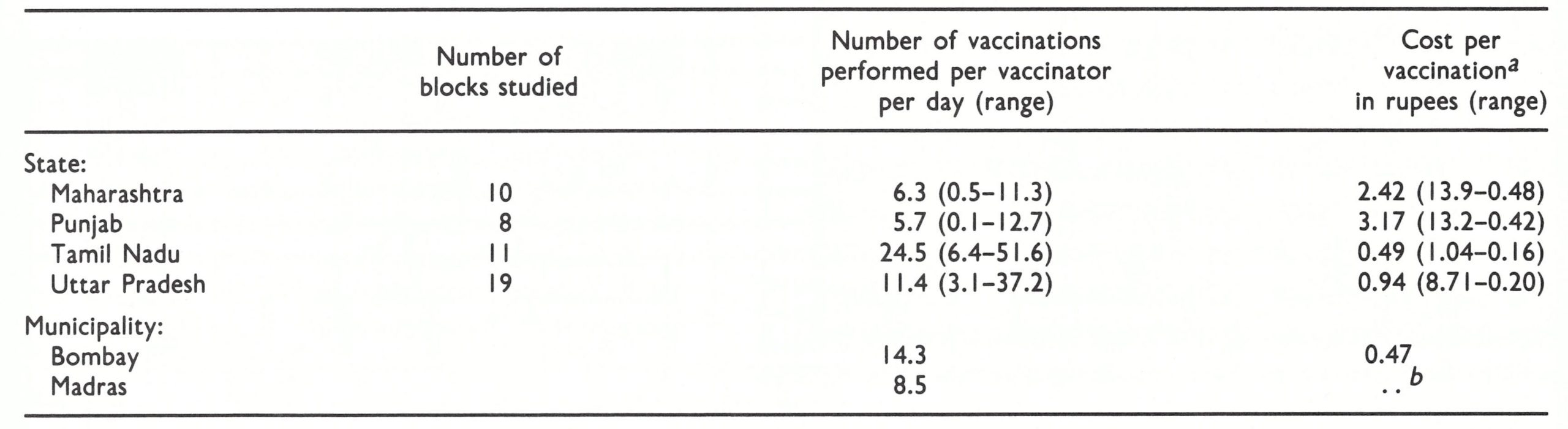
a Salary costs only—i .e., not including costs of vaccine, supervision, supplies or transport b . . . (In 1967, I rupee was equivalent to US$0.13.)
b..=data not available.
Levels of achievement
- Smallpox incidence, the ultimate yardstick for measuring success, is noted to be rising. The total number of cases by the end of 1967 will represent the greatest incidence to be recorded in a decade. Even so, this total will represent 10% or less of the actual incidence.
- Cases are occurring in all age groups, although two-thirds or more in the states assessed are found in individuals under 15 years of age [Table 15 .6].
- The proportion of the population reported to be receiving primary vaccination each year is less than 4% in all 4 states. With an estimated birth rate of 4% and many children born in previous years remaining unvaccinated, it is apparent that the number of susceptible subjects is accumulating.
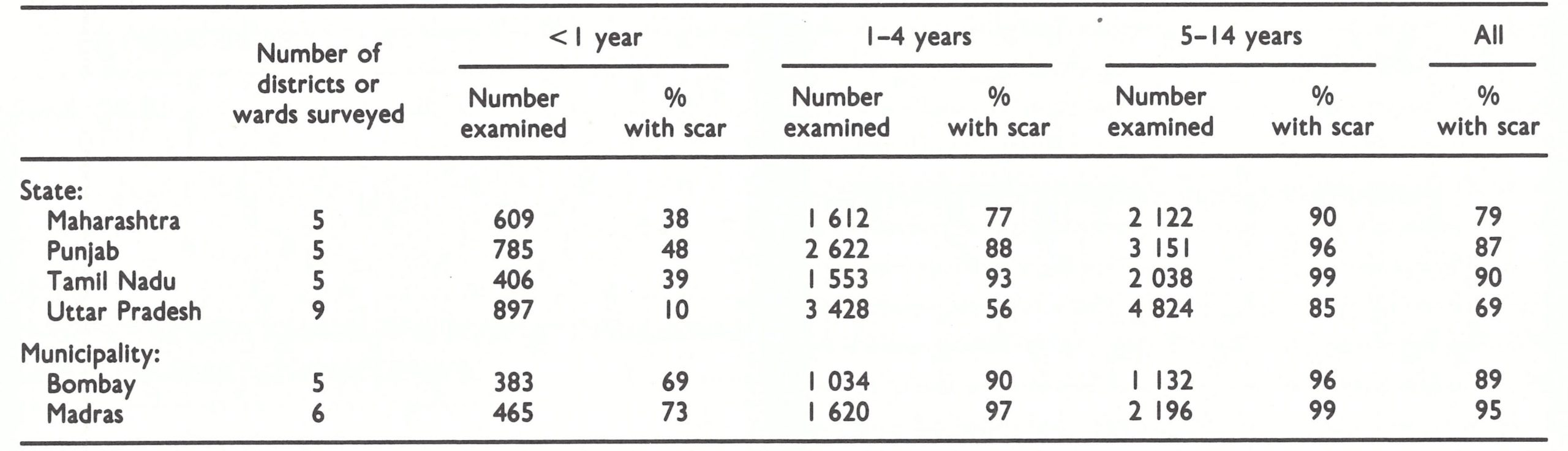
- Sample surveys conducted among individuals under 15 years of age in randomly selected districts of the 4 states and wards of the cities of Madras (Tamil Nadu) and Bombay (Maharashtra) reveal widely different levels of performance [Table 15 .7]. Uttar Pradesh has a higher proportion of unvaccinated children than was found in a survey conducted 10 years ago. In contrast, 90% of those in Tamil Nadu and 87% of those in the Punjab have vaccination scars. Vaccination levels in Madras and Bombay are substantially better than in the non-urban areas, a result attributed, in part, to the vaccination of children at birth (nearly 80% of them are born in hospital).
The team offered a detailed series of recommendations prefaced by the statement “The Central Government should develop a new and long-term strategy to meet the problem.” In brief, it recommended that greater emphasis should be given to case detection and the containment of outbreaks, especially during the summer months, when the incidence was lowest ; and that primary vaccination, including the vaccination of newborn infants, should be given priority. An increase in the personnel complement of the national directorate from 1 to 5 professionals and a concomitant extension of their scope of responsibility were also recommended, along with the strengthening of supervision at all other administrative levels. It was suggested that vaccine production should be centralized and financed under national rather than state authority, that the use of liquid vaccine should cease throughout India, that the bifurcated needle should replace the rotary lancet, and that the family registers should be abolished.
Table 15.6: India: age distribution of cases of smallpox in 4 states, 1967
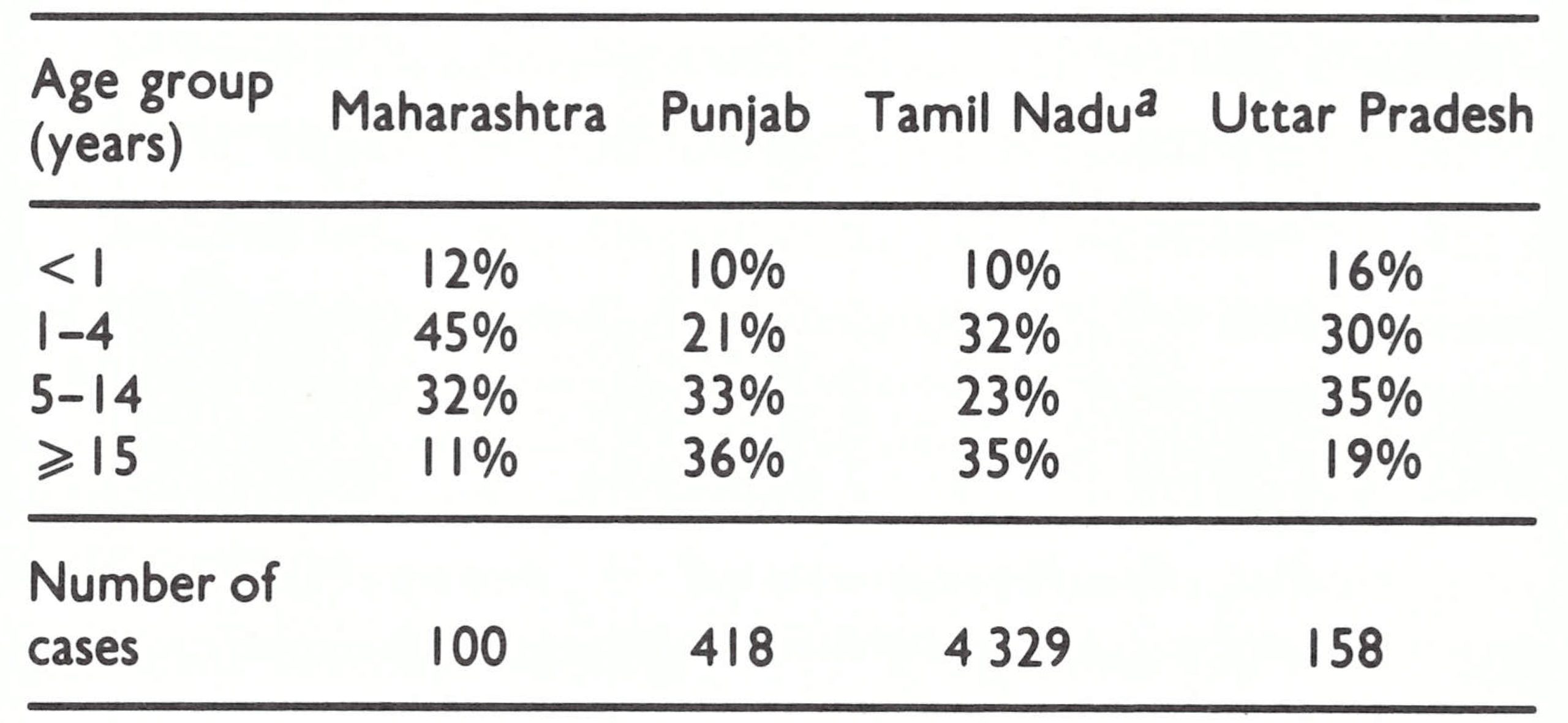
a Data pertain to 1965-1967.
Table 15.7: India : results of vaccination scar surveys in children in 4 states and 2 municipalities, by age group, 1967
Progress Achieved in the Programme, 1968-1970
The recommendations of the joint assessment team were basically sound but smallpox eradication was not high among the government’s priorities. Nevertheless, over the succeeding 3 years, the production of freeze-dried vaccine increased and its quality was improved, many laboratories producing liquid vaccine were closed, the bifurcated needle was introduced, the number of primary vaccinations increased, the vaccination of newborn infants was initiated in several areas, and in some states effective surveillance-containment programmes were conducted.
Vaccine and the vaccination programme
On the basis of WHO recommendations, Dr Singh stressed in a number of directives the importance of primary vaccination, and, as from 1968, the proportion of the population reported to have been given primary vaccination increased significantly (see Table 15.4). However, even with the increase, this proportion barely exceeded the birth rate. At the same time, the total number of reported vaccinations declined steadily.
The vaccination of infants at birth was recommended as a national policy. Traditionally, primary vaccination in India had been deferred until children reached at least 3 months of age. Studies begun in 1959 by Dr A. R. Rao in Madras showed that the vaccination of neonates was safe and that systemic symptoms were minimal (Rao & Balakrishnan, 1963). With the liquid vaccine then in use, 80% were successfully vaccinated but, when freeze-dried vaccine and the bifurcated needle became available, this rate rose to more than 95%. It was clear that if vaccinators could vaccinate all children whom they encountered, overall vaccinial immunity would be enhanced. Equally important, higher levels of vaccinial immunity could be achieved in large urban areas, where 75—80% of women were delivered in a hospital or nursing home. Because the high concentration of people in urban areas played an important role in sustaining smallpox transmission, it was hoped that routine vaccination of newborn children in cities might have a significant impact in diminishing incidence throughout the country.
The routine vaccination of neonates began in Madras and Bombay in 1967 and in several other cities of Tamil Nadu in 1968 . However, the practice was not enthusiastically pursued in most areas, partly because of the lack of interest shown by the autonomous municipal health officers and partly because mothers were reluctant to let their babies be vaccinated . They had observed in other children the severe lesions induced by the rotary lancet and had had no opportunity to see the results of vaccination with the bifurcated needle.
From 1968 to 1970, efforts were made to increase the volume and quality of vaccine produced in India and to improve the distribution system and storage of the product. In 1969 the government appointed a central director for vaccine production and distribution, Dr S.N. Ray, and the following year, the 4 vaccine production centres were placed under central government authority and financed by central government funds rather than state funds. This simplified distribution, because vaccine produced in any one of the institutes could then be sent to any state of India without special payments being required. Previously, vaccine produced in each of the state laboratories had been used mainly in that state, while vaccine donated to India, primarily by the USSR, was sent to other states.
Vaccine production in India gradually increased in volume but less rapidly than had been expected. Not until 1974, in fact, did the country become completely self-sufficient (Table 15.8). In part, the delays could be attributed to preoccupation on the part of the director of the Patwadangar laboratory, the principal production laboratory, with the introduction of comparatively new, more elaborate machines for freeze—drying the so-called shelf-driers. Relatively simple centrifugal freeze-driers were then in use in many countries and when installed in competent laboratories, as in Indonesia and Years Patwadangar Belgaum Kenya for example (see Chapter 11), could be used at full capacity within a year. The director justified the need for the shelf-driers on the grounds that extremely large quantities of vaccine would be required, estimating the need for far greater amounts than had been used during the 1962-1966 mass vaccination campaign. Moreover, he argued that the bifurcated needles, although they used less vaccine and had been adopted in most other countries, would never be acceptable in India. WHO smallpox eradication programme staff, however, foresaw the need for smaller quantities of vaccine, especially if the bifurcated needles could be used, and argued for the purchase of the less complex centrifugal driers. After an impasse lasting almost a year, a staff member of the WHO regional office, who was responsible for providing advice to laboratories, gave approval for the purchase of the shelf-driers, although he himself was not competent in vaccine production. With the promise of purchase of the shelf-driers, the laboratory director gave approval for studies of the bifurcated needle to be undertaken in India (see below). As had been feared, the shelfdriers proved difficult to operate and production increased only slowly but, because of the introduction of the bifurcated needle and the continued provision of vaccine by the USSR, vaccine shortages did not occur.
With an assured supply of freeze-dried vaccine available throughout India, it became possible for the government to insist on the cessation of production of the thermolabile liquid vaccine. However, closure of the 14 state institutes which produced it proved to be difficult. The central government lacked the necessary authority; one by one, each state and centre had to be visited by officials of the central government and persuaded to cease production. This was finally accomplished in 1970, the last centres being in Calcutta and the eastern states. Even after closure of the production centres, however, problems remained. In several states, the stocks of liquid vaccine occupied all the available refrigerated storage space and, without the sanction of the finance department to destroy the vaccine, programme officers could take no action . Accordingly, in several areas, including Bihar State, in which smallpox was eventually to prove a major problem, stocks of freeze-dried vaccine continued to be stored at room temperature while the obsolete liquid vaccine was kept under refrigeration.
Table 15.8: India : number of ampoulesa of freeze-dried vaccine produced each year, 1962-1977, by vaccine production centre, and donated vaccine distributed, 1970-1974
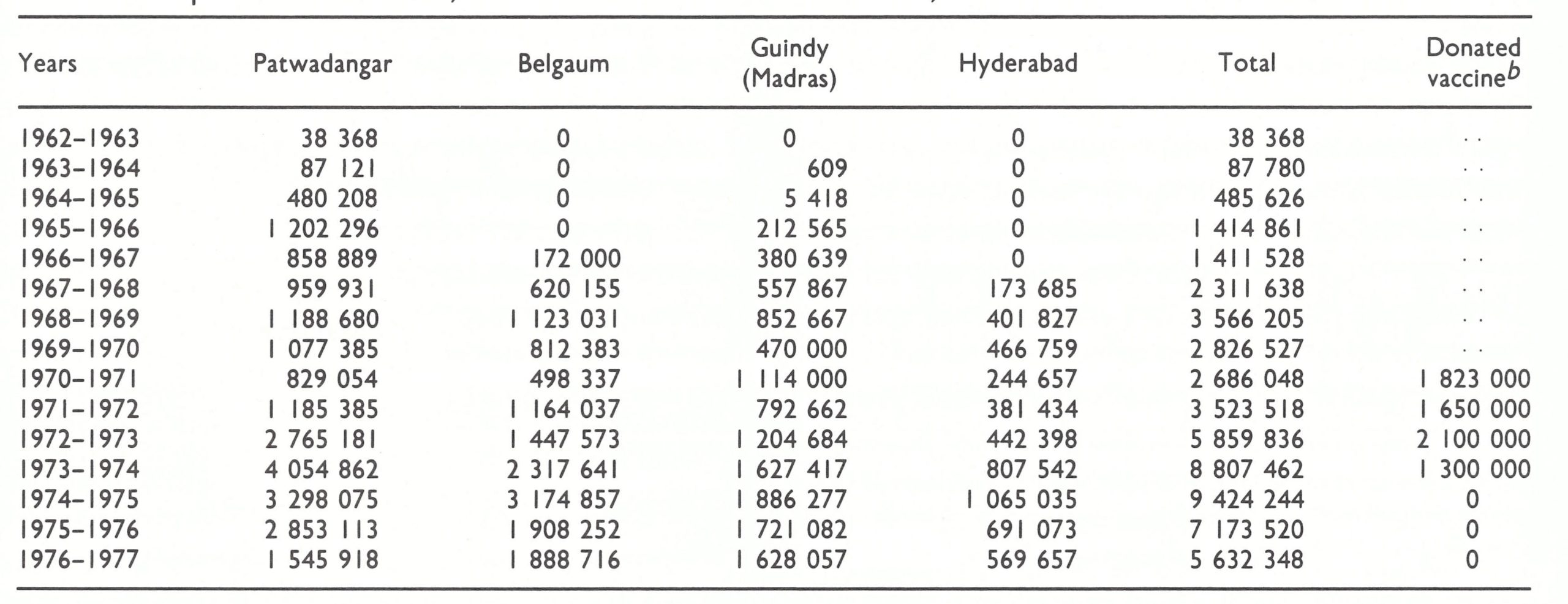
a With the rotary lancet, the contents of I ampoule were required to vaccinate 12-15 persons. When the bifurcated needle was used, the same quantity of vaccine sufficed to vaccinate as many as 100.
bThe USSR donated from 5 to 6 million ampoules of vaccine annually beginning in 1962, but data regarding the distribution of this vaccine are not available before 1970-1971 .
The provision of satisfactory refrigerated storage for vaccine was a continuing problem in other areas as well. The freeze-dried vaccine was supposed to be kept at ambient temperature for not more than 30 days but could be stored almost indefinitely at temperatures of 4°C or less. Because, for reasons of logistics, most vaccinators could obtain vaccine supplies only once a month, it was important to ensure that vaccine stored in district offices, as well as in the state and national depots, was kept under refrigeration. Satisfactory storage at state and national distribution centres was gradually achieved through the provision of refrigerators by UNICEF and WHO and through the use of other facilities such as cold-rooms normally used for the storage of fruit and vegetables. In the districts, however, satisfactory storage was uncommon. Although virtually all district offices were provided with refrigerators for the storage of drugs and vaccines for a variety of programmes, few were maintained in working order. For example, as late as 1975, 85% of the refrigerators in district offices in Uttar Pradesh were found to be inoperative. Fortunately, as tests of vaccine showed, much of the vaccine produced in the USSR and India maintained levels of potency adequate for primary vaccination even after 3-4 months at high ambient temperatures (Sehgal, 1974 ; Sehgal & Ray, 1974).
The assessment team had also recommended that at least one-third of all batches of vaccine produced and tested in the separate laboratories should be independently tested by a national vaccine control laboratory and that the results should be confirmed by a WHO smallpox vaccine reference centre (National Institute of Public Health, Bilthoven, Netherlands). In 1969, an Indian central control laboratory was established at the National Institute of Communicable Diseases, New Delhi, although it was not until 1972 that the laboratory actually monitored the recommended number of batches. In 1969, some batches of vaccine also began to be sent to the WHO reference centre for testing . During the period 1969-1976, of the 241 batches tested by WHO only 9 (3.7%) were found to be substandard (Basu et al.,1979). Although these data would suggest a consistently high level of satisfactory production, it must be noted that all batches dispatched to WHO had been determined, first by the production laboratory and then by the central control laboratory to be completely satisfactory. The producers and the central testing laboratory found a much higher proportion of batches of vaccine to be of inferior potency or stability or unacceptably contaminated with bacteria. Some such batches were destroyed but, in the first few years, most were distributed anyway because vaccine was in short supply. Properly, it was considered preferable to use substandard freeze-dried vaccine than to use liquid vaccine or to have no vaccine at all. No compilation of data on vaccine quality is available, but it was known that the Hyderabad and Guindy laboratories both had persistent difficulties in producing satisfactory vaccine. However, together they accounted for less than one-fifth of all vaccine distributed in India and most of the vaccine they produced was distributed to states in southern India in which health services were generally better and smallpox incidence was lower.
The improved quality of vaccine and a better storage system undoubtedly resulted in a higher proportion of successful vaccinations in the field, although no data are available to substantiate this.
Introduction of the bifurcated needle
The bifurcated needle had been tested by WHO in late 1967 and early 1968 and was rapidly made available throughout most countries by the middle of 1968. In India, however, the traditional rotary lancet had been in use since before the turn of the century and a number of prominent senior health authorities as well as the director of the vaccine production laboratory in Patwadangar resisted the introduction of the new instrument. They argued that it would produce fewer successful vaccinations, that vaccinators would find it too difficult to use, and that the population would resist vaccination with an unfamiliar device. Finally, it was agreed that comparative studies of the two instruments would be undertaken by the National Institute of Communicable Diseases and the Central Health Education Bureau (WHO/SE/70.16).
In 1969, the National Institute assessed the efficacy of the two techniques (Pattanayak et al .,1970). In one study, previously vaccinated children were vaccinated on one arm with the rotary lancet and on the other arm with the bifurcated needle. Vaccines of three different levels of potency were employed. The results showed that the bifurcated needle had a clearcut advantage over the rotary lancet (Table 15.9).
Table 15.9: India: results of simultaneous revaccination of children with the rotary lancet and the bifurcated needle

Comparative data derived from a study of a small number of children given primary vaccination showed similar results . It was found that vaccinators readily learned the new technique and used it successfully.
During the same period, the Central Health Education Bureau investigators assessed the acceptability of the new technique, with surprising results. Persons in 5 villages were vaccinated with the bifurcated needle, but they were given no explanation about the new device. One week later, the vaccinees were examined to determine the proportion with successful vaccinations and were interviewed about the new technique. All those given primary vaccination, and 79% of those who had been revaccinated, had successful takes. As the investigators noted, “surprisingly, few realized that the technique applied was different from the customary rotary lancet method” (WHO/SE/70.16). With these results, the needle was accepted by the national health authorities for use in India.
Needles were provided by WHO in large numbers and, by late 1969, they were in wide use in many states. However, the adoption of the new technique required that a decision should be taken separately by each state and municipality, and some were not persuaded. Not until 1971, for example, were the needles used in the states of Uttar Pradesh and Bihar. In many municipalities, vaccinators continued to use the rotary lancet until late 1973, when municipal smallpox eradication staff were brought under state jurisdiction.
The use of the bifurcated needle, however, brought a curious and unforeseen administrative problem. Auditors in India continually scrutinized the number of vaccinations performed in an area and compared it with the number of vaccinations reported in order to detect wastage. The vials of vaccine containing 0.2 ml allowed for only 15 vaccinations if the rotary lancet was used. With the bifurcated needle as many as 100 vaccinations could be performed with the contents of one vial, but in practice, an average of only 40-50 vaccinations was achieved because whatever reconstituted vaccine remained at the end of the day was supposed to be discarded. Although, in fact, more vaccinations were performed per vial supplied, the auditors calculated that each vial should now yield 100 doses of vaccine. Their assertions that vaccine was being wasted were to plague smallpox eradication staff throughout the rest of the programme.
Sample surveys to determine vaccination status
In 1969, the technique for vaccination scar surveys which had been developed in Afghanistan (see Chapter 14) was introduced into India. Through such surveys it was hoped that responsible officials would identify for themselves deficiencies in their vaccination programmes and correct them. The simplified methodology for scar surveys, using a cluster sample technique, was enthusiastically received in many states and numerous surveys were undertaken, some of which were state-wide. Not all the surveys were well designed, but the results consistently revealed a remarkably high proportion of vaccinated persons . The surveys showed that vaccination scars were borne by 92-99% of individuals in the age group 5 years and above; by 78-92% of those aged 1-4 years; and by 10-60% of infants under 1 year. Although the results were dutifully compiled and reported, few used the data constructively to identify populations or areas in which vaccinial immunity was low and to improve performance in such areas. The idea of assessing vaccination status in this way was reasonable but, in retrospect, the approach was probably counter-productive in that it served to reinforce the notion that mass vaccination was the principal foundation of the programme, rather than surveillancecontainment measures.
The decline in smallpox incidence
Between 1967 and 1970, the reported number of smallpox cases fell dramatically—from 84 902 to 12 773, the lowest total ever recorded in India. Both government and WHO staff recognized that this reflected, at least in part, the normal periodic fluctuations of smallpox. Peaks in smallpox incidence in India normally occurred every 4—7 years, a periodicity extending back many decades. The peak in 1967 occurred just 4 years after the peak in 1963, which had been preceded, 5 years before, by the peak in 1958. This pattern was said to occur as a result of the gradual increase in the number of susceptible persons because of the waning of immunity in the population at large and the addition of susceptible newborn children. It was believed that when a sufficient number of susceptible persons had accumulated, an epidemic would ensue which would diminish this pool of susceptible individuals and thus the ease with which smallpox could spread. Following the epidemic, smallpox incidence would again decline. The decrease in the number of reported cases between 1967 and 1970 was thus not unexpected, but because the incidence had fallen to such low levels, some government and WHO staff were both optimistic and, to a certain extent, unduly satisfied with progress in the redirection of the programme. The archaic notification system, with its delays in reporting, only served to reinforce this optimism. By mid January 1971, for example, only 8026 (63%) of the 12 773 cases eventually recorded for 1970 had been reported to the Central Bureau for Health Intelligence.
Southern India, 1967-1970
The decline in smallpox incidence between 1967 and 1970 was especially notable in the 6 states and 5 union territories which formed the entire southern part of India. This area had a population in 1967 of 196 million (38% of the national total). The number of cases fell from 42 633 in 1967 to only 795 in 1970. Many districts reported no cases in that year (Fig.15.5) and none was detected in the entire state of Tamil Nadu (population, 41 million) (Table 15.10).
In part, this decline was attributable to a generally more developed health service structure, especially in the states of Kerala and Tamil Nadu and, in consequence, a better execution of the mass vaccination campaign. It was also associated with the development of an effective surveillance-containment programme—first in Tamil Nadu and later in parts of Andhra Pradesh.
To evaluate the applicability of surveillance-containment in India, it was decided in 1968 to investigate and contain all outbreaks in Madras, the capital of Tamil Nadu, and subsequently in the state itself, employing a surveillance team directed by Dr A. R. Rao, then Health Officer of the Madras Municipal Corporation . Support for this operation was provided by the Indian Council for Medical Research and WHO (WHO/SE/68.6 and WHO/SE/68.7, A. R. Rao). Dr Rao, for many years the Director of the Madras Infectious Diseases Hospital, had conducted extensive investigations into the clinical and epidemiological behaviour of smallpox (Rao, 1972). He was an ideal person for the task and interested in taking up the challenge.
Smallpox incidence in Tamil Nadu had declined sharply, from 8901 cases in 1963 to only 263 cases in 1967, of which 38 cases had been reported by the Madras Municipal Corporation . The joint India-WHO assessment team (1967) believed that reporting was better in Tamil Nadu than elsewhere in India and, if indeed there were as few cases as notifications suggested, it should be possible to stop transmission with a comparatively modest outbreak containment programme. If successful, it would serve as an example for other states in India.
Between January and June 1968, the season of highest smallpox transmission, Dr Rao investigated 13 outbreaks in Madras, which were detected when patients were brought to the hospital or when fatal cases were registered at the burial grounds. The source of 7 outbreaks could be traced, 6 of them coming from adjoining states. Eight of the index cases were hospitalized within 10 days of onset and none of them spread the disease. Five of the infected persons were hidden at home and, before discovery, 8 second generation and 4 third generation cases occurred. However, the total number of cases was small and, as Dr Rao emphasized, smallpox did not spread rapidly in this population despite its high density and the season of the year. In mid June, the team began to extend its activities beyond the boundaries of the city. The investigation of a case brought to the hospital from a village 24 kilometres away revealed an outbreak of 44 cases in 5 villages. The outbreak had begun in January, when migrant workers returned from the neighbouring state of Andhra Pradesh. As in the city, smallpox had spread surprisingly slowly, suggesting again that outbreaks might be readily controlled. Between July 1968 and June 1969 only 2 additional outbreaks were found in all of Tamil Nadu: one comprised 6 cases imported from Madhya Pradesh State, and the other involved a single patient who had been infected in Gujarat State (WHO/SE/70.19, A. R. Rao). Transmission in Tamil Nadu had been interrupted less than 6 months after a single surveillance team had begun its work ; after May 1968 the state remained smallpox-free except for importations.
Table 15.10: Southern India: number of reported cases of smallpox, 1967-1970
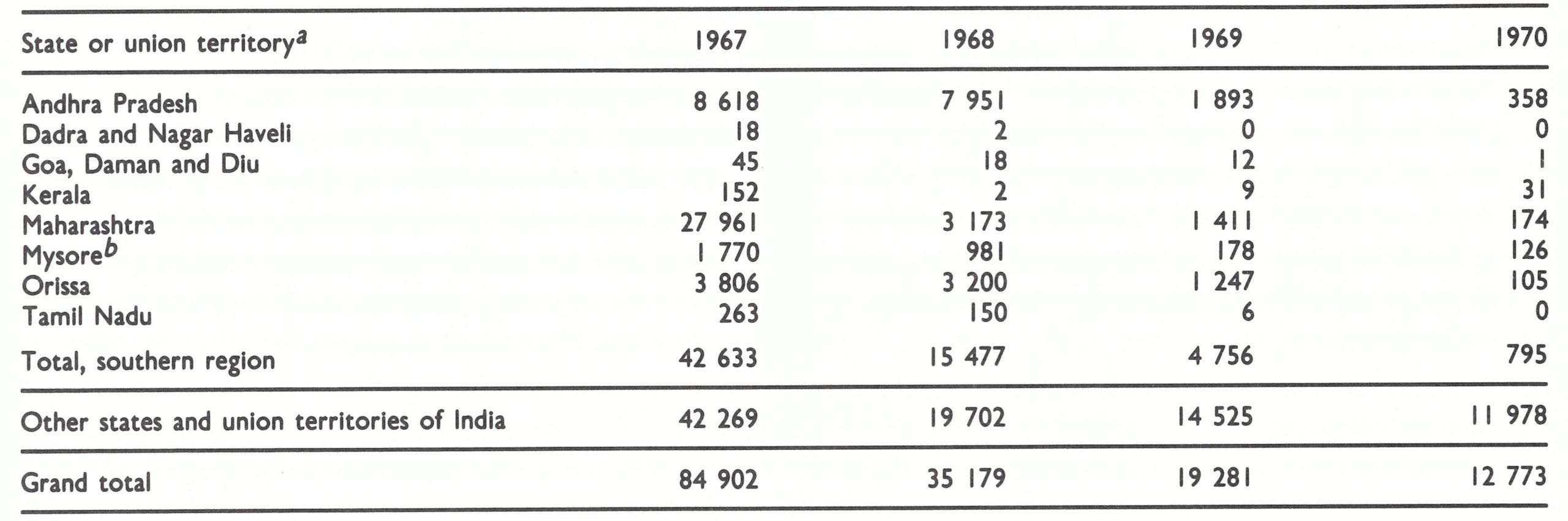
a No cases were recorded during this period in the union territories of Andaman and Nicobar Islands, Lakshadweep and Pondicherry.
b Became the state of Karnataka late in 1973.
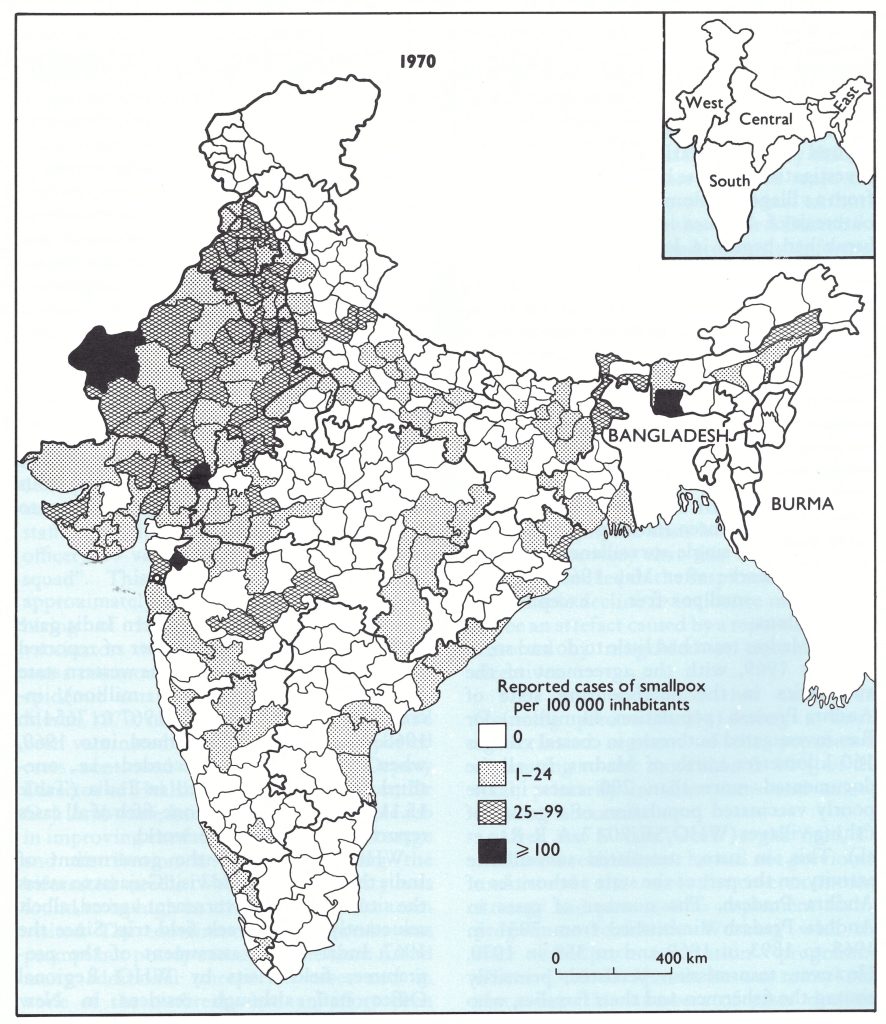
Fig. 15.5. India: number of reported cases of smallpox per 100 000 inhabitants, by district, 1970.
The Madras team had little to do and so, in October 1969, with the agreement of the authorities in the neighbouring state of Andhra Pradesh (population, 43 million), Dr Rao investigated outbreaks in coastal villages 160 kilometres north of Madras. In all, he documented more than 200 cases in the poorly vaccinated population of a group of fishing villages (WHO/SE/70.17, A . R. Rao et al.). This, in turn, stimulated surveillance activity on the part of the state authorities of Andhra Pradesh. The number of cases in Andhra Pradesh diminished from 7951 in 1968 to 1893 in 1969 and to 358 in 1970. However, transmission persisted, primarily among the fishermen and their families, who migrated seasonally from this area northwards to Orissa State.
The success of surveillance and containment measures in both Andhra Pradesh and Tamil Nadu was dramatic, but, despite Dr Rao’s presentations at subsequent national and international meetings, little notice was taken of the achievement. The state smallpox eradication programme officer who accompanied Dr Rao to the meetings rightly noted that the vaccination campaign in Tamil Nadu had been exceptionally well executed, but he argued that it was for this reason, and not because of the surveillance containment activities, that transmission had been interrupted there. Authorities in other states dismissed the attainment as not surprising in the generally more prosperous southern states and of no applicability to most of the rest of India.
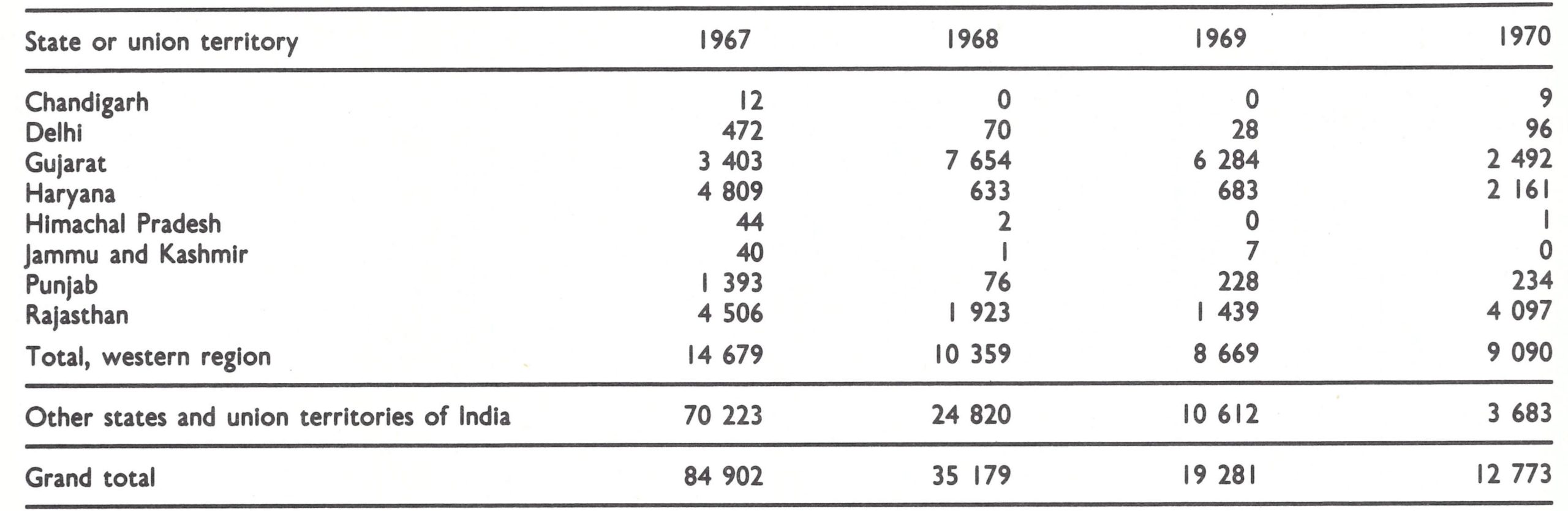
Western India, 1967-1970
Although progress in southern India gave cause for optimism, the number of reported cases of smallpox doubled in the western state of Gujarat (population, 27 million), increasing from 3403 cases in 1967 to 7654 in 1968. The epidemic continued into 1969, when 6284 cases were recorded-i .e., onethird of all cases reported in India (Table 15.11) and, in fact, almost one-fifth of all cases reported throughout the world.
WHO proposed to the government of India that a team should visit Gujarat to assess the situation. The government agreed, albeit reluctantly, to a 1-week field trip. Since the 1967 India-WHO assessment of the programme, field visits by WHO Regional Office staff, although resident in New Delhi, had been discouraged. It was the government’s view that WHO staff could contribute little to a programme that was directed by a national staff who had been engaged in eradication since 1962. Field visits by national staff were likewise uncommon, Dr Singh rarely being able to leave New Delhi because of his innumerable responsibilities. Moreover, his authority was circumscribed because the responsibility for programme execution rested primarily with the states.
In April 1970, a 3-man team, comprising Dr Andrzej Oles, from the WHO Regional Office for South-East Asia, Dr Singh and Henderson, visited Gujarat State and its capital, Ahmedabad (population, 1.7 million). The epidemic in Ahmedabad was considered by local staff to have begun in November 1969 and, to combat it, 150 temporary vaccinators had been hired to supplement a staff consisting of 1 supervisor (medical officer), 39 vaccinators and a 6-man “flying squad”. This provided 1 vaccinator for approximately every 9000 person. The hiring of large numbers of temporary vaccinators without additional supervisors was a common response throughout India to epidemic smallpox. Between January and March 1970, more than 360 000 people had been vaccinated but the number of reported cases continued to increase. The Deputy Director of Health and Medical Services, Dr G. J. Ambwani, had done a commendable job in improving the facilities for vaccine storage and distribution and in introducing the bifurcated needle. Vaccinial immunity was found to be high in all areas which the team visited. The containment of outbreaks was prompt but poorly executed. The team found many additional unreported cases and in none of the outbreaks had an effort been made to identify the source of infection and, thereby, additional outbreaks. Although local civil authorities were responsible for case reporting, almost all the cases were reported by vaccinators.
More disturbing was the discovery that the large numbers of cases reported were not reflected in reports to the national authorities. It was found that the Central Bureau for Health Intelligence had recently informed state statistical sections that it wanted a final report from all districts within 3 weeks of the notification of an outbreak. In Gujarat, this was interpreted to mean that any additional cases that were found after this period or any cases that had experienced the onset of illness more than 3 weeks previously should not be reported to the Central Bureau. The cases were, however, recorded by the state’s smallpox eradication programme office. Not only was the epidemic in Gujarat of a far greater magnitude than had been suspected, but the discovery that this new policy had been adopted led to the suspicion that India’s remarkable decline in incidence might possibly be an artefact caused by a reporting system distorted by misguided or misunderstood directives.
The team concluded that cases were occurring predominantly among a small, unvaccinated segment of the population, amounting to not more than 5-10% of the total, primarily in slum areas and among migrant labourers.
After just 5 days’ work in the field, Dr Ambwani realized that he had not previously understood the surveillance-containment strategy and promised to implement such a programme forthwith. Working with the state smallpox eradication programme officer, Dr S. D. Verma, he was remarkably successful . The numbers of cases declined rapidly and in June 1971, only 14 months after the team’s visit, transmission ceased. Other cases occurred later but they were traced to importations from other states. The success in Gujarat suggested to both senior Indian and WHO staff that if states were given modest assistance to foster surveillance-containment programmes, these results might be replicated elsewhere. Unfortunately, Gujarat, like Tamil Nadu, was to prove an exception.
Table 15.11: Western India: number of reported cases of smallpox, 1967-1970
The team returned to New Delhi encouraged by Dr Ambwani’s interest in and responsiveness to the surveillance-containment strategy but now less confident that the remarkable decline in the number of reported cases was real. A recommendation was made that the reporting system should be changed but this was vigorously resisted by the director of the Central Bureau for Health Intelligence. Thus, the programme continued, its personnel less certain of the true incidence of smallpox but now placing increased reliance on data provided by state eradication programme officers rather than on official government statistical reports. However, because the quality of the programme officers varied greatly from state to state and because the Central Bureau’s directives were variously interpreted by officials at different levels, it was difficult to known what the different sets of numbers really meant without field visits to every state and no staff were available to undertake such visits.
Yet another disturbing observation was made in the western states in the spring of 1970. It began to appear that smallpox might be moving as an epidemic wave in a clockwise direction around India. In 1967, immediately before the 1968-1969 Gujarat epidemic, Maharashtra, the state immediately to the south, had reported especially severe epidemics. That year, it had recorded 27 961 cases, one-third of all cases reported from India. The number dropped to 3173 in 1968 and to 1411 in 1969. In the spring of 1970, the states of Rajasthan and Haryana, immediately to the north of Gujarat, began to experience major epidemics.
This had not been expected. Since the 19th century, major epidemics in the Indian subcontinent had been observed to occur every 4-7 years, but the periodic fluctuations had been thought to take place more or less simultaneously throughout the country. The wider availability of vaccine had not altered this pattern. That the periodicity had persisted until 1962 was understandable because intensive and widespread vaccination had been conducted during and immediately after epidemics, but as smallpox waned so did interest in vaccination. However, it was quite unexpected that the intensive ongoing national vaccination campaign begun in 1962 had not prevented the 1967 epidemic. To explain this recurrence, it was suggested that many states had not conducted effective campaigns, and because much of the vaccine used had lacked potency, the large pool of susceptible persons had not significantly diminished. Between 1967 and 1970, however, most of the vaccine reaching recipients was believed to be fully potent and because the number of primary vaccinations had substantially increased, the opinion was held that India should not again experience a major epidemic year. Thus, the recurrence of epidemic smallpox, apparently moving in a clockwise direction around India, was totally unexpected but a critical factor in the formulation of subsequent strategy.
In 1970, senior national government staff began to take a greater interest in the smallpox eradication programme. Epidemic areas in Haryana and Rajasthan abutted on New Delhi, the national capital. Reports of the outbreaks appeared in increasing numbers in New Delhi newspapers, and members of Parliament expressed concern through “call-attention” motions, obliging the government to give an account of what was being done.
The Gujarat team had concluded in its recommendations to the government: “. . . of greatest importance . . . is the need to augment the staff at state level to provide leadership to the programme and to develop and coordinate, by active field work, the very critical surveillance-containment activities.” WHO proposed to the government that 4 WHO epidemiologists should be recruited to work as advisers with state programme officers. One would be assigned to Rajasthan, in which smallpox incidence was rapidly rising ; one each would be allocated to Uttar Pradesh and Bihar, the two densely populated states comprising most of the northern Ganges river plain, and, if assumptions regarding the clockwise movement of epidemic smallpox were correct, the next to experience major epidemics ; the fourth epidemiologist would be assigned to work with state programme officers throughout the southern states in an effort to interrupt transmission in this vast area . Dr Singh, meanwhile, would plan to work with programme officers in the small neighbouring states of Haryana, Punjab and Himachal Pradesh as well as the Delhi Municipal Corporation.
The Director-General of Health Services and the Secretary of Health were initially of the opinion that 2 advisers would suffice but ultimately agreed to 4. On 9 September 1970, an agreement was signed by the government and WHO which committed WHO to provide : (1) 4 epidemiologists and 3 shortterm consultants for 3 months each in 1970 and 1971, plus the costs of their travel ; (2) vehicles and other supplies ; and (3) funds to pay salaries, travel and per diem “for additional personnel employed full-time in smallpox units at the national and state levels up to the limit of Rs. 1 125 000 each year” (US$146 250). In 1970, WHO support to the programme for the first time exceeded US$100 000. During the succeeding 7 years, more than US$11 million would eventually be provided, most of which represented contributions from the government of Sweden (Table 15.12). Additional funds were allocated to the WHO Regional Office for South-East Asia, which as the Indonesian programme concluded, began to devote more time to the programme in India.
Table 15.12: Western India: number of reported cases of smallpox, 1967-1970
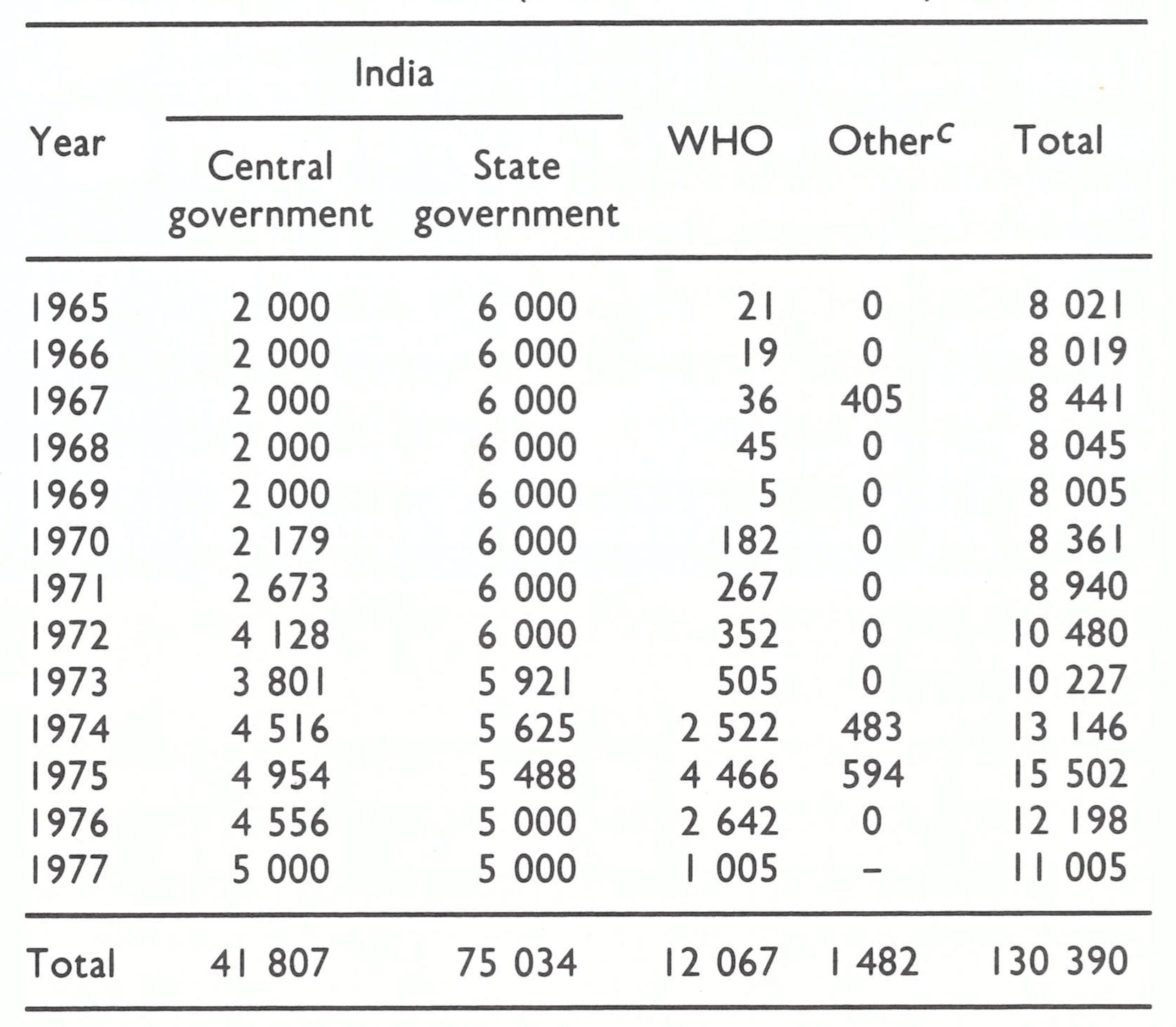
aExpenditures by the central government (1965-1969) and state governments (1965-1972) are estimates. Of funds expended by WHO between 1974 and 1977, US$8 .1 million were provided by the Swedish International Development Authority.
bExcludes the estimated value of vaccine provided between 1965 and 1974, which amounted to 701 million doses from the USSR and 5 million doses from WHO.
cValue of contributions in cash and in kind from Tata Industries (US$600 000), USA (US$402 000), UNICEF (US$380 000), and OXFAM (US$ 100 000).
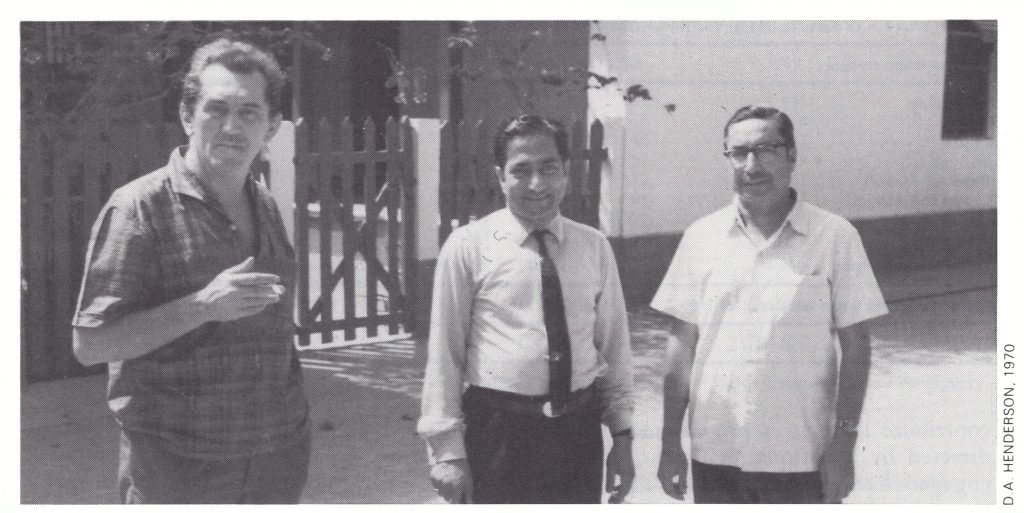
Plate 15.3. Members of an Indian/WHO team to assess the smallpox epidemic in Gujarat State in April 1970. Left to right: Andrzej J . Oles (b . 1923), an epidemiologist with the WHO Regional Office for South-East Asia; Mahendra K . Singh; and G . J . Ambwani, Deputy Director of Health and Medical Services of Gujarat State.
The Foundations are Laid for the Intensified National Campaign, 1971-1973
From 1971 until the summer of 1973 the programme gradually evolved and, in doing so, laid the foundations for the intensified national campaign, termed “Smallpox Zero”, which began in the autumn of 1973. A closer working relationship was established between the government of India and WHO ; the bifurcated needle replaced the rotary lancet in all but a few municipal corporations; the use of liquid vaccine ceased completely ; larger quantities of good-quality freeze-dried vaccine produced in India became available; the reporting system was changed ; and a procedure for the detection of cases was elaborated.
WHO recruited 2 new regional smallpox advisers, for what was then called the Regional Epidemiological SurveillanceTcam, as well as 4 epidemiologists for assignment to India. Dr Nicole Grasset, a French virologist and epidemiologist, became the regional adviser in 1971, replacing Dr Keja, who had been transferred to Indonesia. She had worked previously in smallpox and measles control activities in eastern Nigeria and had proved to be a charismatic leader. She was joined in the regional office in 1972 by Jezek as the second regional adviser. Although they were responsible for smallpox eradication activities throughout the South-East Asia Region, much of their work was to be devoted to the programmes in India and Nepal. The 4 epidemiologists for the programme in India were assigned to the states. Dr Alberto Monnier, a Mexican epiSMALLPOX AND ITS ERADICATION demiologist who had been with the Indonesian smallpox eradication programme, began work in Rajasthan in January 1971 and Dr V. A. Moukhopad, a Soviet epidemiologist, arrived a month later to begin work in Uttar Pradesh. That summer, a Czech epidemiologist, Dr Vladimir Zikmund, began work in the southern states. Another epidemiologist reported for duty in Bihar during the summer but stayed only 6 months before resigning. At that time, the post in Bihar was felt to be the least critical, since the available data for 1971 showed smallpox was then concentrated in the north-western part of the country (Fig. 15.6), geographically distant from Bihar. A principal problem in Bihar, as well as in the other states, was the stipulation that each state should provide a vehicle for each adviser and cover the costs of its operation. Rarely before had WHO staff been assigned to work at state level in India and, with vehicles in the states in short supply and poorly maintained, the provision of transport for the advisers was a problem. In Bihar, none was made available and, in general, state officials showed little interest and offered the minimum of cooperation in helping to solve difficulties of this kind. Not until 2 years later were the inadequacies of the Bihar health structure fully appreciated. Conceivably, more energetic measures in Bihar at that time might have averted the catastrophe that lay ahead.
Smallpox eradication activities continued in all states throughout 1971-1973, with varying levels of success. During this period there were developments of particular note in the western states and in Uttar Pradesh, as well as in certain of the areas of low incidence in the south, and an unanticipated setback originating in a Bangladeshi refugee camp in West Bengal. These are described below.
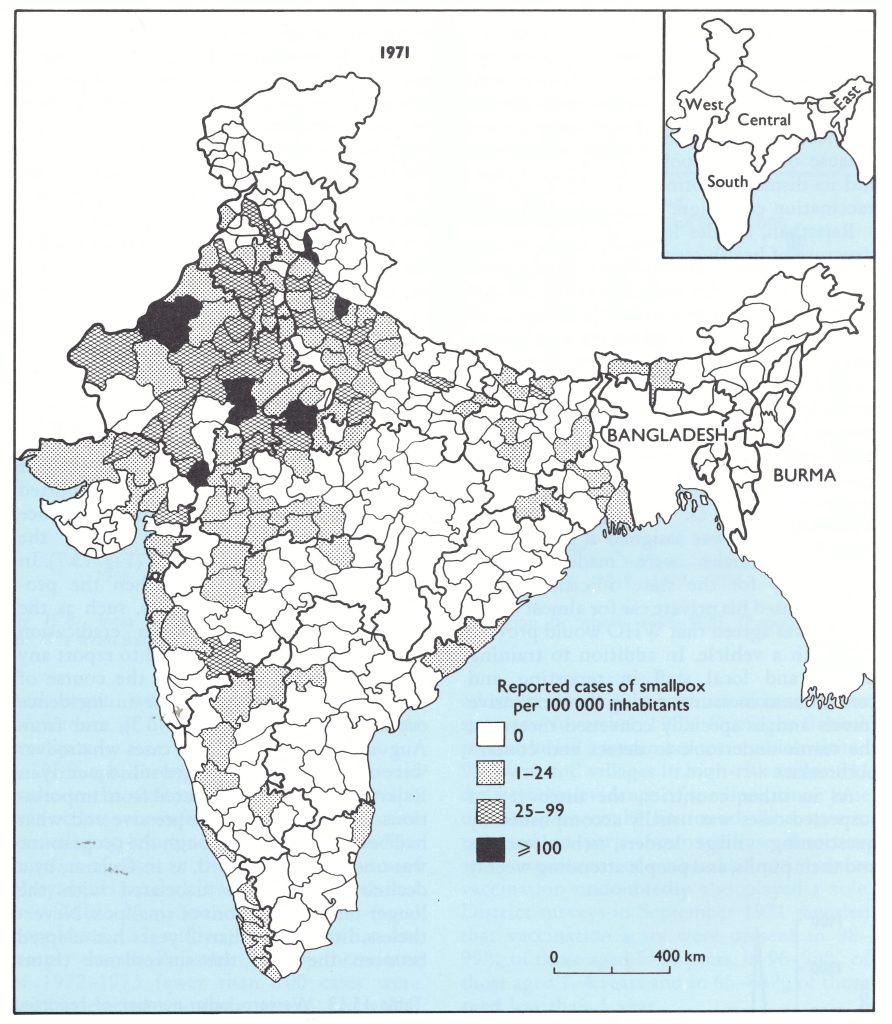
Fig. 15.6. India: number of reported cases of smallpox per 100 000 inhabitants, by district, 1971.
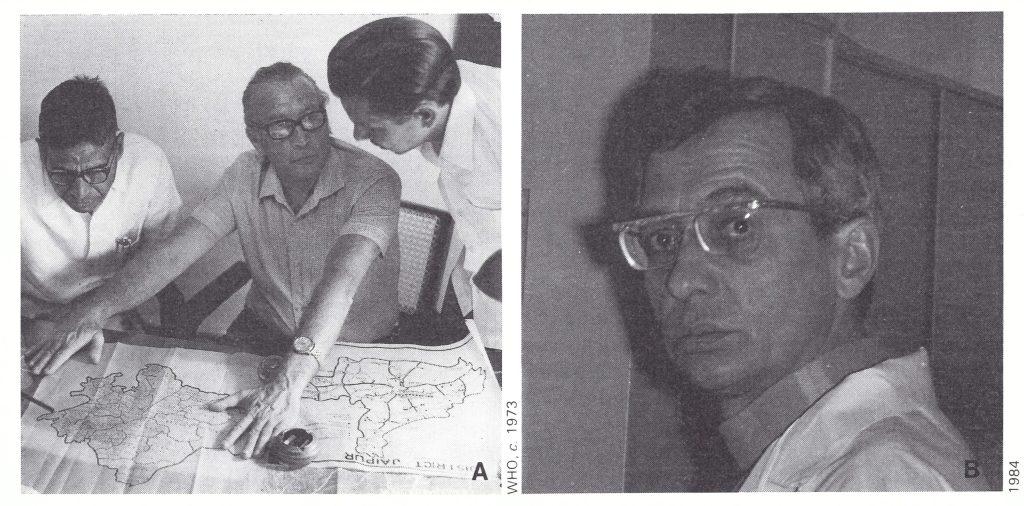
Plate 15.4. A: Alberto M . Monnier (1914-1979), an epidemiologist, served as the WHO smallpox officer in Rajasthan State from 1971 to 1976. B: Viatcheslav A . Moukhopad fulfilled the same role in Uttar Pradesh State
from 1971 to 1976.
Western India, 1971-1973
It had been hoped that the dramatic success of the surveillance-containment programme in Gujarat might be repeated in the other western states and in Uttar Pradesh, in which epidemics were then beginning. Dr Monnier, assigned to Jaipur, the capital of Rajasthan, and Dr Moukhopad, assigned to Lucknow, the capital of Uttar Pradesh, provided needed support. Full-time assignments were deemed advisable: in Rajasthan because health and other services were less well developed in this conglomerate of former princely states than in most of India; and in Uttar Pradesh because of its vast population (91 million) and its dismal performance during the mass vaccination campaign.
Rajasthan, besides having a less adequate structure of health services and a less literate population than much of India, was geographically a problem, nearly two-thirds of its area being desert and semi-desert. Roads were few and working conditions demanding. The population of 26.5 million was principally settled in 151 towns and 33 305 villages, but there were nomads as well. Three state teams were created which were directed, respectively, by the Deputy Director for Communicable Diseases, Dr M. L. Aggarwal ; his deputy, Dr D. K. Jagdev ; and Dr Monnier. Each was assigned a paramedical assistant. Vehicles were made available sporadically for the state officials but Dr Monnier used his private car for almost a year until it was agreed that WHO would provide him with a vehicle. In addition to training district and local staff in reporting and containment measures during their extensive travels and in specially convened meetings, the teams undertook to detect and contain outbreaks.
As in other countries, the discovery of suspected cases was usually accomplished by questioning village leaders, schoolteachers and their pupils, and people attending weekly markets. In Rajasthan and in many other parts of India, there were two additional methods, unique to India, by which cases could be detected. One consisted in questioning visitors to the Sltala mata temples. Many villagers came to give thanks to the goddess for recovery from smallpox or to offer homage in the hope that they and their families would be spared a visitation by the goddess. Cases could also be detected in villages when, as was customary in many areas, branches from the neem tree were hung over the front door of a house in which a patient lived. The leaves of the neem were considered to have special cooling properties when applied to the skin of the patient and other, less tangible, properties when hung above the doorway.
The programme in Rajasthan made commendable progress. At the beginning of the summer of 1971, the number of reported cases declined steeply, and the incidence remained comparatively low during the spring smallpox season of 1972 (Fig. 15.7). In October, in order to strengthen the programme, other health workers, such as the family planning and malaria eradication programme staff, were directed to report any smallpox cases found during the course of their work. A further decline in incidence occurred in 1973 (Table 15.13), and from August to October 1973 no cases whatsoever were detected. Cases occurred subsequently in Rajasthan, but they originated from importations. The results were impressive and what had been hoped for, although the programme was undoubtedly assisted, as in Gujarat, by a decline in incidence associated with the longer-term fluctuations of smallpox. Nevertheless, little more than 2 years had elapsed between the time the surveillance teams had begun work and the unprecedented occurrence of 3 months without detectable smallpox.
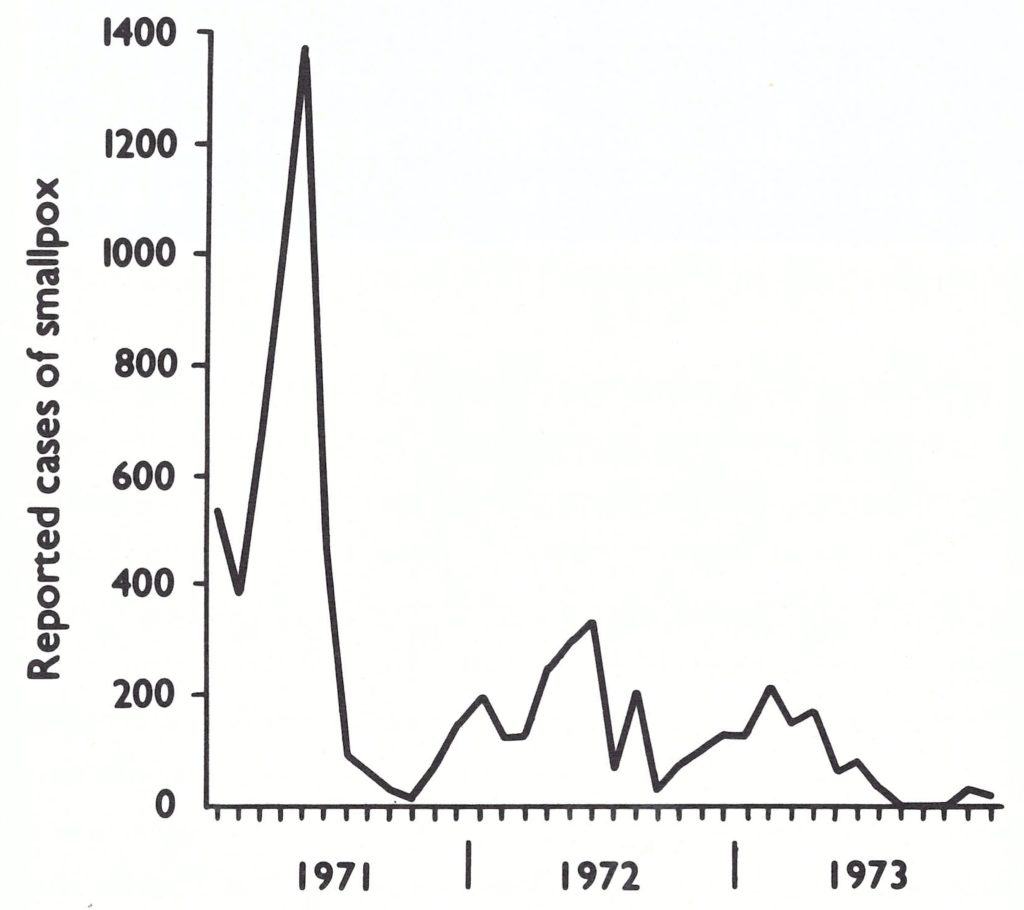
Fig. 15.7. Rajasthan State: number of reported cases of smallpox, by month, 1971-1973.
Table 15.13: Western India: number of reported cases of smallpox, 1971-1973
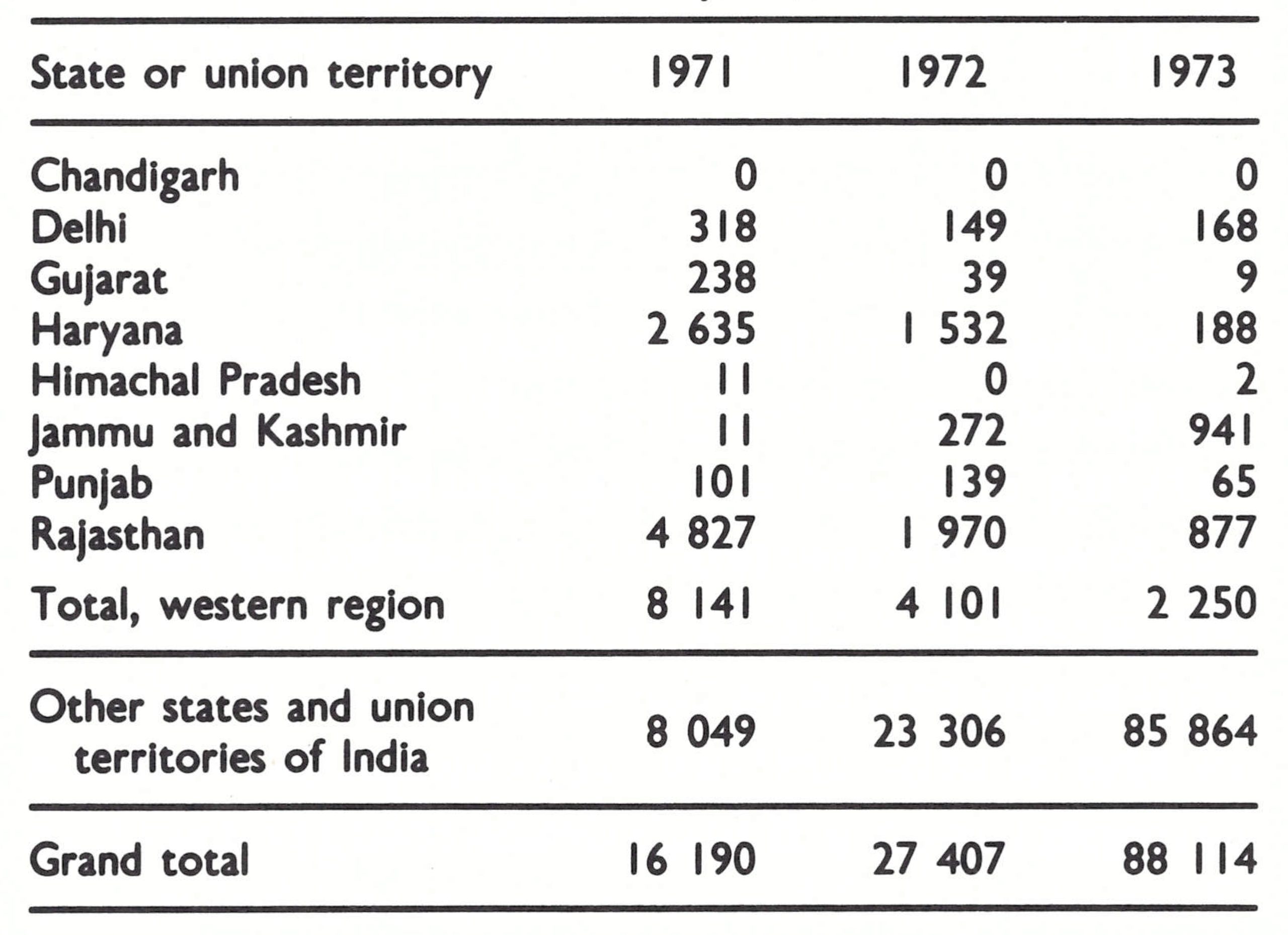
Dr Singh, through such visits as he could make to the western states near New Delhi, was no less successful in stimulating effective surveillance-containment programmes. The number of cases in the contiguous states of Haryana, Himachal Pradesh and Punjab and in Delhi Municipal Corporation (total population, 32 million) fell somewhat less steeply than in Rajasthan, but by the winter of 1972-1973 fewer than 100 cases were being detected monthly, many of which resulted from importations from the neighbouring state of Uttar Pradesh. By September 1973, transmission had been interrupted throughout this entire area, the only reported cases resulting from importations into New Delhi.
Meanwhile, the programme in Gujarat had progressed so satisfactorily that only 44 outbreaks were detected during the first 6 months of 1971, and none whatsoever from July to the end of October. It seemed impossible that transmission could have been stopped in a state so heavily infected as recently as 1970. Accordingly, Arita was asked to direct a special assessment of the state in November 1971. During a 3-week period, he led a 6-member team which visited 90 towns and villages in high-risk areas of 11 districts. No evidence of smallpox since June of that year could be found. The success reflected, in part, improved case detection and containment of outbreaks, but intensive vaccination undoubtedly also played a role. District surveys in September 1971 revealed that vaccination scars were present in 98- 99% of those aged 5-14 years, in 96-99% of those aged 1-4 years and in 66-88% of those aged less than 1 year.
The smallpox eradication programme throughout the western states was progressing everywhere as had been hoped (Fig. 15.8) with a single exception—the northern state of Jammu and Kashmir (population, 48 million), which had once been free of smallpox. In the autumn of 1972, the state began reporting increasing numbers of cases. Until October, Jammu and Kashmir had experienced only occasional importations which, according to state reports, had been quickly contained. It had been hoped that by preventing smallpox from becoming reestablished in Himachal Pradesh, a geographical barrier to the northward spread of the epidemic would be created, preventing the disease from reaching Jammu and Kashmir. Dr Singh, working with effective state programme staff, proved successful in maintaining the non-endemic status of Himachal Pradesh. Unfortunately, many travellers to Jammu and Kashmir imported smallpox from infected areas more than 50 kilometres away. Because of the paucity of senior smallpox advisers, assistance had not been provided to state staff in Jammu and Kashmir and the health services had been unable to cope. The failure to strengthen activities in this state was an omission for which the programme would subsequently pay dearly in additional effort.
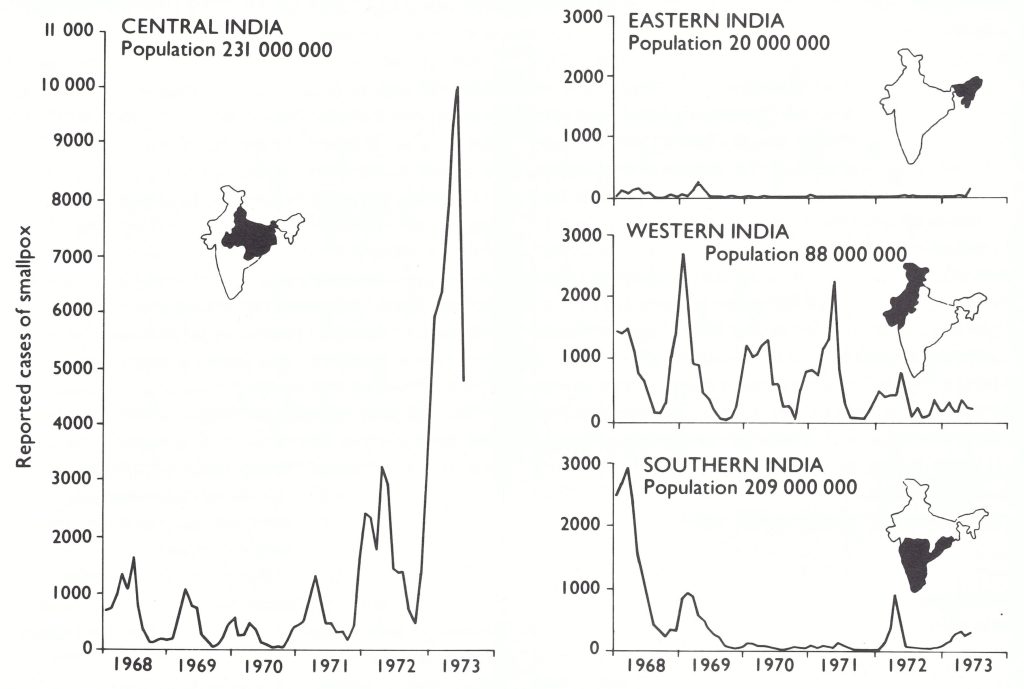
Fig. 15.8. India: number of reported cases of smallpox, by region, by month, 1968-1973. (Population data for 1971 from Basu et al ., 1979.)
Uttar Praderh, 1971-1973
The development of surveillance-containment programmes in the western states proved to be comparatively straightforward, but in the adjacent state of Uttar Pradesh, the experience was entirely different. Uttar Pradesh was India’s most populous state (population, 91 million) with a density of 300 persons per square kilometre. Most of the state comprises the Ganges river plain, where population densities were among the highest in India and where transport and communication services were quite well developed. There was an extensive, well-established infrastructure of health services and a large, reasonably well trained health staff. In retrospect, unexpected problems might perhaps have been foreseen because of Uttar Pradesh’s poor performance in the mass vaccination campaign, and because it was the last state in India to replace the rotary lancet with the bifurcated needle (1971).
During 1971, Dr Moukhopad and the state programme officer travelled extensively to conduct regional training programmes for all district health officers and their programme staff. However, almost as soon as they were trained in reporting and in surveillancecontainment procedures, they were transferred to other districts or assumed other duties. Many who reported substantial numbers of cases of smallpox from their districts were disciplined by the state Director of Health Services by being transferred to hardship posts on the grounds that the presence of cases was tacit evidence that they had not conducted an effective vaccination campaign. Although other states followed this practice, none did so as frequently as Uttar Pradesh and neighbouring states in northern India. Continuing efforts were made by national staff and WHO advisers to persuade state officials that their actions were counter-productive, but with only partial success.
Progress in the programme in Uttar Pradesh was difficult to assess, in part because of the suppression of reports by district officers and in part because of the archaic state and national reporting system. During 1971, the number of cases reported from Uttar Pradesh to the Central Bureau for Health Intelligence never reached 500 per month, and indeed between July and September of that year fewer than 100 cases were notified each month for the entire state. The relevant data, reported to the Central Bureau and to WHO up to 26 October 1971, are shown in Table 15.14 (Wkly epidem. Rec., 1971b). Even if one were to assume that there were 10 times as many cases as had been reported, not only Uttar Pradesh but India as a whole appeared to have very few chains of smallpox infection. On the basis of a growing experience with surveillance-containment programmes, it seemed reasonable to expect that transmission could be interrupted comparatively easily and rapidly. The greatest impediment in assessing the true situation and in deciding how best to deploy resources to achieve this goal was the reporting system.
In November 1971, the government and a new acting director of the Central Bureau for Health Intelligence agreed to modernize the reporting system so that its procedures would resemble those used in other countries. Each primary health centre was directed to notify to the district on Saturday of each week the total number of cases detected that week irrespective of the date of onset. If no cases were reported, a “nil” report was to be submitted. The submission of a nil report was a most important feature. Previously, the absence of a report had been assumed to mean an absence of cases when, in fact, the responsible medical officer may have been negligent in reporting or had decided not to report because there were a great many cases. Officials who had been accustomed to suppressing information through the simple expedient of not submitting a report found it difficult to indulge in deliberate falsification. The districts were asked to ensure that reports from all primary health centres were submitted and to compile all reports then available on the following Tuesday and to send them to the state smallpox eradication programme office. The state, in turn, was made responsible for ensuring that all districts reported and, on each Thursday, for telegraphing a report to the Central Bureau for Health Intelligence and the National Smallpox Eradication Programme office. Many months, and in some states several years, of work were required before the reporting system functioned well but a major obstacle to the achievement of eradication in India had at last been removed.
Table 15.14: India: number of reported cases of smallpox, by state and union territory and by month, 1971a
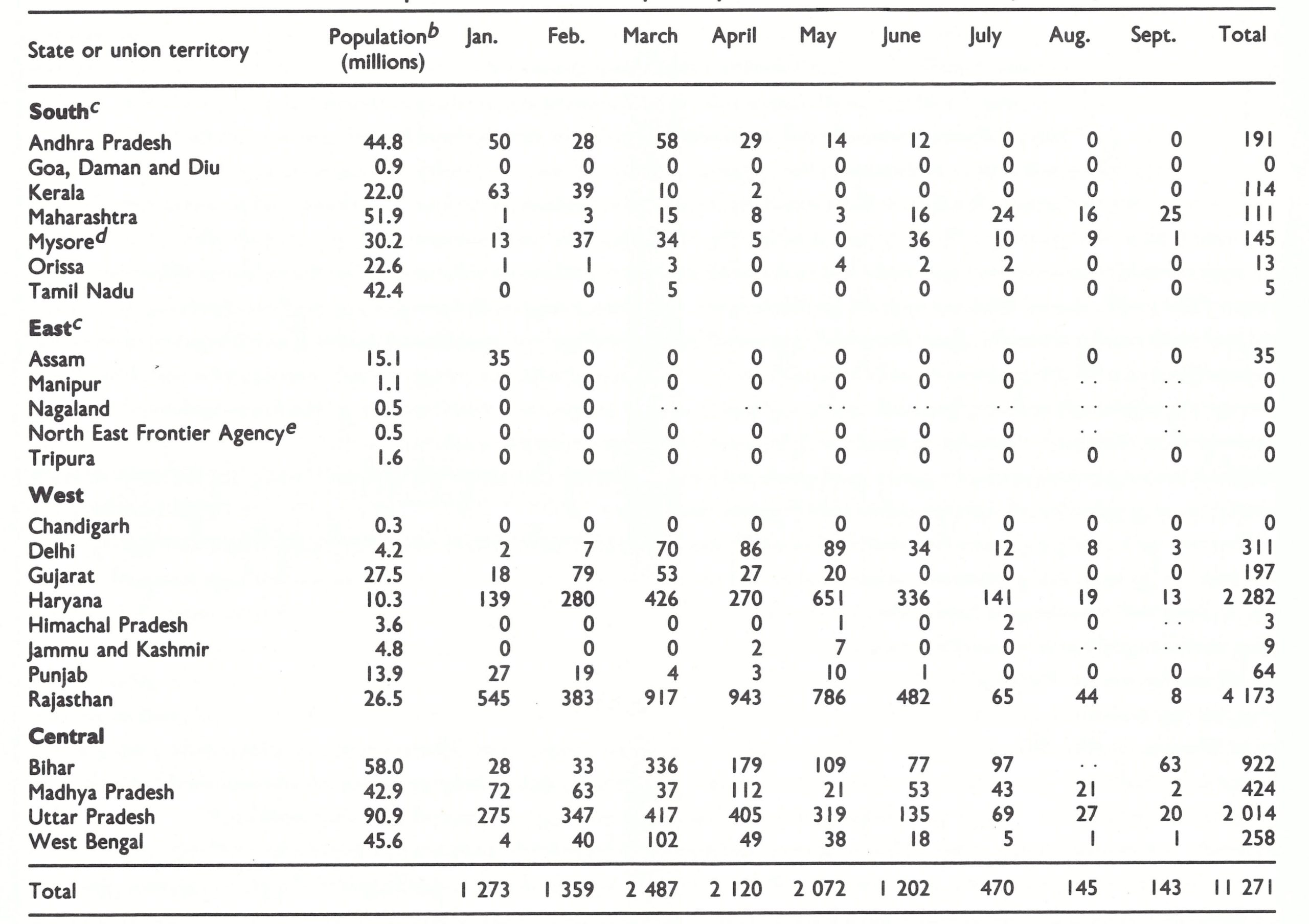
a Data reported to WHO up to 26 October 1971 ((Wkly epid. Rec.,1971b).= data not recorded.
b Population estimates by state are based on United Nations (1985) data for all of India proportionately allocated by state on the basis of the 1971 census.
c No cases were reported during this period in the union territories of Andaman and Nicobar Islands, Dadra and Nagar Haveli, Lakshadweep, Pondicherry, and Mizoram, and the state of Meghalaya.
d Became the state of Karnataka late in 1973.
eBecame the union territory of Arunachal pradesh in 1972.
In November 1971, Uttar Pradesh was the first state to implement the new reporting scheme. By February 1972, the number of districts which had not reported for 3 weeks or more had fallen from 17 to only 5, and by summer, 48 of the 55 districts were submitting reports promptly each week. Whether because of improved reporting or because of an actual increase in incidence, the number of recorded cases rose during the winter of 1971-1972 to between 1200 and 1600 each month (Fig . 15.9)—but still, in a population of 91 million, this was not a great number. Senior staff continued to believe that with sustained support to the surveillancecontainment effort, Uttar Pradesh would repeat the experience of the western states . It was not to be. Smallpox eradication staff were diverted to perform cholera vaccinations between September and December 1972, at a time when the containment of smallpox outbreaks was most crucial. Although cholera vaccine had been shown to be of little value, this was the usual and politically acceptable response of the health services when cholera occurred. Explosive outbreaks of smallpox spread across the state ; the number of cases increased rapidly during the early months of 1973, reaching a peak in May, when 5000 cases were reported.
Particularly discouraging was the continuing antipathy of state officials to the surveillance-containment strategy. An episode in early April 1973 in the district of Muzaffarnagar vividly illustrated the prevailing attitude. This district, located less than 100 kilometres north of New Delhi, began experiencing outbreaks of smallpox in the autumn of 1972 and, in January, reported 440 cases. This greatly exceeded the number reported that month by any other district of India except 2 districts in West Bengal associated with the Salt Lake Refugee Camp disaster (see later in this chapter). In February 1973, Arita joined Dr Moukhopad in a special investigation of the problem. Active searches at schools and markets soon revealed that although the reported smallpox incidence was high, there were many other undetected and uncontrolled outbreaks occurring throughout the district. With the cooperation of a responsible, energetic district health officer, they decided to mobilize all health staff throughout the district by closing the health centres and training the staff to undertake a 2-week systematic village-by-village search for cases. The health staff responded with enthusiasm and efficiency and soon discovered that cases were occurring in more than half the villages. In all, 641 cases were discovered in February and 1219 in March. Containment measures had scarcely begun, however, when the state Director of Health Services ordered the cessation of all surveillance-containment operations and the immediate vaccination of the entire population of the district. He then warned that when this had been completed the report of any further cases would result in the transfer of the district health officer to the most unpleasant post in the state. It was clear that considerable persuasion of state officials and heroic efforts in the field would be required if Uttar Pradesh was to become free of smallpox. However, the demonstration that it was possible to mobilize effectively the poorly supervised army of health staff offered hope for the future.
The southern states, 1971-1973
In the southern states, it had been hoped that the WHO adviser, Dr Zikmund, working with state programme officers might succeed reasonably quickly in developing surveillance-containment activities to the point of interrupting transmission throughout the entire area. Tamil Nadu continued its successful programme and from the beginning of 1971 to the end of 1973 only 11 cases were recorded (Table 15.15), all following welldocumented importations. Mysore (renamed Karnataka in 1973) and Andhra Pradesh, the contiguous states to the north, were targets of high priority. Virtually all cases in Andhra Pradesh occurred during the first half of 1971 among generally uncooperative, poorly vaccinated fishermen who migrated seasonally between Andhra Pradesh and Orissa. District health officials, considering them to be temporary residents, had ignored them. Once vaccination and outbreak containment began, transmission quickly stopped. In Mysore, 185 of the 223 cases reported during 1971 were from a single district and these outbreaks were contained by midsummer. Maharashtra was also successful in stopping transmission. In the entire southern area, between October 1971 and January 1972, only 45 cases were detected, all of them occurring in 3 districts. Considering that the southern states accounted for 38% of India’s total population, there was reason for optimism about the prospects for the eradication of smallpox in India. Uncertainty persisted, however, about the situation in the state of Kerala. There, smallpox transmission appeared to have been interrupted in 1967, only 42 cases, presumably importations, having been detected between 1968 and 1970. However, between January and May 1971, 105 cases were reported, with 1 additional case in September and 2 in November. Kerala’s health services, among the best in India, reported that the cases had not occurred in outbreaks as one would expect, but rather were scattered across 7 of its 10 districts. Because the epidemiological pattern of the cases was difficult to explain, Arita joined state officials in a special study in February 1972. Of the reported cases, 70% were found to be in persons over 15 years of age, and of the patients whose vaccination status was known, 102 had previously been vaccinated. Arita and his collaborators examined 35 patients who had recovered, but none had the residual pockmarks typical of smallpox. As it turned out, the state in late 1970 had requested health staff to begin to collect specimens from patients with chickenpox as well as from those with suspected smallpox to confirm with greater certainty that the state was smallpox-free. A state laboratory with little experience in the identification of variola virus had examined the specimens using the gel-precipitation technique and reported that 104 out of 386 tested were either “positive” or “doubtful” for variola virus. Although there was little doubt on the part of physicians about the clinical diagnosis, the virological reports were accepted and the cases duly notified. The team eventually concluded that none of the reported cases was smallpox and the reports were retracted. Except for 4 imported cases in 1974, Kerala was to remain smallpox-free.
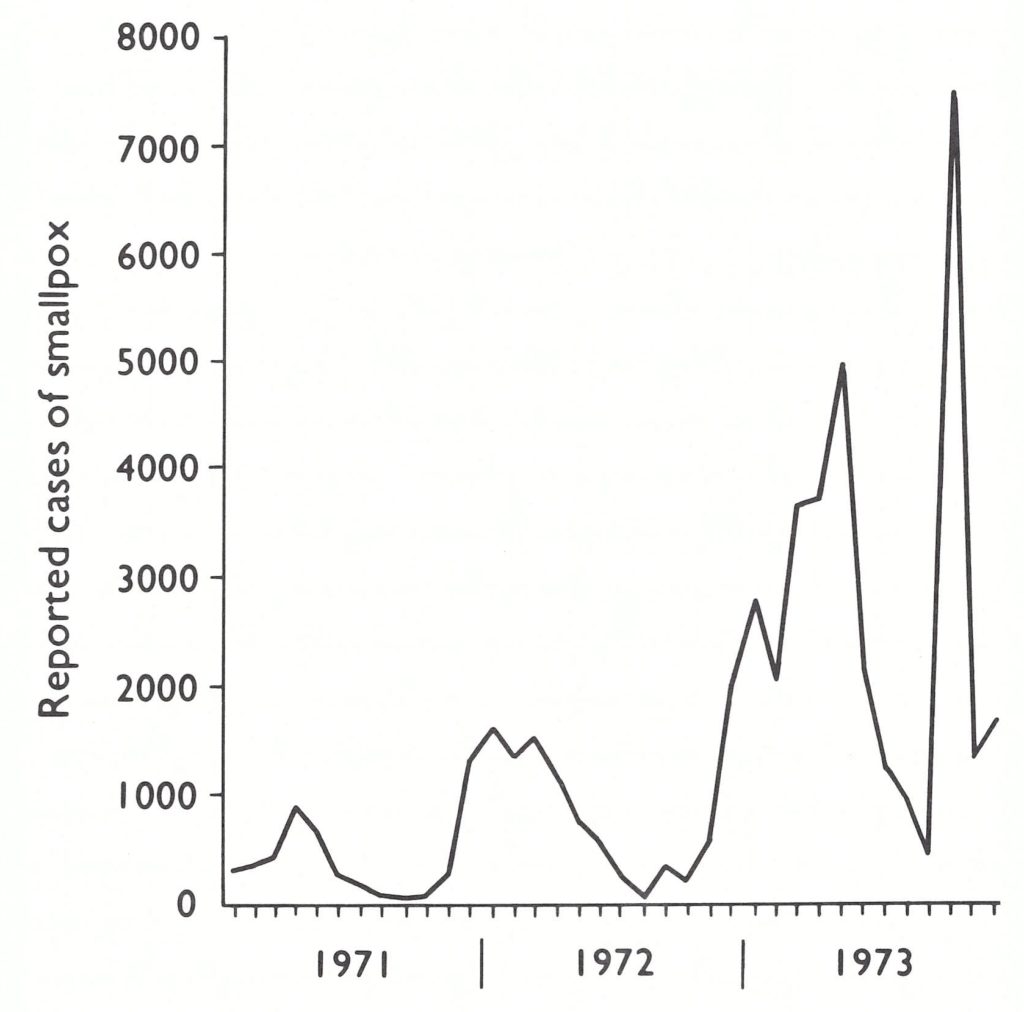
Fig. 15.8. Uttar Pradesh State: number of reported cases of smallpox, by month, 1971-1973.
Table 15.15: Southern India: number of reported cases of smallpox, 1971-1973a
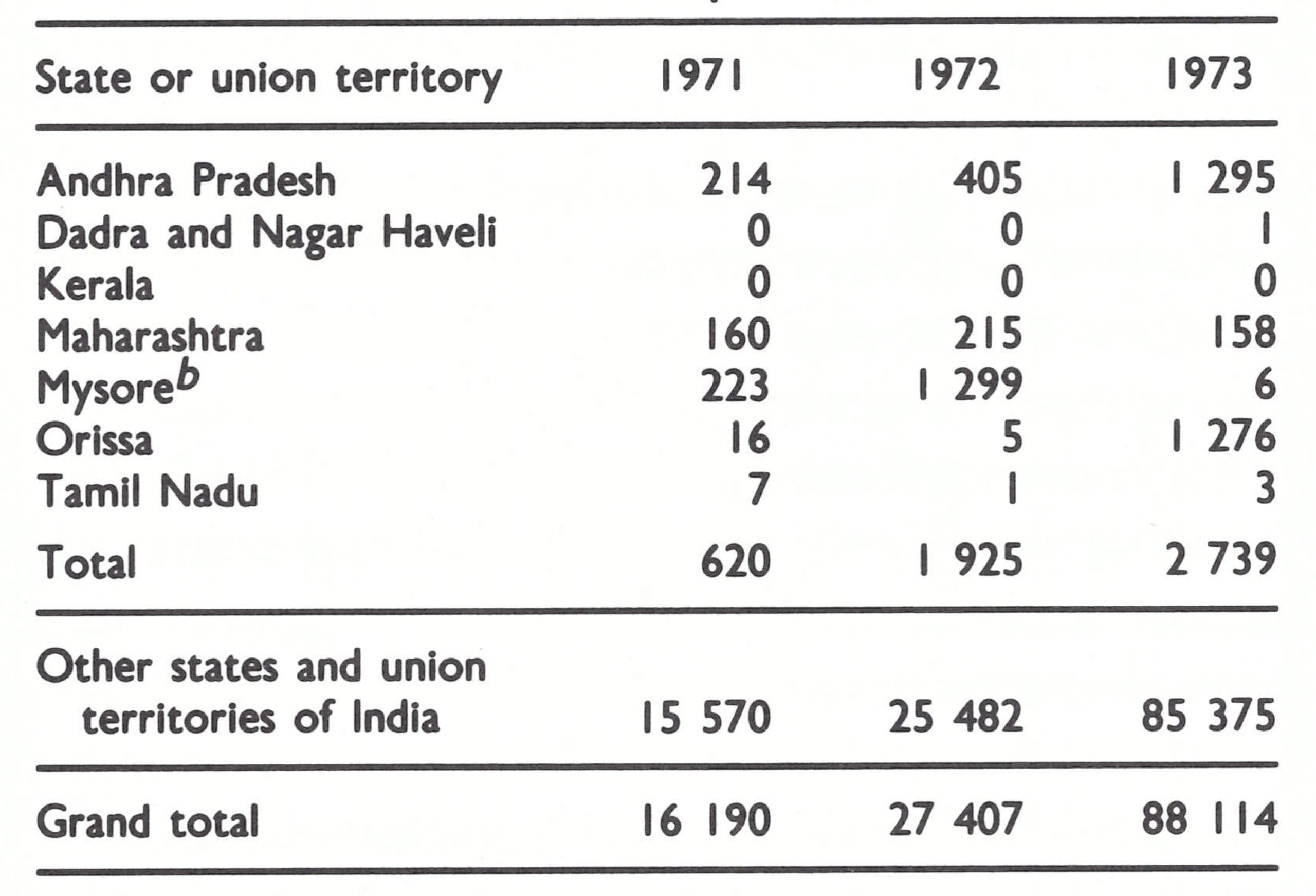
a No cases were reported during this period from the union territories of the Andaman and Nicobar Islands, Goa, Daman and Dlu, Lakshadweep, and Pondicherry.
b Became the state of Karnataka late in 1973.
The findings in Kerala provided further encouragement but, in February 1972, it suddenly became apparent that there were serious, hitherto unrecognized, problems in Mysore. The discovery of smallpox in Mysore was made by surveillance teams in the neighbouring state of Andhra Pradesh, whose programme was directed by Dr M . C. Appa Rao. There, case detection had improved significantly when, at the end of 1971, a sum of 10 rupees (US$1.33) was awarded by the government for the discovery of a case—the first time in India that such a reward had been offered. The teams detected outbreaks in Hyderabad whose source of infection was a village in Gulbarga District, one of 19 districts of Mysore State. The outbreak was unknown to the Mysore state programme officer. The district (population, 1.7 million) had an extensive network of health facilities, including a large general hospital, 71 health centres and dispensaries, a medical college, and special programmes for the control of malaria, filariasis and tuberculosis and for family planning. It was assumed that if smallpox cases had been present, they would have been quickly detected. State officials, in collaboration with Dr Zikmund, began an immediate investigation. It soon became apparent that not one but numerous outbreaks had occurred, beginning almost 15 months earlier, in December 1970. By the end of March, the investigators had discovered 81 outbreaks and 730 cases. They found that even the staff members of primary health centres who lived in villages with major outbreaks had not reported them; many directors of primary health centres who were notified of cases dismissed them as chickenpox; and, indeed, the District Director of Health and Family Planning, who had been officially informed of smallpox cases as early as September 1971, had suppressed the reports. It was concluded that radical measures would be required to stop the epidemic.
Able leadership was provided by a newly appointed District Medical Officer of Health, Dr Rama Rao; health staff were transferred from other districts; and all health and family planning staff in Gulbarga District were mobilized to undertake repeated houseto-house searches for cases throughout the district. When outbreaks were discovered, they were promptly contained. New outbreaks rapidly decreased in number, from 34 in April to 12 in May and 4 in June. To counter the tendency to conceal cases, a reward of 25 rupees (US$3.33) was offered to anyone who reported a case of smallpox. However, cases spread from Gulbarga to 5 other districts in Mysore, to 2 districts in Andhra Pradesh and to at least 1 district in Maharashtra. More than 1400 cases in all were traced to this single district. Although the outbreaks were largely contained in a period of 2 months, fully 6 months elapsed before transmission finally ceased. Most surprising to senior Indian and WHO staff alike were the numbers of health staff who could be mobilized, the rapidity with which a search programme could be organized, and the responsiveness of staff in executing a wellconceived plan. This experience was subsequently replicated in Muzaffarnagar District, Uttar Pradesh (see previous section) and, in May 1973, throughout Orissa State. It ultimately led to the plan to undertake nation-wide searches for smallpox cases-the essential strategic component of the campaign beginning in the autumn of 1973.
Although transmission was successfully interrupted in Mysore by September 1972, Hyderabad, the capital of Andhra Pradesh, had by then been reinfected; from there the disease spread to 8 other districts. Dr Appa Rao, who was responsible for other programmes in addition to smallpox eradication, was unable to devote sufficient time to the programme and smallpox continued to spread, albeit slowly. Smallpox was reasonably well contained, with the help of Dr Zikmund, until January 1973, when he was forced to leave for Orissa because of outbreaks there resulting from importations from the Salt Lake Refugee Camp. Smallpox continued to spread in Andhra Pradesh. Between January and June 1973, 924 cases occurred. In view of the size of the population (47 million), the number of cases was not large but, clearly, transmission in Andhra Pradesh and the southern states was not being interrupted as quickly or as easily as had been hoped. The potential for epidemic spread remained, as the Gulbarga experience had shown. The movement of smallpox was too rapid and effective to be contained by the few epidemiologists available.
West Bengal and the Salt Lake Refugee Camp, 1971
The densely populated state of West Bengal (population, 46 million), with its crowded capital city of Calcutta (population, 7 million), was a demographic centre of vital importance to smallpox eradication in the eastern states of India. In West Bengal, progress in the control of smallpox appeared to be satisfactory-until December 1971. The number of recorded cases had diminished to only 374 in 1970 and to 217 in 1971, the lowest totals ever reported. The Eastern Province of Pakistan (later Bangladesh) on its eastern border, predominantly Muslim but also Bengali-speaking, had detected its last case in August 1970 (see Chapter 16). Thus, importations of smallpox by travellers who frequently crossed the border were not a threat. However, civil war began in March 1971 in East Pakistan, and during that year an estimated 10 million refugees fled across the border into India. Numerous refugee camps were set up, primarily in West Bengal, Madhya Pradesh and Assam. It was feared that if smallpox were introduced into the camps, devastating epidemics would rapidly develop. On the orders of the National Smallpox Eradication Programme staff, all refugees entering the camps were examined for the presence of smallpox, but no cases were found. As a preventive measure, state officials were requested to ensure that all persons entering the camps were vaccinated. Indian national staff and WHO advisers visited and confirmed that this procedure had been followed in a number of camps, but not in West Bengal, where the state authorities refused to permit national intervention. The largest refugee camp, the Salt Lake Camp near Calcutta, sheltered an estimated 200 000-300 000 persons, and there an international private voluntary organization had been given responsibility for providing health services. For reasons unknown, no vaccination campaign was conducted.
Smallpox was probably introduced into the Salt Lake Camp in November. Many cases were hospitalized within the camp but were diagnosed as chickenpox. The diagnosis of probable smallpox was finally made on 19 January 1972 by an epidemiologist in the USA while viewing a television news documentary made in the camp. The report was relayed rapidly from Atlanta to Geneva to New Delhi. The Director of Health Services of West Bengal categorically denied there were cases, but Dr S. N. Ray, from the National Programme office, flew to Calcutta and, on visiting the camp, found an extensive outbreak. A vaccination programme was begun, but it was too late. On 16 December 1971, one month earlier, the independence of Bangladesh had been proclaimed. By 20 January 1972, an estimated 50 000 refugees had already departed for Bangladesh. The epidemic spread from the camp through West Bengal and from there to the neighbouring states of Orissa and Bihar. West Bengal, which had detected only 217 cases in 1971, reported 4753 in 1972; Bihar reported 1307 cases in 1971 and 4153 in 1972.
The number of cases that occurred in the camp can never be known, but as from 22 January, infected persons among the refugees remaining in the camp were admitted to the Calcutta Infectious Diseases Hospital ; admissions continued until the end of February. During this period, the hospital admitted 764 patients, of whom 48% died (Guha Mazumder & Chakraborty, 1973).
West Bengal, which had been comparatively free of smallpox in 1971, became a major epidemic focus in 1972 (Fig. 15.10) and Bangladesh was again reinfected (see Chapter 16).
Chickenpox - A Problem in Surveillance in Kerala
Cases of and deaths from severe chickenpox proved challenging for differential diagnosis, especially among adults. In Kerala (population: 24 million), adult chickenpox cases occurred unusually frequently, leading to erroneous reports and special investigations. To confirm that transmission had been interrupted in India, a study in Kerala verified the accuracy of death diagnoses attributed to chickenpox (White, 1978).
Age Distribution of Deaths Due to Chickenpox, January 1975–March 1976
| Age Group (years) | Males | Females | Total | Prevalence per 100,000 of Chickenpox Cases |
|---|---|---|---|---|
| 0–4 | 6 | 3 | 9 | 64 |
| 5–9 | 2 | 1 | 3 | 102 |
| 10–19 | 4 | 3 | 7 | 87 |
| 20–29 | 1 | 3 | 4 | 59 |
| 30–39 | 14 | 3 | 17 | 56 |
| 40–49 | 34 | 1 | 35 | 69 |
| 50–59 | 34 | 5 | 39 | 48 |
| 60–69 | 31 | 14 | 45 | 31 |
| ≥ 70 | 74 | 27 | 101 | 36 |
| Total | 200 | 60 | 260 | 71 |
a Based on a special search in April 1976 in 11 primary health centres.
Of the 260 chickenpox deaths over 15 months, 241 were adults aged 20 and above. Many deaths were attributed to "old age" or other health issues, with chickenpox as a contributory factor.
The frequency of adult cases was thought to be due to the dispersed population in Kerala, where travel between villages was challenging, delaying exposure to chickenpox until adulthood. However, similar adult chickenpox prevalence was not observed in other isolated areas of Africa and Asia, suggesting additional factors were involved.
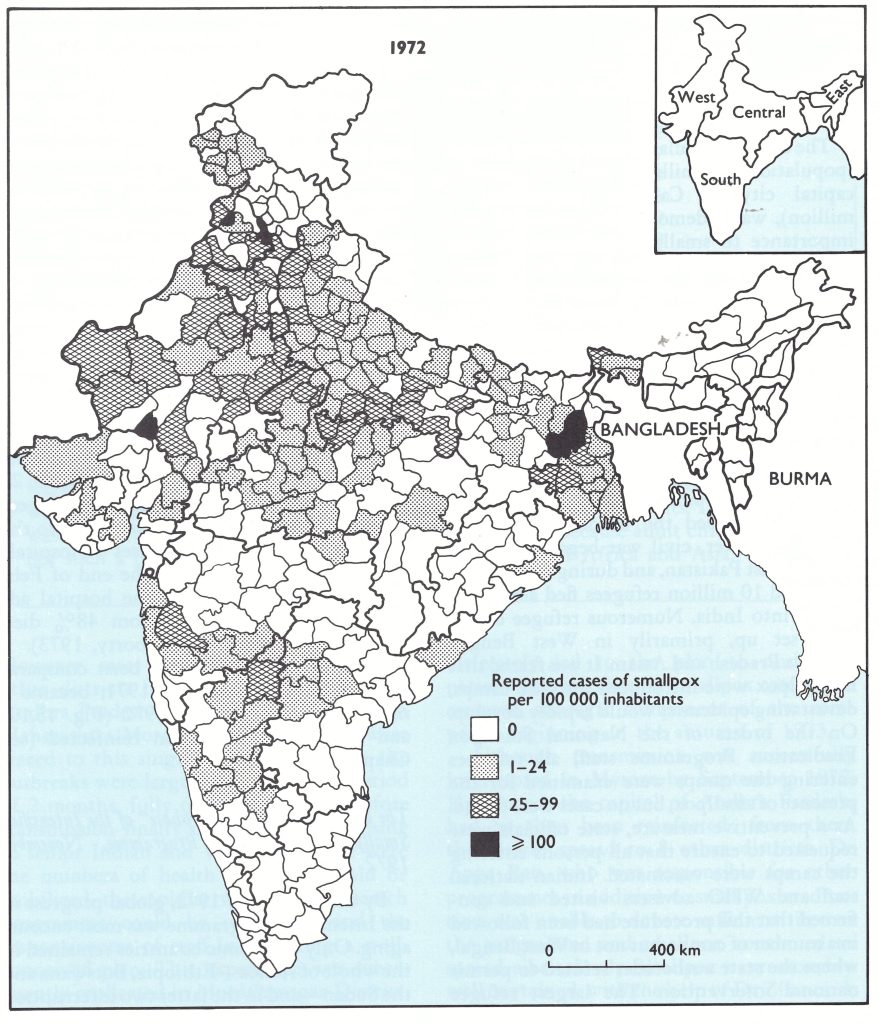
Fig. 15.10. India: number of reported cases of smallpox per 100 000 inhabitants, by district, 1972.
The beginning of the ‘final phase” of the Intensified Smallpox Eradication Programme, November 1972
By the autumn of 1972, global progress in the Intensified Programme was most encouraging. Only 3 endemic countries remained in the whole of Africa—Ethiopia, Botswana and the Sudan—and in the latter two interruption of transmission appeared imminent. Both South America and Indonesia were smallpox-free and Afghanistan was almost so. Bangladesh had been reinfected but it had re-established its national programme and Pakistan’s programme had been extended to the entire country. India was reporting increasing numbers of cases as epidemic smallpox began moving across the Ganges plain from the west and from Calcutta in the east. However, the extent of the infected areas in India, as well as in other Asian countries, had diminished significantly (Fig. 15.11).
With endemic smallpox so limited geographically and some form of surveillance operating in all areas, it seemed to WHO propitious to encourage a more concentrated effort in the remaining infected areas: the “final phase” of the Intensified Programme. The proposed target was ambitious-to interrupt smallpox transmission during the following 2 smallpox seasons, a period of about 18 months. To encourage the renewed effort, special seminars were convened in September-November in Addis Abeba (mainly for staff in Ethiopia and the Sudan); in Karachi (principally for staff in Afghanistan and Pakistan); and in New Delhi (for staff in Bangladesh, Bhutan, India and Nepal).
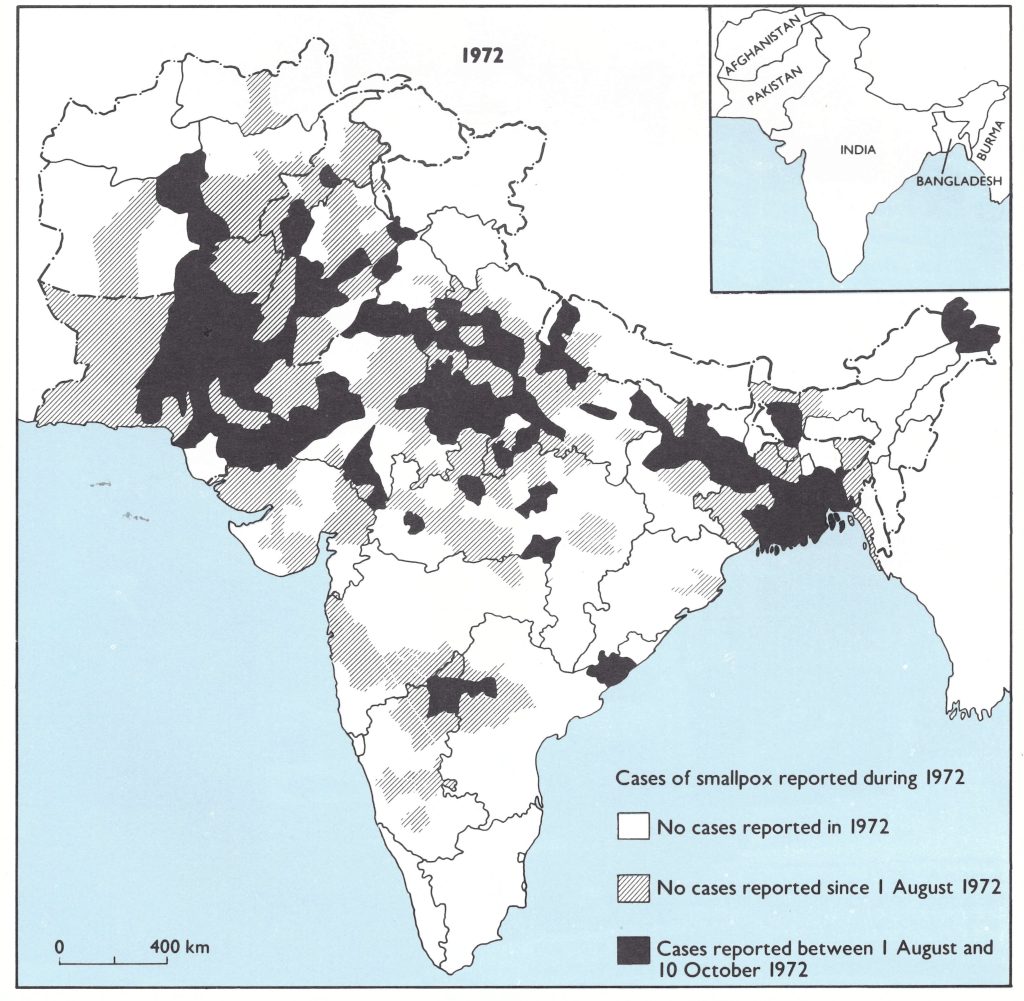
Fig. 15.11. Indian subcontinent and adjacent countries: areas reporting cases of smallpox during 1972 (as of 10 October).
Plate 15.5. Refugees from East Pakistan, many infected with smallpox, leave the Salt Lake Camp near Calcutta in December 1971 to return to their newly independent country, Bangladesh.
In India, despite the success of surveillance-containment measures in southern and western states, many state health officials still persisted in their belief that 100% vaccination was the only way to achieve eradication. With officials from all over India attending the seminar, attention was focused explicitly on the surveillance-containment strategy. The success in Indonesia was a helpful stimulus in encouraging a change in direction, as is illustrated in the following extract from Henderson’s opening address:
“Two years ago, in December 1970, a seminar on smallpox eradication was held in this very room. I said at that time that the question was repeatedly asked as to how such major changes [in the smallpox eradication programme] could occur so rapidly when, for years, many endemic countries had been conducting mass vaccination programmes with only limited success. The principal difference between present and past efforts is one component—surveillance. In every country where a concerted effort has been made to investigate promptly and to contain every outbreak, smallpox transmission has been interrupted within two years or less. Many of you will recall that at that Seminar the director of the Indonesian programme presented a provocative paper which stated `a proper surveillance-containment action brought smallpox under control in a short period, while on the contrary, routine vaccination and mass vaccination campaigns had little effect in interrupting smallpox transmission’. That year, Indonesia reported 10 000 cases of smallpox, only 20°o fewer cases than in India. Many at that Seminar took violent exception to the Indonesian director’s contention that all available resources should be diverted to surveillance even at the expense of a vaccination campaign. Who was SMALLPOX AND ITS ERADICATION right? I would ask you to note that the number of cases in Indonesia decreased from 10 000 in 1970 to 2000 in 1971 and to 34 this year. Despite a continuing active search for cases, none have been found in all of Indonesia for over eight months .”
State health authorities in India had argued that there were not enough health staff. However, it was noted that, even in countries with less well developed health infrastructures, such as Ethiopia, only 80 workers were employed (1 for every 300 000 persons) and in Afghanistan the corresponding ratio was 1 for every 100 000 persons. In India, 1 smallpox vaccinator was available for every 8000-20 000 persons.
The need for surveillance was echoed in the address by the Indian Minister for Health and Family Planning and by Dr P. Diesh, the Additional Director-General of Health Services, who concluded the seminar with the statement: “History tells us that whoever rules the Indo-Gangetic plain rules the country. The battle of smallpox will be fought in the Indo-Gangetic plain, where 70 % of the cases are reported now.” And this indeed was where the major battle was fought over the following 3 years.
The seminar report concluded with a number of recommendations which stressed surveillance
- It is essential to delineate smallpox endemic and non-endemic areas within a state or country. The endemic areas should receive highest priority and the major part of the resources at present available. In the non-endemic areas, an active search for cases should be planned and implemented to ensure their smallpox-free status. Any suspected cases should be dealt with as a national public health emergency.
- In states where surveillance teams are not yet in existence, state teams should be created by 1 December 1972.
- The investigation of all outbreaks by the state programme officer or at least by state surveillance teams is essential.
Other recommendations emphasized the importance of containment and the need to trace the source of outbreaks. It was also noted that “the newly introduced reporting system in India should be improved as rapidly as possible” . The new system was that previously described, in which primary health centres, districts and states reported weekly all cases of smallpox detected during a given week or reported “nil” if no cases were found.
The central programme office was further strengthened in the autumn of 1972, with the appointment of a senior publicihealth officer to head the programme, Dr R. N. Basu, Assistant Director-General of Health Services (Smallpox), who continued in this position until the conclusion of operations. Dr Basu, who held a more senior rank than Dr Singh, carried greater weight with national and state officials. Dr Diesh, who was effectively second in command to the Director General of Health Services in the Ministry, also took a special interest in the programme and made a number of visits to the state capitals to meet health ministers and directors of health services in order to encourage greater activity. Visits by an official of this rank were uncommon and implicitly indicated that the government accorded high priority to the smallpox eradication programme. Meanwhile, working relationships between WHO staff and Indian national and state staff had gradually become less formal. Arrangements for WHO staff from the regional office to travel to the field and for state-assigned staff to travel from state to state had become a simple matter of discussion and verbal agreement. This was in marked contrast to the earlier formal relationships which required that, before each trip, a written request should be submitted by the WHO Regional Director to the Ministry of Health and that this request should be considered within the Ministry and eventually a formal reply—prepared a process that often took weeks. With each adviser in possession of a vehicle purchased by WHO and an agreement by WHO to defray all travel costs, a further obstacle to the execution of the programme was removed.
Plate 15.6. Rabinder Nath Basu (b . 1928), Assistant Director-General of Health Services, was appointed to direct the National Smallpox Eradication Programme in the autumn of 1972 and continued in this capacity until after the certification of eradication in 1977 . He subsequently directed the development of India’s Expanded Programme on Immunization and later became the Director of the National Institute of Communicable Diseases.
At the November seminar, goals were fixed in terms of geographical areas within which it was hoped endemic smallpox could be contained by the end of March 1973. For India, it was agreed that by that date the objective would be to eliminate endemic smallpox from all areas except the state of Bihar and 49 districts comprising parts of Uttar Pradesh, Madhya Pradesh and West Bengal.
As early as the end of December 1972, it was evident that the problems once again were greater than had been anticipated. As has been mentioned earlier, major epidemics were discovered in the previously smallpox-free state of Jammu and Kashmir. In Bihar State, health workers went on strike, bringing all work to a standstill. In Uttar Pradesh, then the principal focus of smallpox, eradication staff had been diverted to a cholera vaccination campaign. The new reporting system was an improvement over the old one but, even so, half or more of the states and union territories were consistently up to 5 weeks late in reporting cases.
During 1972, 27 407 cases of smallpox were reported from India, an increase of 69% over the 16 190 cases reported the year before. More complete notification undoubtedly accounted for some of the increase but there was no way of measuring the magnitude. In January 1973, predictions as to the expected incidence of smallpox in 1973 were made by WHO Headquarters staff, in consultation with national staff, on the premise that such predictions served to gauge familiarity with the problems in each area, the rate of progress being made or anticipated and the understanding of the epidemiological situation. It was forecast that 30 700 cases would occur throughout the world, of which 17 000 would be in India. It soon became evident that neither WHO nor Indian staff had comprehended the magnitude of India’s smallpox problem.
By the end of March 1973, India had recorded 14 376 cases, of which 29% were outside the established target area. Not only were serious problems present in Bihar, Uttar Pradesh, and Jammu and Kashmir, but it had also become apparent that West Bengal had not done well in controlling the epidemic which had spread from the Salt Lake Camp area. By the end of February, 19 cases imported from Calcutta were detected in Orissa and 30 in Bihar. The estimate of the total number of cases in India projected for 1973 was revised upwards from 17 000 to 35 000 and then to 60 000, a figure which would represent the highest number of cases since 1967. Although reporting had undoubtedly improved, smallpox was far more extensive than had been expected; many still did not subscribe to the new strategy of surveillance and containment . During the spring of 1973, smallpox incidence continued to rise and by the end of June, 49 478 cases had been reported, of which 45 697 (92%) were from the 4 contiguous states in or immediately adjacent to the Gangetic plain Bihar, Madhya Pradesh, Uttar Pradesh and West Bengal. The total number of cases was almost 3 times greater than the number recorded during the same period in 1972. Comparisons with trends in Pakistan and Bangladesh (Wkly epidem. rec ., 1973b) portrayed the unfavourable situation in India (Fig. 15.12).
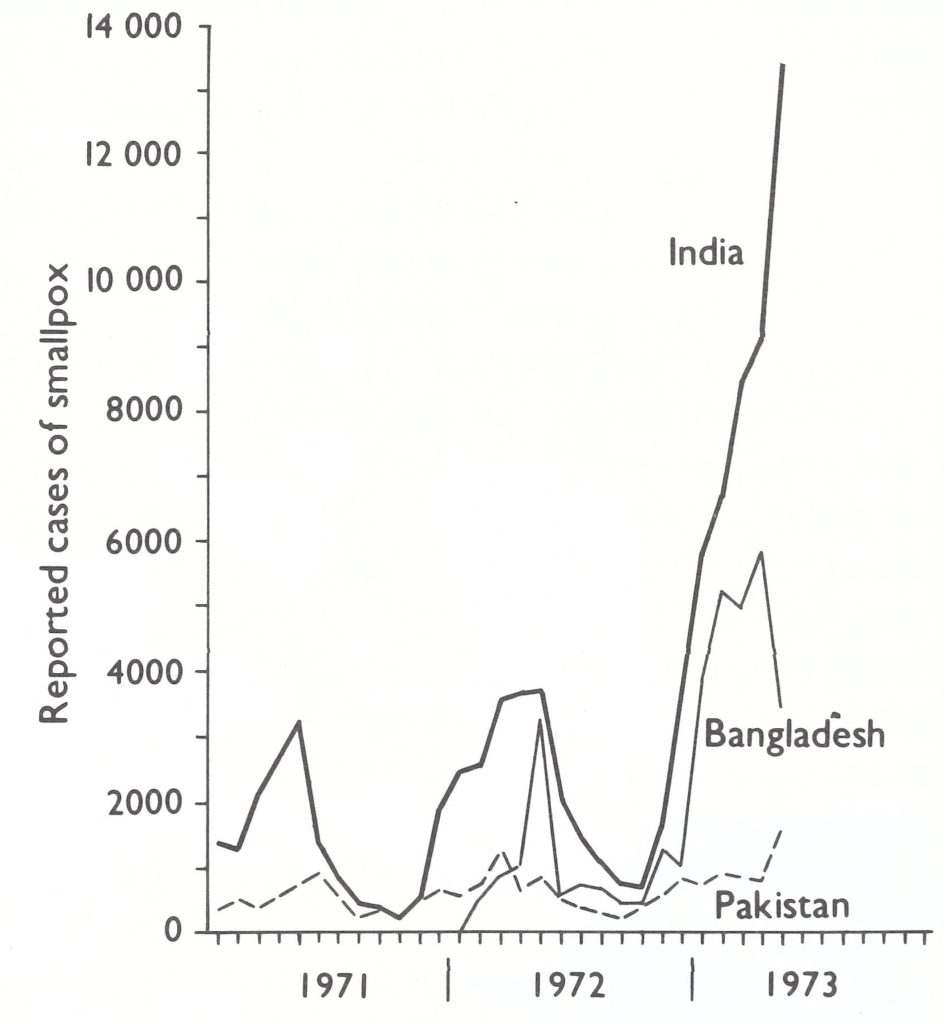
Fig. 15.12. Bangladesh, India and Pakistan: number of reported cases of smallpox, by month, 1971-1973 (as of 19 June 1973).
India was then one of only 4 countries in the world with endemic smallpox, and it accounted for nearly 60% of the world’s cases. Politicians and senior health officials alike had become increasingly concerned and had taken a greater interest in the programme. The Twenty-sixth World Health Assembly in May 1973 provided an added stimulus.
During discussions in the Health Assembly regarding the smallpox eradication programme, the delegate from Malaysia bluntly assessed the situation. His observations were summarized as follows (World Health Organization, 1973b):
“. . .an alarming development in recent months had been that serious smallpox epidemics were raging in two of the endemic countries, despite the fact that WHO was now entering the seventh year of its intensified smallpox eradication programme. Among the reasons for the setback, as given in the Weekly Epidemiological Record . . . were: lack of staff; inadequately developed surveillance programmes; periodic diversion of smallpox staff to other programmes; delayed and incomplete reporting; and inadequate containment measures. Lack of staff should not be an insurmountable problem; it could be overcome by improved deployment of staff and crash recruitment and training programmes. Nor should it be too difficult to organize and develop surveillance programmes. In view of the vital importance of smallpox eradication, any diverting of staff to other programmes would be premature and illadvised, and inadequate reporting and containment measures indicated a lack of appreciation of the urgency of the problem . He did not wish to criticize any individual country, but he hoped that the points he had raised would be taken in a constructive spirit.
“WHO had declared that it was willing to send emergency aid on request . . .to any country facing problems in smallpox eradication. He wondered whether the countries now suffering from outbreaks had taken full advantage of that offer . . .”
In the World Health Assembly, criticism such as this of another country’s health programme was unusual; to India’s Director General of Health Services, it was acutely embarrassing. He returned to India determined to strengthen the programme.
Endemic smallpox in India remained comparatively limited geographically (Fig. 15.13) although the number of cases was large, and it appeared that an intensified programme would require a special mobilization of resources in only a few states of India. With the season of diminished transmission immediately ahead, it was decided to initiate an “epidemic of activity” preceding the usual season of epidemic smallpox.

Plate 15.7. Outbreaks of smallpox occurred among poorly vaccinated pavement dwellers in crowded urban areas. The discovery and containment of such outbreaks were a continuing problem throughout the course of the Intensified Programme.
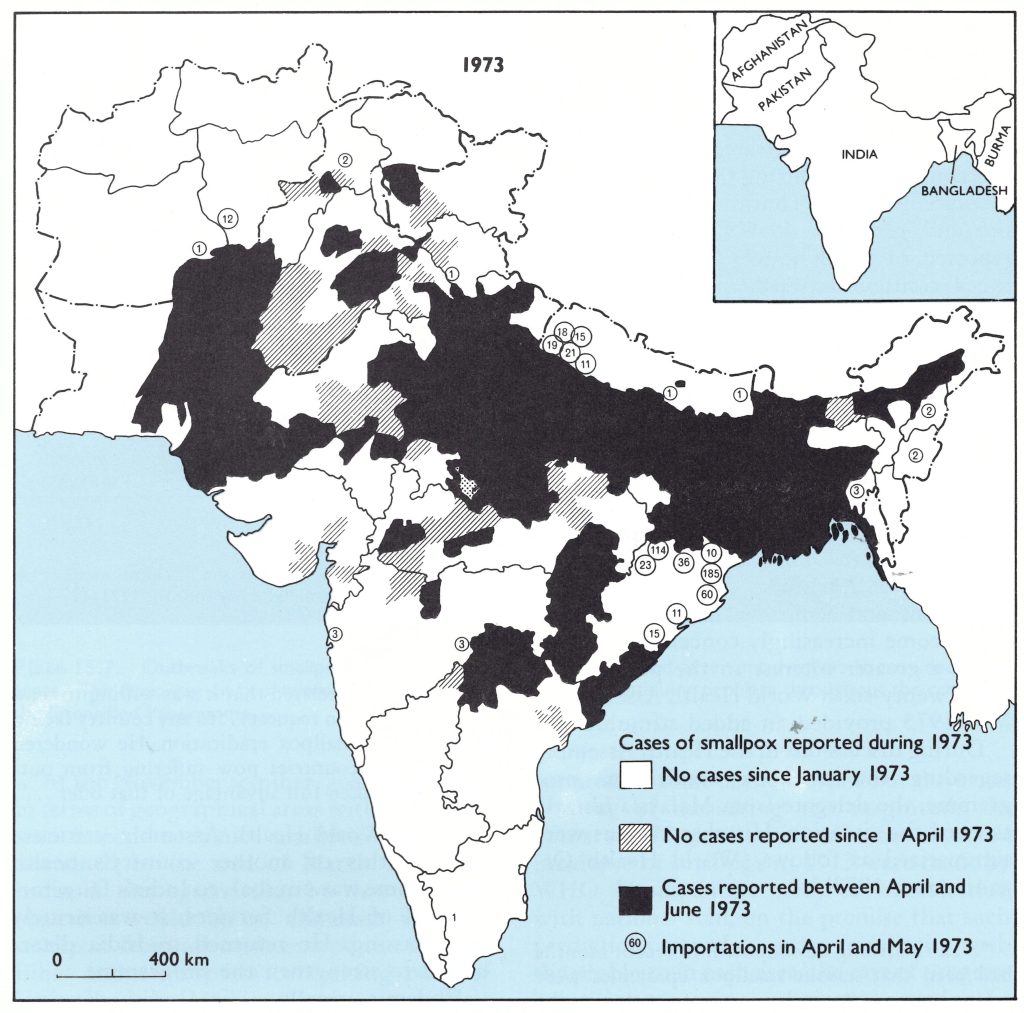
Fig. 15.13. Indian subcontinent and adjacent countries: areas reporting cases of smallpox during 1973 (as of 19 June) .
The Intensified Programme in India, June-December 1973
At the end of June 1973, WHO staff from Headquarters and the Regional Office for South-East Asia held meetings with Indian national and state health personnel to devise a new campaign plan whose strategy would be to detect and contain the comparatively few outbreaks expected to occur during the autumn months of seasonally low incidence. If most of these could be contained by December, it was expected that the remaining foci could also be contained by state and district surveillance teams during the January June period.
The most highly infected states were Bihar, Uttar Pradesh and West Bengal. There, the deployment of an epidemiologist-adviser and a few surveillance teams for motivating local staff to report cases and to contain outbreaks had clearly failed. A different approach was required. The early detection of cases was of the greatest importance. Once cases were found, a comparatively small number of containment teams could deal with the outbreaks. Everyone had been impressed by the experiences in Gulbarga District (Mysore) and Muzaffarnagar District (Uttar Pradesh), in which it had proved quite simple to plan and execute a village-by-village programme of case detection which could reach all parts of a district within 1-2 weeks. It was reasoned that if a systematic search of this type could be conducted throughout entire states, in combination with an effective containment programme, it should be possible to contain smallpox quickly. To execute such a search in a state, in a group of states or in the whole of India posed problems of organization and motivation of an entirely different magnitude from those involved in carrying out the operation in a single district. However, it was apparent that throughout the length and breadth of India a large complement of generally well-trained health staff existed albeit often poorly supervised and supported. It seemed plausible that an increased number of senior smallpox eradication programme supervisors, following a carefully designed plan, could harness this considerable resource for a concerted effort over a period of a few months. This was the basic strategy decided on, and thus began what was to become one of the most ambitious and intensive national health programmes yet undertaken. Eventually, it would involve more than 130 000 staff who, within a 2-week period, could visit more than 90% of the 120 million households in India.
The principal problem area comprised the states of Bihar, Madhya Pradesh, Uttar Pradesh and West Bengal. Their combined population amounted to 249 million, or about 42% of the entire population of India. It was planned to assign a senior Indian epidemiologist and a counterpart WHO epidemiologist-adviser to assist each state smallpox eradication programme officer in these 4 states. An additional WHO epidemiologist would continue to work in the neighbouring state of Rajasthan, in which transmission appeared to have been interrupted but which was experiencing many importations. A sixth WHO epidemiologist would be based in Orissa State to assist in the development of search programmes and the investigation of outbreaks in the low-incidence states and union territories geographically close to the 4 highly infected states. He would also assist with any problems in a third group of states which were thought to have interrupted transmission or were expected to do so by September—the smallpox-free group (Fig. 15.14). Additional transport, supplies and equipment were made available by WHO to supplement the already considerable resources deployed by India.
For the 4 highly endemic states, a 3-phase programme was formulated. Phase One, planned for the late summer of 1973, would consist of an active search for outbreaks in municipal areas. It was hoped by this search to find and eliminate urban foci, which often served to sustain smallpox transmission through the summer monsoon season. Because there was insufficient time for preparation, the first phase achieved little except to bring the smallpox eradication activities of most of the autonomous municipal corporations under the supervision of the state smallpox eradication programme office. Phase Two of the programme, from September to December 1973, would consist of statewide, week-long, village-by-village searches on 3 separate occasions approximately a month apart. Two searches would be conducted in the states with a low incidence, and at least I search in the states believed to be smallpox-free. Other health personnel and family-planning workers would be utilized to supplement the work of the smallpox eradication staff. The nature of Phase Three, commencing in January 1974, would depend on the status of smallpox at that time ; it was expected that it would consist primarily of a search for cases by surveillance teams and the containment of a few remaining outbreaks.
The government of India and WHO agreed to increase the number of senior supervisory staff for this effort. The government provided an additional senior Indian epidemiologist for each of the 4 priority states. It assigned to the programme Dr M. I. D. Sharma, then the Director of the National Institute of Communicable Diseases ; two of his epidemiologists, Dr C. K. Rao and Dr R. R. Arora ; and the Assistant Director-General for Cholera, Dr Mahendra Dutta. With Dr Basu and Dr Singh of the National Smallpox Eradication Programme, and Dr S. N. Ray, who was responsible for vaccine production, they constituted the Indian component of a group officially termed the “Central Appraisal Team”. The WHO component consisted of the intercountry team (formally, the Smallpox Eradication and Epidemiological Advisory Team), Dr Grasset and Jezek, who were joined that summer by Dr William Foege, who had formerly worked in Nigeria and then at the Communicable Disease Center (later called the Centers for Disease Control) in Atlanta, GA, USA, in directing the smallpox eradication effort in western Africa. In January 1974, Dr Lawrence Brilliant, a new member of the WHO smallpox eradication programme staff, became part of the team.
Plate 15.8. State review meeting in Lucknow, Uttar Pradesh, in 1975. Seated, left to right: M. C. Chaturvedi, Additional Director of Medical and Health Services of Uttar Pradesh; C. K. Rao, member of the Central Appraisal Team; J. M. McGinnis, WHO consultant from the USA; M. I. D. Sharma, Commissioner of Rural Health for India; and N. C. Grasset, smallpox adviser from the WHO Regional Office for South-East Asia. Standing: M. Dutta, member of the Central Appraisal Team.
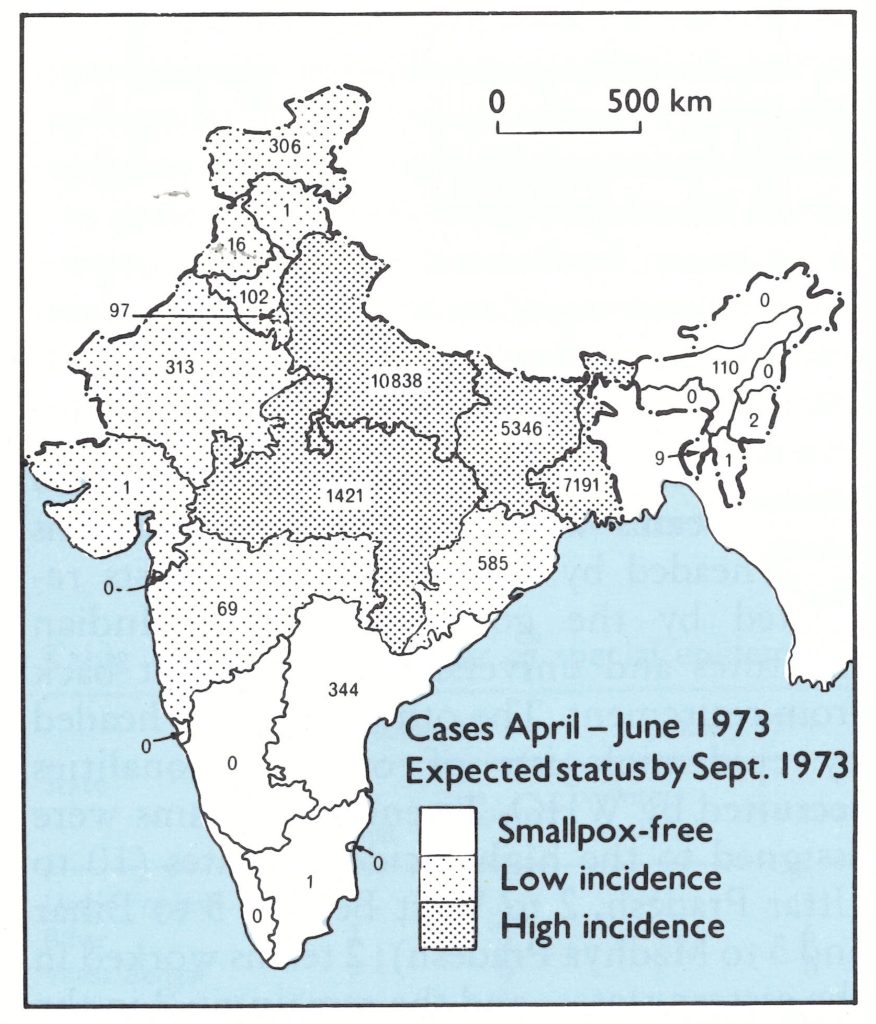
Fig. 15.14. India: autumn campaign of 1973. Number of reported cases of smallpox by April -June 1973 and the expected status of smallpox incidence, by state, in September 1973.
Beginning in June 1973, the group held frequent meetings, preparing, reviewing, and revising drafts of a “Model Operational Guide for Endemic States” and a “Model Operational Guide for Non-endemic States”. To implement the programme in the field, 26 special teams were created. Half the teams were headed by Indian epidemiologists recruited by the government from Indian institutes and universities or brought back from retirement. The other half were headed by epidemiologists of other nationalities recruited by WHO. Twenty-two teams were assigned to the high-incidence states (10 to Uttar Pradesh, 2 to West Bengal, 5 to Bihar and 5 to Madhya Pradesh); 2 teams worked in the eastern states; and the remaining 2 in the smallpox-free and low-incidence states in the south.
Eventually, a total of 230 epidemiologists from 31 countries and a comparable of Indian epidemiologists would head such teams for periods of 3-24 months each. As many as 90 epidemiologists would be participating at any one time. Each epidemiologist was given 5 days’ training before going to the field. Particularly useful for this purpose was a series of slides prepared by WHO illustrating clinical smallpox and 2 casehistory studies, one of which dealt with the day-by-day management and investigation of a smallpox outbreak and the other with the management of a district smallpox eradication programme. (The latter eventually found its way into the syllabus of the Harvard School of Business Administration.)
As the autumn campaign began, there were only 26 epidemiologists in the field (Table 15.16). Each epidemiologist in the highincidence states worked in a zone covering an average of 5-6 districts (approximately 10 million people) and had as his counterpart the division and/or district health officer responsible for the area. The special teams conducted training sessions for district and local staff to explain and organize the searches. In addition, they supervised the implementation and evaluation of surveillance activities and verified the diagnosis when cases were reported. When smallpox was detected, they organized outbreak containment and identified the source of infection.
Table 15.16: India: number of special epidemiologists working in the field, October 1973-July 1975
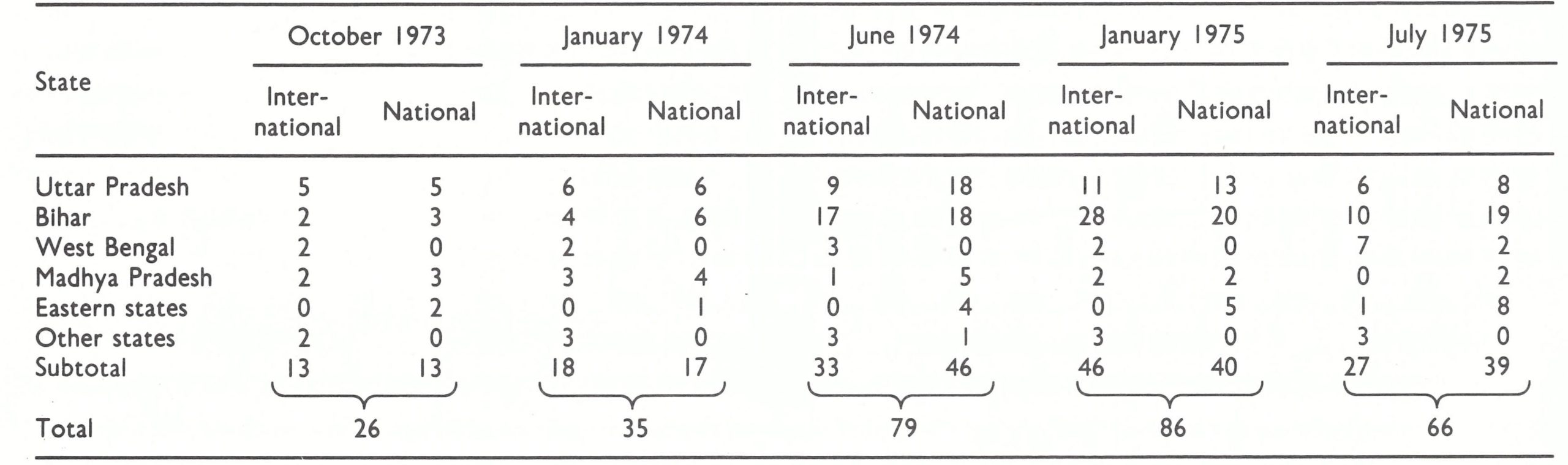
Additional vehicles were essential and these were quickly obtained through the purchase by WHO of jeeps manufactured in India. For WHO, this was a departure from a long-standing policy that the country itself should-purchase locally produced equipment and supplies. Prompt delivery of the vehicles would have been impossible if traditional procedures had been followed—i.e ., the purchase of Indian-made jeeps by the government or the purchase of foreign-made vehicles by WHO. To have manoeuvred such a purchase through the complex Indian bureaucracy, even with the highest level of government support, would have taken anything up to a year; the delivery of vehicles from foreign sources was even more protracted at that time. The Indian-made jeeps, although more susceptible to mechanical failure, were simpler in design and easier to repair. A most important consideration was that spare parts were widely available and there were many mechanics who were familiar with the vehicle. On balance, the Indian Jeeps proved more utilitarian than did imported vehicles.
Each of the epidemiologists was assigned a driver and a paramedical assistant and given a monetary advance (an imprest account) to be used, as necessary, for petrol and vehicle repair, travel allowances and supplies. The funds were accounted for at regular intervals before further advances were made. The disbursement of funds for the discretionary use of the field epidemiologists was also a departure from customary administrative practice, but it was one of the most important steps in facilitating the execution of the programme.
The strategy of the search programme and of the surveillance-containment activities was explained in detail at state-level meetings presided over by state officials and attended by senior officials of the national government and WHO, as well as by state and divisional and/or district health officers. These discussions were followed by similar meetings at the divisional level (for states with a divisional structure) convened by the commissioners of the divisions and attended by chief medical officers of health from the districts and municipal corporations. Meetings were then held at the district level, attended by the district health officers and primary health centre medical officers. Lastly, searchers and number supervisors at each primary health centre were instructed in the specific techniques of search, outbreak containment and reporting. Such meetings at different administrative levels were subsequently conducted before each new search; the experiences of the previous search were evaluated and additional or revised procedures implemented.

Plate 15.9. Project vehicles in Patna, Bihar State, at the beginning of the programme.
To organize the numerous meetings and to develop strategy over the extensive area involved required an extraordinarily intensive effort on the part of the Central Appraisal Team . As an illustration of this endeavour, one may cite the experience of a member of the team who travelled more than 1800 kilometres by car in 5 days, during which he participated in 7 district and regional meetings. To do so necessitated driving all day and through the night; the team member and his driver shared this task, alternately driving and sleeping in the cramped jeep.
The organizational plan called for one search worker to visit one village or section of a city each day. The hundred or more villages in each primary health centre area were divided up among the staff of 15-20 health workers. To facilitate supervision, a search schedule determined which worker would be in which village on which date. Each search was planned to be completed within 7-10 days. A supervisor oversaw the work of 4 or 5 workers and was assigned villages to be checked at random.
The searchers were instructed to show the WHO smallpox recognition card (see Chapter 10, Plate 10.11) and to inquire about any suspected cases that had occurred during the preceding 2 months. All village leaders and watchmen were to be contacted, as well as schoolteachers and their pupils, and persons congregating in tea-shops and market areas. Two or 3 houses in each of 4 parts of a village and the section of a village or town in which the poorest families lived were also to be visited. When the teams travelled from village to village, they were instructed to stop at brick kilns, bus stands, migrant camps and festivals to solicit reports of possible cases of smallpox.
Suspected cases were to be notified immediately to the primary health centre physicians, who were asked to verify the diagnosis. In addition to the assessment of work by the supervisors, each primary health centre medical officer was expected independently to assess one village or urban area assigned to each supervisor; each district-level supervisor was expected to visit one village, one school and one market in each primary health centre area; and each state surveillance team was expected to check 100 villages, 10 markets and 30 schools after each search. Areas selected for assessment were the least accessible villages and those most distant from the primary health centre. It was assumed that if the work was well done in the more distant and difficult areas, it was likely to be satisfactory in the areas easy of access. Radio, press, and other media were utilized to inform the public where to report cases of smallpox.
The first searches in the highly endemic states began in September. With such large populations and with so many health staff involved, the logistic requirements were formidable, as will be appreciated from the following inventory of material supplied to West Bengal for its first search: 100 copies of the Operational Guide; 10 000 small smallpox recognition cards and 3000 large recognition cards; 100 copies of each district map to be used to plan search workers’ schedules; 3000 copies of the searchers’ village-by-village schedules; 16 000 copies of forms for recording the results of the village visit; 400 copies of forms for listing outbreaks; and 3000 copies of the weekly reporting form to be dispatched from the primary health centres to the district. For a country-wide search, it was calculated that 8 tonnes of forms would be necessary.
Because of floods, only 9 out of 16 districts in West Bengal could be reached during the September search; but only 75 cases of smallpox were detected . It was uncertain whether the search had been good and the few cases that existed had been found, or whether it had been poor and many cases had been missed. However, a more extensive search conducted throughout the state in early October identified only 143 infected villages among West Bengal’s 38 000 villages and 137 towns. Moreover, Calcutta, which many had feared might harbour extensive foci, had far fewer cases than had been expected.
The encouraging reports from West Bengal were quickly followed by alarming almost unbelievable reports from Uttar Pradesh and Bihar. During the week preceding the search, only 354 cases in 21 districts had been reported in Uttar Pradesh and only 134 cases in 8 districts in Bihar. However, the 1-week October search revealed 1525 outbreaks with 5989 cases in Uttar Pradesh and 614 outbreaks with 3826 cases in Bihar (Fig. 15.15 ; Table 15.17). It should be noted, however, that outbreaks occurred in only 1.3% of all villages in Uttar Pradesh and in only 0.9% in Bihar. However, smallpox was found in 42 out of the 293 municipalities in Uttar Pradesh, in 13 out of 161 in Bihar, and in almost all districts of both states.
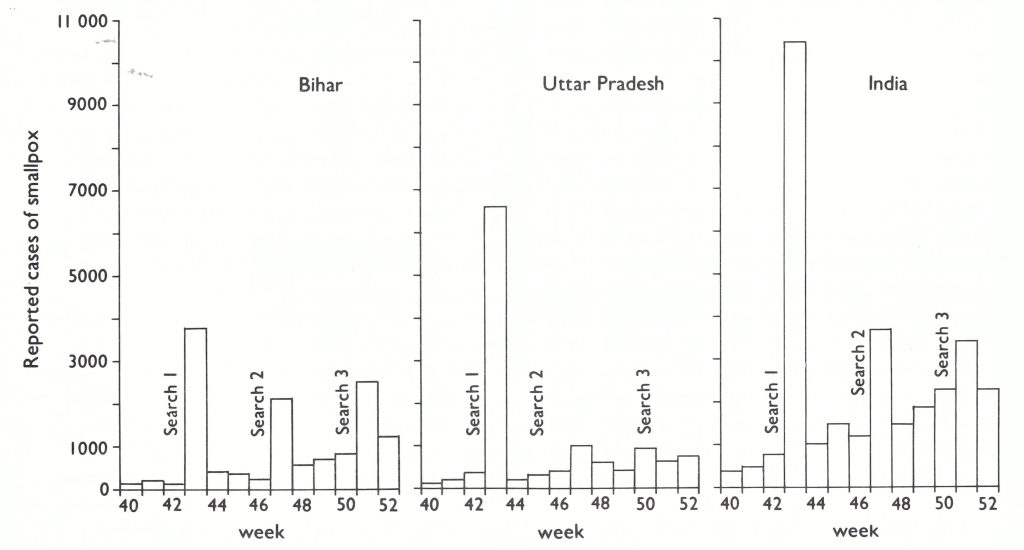
Fig. 15.15. Bihar State, Uttar Pradesh State, and India as a whole: number of reported cases of smallpox, by week, showing results of special searches, October-December 1973.
Table 15.17: Bihar, Uttar Pradesh and Madhya Pradesh : results of the 1973 search for outbreaks of smallpox
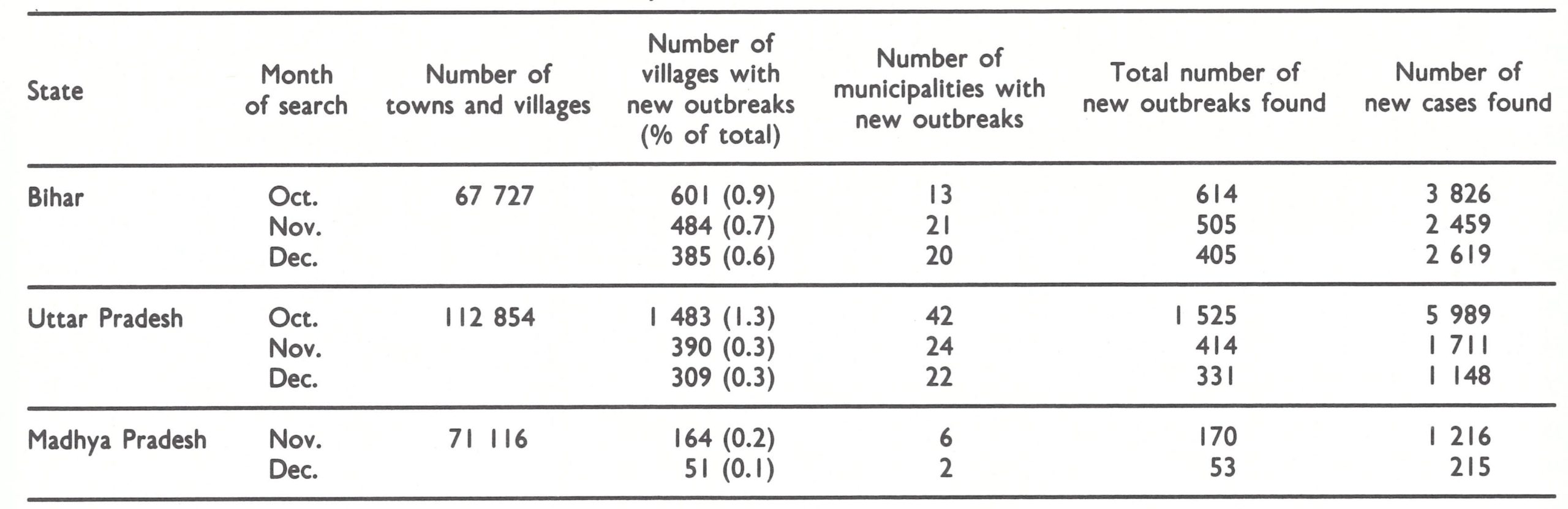
The staff had cause for alarm because, in October, smallpox incidence was at a seasonal low. Moreover, the percentage of villages then infected was equivalent to the percentage infected at any time during the course of an entire year in the studies by Dr D. B. Thomas and his colleagues in Sheikhupura District in Pakistan (Thomas et al .,1972 ; see Chapter 14). Until this time, Sheikhupura District had been considered to be the prototype of a district with an unusually high incidence of smallpox in the generally well-vaccinated Indian subcontinent.
Despite the extensive planning and training, assessment revealed that many villages, indeed entire areas, had not been searched, and thus even the high figures recorded understated the problem. With smallpox present throughout both states and in many urban areas, it was apparent that when transmission rates increased, a major epidemic would be possible. In neither state were the health services functioning well and a 3-month period of intensive training and supervision provided little time in which to improve the performance.
The November and December searches were more thorough than the October search. Nevertheless, the number of infected villages which were discovered decreased in both states—more sharply in Uttar Pradesh, suggesting that the new strategy was having an impact. In Madhya Pradesh, geographically India’s largest state, the first search was delayed until November because of floods. The results there were highly encouraging. Only 170 outbreaks were found in November and only 53 in December.
Searches in 8 “low-incidence” states revealed only 4 with outbreaks and, during 2 separate searches, fewer than 200 cases were discovered in each (Table 15.18).
Of 10 states which had been expected to be free of smallpox by September, only Andhra Pradesh was found to have had outbreaks, and, in all, only 197 cases were discovered (Table 15.19).
As 1973 ended, it was apparent that large areas of India had remained free of smallpox (Fig. 15.16), and the search programme had confirmed this. In December only 6 states recorded 100 or more cases, and 2 of them—Bihar and Uttar Pradesh—accounted for 84% of the total (Table 15.20 ; Fig. 15.17). Although the total number of cases recorded in India was 88 114, the highest since 1958, reporting was far more complete than it had ever been.
The autumn campaign had shown that it was possible to mobilize health resources effectively throughout entire states to search for cases and to contain outbreaks. However, with smallpox still widely prevalent in the 4 central states and the period of high transmission again beginning, it was clear that Phase Two of the campaign had to be extended into 1974.
In early January 1974, Henderson had meetings in New Delhi with Indian and WHO staff to assess possible strategies and needs for the coming months. The situation was critical. If the intensified search campaign was to continue, a commitment of additional funds was urgent. Funds earmarked for India in the WHO regular budget were sufficient to cover the campaign activities for 2-3 more months at most. To obtain additional money from WHO was a problem. WHO’s budget for smallpox eradication had remained at a constant level since 1967. The funds had been proportionately allocated to each of WHO’s regional offices in 1967 and the proportions had not changed thereafter. With the certification of eradication in the Americas in 1972, it had been requested that the 1973 allocation for that region should be transferred to the SouthEast Asia Region. However, the proposal was turned down. Within the South-East Asia Region, some diversion of funds from Indonesia, now free of smallpox, was possible but the amount was not great. Meanwhile, repeated appeals to governments for support had brought generous donations of vaccine but little cash. A further emergency appeal was considered but thought to be futile because governments could seldom respond to such requests in less than several months to a year. Although the programme in India had achieved a momentum which offered hope of success, little could be done without additional resources and there appeared to be no solution forthcoming. Henderson returned to Geneva to consult the newly elected Director-General, Dr Halfdan Mahler. Later that week the WHO Executive Board was to meet. On the agenda was the question of how to use US$900 000 allocated to China, a new Member State of WHO, which had declined to accept WHO funds provisionally allotted for the support of its health programmes. The Director-General agreed immediately that a cable could be sent to India indicating that these funds would be used for its smallpox eradication programme, a decision later endorsed by the Executive Board. Another emergency in an apparently never-ending series of financial crises in the programme had been averted.
Table 15.18: India: searches for outbreaks of smallpox in low-incidence states and union territories, 1973
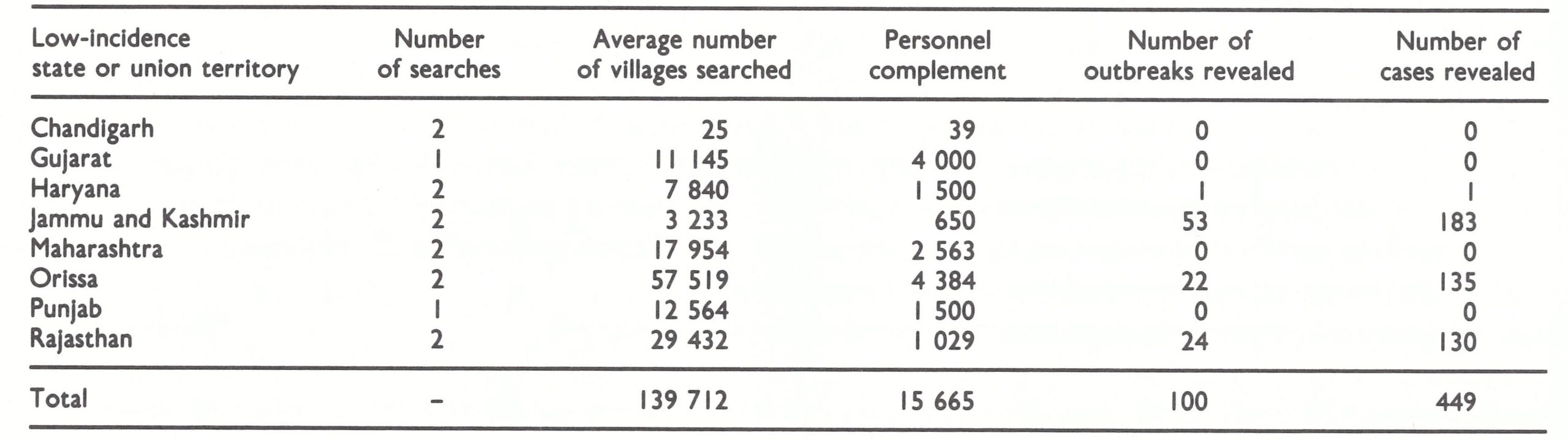
Table 15.19: India: searches for outbreaks of smallpox in smallpox-free states or union territories, 1973
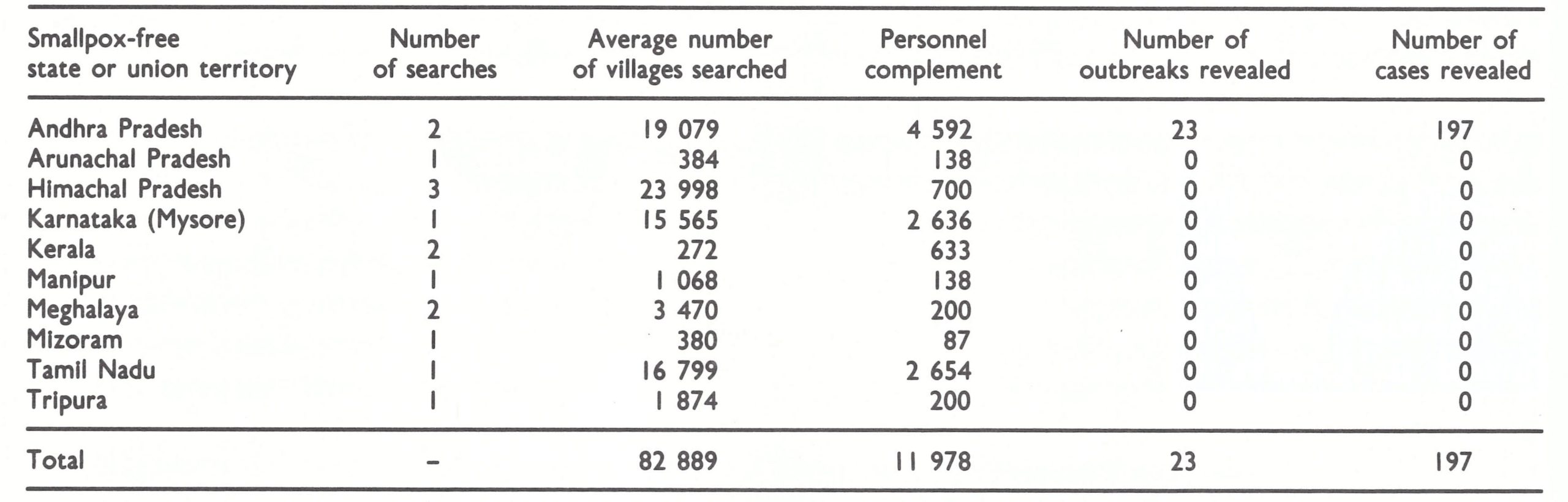
Table 15.20: India: number of reported cases of smallpox, by state and union territory and by month, 1973
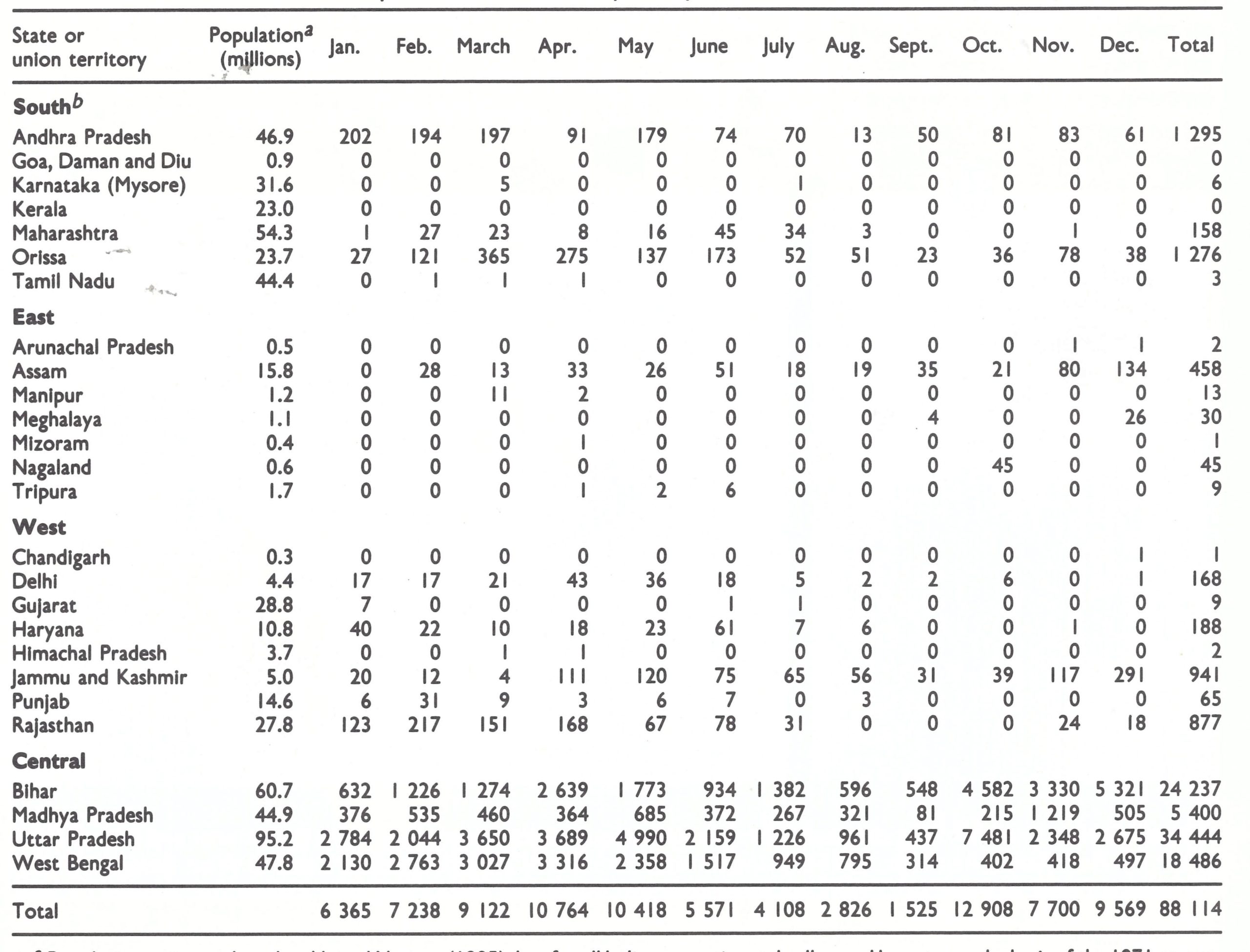
a Population estimates based on United Nations (1985) data for all India proportionately allocated by state on the basis of the 1971 census.
bNo cases were reported during this period in the union territories of Andaman and Nicobar Islands, Dadra and Nagar Havell, Lakshadweep, and Pondicherry.
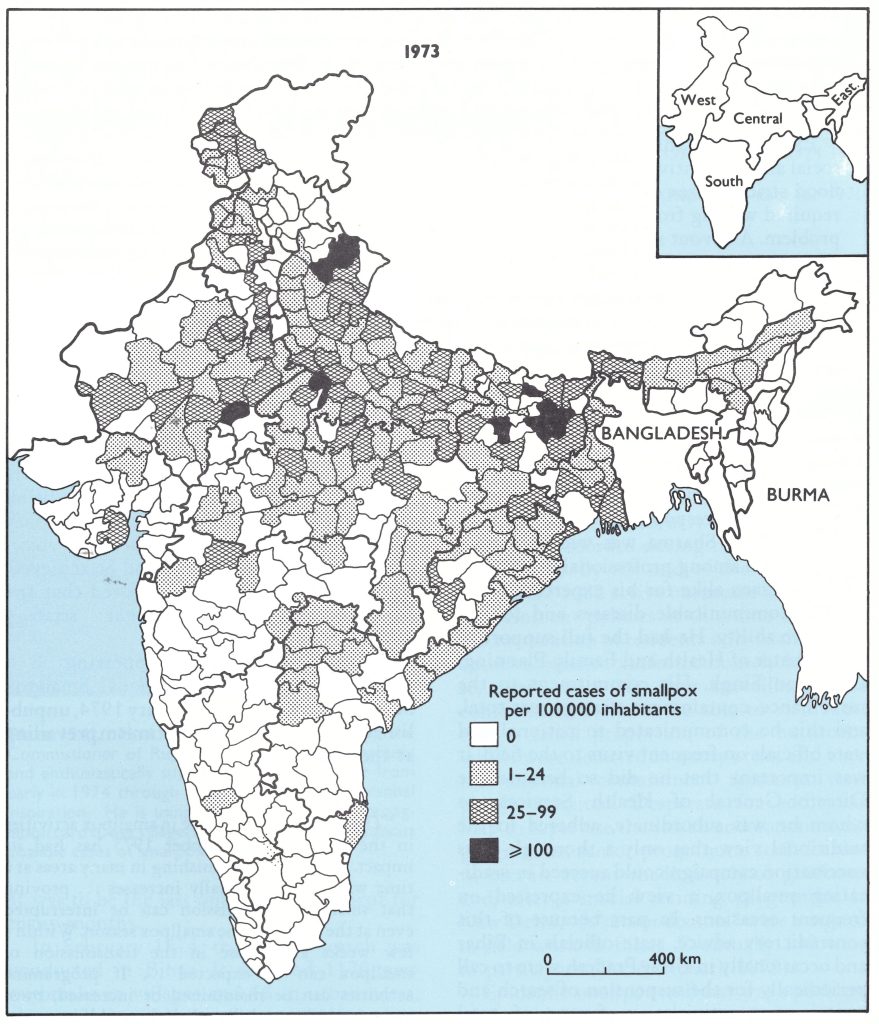
Fig. 15.16. India: number of reported cases of smallpox per 100 000 inhabitants. by district. 1973.
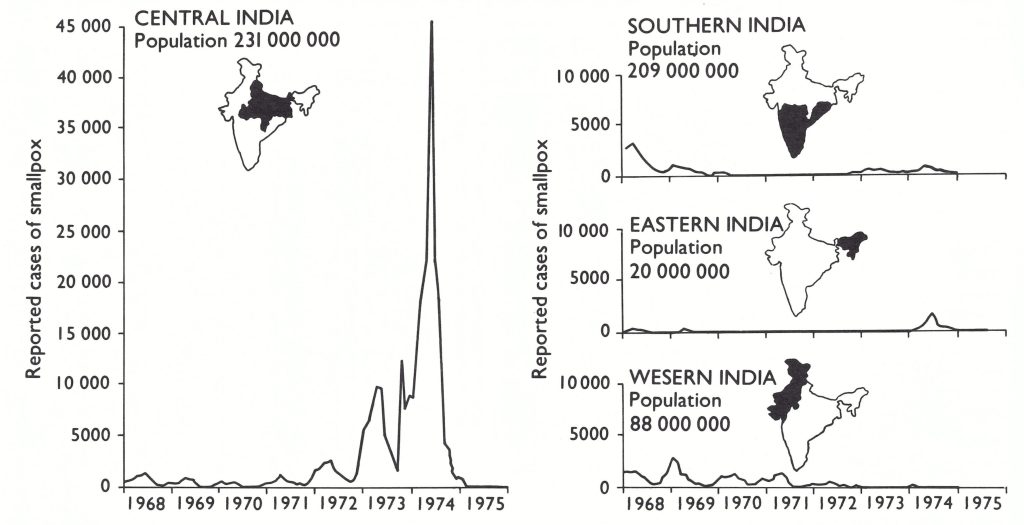
Fig. 15.17. India: number of reported cases of smallpox, by region, 1968-1975. (Population data for 1971 from Basu et al .,1979.)
The Dedication of the Smallpox Programme Staff
The commitment and determination of staff who worked in the programme were extraordinary and indeed might well be the subject of a separate book. The meeting in New Delhi on 1 January 1974 of the Indian and WHO Central Appraisal Team and Henderson provides an illustration. All members of the team had been working a 7-dayweek for nearly 4 months, travelling to some of the country's most remote and inhospitable areas in a frantic effort to motivate the army of health workers to contain the vastly larger number of outbreaks than anyone had foreseen. All had lost weight and were exhausted, one person had incapacitating renal colic, a second a painful facial herpes zoster infection, a third a serious fungus infection of the foot (which eventually required surgery) and a fourth atypical pneumonia with high fever and pleuritic pain. The only question asked at the meeting was how to find additional resources to sustain the momentum. When Henderson expressed scepticism of their own ability to work, let alone to continue the schedule proposed even if given the needed resources, the reply was simple: "We've considered the question and have decided that things can't get worse; therefore they must get better".
Exemplifying this determination in the field was a 50-year-old Indian professor of social and preventive medicine, Dr T. P. Jain, who was assigned as an epidemiologist in a flood-stricken area of Assam. Investigation and containment of many of the outbreaks required wading from house to house in areas in which leeches were legion and snakes a problem. A devout member of the Jain religion, he had requested a week's leave to attend ceremonies in another state commemorating the 2500th birthday of Mahavira, founder of the religion, a long-anticipated and sacred event. Another epidemiologist, arriving in the area to check the existing outbreaks in Jain's absence, found him waist-deep in water trudging from house to house, unwilling to leave for even a day so long as smallpox persisted in his area.
Plate 15.10. Implementing the search programme required extensive fieldwork by national and international staff. A: Ram Rakha Arora (b.1925), an Indian member of the Central Appraisal Team in West Bengal. B : Left: Lawrence Brent Brilliant (b.1944), an epidemiologist from the WHO Regional Office for South-East Asia; right: Anatolij N. Slepushkin (b.1929), an epidemiologist from the Smallpox Eradication unit at WHO Headquarters.
The Darkest Months of the Programme, January-June 1974
In January 1974 optimism prevailed. Funds were available to continue the programme, case notification was far more complete than ever before, and the search programmes were showing steady improvement in all states. In Bihar, in which the greatest numbers of cases were being recorded and the health services were the least adequate, the programme office reported that 50% more villages had been visited during the third search, in December 1973, than during the first in October. Despite a more extensive search and despite seasonally higher transmission rates, fewer villages with new outbreaks had been found.
The results in Uttar Pradesh had been even better, with the number of newly found outbreaks declining from 1525 in October to 331 in December. Progress in West Bengal was no less encouraging. There, Arita had introduced a new system to document progress in the programme. From October 1973, each newly discovered outbreak was added to a master list as an “active outbreak” and not removed from the list until 4 weeks had elapsed since the last case. At the end of December, there were only 124 active outbreaks in the whole of that populous state. In Madhya Pradesh, the last of the 4 key central states, a search conducted during 7-12 January 1974 revealed only 49 new outbreaks, two-thirds of which consisted of 3 cases or less. Of 5000 outbreaks discovered in these 4 states between October and December, it was estimated that not more than 1700 were still active. In the other states, the number of reported cases—many of them resulting from importations—remained low. Meanwhile, Bangladesh reported that only 172 of its villages were infected; in Nepal, virtually all outbreaks were said to have resulted from importations.
The commitment of the government to the programme was demonstrated early in 1974, when Dr Sharma was promoted to the position of Commissioner of Rural Health while retaining responsibility for smallpox eradication. Dr Sharma was widely known and respected among professional health staff and politicians alike for his expertise in the field of communicable diseases and for his executive ability. He had the full support of the Minister of Health and Family Planning, Dr Karan Singh. His commitment to the surveillance-containment strategy was total, and this he communicated to national and state officials on frequent visits to the field. It was important that he did so because the Director-General of Health Services, to whom he was subordinate, adhered to the traditional view that only a thorough mass vaccination campaign could succeed in eradicating smallpox, a view he expressed on frequent occasions. In part because of this contradictory advice, state officials in Bihar and occasionally in Uttar Pradesh were to call periodically for the suspension of search and containment activities in favour of total mobilization for a mass campaign to vacci SMALLPOX AND ITS ERADICATION nate everyone in the state. The mass vaccination approach was more easily understood and although it had been demonstrably unsuccessful in the past, there was the belief that if the health personnel were really properly organized and motivated the objective of 100% vaccination could be achieved . Dr Sharma’s appointment ensured that the basic surveillance-containment strategy would be sustained.
A summary statement appearing in a WHO South-East Asia Regional Smallpox Surveillance Report (4 February 1974, unpublished) is indicative of the optimism prevailing at the beginning of 1974:
“The tremendous increase in smallpox activities in the region since October 1973 has had its impact. Smallpox is diminishing in many areas at a time when it traditionally increases . . . proving that smallpox transmission can be interrupted even at the height of the smallpox season. Within a few weeks a decrease in the transmission of smallpox can be expected . . . If programme activities can be maintained or increased, most areas in India and Bangladesh could interrupt transmission before the monsoons.”
Plate 15.11. Mudi Inder Dev Sharma (b. 1919), the Commissioner of Rural Health for India, vigorously and enthusiastically supported the programme from early in 1974 through extensive travel and personal inspiration. He is using the WHO smallpox recognition card to ask villagers in Uttar Pradesh State about possible cases of smallpox.
It was to be the last optimistic statement for many months. In February 1974, the fourth search was conducted in Bihar. It revealed 1170 new outbreaks in villages and 18 in urban areas, almost 3 times the number (405) found in December, and more than twice as many cases as in January 10 697 as against 4816 (Table 15.21). The most seriously affected areas were the eastern districts. From here, smallpox began to spread to West Bengal (65 importations by mid-February) and to Nepal (11 importations).
Additional Indian and WHO epidemiologists were hurriedly recruited and assigned to Bihar. The fifth search (11-16 March) revealed 2374 new outbreaks, double the number found in February: more than 7000 Q cases were recorded during the search period (Fig. 15.18). By the end of the fifth search, there were 3682 active outbreaks in the state. 0 Containment policies at this time called for the vaccination of residents only in the 20-30 o houses adjacent to infected households. Even so, there were too few surveillance and containment teams to be able to visit more than a small proportion of the outbreaks, which were detected in many areas, and even the minimal containment measures were poorly executed. Desperate for additional help to supervise the search and containment programme, senior programme staff decided to recruit recent medical school graduates and, after a special training programme in New Delhi, 40 “junior doctors” were assigned to field work in Bihar. Eventually 140 were to participate (Jha & Achari, 1975).
Epidemic smallpox in Bihar was a problem of formidable proportions, and the occurrence of one natural or man-made calamity after another further hampered the eradication effort. Indian Airlines workers went on an extended strike, making it difficult to ship vaccine and for senior personnel to travel. The railways began to be extensively used until railway workers likewise went on strike. Meanwhile, the international oil crisis had developed and, in April, petrol costs in India doubled and shortages occurred. Drought in southern Bihar, sufficiently severe to require international assistance, resulted in the migration of large populations of refugees seeking food and spreading smallpox. This was soon followed by the most severe floods in a decade in northern Bihar and even more refugees fleeing in search of food and refuge. Civil disorder and political disturbances began to occur throughout Bihar and, over large areas, government authorities were totally occupied with maintaining law and order. Throughout this period, heroic efforts were made to ensure an adequate flow of supplies and to stockpile materials such as vaccine and reporting forms in anticipation of expected shortages; however, most supplies were barely adequate to meet the current needs.
That the programme in Bihar functioned at all was remarkable and for this due credit must go to its Smallpox Programme Director, Dr A. G. Achari, a conscientious and tireless worker who, with the officers of the Central Appraisal Team, Dr Foege and Dr Dutta, sought valiantly to mobilize a lethargic health staff and to sustain morale among the Indian and WHO epidemiologists, who were overwhelmed by the explosive spread of smallpox.
When it seemed that little else could possibly go wrong, the health workers in Bihar threatened to go on strike. Dr Achari, Dr Dutta and Dr Foege sought desperately to develop a contingency plan but with little support. The observation of one district health officer was characteristic of the attitude of some supervisory health staff: “If we don’t have a strike, we don’t need a contingency plan; if we do have a strike, it is no longer my responsibility.
Table 15.21: India : number of reported cases of smallpox, by state and union territory and by month, 1974
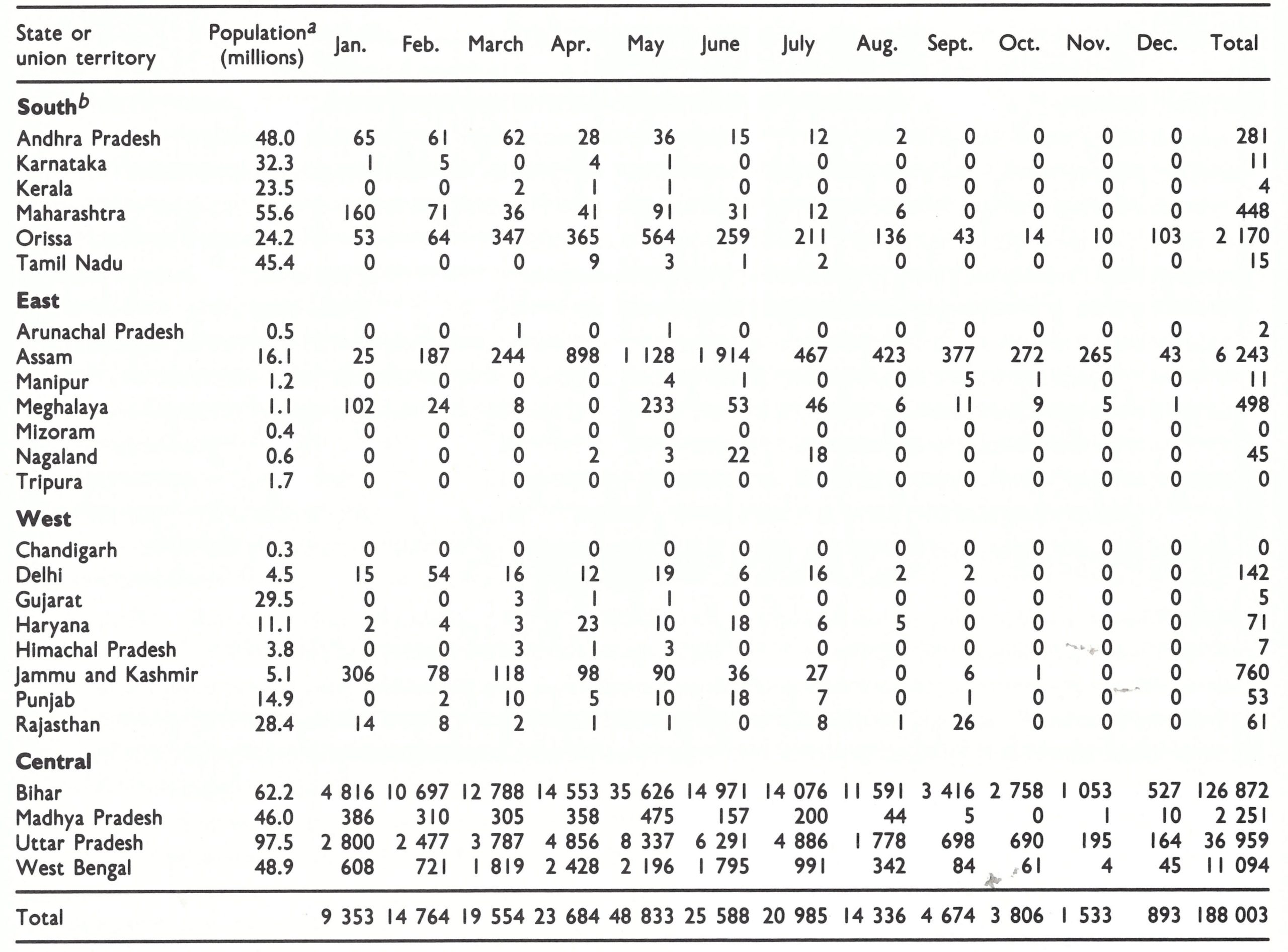
a Population estimates by states are based on United Nations (1985) data for all of India proportionately allocated by state on the basis of the 1971 census.
b No cases were reported during this period in the union territories of Andaman and Nlcobar Islands, Dadra and Nagar Havell, Goa, Daman and Diu, Lakshadweep, and Pondicherry.
Plate 15.12. Karan Singh, Minister of Health and Family Planning of India from 1973 to 1977, provided strong political support for the programme and for the surveillance-containment strategy.
The sixth search in Bihar (29 April-4 May) recorded 2658 additional outbreaks—the number of active outbreaks increasing to 4921. More than 7% of all villages and municipal areas in the state were infected, the most heavily afflicted being in the north-east (Fig. 15.19), where, in 3 districts, 25% of all villages were infected.
India’s Director-General of Health Services, still an advocate of mass vaccination, became increasingly alarmed and advised Bihar’s Minister of Health to withdraw staff from the infected areas and to begin mass vaccination campaigns in the areas still free of smallpox to prevent them from becoming infected. Dr Sharma, learning of this only after the minister in Bihar had begun to take action, protested direct to India’s Minister of Health and Family Planning, Dr Karan Singh, and together they flew to Bihar to intercede. The Bihar minister rescinded his order. In an epidemic as extensive as that occurring in Bihar, some of the Indian and WHO programme epidemiologists began to speculate that Bihar might represent a special case in which the now well-tested surveillance and containment strategy might not be applicable.
Throughout May and into early June, the epidemic continued to intensify. With daytime temperatures normally exceeding 40°C, field work became ever more difficult, morale began to deteriorate and, again, the question of a return to state-wide mass vaccination arose. The minister was more resolved than before and, in the June meeting of state and district programme officers, strongly advocated this approach. Senior programme staff argued in vain, until an Indian physician, working in one of the districts, pointed out in a deferential manner that he had grown up in a village and there, when a house was on fire, they put water on that house and not on all houses in the village. The minister reluctantly agreed to defer a mass vaccination campaign for one more month but only on the understanding that if no apparent progress had been made by then, mass vaccination would be initiated. Senior staff hoped that, even if containment were less than optimum, the seasonal decrease in transmission would partially stem the epidemic and so preserve what they believed to be the only possible effective strategysurveillance and containment.
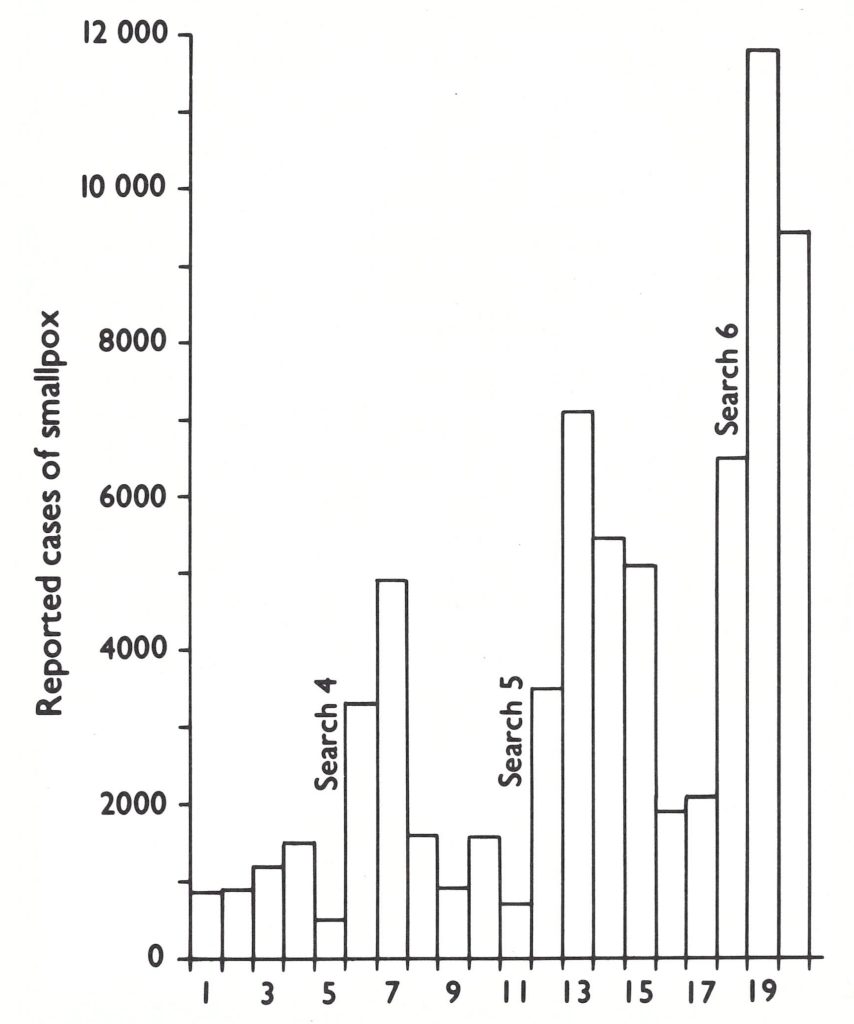
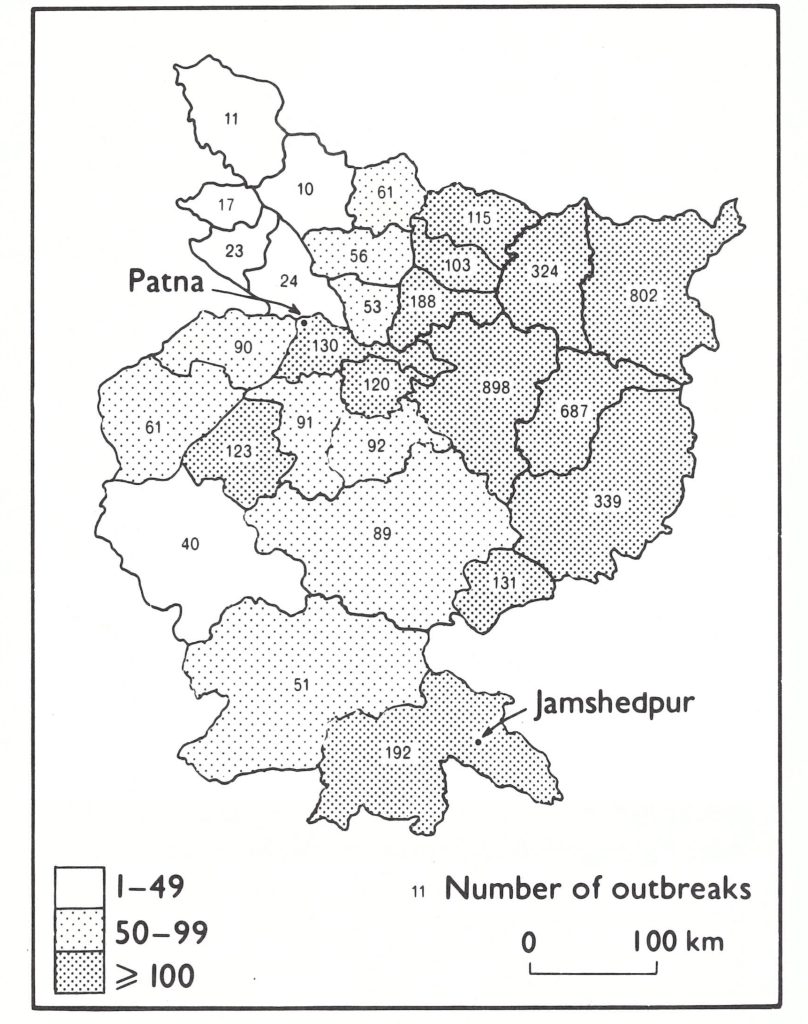
Fig. 15.18. Bihar State: number of reported cases of smallpox, by week, showing results of special searches, January -May 1974.
Fig. 15.19. Bihar State: number of active outbreaks of smallpox, by district, as of 5 May 1974.
In the other states of India, the situation was better than in Bihar but not so good as had been expected in February. Uttar Pradesh was the next most heavily infected state. The numbers of reported cases and outbreaks had risen steadily since January, although less precipitously than in Bihar. A peak of 1905 active outbreaks was reached in May, with 8337 cases reported that month. Outbreaks were reported from 442 (51%) of the state’s 875 primary health centres and in 47 of its 55 districts (Srivastava & Agarwala, 1975). However, 82~of the outbreaks occurred in only 15 districts, primarily in eastern Uttar Pradesh, where their large number precluded the taking of effective containment measures. Elsewhere in the state, with the support of the Director of Medical and Health Services and Family Planning, Dr G. P. Srivastava, the health staff had begun to function well.
In West Bengal, the number of active outbreaks increased steadily, from 124 in December to 556 following the seventh search in mid-April. However, more than 75°,0 of the outbreaks took place in only 5 of the state’s 16 districts, and here village volunteers began to be recruited and trained for containment operations, an effective practice later adopted in other states. The increase in the number of outbreaks in West Bengal was largely accounted for by importations, mostly from Bihar. Between January and May, programme staff documented 386 imported outbreaks, and others occurred as a result of spread from these importations.
Importations, principally from Bihar, Uttar Pradesh and West Bengal, accounted for an increase in the number of cases in Madhya Pradesh, Maharashtra and Orissa. Each state worked diligently and effectively to discover and contain the outbreaks as rapidly as possible, but by May, both the smallpox eradication staff and the general health service personnel were reaching a critical point of fatigue and frustration. Meanwhile, the eastern states, hitherto all but free of smallpox, experienced a sharp increase in the number of cases, resulting from importations from Bangladesh, Bihar and Uttar Pradesh. This was cause for additional alarm because, in the eastern states, health services were generally less extensive and not much better organized than those in Bihar. Although they were not populous states, road and rail services were poor and both search and containment activities were difficult to organize and to execute.
The unexpected and explosive epidemic of smallpox in Bihar and its spread to other states had required the mobilization of far more Indian and WHO epidemiologists (see Table 15.16) than had been foreseen and had necessitated the emergency purchase of more vehicles and supplies of all types than had been planned. By April, funds to support the smallpox programme were again at a low level. Requests were made to numerous governments for additional finances; few showed any interest and no country indicated it was in a position to act quickly in answering an appeal. Privately, many expressed scepticism about the programme’s prospects of success. The reaction was not surprising in view of the fact that the number of cases of smallpox recorded in India in the spring of 1974 was the largest for nearly two decades. WHO’s frequent appeals in the past for funds to bolster its malaria eradication campaign, and the continuing setbacks in that programme despite infusions of ever larger sums of money, were well remembered. Once again, the programme approached a critical point, but, unexpectedly, substantial help materialized from a new source, the Swedish International Development Authority (SIDA). In a casual conversation with the Personnel Officer of the WHO Regional Office for South East Asia—an official of Swedish nationality—Dr Grasset learned that SIDA planned to examine alternative uses for Swedish funds which had become available because of the cancellation of another project in India. Discussions promptly followed with Mr J. Tranaeus, at the Swedish Embassy in New Delhi. Convinced, as few others were, that an effective and well-directed campaign was in progress whatever the smallpox incidence might suggest, he persuaded the Planning Commission of the government of India, as well as his superiors in Stockholm, of the merits of the programme. Within a few weeks, a memorandum of agreement had been signed on behalf of the governments of India and Sweden which made available to WHO US$2.8 million in support of the smallpox programme. With Mr Tranaeus’s continuing enthusiastic interest, SIDA was eventually to provide US$10 million to the programme. The government of India also increased its own central allocation of funds. For 1974, a sum of US$13 million was made available for field operations.
Time was required to effect the necessary transfer of funds, but the Division of Budget and Finance in WHO Headquarters readily agreed to permit funds to be obligated even though they were not yet in hand. Meanwhile, the administrative staff in the WHO regional office were experiencing difficulties, because of the substantial expansion in the number of personnel in the programme receiving a stipend from WHO, the larger numbers of imprest accounts to be handled and the need to procure a greater volume of supplies (Table 15.22). It was essential that additional personnel should be recruited and that budget and finance operations should be established for the programme. The Center for Disease Control (formerly the Communicable Disease Center) in Atlanta, which was already providing many field epidemiologists, responded to this need by sending its most capable senior administrative staff to help to bring some order into an increasingly chaotic administrative situation. Beginning with the Center’s Deputy Director, Mr William Watson, an exceptionally imaginative group of administrators worked tirelessly with the group of no less talented WHO administrative staff to provide essential services in support of the field staff.
Plate 15.13. Jarl E . Tranaeus (b.1923), Head of the Development Co-operation Office of the Swedish Embassy in New Delhi from 1973 to 1978, persuaded Swedish authorities and the Indian government’s Planning Commission of the need for substantial additional assistance to the smallpox eradication programme at a crucial moment.
Table 15.22: India: principal supplies and items of equipment provided by WHO, 1970-1976a

a Between 1972 and 1976, it is estimated that WHO, in addition, arranged to print and distribute the following material : approximately 31 million forms for use in reporting and in search and containment operations ; 500 000 booklets for use in outbreaks and in market searches ; 400 000 posters; I million smallpox recognition cards ; and 500 000 other guides and miscellaneous publications .
Although the smallpox epidemic was featured more often and with greater prominence in Indian newspapers, little was known of the problem outside the country. However, in May 1974, the epidemic became international news. On 18 May 1974, India tested its first atomic device in an underground explosion in Rajasthan. At that time, the smallpox epidemic was at its height, more than 11 000 cases being reported in a single week. International news reporters who had flown to India to cover the atomic test arrived just as the smallpox epidemic hit the headlines in the local press; international media coverage of both events was extensive. Programme staff repeatedly explained that more complete reporting accounted in major part for what appeared to be the largest epidemic for many years, but scepticism was prevalent and understandable.
Although the problem in Bihar was serious, the eradication programme throughout India was steadily improving and gaining momentum. Week-long village-by-village searches were being performed each month throughout the high-incidence states and less frequently in the others (Table 15.23). The number of those engaged in the searches was increasing (Table 15.24).
As serious and frustrating as the situation appeared, yet another disaster aggravated it—the Jamshedpur epidemic in Bihar State. Its discovery resulted from investigations in Madhya Pradesh. Special efforts had been made to interrupt transmission in Madhya Pradesh. It was one of the 4 central states considered to be of highest priority, and was geographically the largest state in India, with a population of 46 million. Most of the outbreaks which had been discovered during the autumn searches were in the northern and eastern districts of the state, bordering on Bihar and Uttar Pradesh. The December 1973 search had revealed only 215 cases and 53 new outbreaks. By the beginning of March 1974, and after 5 monthly searches of its 10 million households, smallpox appeared to be present in only a single, geographically limited focus, in a tribal area and one of the least developed parts of the state.
In late March 1974, however, reports of smallpox outbreaks began to arrive from many areas of Madhya Pradesh which had been considered to be smallpox-free. Investigations revealed these to be the result of recent importations from the neighbouring state of Bihar. The source of infection of many was traced to an industrial complex in southern Bihar: Jamshedpur in Singhbhum District. Adivassis (tribal people) often travelled 300-800 kilometres to Jamshedpur from their homes in Madhya Pradesh in search of seasonal employment. If they became ill with fever, they returned to their native villages, where many subsequently developed rash and spread smallpox to others.
Dr Brilliant was dispatched to Jamshedpur in late April to assess the situation. He found a major problem of unexpected magnitude.
Table 15.23: India : frequency of active searches for outbreaks of smallpox, 1973-1975
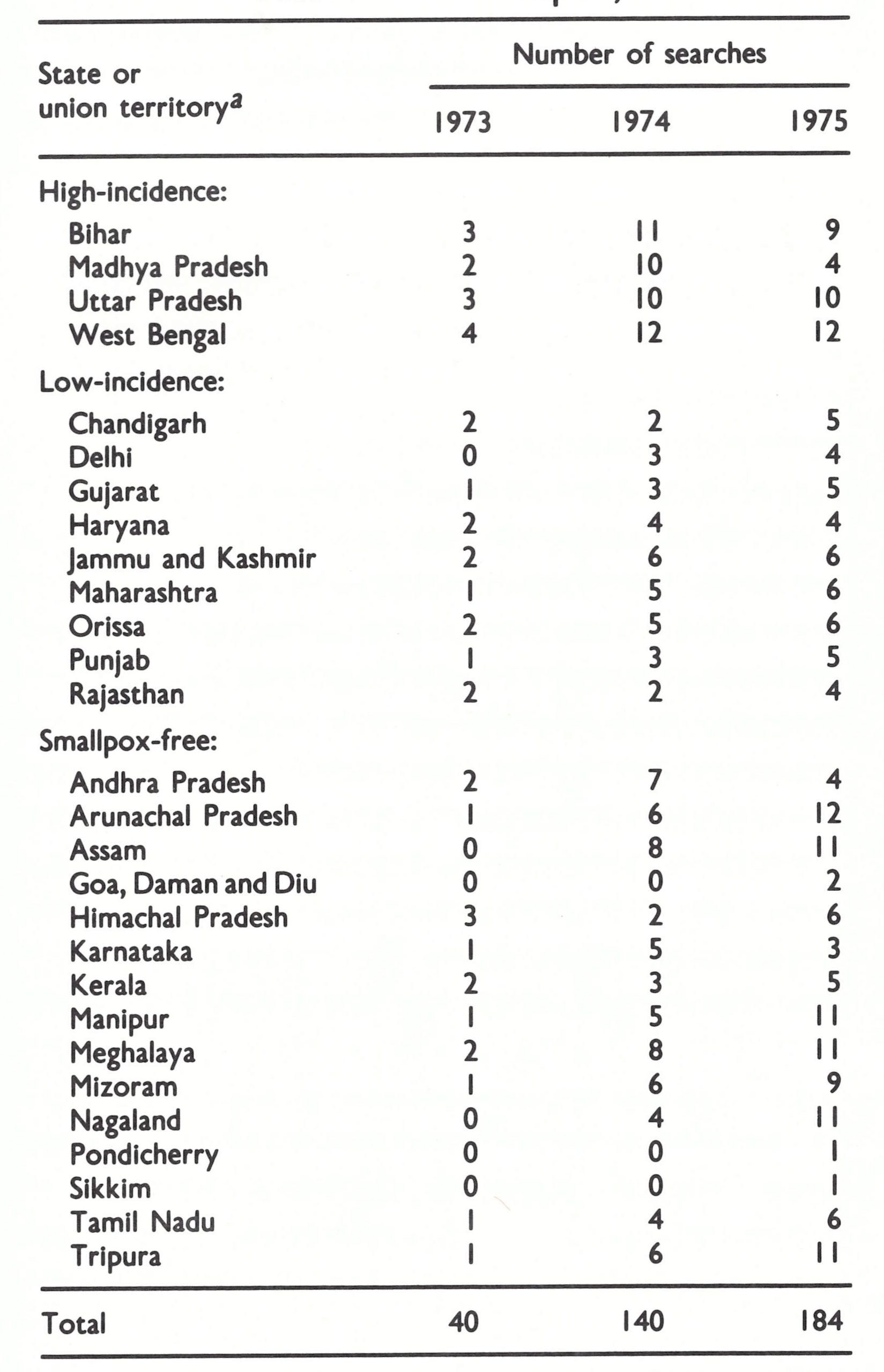
a Relative incidence as defined in 1973.
Table 15.24: India: approximate number of workers, per search, 1973-1976
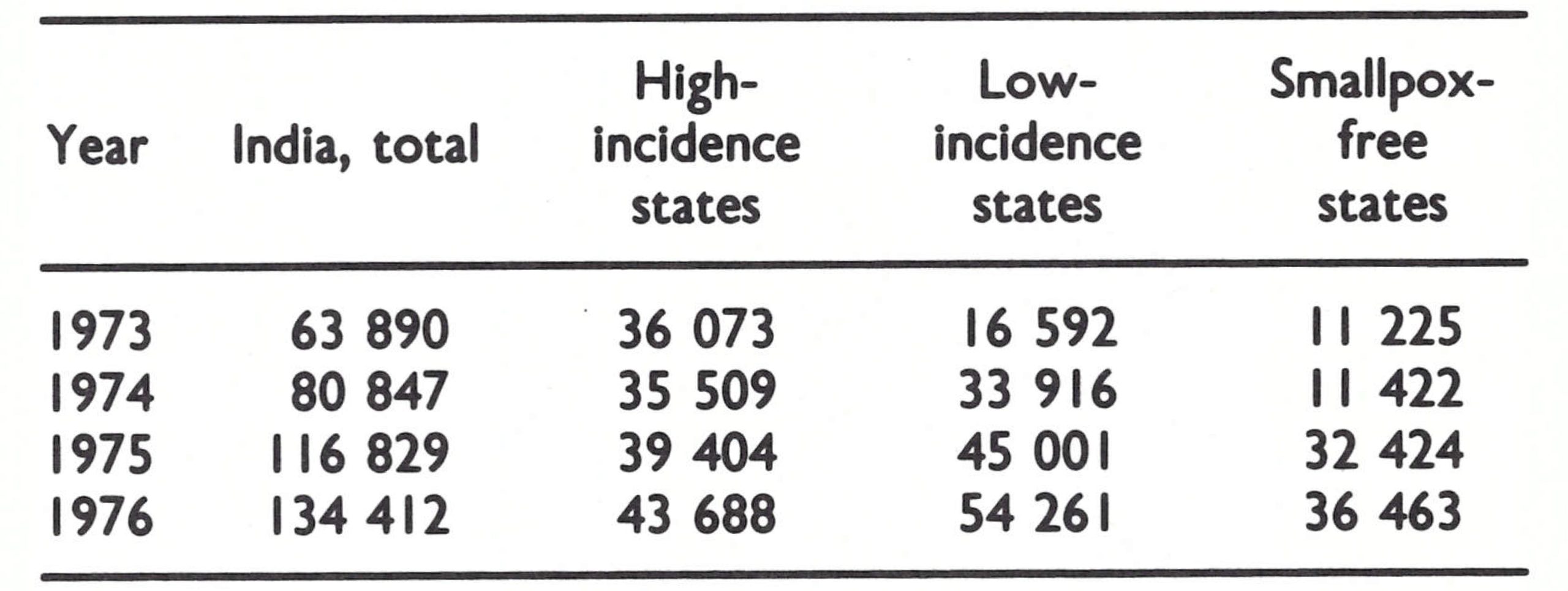
The epidemic in Jamshedpur, Singhbhum District, Bihar
The Jamshedpur industrial complex is one of India’s most important steel-producing areas, its prosperity contrasting sharply with economically depressed neighbouring areas of southern Bihar, eastern Madhya Pradesh and northern Orissa. As such, it attracted numerous seasonal workers, beggars and transients.
The special investigation began in early May. The District Medical Officer of Singhbhum disclosed that during the preceding 6 weeks, he had received 125 notifications of outbreaks in other districts of Bihar and in other states which were suspected of having originated in his district, and that 12-15 notifications were then being received daily. Little action had been taken, the government health structure in this district being poor. In addition to 27 primary health centres that reported to him, all of which were then known to have smallpox cases, there were 15 autonomous and separately administered health units in Jamshedpur (population, 800 000). The health units included small company towns, corporations, large colonies of railway employees and others. No one was charged with the task of reporting cases among the large migrant population, and the railways denied all responsibility for the reporting of cases from the areas they administered. Half the health units were found still to be using rotary lancets.
At the industrial complex, a group of heavy industries of the Tata group, officials professed ignorance of the problem but immediately agreed to provide help in a search of the city and of 1760 villages within a 45-kilometre radius. In a search that took place in mid-May, 50 physicians, 200 paramedical supervisors and 900 searchers discovered 1479 cases in the city and 726 cases in the 456 villages found to be infected (Basu et al ., 1979). An intensive programme of containment and case detection was immediately undertaken. This involved, in addition to government and WHO health staff, personnel and transport provided by 7 of the Tata industries as well as voluntary organizations, including the Rotary Club, the Lions Club, the Bihar Flying Club, the local blood bank and the All-India Women’s Council (Bharucha, 1975). All bridges and major roads were barricaded and no one was permitted to pass unless vaccinated. A special programme dealt with railway travellers, especially third-class passengers, of whom perhaps one-third travelled without tickets. Trains were diverted to special platforms, which permitted all passengers to be checked when boarding or leaving a train. Checkpoints were established at bus stations, and employers ensured that workers and their families were vaccinated. Meanwhile, the containment of all known outbreaks began, an effort which in fact necessitated house-tohouse vaccination of the entire urban complex and most of the surrounding villages.
Two months were required to bring the epidemic under control. Meanwhile, 300 outbreaks and at least 2000 cases occurred in 11 states of India and in Nepal as a result of travel from Jamshedpur (Fig. 15.20). The area most affected was Bilaspur District (Madhya Pradesh), with 484 cases in 72 villages.
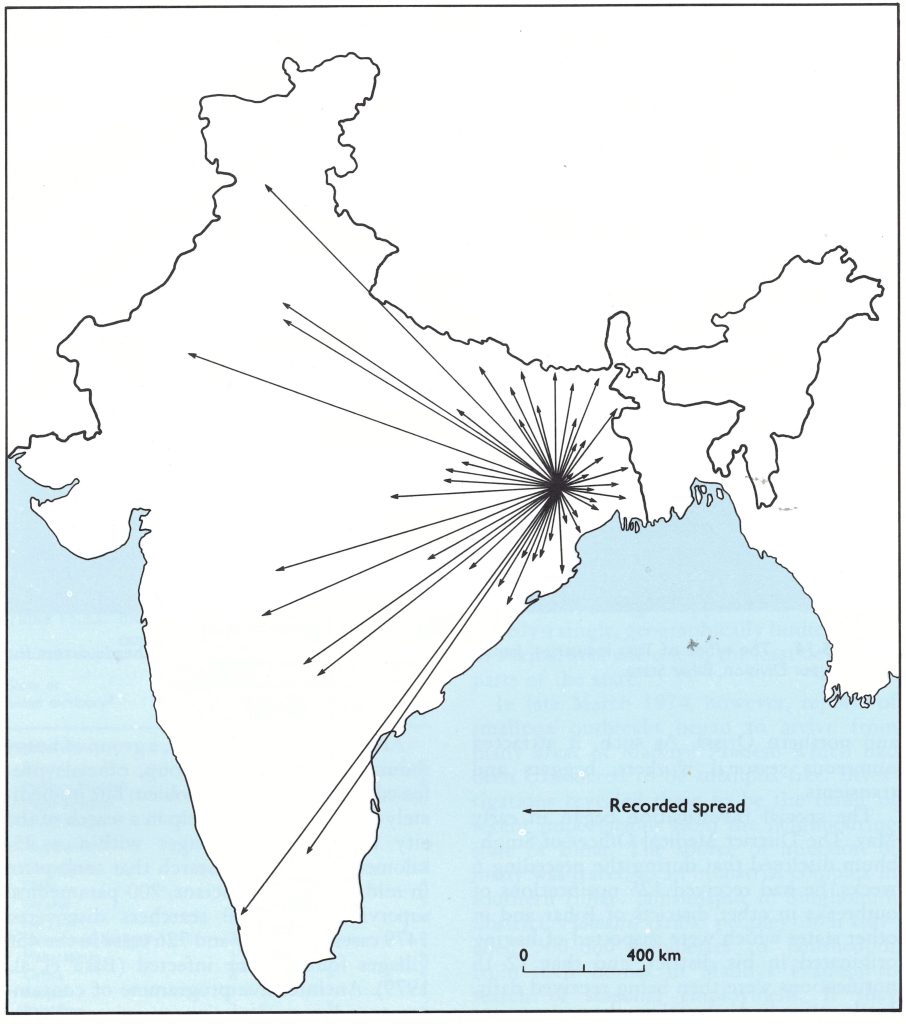
Fig. 15.20. Spread of smallpox from the Jamshedpur urban industrial complex to the rest of India, 1974.
A Redoubled Effort, June-December 1974
Early June 1974 was the psychological low point of the Indian smallpox eradication programme, if not of the global Intensified Programme itself. A 9-month intensive campaign had been conducted throughout India with senior staff and numerous field staff working 7 days a week. Despite the large expenditure of money and effort to date, and despite what appeared to be an increasingly successful effort in surveillance and containment activities, there were 8664 known outbreaks. Moreover, up to the end of May, India had already recorded 116 188 cases, a number greater than that reported for the entire world during any of the preceding 6 years of the Intensified Programme. Cases were reported in May from nearly one-third of the districts in India, of which 80 reported 50 cases or more (Fig. 15.21). Many areas of India remained free of smallpox or had only a few outbreaks resulting from importations (Fig. 15.22), but the epidemic wave then surging through Bihar seemed to be moving both east and south. It was clear that the efforts made so far in Bihar had been inadequate to contain smallpox, and the states which appeared to be the next candidates for epidemic smallpox-Orissa to the south and the states to the east-had health services which were not much better in quality than those in Bihar.
During June, with the beginning of the monsoon period, smallpox transmission normally declined in India and the number of outbreaks diminished. However, with the disease so widely seeded throughout Bihar and adjacent areas, it was clear that unless a concerted effort were made to contain the outbreaks during the summer, smallpox would remain widely disseminated at the commencement of the next season and the experience of the spring of 1974 would be repeated. Activities of all types usually diminish in India during the summer months-the hottest, the most humid and the most difficult months of the year in which to work. A staff which had toiled to the point of exhaustion between September and May would have to mount one more effort.
On 17 June 1974, the Central Appraisal Team met the Secretary of Health and the Director-General of Health Services to discuss an emergency programme for the whole of India, but especially for Bihar. It was decided to increase the number of special epidemiologists from the 50 who were in the field at the time to more than 100. WHO would initially provide 12 additional international epidemiologists, and 6 non-medical surveillance officers ; the government of India would attempt to recruit 40 epidemiologists. If that proved impossible, WHO would try to obtain the services of more international epidemiologists.
Six central-level surveillance teams would be established which would respond to emergency smallpox problems as they developed. State surveillance teams, hitherto restricted in travel to the state in which they were assigned, would be directed to cross state borders whenever necessary to seek the source of infection of outbreaks.
Three hundred additional containment teams would be recruited, each to be headed by recent Indian medical graduates. A further 375 Jeeps would be purchased or hired. To fund these activities, SIDA offered additional financial assistance, which was rapidly made available.
It was recognized that special efforts would be required in Bihar. Following consultations between the staff of the WHO regional office, the Governor and the State Health Minister, the Chief Secretary of the State of Bihar sent a special letter to all district magistrates, informing them that as from the end of June they and the block development officers would assume responsibility for the conduct and organization of the campaign in their districts. Dr Achari would continue in his role as State Smallpox Eradication Programme officer but more effective senior administrative staff would replace the health service staff in bearing primary responsibility for the programme.
The president of Tata Industries was approached for help in dealing with smallpox in the 6 southern districts of Bihar comprising Chotanagpur Division. He agreed to assist and the company’s Board of Directors approved the expenditure of 7.2 million rupees (US$900 000) and the assignment of personnel and vehicles. An unusual semi-autonomous public and private sector programme was created in this division, involving personnel and equipment from WHO, Tata Industries, the government of India, the state of Bihar, and OXFAM, a private voluntary organization. The consortium participating in the Chotanagpur Division programme was to function capably and with remarkable cooperation over the following 12 months.
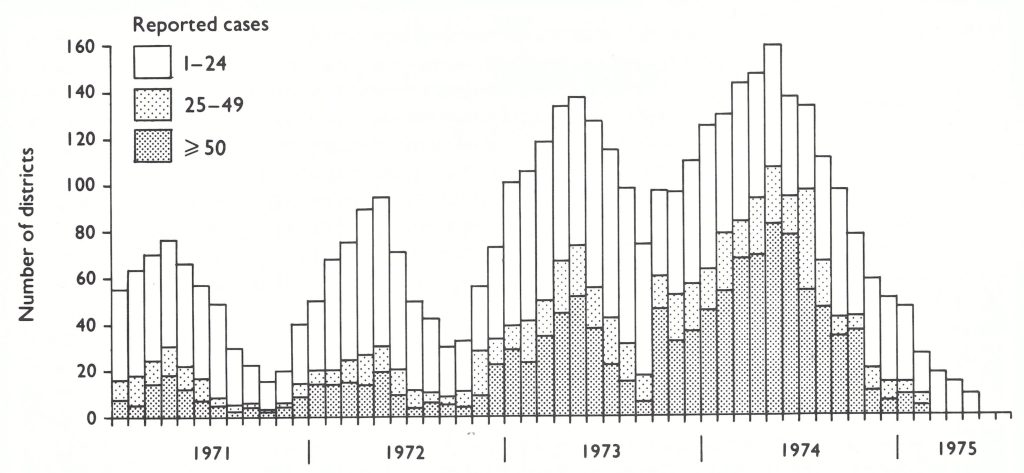
Fig. 15.21. India: number of districts reporting cases of smallpox, by month, 1971-1975 .
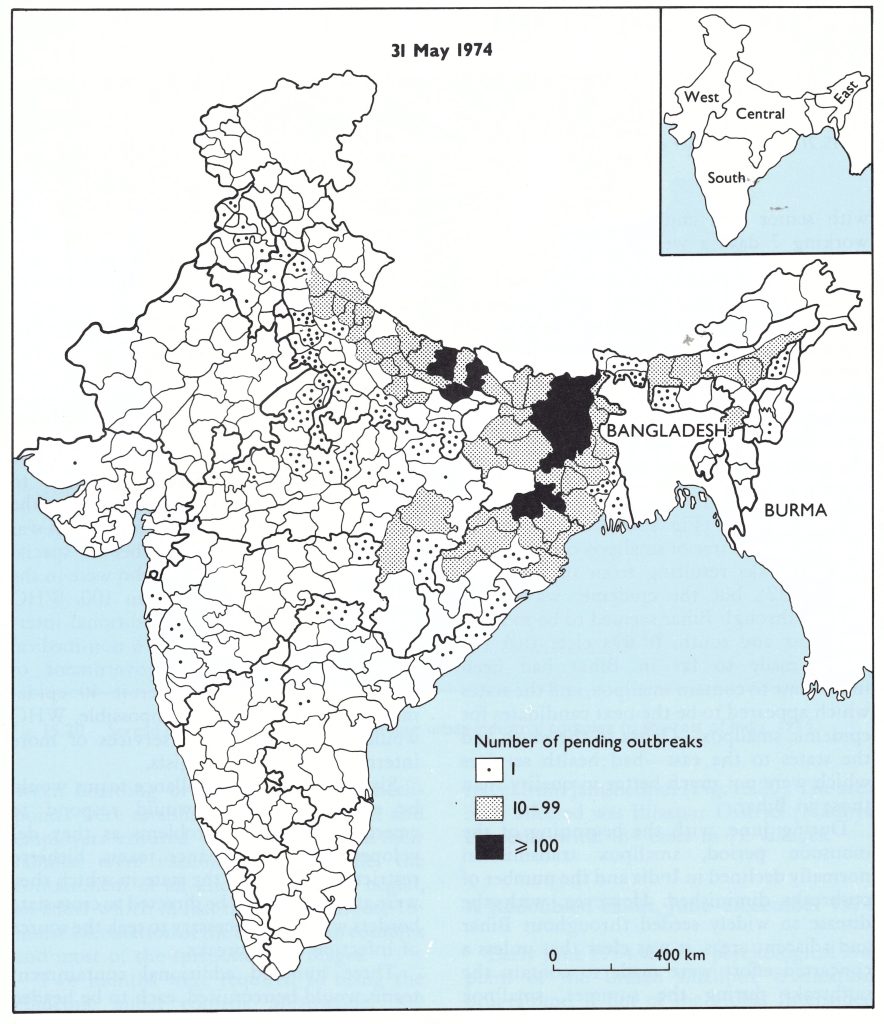
Fig. 15.22. India: number of pending outbreaks of smallpox, by district, as of 31 May 1974.
Deficiencies in the containment of outbreaks had proved to be a serious weakness of the programme in most states, particularly Bihar and Assam. Where smallpox outbreaks were few, state surveillance teams had usually assisted local staff in their investigation and in the vaccination of village residents. Where smallpox was widely prevalent, procedures called for the detection of all cases in the area and the vaccination of those in the 20-30 nearest households. The names of any absent household members were supposed to be recorded and the village visited on a later occasion to ensure that all were vaccinated. This directive was rarely followed, however. In many areas of the world, and indeed in many parts of India, simple containment measures had sufficed to stop transmission. In the more densely populated parts of India, however, they proved ineffective. Many persons left their homes during the day to go to the fields, to market or elsewhere ; some who objected to or feared vaccination simply hid themselves and their children when the teams were in the villages ; many visited relatives and friends, including those with smallpox, in other villages. The result was that even after intensive containment vaccination, numerous susceptible persons remained and smallpox transmission persisted.
It was therefore decided to systematize the containment activity in a manner that could be readily understood and widely applied and that was subject to verification by a supervisor. “Containment books” were designed, printed and distributed in August 1974. One book was used for each outbreak. The name of each person in each of 500 houses surrounding an infected household in a rural area (1000 houses in an urban area) was to be listed in the book and repeat visits made to the village until all persons had been vaccinated and the fact duly registered in the book (Sharma & Grasset, 1975). In a separate section of the book, information regarding each case was recorded.
Three specific standards were also established at this time as indices of the effectiveness of, respectively, surveillance, containment, and outbreak investigation activities. The provision of standards by which a programme in any area could be measured was thought to be helpful in improving the quality of supervision. An indication of the degree of effectiveness of surveillance was the lapse of time between the onset of the first case and the detection of the outbreak. The detection of at least 75% of outbreaks within 14 days of the onset of the first case was felt to be attainable. If adequate containment were performed, all susceptible contacts would be vaccinated and none should develop smallpox once vaccinial immunity had developed say, after 7-12 days. Assuming that it would take several days to identify and vaccinate susceptible persons, it seemed reasonable to establish a second goal namely, that no cases should develop more than 17 days after an outbreak was detected. The quality of the investigation of an outbreak was more difficult to measure, but such quantification was considered important because experience had shown that the least well performed part of an investigation was usually the identification of the source of infection. The concept that each individual with smallpox must have been in face-to-face contact with another individual with smallpox just 7-17 days before onset was a surprisingly difficult concept for many to grasp. On investigation forms, many simply listed “sporadic” as the source of infection. To identify the source, however, was vital because often other, as yet undiscovered, outbreaks were unearthed in this manner. Thus, the third goal called for the identification of the source of the outbreak in 90% of outbreaks, a level of success which had been achieved by competent epidemiologists in other areas.
The measurement of progress based on the number of the then existing infected villages and urban mohallas (sections of a city) had been initiated in October 1973 in West Bengal and had been introduced in some other states as well, particularly those with a low incidence of smallpox. In June 1974, uniform definitions for this method of measurement were developed and it was formally adopted throughout India. Any village or mohalla in which a case had occurred within the preceding 4 weeks (subsequently extended to 6 weeks) was considered to be the site of a “pending outbreak”. This concept recognized the potential for the spread of smallpox from the patient to susceptible contacts throughout the period concerned and the need to check the outbreak repeatedly to ensure that transmission did not continue. A list was kept in each primary health centre and each district (later, each state) showing the name of the infected village or mohalla, the date of onset of each case, the date of discovery, the date on which containment began, the source of infection, and the dates on which supervisory personnel had visited it. The outbreak was not removed from the list until the site was visited and searched again, not less than 4 weeks (later, 6 weeks) after the onset of the last case.
As at the end of June 1974, there were 6401 pending outbreaks in 17 states and Delhi Municipal Corporation (Table 15.25).
Table 15.25: India: pending outbreaks of smallpox at the end of each month, 1974-1975
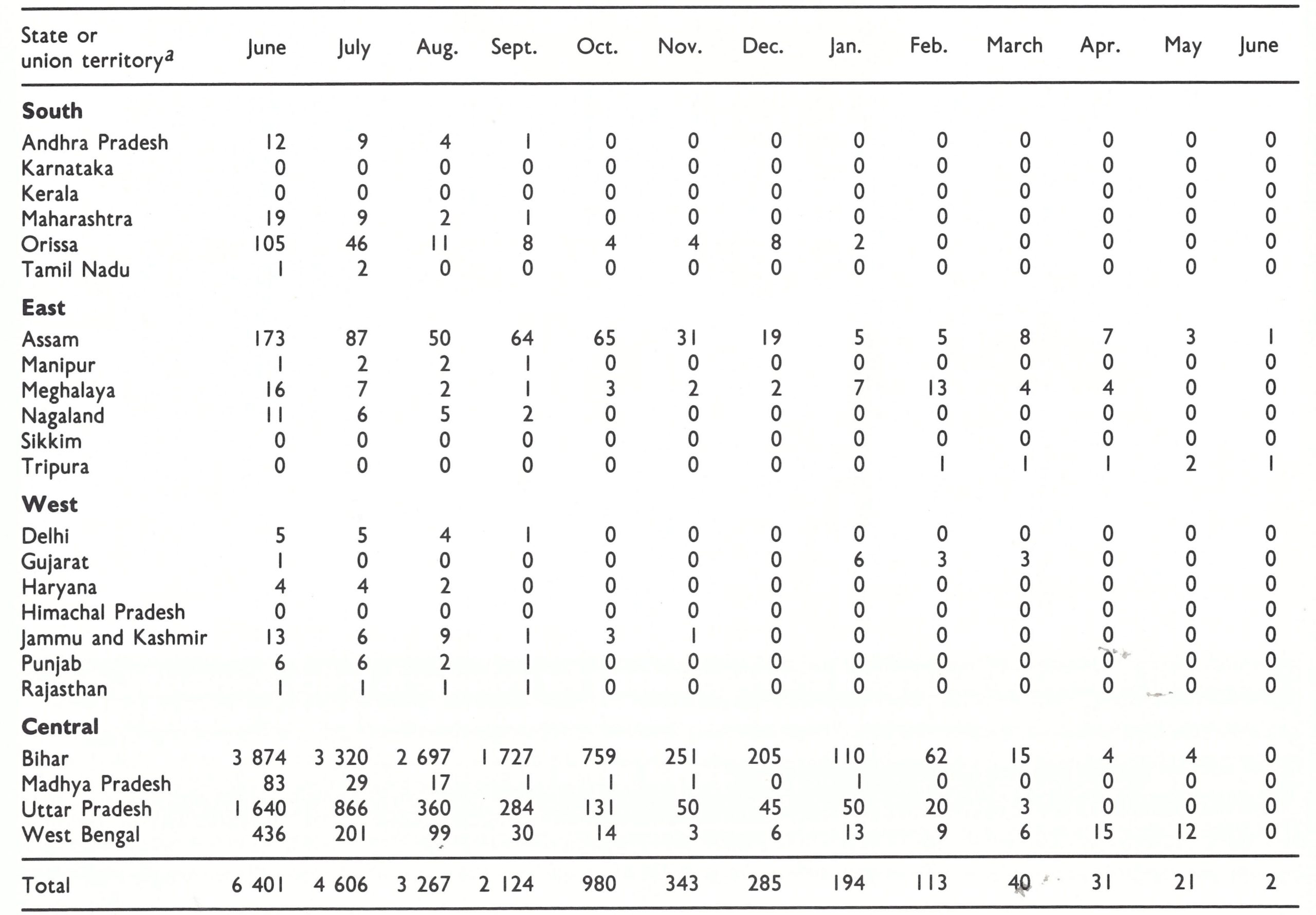
a No outbreaks were recorded in the union territories of Andaman and Nicobar Islands, Arunachal Pradesh, Chandigarh, Dadra and Nagar Haveli, Goa, Daman and Diu, Lakshadweep, Mizoram and Pondicherry.
With additional resources and an increased complement of supervisory personnel, statewide search and containment programmes continued throughout the summer. Most of the resources were assigned to Assam, Bihar, Uttar Pradesh and West Bengal, in which searches were conducted monthly. In Bihar alone, 35 national and international epidemiologists and more than 100 state epidemiologists and paramedical personnel assisted state, district and local health personnel (Jha & Achari, 1975) ; in Uttar Pradesh, there were 27 national and international epidemiologists and 19 state surveillance teams (Srivastava & Agarwala, 1975). Most other states conducted one search during this period, although some conducted two. The number of pending outbreaks began to decline sharply, and with fewer outbreaks surveillance teams were able to provide increasingly better supervision of search and containment activities. The quality of both procedures rapidly improved. In addition, the teams devoted more time to visiting markets and schools to inquire about rumours of possible cases. The number of pending outbreaks decreased to 4606 at the end of July and to 3267 at the end of August. The first hopeful note since February was sounded on 26 August in a WHO South-East Asia Smallpox Regional Surveillance Report: “The opportunities for interrupting smallpox transmission in India, Nepal and Bangladesh are better than at any time since the programme started.”
By the end of September, there were only 2124 pending outbreaks, of which 1727 (81 %) were in Bihar (Table 15 .25 ; Fig. 15 .23). The north-eastern districts of Purnea and Katihar in Bihar had more than 600 pending outbreaks, but in only 8 other districts were there more than 50. Almost none were to be found in all of southern and western India. In September, 4674 cases were reported, one-tenth the number recorded in May.
The staff were optimistic but still concerned. The analysis of data from previous years indicated that some increase in transmission occurred at the beginning of October, coinciding with an increase in the numbers of persons travelling from place to place to attend festivals and marriages. Thus, there was a heightened concern about the spread of smallpox over greater distances. Moreover, active outbreaks persisted in 50 municipalities which were recognized to be important sites of dissemination to rural areas. Finally, in Assam, the number of pending outbreaks had actually increased from a low of 50 in August to 64 in September;, in this state, field operations were greatly hampered by floods, a poor transportation network and a less than adequate health service. Its neighbour, Bangladesh, appeared to pose no threat, since there were only 163 infected villages in the country at the end of September, a competent programme was in place and the numbers of reported cases and outbreaks were declining as rapidly as in India. In Nepal, to the north, only 4 outbreaks were detected in September 1974.
Additional measures were implemented in October to strengthen surveillance and containment. In all urban areas with active outbreaks, a house-to-house search was conducted every 2 weeks. Additional personnel were assigned to work in Assam. Perhaps of greatest importance was the decision to offer throughout India a reward for the notification of a previously unreported outbreak of smallpox in which a case had occurred within the preceding 6 weeks. This, it was hoped, would permit earlier detection of cases and discourage the suppression of reports which, despite all efforts, remained a problem in some areas. In addition, smallpox cases were sometimes hidden by villagers who held religious objections to vaccination or feared that patients might be removed to hospital. The offer of a reward had originally been proposed in 1972 in areas with a low incidence of smallpox, but many health officials had been reluctant to adopt the practice, fearing that it would create a precedent with regard to the reporting of cases of other diseases. However, as has previously been described, 5 of the southern states began offering rewards of 10-25 rupees, following the extensive suppression of reports which resulted in the Gulbarga (Mysore) outbreak in 1972. Early in 1974, some other states that had a low incidence or were thought to be smallpox-free also began to offer a reward, which was now increased to 50 rupees. The inducement had not been particularly effective, however, because information about the reward was not widely disseminated by the health workers, who wanted to claim the money for themselves. To overcome this problem, it was decided to offer 50 rupees to the person first reporting a previously undiscovered outbreak and 50 rupees to the health worker who received the report.
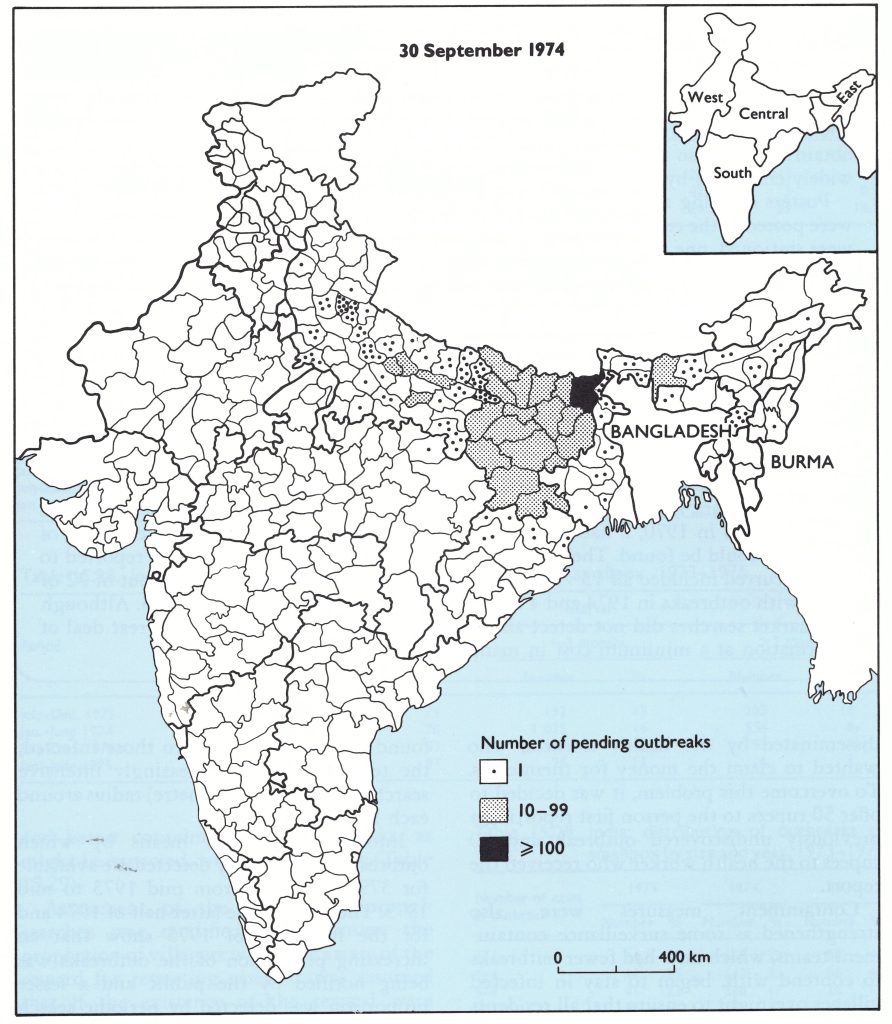
Fig. 15.23. India: number of pending outbreaks of smallpox, by district, as of 30 September 1974.
Containment measures were also strengthened as some surveillance-containment teams, which now had fewer outbreaks to contend with, began to stay in infected villages overnight to ensure that all residents were vaccinated. One or two local inhabitants, termed “watchguards”, were hired to stay at each infected house to prevent the patient from leaving and to vaccinate anyone who could not be dissuaded from visiting. Eventually, 4 watchguards were engaged to guard each house with a patient, 2 of them working during the day and 2 at night. This meant that if one watchguard had to absent himself, one would remain on duty. When it was found, in some areas, that visitors avoided the watchguard by entering through a back door, the back entrance was barricaded. Observing that new outbreaks were often found in villages adjacent to those infected, the teams began an increasingly intensive search in a 5-mile (8-kilometre) radius around each infected village.
Information on the means by which outbreaks were actually detected are available for 3798 outbreaks from mid 1973 to mid 1975. The data for the latter half of 1974 and for the first half of 1975 show that an increasing proportion of the outbreaks was being notified by the public and a lesser proportion was detected by periodic search (Table 15.26). In the non-endemic states, notification by the public played a more important role, the proportion of outbreaks so notified increasing from 15 % in the first 6 months of 1974 to 29% in the second 6 months and to 36% in 1975.
The outbreaks were detected increasingly earlier after the onset of the first case (Table 15.27), although the standard which called for 75% to be detected within 14 days was never reached . The outbreaks persisted for a shorter time (Table 15 .28) but in some of them cases continued to be found more than a month after detection . With earlier detection and better containment, the outbreaks, as might be expected, were less extensive (Table 15.29).
Assessment of the ever-more-thorough searches was modified to determine the proportion of villagers who were aware of the reward for reporting cases. It was assumed that if the existence of the reward were generally known, cases would not be hidden for long. Personnel searching for cases were instructed to convey the fact of its existence to all the villagers. Radio, posters, leaflets, rickshaws with loudspeakers and announcements at weekly local markets were also used as a means of information.
During the autumn, the number of pending outbreaks fell steadily, from 2124 at the end of September to 980 at the end of October and to 343 at the end of November (Fig. 15.24), but then the rate of decline slowed considerably. Almost as many new outbreaks were being added to the list as were being removed. The winter season of more rapid transmission had begun . The numbers of outbreaks and cases were at a record low, but, if smallpox transmission was to be interrupted, even more rigorous methods of case detection and containment would be required.
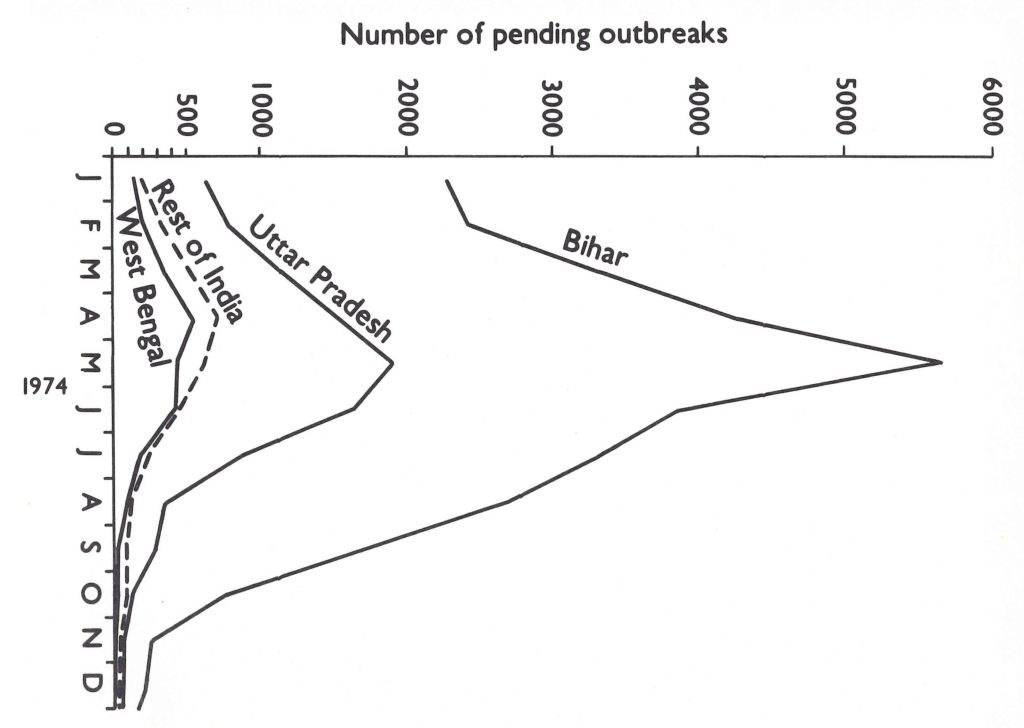
Fig. 15.23. India: number of pending outbreaks of smallpox, by district, as of 30 September 1974.
Market Searches
Surveys in the traditional weekly markets, held throughout India, were especially useful in detecting cases of smallpox. It was found that 2 searchers could readily question 300-500 market visitors in the course of a working day (Basu & Khodakevich, 1978b) and obtain information about cases in villages 10-20 kilometres distant. It was a technique widely employed by surveillance teams.
Posters showing a smallpox patient and announcing the reward for reporting a case were posted at the entrance to the market and in tea-shops. At each entry point 2 workers were stationed, one of whom asked those entering the market if they knew of cases and which village they were from ; the second worker recorded the information. Later, the searchers moved to the tea-shops to continue the questioning. The investigation of all reported or rumoured outbreaks was undertaken the following day.
taken the following day. To assess how effective the market search technique had been, a special study was conducted in a mountainous area of Assam (Khodakevich & Rao, 1978) in January 1976. In a district comprising 695 villages scattered over an area of roughly 15 by 55 kilometres, 7 markets were searched to determine whether outbreaks occurring over the preceding 3 years could be detected. The searchers were health workers who had not been associated with the programme and had no information about previous smallpox in the area. Visitors to the market reported 64 villages as having been infected with smallpox during the preceding 3 years. Investigation revealed that 18 of the villages were in another district, 2 had outbreaks in 1970, 2 had outbreaks of chickenpox, and in 8 others no evidence of outbreaks could be found. The remaining 34 villages in which smallpox was reported to have occurred included all 13 villages which had had outbreaks in 1975, 17 out of 32 of those with outbreaks in 1974 and 4 out of 13 of those with outbreaks in 1973. Although the market searches did not detect all outbreaks, they served to provide a great deal of information at a minimum cost in manpower.
Table 15.26: India: methods of detecting outbreaks of smallpox, 1973-1975
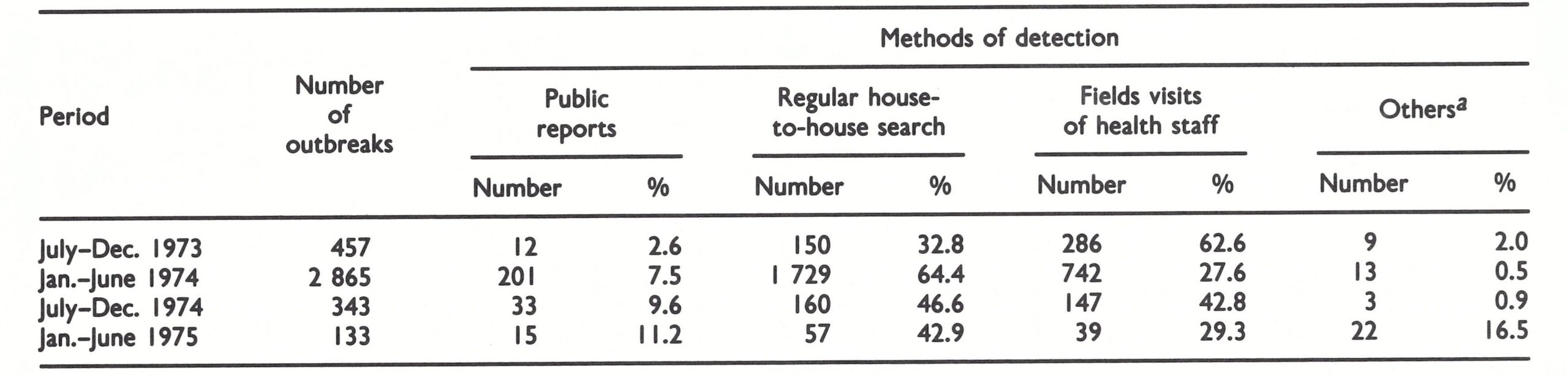
a Market searches, special searches, cross-notification.
Table 15.27: India: interval between onset of outbreaks of smallpox and their detection, 1973-1975
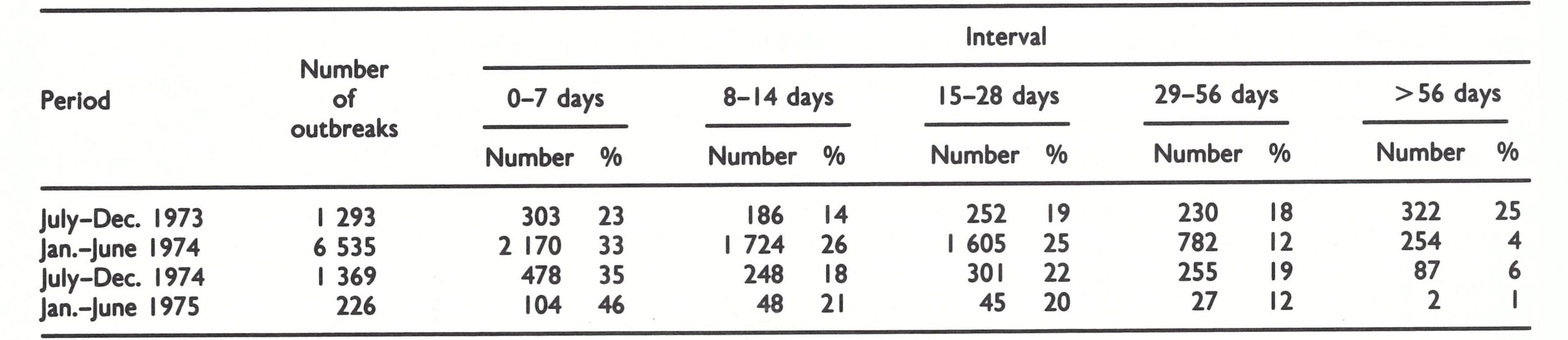
Table 15.28: India: interval between onset of first and last case of smallpox, 1973-1975
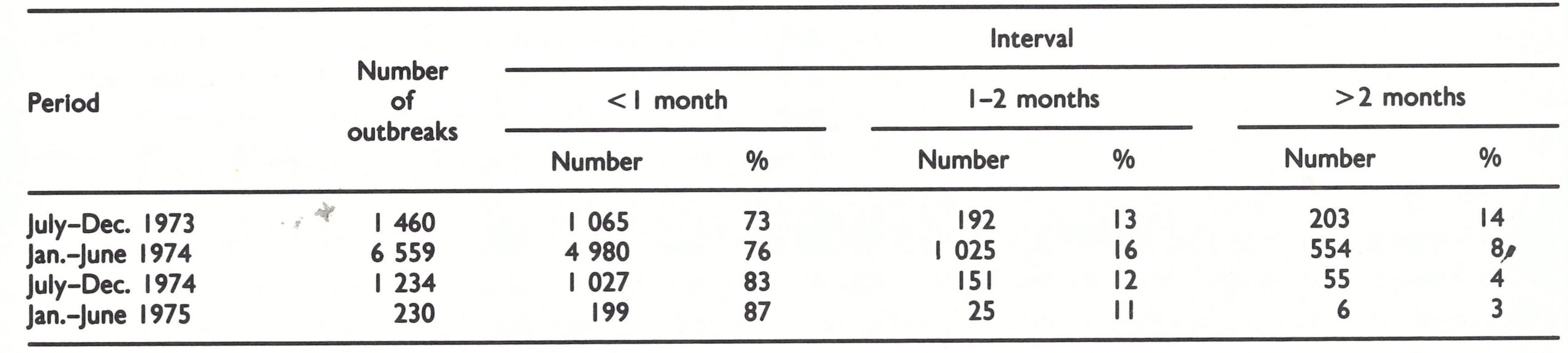
Table 15.29: India: distribution of outbreaks of smallpox by size and year, 1973-1975
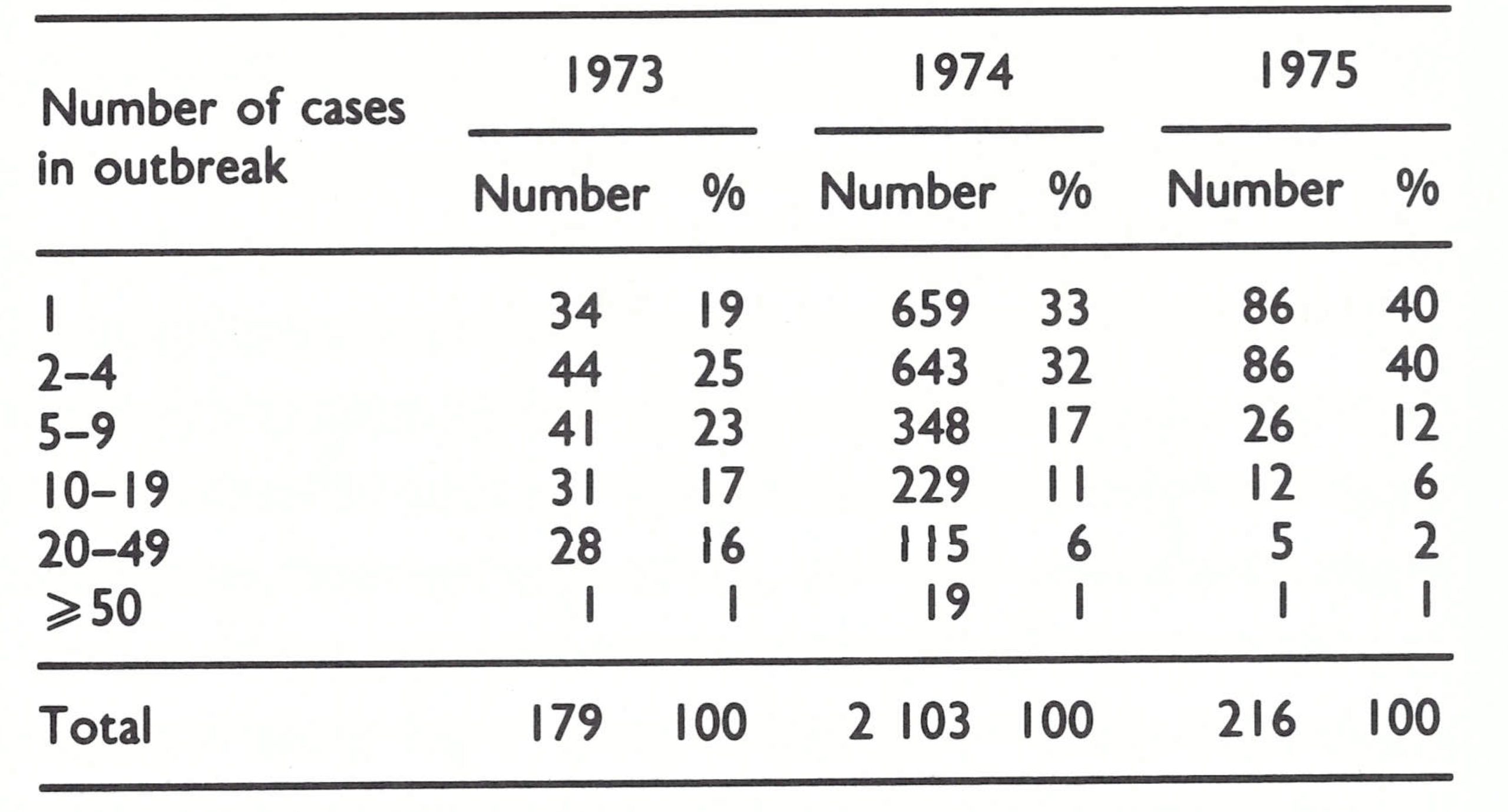
Concern about the programme’s progress suddenly turned to alarm in mid-December 1974 as major epidemics unexpectedly began in Bangladesh. Catastrophic floods, the worst in 20 years, had swept the northern districts of Bangladesh in August and September and, with the subsequent famine, tens of thousands of refugees migrated to other parts of the country. In December, smallpox began spreading rapidly and once again infected the major cities. The most heavily affected areas were along the northern Bangladeshi-Indian frontier and because of frequent travel across the border, numerous importations were to be anticipated. Of particular concern were the eastern states of India, in which the health services and the smallpox eradication programme itself were the least able to cope.
Realization that a difficult spring might lie ahead was soon followed by the ominous discovery of a cluster of outbreaks at a major pilgrimage site of the Jain religion about 85 kilometres from Patna, the capital of Bihar (Jha & Achari, 1975). The largest outbreak was detected in December 1974 at Puri village, in which the founder of the Jains had died 2500 years earlier. Forty households were infected at the height of the pilgrimage season. Complicating the problem was resistance to vaccination, common among Jains. A special appeal was made to the principal religious leader, who agreed, reluctantly, to recommend vaccination. The entire village was quarantined by the Bihar military police. Twenty-four-hour watchguards were posted at the houses of infected persons and at key areas in the village. A community kitchen was set up to feed patients so they would not have to leave their homes for food. Pilgrims were not allowed to enter sacred pilgrimage areas until they had been vaccinated. Although smallpox spread to 5 adjacent villages, the outbreak in Puri was finally controlled by the end of February 1975.
Elsewhere in the district, the number of outbreaks had increased from 16 to 75. Assessment revealed poorly conducted search operations and inadequate containment. Emergency measures were introduced. Whenever an outbreak was discovered, 20-25 vaccinators were dispatched to the infected village; containment vaccination was completed within 48 hours; 24-hour watchguards were posted at every infected household; and food was brought in to ensure household quarantine. Entire villages were cordoned off when necessary. Instead of a few vaccinators, dozens were assigned to each newly discovered infected village and camped there until no active case remained. In all, 102 new outbreaks were discovered in Bihar in January 1975.
Status of the Programme in Early December 1974
Memorandum, dated 9 December 1974, from the Chief of the WHO Smallpox Eradication unit to all smallpox eradication staff:
"The autumn saga of 1974 has been marked by weeks of unexpectedly rapid decreases in the number of pending outbreaks in Asia interspersed with weeks when there has been little or no decline. At present, we seem to be again in the latter phase. Does this signal the beginning of a phase where seasonally increased rates of transmission overbalance our capability to contain the outbreaks or does it represent but a pause in the countdown as we regroup to redeploy forces and to tighten up containment procedures and so recommence the countdown? Unquestionably, a greater effort is required during the winter months to ensure containment of each outbreak, but the task can be accomplished.
"With search activities now reasonably well developed in most districts and with market searches and the system of rewards serving to assure discovery of outbreaks missed in search, it seems to me that now is the time to deal far more rigorously with containment measures. In many areas . . . staff have not dealt with containment as rigorously as is now required. This is not surprising. During the summer and early autumn months, further spread of smallpox occurred only infrequently even when containment measures were less than optimal. Inevitably, emphasis shifted to improving the search procedures, sometimes perhaps at the expense of the arduous and meticulous work required to assure 100% containment. With increased rates of transmission and more population movement, containment procedures which were effective in October are no longer so.
"At this stage, and with the comparatively few outbreaks we have, every patient must be subjected to 24-hour guard and, as required, food provided to the families to provide further incentive for them to stay put. If the guard is fully effective, every subsequent contact will be protected by vaccination. But frequent supervision by epidemiologists and senior staff is mandatory if the system is to work. Then begins the now necessary but arduous task of tracing all contacts of the patient from the time of onset of rash . This procedure is in effect in some areas but, as of the time of my visit two weeks ago, it was not in effect everywhere.
"Most important now is for each epidemiologist to consider each new outbreak as being indicative of a possible failure in the system. The question for each outbreak must be asked—'Why did this outbreak occur and what should be done to prevent a repetition of the episode?"'
“Operation-Smallpox Zero”, January 1975
With smallpox present in only 285 of the more than 575 000 villages of India at the end of December 1974 and with reasonable confidence that there were few undetected outbreaks, it appeared that the elimination of smallpox was at hand However, from the experience of the past year in Bihar, it was clear that smallpox could spread rapidly in this densely populated area during the winter and early spring. Analysis of the experience in the autumn of 1974 showed that deficiencies in containment were primarily responsible for the failure to stop outbreaks. Vaccination of the population of affected villages was not as rapid as it might have been, visitors to the villages were often not vaccinated and some villages were declared free of smallpox without a thorough follow-up search. Although searches were conducted within a 5-mile (8-kilometre) radius of infected villages, some outbreaks traced to those villages were found to occur at distances of up to 16 kilometres.
At the end of December, new instructions were issued by the government entitled “Operation—Smallpox Zero”. The following passages are extracts from the instructions:
“With the outbreaks so few in number, each outbreak must now be dealt with as an absolute emergency with maximum mobilization of staff and volunteers. As much concern should be directed to each outbreak as would be directed to control an outbreak in a non-endemic country such as in Europe. Never should a case occur more than 21 days after discovery of an outbreak.
“With the very small number of outbreaks present and with fully effective containment, smallpox transmission should be stopped in India in not more than 6-8 weeks. An all-India, all-out effort to achieve this objective will commence immediately and at all levels of the programme. These activities will be conducted under the code name ‘Operation—Smallpox Zero’ with the objective that no case of smallpox would occur after February.
“PROCEDURES
“1.0 A special Central command comprised of senior experienced Government and WHO staff will visit every new outbreak detected after 1 January and will revisit every outbreak in which a case is discovered more than 21 days after its discovery to ensure that every possible measure is being taken. These will supplement, not replace, other supervisory visits. To facilitate this, all new confirmed outbreaks must be reported immediately by cable to the State Programme Officer and to New Delhi. Any case occurring more than 21 days after discovery of an outbreak must similarly be reported by cable.
“2.0 Every outbreak must now be dealt with rapidly and with a massive containment effort. Instead of three or four workers, the containment teams should consist of 15 to 20 workers or more, headed by the District Medical Officer of Health assisted by a national or WHO epidemiologist. In urban areas, this number may be several times greater. Vaccination in an infected village/mohalla must be essentially completed within two or at most three days. Three or four workers must camp in the village/mohalla until all scabs have separated from the last case. Two watchguard-vaccinators must be assigned to each infected house to maintain a 12- hour watch during the day while a second pair maintains a 12-hour watch at night. Watchguards will be responsible for (1) vaccinating all persons visiting the houses of smallpox patients ; (2) identifying all household contacts who leave to go to other areas ; (3) maintaining isolation of smallpox cases; and (4) maintaining an hour-by hour log book record of activities and of movement of people in and out of the households. Food, necessary medicines and housing may be supplied to the family of an infected patient on a daily basis to ensure cooperation and isolation. Smallpox containment field books with complete enumeration of the village/mohalla must be completed on each outbreak. A typical containment team might include:
- 4 Watchguard-vaccinators for each infected house
- 8 vaccinators of which 4 should camp each night in the village
- 2 motivation workers (village-level workers who know the village/mohalla and are respected by the villagers)
- 1 supervisor and 2 vaccinators to trace household contacts who have gone to other areas
- 3 supervisors
- 1 containment team leader.
“3 .0 House-to-house search will be made in a 10-mile [16-kilometer] radius around an outbreak’ as well as in high-risk areas which may be outside the 10-mile radius. In the urban areas the surrounding mohallas will be searched in a similar manner. This will be followed in two weeks by a second house-to-house search within a five-mile [8-kilometre] radius to find cases which might have been in the incubation period during the first search .
“4.0 In case of a death, the vaccinator will accompany the remains to be certain that the body is properly disposed of and that all garments are buried. All attending the funeral will be vaccinated, a register of participants and their addresses will be prepared and all villages from which they came placed under surveillance.
“5.0 After 1 January, a laboratory specimen from one or two cases in each new outbreak will be collected.”
It was decided that the periodic routine, search programmes would consist of house-to-house visits, whereas previously searchers had checked only a sample of houses in each village. The reward for reporting a case was increased from 50 rupees to 100 rupees . Each suspected case-i.e., one with a rash and fever-was to be recorded in a “rumour register”, which was established at every primary health centre. Each patient was to be visited immediately by the local health officer and the diagnosis confirmed by an epidemiologist. If the diagnosis was uncertain, it was to be considered smallpox and watchguards were to be posted. By experience, it was found that good performance on the part of watchguards could be ensured by the simple expedient of not paying them until they were relieved of duty. If, at any time, a watchguard was not found on duty, all 4 were dismissed without pay and new watchguards were recruited. Containment vaccination was to include all persons within a 1-mile (1.6-kilometre) radius of the outbreak. In all, this meant vaccinating some 4000-5000 people in rural areas and 80 000 in urban areas (Sharma & Grasset, 1975). Search throughout an area with a 10-mile (16-kilometre) radius, performed by locally recruited and trained staff, usually encompassed 300-600 villages. The costs of a typical containment operation in 1975 were estimated by Jezek to be about US$2700 (Table 15.30).
Investigations into the source of the outbreak were intensively pursued by national and international epidemiologists, but now, instead of notifying neighbouring states or districts of the existence of a suspected source, they themselves proceeded to the locality. This ensured that the sources would not be missed because of difficulties with telegraphic communication or confusion due to information being received from illiterate villagers and the consequent need to spell village names phonetically.
To guard against importations from Bangladesh, special surveillance teams were assigned and special searches conducted in Muslim Bengali areas and communities in India. Special attention was given to Calcutta, in which repeated night searches were made among the 48 000 street dwellers (Spring, 1975).
Table 15.30: India: estimated manpower employed and costs of a typical containment operation, 1975
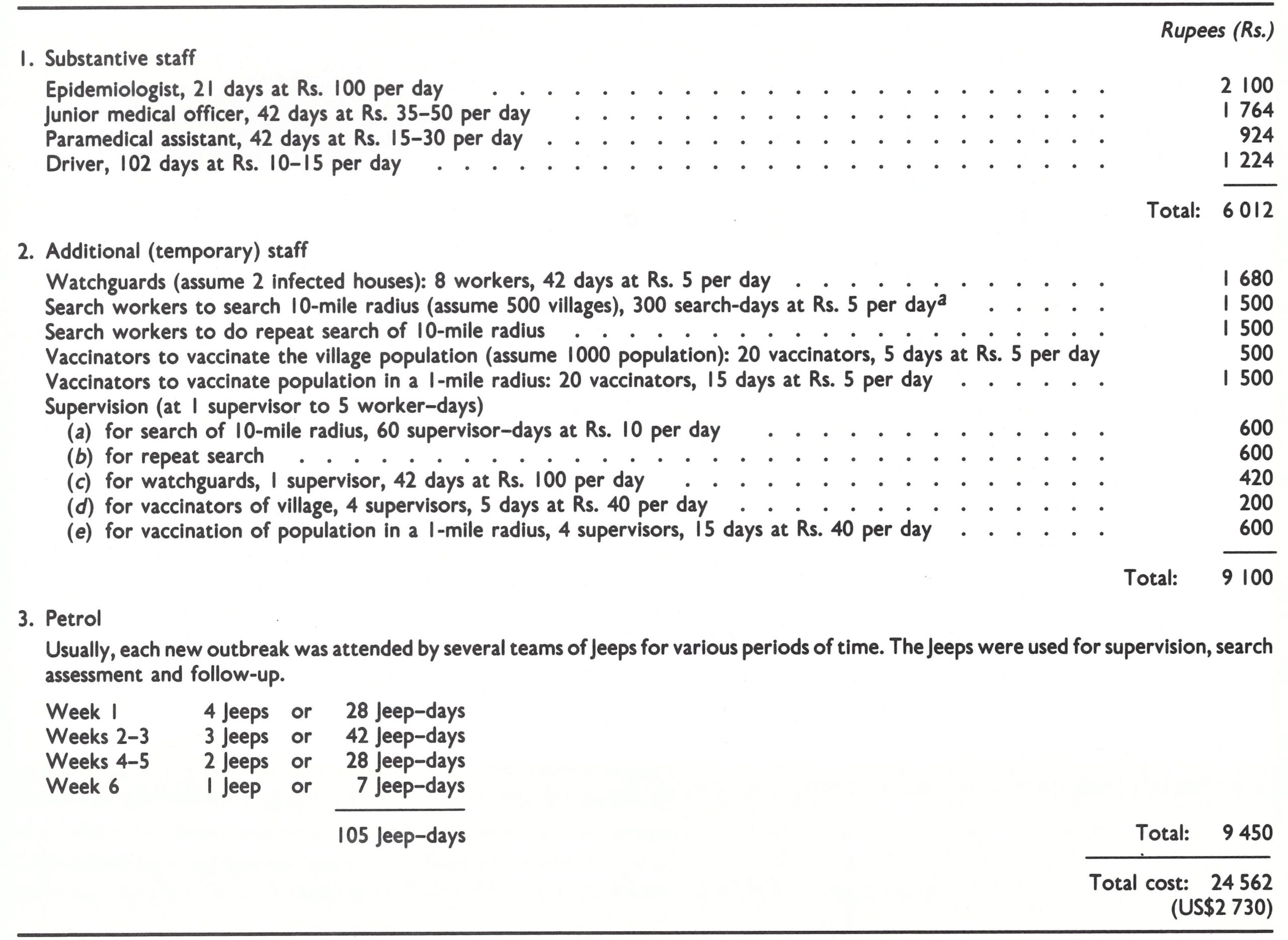
abased on petrol costs averaging Rs. 90 per day.
Table 15.31: India: number of reported cases of smallpox, by state and by month, 1975
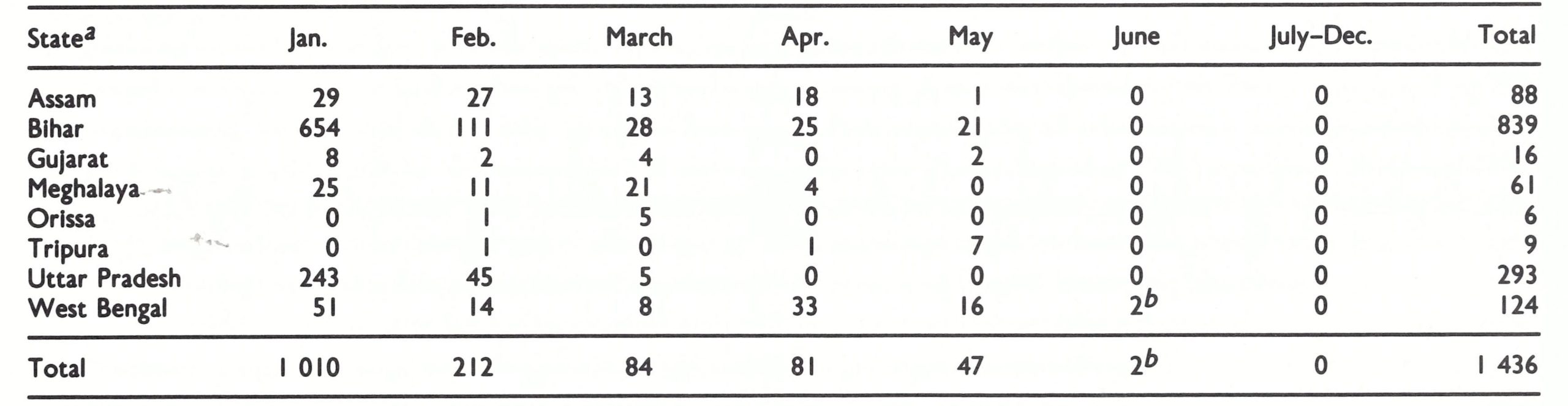
a Nil reports were received from other states and all the union territories.
b The data of onset of the last case was 26 May (cases are listed by month of report).
Table 15.32: India: newly detected outbreaks of smallpox by state and by month, 1975a
a Outbreaks were reported immediately by telegraph or telephone; case reports (Table 15.31) were submitted through routine notification channels and were somewhat delayed in receipt.
“Operation—Smallpox Zero”, begun in January 1975, proved to be most successful. From November to December 1974, the number of pending outbreaks had decreased from 343 to 285 (17%) ; in January, to 194 (32%) ; and in February, to 113 (42%). As had been feared, cases were imported from Bangladesh, 30 importations being detected in West Bengal, Assam and Tripura (Fig. 15.25). Two-thirds were detected within 2 weeks of the onset of illness in the first case and only 8 additional outbreaks occurred as a result of further spread.
In all, only 308 outbreaks and 1436 cases were detected in India after 1 January 1975 (Tables 15.31 and 15.32). All were in the eastern part of India except for 10 in the far western Kutch desert of Gujarat, introduced by migrants probably infected in Bihar.
In April, 115 000 health workers undertook a week-long, house-to-house search throughout the whole of India. Independent assessment of some 5% of villages showed that 85%-96% of all villages in the various states had been searched. Among 574 517 persons interviewed, 61% knew about the reward for reporting a case and knew the amount of the reward. Only a few outbreaks were found, all of which had resulted from importations. Smallpox had been virtually eliminated during the season of most rapid transmission. In May, the last cases and outbreaks in India were discovered.
The Last Case in India, May 1975
As in many other countries, so in India the last case presented some unusual features (Jezek et al .,1978a). Saiban Bibi, a 30-year-old homeless Bangladeshi beggar, developed a rash while living on the Karimganj railway station platform in Assam, where she was begging for food. She had contracted smallpox from a patient in Sylhet District, Bangladesh. On 26 May, she went to the Civil Hospital in Karimganj, which forthwith notified the District Health Officer. Accompanied by a WHO epidemiologist and the state surveillance team, he immediately went to investigate.
The situation was alarming. For the first 4 days of illness, the patient had lived on the platform of the railway station, the gateway to the states of Assam and Tripura and the union territory of Mizoram. Between 22 and 26 May, 9 trains had stopped at the station and 4535 railway tickets had been issued to 68 different towns and cities. A programme was immediately launched to search and vaccinate in the city wards in which the railway station and the Civil Hospital were situated . Later, containment activities extended to the whole town, as well as to all villages visited by the patient since 21 May. Railway authorities were instructed to intensify surveillance activities in and around the railway stations and railway colonies. All district health authorities in Assam and neighbouring states through which the railway passed were asked to initiate intensive searches during the subsequent 14 days. Special searches were conducted in all villages within 10 miles (16 kilometres) of the district border with Bangladesh.
The patient was isolated and 4 watchguards were stationed in the isolation ward for round-the-clock duty. All patients, visitors and hospital staff, together with their relatives, were enumerated and vaccinated. The hospital was closed to visitors and the discharge of patients was stopped. One watchguard was placed at the railway station to carry out surveillance and vaccination.
Three border checkposts were established and all incoming and outgoing travellers were checked and vaccinated. All border security forces and police outposts were alerted to look for possible cases .
Surprisingly, despite the time of year and the many persons who had been in contact with the patient, no further cases were found.
Fig. 15.25. Importations of smallpox from Bangladesh to India, 1975.
India Celebrates Independence Day and Freedom from Smallpox, August 1975
Six weeks passed after the onset of illness in the last patient and the last outbreak was deleted from the list of pending outbreaks. On 1 July, the reward for reporting a case was increased to 1000 rupees (US$1 25), the equivalent of 4 months’ salary for an Indian labourer. This was done with some trepidation, since it was feared that unscrupulous persons might smuggle smallpox cases from Bangladesh to claim the reward. Indeed, on one occasion this did happen, but the ruse was readily detected. With a reward of this magnitude, thousands of patients with rash and fever were reported to the health authorities. Each was investigated; none proved to have smallpox.
On 15 August 1975-India’s Independence Day-the government held a special celebration honouring India’s freedom from smallpox, which was attended by the Director-General of WHO.
Less than 3 months had elapsed since the onset of the last case, and with smallpox still present in Bangladesh the staff were understandably apprehensive that at the last moment another focus might be found. The search continued, but an unexpected event of quite another type occurred. On the night of 15 August, the President of Bangladesh was assassinated. The government closed the airports and sealed the borders-to the extent that this was possible. It was feared that there might be yet another mass exodus of refugees.
An emergency surveillance programme was immediately put into operation, focusing on Bengali-speaking areas. Possible migration routes were identified, dozens of surveillance posts were set up at border crossings, special searches were conducted in designated high-risk areas and surveillance was intensified in Calcutta. Happily, the refugees were few and no further importations occurred.
On 16 October 1975, the last case of smallpox occurred in Bangladesh and the 2-year search began to confirm eradication throughout Asia.
Plate I5.17. A wall-sized poster, in the style of a cinema advertisement, depicts a hero slaying the smallpox demon with a bifurcated needle. This poster, also used in smaller sizes, was displayed widely in India to promote the reward for reporting a case of smallpox.
Why the Smallpox Eradication Programme Succeeded
Two papers have been published by members of the smallpox eradication staff which comment on distinctive features of the smallpox eradication programme in India that were crucial to its success. Extracts are given below:
"The strategy used and the manpower and other resources provided . . . greatly contributed to the rapid success of the programme; but without the passion given to the planning and implementation of the programme by the workers, achievement would not have been possible. Jawahar Lal Nehru once said `Planning would be meaningless unless behind the plan there was a passion—passion with a tinge of anger at delays, anger at anybody not doing his part, anger at not achieving where achievement is possible’. The national and WHO staff have fought with passion the battle against smallpox . . . Hundreds of men and women—nationals and internationals—have worked up to 18 hours a day for seven days a week in the belief of an ideal which they have put above their personal happiness, their family life, their career and their health. The central level staff both of the WHO and the Government of India have spent on an average three weeks a month working in the field throughout the country to train, motivate, encourage the local staff. During the 1974 summer epidemic of smallpox in Bihar and [Uttar Pradesh], a number of WHO, central and state officers were publicly laughed at for having predicted that their states and the country would be free of smallpox in less than a year . . . Men and women from different states in India and from many countries of the world put aside their racial, national, religious or social prejudices and bore together all the difficulties and hazards . Many took risks in putting aside conservative regulations, red tape and antiquated technical methodologies, when these threatened to delay their task or obstruct the path to success. The toughest of men and women on many occasions were on the verge of discouragement—from physical tiredness and mental frustration, when having to cope with hundreds of infected villages in their area of responsibility. They persevered, waiting days, weeks, sometimes months, until it was possible to send them more men, better vehicles, funds for petrol, etc. In the smallpox offices in New Delhi and also in the state, district and block headquarters, medical officers, administrators and secretarial staff worked most of the days far into the night, over the weekends and public holidays so as to make sure that those in the field received the necessary support. However, even during the most difficult stages of the programme, men and women in the field and offices discovered like Rabindra Nath Tagore that they `acted and behold duty was joy' ." (Sharma & Grasset, 1975.)
"The decentralisation of authority to implement the strategy to the district health authorities and epidemiologists who were responsible for proper utilisation of available resources resulted in the early detection and effective containment of large numbers of disease foci in the shortest possible time and the consequent quick interruption of transmission. If one considers that . . . India . . . [was] spending over 40 million rupees a year for the past ten years on NSEP and [that an] additional amount of about Rs. 20 million each [year was being spent by WHO] during the campaign years 1973-74 and 1974-75 . . . it becomes apparent that it has not been the quantum of money spent but the manner of doing it which made all the difference between success and failure. Relative freedom at district levels to take on-the-spot decisions to spend this additional amount. . . greatly contributed to the realisation of smallpox free status. Administrative and operational restraints in implementing the strategy were also minimal.
"All the national health programmes have built-in evaluation methods. The interval between occurrence of a defect/problem and its detection and the interval between the detection and correction has always been considerable . . . In this smallpox campaign the continuous monitoring of the smallpox status, feedback from the field staff and the authority for taking on-the-spot decisions regarding fiscal, administrative and technical matters have narrowed down the unknown and the unsolved problems to the minimum ." (Dutta et al ., 1975.)
Morbidity and Mortality Data
Information regarding the age, sex, vaccination status and survival or death of the patient was obtained for all cases in India. However, data were tabulated nationally for only a proportion of the total for the years 1974-1975 (Basu et al., 1979). These data were obtained from 4 high-incidence states and 13 low-incidence states and union territories, although most of the cases were from the former group. The age distribution of cases and case-fatality rates were similar to those observed elsewhere in the Asian subcontinent (Table 15.33).
Data are available for 23 546 of the 189 439 cases which occurred in 1974 1975. In all, 31%, occurred in individuals less than 5 years of age, 40% in those aged 5-14 years, and 29% in those aged 15 years and over. The disease was equally prevalent among males and females.
A similar distribution of cases by age and sex was observed in all states with a high incidence. Imported cases in smallpox-free states, however, occurred predominantly in males (64.6% ) in the older age groups, 18.7 % being in men aged 50 years and over. This was attributed to the occurrence of many cases among migrant labourers and pilgrims, a much larger proportion of whom were adult males.
Data regarding the vaccination status of 14 463 cases from the same 17 states and union territories reveal that two-thirds of the persons concerned were unvaccinated (Table 15.34). Patients were classified as “unvaccinated” if they had no vaccination scar (regardless of whether they claimed to have been vaccinated) or if they had been vaccinated during the incubation period of the disease, too late to prevent infection.
The proportion of cases among individuals with an apparent vaccination scar was markedly higher than in other countries. This is explained by the frequent occurrence of vaccination-like scars associated with the use of rotary lancets in which secondary bacterial Initially, most cases and deaths were reported from infectious disease hospitals, to which the more seriously ill were taken and which recorded high case-fatality rates. As time progressed, differences between case-fatality rates in the various states narrowed considerably. Moreover, a much higher proportion of cases in otherwise smallpox-free areas was found among older children and adults, who experienced a lower case-fatality rate than did young children. Data for 23 546 cases that occurred in 1974-1975 show an overall case-fatality rate of 17.4%, but among infants under 1 year of age the rate was 43.5 whereas it was only 6.5% among the 15-19- year-olds. Although wide variations in case-fatality rates were observed in different epidemics, these variations were considered to be due to differences in the age distribution of the cases, the nutritional status of patients, and the history of previous vaccination.
infections occurred but vaccinia virus did not grow. Most of the cases among “vaccinated” children under 5 years of age occurred in Bihar and Madhya Pradesh, in which, as late as 1973, rotary lancets were still being used in some areas, especially the large municipalities. In Andhra Pradesh, in which the use of rotary lancets was abandoned in 1969, only 15.4% of cases occurred among those with what appeared to be a vaccination scar.
Case-fatality rates in India varied from 21 % to 31 % during 1950-1967 but for most years they were in the range of 25-30%. During the course of the eradication programme, the case-fatality rate dropped steadily, from 31.2% in 1967 to 16.6% in 1974 and to 12.3% in 1975 (Fig. 15.26). The decline is accounted for by an increasing completeness of the notification of cases.
Table 15.33: India: number of reported cases of and deaths from smallpox and case-fatality rate in 17 states and union territories, by age group, 1974-1975a,b
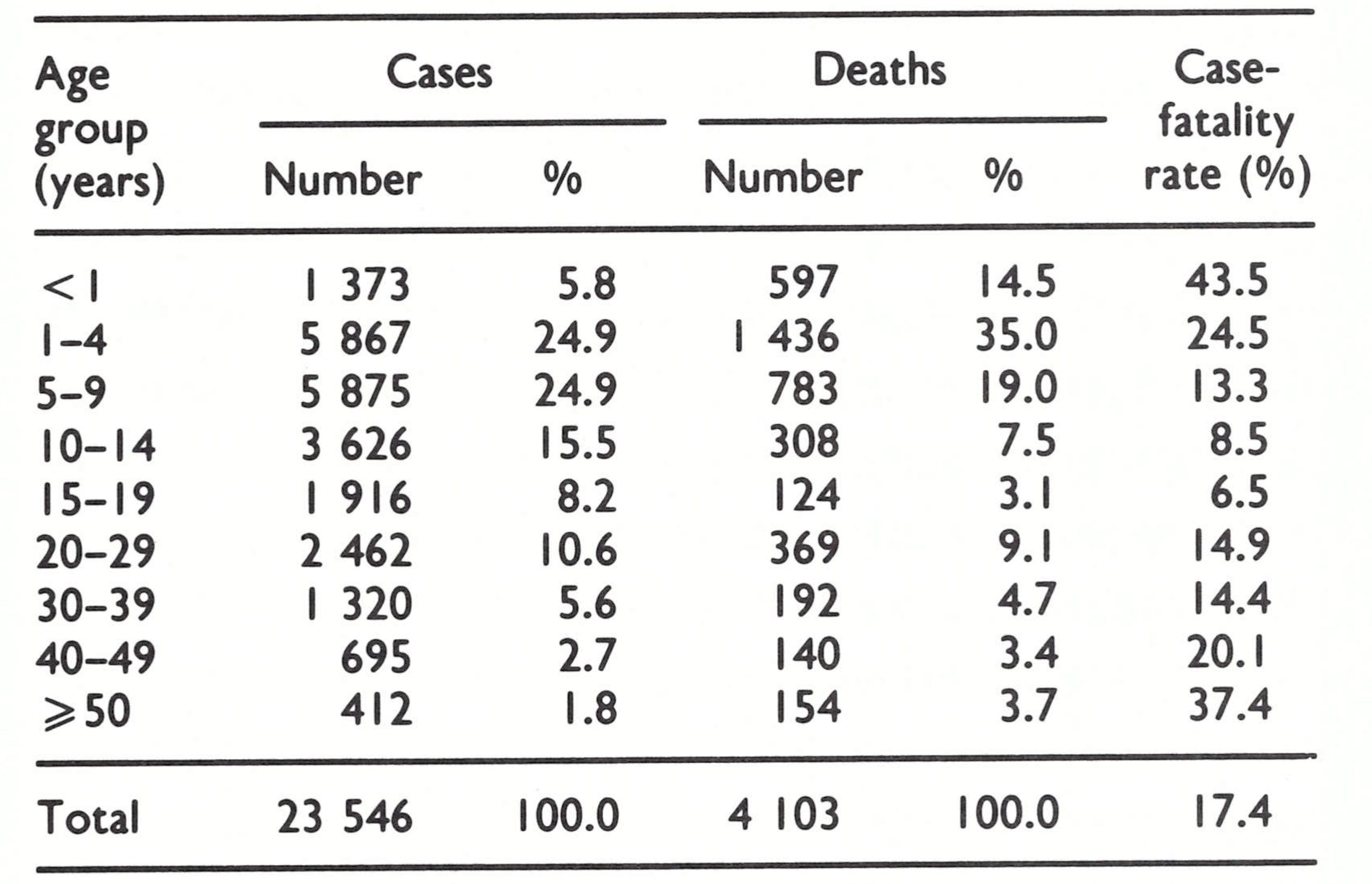
a From Basu et al. (1979).
b States with a high incidence: Bihar, Madhya Pradesh, Uttar Pradesh and West Bengal. Others: Andhra Pradesh, Assam, Gujarat, Haryana, Jammu and Kashmir, Karnataka, Maharashtra, Orissa, Punjab, Rajasthan, Tamil Nadu, Tripura, and the union territory of Delhi.
Table 15.34: India: vaccination status of cases of smallpox in 17 states and union territories, by age group, 1974-1975
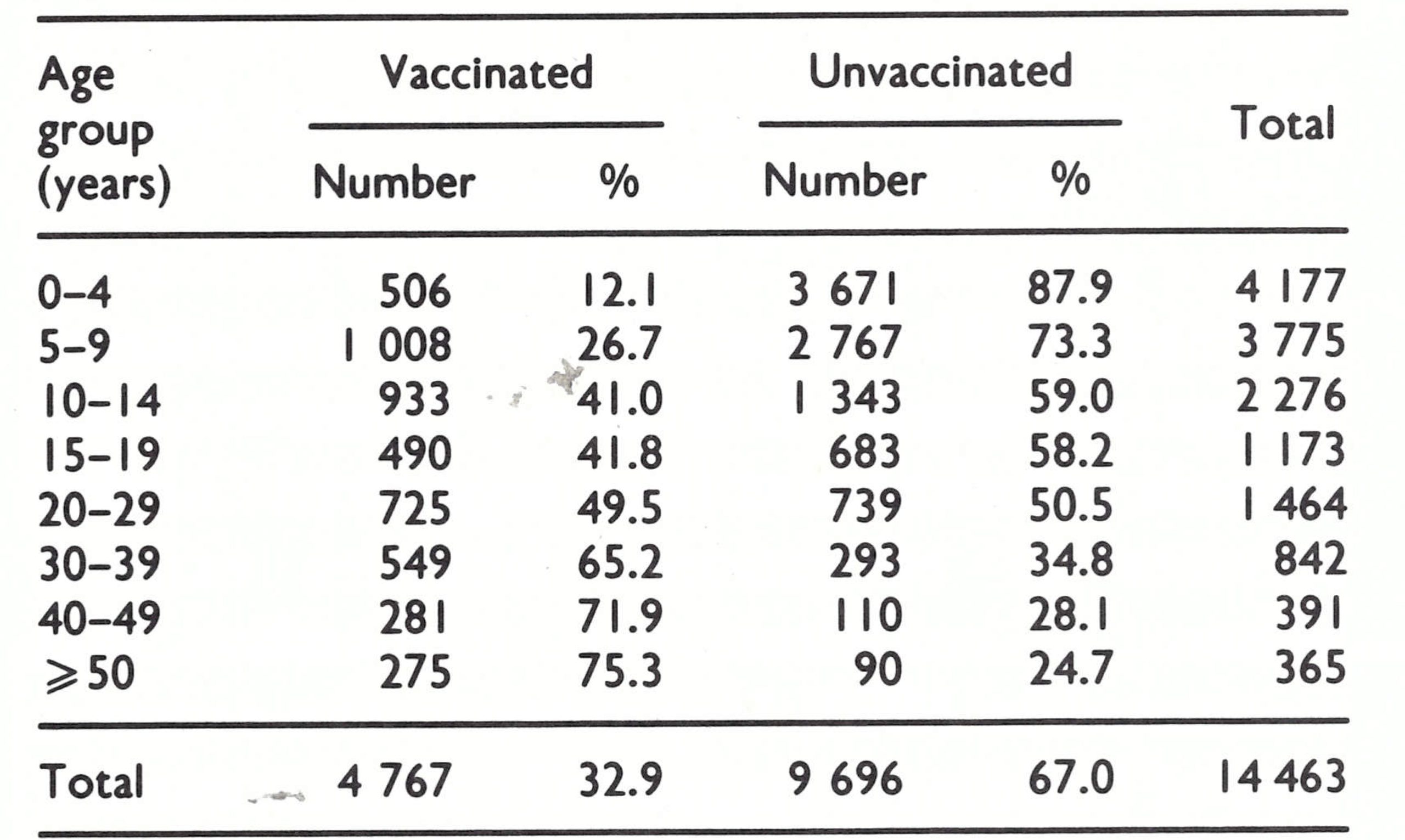
Fig. 15.26. Case-fatality rates for India and the states of Andhra Pradesh, Assam, Bihar, Gujarat, Haryana, Jammu and Kashmir, Karnataka, Madhya Pradesh, Maharashtra, Orissa, Punjab, Rajasthan, Tamil Nadu, Tripura, Uttar Pradesh and West Bengal, by year, 1967-1975. Each dot represents the case-fatality rate in a state in a year. For each year rates are plotted only for the states that recorded at least 100 cases that year. The bold lines denote the overall rate for India in the year shown.
NEPAL
INTRODUCTION
Epidemiologically, Nepal was a mountainous extension of the Indian states of Bihar and central and eastern Uttar Pradesh, but its programme differed significantly from that in India. Of the country’s 10 .8 million population (in 1967), 37% lived in the Terai, a northern strip of the broad Ganges river plain (see Fig. 15.1), which in Nepal was about 25-35 kilometres wide; another 53% lived in the adjacent Middle Hills area, which ranged from 30 to 50 kilometres in width. Most of Nepal’s population thus lived within some 80 kilometres of the border with India and the majority were Hindu. Many had relatives in adjacent areas of India, and travellers and migrant labourers moved freely across the border. Roads were few, communications were difficult and the health services and other governmental structures were in an early phase of development.
In 1962, a WHO nurse working in Nepal assisted in the development of a pilot mass vaccination campaign in the Kathmandu valley, comprising 3 of Nepal’s 75 districts with a population of 500 000. In 1968, the campaign was extended to other districts and by 1973 it included the entire country. Little was done to develop a reporting system until 1971. Data prior to this time represent only a partial enumeration of cases in the Kathmandu valley.
Strategically, the programme in Nepal was initially not of high priority in the global strategy because eradication there depended on the progress of the campaign in India, particularly in Bihar and Uttar Pradesh. Moreover, the mainly mountainous terrain, the predominantly rural population and the poor communications between villages in Nepal suggested that smallpox transmission could not be long sustained in most of the country. Since the population of the Terai was only about 4 million-the equivalent of 2 districts of India-it was expected that the interruption of transmission in that area and in the country as a whole would not constitute a major problem once smallpox had been controlled in India.
Because the health structure in Nepal was rudimentary and vaccine was available to only a small proportion of the population, additional WHO support was provided from 1968. The eradication programme was in tended to make vaccination more widely available initially in the most populous areas along the border with India. Three years later, a plan was implemented to extend reporting and surveillance-containment measures progressively throughout the 75 districts. Progress in achieving these goals was remarkably rapid: by 1972 each outbreak was being investigated and contained and its source identified. Continuing transmission was, in fact, largely stopped in that year. Epidemic smallpox in the neighbouring Indian states of Bihar and Uttar Pradesh, however, resulted in an additional 239 outbreaks in 1972 and 1921 cases during the period 1973-1975. Most of these outbreaks could be traced directly or indirectly to importations and although they sometimes remained undetected for many weeks and were not always well contained, smallpox did not usually spread widely. On 6 April 1975, the last known case of smallpox occurred in Nepal as a consequence of an outbreak resulting from an importation from Bihar.
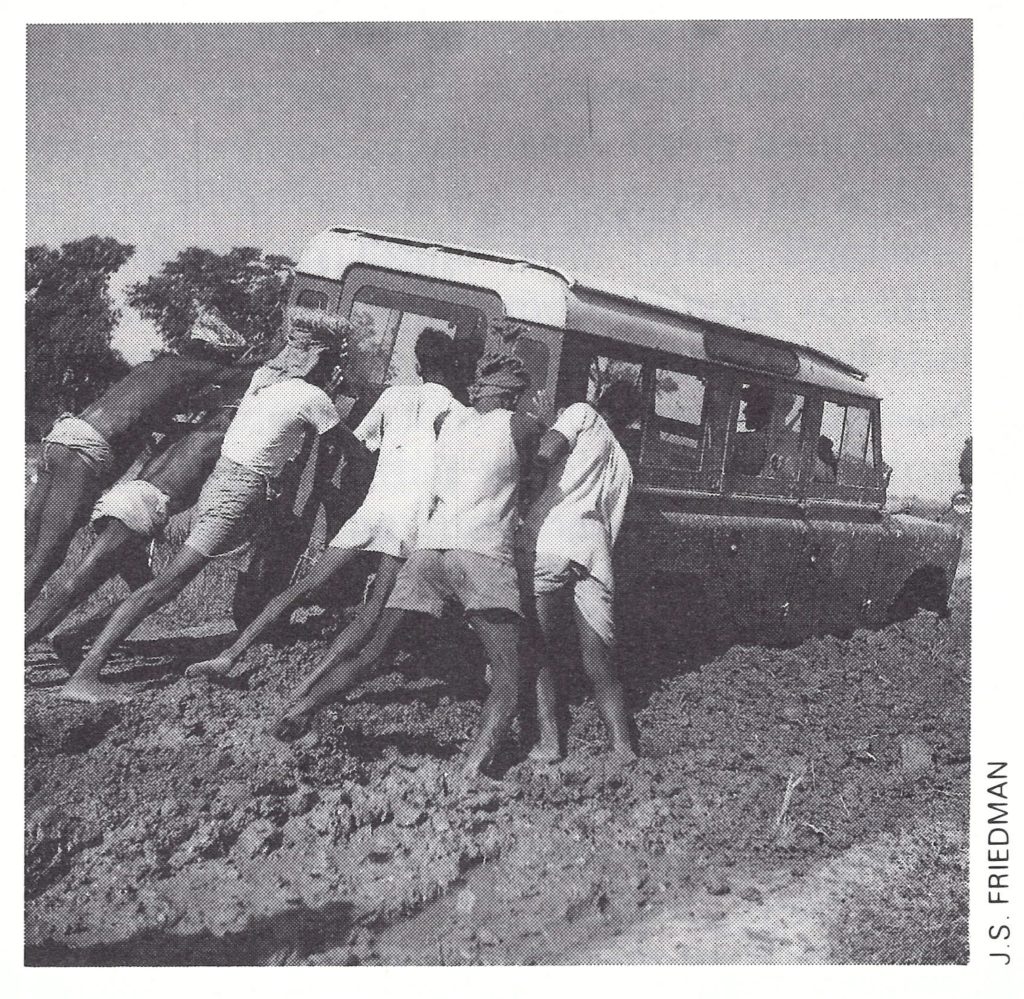
Plate I5.18. At times, the roads in Nepal were almost impassable.
The Country: Geographical and Sociocultural Considerations
Until 1951 Nepal, ruled by hereditary prime ministers, had been closed to the outside world, and no organized health services or educational facilities existed . When a constitutional monarchy was instituted in 1951, Nepal began the arduous task of building a transport, communication, health and educational infrastructure. Because of the mountainous nature of the country and the dearth of human and natural resources, progress was slow. Throughout the 1970s, Nepal remained one of the world’s least developed countries.
Administratively, the country was divided into 14 zones, which were subdivided into 75 districts; the population of a district ranged from 7000 to 350 000, a far smaller figure than that for a district in India. The smallest administrative unit was the panchayat, of which there were some 4000.
Until the 1960s smallpox had occurred widely throughout Nepal . According to a health survey conducted in 1965-1966, 24% of people over 30 years of age in the capital city of Kathmandu bore the facial pockmarks of smallpox, as did 13% of those aged 10-29 years and 6% of children under 10 (WHO/SE/78.107, Shrestha). Variolation was known to have been widely practised until recent years and many older persons bore the resulting scars. However, unlike the situation in Afghanistan (see Chapter 14), the practice had died out in Nepal by the time the Intensified Smallpox Eradication Programme began. No cases attributable to variolation were discovered during the course of the programme.
As in India, smallpox epidemics were reported to have occurred approximately every 5 years, the last having happened in 1958 (WHO/SE/78.107, Shrestha). However, up to 1963, there was no reporting system; indeed, until 1971 few reports were received from anywhere except the small districts comprising the Kathmandu valley, the site of the capital city. Some Nepalese, especially those living in the Terai, had been vaccinated in India, as had some living near Kathmandu or in the vicinity of the few health units that had vaccine. Otherwise, vaccination was little practised in Nepal.
Socio-economic and demographic factors played unusually important roles in the development of the programme and in the pattern of occurrence of the disease . Geographically, the country consisted of three horizontal belts (Fig. 15.27) extending across the country: the flat Terai of the Ganges river plain, with a population density ranging from 750 per square kilometre in the east to fewer than 100 per square kilometre in the less fertile west (Fig. 15.28); the Middle Hills area, with a terrain rising as high as 3000 metres and containing a few broad populous valleys including the Kathmandu valley, which had a population density of almost 1000 per square kilometre and about 5% of the country’s inhabitants; and the Himalayan mountains, comprising 30% of the land surface but containing only 5% of the population. Very few people crossed the Nepal-China border, but travel across the Nepal-India border was unimpeded and frequent.
With only 680 kilometres of paved roads and 2 short railway lines (Fig. 15.27), there was little easy communication between the different areas of Nepal, although a network of footpaths connected the 29 000 villages and market centres in which 95% of the population resided. Kathmandu (population in 1971, 150000) and Biratnagar (population, 45 000) were the only significant urban centres. On the other hand, contacts between the Terai and Kathmandu and India were numerous and were facilitated by the few motorable roads between the two countries.
The Nepalese of the Terai are Hindu and ethnically similar to their Indian neighbours. Many resisted vaccination for religious reasons ; temples to Sitala mata, the goddess of smallpox, were to be found throughout the region. The relatively rich agricultural and industrial area of the eastern Terai attracted numerous Bihari and Bengali seasonal migrants, who formed a sizeable proportion of the labour force. Travel to and from the less prosperous western Terai was limited primarily to family visits, and few travelled long distances. Those living in the Middle Hills were predominantly Hindu, but with the exception of some segments of the Newar ethnic group in the Kathmandu valley most people readily accepted vaccination. Travel to and from the Middle Hills was less frequent than within the Terai, although many moved to the Terai and to India for the winter months. Numerous inhabitants of the Eastern Hills worked on tea estates and as forest labourers in the Indian state of Assam and those in the Western Hills travelled to western Uttar Pradesh and cities of western India for work and trade. In the sparsely populated Himalayas, villages were isolated. To reach most districts from the endemic areas of India required a trek of more than 14 days-longer than the incubation period of smallpox. Because of these factors, smallpox proved to be primarily a problem of the Terai, only 4 outbreaks ever being detected in the extensive northern mountainous areas (SME/77 .1, Shrestha et al.).
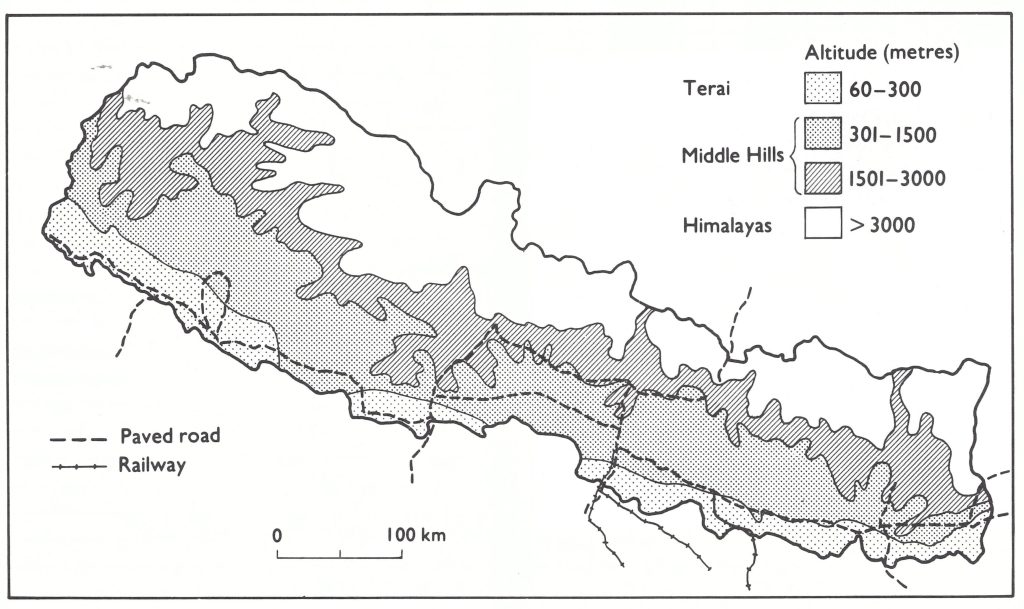
Fig. 15.27. Nepal: physical topography, showing paved roads and railways.
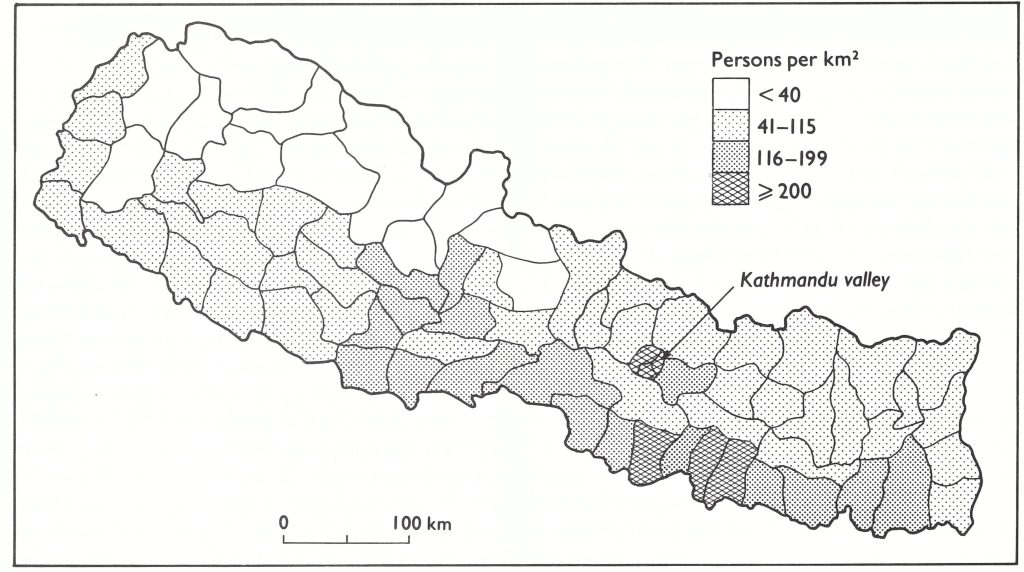
Fig. 15.27. Nepal: population density, by district.
A Smallpox Control Pilot Project Begins, 1962
A smallpox control pilot project was initiated in 1962 in the 3 districts comprising the Kathmandu valley, which had a population of about 500 000 at that time (WHO/SE/69.10, Singh). With assistance provided by a WHO nurse already employed in another project in Nepal, a house-to-house mass vaccination campaign was begun, utilizing the multiple pressure method of vaccination and freeze-dried vaccine provided by WHO. As in India, all records were maintained in family registers in which the names of all residents of households were laboriously compiled, revised and updated. The programme was poorly funded, poorly supervised and poorly executed and with the additional impediment of resistance to vaccination progress was slow. A sample survey carried out late in 1964, 21 years after the programme began, revealed that only 31% of the population had vaccination scars. In 1963, for the first time Nepal began to report cases of smallpox to WHO, but virtually all of them had occurred within the city of Kathmandu. In 1966, a WHO medical officer was assigned to assist the programme, but no effort was made to develop a national reporting system, and until 1968 the programme remained what it had been-an ineffective vaccination campaign confined to the Kathmandu valley. Repeat surveys in May 1967, conducted among various population groups in that area, showed that only 40-65% of the people examined had vaccination scars or the pockmarks of smallpox (WHO/SE/69.10, Singh).
The Programme Extends Beyond the Kathmandu Valley, 1968
In 1967 the government and WHO agreed on a phased plan to extend the programme zone by zone throughout the country. This commenced the following year with the hope that the last of the zones would be included in the programme by 1972. Additional resources were made available by the government, and WHO provided support in the form of personnel, vehicles and equipment and also covered the cost of petrol (Table 15.35). Staff were recruited, trained and assigned to district offices to serve as “senior vaccinators”. During the first 3 months of a new vaccination campaign in a district, temporary vaccinators were hired to vaccinate widely throughout the district. Subsequent vaccination and surveillance were then the responsibility of the senior vaccinator. The family registers were abandoned and multiple puncture vaccination with bifurcated needles was introduced.
The number of districts covered by the programme grew from 3 in 1967 to 15 in 1968 and to 41 by the end of 1970. The number of vaccinations performed increased 10-fold, from 201 000 in 1965-1966 to 2 196 000 in 1968-1969 and to 2 823 000 in 1970-1971 (Table 15.36).
Community leaders and such health staff as were available were contacted and requested to report cases, but the numbers of cases notified remained few: 110 cases were reported in 1967, 249 in 1968, 163 in 1969 and 76 in 1970 (Table 15.37). Although reporting was very incomplete, it is probable that the true incidence in Nepal during these years was not high because the corresponding incidence in the neighbouring Indian states of Bihar and Uttar Pradesh was low.
Table 15.35: Nepal: financial inputs by the government of Nepal and WHO for smallpox eradication, 1962-1976 (US$)
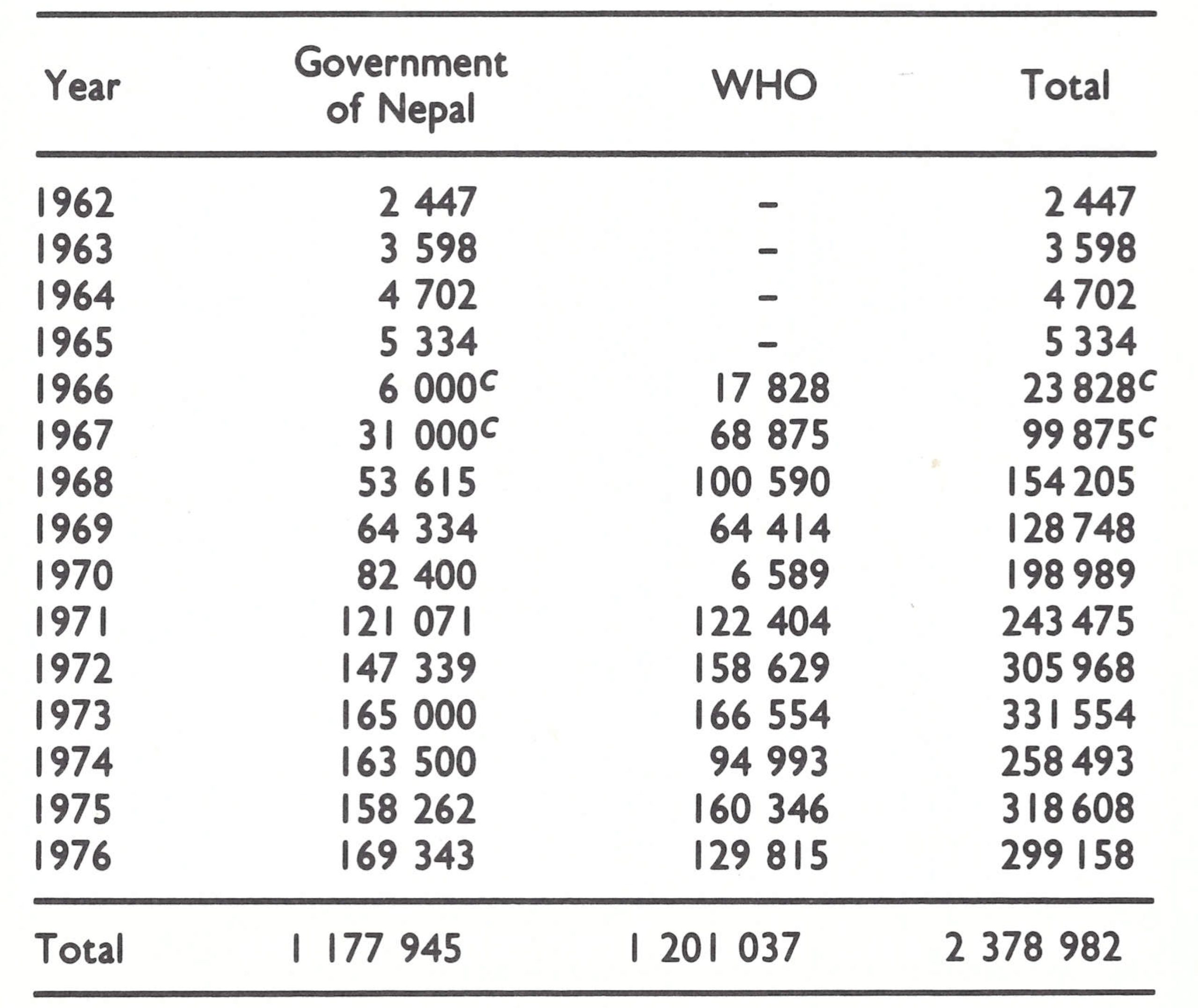
a Based on WHO financial records and data the government of Nepal (SME/77.1, Shrestha et al.).
b Excluding the cost of 160 000 vials of vaccine.
cEstimated.
Table 15.36: Nepal: number of vaccinations performed, 1962-1976
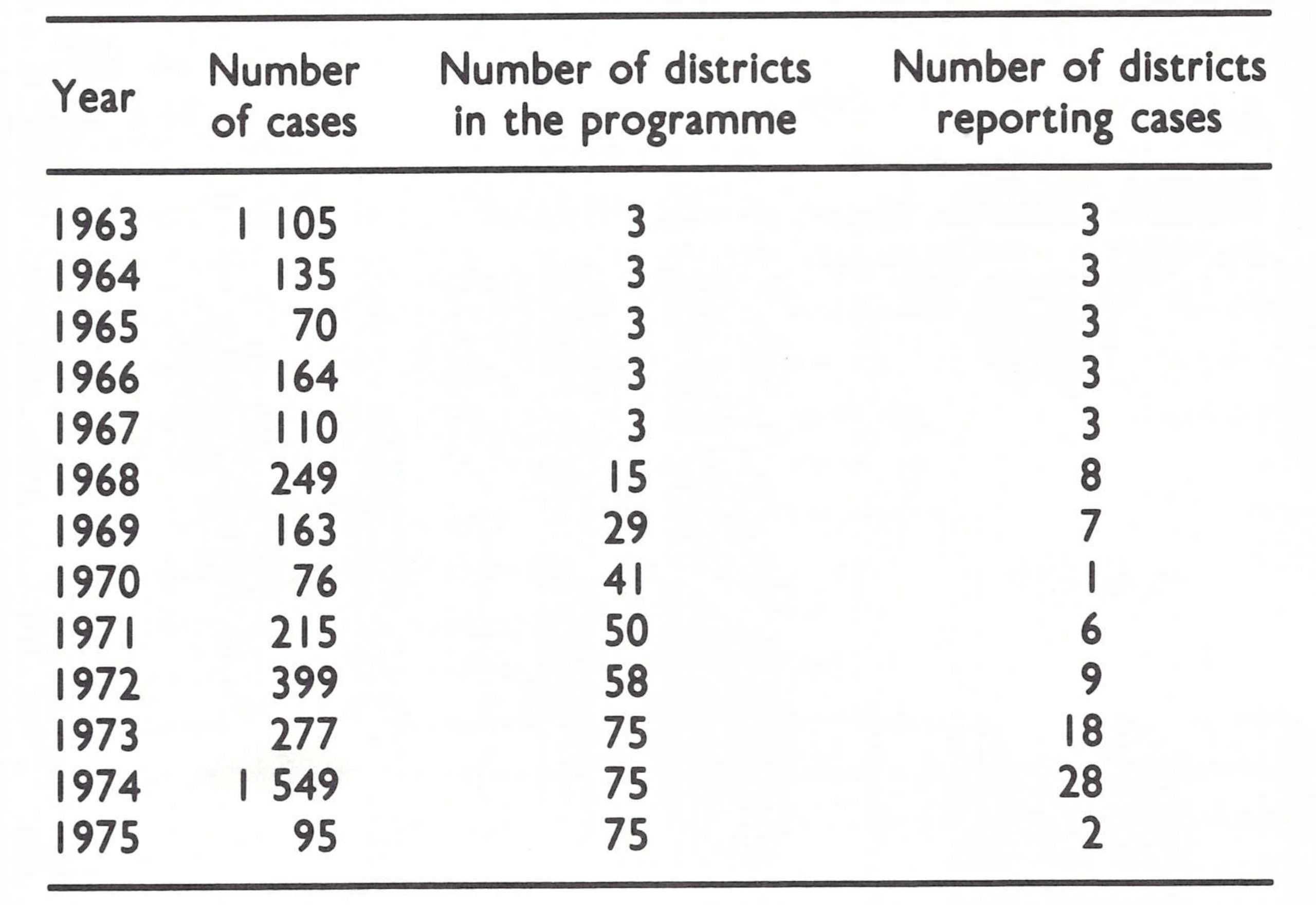
a ..=data not recorded.
Table 15.37: Nepal: reeported number of cases of smallpox, by districts reporting cases, 1963-1975
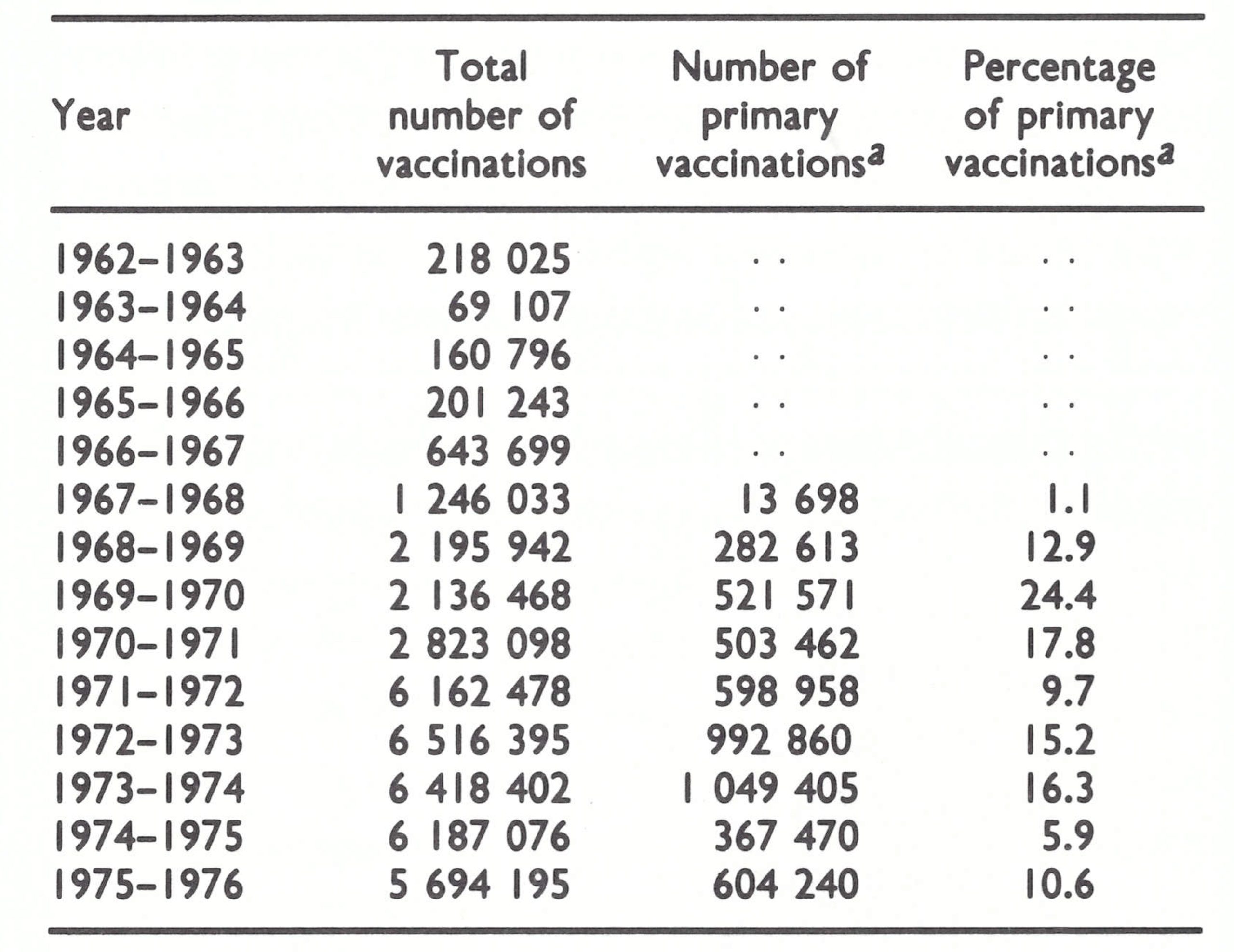
The Programme Strategy Changes, 1971
Early in 1971, a new strategy, unique to Nepal, was adopted and effectively executed by an energetic Nepalese programme director, Dr P. N. Shrestha, and an experienced WHO smallpox adviser, Dr M. Sathianathan, from Sri Lanka, assisted by 2 United States technical officers—veterans of the western Africa programme—Mr Jay Friedman and Mr David Bassett. It was decided to extend the programme as soon as possible to cover the entire country. Forty-five Nepalese district supervisors were recruited and assigned to most districts in the Terai and Middle Hills, and assistant supervisors or senior vaccinators were sent to the other 30 districts, where each worked under the direction of one of the district supervisors. A senior supervisor was responsible for managing the programme in each of Nepal’s 14 zones. In 6 districts, responsibility for smallpox eradication was assigned to a newly planned integrated health services project office (Fig. 15.29).
WHO and Nepalese staff decided that the vaccination campaign would be conducted during a single month in the winter of each year, and for this purpose temporary vaccinators (1 for each panchayat, comprising about 3000 persons) were recruited and trained during a 3-day training session. Simple tally sheets replaced the more elaborate record forms. During the remaining 11 months of the year, the assigned permanent smallpox eradication staff, numbering in all about 600 persons, travelled from village to village throughout the districts seeking information about smallpox from local leaders, schoolteachers and the personnel of health units. When cases were discovered, the staff were responsible for containment. Four central containment teams were formed to assist in this effort but were soon disbanded, since it proved impossible for them to reach the site of an outbreak before several days—or even weeks—had elapsed because of problems of communication and travel.
Despite the fact that mass vaccination was conducted during the course of a single month each year, the number of reported vaccinations increased to more than 6 million in 1971-1972—a number equivalent to 50% or more of the population—and continued at this level over the next 5 years. Surveys of vaccinial immunity, conducted in 1975 in many of the more accessible areas, revealed that in most of these areas more than 95 % of the population bore vaccination scars.
Reporting improved as the programme extended its operations; by early 1973 weekly telegraphic reports were being received from each district regardless of whether any cases had occurred.
Because of the difficulties of travel, responsible district supervisors proved to be the vital element in the programme. They were brought to Kathmandu annually for refresher training and were visited as often as possible in the field by Nepalese and WHO staff, who, beginning in 1972, undertook to visit the site of each outbreak to assess the efficacy of the containment measures. To facilitate travel to the most remote districts, arrangements were made by WHO to permit the charter of a helicopter; it was used on perhaps a dozen occasions during the subsequent 3 years.
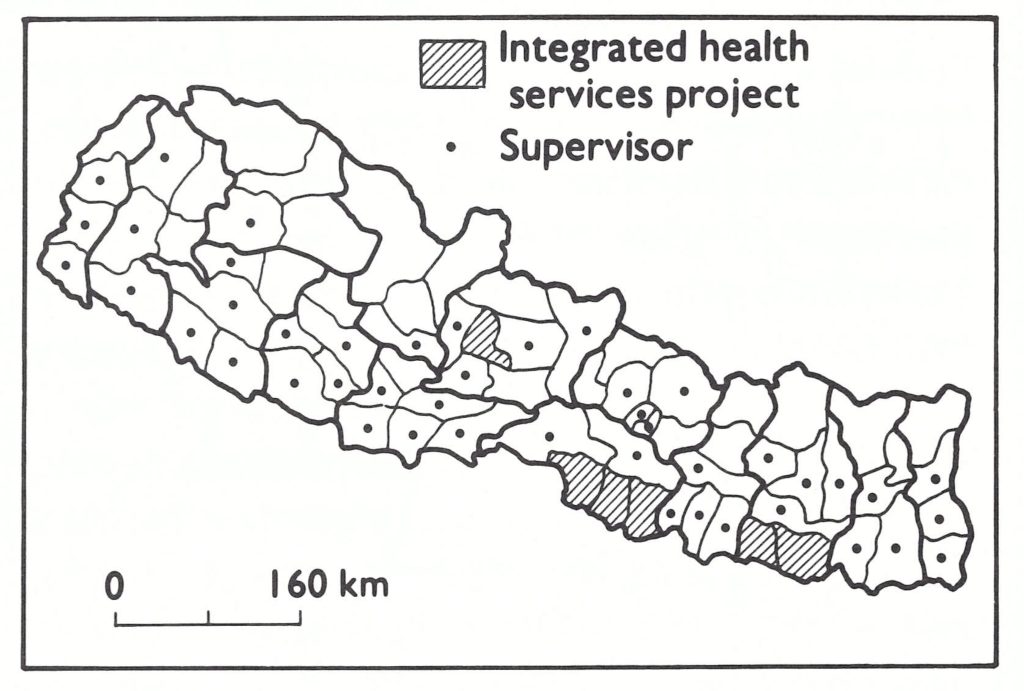
Fig. 15.27. Nepal: administrative divisions and location of district supervisors, 1971.
Plate I5.19. A: Purushollam N. Shrestha (b. 1939), the director of the smallpox eradication programme in Nepal from 1971. B: Jay S. Friedman (b. 1940), a WHO technical officer, being presented with a certificate of appreciation by the Prime Minister of Nepal, Tulsi Giri.
In 1972, the programme was extended to include all districts in the Terai and Middle Hills—the districts of greatest concern. Because of the isolation of the villages, most outbreaks were readily contained, and by the end of June 1972, transmission appeared to have been interrupted. During the last 6 months of the year, only 5 outbreaks, with 34 cases, were discovered (WHO/SE/74.71, Shrestha et al.); 4 resulted from importations from Uttar Pradesh and 1 from Bangladesh, whose north-western border with India was less than 50 kilometres—merely a day’s journey—from Nepal.
However, as epidemic smallpox swept across Uttar Pradesh and Bihar in 1973, increasing numbers of cases began to be imported into Nepal (Fig. 15.30). In all, 43 outbreaks and 277 cases were reported that year, of which 35 outbreaks resulted from importations from India. Twenty-eight more cases occurred in these outbreaks that were not officially notified until 1974 . Most of the imported cases had been infected in bordering districts of Uttar Pradesh and Bihar. The sources of the outbreaks included 12 districts in Uttar Pradesh and 9 in Bihar. One infected traveller came from the state of Maharashtra, although he was probably infected while travelling through Uttar Pradesh. All but 4 of the importations occurred in districts bordering on India.
Smallpox did not spread extensively, however. From the 35 importations, secondary spread to other villages occurred on only 7 occasions, one of these villages being the source of a further outbreak . The number of cases in each outbreak ranged from 1 to 38 with a mean of 8.3 cases, of which almost onethird (13 out of 43) were single-case outbreaks (Table 15.38).
In November and December 1973, the number of importations began to increase and in January 1974, 14 importations were detected, of which 8 were from Bihar and 6 from Uttar Pradesh (Fig. 15.31) . The number rapidly increased during May and then abruptly diminished, which was consistent with the seasonal decline in smallpox. In all, 180 outbreaks and 1549 cases occurred, of which 115 outbreaks were due to importations. As was the case in 1973, most of them (106 out of 115) occurred in districts bordering on India, the eastern districts of the Terai being the most heavily infected. In contrast to 1973, when the sources of infection were widely dispersed geographically, 68% of all importations during 1974 came from 5 heavily infected districts in Bihar. These districts, besides being among the most heavily infected in India, experienced severe food shortages in the spring of 1974 and, in consequence, many people migrated to Nepal.
Table 15.38: Nepal: number of outbreaks of smallpox, by number of cases in each outbreak, 1973-1975
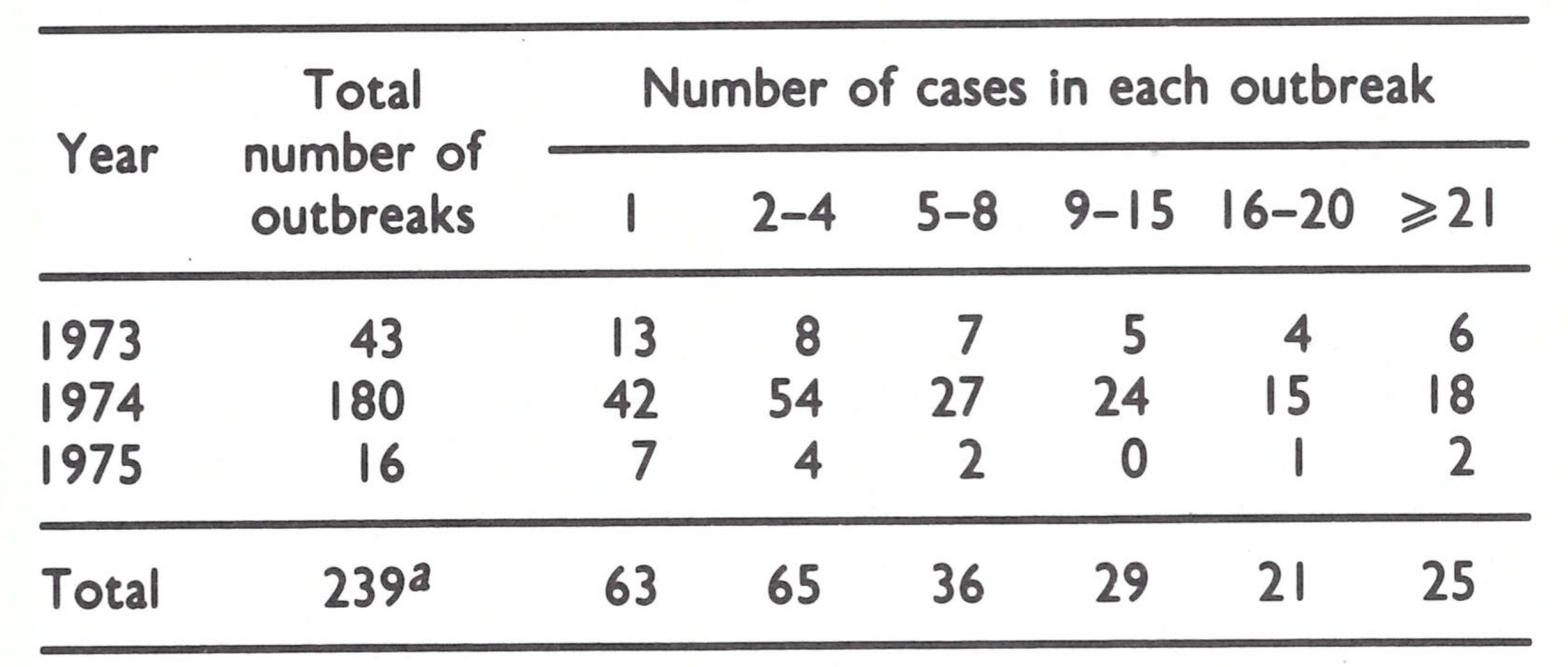
aData for 28 outbreaks not available.
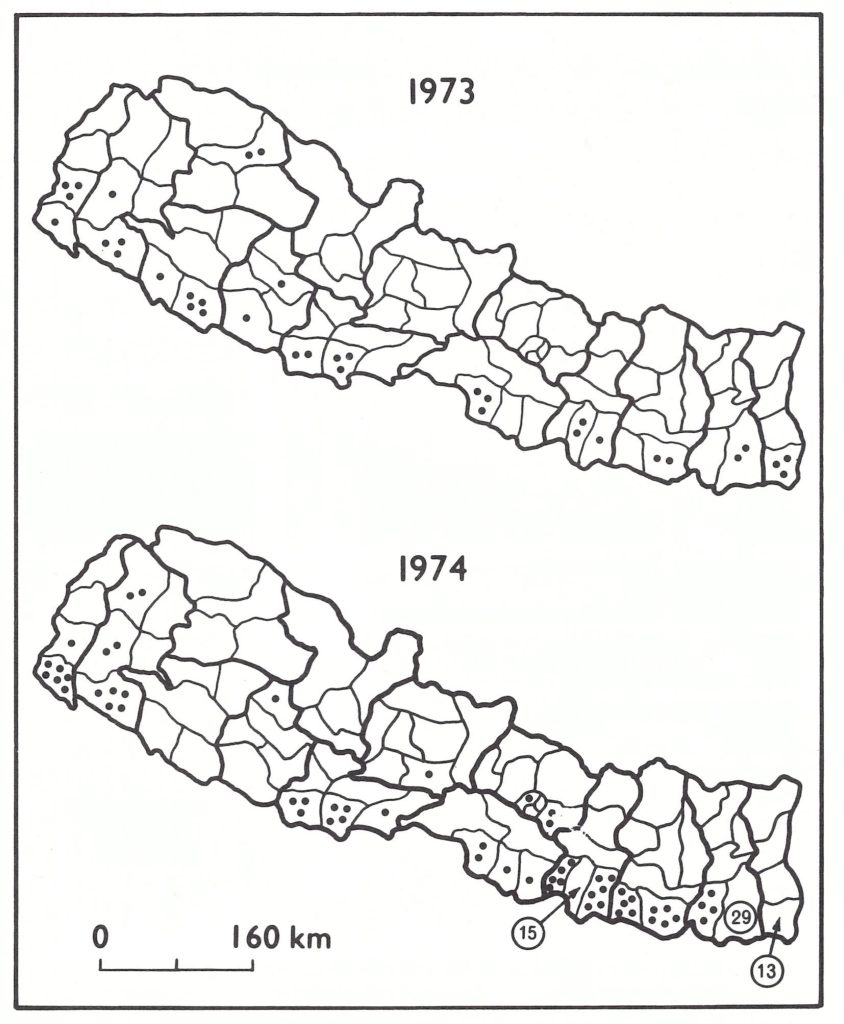
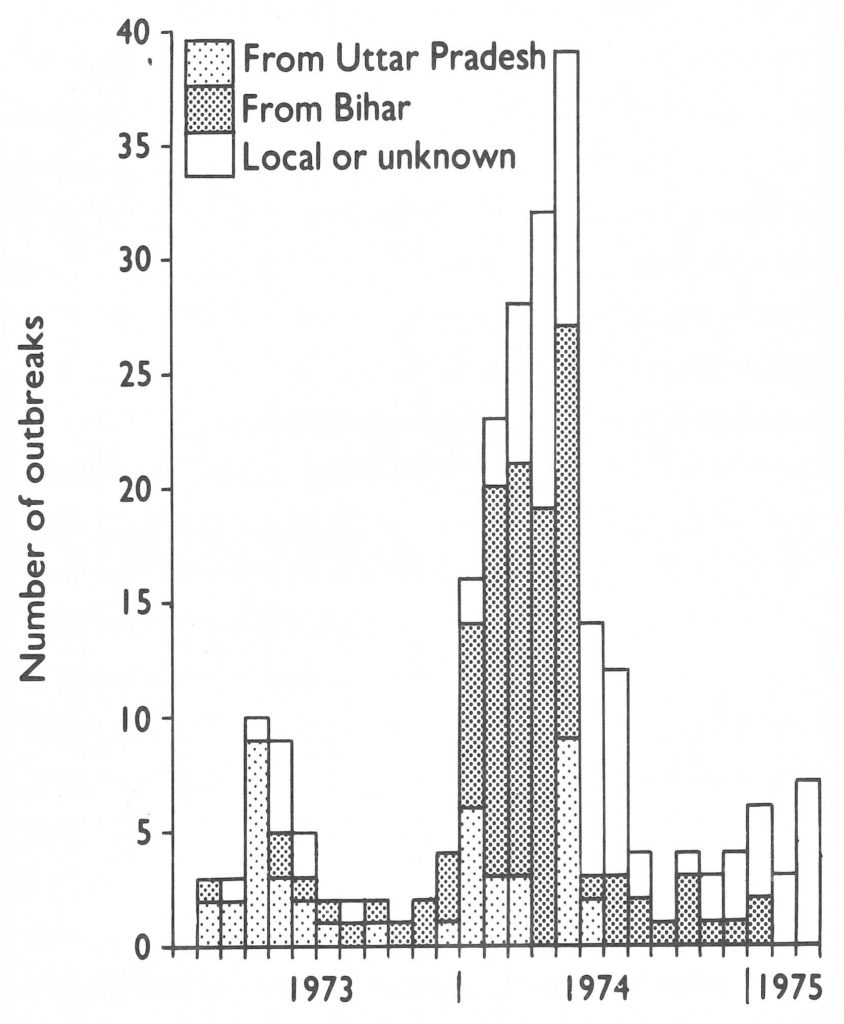
Fig. I5.30. Nepal: importations of smallpox, 1973 and 1974. Each dot denoted one outbreak.
Fig. I5.31. Nepal: number of outbreaks of smallpox, by source, by month, 1973-1975.
In early 1974, WHO arranged for the prompt, reciprocal cross-notification by telegram between India and Nepal of possible sources of infection in each country. Programme staff agreed to investigate every report of this kind and to confirm whether an outbreak had been found. Nepalese staff fulfilled this responsibility well and detected a number of outbreaks not previously known. In India, especially in Bihar, the system operated far less well: with numerous outbreaks and a poorly organized health system, many reports were ignored (WHO/SE/74.71, Shrestha et al.).
The increase in the number of outbreaks in Nepal taxed the resources for surveillance and containment, and a greater number of outbreaks began to result from local spread. Nineteen out of 57 such outbreaks (167 cases) occurred between February and September following 2 importations into the Kathmandu valley. Most were in the Newar ethnic group, who had resisted vaccination for religious reasons, and among whom it was a common practice for the relatives and friends to visit those who were ill with smallpox. Detection was also difficult because families did not report cases and sometimes hid the patients from health officials. Smallpox could therefore spread widely and containment was difficult.
A second problem area was in the western Terai, in which another ethnic group who also resisted vaccination had the custom of granting any wish to a child with smallpox in the belief that the child was possessed by the goddess of smallpox, Sitala mata. The child’s wish was frequently to be taken to see relatives or friends in other villages. In this area, smallpox spread unusually rapidly among groups of villages (SME/77.1, Shrestha et al.).
A third area which proved difficult was a south-eastern district, Morang, which experienced 29 importations in 1974 and 1 in 1975. It was the centre of jute production in the eastern Terai and contained the industrial town of Biratnagar. Numerous migrant labourers from India were attracted to the area and, in the autumn of 1974, because of food shortages in Bihar, many beggars from India arrived there . Quite a few of the migrant labourers and most of the beggars belonged to a tribal group which worshipped Sitala mata and resisted vaccination (SME/77.1, Shrestha et al.). The last chains of transmission began in December 1974 and January 1975, when 21 cases, primarily among beggars, occurred in a large market area, and from there smallpox spread to 6 nearby villages. More vigorous containment efforts were required; thus, in January, watchguards were posted at each infected house, as was done in India. In addition, systematic search and vaccination programmes were conducted over wide areas encircling the site of an outbreak. The system had been in use in many states of India for more than a year but in Nepal, in which the population was sparse, the containment of outbreaks had been less of a problem and, with fewer personnel, it had been impossible up to this time to adopt the Indian methods of containment. With the numbers of outbreaks diminishing both in India and in Nepal, a more elaborate scheme was possible . Resistance to vaccination was usually overcome with verbal persuasion although, on occasion, police accompanied the vaccinators to lend their authority. The number of outbreaks declined rapidly, and on 6 April 1975 the last cases occurred in Nepal.
Plate I5.20. Tibetan pilgrims being vaccinated in front of a Buddhist temple at Bodnath in the Kathmandu valley, Nepal.
Data regarding the age distribution of cases are available for 1286 of the 1921 cases which occurred in the period 1973-1975 (Table 15.39). Smallpox in Nepal occurred more frequently among older children and adults than in India. Less than one-third of all cases were in children under the age of 5 years and 29% were in persons over 15 years of age. The fact that more cases tended to occur in the older age groups in Nepal than in India probably reflected lower levels of vaccinial immunity throughout the population as well as a lower level of naturally acquired immunity due to the relative isolation of villages. Although villages in Afghanistan were comparable in their degree of isolation, variolation had been extensively practised there and many persons were immune as a result. In Nepal, however, the procedure had been largely discarded in recent decades.
Table 15.39: Nepal: age distribution of 1286 cases of smallpox, 1973-1975
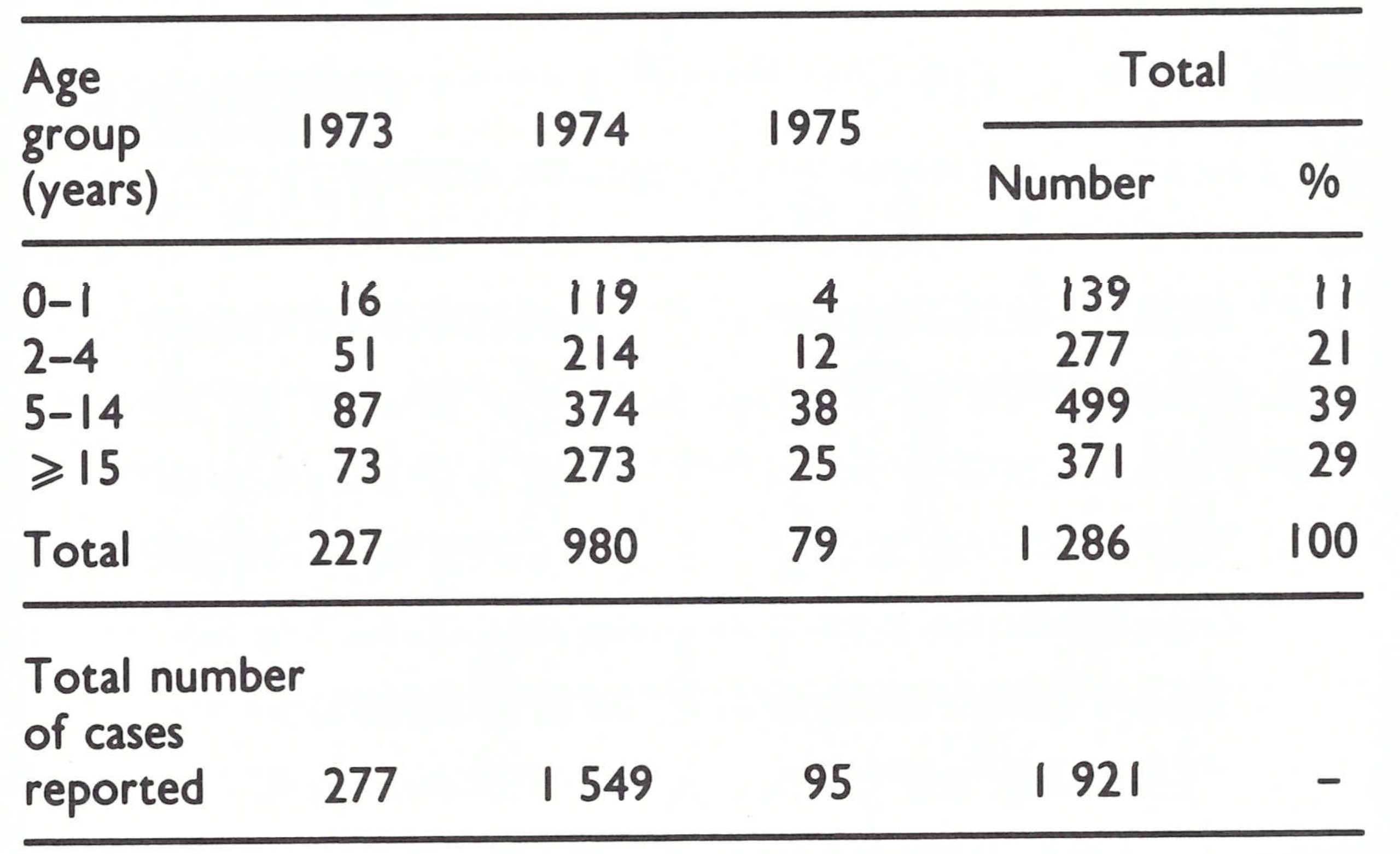
aData for 28 outbreaks not available.
Plate I5.21. A Nepalese vaccinator at work. The plastic holder for bifurcated needles in the foreground was designed and first made in Pakistan; the vaccine came from the USS.
Only 40 out of 1915 patients (2.1%) for whom data are available had been vaccinated before exposure—a far lower proportion than that reported from India. Several factors could account for this. In India, in which rotary lancets had long been in use, many apparent vaccination scars resulted from sepsis rather than successful vaccination. In Nepal, few had been vaccinated with the rotary lancet. Moreover, in the vast majority of instances the vaccination had been performed after 1967 so that vaccinial immunity was likely to be at a higher level.
The case-fatality rate was 21.5% (411 deaths among 1915 patients), a figure consistent with observations elsewhere in the Asian subcontinent.
At the time that the last case occurred, a reward of 100 rupees (US$9.50) was being offered to anyone reporting a case, and later this sum was increased to 1000 rupees. After 6 April 1975, however, no reported case was confirmed and no further cases were detected in subsequent laborious house-to-house searches.
Cost of the Programme
The total outlay on smallpox eradication by the government of Nepal and by WHO during 1962-1976 amounted to US$2 378 982, or just over US$0.15 per head of population. For the period 1972-1976, approximately 2% of the Ministry’s health budget was spent on the programme. The expenditure, however, was low compared with the cost of other programmes such as that for malaria control, on which, in the year 1976-1977 alone, Nepal spent more than US$4.5 million (SME/77.1, Shrestha et al .).
SIKKIM AND BHUTAN
East of Nepal in the Himalayan mountains lay 2 small sparsely settled political—entities Bhutan and Sikkim (Fig. 15.32). Bhutan, an independent monarchy, had an estimated population (in 1967) of 987 000, which was concentrated in the central and southern parts of the country and had contact through trade and travel with the inhabitants of Assam, West Bengal and Bihar in India. Between Nepal and Bhutan was the even smaller and less populous Indian protectorate of Sikkim (population in 1967, 196 000), which in 1975 became a state of India. Both areas shared a northern border with China, but few travellers crossed it.
Sikkim and Bhutan were both at risk of smallpox imported from India, although in neither area had it seemed likely that smallpox transmission could be long sustained among the population of the scattered mountain villages. Thus, until smallpox transmission was interrupted in India and Bangladesh, little support was provided by WHO to either Sikkim or Bhutan and, in fact, information about the smallpox situation in both areas was scanty until late in the Intensified Programme. With the interruption of smallpox in India, attention was directed to these and other more remote areas of the subcontinent to ascertain something of the history of smallpox and smallpox control in recent years and to confirm that transmission was not continuing.

Fig. 15.32. Bhutan and Sikkim and adjacent countries.
Sikkim
Cases of smallpox had been officially reported in Sikkim since 1954. In 1966-1967, 78 cases in all were recorded at a time of high incidence in northern India. After this, no further cases were reported until 1973, when an outbreak of 34 cases occurred in Gangtok, the capital, the first case having been infected in Darjeeling, West Bengal. A second outbreak, of 11 cases, occurred that year in 2 villages along Sikkim’s southern border, the source of infection again being West Bengal. No further cases were detected subsequently. Although reporting was undoubtedly very incomplete, the sporadic occurrence of smallpox was characteristic of an area in which importations were rare, and when they did occur, the disease did not spread easily.
Vaccination had been offered at the 4 district hospitals and 27 dispensaries, and the number of vaccinations relative to population, at least from 1967, was quite substantial (Table 15.40). That vaccinial immunity was comparatively high was confirmed during a vaccination scar survey in November 1975, which revealed that 79% of the population had scars and only 42 of 1495 persons (2.8%) had the facial pockmarks characteristic of smallpox (Basu et al.,1979).
Table 15.40: Sikkim and Bhutan: number of reported vaccinations, 1967-1975
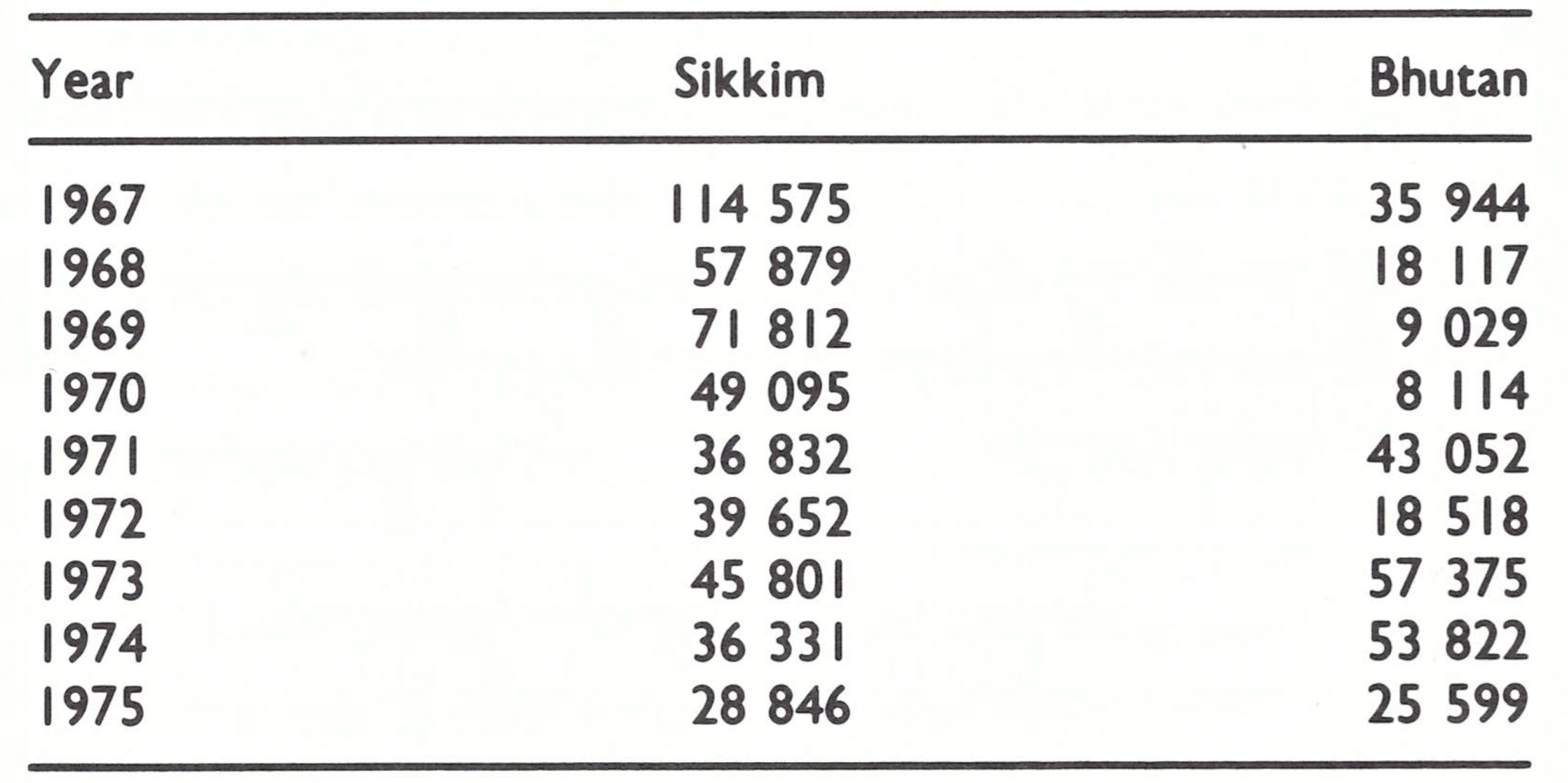
Bhutan
Information about Bhutan is less complete than for Sikkim. Until 1961 no health department had been established in the country. In 1964, the government created 19 posts for vaccinators, and increased the number to 25 in 1966, when a mass vaccination campaign was begun following an outbreak of 74 cases of smallpox in 1965- 1966 in the capital city of Thimbu. The outbreak had begun among Indian and Nepalese workers employed in a road-building project and then spread to the local population. The number of vaccinations reported to have been performed between 1967 and 1975, however, was small in relation to the population of 987 000 (1967 estimate).
After the 1965-1966 outbreak, only 4 further outbreaks were reported. In 1967, 2 outbreaks originating in Assam caused 14 cases. The third outbreak, of 6 cases, occurred in April 1973 in a village near the southwestern border with India, the initial case having been infected on a tea estate in West Bengal. The fourth outbreak, near the same border area, occurred in February 1974 and consisted of 3 cases, of which the first had been infected in Assam. Surveys conducted in 1976 to detect individuals with facial pockmarks, as well as interviews with village officials, indicate that other, unreported, outbreaks had occurred although none had produced more than a few cases. This was attributed in part to the fact that the villages Table 15.41. Bhutan: survey of vaccinial immunity and facial pockmarks in children, by age group, 1976 were scattered and isolated, and in part to the sensible traditional practice of isolating the patient and his family at the onset of illness in a place some distance away from the village . In these circumstances, the spread of smallpox was difficult.
Sample surveys conducted in Bhutan in the autumn of 1976 confirmed that vaccinial immunity among children was generally low, especially in the central and northern parts of the country (Table 15.41).
Facial pockmarks indicative of past smallpox were not seen in anyone under 15 years of age in central and northern Bhutan but were observed in 11 children in southern Bhutan. In northern Bhutan, where adults also were examined, only 10 out of 244 persons (4%) over 15 years of age had the facial scars characteristic of smallpox, the youngest being in his late twenties.
In addition to the 11 children with facial pockmarks detected in the village surveys of southern Bhutan, 3 others were discovered during surveys of schools in this area. Nine of the 14 had experienced illness in 1967 or later, and in each instance efforts were made to identify the source of infection; all were traced to India. One had contracted smallpox while living in Allahabad, Uttar Pradesh, before moving to Bhutan. The other 8 became ill in outbreaks resulting from importations (Table 15.42).
Summary
The surveys confirmed the belief that the continuing transmission of smallpox in these sparsely populated, isolated countries had not occurred recently-even in Bhutan, in which vaccinial immunity was low. The tradition of isolating the patient and his family, observed in Bhutan, undoubtedly contributed significantly to stopping transmission. This custom, interestingly, was current throughout most mountainous areas of Asia, but was much less frequently practised in the lowlands.
Table 15.41: Bhutan: survey of vaccinial immunity and facial pockmarks in children, by age group, 1976

Table 15.42: Bhutan: number of reported cases of smallpox and sources of outbreaks, 1966-1974
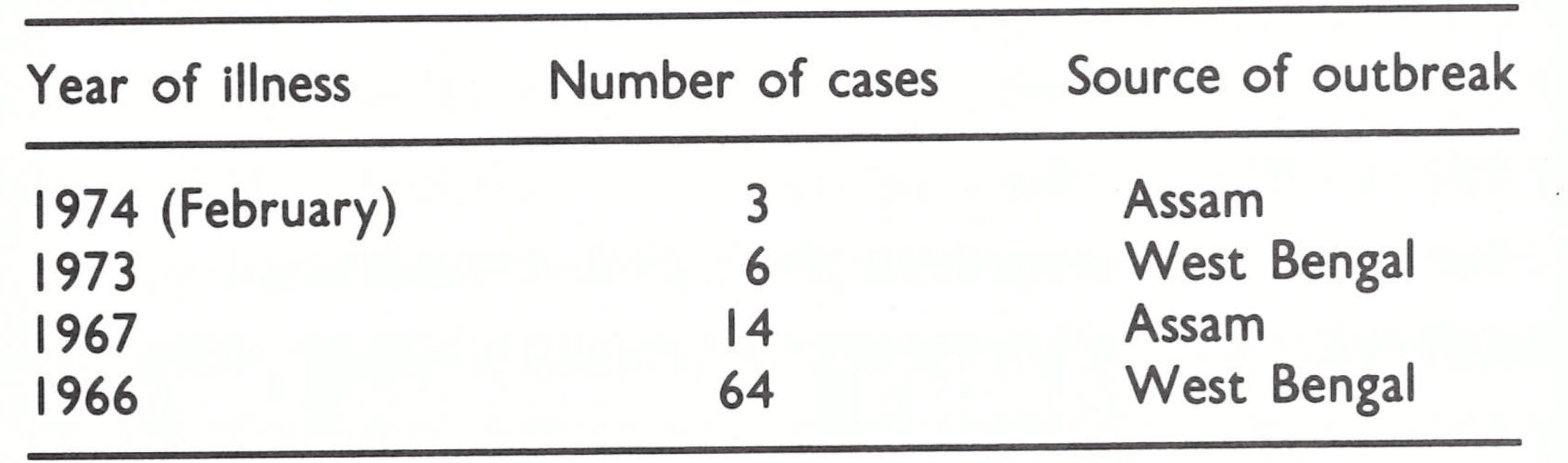
CONCLUSION
From 1961, when India first decided to embark on a national eradication programme, to 1975, when the last case was detected, the programme gradually improved—in the quality of vaccine employed, in the vaccination technique used, in the reporting system, in the extent and intensity of surveillance and containment and, most important, in the quality of supervision. To undertake a national programme in a country so vast, with a population so large and a bureaucracy so complex, was inevitably difficult. To modify and redirect such a programme proved no less difficult. The dimensions of the effort, which involved at least the parttime participation of more than 150 000 field staff and contact with more than 550 million persons, are hard to grasp or communicate.
India’s population, in 1967, constituted almost half of the total number of inhabitants of the endemic countries and, indeed, 15% of the world’s entire population. The central direction of the enormous national campaign then in progress rested with only 1 medical officer and a small staff of clerks. In the states, of which 7 each had a population of more than 40 million, direction was generally entrusted to a single medical officer, for whom, in most instances, smallpox eradication was but a part-time responsibility. Working in the cities, towns and villages, however, were tens of thousands of vaccinators, basic health workers, family planning and malaria eradication programme staff and many other categories of health worker. Many were responsible, experienced individuals, conscientious about their jobs and willing to work, but they were seldom provided with much in the way of support or stimulus or the necessary supplies to carry out their assigned tasks. New directions or new policies were more often than not impersonally communicated by official memoranda which frequently demanded the impossible for example: “All persons in the state will be vaccinated cent per cent [100%] during the next 12 months.” Vehicles stood idle and refrigerators remained inoperative for want of petrol or a few spare parts because the monetary resources provided had proved inadequate and/or fiscal procedures were so cumbersome as to prevent the disbursement of the funds. Vaccine deliveries were erratic and numerous batches were unfit for use because of the lack of refrigerated storage.
In the opinion of many, the solution to the disappointing level of productivity throughout the health sector was to eliminate special programmes such as that for smallpox eradication and to integrate all programmes into a unified primary health care programme in which each health worker would assume a multiplicity of responsibilities as a “basic health worker”. This was the panacea which had been repeatedly proposed by both Indian and WHO expert groups since the 1950s. It was the course of action recommended in 1966 as India’s intensive national vaccination campaign drew to a close, with smallpox almost as widespread as it was before the campaign had begun. In a number of states such integrated programmes were started in the mid- and late 1960s but the productivity of the workers was, if anything, even lower than it had been before.
Given the difficult problems and the paucity of senior leaders, the achievements of the smallpox eradication programme between 1967 and 1973 were remarkable. By the summer of 1973, smallpox transmission had been virtually interrupted in the southern states and was declining in the western states. It seemed that a comparatively modest investment in time by senior epidemiologists to help to develop surveillance and containment activities in the other states should rapidly succeed in interrupting transmission throughout India. The deplorable condition of the health services in some of these states, especially Bihar, Assam and Uttar Pradesh, was not then comprehended, nor were the coming disastrous epidemics anticipated. However, the administrative changes which were made in the summer of 1973 had profound consequences in that they permitted the vast resources of health man power in India to be utilized effectively and gave scope to the imagination and problemsolving abilities both of senior staff and of field workers. With the active support of the Minister of Health and Family Planning and an adequate complement of senior Indian and WHO staff to travel to the field to explore alternative solutions to problems, to instruct, to assess and to measure results, field staff took an increasing interest in the programme. Knowing what should be done, they themselves sought new solutions. The onerous fiscal constraints were ultimately resolved through the use of the flexible imprest accounts provided by WHO. With the most senior Indian staff, initially Dr Diesh and later Dr Sharma, not only travelling to state capitals but also visiting field staff in districts and villages, the example was set for otherwise desk-bound lower-level supervisory staff to do likewise. By doing so, they motivated and inspired staff at all levels.
The strategy adopted for the programme also played an important role, the country being divided into 3 different areas, with the objective of preventing smallpox from reestablishing itself in smallpox-free states, of eliminating the few remaining foci in states with a low incidence, and of conducting a major offensive in the 4 states with the highest endemicity. Each of the states thus had specific goals and programmes appropriate to those goals. Measurable indices of progress in achieving eradication were important. These were identified first in terms of the numbers of cases of smallpox occurring each week and then in terms of the numbers of outbreaks in which a case had occurred during the preceding 4 weeks. In the last year of the programme, other standards were formulated to measure the quality of surveillance, of containment and of outbreak investigation. With specified and achievable objectives, all personnel could assess progress in their own area, be it a primary health care centre, a district or a state. Monthly meetings and regular surveillance reports served as refresher training, permitting new approaches to be introduced and serving as a stimulus to all concerned.
The problems that emerged after the intensive campaign was launched in the summer of 1973 were far greater than anyone had expected, but the conviction of the senior leadership and the programme’s momentum were sustained in the face of often hostile criticism by some senior Indian and WHO officials, natural calamities of flood and famine, civil disorder and strikes, and the inevitable bureaucratic inertia. The programme improved so rapidly that the transmission of smallpox was interrupted in India less than 20 months after the first search had begun. Because of the quality of the programme and the confidence achieved through assessment of its merits, it was possible only 3 months after the occurrence of the last case to celebrate India’s freedom from smallpox on India’s Independence Day in August 1975. In no other country up to that time had it been possible to feel so confident so soon. However, over the next 2 years, the programme staff conducted the most elaborate and extensive search programme of any in Asia to confirm for themselves and—just as important—to convince an incredulous world community that India was truly free of smallpox.
What many failed to appreciate was that the achievement was not the product of a special army dedicated to smallpox eradication, but one in which existing health staff of all types participated actively in managing and executing a programme with measurable objectives. When eradication was certified in 1977, only a handful of long-term smallpox vaccinators and a few senior staff remained to be reassigned to other programmes.
As had been expected, smallpox in Nepal, Bhutan and Sikkim reflected the experience in the neighbouring densely populated Indian states. In Bhutan and Sikkim, the only special activities undertaken, aside from routine vaccination programmes, were those concerned with certifying the absence of smallpox. In Nepal, far more populous and epidemiologically more closely related to India, a special programme was required.
The programme of vaccination and later of surveillance and containment in Nepal represented its first national health programme, and one which extended to all parts of this mountainous rugged country. Since travel throughout much of Nepal was of necessity by footpath, and health facilities were nonexistent in many parts of the country, district smallpox supervisors played a vital role. With encouragement from national staff and repeated refresher training, most of these local workers responded well to their responsibilities. The first national disease reporting system was established, and vaccination—all but unknown in most of the country in 1967—reached more than 90% of the population within a period of little more than 5 years. It was an impressive achievement, especially in view of the fact that the ratio of programme staff to population was at best 1 to 20 000. Nepal’s successes were different from India’s but no less remarkable.
The programme in India was slow to gain momentum and undoubtedly eradication might have been attained far sooner if an adequate complement of well-motivated senior supervisors had been provided at an earlier stage. In all probability, the greatest catastrophe of the Intensified Programme would have been averted—namely, the 1971 epidemic in the Calcutta Salt Lake Refugee Camp, which led to the reintroduction of smallpox into Bangladesh and to tens of thousands of deaths.