Chapter 16:
Bangladesh

INTRODUCTION
The last case of smallpox in Asia and the last case of variola major, the more severe form of the disease, occurred in Bangladesh (Fig. 16.1) on 16 October 1975. It might not seem surprising that Bangladesh was the last Asian country to eliminate smallpox. Of all the countries of the world, it was one of the poorest and most densely populated. However, Bangladesh (East Pakistan until December 1971) had already succeeded once in interrupting transmission 5 years earlier, in August 1970. The achievement had been remarkable and unexpected, occurring just 8 months after limited resources had been diverted from an extensive mass vaccination campaign to a simple surveillance and containment programme. Most observers believed that other undetected foci would 807 become apparent during the subsequent dry season, from October 1970 to the end of March 1971, when more rapid transmission occurred. However, 6 months went by without further cases being found. Suddenly, in March 1971, a tragic and violent civil war broke out, 10 million refugees fled to India, and health programmes and organized surveillance activities virtually ceased. However, up to the end of December 1971, no smallpox patients were admitted to the infectious disease hospitals, no cases were reported by health staff and none were detected among the continuing flood of refugees entering India.
Many of the refugees who fled to India were housed in special camps, hurriedly set up in areas near the border. They were supposed to have been vaccinated on arrival, but in several camps, including the largest, near Calcutta, few were, in fact, vaccinated. Smallpox broke out in November 1971 and spread rapidly. Because cases were incorrectly diagnosed, nothing was done to contain the epidemic until late in January 1972.
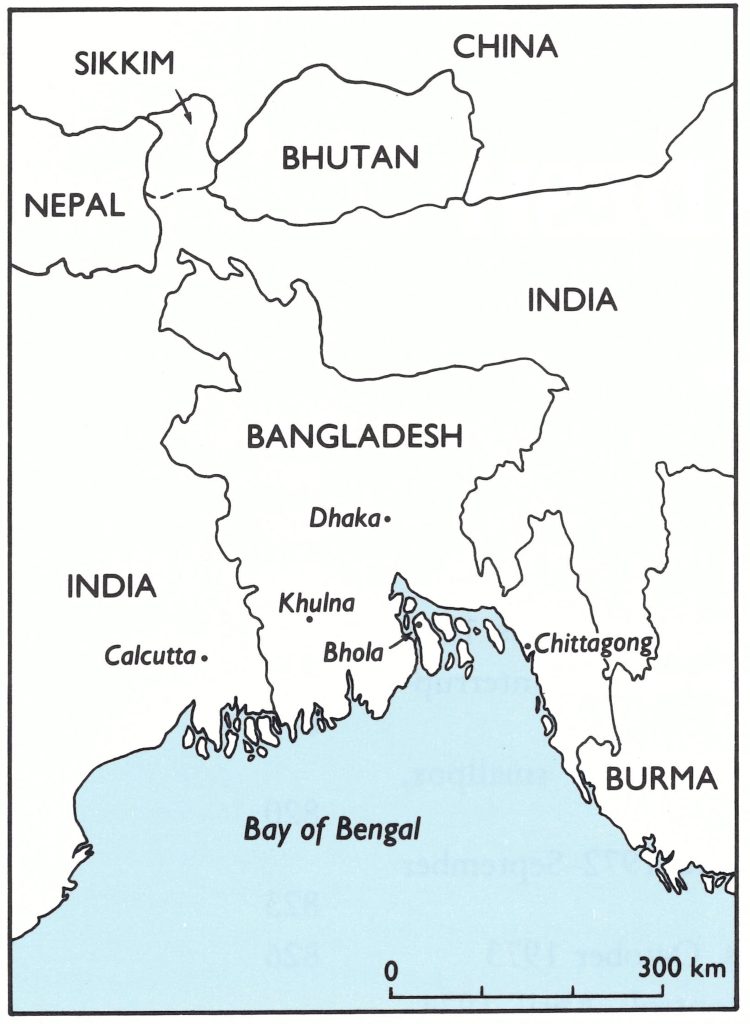
Fig. 16.1. Bangladesh and surrounding countries.
Meanwhile, on 16 December 1971, Bangladesh became an independent state, and every day thereafter thousands of refugees, many of whom were infected with smallpox, began to return home. This mass migration took place at the beginning of the season of highest transmission. The health service, devastated by civil war, could not cope with the situation; epidemic smallpox swept through temporary refugee camps, cities and rural areas.
The eradication programme was reconstituted and strengthened, but, despite far more intensive efforts than had been made in 1970, transmission persisted year after year between 1971 and 1975, as one disaster followed another. At different times, famines, floods, civil disorder and the forcible displacement of urban slum dwellers caused hundreds of thousands of people to flee their homes. The national health services were reorganized at a critical time, in 1973, seriously hampering field activities; and national leaders periodically redirected the smallpox eradication programme towards mass vaccination campaigns.
In the spring of 1975, a greatly strengthened although frustrated and demoralized staff made one more concerted effort to stop transmission and ultimately succeeded in October 1975, when the last case occurred.
During its final year the eradication programme in Bangladesh utilized and further developed methods that had been elaborated over the preceding 8 years of the Intensified Smallpox Eradication Programme and employed experienced personnel from many other countries. The national programme is thus of special interest. However, if the refugees in the camps in 1971-amounting to perhaps 300 000 persons-had been vaccinated, this chapter would have been very brief; 223 000 fewer cases of smallpox would have occurred and more than 40 000 deaths would have been averted.
Of the national smallpox eradication programmes, that in Bangladesh is one of the better documented; much of the material for this chapter is drawn from a book by Joarder et al. (1980), The Eradication of Smallpox from Bangladesh. The book also describes the eradication staffs experience in the practical application of techniques for surveillance and assessment in other health programmes.
BACKGROUND
The richly fertile country of Bangladesh lies at the delta of three of Asia’s great rivers—the Ganges, the Brahmaputra and the Meghna. More than nine-tenths of the country is less than 15 metres above sea level, and as much as one-third of the agricultural land is flooded during the June-September monsoon. In 1967, Bangladesh had a population of some 62 million, one of the fastest growing and with the highest density of any major country (428 persons per square kilometre). The central and southern parts of the country were the most densely settled (Fig. 16.2). Even in areas in which vaccinial immunity was comparatively high, the number of susceptible individuals per square kilometre was greater than in most endemic countries.
There was considerable population movement throughout the country. Nearly 95% of the people lived in rural areas, but 30% were landless and even those with some land of their own often sought part-time work elsewhere as tenant farmers or labourers. At planting and harvest times, hundreds of thousands of people travelled up to 200 kilometres in search of work. Although there were only 3 cities in 1974 with populations of more than 300 000—Dhaka (1.8 million), Chittagong (970 000) and Khulna (480 000)—all cities and towns had large unenumerated transient populations entering and leaving each day. A study in Dhaka in 1976, for example, showed that more than 110 000 persons passed daily through its main points of entry. However extensive the movement of people, village and family ties remained especially important in this traditional Muslim society, so that those who fell ill frequently travelled long distances to be cared for in their home villages by their families. In this setting, the transmission of smallpox from urban to rural areas was rapid and widespread.
Undernutrition and malnutrition were common even when harvests were good. In 1962-1964, it was estimated that the residents of only 54% of rural households were adequately fed, and by 1975-1976 this proportion had decreased to 41%. Because of the precarious nutritional situation, even a small decrease in food supplies had a disproportionately heavy impact, causing hundreds of thousands of people to migrate from one area to another, many to the cities. At such times, smallpox spread with facility.
Travel by land was time-consuming and difficult, making it hard to supervise the programme effectively and to transport supplies to smallpox eradication staff in the field. A network of 4000 kilometres of all-weather roads radiated from Dhaka to district towns but major ferry crossings were encountered frequently and roads were often damaged or washed out by monsoon rains. Hundreds of thousands of river-boats provided transport for many travellers; although they were slow, they were inexpensive and permitted extensive population movement, especially during the monsoon season.
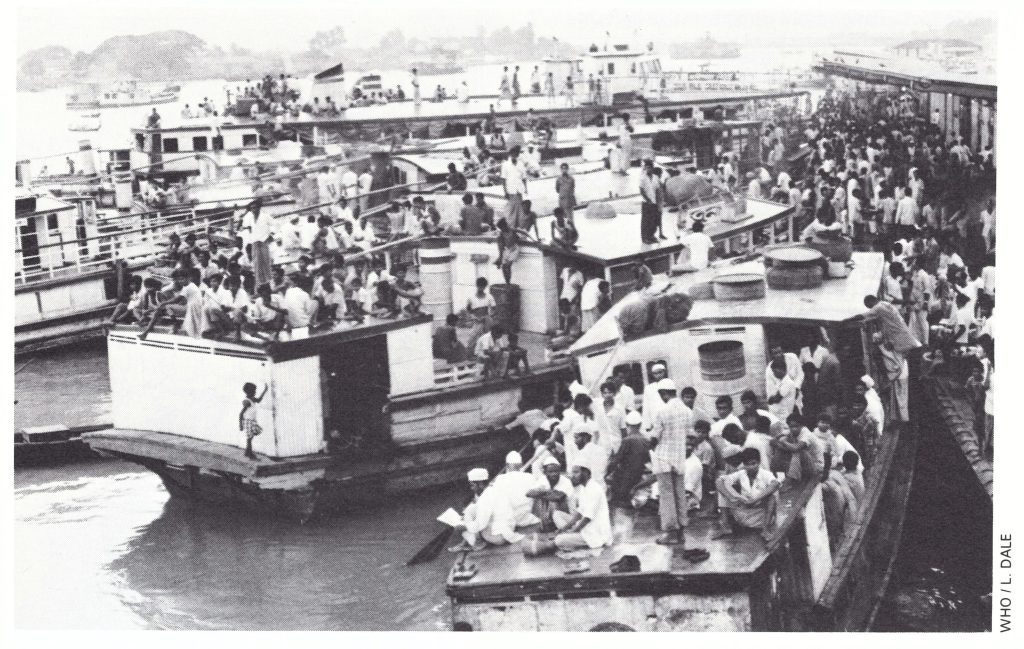
Plate 16.1. RA: Lekie Botee (b. 1930), the first Zairian co-director of the smallpox eradication programme in Zaire; when, later, he became Director-General of Health Services of Zaire he continued to play an active role in the programme. B: Pierre Ziegler (b. 1925), WHO co-director from 1968, was instrumental in redirecting operations and in establishing a management system
The various administrative units, to which reference is made later, as well as their average area and population size, are enumerated in Table 16.1. Division and district boundaries are shown in Fig. 16.3.
Each village was composed of a number of baris. A bari usually corresponded to a household, but it also referred to a compound occupied by an extended family and sometimes included the houses of servants and other employees in the wealthier families.
In each district and subdivision, civil surgeons were responsible for all curative and preventive services except for the malaria eradication programme, which operated as an autonomous activity until late 1973. One or two medical officers were usually assigned to each than, the basic administrative unit, but preventive measures were the responsibility of a sanitary inspector, who supervised some 5-10 government health assistants. Each government health assistant—a category of staff usually recruited locally—was in charge of a union. Many of the government health assistants had had no more than an elementary-school education; none were well paid or adequately supervised. Until late 1973, the malaria eradication programme, one of the best of its kind in Asia, had an independent but roughly parallel structure. Its staff, however, was of a generally better quality, received higher pay and was far more reliably supervised.
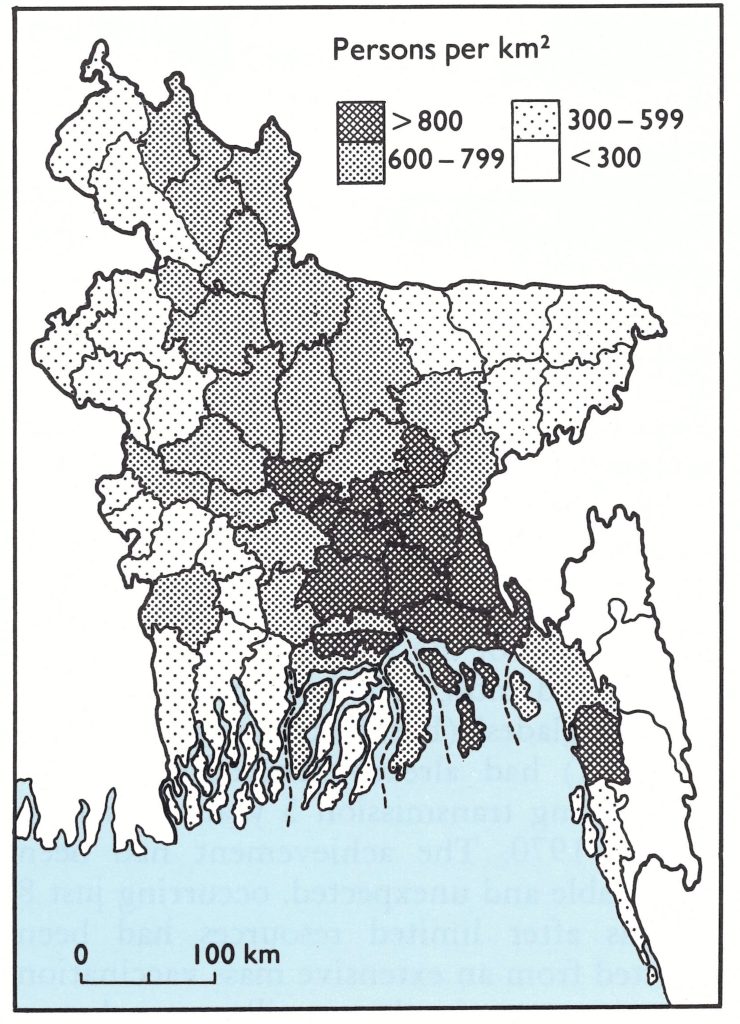
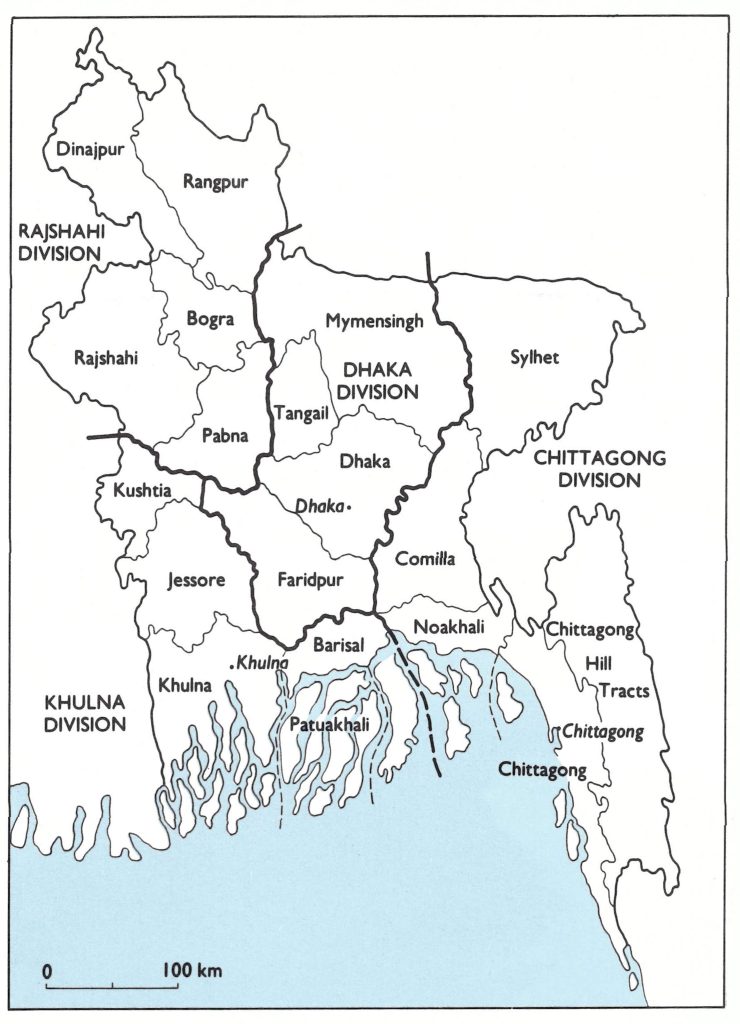
Fig. 16.2. Bangladesh: population density by subdivision in 1967.
Fig. 16.3. Bangladesh: divisions and districts as of 1972.
Table 16.1: Bangladesh: administrative units in 1972a
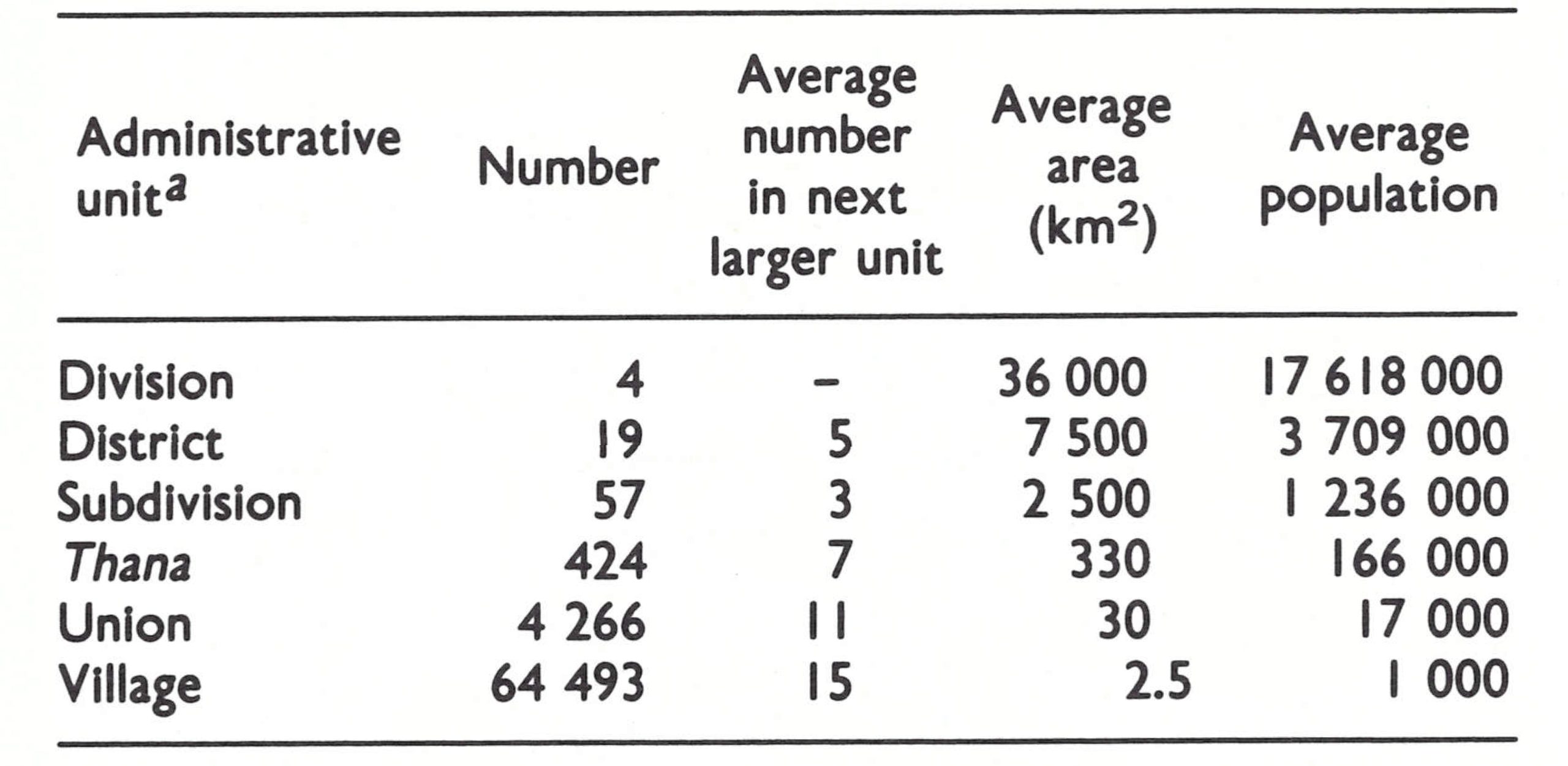
a in 1983-1984, the structure was changed so that each Subdivision was designated a District and thanas were renamed upazilas.
SMALLPOX AND ITS CONTROL BEFORE 1968
As elsewhere in the Indian subcontinent, only the variola major variety of smallpox was known to have occurred, and this fertile, heavily populated delta area may well have been one of the earliest endemic areas in Asia. Until late in the 19th century, protection was afforded primarily by variolation, performed by indigenous practitioners. Vaccination, with liquid vaccine produced in Calcutta, was introduced in 1860 in areas near Calcutta and in certain of the district towns of what is now Bangladesh. In 1874, the authorities decided that variolation should be abolished and they encouraged the variolators to replace variola virus by vaccinia virus. By the turn of the century, as vaccination became more widely available, variolation ceased altogether. In 1947, the production of liquid vaccine began in Dhaka, and up to 1961, vaccination was performed throughout the country by government-paid vaccinators supervised by health inspectors in each thana. The extent of vaccinial immunity is unknown but with only the thermolabile vaccine available in this subtropical area, many vaccinations were probably unsuccessful.
Smallpox was known in Bangladesh as boshonto, the Bengali word for spring, the season of highest incidence of the disease. As in India, major epidemics were recorded every 4-7 years. After 1947, the year in which Pakistan became independent, major epidemics were recorded in 1951 and 1958 (Fig. 16.4), the latter being so extensive that assistance for its control was sought from other countries. In all, 79 060 cases with 58 891 deaths were reported that year, a figure which, because of poor reporting, was undoubtedly one-tenth or less of the actual total. One of the groups providing assistance was a team from the United States Communicable Disease Center (later, the Centers for Disease Control), Atlanta. This team estimated that 60-70% of the people had vaccination scars but could find no correlation between the level of vaccinial immunity and the intensity of the epidemic in different areas. The team members were impressed by the size of the epidemic and the density of the population and suggested that “the number per square mile of unvaccinated persons would be a better index of the susceptibility . . . than the index that is ordinarily used, the proportion of the population that has been vaccinated” (Usher, 1960). They concluded that the “feasibility [of global eradication] under presently existing circumstances is dependent on the likelihood of success in countries where eradication is likely to be most difficult to accomplish and the obstacles greatest. One of these countries is Pakistan . . .” (Usher, 1960). As an outcome of the epidemic, it was decided to develop a laboratory in Dhaka capable of producing freeze-dried vaccine, but substantial quantities of such vaccine did not become available until 1966.
Resolution WHA12.54, adopted by the Twelfth World Health Assembly in 1959, called on all countries to join in a mass vaccination programme with the aim of eradicating smallpox. This initiative was enthusiastically supported by the Pakistani government and a campaign commenced in East Pakistan in 1961. The intention was to vaccinate the entire population within two or three years.
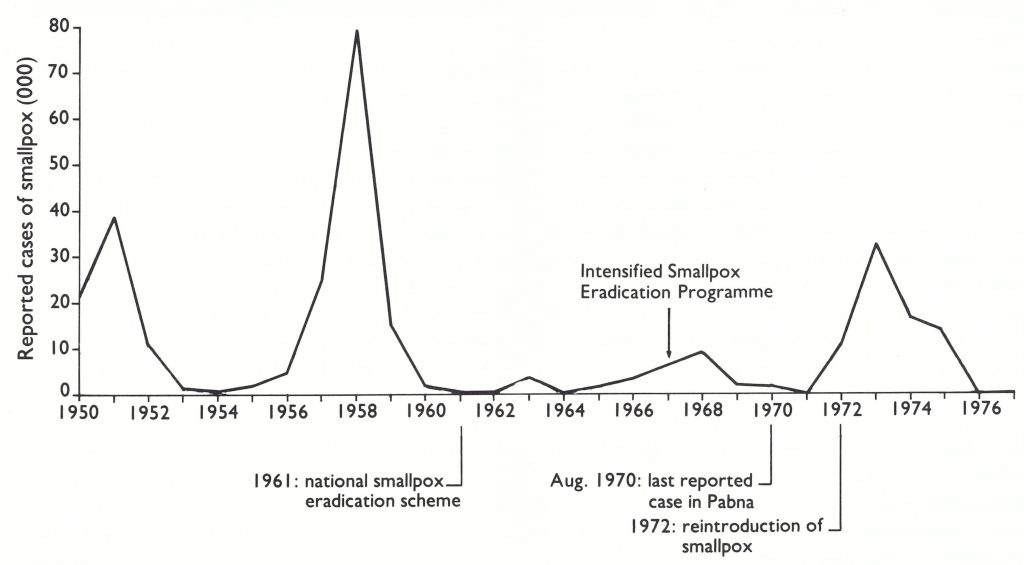
Fig. 16.4. Bangladesh: number of reported cases of smallpox, by year, 1950-1977.
During the 3-year period 1961-1963, 72 million vaccinations were reported to have been performed and, during the succeeding 3 years, 68 million more—in all, more than twice the population of the country (Table 16.2). From field observations in 1967 and 1968, it was apparent that the reported number of vaccinations was greater than the number actually performed and, as was the case elsewhere in Pakistan and in India, the most accessible persons, such as schoolchildren, were vaccinated repeatedly while others were not vaccinated at all. Nevertheless, vaccinial immunity in the population undoubtedly reached higher levels than ever before. Only 69 cases of smallpox were reported in 1964, and 316 in 1965. In 1966, the number of cases again increased, reaching 3207 that year and 6648 in 1967.
During the summer of 1967, epidemiologists who had conducted studies of smallpox in West Pakistan (see Chapter 14) decided to undertake similar studies in rural East Pakistan. A combined team from the Pakistan Medical Research Centre in Lahore, the Cholera Research Laboratory in Dhaka, and WHO studied the epidemiology of smallpox in an area in which cholera vaccine trials were then in progress. These investigations, along with those in West Pakistan, were the most comprehensive epidemiological studies conducted during the entire global eradication programme and provide an interesting overview of the smallpox situation at that time in one subdivision of the country (Thomas et al .,1971a,b).
The area studied was Matlab Thana, Comilla District, 65 kilometres from Dhaka ; it Table 16.2 . Bangladesh : population and number of reported vaccinations and number of reported cases of smallpox, 1961-1976a a Population estimates from United Nations (1985). included 132 small rural villages (population, 113 000) scattered over approximately 200 square kilometres . Vaccinators had been employed in the district since 1930, travelling from village to village to vaccinate newborn children and revaccinate others, using the rotary lancet and liquid vaccine. Comilla District had served as a pilot programme area for the 1961-1963 mass vaccination campaign and, for this operation, additional vaccinators had been employed. Therefore, as the investigators noted, vaccinial immunity among individuals over 5 years of age may have been better than in other parts of East Pakistan.
In May 1967, experienced interviewers, employed in the cholera vaccine trials, visited each house throughout the area to assess vaccinial immunity ; in all, 103 539 persons were examined. In July, each house was again visited in an effort to identify, by means of an interview, all cases which had occurred between 1 July 1966 and 30 June 1967.
Of the people examined, 80.8% had a vaccination scar, the largest proportion of the unvaccinated being among children under 5 years of age (Table 16.3). This age group should have been vaccinated during the “maintenance vaccination” campaign, but, as is apparent, that programme was far from satisfactory.
Thirty different outbreaks, occurring in 27 villages, with a total of 119 cases, were identified. Of these, only 5 outbreaks and 13 cases had been officially reported but, as in West Pakistan, the reported outbreaks included 5 of the 6 largest, in which 54 cases had occurred. In 7 outbreaks, special vaccination control campaigns had been conducted by government vaccinators but with little apparent effect.
Table 16.2: Bangladesh: population and number of reported vaccinations and number of reported cases of smallpox, 1961-1976a
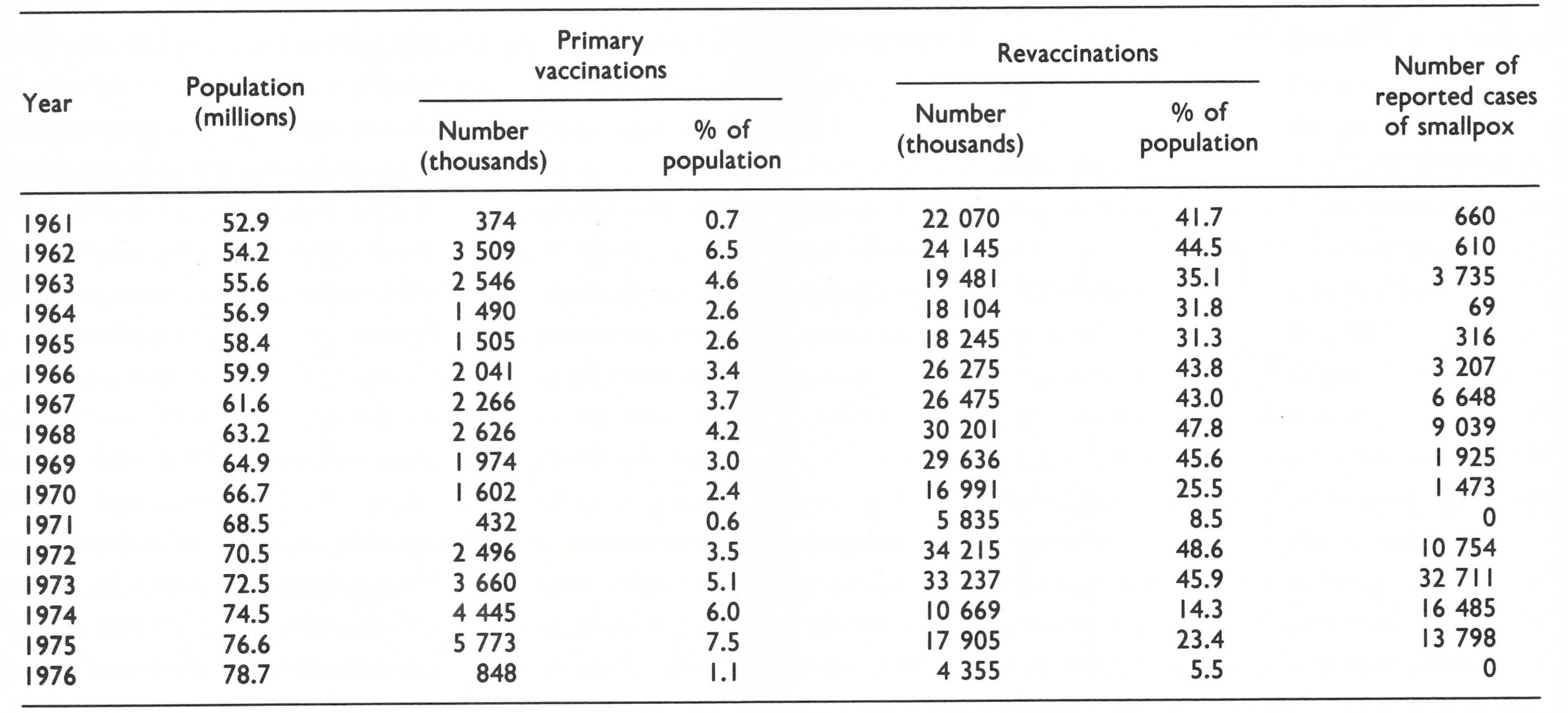
a Population estimates from United Nations (1985).
Table 16.3: Matlab Thana study area, Comilla District : vaccination scar survey, 1967, by age groupa
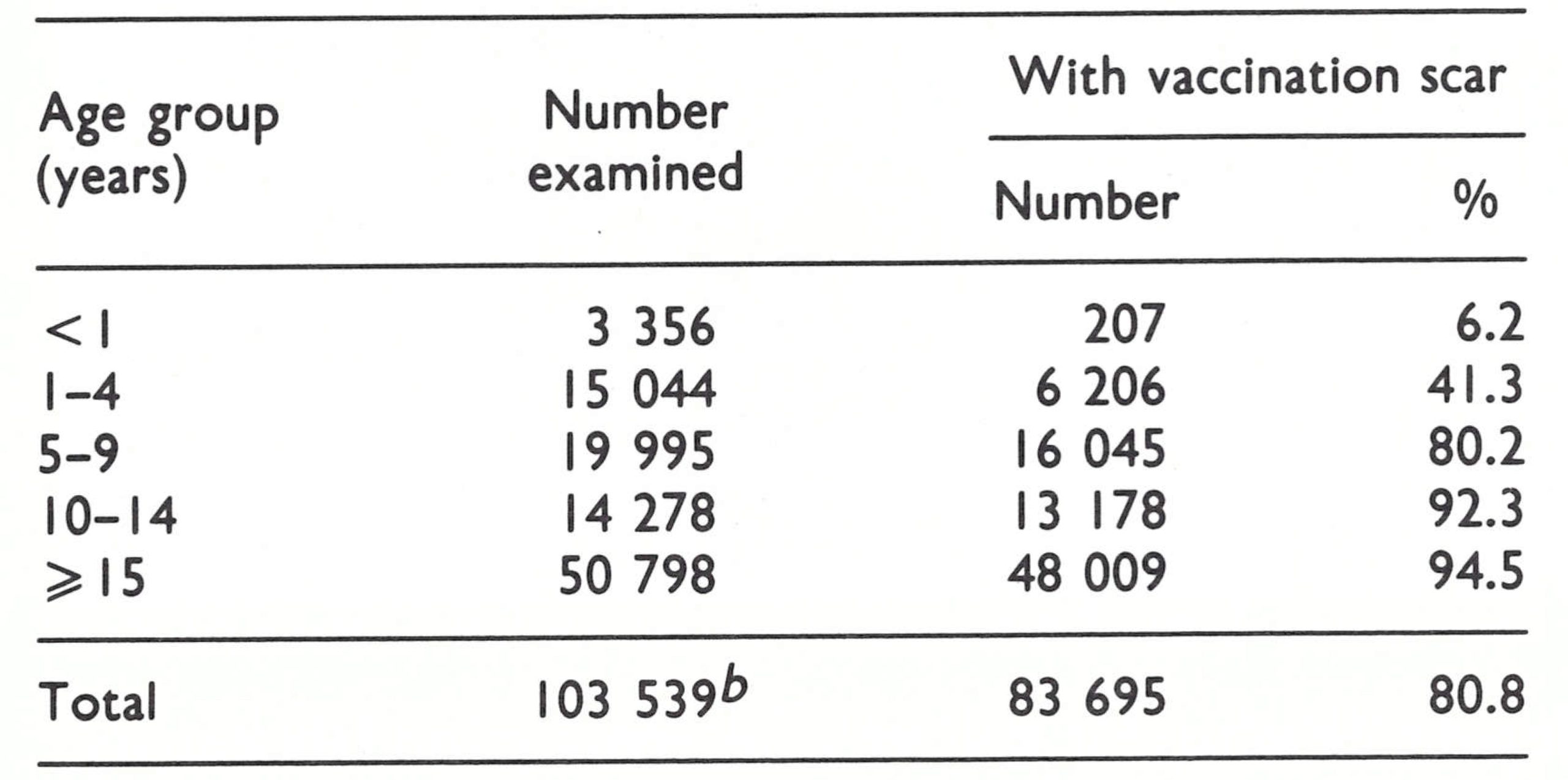
a From Thomas et al. (1971 a,b).
b Includes 68 persons of unknown age of whom 18 were without a vaccination scar.
The age distribution and case-fatality rates (Table 16.4) were similar to those observed elsewhere in Pakistan and in India. Thirtyfour (29%) of the cases were in children under 5 years of age, 55 (46%) in individuals aged 5-19 years and 30 (25%) in those aged 20 years and over. Thirty-four of 111 persons (31%) of known vaccination status had previously been vaccinated, all except 6 of them being 10 years of age and older . With data available regarding the vaccination status of the population as a whole, it was possible to calculate vaccine-efficacy ratios by age based on vaccination at some time in the past (WHO/SE/69.11, Thomas et al.). The ratios showed 94-96% protection for those aged up to 14 years; 89% for those aged 15-24 years ; and 74% for those aged 25 years and more. The ratios were remarkably high, although not so great as those found in South America, in which only the mild variola minor variety of smallpox was present.
The epidemiological pattern of spread was of special interest. Thirteen of the 30 outbreaks consisted of only a single case, and in 9 others the disease was not transmitted beyond the initially infected bari. Moreover, 24 of the outbreaks terminated after less than 2 generations of spread . Despite the density of population and a lower level of vaccinial immunity, smallpox tended to spread less rapidly and to remain more localized than in West Pakistan. The sources of 22 outbreaks were identified. All but 1 of the sources were outside the study area and 15 of the 22 originated in cities of 100 000 inhabitants or more, in which only 5% of the population of the province resided. In this study population, continuing transmission of smallpox from village to village had not occurred and, in fact, no cases whatever were detected whose onset took place between September and December 1966.
The investigators concluded that it was even more important in East than in West Pakistan to eliminate smallpox from urban areas, an objective which, if achieved, would prevent a high proportion of rural cases. Moreover, it appeared that most outbreaks in rural areas might be contained simply by vaccinating the inhabitants of the affected and neighbouring baris rather than the population of the entire village. Noting the high vaccine-efficacy ratios, the investigators recommended that a continuing programme of maintenance vaccination should concentrate on vaccinating those who had never been previously vaccinated, especially children aged 5-14 years not attending school and landless labourers working in urban areas—identified as the two groups most likely to transmit smallpox from place to place.
For a settled population and one which was as well vaccinated as that of Matlab Thana, the recommendations were sound and in 1970 the programme would substantiate their validity. However, when mass migrations of refugees took place, as happened repeatedly after the country became independent, and when smallpox outbreaks occurred in areas in which vaccinial immunity was low, more extensive containment measures were found to be required.
Table 16.4: Matlab Thana study area, Comilla District: number of reported cases of deaths from smallpox and case-fatality rates, 1967, by age groupa
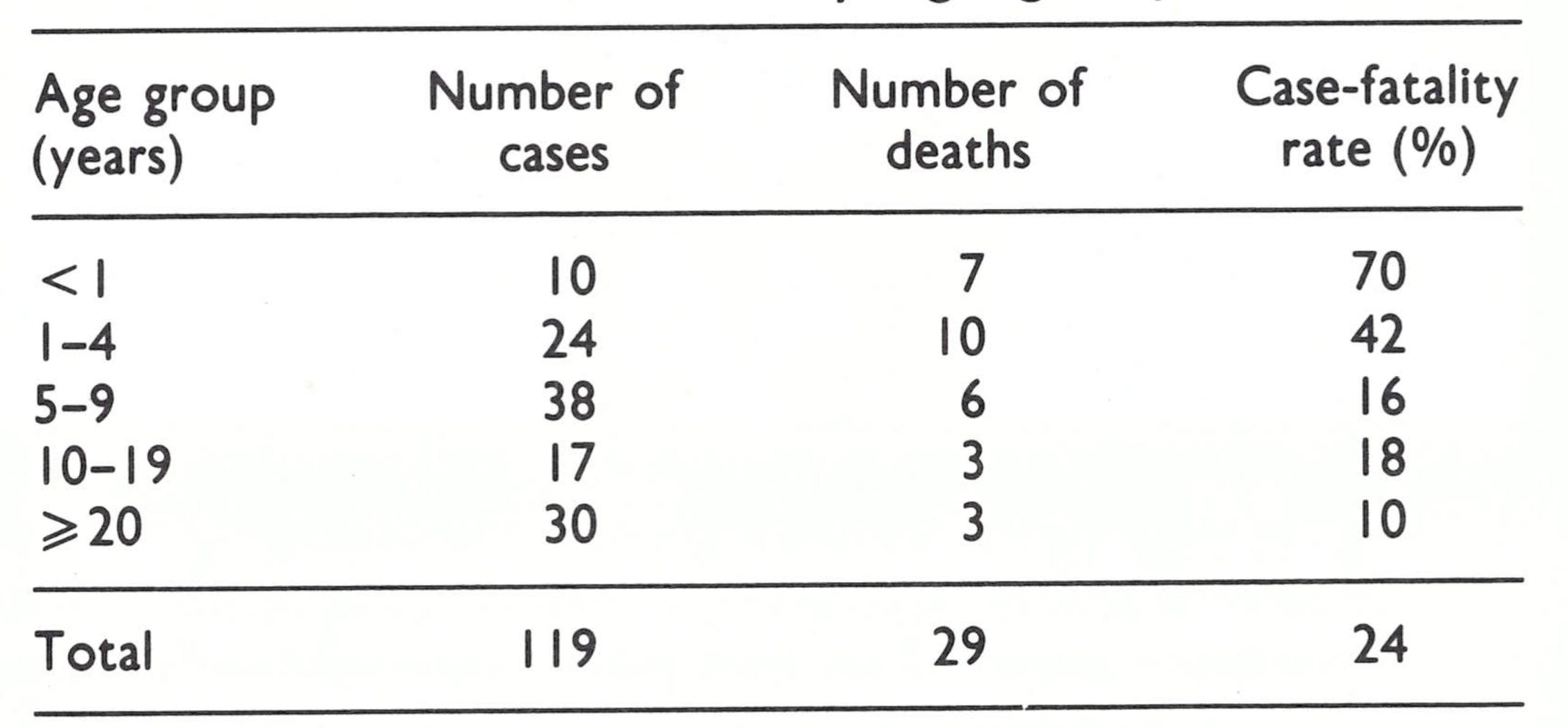
a From Thomas et al. (1971 a,b)
THE WHO-SUPPORTED ERADICATION PROGRAMME BEGINS, 1968
In July 1967, Dr Ehsan Shafa, the regional smallpox adviser from the WHO Regional Office for the Eastern Mediterranean, and Arita held meetings with government officials in Islamabad, the national capital, and Dhaka, the capital of East Pakistan, and developed a draft plan of operations. The government agreed to the plan in principle and submitted a letter to the WHO Regional Office requesting assistance. This letter permitted funds to be obligated and supplies to be procured well before a more formal agreement was signed by WHO and the government, inevitably a long process. (The agreement was not, in fact, signed until 26 April 1968.)
The principal component of the plan was a mass vaccination campaign, as in West Pakistan. It was thought that a well-organized campaign and concurrent assessment of the results, coupled with the use of freezedried vaccine and bifurcated needles, would achieve a higher level of vaccinial immunity than had previous campaigns. Provision was made for surveillance teams in areas in which mass vaccination campaigns were in progress, but the concept of a national surveillance programme did not take shape until 1969. Although the findings and recommendations of the research team were available to national and WHO staff by early 1968, they were almost wholly ignored in the implementation of the national programme.
The plan called for a special full-time staff comprising a headquarters office with physicians and supporting staff, 2 medical officers in each district, a medical officer in each subdivision and vaccination teams totalling some 1500 persons. The programme was to begin in 6 of the 17 districts and was to be completed in these districts during the first year of operation. Vaccination campaigns would subsequently be conducted in the remaining districts during the second and third years. The vaccination teams would move progressively from one union to the next and assessment teams would check the coverage. It was expected that sufficient freeze-dried vaccine could be produced by the Dhaka laboratory for both East and West Pakistan. For the first year, WHO provided the following items : 10 motor vehicles, 130 motor cycles, 5 boats and 1500 bicycles, in addition to other supplies . Up to the end of 1971, WHO support to the programme ranged between US$ 67 000 and US$ 201 000 per annum (Table 16.5) . It did not increase significantly until 1974.
A WHO epidemiologist, Dr Karel Markvart, arrived in January 1968 to help with the organization of the national mass vaccination campaign. The problems in mobilizing and training so large a staff were staggering. Additional government funds were required to implement the programme (2.5 million rupees—i.e .,US$ 250 000) but because the agreement was not signed by the government until April 1968 no funds were made available before the fiscal year beginning 1 April 1969. A full-time national counterpart—Dr A. M. Mustaqul Huq, an able and dedicated public health officer— was not assigned until July 1969.
Table 16.5: Bangladesh: support provided to the smallpox eradication programme, 1967-1977, by source (U$)a
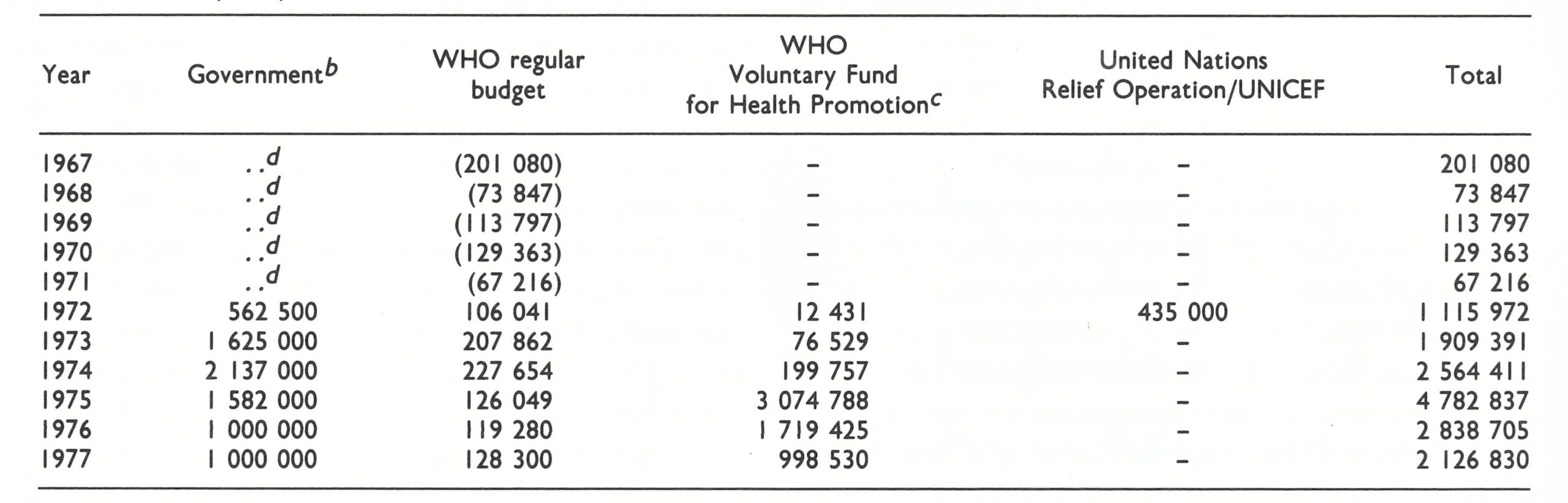
NOTE: WHO records for 1967-1971 reflect support to both East and West Pakistan . Approximately half (the figures shown in parentheses In this table) was provided to East Pakistan . The principal contributors to the WHO Voluntary Fund for Health Promotion were Canada, Denmark, Norway, Sweden and the United Kingdom . The United Nations Relief Operation, Dacca (UNROD), provided US$415 000 ; UNICEF provided US$20 000.
a From Joarder et al . (1980) and WHO financial records.
b Estimated.
c Not including the cost of 45.3 million doses of vaccine.
d ..=data not recorded.
Plate 16.2. A: Mohammad Ataur Rahman (b 1925) as deputy director of the vaccine production laboratory in Dhaka, Bangladesh, played an important role in its development and, later, as health adviser to the Planning Commission, provided essential support for national mobilization for smallpox eradication in 1975. B: Karel Markvart (b.1933) was a WHO adviser to the programme in Bangladesh from 1968 to 1971.
In 1968, the organization of health services in 12 of the 19 districts was chaotic. In the 12 so-called “non-provincialized” districts, there was a dual management structure. A district council appointed and paid the salary of a district health officer, who was responsible for preventive activities, while the provincial government appointed and paid a civil surgeon, who was responsible for both curative and preventive activities. At the next lower level, the subdivision, health activities were under the direction of a subdivisional medical officer of health, appointed and paid by the provincial government. He was required to supervise sanitary inspectors, who were appointed and paid by district councils. In their turn, they were expected to supervise vaccinators, who were recruited and paid by the provincial government. In addition, municipal staffs were independently directed by municipal committees and were not responsible to provincial or subdivisional government health staff. Appointments by district councils and municipal committees were as often decided by political considerations as by qualifications; discipline in performance and coordination were chronic problems which plagued the programme throughout its course. In the remaining 7 districts, the health services had been “provincialized” and there, with all health staff appointed and paid by the provincial government, the health structure operated more effectively.
At the end of 1968, the Dhaka municipal committee was persuaded to provide funds and staff to undertake a mass vaccination campaign, in part as a pilot study, but also in recognition of the role of this urban area as the country’s principal focus of the spread of smallpox. The campaign was reasonably successful as measured by a vaccination scar survey ; by the end of the campaign, more than 90% of the population had vaccination scars (Table 16.6). After May 1969, no smallpox cases were detected in Dhaka for more than 2 years.
Vaccine production, meanwhile, proved to be an unexpected problem. The quantity of vaccine produced was less than had been expected and barely sufficient to supply East Pakistan. Between 1966 and 1971, the laboratory produced an estimated total of 4 million vials of freeze-dried vaccine. Vaccine quality was said by the laboratory director to be satisfactory, but when samples from 7 batches were tested in the WHO smallpox vaccine reference centre in Bilthoven, Netherlands, in late 1968, only 3 met the accepted standards. Thereafter, the director permitted no one to have access to the laboratory’s records. He asserted that the vaccine was satisfactory, but examination of a further 10 batches in 1969 showed that only 3 were up to standard. Because of production problems, a consultant was recruited by WHO to work with the laboratory staff and after this the quality of the vaccine improved and the records again became accessible. However, some difficulties in producing a stable vaccine persisted throughout the programme.
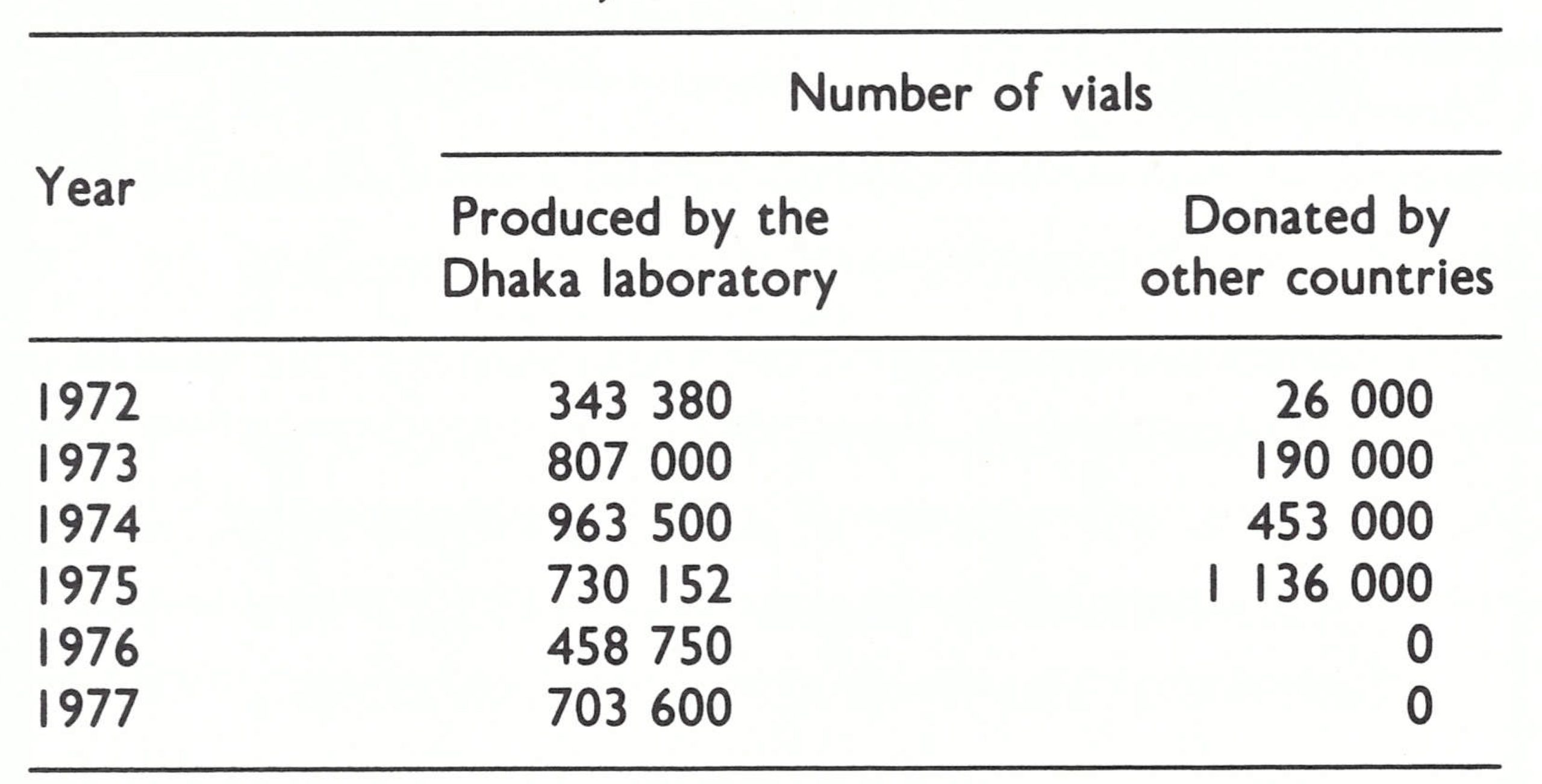
Vaccine production data by year are available only for the period 1972-1977. The quantity produced was gradually increased after the provision by WHO of additional equipment and supplies, so that by 1973 more than 10 000 vials a week were being manufactured. Nevertheless, up to 1975, additional vaccine was required and this shortfall was met by a number of donors through contributions to the WHO vaccine reserve stocks (Table 16.7).
In April 1969, the government-funded posts for the vaccination campaign were finally established, but recruitment proved to be such a cumbersome procedure that not until January 1970 did sufficient staff become available to permit mass campaigns to begin in 15 of the 21 subdivisions in 7 of the country’s 19 districts. In the execution of the programme and in the reporting of cases, it was agreed that the divisional and district health authorities would be bypassed, thus streamlining the structure so that only 4 levels would be involved in administrative direction and case reporting-headquarters, subdivisions, thanas and unions.
The vaccination campaign made slow progress, however. By November 1970, the teams had vaccinated only 4.5 million persons, little more than 6 % of the population of the country (Sommer et al.,1973). Meanwhile, local vaccinators reported that they had vaccinated 32.8 million people in 1968 and 31.6 million in 1969, although these figures were considered to be inflated. In 1970, vaccination scar surveys in the 7 districts in which mass vaccination had been performed showed 4 in which the proportion of the population with vaccination scars ranged from 64.9% to 72.1%, substantially lower than the 80.9% found by the research team in Comilla. In the other 3 districts, the proportions with vaccination scars were, respectively, 75.6%, 77% and 86.2%.
The number of reported cases reached a peak of 9039 in 1968, the highest total in a decade, but declined to 1925 in 1969. What, if anything, this implied was unknown since little had been done to improve the reporting system
Table 16.6: Dhaka Municipality: vaccination scar survey, 1969, by age group
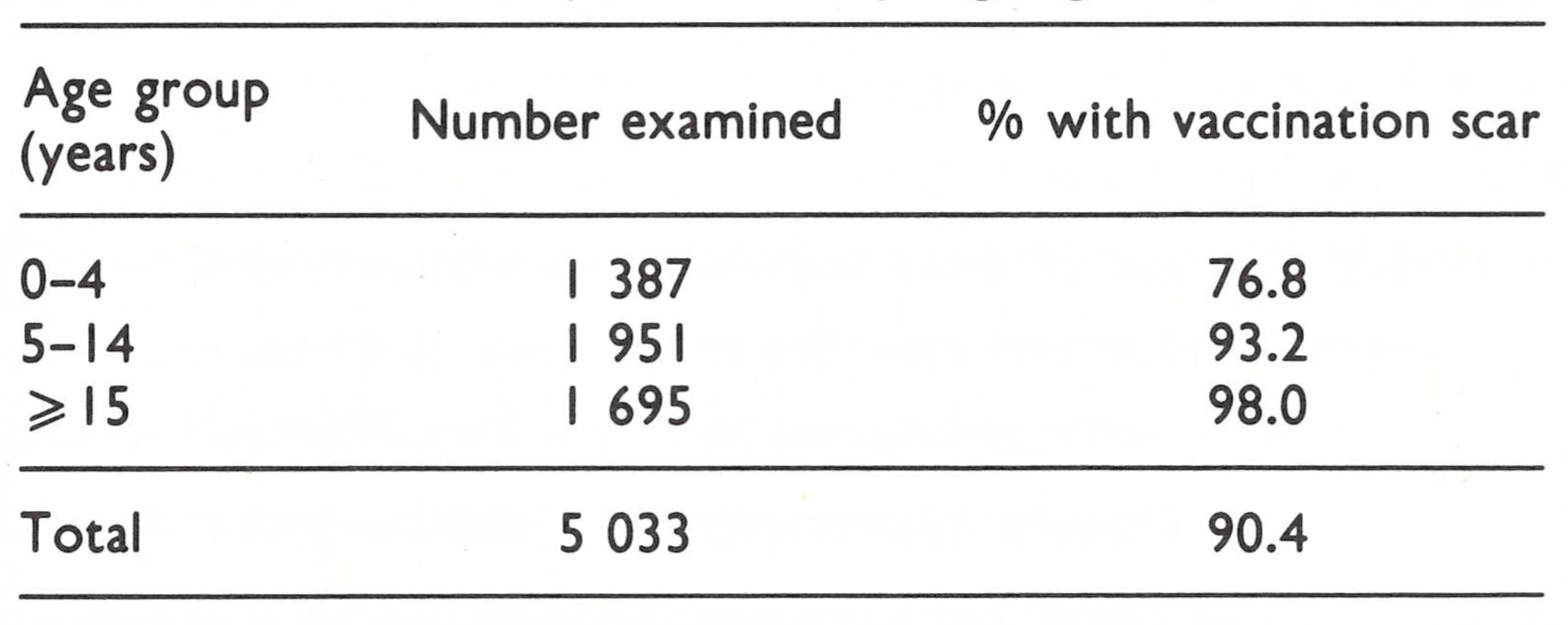
Table 16.7: Bangladesh: vaccine production at the Dhaka laboratory and vaccine donations, 1972-1977
INITIATION OF SURVEILLANCECONTAINMENT AND THE INTERRUPTION OF TRANSMISSION, 1970-1971
It had been agreed that in addition to the vaccination staff, there should be a surveillance team for each subdivision in which the mass vaccination campaign was conducted. As the plan of operations stated, the team would (1) control any reported attack of smallpox, and (2) if no cases were reported, vaccinate any person who had been missed after the operational (vaccinator) group had left the area. This first official recognition that there should be surveillance teams was encouraging but, conceptually, still far removed from the objective of establishing teams solely responsible for developing the reporting system, detecting cases and containing outbreaks throughout the country.
In November 1969, a WHO intercountry seminar on smallpox was convened in Dhaka which illustrated, on the basis of reports from western Africa and Brazil, what could be achieved with more effective case detection and outbreak containment. East Pakistan had reported only 4 cases in September and 1 case in October 1969. With so few reported cases, it was decided that from January 1970 an effort would be made to investigate every reported case. A surveillance section, headed by a medical officer, was established and 1 central and 4 divisional surveillance teams were recruited to improve reporting and to investigate outbreaks throughout the country. Because government travel allowances were too meagre to cover even the most modest board and lodging, WHO agreed to provide the teams and other senior supervisors with a supplementary per diem allowance to permit them to travel in the field. The leaders of the 4 divisional teams, Dr M. A. Sabour, Dr M. Yusuf, Dr M. Shahabuddin and Dr M. A. Khan, proved to be exceptionally able and dedicated and served in this capacity throughout the entire programme. In January 1970, the first monthly surveillance report was issued, and this series continued to appear, with interruptions due to civil war, throughout the programme.
Because the time of Dr Markvart and Dr Huq was fully taken with the complex logistics of the mass campaign, Arita was assigned from WHO Headquarters for the months of February and March to help to develop the surveillance programme. In collaboration with the newly constituted surveillance teams, he investigated reported outbreaks in various parts of the country. To the surprise of all concerned, the teams discovered that cases being reported from the central and southern parts of the country were not smallpox but chickenpox and other skin diseases. On the other hand, in a northern district, the investigation of a newspaper report of 6 cases led to the detection of 93 cases of smallpox. By the end of March, it appeared that smallpox was localized in only 5 northern districts of the country. Arita suggested that the vaccination campaign should be temporarily suspended in favour of an emergency surveillance-containment campaign whose objective would be to interrupt transmission before the monsoon rains. With the agreement of a newly appointed and highly competent Minister of Health, Colonel M. M. Haque, and after the surveillance teams had been specially trained, such a campaign began; it was one of the most dramatically successful of the entire global eradication programme.
To facilitate surveillance, the reporting system was changed. The detection and identification of cases had depended on a traditional routine in which a local government employee, the chowkidar (who served also as the village watchman), was responsible for the weekly reporting of births, deaths and notifiable diseases to the than headquarters. The chowkidars were frequently illiterate, poorly paid and ineffectual. Reports received at the thana were forwarded by mail to the subdivision, and then to the statistical section of the Ministry of Health. Reports were submitted sporadically, often after delays of several weeks, through a mail system that was anything but reliable.
Beginning in April 1970, all health workers and the malaria eradication programme staff were asked to report each suspected case of smallpox they encountered to the than sanitary inspector. The betterpaid, better-supervised and generally more responsible malaria eradication workers visited all houses throughout the country once every 2 weeks, searching for persons with fever who might have malaria and confirming this by the examination of blood smears. For them to report suspected cases of smallpox entailed little additional work and no disruption of activity. Thana sanitary inspectors were instructed to forward weekly reports of all cases in their than to the subdivisional medical officers. They in turn were to report cases by telegram rather than by mail to the Dhaka smallpox eradication programme headquarters. When outbreaks were detected, the subdivisional medical officers as well as the thana health inspectors were instructed to investigate and contain them. This system brought health workers into the reporting system and streamlined reporting by introducing telegraphic notification directly from the subdivision to the smallpox eradication headquarters, thus bypassing the largely uninterested bureaucracy of the statistical section of the Ministry of Health.
The investigation of outbreaks generally confirmed the findings of the Comilla study: that most outbreaks originated in cities ; that the spread of smallpox from village to village was surprisingly infrequent; and that outbreaks could be readily contained by vaccinating the inhabitants of an infected bari and those of a few baris surrounding it. In the northern part of the country, in which health services were less adequate and vaccinial immunity was lower, village-to-village spread was documented in 3 thanas in which 13 outbreaks and 149 cases had occurred. Even here, however, the spread of smallpox was slow and although 3-7 months had elapsed between the introduction of smallpox and its detection, there were comparatively few cases in each generation of transmission and the outbreaks were readily contained (Wkly epidem . rec ., 1970b). Between January and March 1970, 1024 cases were detected and reported but many of these represented cases which had occurred some months previously. Few active cases were discovered.
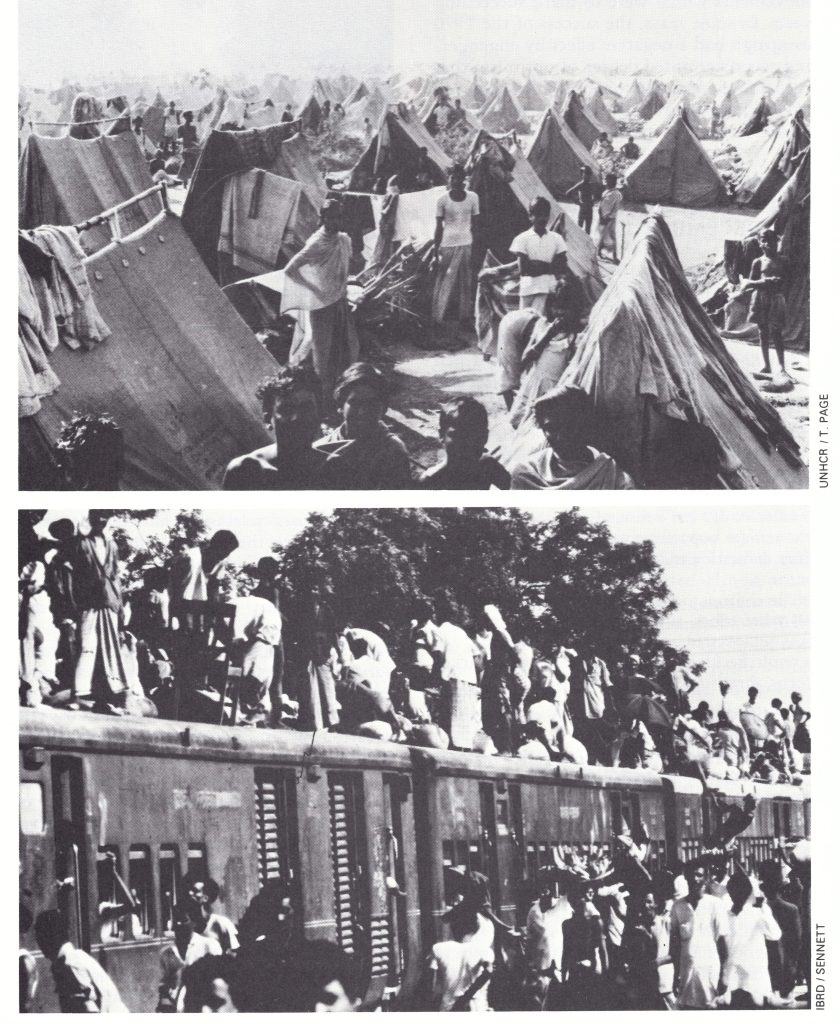
Plate 16.3. Bangladeshis, infected with smallpox while living as refugees in India, returned to their newly independent country, only recently freed of smallpox, from December 1971. Travelling in crowded trucks and trains, many lived in resettlement camps until their houses could be rebuilt. Smallpox spread widely and rapidly through the camps and across the country.
In the entire country, only 263 cases were detected in April and only 116 in May . Moreover, the cases were localized : 4 out of 19 districts accounted for all but 59 cases. In June, the 5 surveillance teams were assigned to work intensively in the remaining infected areas and 10 surveillance teams previously working with the vaccination teams were also sent to these areas to contain outbreaks. Thirty-eight cases were discovered in June, 23 cases in July, and 9 cases in August. In August, the teams detected and contained the last known outbreak—in Pabna District. Effective surveillance continued for another 6 months but no further cases could be found.
In March 1971 civil war broke out, and until December 1971 the country was totally disrupted. During this period, it is estimated that between 1 and 3 million civilians died, 10 million refugees fled to India and an estimated 16.6 million people left their homes for other parts of the country (Chen & Rohde, 1973). Bridges were blown up, 1.5 million houses were destroyed, and severe famine occurred (Greenough & Cash, 1973).
Such evidence as is available substantiates the belief that, until 16 December 1971, when Bangladesh became independent, endemic smallpox was absent from the country—a smallpox-free interval of 16 months. During the period of civil war, no cases were found in any of the major cities, the usual sites of endemic transmission. The divisional surveillance teams were proud of their achievements and continued to travel widely throughout the country—albeit at considerable risk—seeking information about possible cases but finding none. The refugees who streamed ceaselessly across the border throughout this period were reasonably thoroughly screened by Indian civilian and military health staff in an effort to detect cases of smallpox, but none was discovered. Moreover, when smallpox was reintroduced into Bangladesh, investigation revealed that the primary source of each outbreak was a refugee who had contracted the disease in 1 of 4 infected refugee camps in India or on the way home. During April 1972, almost all cases occurred among returning refugees and their immediate contacts (Sommer et al ., 1973).
The comparative ease and rapidity with which smallpox transmission was interrupted in Bangladesh in the summer of 1970 was in stark contrast to the staggering difficulties which were to mark the 4 years following its reintroduction . In retrospect, the timing of the 1970 spring surveillance-containment campaign had been ideal, from the standpoint both of the season and of the longer-term periodicity of smallpox. It had begun in the late spring, when rates of transmission customarily declined and many outbreaks terminated spontaneously (Fig. 16.5) . With regard to the longer-term periodicity, smallpox incidence had peaked in 1968, with 9039 cases, and in 1969 the annual reported incidence had declined sharply to 1925 cases. In 1970, it is probable that no more than 150- 200 cases would have been reported had not the special programme improved the completeness of notification. Even so, only 1473 cases were recorded. Moreover, at this time, neither flood, drought nor civil disorder resulted in famine and the extensive refugee movements which were to mark succeeding years. In some ways, the success of the 1970 campaign had a negative effect by engendering an unwarranted degree of optimism that such a favourable outcome could be achieved as readily and as rapidly again in Bangladesh as well as in other parts of the subcontinent.
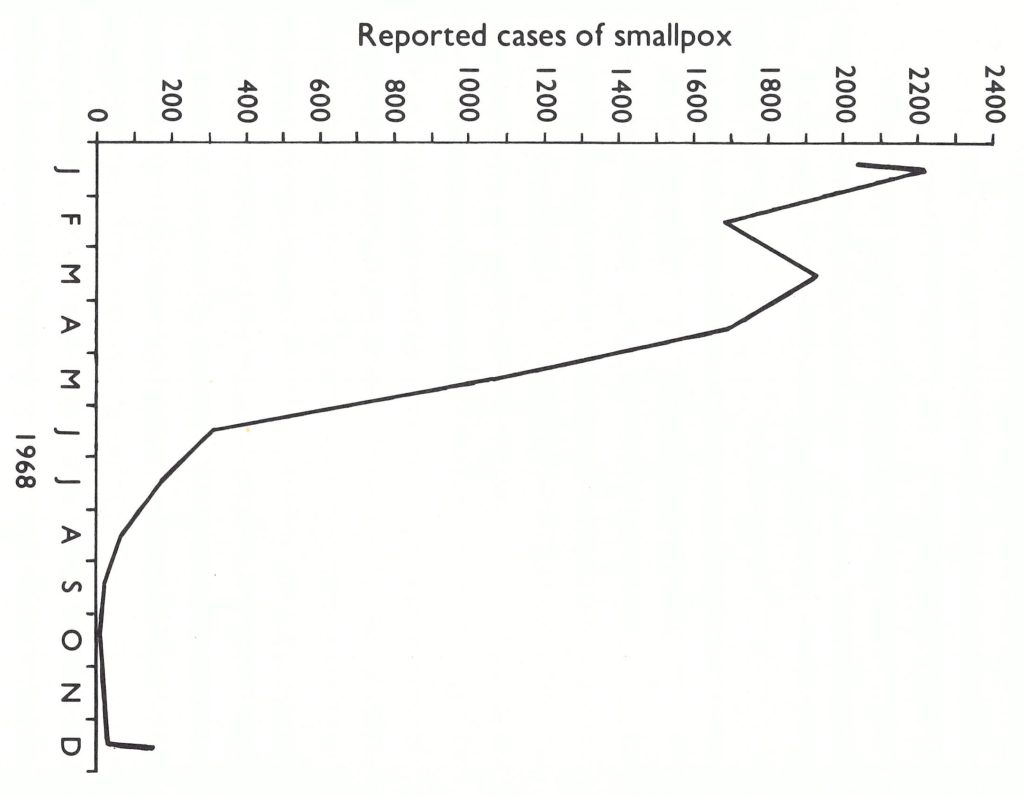
Fig. 16.5. Bangladesh: typical seasonal variation in smallpox incidence, as shown by the number of reported cases in 1968.
THE REFUGEE CAMPS AND THE REINTRODUCTION OF SMALLPOX, DECEMBER 1971-MAY 1972
Of the estimated 10 million persons who left the country, most were housed in crowded camps. The largest, near Calcutta, was the Salt Lake Camp which sheltered an estimated 200 000-300 000 refugees. Government priority was given to supplying food, shelter and sanitary facilities. As noted in one report (Rohde & Gardner, 1973):
“The provision of relief to 10 million refugees . . . represented a monumental humanitarian achievement. That mass starvation and galloping epidemics did not consume a greater portion of the refugee population is a tribute to the leadership, dedication and energy of the Indian Government . . .
“In contrast to the efficient conduct of the overall relief effort, authority over health programs was not invested in any one group or person . . . As a result, health policies and programs often lacked focus, direction, and coordination.”
The provision of smallpox vaccination was one of these policies.
The Indian Ministry of Health had instructed state governments to ensure that all refugees were vaccinated against smallpox. In some camps, vaccinations were given by government staff and/or the personnel of voluntary relief agencies, and the conscientious performance of this task was confirmed by visiting Indian and WHO staff. However, state officials did not permit national health personnel or WHO staff to visit the camps in West Bengal so confirmation there was not possible. Medical care in the Salt Lake Camp was under the supervision of a voluntary relief agency; at that camp, as it was learned later, vaccination was ignored. It is likely that cases of smallpox began to occur in November, the source of infection being villages in West Bengal. The cases were recorded as chickenpox by the health staff.
The epidemic was discovered by chance. On 19 January 1972, an American epidemiologist thought he could identify cases of smallpox in a television film of the camp transmitted to the USA. He telephoned the Communicable Disease Center, which telephoned WHO Headquarters. WHO telexed the government of India, which in turn contacted the West Bengal Ministry of Health. Although the state Director of Health Services categorically denied there were cases, one of the national staff flew to Calcutta and immediately found numerous patients. The isolation of cases and vaccination began on 23 January, but by then it was too late. On 16 December 1971, Bangladesh had become an independent country and refugees began returning home forthwith. By mid-January, an estimated 50 000 had left the Salt Lake Camp. Infectious cases, patients in the incubation period and unvaccinated contacts were all loaded together on trucks for the trip to the border. It was the season when the transmission of smallpox was most rapid and with 26 million displaced persons moving from place to place, herded together in temporary camps and crowding the bustees (city slums), smallpox spread rapidly.
Under the best of circumstances the problem would have been difficult to cope with but at this time the health services were seriously disrupted. So many motor vehicles had been damaged or stolen that less than half remained in working order, and only one third of the number of bicycles required were available. Boats had been damaged or sunk and because of the destruction of roads, bridges and ferries, travel from place to place was difficult and time-consuming.
Plate 16.4. Left to right: D. J. M. Tarantola, WHO smallpox eradication adviser in Bangladesh, 1974- 1977; M. Sathianathan, a medical officer in Bangladesh, who had previously served as the WHO adviser for smallpox eradication in Nepal; A. K. Joarder, Assistant Director of Health Services of Bangladesh and director of the national smallpox eradication programme, 1972-1977.
Arita, then on duty travel in India, flew immediately to Dhaka, and working with Dr M. Huq, the Director of Health Services, endeavoured to control the outbreaks. By March 1972, the smallpox eradication headquarters had been re-established under Dr A. K. Joarder, Assistant Director of Health Services ; divisional surveillance teams had been reconstituted and were endeavouring to detect and contain outbreaks as best they could. Smallpox continued to spread, however, and 4 WHO epidemiologists were hurriedly dispatched. Among them were Dr Stanley Foster, who had previously served as the chief smallpox adviser in Nigeria, and Dr Nilton Arnt, one of the principal epidemiologists who had worked in the eradication campaign in Brazil. Some 3800 temporary vaccinators were hired to perform vaccinations, primarily in the large temporary refugee camps and surrounding districts. At first the epidemic was largely confined to 3 south-western districts-Barisal, Faridpur and Khulna. Active search, however, revealed the presence of smallpox in 27 of the country’s 57 subdivisions, although most had only a few cases . The refugees were mainly Hindus and initially the outbreaks afflicted Hindu areas and villages, but within a few generations of disease transmission, other groups were infected as well. In March, epidemic smallpox was detected in Khulna Municipality, the third largest city in Bangladesh. The control of smallpox in urban areas was recognized to be vital, and here a vigorous and remarkably successful programme was begun on 28 April (Sommer, 1974; Sommer & Foster, 1974). Eight 4-man surveillance teams were organized and trained to identify infected cases through interviewing patients at the Infectious Disease Hospital and by visits to the bazaars. When a case was found in the city, all persons in the household and compound were vaccinated and house-to-house searches were conducted throughout the village or bustee. The area was revisited after 2 or 3 days and again 3 weeks later to vaccinate individuals who had been missed during the first visit and to be certain that transmission had stopped. Containment measures were necessarily limited in scope because of the paucity of staff and the extent of the epidemic. In fact, it was necessary to divide the city into 3 segments and to deal with each in turn. Although 1073 cases were detected, smallpox was effectively contained within a matter of 4-6 weeks in each of the areas (Fig. 16.6). Meanwhile, the disease had broken out in a city refugee camp housing 30 000 persons. It was decided to vaccinate everyone in the camp by the simple expedient of making vaccination a prerequisite for the receipt of relief supplies. Altogether 233 cases were detected; however, the outbreak was as successfully dealt with as the one in Khulna Municipality (Fig. 16.7). To have achieved so much so quickly, with so few health personnel, at a time of considerable civil turmoil was a remarkable accomplishment and encouraged staff in the belief that the flood of importations might yet be successfully contained.
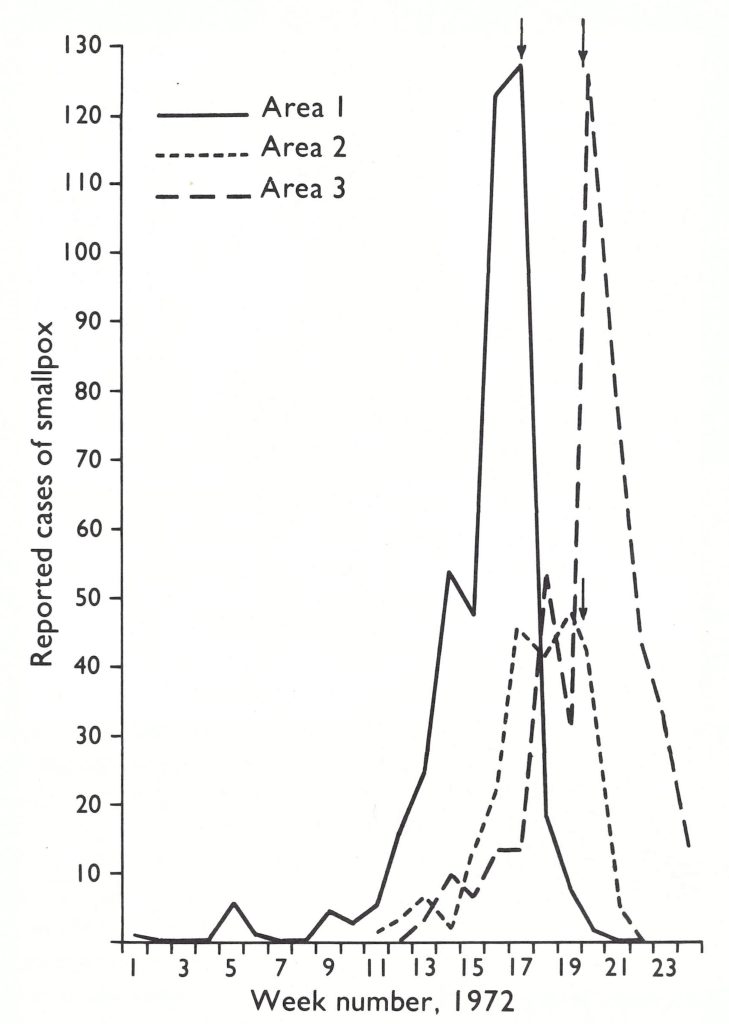
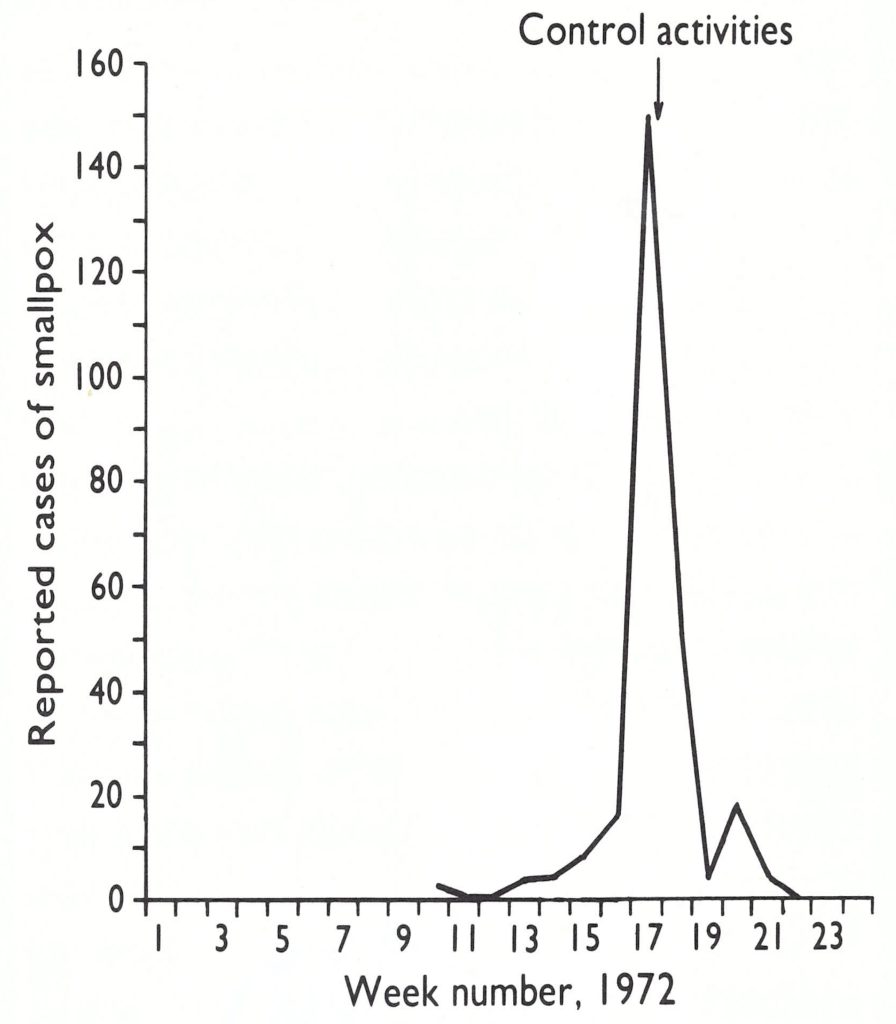
Fig. 16.2. Khulna Municipality: number of reported cases of smallpox in 1972 by week of onset in 3 areas of the city. Arrows indicate the week surveillance-containment activities started in each area.
Fig. 16.3. Kalishpur Bihari camp: number of reported cases of smallpox in 1972 by week of onset.
However, smallpox was spreading rapidly through rural as well as urban areas, wherever returning refugees settled. A survey of one rural than in May revealed 2298 cases among 250 000 inhabitants—approximately 1 case per 100 population . Meanwhile the disease continued to spread through refugee resettlement camps, some of which housed Bangladeshis of Bihari origin. From these camps, it spread to adjoining thanas. Small outbreaks developed in Dhaka and Chittagong but these were controlled. Intensive studies of a number of the outbreaks in which cases and deaths were thoroughly investigated revealed case-fatality rates of up to 28%, higher than those found elsewhere in the subcontinent and undoubtedly reflecting the extensive malnutrition then prevailing.
By the end of June 1972, 6144 cases had been reported in Bangladesh, of which 5834 (95%) were from only 4 districts (Fig . 16.8). Although reporting was recognized to be incomplete, it sufficed to indicate that large parts of the country had few or no cases. With a concerted effort such as had been made in Khulna and conducted throughout the monsoon period of diminished transmission, the staff hoped that the epidemic spread could be contained. Special assistance was given to the programme by the United Nations Relief Operation, Dacca, in the form of motor vehicles, boats, outboard engines and bicycles. WHO provided motor cycles and additional bicycles to facilitate the effort (Table 16.8). However, much of the transport served only to replace that which was worn out or had been destroyed during the civil war.
Of the 4 WHO epidemiologists who had assisted during the spring emergency, Dr Arnt and Dr Foster continued on permanent assignment in what proved to be one of the most arduous and taxing endeavours of the global eradication programme. They were soon joined by 3 other staff, who remained with the programme essentially full time until transmission had been interrupted: Dr Nicholas Ward, who had previously been employed as a District Medical Officer in Botswana; Dr Stanley Music, a Bengali speaking epidemiologist who had previously been stationed in Dhaka on assignment from the Communicable Disease Center; and Dr Daniel Tarantola, a physician who had been working at a hospital in northern Bangladesh with a French voluntary organization.
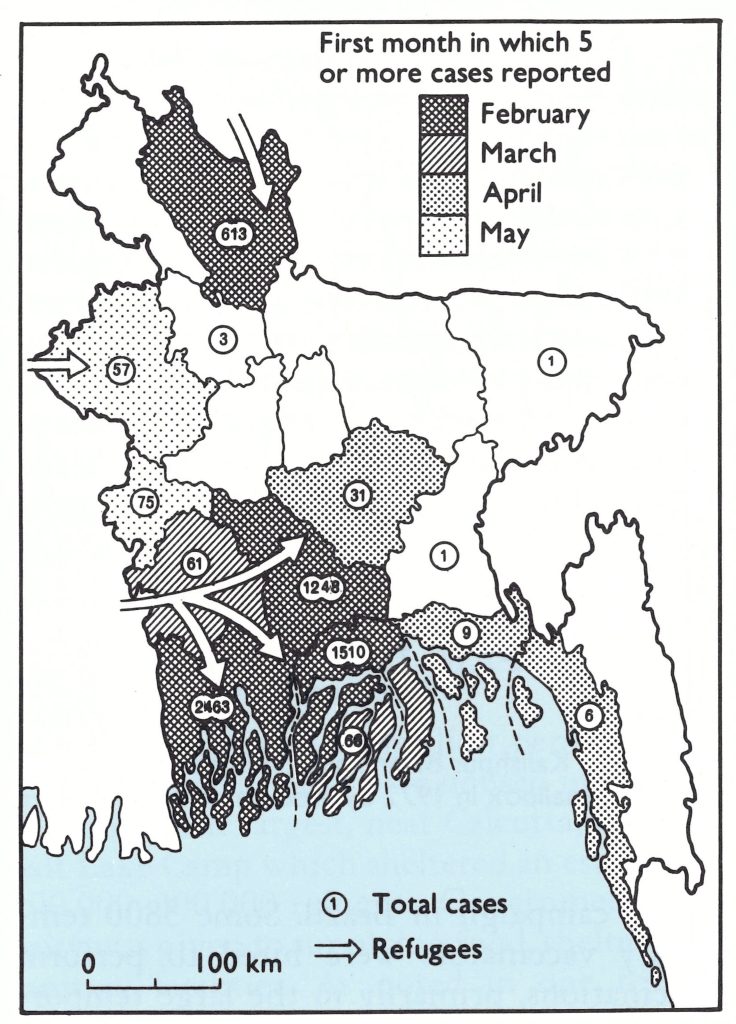
Fig. 16.8. Bangladesh: infected districts and number of reported cases of smallpox as of 30 June 1972.
Plate 16.5. Harkishan D. Mehta (b.1934), a WHO epidemiologist with the Bangladesh programme, 1974-1978, on the left, with Stanley O. Foster (b .1933), a United States epidemiologist who had previously served as senior adviser to the smallpox eradication programme in Nigeria, 1966-1972, then served in Bangladesh as a WHO adviser for smallpox eradication, 1972-1977.
Table 16.8: Bangladesh: transport provided to the smallpox eradication programme, 1967-1975

aSupplied by the United Nations Relief Operations, Dacca.
THE PROGRAMME IS RE-ESTABLISHED, JUNE 1972- SEPTEMBER 1973
The reporting system, which required weekly telegraphic reports from each of the 57 subdivisions, was reinstituted in March 1972 (Foster et al., 1980). Reports to the subdivisions were provided through than sanitary inspectors by government health assistants, each of whom worked in a union, the health assistant/population ratio being approximately 1 to 15 000. During the summer, 4-man surveillance teams, headed by a sanitary inspector, worked in each infected subdivision; in each infected thana, vaccinators were grouped into 3-man teams for active search and containment. Particular emphasis was placed on the search in weekly markets by health workers using megaphones. This approach was later shown to detect approximately 80% of all outbreaks within an area of 65 square kilometres.
A mass vaccination campaign in the 4 most heavily infected districts had begun in the spring, but was stopped when it became apparent that it would accomplish little more than the 1970 campaign. As Dr Huq and his colleagues stated in a report dated October 1972: “It is now clear that eradication through mass vaccination is not feasible . . . The orthodox principle of blind, systematic vaccination has already been given up.”
Between June and October 1972, 400-800 cases were detected monthly, a substantial number for that season of the year. However, up to the end of October, outbreaks had been documented in only 88 of the 409 thanas in the country, and by then only 36 were still infected . By the end of 1972, 10 754 cases had been reported, approximately one-tenth of the number which had actually occurred, as a survey for facial pockmarks carried out 4 years later was to show (Hughes et al ., 1980; Fig. 16.9 ; Table 16.9). The system for detecting and reporting cases, although well designed, lacked adequate supervision.
After the monsoon season, with high transmission approaching, it was decided that resources should be concentrated in the subdivisions of the 4 most heavily infected districts. A 10-man team, headed by an assistant health inspector, was assigned to each of the infected thanas to search for cases and to contain any outbreaks that were found. A national surveillance team with 5 assessment staff supervised these efforts and made repeated visits to the sites of outbreaks to ensure that they had been contained. Four surveillance teams, working under the supervision of the national eradication headquarters, travelled throughout the areas which had reported only a few imported cases to strengthen surveillance and to contain outbreaks.
The strategy was based on the assumption that smallpox would tend to remain localized in the areas already identified as infected. A key factor in the strategy was the control of smallpox in Dhaka, the capital and largest city in the country, and the potential focus of spread of smallpox into the largely smallpox free areas of central and eastern Bangladesh. In April and May 1972,26 cases had occurred among refugees in Dhaka but the outbreaks were contained. Only a single case was recorded in July and another in August, but early in October scattered outbreaks began to occur in densely populated urban slum areas and resettlement camps, in which the nighttime population densities were estimated to be as high as 195 000 per square kilometre, or 1 person to every 5 square metres. Twentynine cases were detected in October, 80 in November and 216 in December (Table 16.10). The containment of outbreaks in the densely congested areas seemed all but impossible short of an area-wide mass vaccination campaign.
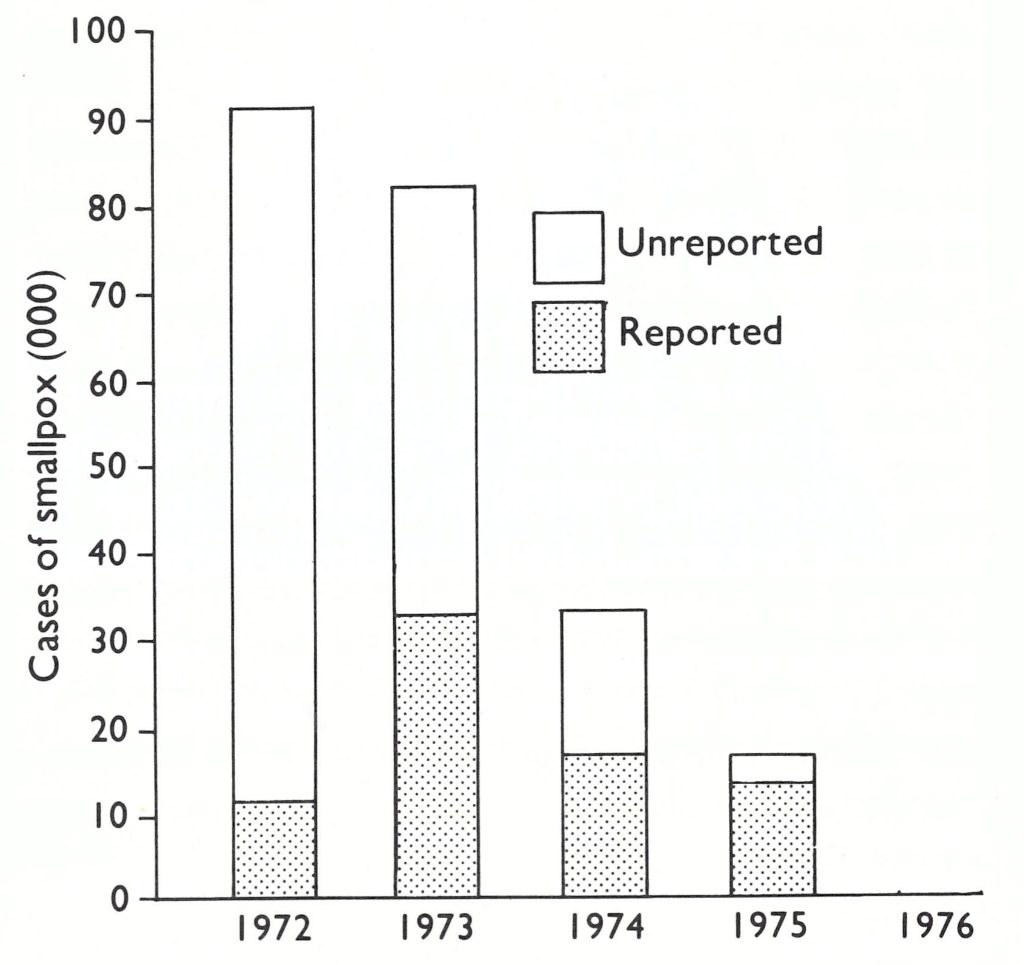
Fig. 16.9. Bangladesh: estimated total number of smallpox cases that occurred compared with the number of cases reported, 1972-1976.
Table 16.9: Bangladesh: number of reported cases of smallpox as a percentage of the estimated number of cases (surveillance efficiency), 1972-1975a
afrom Hughes et al.(1980).
Table 16.10: Dhaka Municipality: number of reported cases of and deaths from smallpox, by month, 1972-1973a
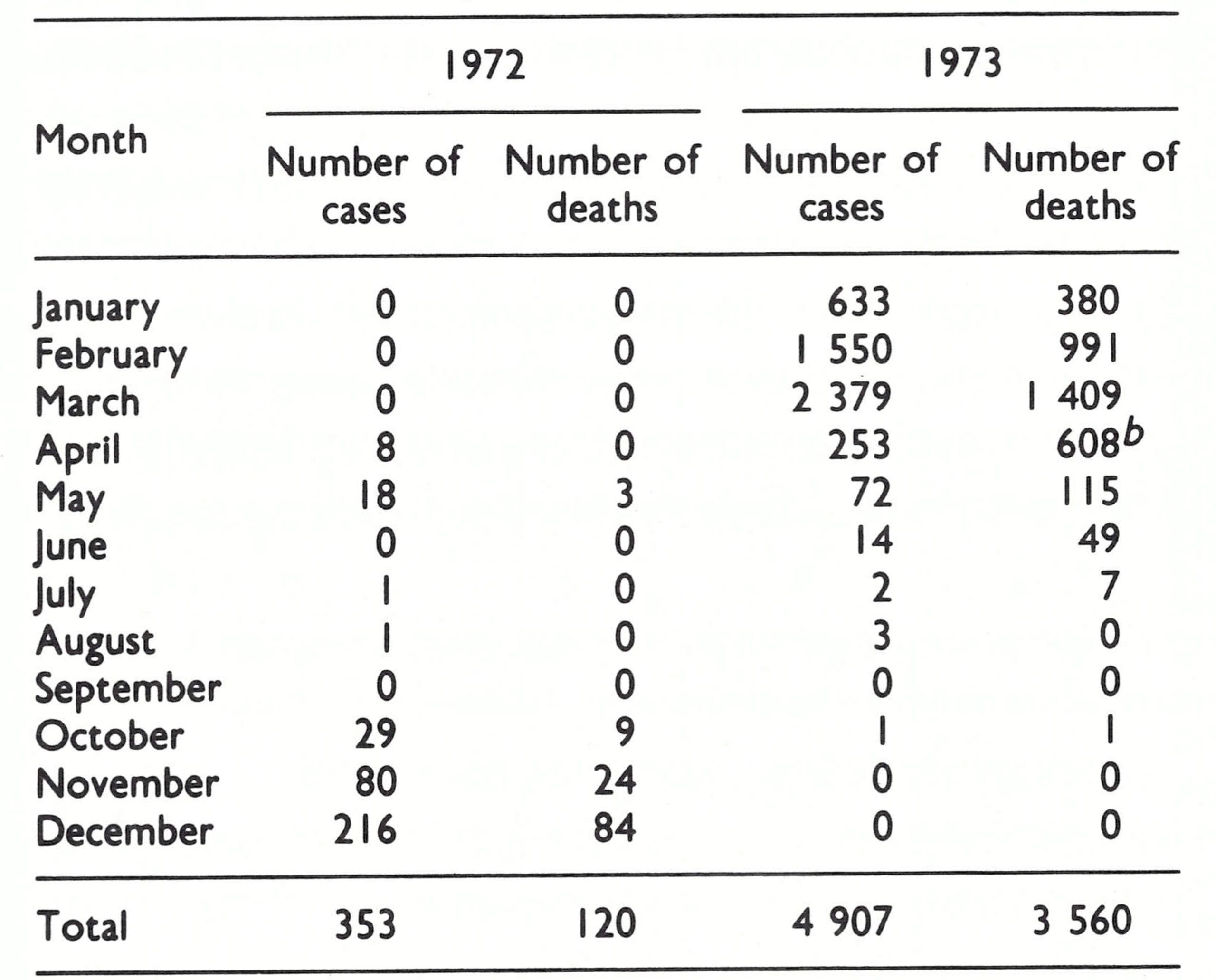
afrom Joarder et al.(1980).
bIncluding deaths related to cases reported in previous months.
Plate 16.6. A: Surveillance during the monsoon season was an especially arduous task as streams washed out roads, and footbridges often consisted of little more than a single bamboo pole. B: Alan H . Schnur (b.1948) served as a US Peace Corps volunteer with the smallpox eradication programme in Ethiopia from 1971 to 1974 before being recruited as a WHO consultant for service in India and Bangladesh.
In January 1973, Dr Ward assumed responsibility for the development of a special programme in Dhaka to control smallpox more rapidly. A municipal headquarters was established and 18 mobile surveillance units were formed.
- The Infectious Disease Hospital and the major graveyards of the city were visited daily to collect information on smallpox cases and deaths.
- Fixed checkpoints were established at transport terminals to collect information and to vaccinate passengers.
- Vaccination of the inhabitants of slum areas and refugee centres was carried out at night as well as during the day.
During 1973, 1,747,000 vaccinations were performed in Dhaka City alone, but the epidemic did not begin to abate until April. Although only 4907 cases were detected, it was apparent from the large number of deaths attributable to smallpox that there were many more cases than this—an estimated 14 000 or more.
Meanwhile, during the spring of 1973, 26 surveillance teams worked throughout the country; 5 of these were national teams each with responsibility for a region, 9 were district teams, 4 were municipal teams and 7 were assigned to the heavily infected subdivisions. Each team moved from thana to thana searching for cases in major markets, schools and selected villages. When an outbreak was discovered, local health staff were mobilized to vaccinate the residents of the 30 houses nearest to those with cases.
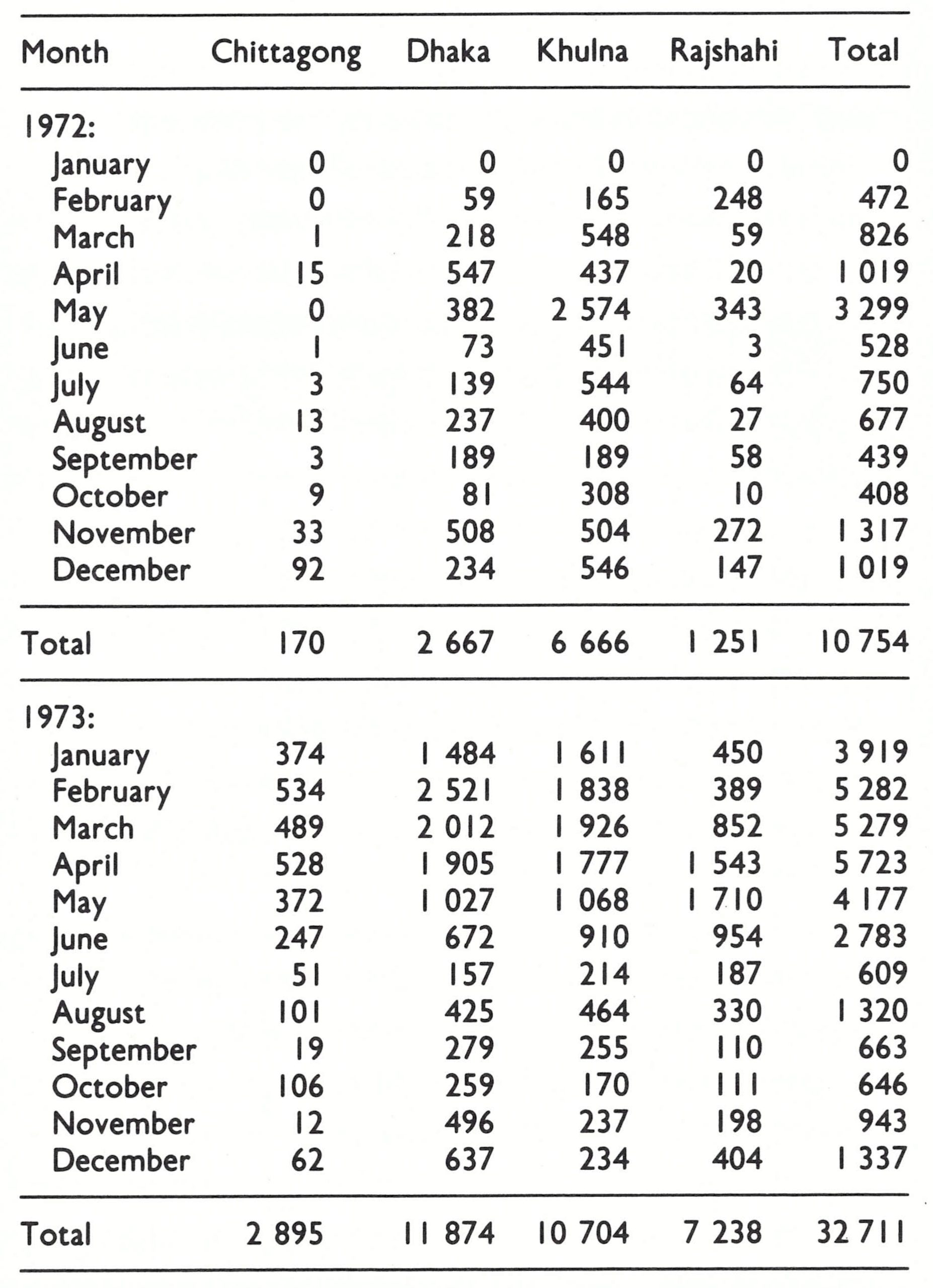
The programme staff worked frantically to contain the outbreaks but, with Dhaka heavily infected, smallpox quickly spread across Bangladesh. The number of reported cases increased from only 1019 in December 1972 (Fig. 16.10) to 3919 in January 1973 and to 5282 in February; in February, cases were reported from every district in the country (Table 16.11).
The epidemic reached its peak in April and once again began to subside with the onset of the monsoon. The number of reported cases was substantially greater than during the preceding year, but since the number of surveillance teams had increased and notification was more complete, it was hoped that during the monsoon season transmission could be brought under control. To facilitate this, containment procedures were changed, since it was found that outbreaks were persisting because of failure to vaccinate household contacts who were absent during the day. Accordingly, each team was required to carry out house-to-house vaccination in each infected village at night or in the early morning.
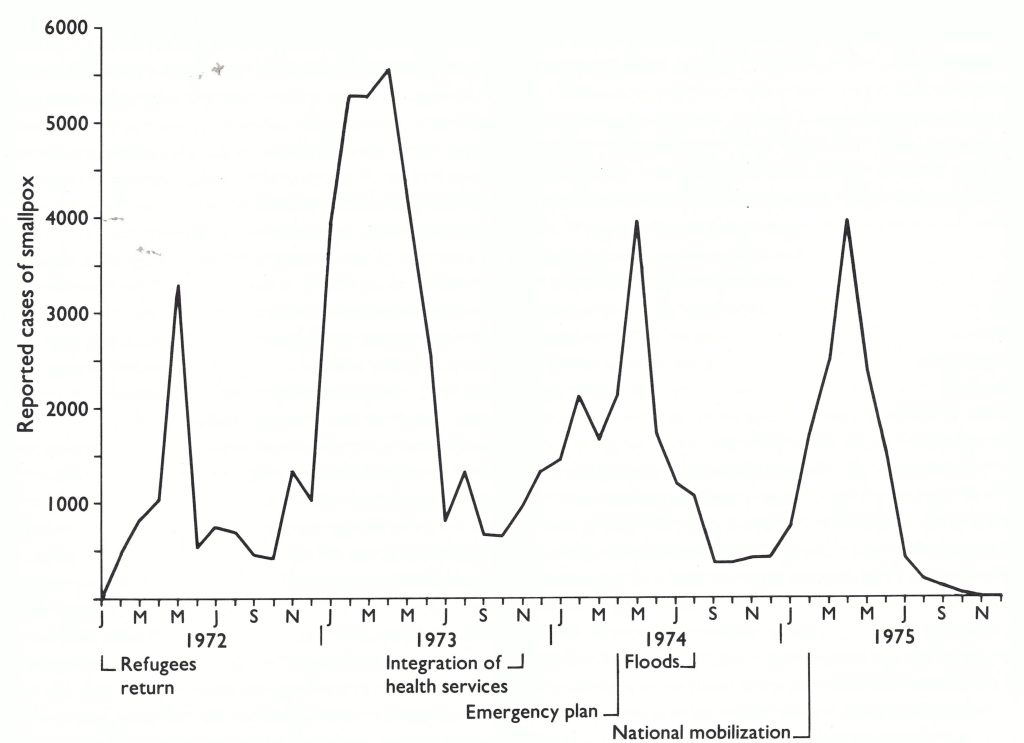
Fig. 16.9. Bangladesh: number of reported cases of smallpox, by month, January 1972-December 1975.
Table 16.11: Bangladesh: number of reported cases of smallpox, by division and by month, 1972-1973
REORGANIZATION OF THE HEALTH SERVICES, OCTOBER 1973
In October 1973, only 646 cases were notified. Reports were being received promptly from 95% of the subdivisions and there was increasing confidence that few outbreaks were being missed. On the assumption of an average of 4 cases per outbreak, it was calculated that there were perhaps 150-175 infected villages in the entire country. Dhaka was free of smallpox, as were most subdivisions of Rajshahi and Chittagong Divisions. To ensure a closer supervision of activities throughout the country, programme staff decided in October to set up 25 district surveillance teams, I for each of 19 districts and an additional team for each of the 6 largest districts. Each team, which consisted of 5 persons, led by a health inspector, was given transport (a motor vehicle, a motor cycle or a boat).
The plan experienced a serious setback, however, when in November, the government decided to suspend health activities temporarily in order to reorganize the health services. The field staff of the hitherto autonomous malaria eradication programme were to be merged with other health workers into a single integrated health care service. The new workers were to be called “family welfare workers”, each assuming responsibility for a specific geographical area containing approximately 5000 people. The tasks assigned to them included preparing individual family health cards, registering married couples and births, performing smallpox vaccination, searching for cases of malaria and smallpox, and distributing vitamin A capsules and contraceptives, as well as providing health education and family-planning materials.
The integration of all health services had long been a tenet of WHO but practical approaches to its accomplishment had never been satisfactorily elaborated. Bangladesh’s experience did not provide a model. A training programme was hastily concocted and, for a period of 4 weeks, virtually all health staff except smallpox surveillance teams were withdrawn from the field for training. They returned to the field to begin a whole range of new and unfamiliar activities for which few of the necessary supplies were provided. Their first task, which required some 2 months to complete, was to prepare a separate health card for each family on which the name and age of each family member were to be listed. Despite the integration of field staff, however, 2 separate supervisory structures were left in place: the malaria eradication programme structure and the previous health service structure. Former malaria eradication staff and health service staff looked to their respective former supervisors for direction. The entire health service, which had not been functioning well, deteriorated further; many employees abandoned their jobs and returned to cultivating their small plots of land.
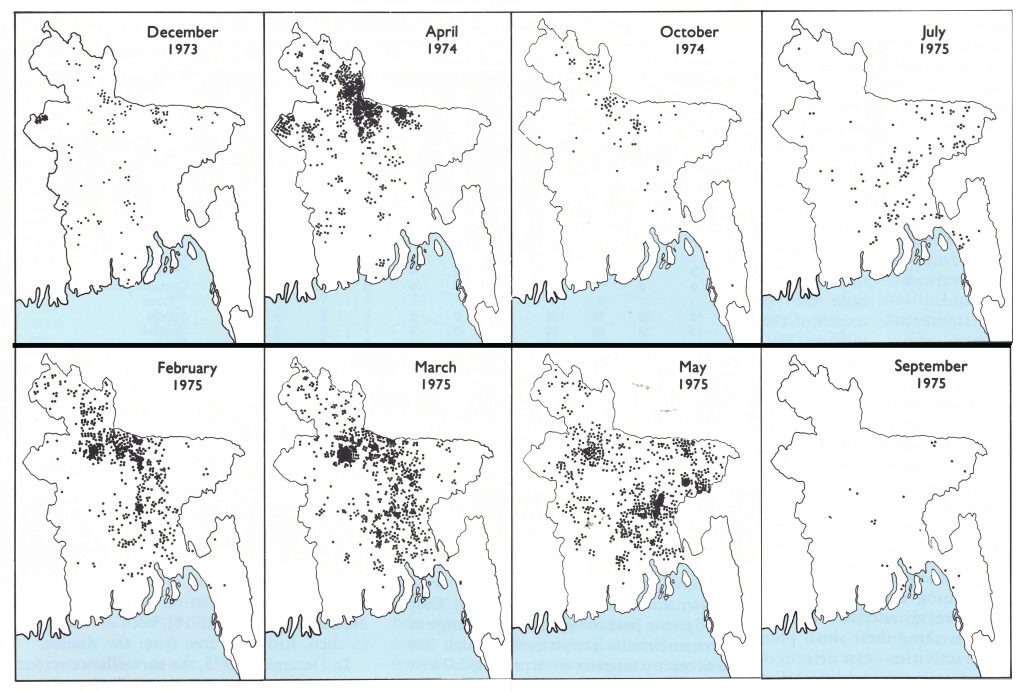
Fig. 16.11. Bangladesh: villages infected with smallpox in 8 months between December 1973 and September 1975.
All activities—case detection, containment and vaccination—sharply diminished after November, but despite less adequate reporting by the health staff the number of cases which were detected doubled between October and December . Smallpox cases, widely but sparsely distributed throughout the country immediately after the monsoon, suddenly began to occur in large numbers in the northern districts of Rangpur and Mymensingh (Fig. 16.11), both of which, up to then, had been free from the disease.
In December 1973, the surveillance system was modified to enumerate “infected villages” as well as the numbers of cases and deaths, a practice that had been adopted earlier in the year in several states of India. In Bangladesh, each village was designated infected until 6 weeks had elapsed after the onset of the last case. (India continued to use a 4-week interval until later that year.)
During the first 4 months of 1974, the number of infected villages increased from 309 in January to 949 in April (Fig. 16.12; Table 16.12). Rangpur and Mymensingh Districts accounted for 660 (69.5%) of the total. In April, Khulna Division, which had been the epicentre of smallpox after the return of the refugees, had only 41 infected villages. The concentration of resources and supervisory personnel in 1972-1973 in the initially heavily infected areas had been remarkably successful in stopping spread, but the programme in other areas had consequently received less attention. With the withdrawal of health staff from the field and the subsequent confusion accompanying the reorganization of health services, a potentially manageable situation had developed into a major problem.
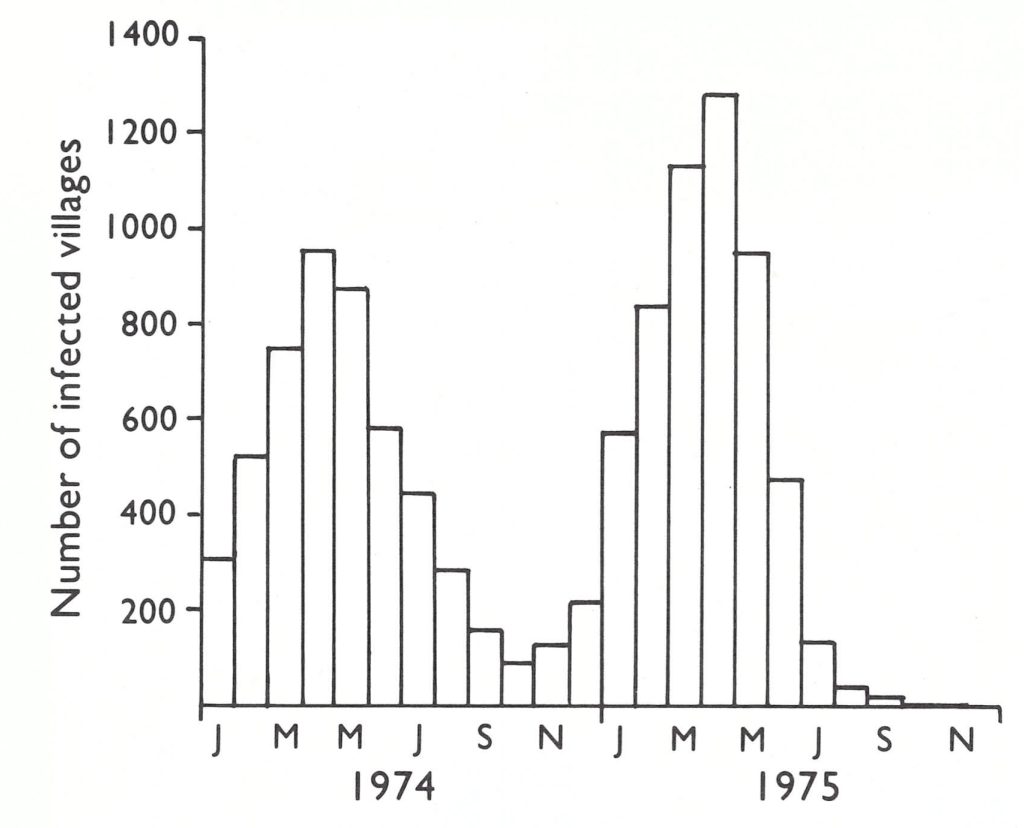
Fig. 16.12. Bangladesh: number of smallpox-infected villages, by month, 1974-1975
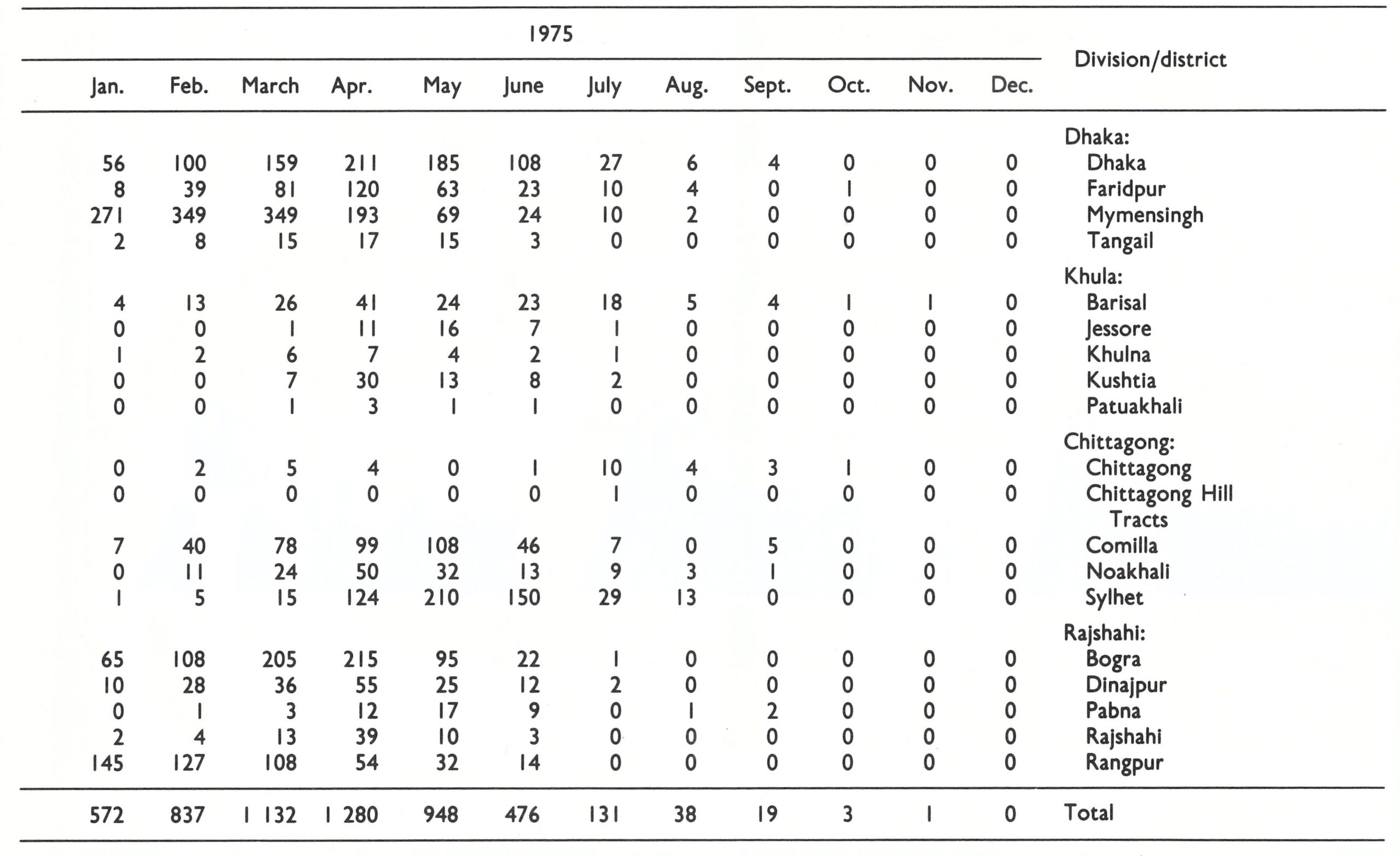
Table 16.12: Bangladesh: number of infected villages, by district and by month, 1974-1975
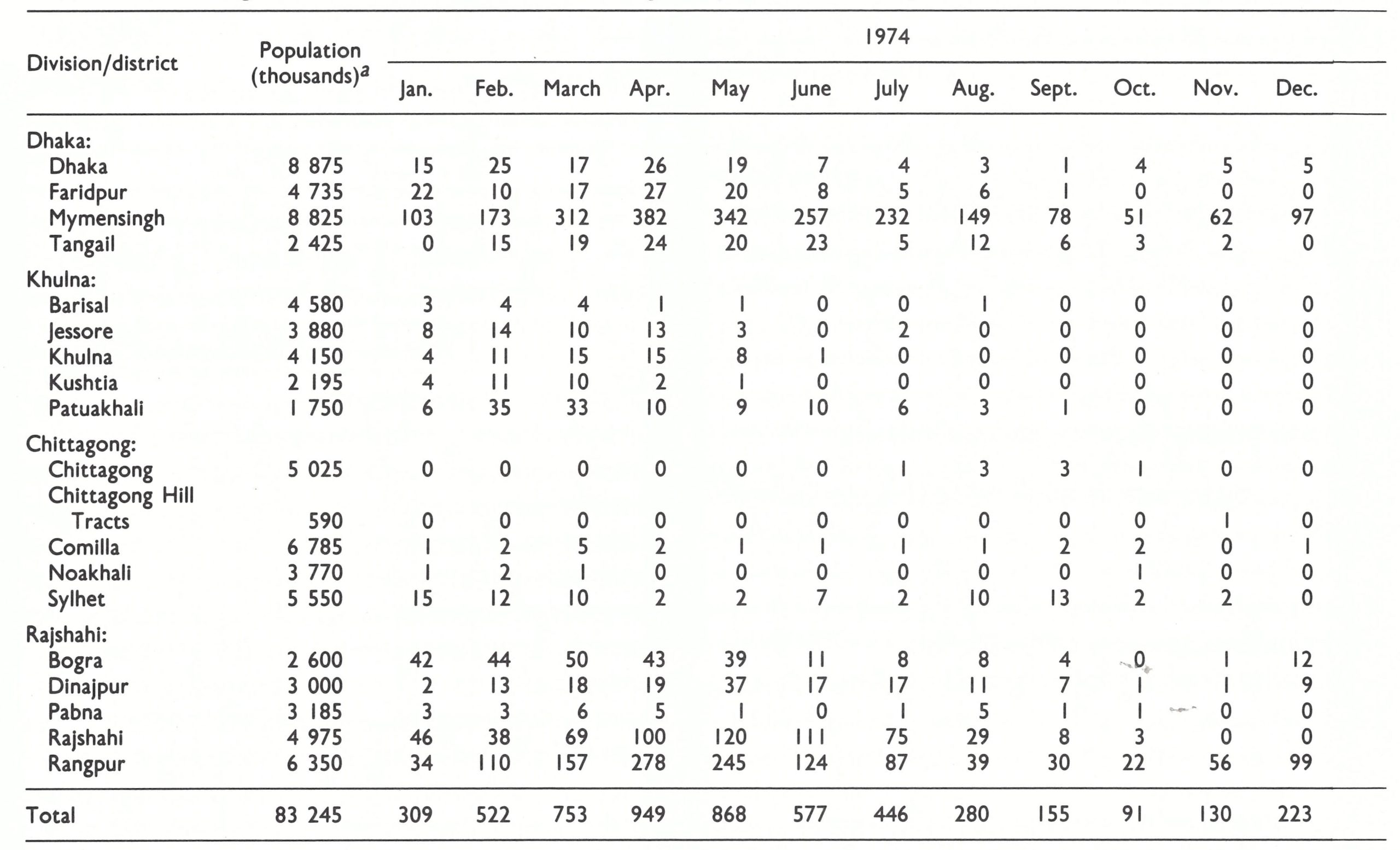
aEstimates calculated for 1977 as given by joarder et al.(1980).
Table 16.12: (continued)
AN EMERGENCY PLAN FOR SMALLPOX CONTROL, APRIL 1974 JANUARY 1975
By April, it was apparent to everyone that the integrated health service scheme was achieving little. A redefinition of the responsibilities of supervisors and workers and of the management structure was required. Accordingly, on 9 April the government issued a detailed “Emergency Plan for Smallpox Eradication under the Integrated Health and Family Planning Programme”, of which an important component provided for unified direction of the health services. Dr Mahboober Rahman, former director of the successful national malaria eradication programme, was asked to supervise all health activities, including smallpox eradication. Within the new administrative structure, responsibilities specific to smallpox eradication were defined . For operational purposes, new posts were created for staff at subdivision and thana levels. Civil surgeons, responsible for health matters in the subdivisions, were requested to appoint an area smallpox eradication officer for each of the 57 subdivisions and a thana smallpox eradication officer for each of the 424 thanas. In some areas, the incumbents were health services staff and in others malaria eradication staff. To assist family welfare workers in containment measures and to improve liaison with villagers, the order also authorized the temporary appointment and remuneration (6 takas, or about US$ 0.75, per day) of an emergency field worker for each outbreak. The field workers were to be recruited and trained in the villages. The employment of emergency field workers afforded an unexpected bonus in that they provided temporary accommodation in the villages for smallpox programme staff.
When a case of smallpox was discovered in a village, the family welfare worker was to cease other duties and initiate containment, with the help of the emergency field worker, and to inform his supervisors. The family welfare worker was to reside in the infected village for not less than 10 days and to vaccinate all its residents as well as all persons living within a half-mile (800 metres) radius. The newly designated than smallpox eradication officers were given the responsibility for organizing and coordinating all outbreak containment programmes. The area smallpox eradication officer was required to visit each thana not less than once a month and to send a weekly progress report to Dhaka.
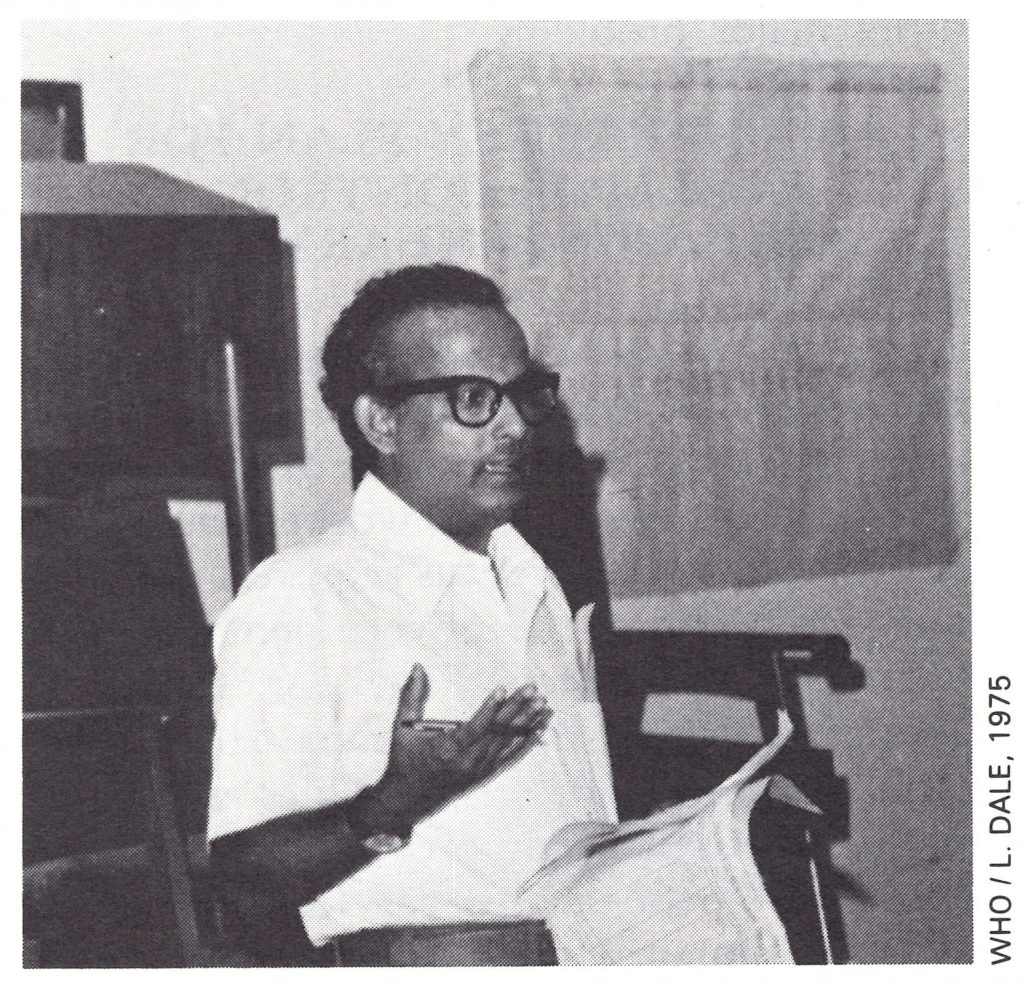
Plate 16.7. Mahboober Rahman (b. 1933), formerly director of the national malaria eradication programme, assumed overall direction of the integrated health programme in April 1974 and brought order to a chaotic administrative structure.
A monthly national meeting of all area smallpox eradication officers was instituted to review progress and to decide on plans for the next month. As was the case in India, the meetings proved to be especially valuable in motivating staff, in providing continuing education and in allowing for an ongoing appraisal of progress and any necessary redirection of the programme.
Each week an epidemiological report of newly detected cases and deaths was compiled at the subdivision level and sent by telegram to the national headquarters. A more detailed written report was prepared every month.
Provision needed to be made for the isolation of patients in the densely crowded areas of Bangladesh. Here it was a more difficult problem than in many other parts of the subcontinent. In rural areas, the patients could be isolated in their houses, but in the urban slums and in refugee resettlement camps, they had to be isolated in a special facility. In the cities and towns of Khulna, Chittagong, Sylhet, Rajshahi and Dhaka, there were infectious diseases hospitals which provided for the isolation of cases but, as elsewhere, they more often became centres for the dissemination of smallpox. Hospital superintendents rarely ensured that patients and visitors were vaccinated on entry. Consequently, smallpox eradication programme staff were obliged to organize and staff vaccination check-points at each hospital, sometimes with local police support. In heavily populated areas in which there were no hospitals, isolation wards or camps were set up in government buildings or even in tents, if necessary.
With 10 500 family welfare workers in the field, a defined supervisory and reporting structure, 25 special motorized surveillance teams, and 12 WHO epidemiologists, it seemed all but certain that transmission would be interrupted during the monsoon and post-monsoon period. Just 4 years previously, with far fewer surveillance teams, assisted by only 2 WHO epidemiologists, and a much less effective reporting system, transmission had been interrupted in less than 6 months.
The number of infected villages fell steadily, from 949 in April to 280 in August, of which 217 (78%) were in the northern districts of Rangpur, Rajshahi and Mymensingh. Even the distribution of the remaining outbreaks, similar to the pattern in 1970, suggested that the situation in 1974 might replicate that obtaining in 1970. The number of cases being detected remained high—1069
in August compared with 2110 in April (Table 16.13)—but detection was occurring earlier and more than 50% of all outbreaks consisted of only 1 or 2 cases. As an incentive for family welfare workers to report cases, it was decided in August to offer a reward of 50 takas (about US$6.50) to anyone who detected an outbreak. The system had proved successful in many states of India and its application at this time in Bangladesh seemed appropriate. Additional help was provided by the United Nations Relief Operation, Dacca (UNROD), which was in the process of concluding its activities; it turned over to the smallpox eradication programme a central transceiver and 8 field radios. Six more field radios were added later and thus a valuable network of communication was established between the smallpox eradication programme headquarters and epidemiologists in the field.
Table 16.13: Bangladesh: number of reported cases of smallpox, by division and by month, 1974
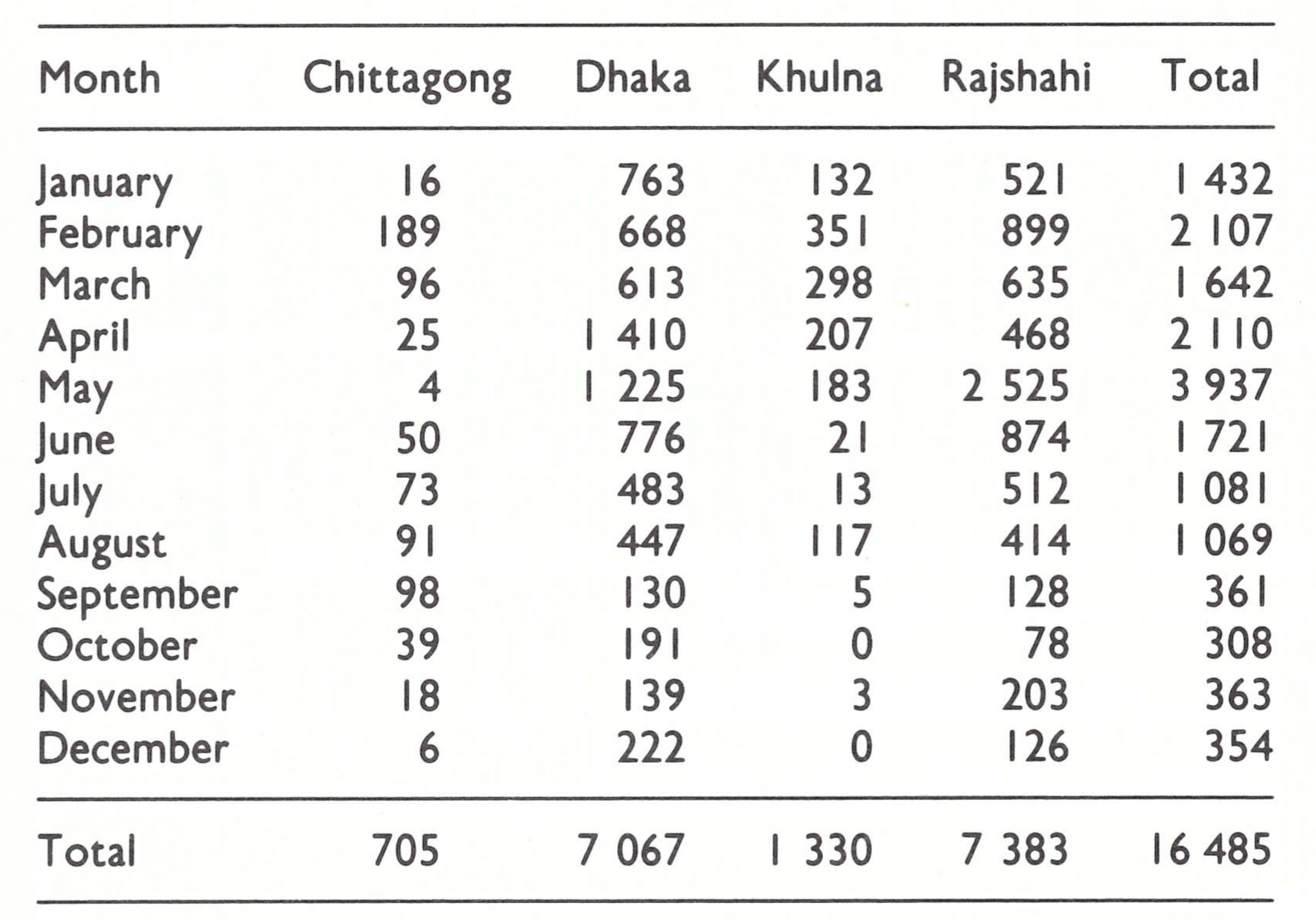
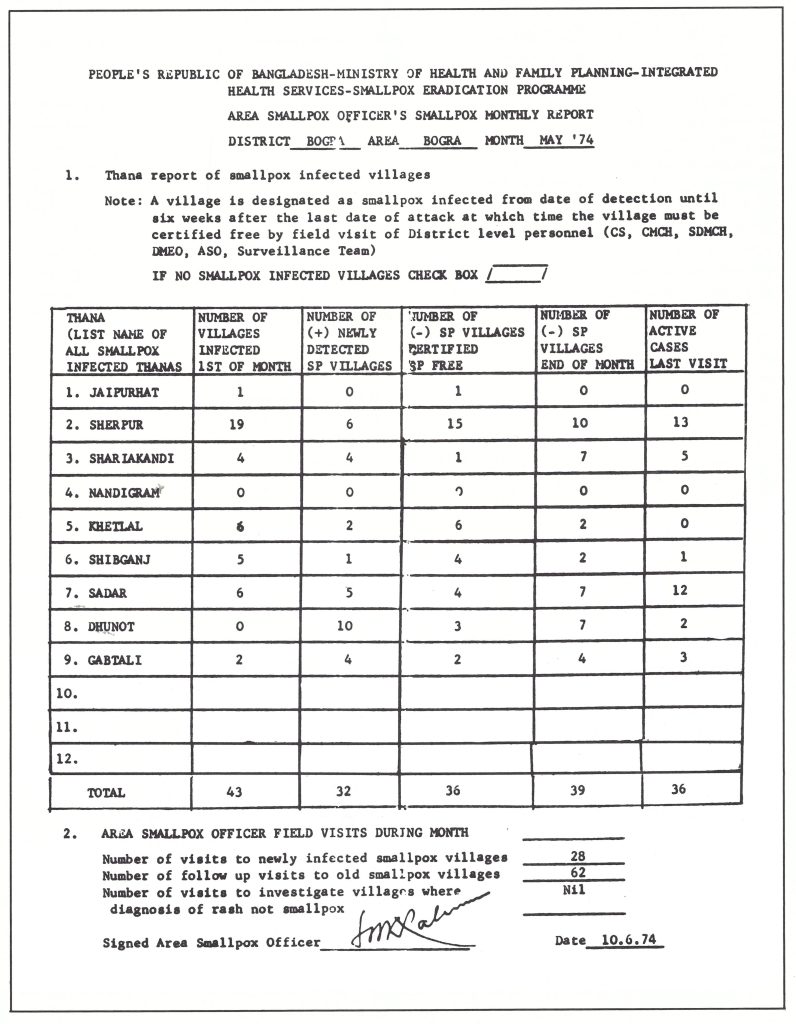
Plate 16.8. Bangladesh: example of monthly smallpox report.
In October 1974, only 91 infected villages remained, and periodic village-by-village searches were initiated. A similar search programme had begun in India a year before and more recently in Pakistan, but such searches in Bangladesh had not been possible before late spring because of the turmoil caused by the reorganization of the health services. During the monsoon months of 1974, national and WHO staff alike felt that searches were not required, in view of the existence of a unified health service and the assignment of a family welfare worker in each population unit of 5000 persons. Since each worker was expected to visit every house within his jurisdiction every 5 weeks and was motivated by the promise of a reward of 50 takas (about 5 days’ pay) for the discovery of a case, it seemed unlikely that many outbreaks would be missed. The initiation of a search programme in October was intended as the first stage in the development of a scheme to confirm that transmission had been interrupted rather than as an operational tool to detect cases, as in India.
The late summer months, however, had brought still another tragedy to Bangladesh. The most extensive and severe floods for more than two decades swept through major parts of the northern districts, where most of the remaining infected villages were located. Some refugees began to move from the area at that time, but in November and December, the season when crops were usually harvested, severe famine struck.
During the first week of October, only 24 cases were detected, but in succeeding weeks the numbers began to increase sharply. By mid-December, there were 168 infected villages, of which only 23 were outside the two flood-afflicted districts, but 20 outbreaks had occurred as a result of spread from these districts. Outbreaks were being detected unusually rapidly— 55% within a week of onset and 88% within 3 weeks. The containment of outbreaks was not optimum but, still, in 84% of them no cases were detected more than 21 days after the onset of the first case.
Because of population movement and crowding, however, smallpox spread explosively. In Rangpur District, a beggar living in a market-place died of smallpox on 2 December; 48 second generation cases in 18 villages occurred among those who had visited the market. In Faridpur District, south of Dhaka, a fatal case in a village was the source of 37 second generation cases in 4 different villages (WHO/SE/74.65, Rangaraj & Yusuf). In midDecember, cases were discovered among famine-stricken refugees in Dhaka and in the district towns of Bogra and Mymensingh. Efforts to control the spread of smallpox among refugees sleeping shoulder to shoulder in the extensive slum areas of the cities was an all but impossible task.
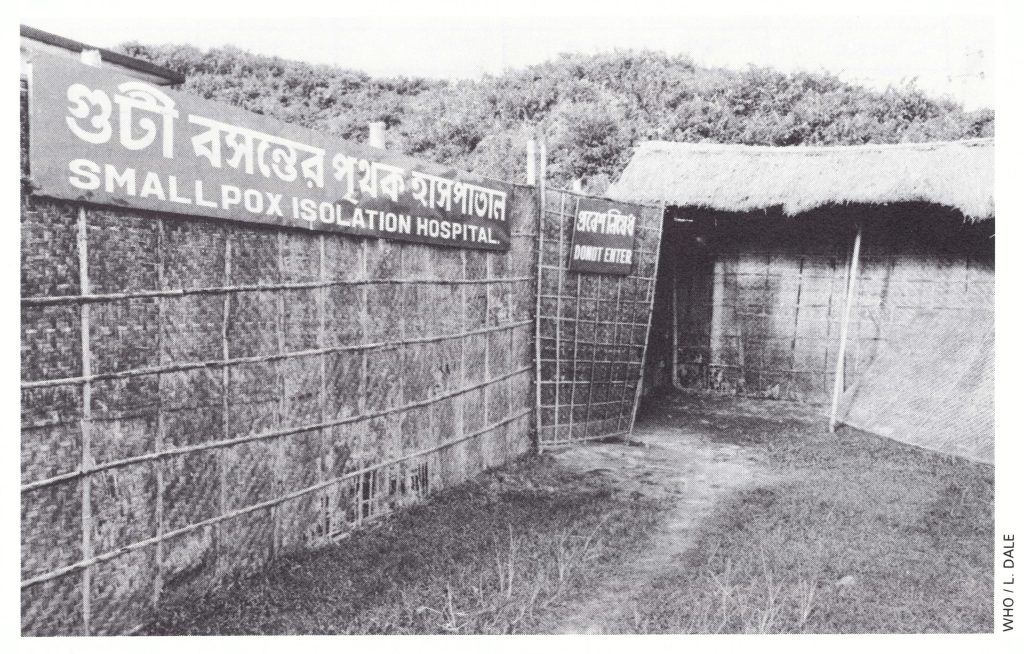
Plate 16.9. When isolation of smallpox patients in their own houses was not possible, hospitals were used, some of which were specially constructed, as was this one in Sylhet District.
An Episode Indicative of Frustration and Misguided Effort
In 1967, when the AID-supported regional programme began, all but 2 of the 21 countries (Equatorial Guinea and Guinea-Bissau) shown in Fig. 17.1 were independent States. Liberia had enjoyed sovereignty since 1847 but 18 others had become independent between 1957 and 1965. Thirteen had been colonies of France and were commonly referred to as francophone countries. These were the Central African Republic, Chad, the Congo, Cote d'Ivoire, Dahomey, Gabon, Guinea, Mali, Mauritania, Niger, Senegal, Togo and Upper Volta. Cameroon, which had been administered jointly by France and the United Kingdom, was officially bilingual. Four-namely, the Gambia, Ghana, Nigeria and Sierra Leone-had recently obtained independence from the United Kingdom.
By the autumn of 1974, Bogra District, once heavily infected, had interrupted smallpox transmission at the conclusion of a thoroughly competent but exhausting campaign. However, in late December 1974 and in January 1975, outbreaks began to recur following importations from the famine-stricken area to the north, and cases were detected in the municipality. The smallpox eradication staff were concerned about the prospects of wide dissemination of smallpox from an urban area and decided that a mass vaccination campaign throughout the city was urgently required. While such a scheme might seem attractive, similar efforts in the past had always proved costly in time and manpower and were rarely successful, in part because of the continual migration of the population. Following a 10-day house-to-house mass campaign, assessment revealed that only 50% of the inhabitants had been vaccinated. A second campaign proved no more successful. Yet a third campaign was organized, this time employing 3 WHO advisers who had been withdrawn from supervision of outbreak containment in rural areas. During the course of 2 weeks, with the staff working 15 hours a day, 7 days a week, a coverage of 93% was finally achieved . No sooner had this task been completed than a major privately sponsored fair opened which drew upwards of 20 000 visitors per day. Thenceforth outbreaks began to recur throughout the district, of which most could be traced to contact with infected persons at the fair. Efforts were made to persuade the organizers of the fair to close it down or to allow all those attending it to be vaccinated when they bought their tickets. The entrepreneurs, however, were also the principal civic officials and they were not anxious to discourage attendance by making vaccination a requirement. Six weeks of discussion were to elapse before the fair was finally closed by order of the central government. By then, Bogra was the world's second most heavily infected district. Not until May did smallpox begin to subside.
The occurrence at this particular time of the most widely celebrated Muslim holiday, the Eid festival (Id ul Fetre), further compounded the problem, since this feast was the occasion for large family gatherings, entailing extensive travel.
Meanwhile, in Nepal and Pakistan, transmission had been interrupted; in India, the incidence of smallpox and the number of infected villages were declining steadily. It became increasingly apparent that the course of events in Bangladesh would determine the success or failure of the endeavour to eradicate smallpox from Asia. Additional international staff were assigned to strengthen the programme in Bangladesh, the number increasing from 8 in June 1974 to 21 in January 1975 . But smallpox continued to spread. As has already been mentioned, only 91 villages were infected at the end of October, but the number had increased to 130 by the end of November, to 223 by the end of December, and to 572 by the end of January. This last number was almost twice the figure recorded for the corresponding period one year earlier.
A catastrophe from the viewpoint of smallpox eradication occurred when the government decided that urban bustees should be demolished. In a matter of a few weeks, bulldozers and police dispersed an estimated 50 000-100 000 additional refugees from the cities throughout the countryside. Some had smallpox or were then incubating the disease. A frustrated, demoralized staff was called upon to regroup and to mount yet another national effort.
Plate 16.10. Increasing numbers of staff and additional resources were provided to the programme in Bangladesh during 1974-1975 in a final intensive effort to eradicate smallpox from Asia. A: Andrew N. Agle (b.1937), a veteran of smallpox eradication programmes in western and central Africa, 1966-1971, then in Afghanistan, 1972-1974, was the WHO administrative officer in Bangladesh. B: Jane Brown (b.1942), seconded from WHO Headquarters for 6 months, directed radio communications. C: CARE, a private charitable organization registered in the USA, built an operations building, “Smallpox Zero”, to house additional programme staff. Additional buildings were constructed for the storage of parts and a garage for the maintenance of a new fleet of Indian-made jeeps.
NATIONAL MOBILIZATION FOR SMALLPOX ERADICATION, FEBRUARY 1975
Beginning in December 1974, national health personnel and WHO staff stationed in Bangladesh, New Delhi and Geneva met repeatedly to decide on a revised strategy and additional measures that might be taken. With the extensive continuing movement of population, it was apparent that efforts would need to be greatly intensified, and that substantial additional funds would be required . However, WHO’s Voluntary Fund for Health Promotion, as well as discretionary funds in the WHO regular budget, had been exhausted in strengthening the programme in India. Additional support would have to be sought, but this would require the approval by the Bangladesh Planning Commission of a revised plan of operations and the concomitant financing. Although the Secretary of Health and the WHO Representative in Bangladesh supported the programme, they were of little help. Both were adamant that eradication could be achieved only through a national mass vaccination campaign conducted through the basic health service structure. They were not persuaded by the argument that this would be futile in an already well vaccinated population, nor could they accept the fact that the newly created basic health service structure had all but ceased to function. Fortunately, the recently appointed principal health adviser to the Planning Commission, Dr Mohammad Ataur Rahman, had a far better and more realistic understanding of the problem and the resources needed. Dr Rahman was a knowledgeable and skilful administrator and virologist who had played a key role in the development of smallpox vaccine production in Dhaka, and subsequently had closely followed the progress of the eradication programme. Through his efforts, the Planning Commission was persuaded to direct an appeal for assistance to a number of international agencies. The Swedish International Development Authority responded—as it had in India—most rapidly and generously, making available US$ 3.5 million. Significant contributions were also made by Canada, Denmark, Norway and the United Kingdom.
In February 1975, a presidential directive was issued which declared smallpox to be a national emergency and ordered the mobilization of all available resources to assist in its eradication. Thirty-five jeeps of Indian manufacture were hurriedly procured and driven to Bangladesh ; others were loaned from other programmes. Additional radios, motor cycles, boats and outboard motors were obtained. Mr Rodney Hatfield, a young volunteer from OXFAM (a charitable organization registered in the United Kingdom), assumed responsibility for transport maintenance and repair; an old garage was transformed into a fully equipped workshop with a staff of 12 mechanics; and numerous Ministry of Health vehicles that had long been in disrepair were made roadworthy. An operations building was rapidly constructed by CARE (a charitable organization registered in the USA), using a new technique of jute and fibre-glass construction. To coordinate field operations, WHO’s former senior smallpox adviser in Afghanistan, Dr A. G. Rangaraj, joined the staff. Dr Stephen Jones and Dr Donald Francis came from India to assist in adapting the most effective techniques employed there to conditions in Bangladesh.
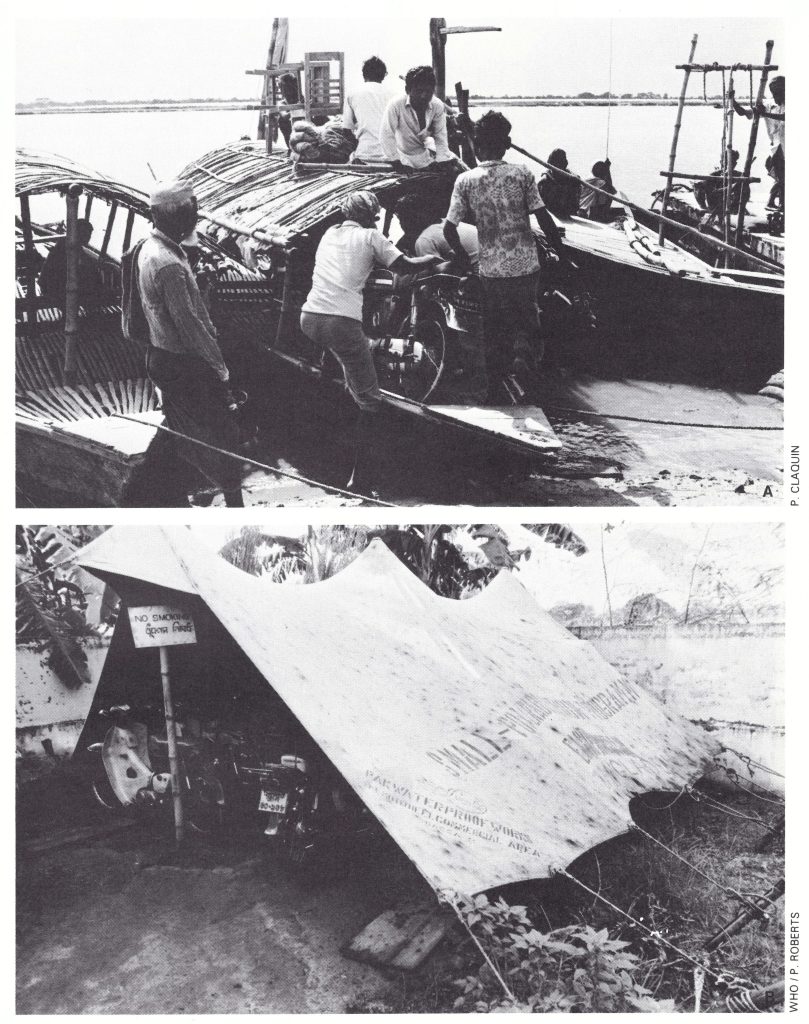
Plate 16.11. A: Small motorcycles were very useful for travelling around the country as they used little petrol, could be readily carried on boats and could be used on the narrow footpaths connecting villages. B: The smallpox programme motor park in Rangpur District in September 1975.
Numerous other WHO staff and consultants were urgently recruited from countries around the world (Table 16.14), many of them having served in Africa, South America and other parts of Asia. It was a group remarkably diverse in nationality, being composed of Brazilian, British, Czechoslovak, Egyptian, French, Soviet, Swedish and Swiss citizens. The Center for Disease Control and OXFAM were especially helpful in recruitment. New colleagues arrived every 2 weeks, to rendezvous in New Delhi for a Monday briefing. On Tuesday they flew to Dhaka and over the next 3 days received intensive field and classroom training before being dispatched to the field. Because there was a shortage of hotel accommodation, a house was leased which could accommodate 18 persons—unofficially called WHOSE House (an acronym for World Health Organization Smallpox Eradication). By May, 71 international staff were working in the field, and during that month the recruitment of Bangladeshi epidemiologists from universities and other settings was initiated.
A formidable challenge was presented by the administrative coordination and financial monitoring of a programme which, operating with US$12 000 a month in September 1974, was spending US$125 000 a week by February 1975. This daunting task was capably handled by Mr Andrew Agle, who had served in the western Africa and Afghanistan eradication programmes and had joined the Bangladesh programme staff in September 1974. He and Mr A. Alim Mia, a Bangladeshi administrator who had served with the programme since its inception, dealt with a considerable array of problems, both expected and unexpected. One of the more vexing was that of disbursing funds to the field epidemiologists for the payment of temporary staff to cover board and lodging, as well as petrol and repairs. The telegraphic transfer of funds to bank branches in peripheral areas would have been the most logical way of coping with the problem, but was technically impossible for many months. The only workable alternative approach was to disburse the funds at monthly meetings of supervisory field staff. However, the largest banknote then available was a 10-taka note (about US$1.25) and, during the intensive period of activity, field staff were receiving 30 000 takas or more each month. The inevitably large bundle of banknotes was difficult to handle, but the problem was solved by using capacious gunny sacks and carrying them into the field tied to the back of a motor cycle; although there was no attempt at concealment, thefts never occurred.
Table 16.14: Bangladesh: averange numbers of international staffaand national epidomiologists employed in the smallpox programme, by 3-month period, 1972-1977b
 a In all, 207 International staff from 28 countries served in Bangladesh at some time during this 4-year period.
a In all, 207 International staff from 28 countries served in Bangladesh at some time during this 4-year period.
bFrom joarder et al. (1980).
Under the national mobilization plan, and with many additional field epidemiologists available, containment measures were greatly expanded from previous strategies which called for one family welfare worker and one emergency field worker to vaccinate everyone living within a half-mile (800-metre) radius of each case. The containment measures were basically the same as those that had evolved in India.
A worker who discovered a case was instructed to isolate the patient immediately and to vaccinate all household members. A resident supervisor was appointed, usually the health worker in the area, who recruited 4 house guards responsible for keeping the patient in the house and for vaccinating all visitors. Food and water were provided if needed. (For the recording of activities, special “house guard books”, such as had been used in India, were introduced in April.) The resident supervisor then hired 4-6 emergency field workers at 6 takas each a day. He trained them to register and vaccinate all residents and visitors within a half-mile radius of the infected house, and to search for cases in all markets, schools and houses within a 2-mile (3.2-kilometre) radius (Fig. 16.13). When these tasks were completed, the workers revisited all persons within the half-mile radius to detect and vaccinate any newcomers or others who had been missed during the intensive vaccination phase.
Resident supervisors were provided with a “containment book” in which the following information was recorded :
- a list of patients and the stage of their illness ;
- information pertaining to the source of infection and contacts of the cases ;
- a list of household members and temporary residents of Zones A and B (i .e., those living within a 100-yard (90-meter) and a half-mile (800-meter) radius, respectively, of the infected house) ;
- a list of staff and work schedules for all involved in containment ;
- a record of visits of supervisory staff from than, subdivision and district levels ;
- a map of the outbreak area showing each house, all houses being numbered ;
- a record of all financial transactions .g ., payments to emergency field workers for petrol, etc.
Plate 16.12. WHO consultants. A: Pierre P.L. Claquin (b.1947), a French epidemiologist, engaged for 3 months in March 1975, eventually spent a total of 27 consultant months in Bangladesh. B: T. Stephen Jones (b.1941) was one of the many epidemiologists provided to WHO by the Centers for Disease Control in the USA. He served for 3 months in India in 1974 before spending 3 months in Bangladesh in 1975.
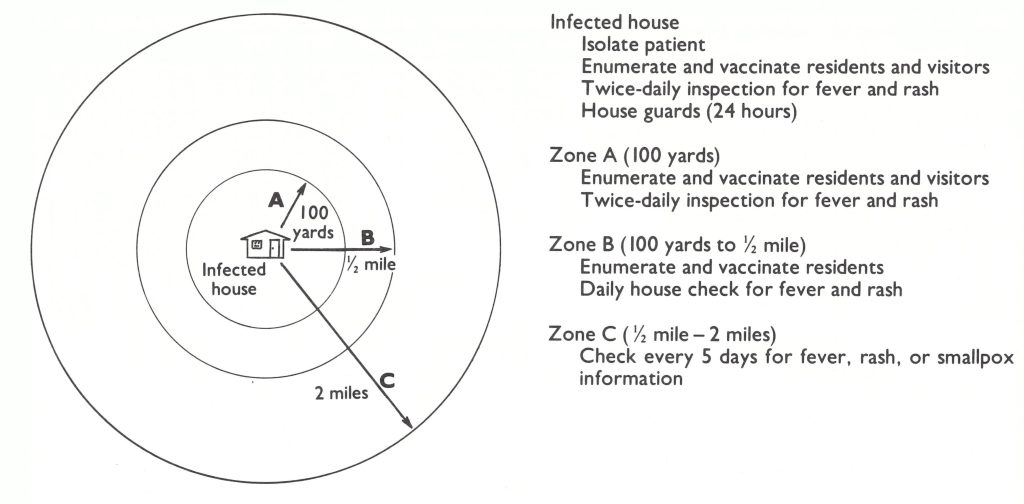
Fig. 16.13. Bangladesh: containment of smallpox outbreaks.
Check-points were set up on strategic paths and roads to collect information about other areas in which cases might exist and to vaccinate passers-by.
The source of infection of each case was examined and all possible contacts were vaccinated. Any contact with fever was isolated and members of the household were vaccinated. Whenever the suspected source of infection was in another than, or whenever a contact had left the village for another area, a special message (cross-notification) was sent by messenger, telegram or radio. District, subdivisional and thana officers, surveillance teams and epidemiologists made periodic surprise visits to assess the efficacy of the work.
At the monthly meetings of supervisory field staff, problems were reviewed and procedures changed as required. An example of an unexpected event was the discovery by a Bangladeshi epidemiologist, Dr M. A. Sabour, that in 11 out of 17 outbreaks for whose containment he was responsible, cases were recorded 15 days or more after containment had begun. As he discovered, most of the cases were relatives of patients and should have been identified and vaccinated. He learned, however, that when a family in an infected home was asked to give the names of all recent visitors, they omitted to mention the names of relatives-since relatives, in their culture, were not considered to be visitors. The steady improvement of containment could be measured by the diminishing proportion of outbreaks in which cases occurred more than 15 days after detection of the outbreak (Fig. 16.14). In November, cases occurred in 27% of the outbreaks more than 15 days after detection ; by June, the proportion was less than 10% (Foster et al., 1980).
With increasing numbers of epidemiologists in the field to investigate the source of outbreaks, to trace contacts who might have left the scene of an outbreak and to discover rumours of outbreaks as yet undetected, many possible additional cases were identified in more distant areas. The radio network was used extensively to forward such information for other staff to investigate. Beginning in February 1975, each cross-notification was recorded and the results of the field investigations were tabulated (Table 16.15). Between February and December 1975, 1468 cross notifications were transmitted, leading to the discovery of 28 previously unknown outbreaks not a large yield for the number of reports transmitted and investigated but important, nevertheless, in hastening the interruption of transmission. Three additional outbreaks were discovered through notifications received from India.
Dr A. B. M. Kamrul Huda
Dedication and sacrifice were characteristic of many who served the programme, and a few gave their lives. One young medical officer who did so was serving at the time as the Subdivisional Medical Officer of Health in Chittagong. He was notified late one night of possible smallpox on an offshore island and arose early the next morning to take a ferry to the island. Because of high winds the ferry was cancelled. Dr Huda was anxious to investigate the rumour and took a small local boat instead. The boat capsized en route and Dr Huda drowned. He died on 3 March 1975, leaving a wife and two young children.
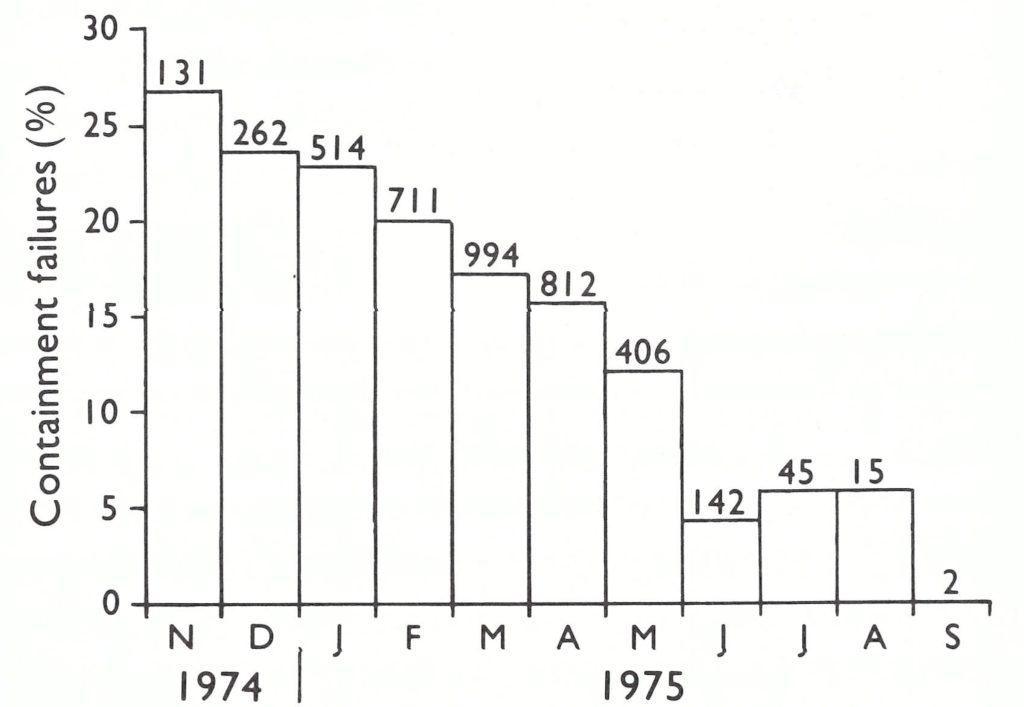
Fig. 16.14. Bangladesh: number of smallpox outbreaks per month, November 1974-September 1975, and the proportion with cases occurring 15 days or more after the outbreak was detected and in which containment measures were considered to have failed.
Table 16.15: Bangladesh: cross-notifications of suspected cases of smallpox within the country, 1975
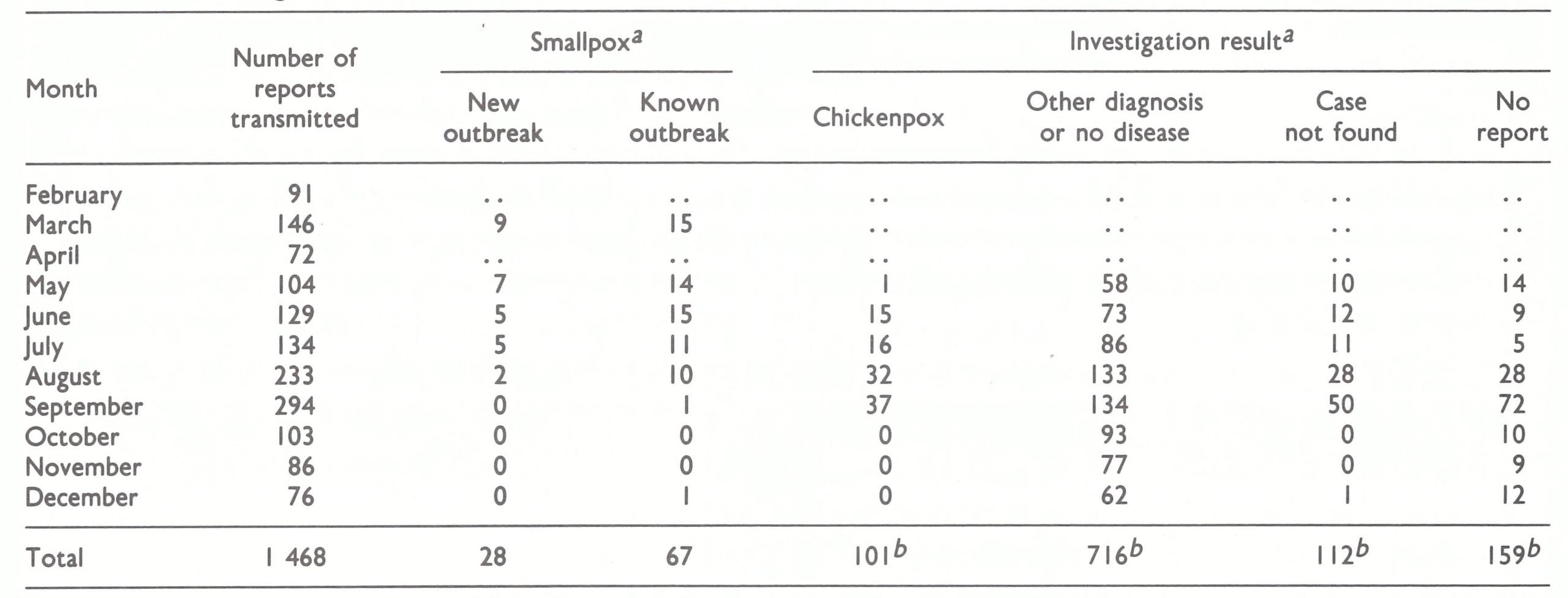 a ..=data not recorded.
a ..=data not recorded.
b Totals for May-December only.
SPECIAL SEARCH PROGRAMMES
A special 6-day village-by-village search for cases had first been organized in October 1974 and a second was conducted in December of that year. It was believed that if the family welfare workers could be carefully instructed to perform well only one of their many assigned functions—i .e ., that of smallpox case detection during a 6-day tour of their area—the results would be better than if this activity were but one of the numerous tasks required of them. Thana supervisors reported that the searches in October and December were reasonably successful but assessment by district and subdivision staff and surveillance teams indicated that there were large areas in which no search had been carried out and few in which searches had been conducted competently.
With additional staff to assist in supervision, some of whom had had experience with this technique in India, more energetic search programmes were introduced in April 1975; these were repeated every 4-6 weeks. Approximately 14 500 staff were engaged in each search, following special training programmes at each operational level.
The workers were asked to visit markets, tea-stalls and every 20th house. They were instructed to show the smallpox recognition card at each location, and ask the viewers whether they recognized the disease—which most of them did. The health workers were told to inform their audience of the reward for reporting an unknown case of smallpox and where to report it; to record any information obtained about persons with rash and fever, including the deaths of any of them; and to report cases to the thana supervisor.
After each survey, 1500 villages were randomly selected to assess the efficacy of search. Assessment in Bangladesh was greatly facilitated by the fact that every house in the country was numbered—a practice begun by the staff of the malaria eradication programme and kept up by the smallpox eradication personnel. An assessment of the results of the April search revealed that surprisingly few villagers knew of the reward for reporting a case. On further investigation, it was found that health workers, wanting to claim the 50-taka reward for themselves, did not publicize it. This situation was corrected in May, when the reward was offered both to the person who reported the outbreak and to the first health worker to confirm it. The April assessment showed that only 30% of villagers knew of the reward, but by September this proportion had increased to 70%.
In contrast to the experience in India, the number of outbreaks discovered during each search was not high (Fig. 16.15). However, in India, the reward was not offered until many searches had been conducted, while in Bangladesh its existence was announced even before the first searches began . The searches in Bangladesh were more effective in increasing public awareness of the reward and in stimulating reporting than in detecting outbreaks. As an illustration, a review of the last 119 outbreaks which occurred showed that 55 (46%) had been detected by reports from the public and 37 (31%) by surveillance teams (Fig. 16.16).
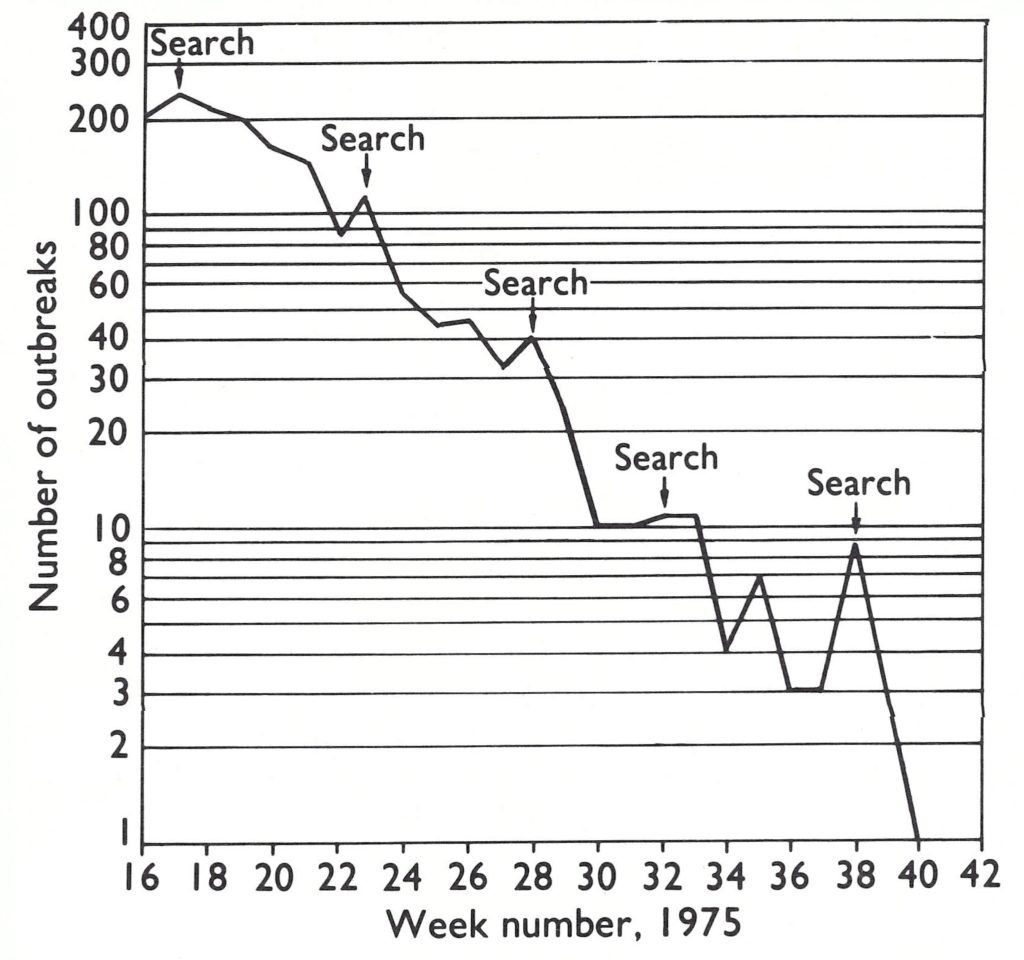
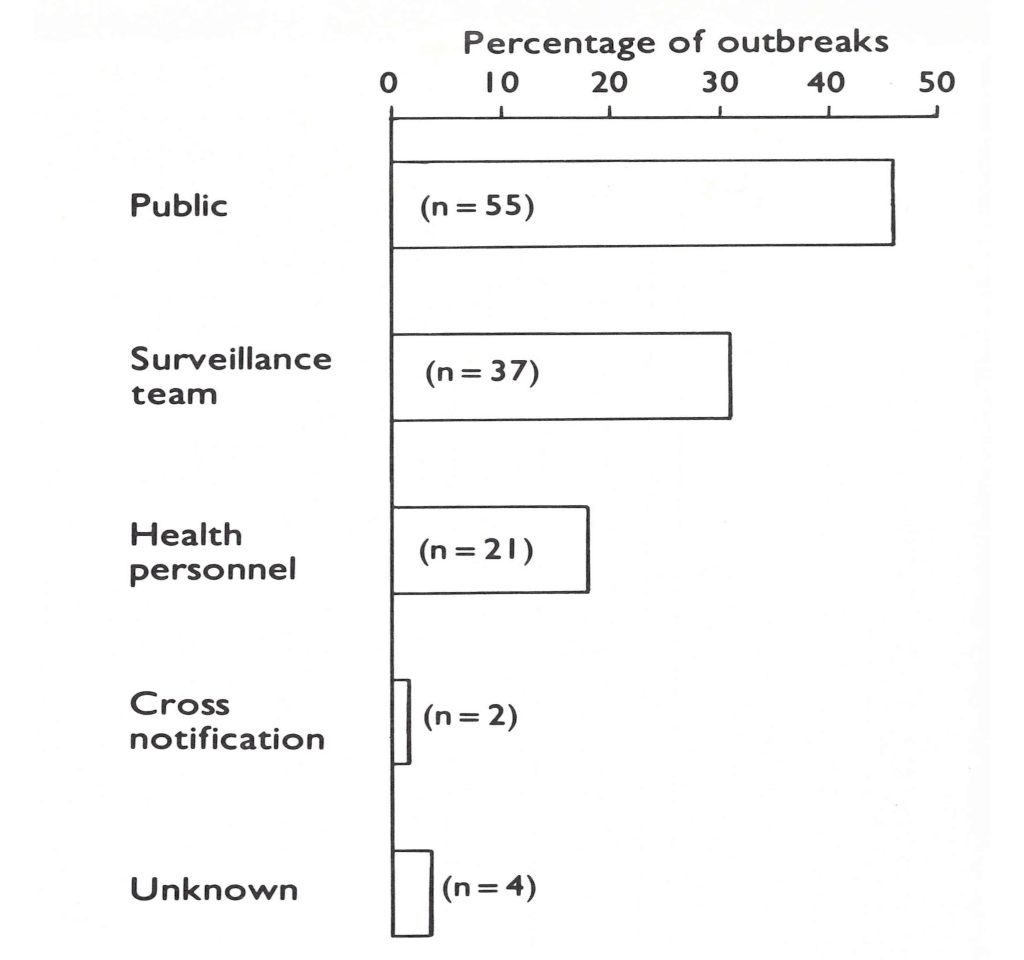
Fig. 16.15. Bangladesh: number of outbreaks detected by week, 1975.
Fig. 16.16. Bangladesh: source of report of the last 119 outbreaks of smallpox.
The number of personnel engaged in the programme was far larger than it had ever been. An estimate during the 3-month period of greatest activity revealed that an average of almost 12 000 persons were working each day (Table 16.16).
Between February and April, the number of reported cases steadily increased, from 1703 in February to 2467 in March and to 3948 in April. Smallpox appeared to be as great a problem in 1975 as it had been in 1974 although, on the basis of later surveys, it was estimated that 83 % of all cases were reported in 1975 compared with only 49% in 1974 (Hughes et al ., 1980).
The occurrence of epidemic smallpox extending throughout Bangladesh for a fourth year was politically uncomfortable for the Secretary of Health, a former surgeon. He fully accepted the idea of mass vaccination but was uneasy about the concept of a programme for detecting cases and containing outbreaks. The success of surveillance-containment operations in 1970 did not convince him. His personal experience with smallpox control in the Ministry had been confined to the period since Bangladesh’s independence, and for the last 4 years optimism had been expressed by the staff during and immediately after the monsoon each year, but epidemics and emergency programmes inevitably followed in the spring. For advice he turned most often to the WHO Representative in Bangladesh, a public health physician but one who understood neither smallpox epidemiology nor the eradication strategy any better than the Secretary of Health. With smallpox incidence rising and with increasing international interest as to whether Bangladesh could or would be able to stop transmission, tensions were great. The Secretary of Health and the WHO Representative repeatedly and vehemently demanded that the surveillance-containment programme should be stopped and the entire population vaccinated forthwith. Dr Mahboober Rahman and his national and WHO colleagues argued that mass vaccination was futile, that vaccinial immunity was already high and that the surveillance-containment approach offered the only possible solution. Indeed, the level of vaccinial immunity, as shown in a 1976 national survey was 91% overall.
However, without notice to the programme staff, the Secretary of Health would periodically order the health staff in a district or subdivision to stop all other activities and to vaccinate everyone in the area concerned. Usually, this was accompanied by threats of punishment if any unvaccinated person was discovered at the end of 7 days or some such brief period. After lengthy discussions, the Secretary would eventually be persuaded to rescind the order, but, not infrequently, for many days outbreak containment programmes were abandoned and surveillance was stopped. Further problems occurred when the Secretary and the WHO Representative made one of their frequent visits to the field. The Secretary would announce that on his trip, he would stop at villages along his route and expect to find that every single person had been vaccinated. A flurry of activity ensued to vaccinate everyone along the route he was expected to follow, again at the expense of outbreak containment measures. An even more serious problem arose when he required senior staff to pledge to resign if cases of smallpox were found after a certain date, an action which resulted in the suppression of reports of cases . The problem was not finally resolved until April, when the WHO Representative returned to Geneva and was replaced by the able Dr Eung Soo Han. The Secretary’s continuing concern about his and his country’s image was reflected in May 1975 by his decision not to attend the World Health Assembly. Instead, he dispatched Dr Rahman to respond to the anxious inquiries he knew would be expressed about the Bangladesh smallpox eradication programme.
Table 16.16: Bangladesh: personnel employed during the 3-month period of maximum containment of the smallpox eradication programme, May-July 1975
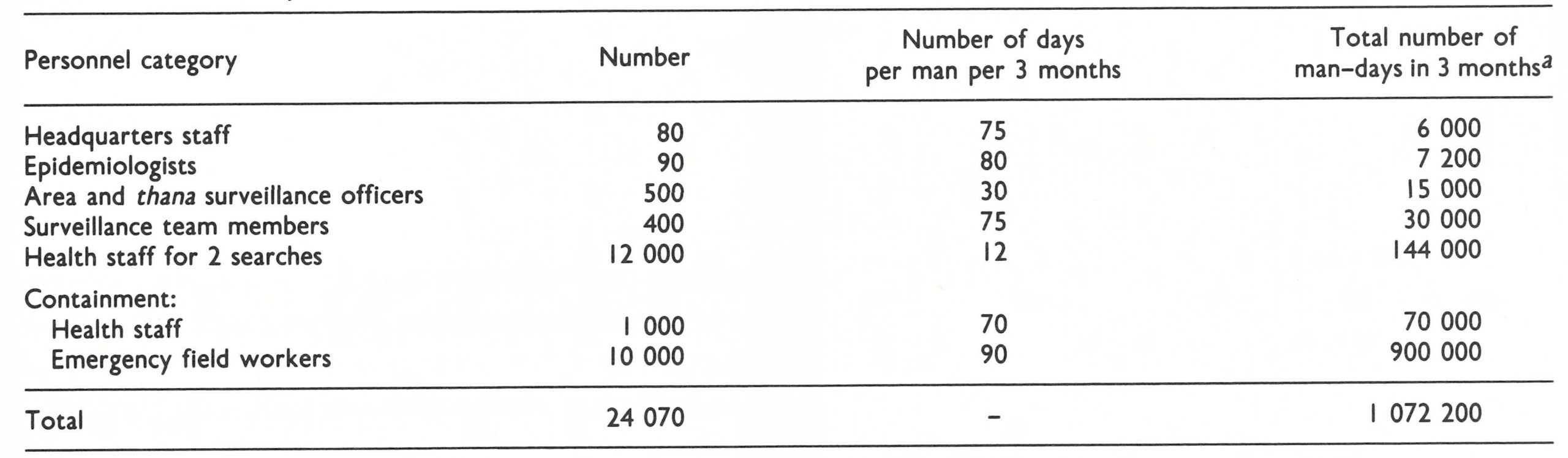 a The number of man-days per month totalled 357 400, or an average of 11 913 persons working every day.
a The number of man-days per month totalled 357 400, or an average of 11 913 persons working every day.
THE FINAL CHAPTER
From April to August, the number of nfected villages decreased at a substantially more rapid rate than in preceding year—from 1280 in April to 131 in July. The staff began to chart weekly the number of “active cases” still present—i.e.., the number of cases in which the scabs had not yet been shed. In a progress report to WHO staff in July 1975, Henderson wrote: “Some years ago . . . we had plotted progress on a country and provincial basis, subsequently on a district basis and then by blocks/thanas. In now monitoring the numbers of individuals capable of transmitting infection, I believe we’ve reached a final stage.” The last case in India, the last of 32 importations from Bangladesh, occurred in May, leaving Bangladesh the only endemic area in the whole of Asia. The search in July detected 33 outbreaks and that in August only 7. With the extensive resources available and a programme functioning so well, the end once again appeared to be in sight. There was, however, one further tragic event.
On 15 August, Sheik Mujibur Rahman, the first President of Bangladesh, revered as the father of the country, was assassinated in a military coup. The airport was closed and the borders sealed. Communications by radio were suspended for 2 weeks and although field staff continued to work, movement in and out of Dhaka was limited. Fearing that vehicles might be seized, the smallpox eradication staff hurriedly dispersed them from the motor pool to locations all over the area. For nearly a month, most of the staff remained apprehensive that civil war might again occur and, with it, the movement of hundreds of thousands of refugees—and renewed epidemics of smallpox. India, meanwhile, greatly strengthened its complement of staff in border areas. Fortunately, the country remained quiet, the monsoon rains were plentiful, an excellent crop was harvested and the enormous movement of refugees ceased.
The post-monsoon period was not, however, without incident, as a Japanese scientific team arrived in Dhaka bringing with them a new laboratory technique for the rapid diagnosis of smallpox. It was a propitious moment at which to undertake the investigations, since Dr Farida Huq, a highly competent virologist, was present in Dhaka at that time and able to perform confirmatory studies on specimens from suspected cases. The new immunofluorescence technique seemed capable of identifying variola virus in pus or scabs within hours (instead of days) after a specimen had been submitted. Only 19 villages were infected in September as the team began its work, but many of the first specimens examined were reported as positive for variola virus. Surveillance teams were then taking many specimens from cases which they had diagnosed as chickenpox, simply to confirm by laboratory test that smallpox was not present. Many of these specimens were reported to contain variola virus and for weeks consternation and bewilderment prevailed as containment operations were begun and then stopped in numerous presumed outbreaks. There was a strong suspicion that something had gone seriously awry when immunofluorescence staining showed that material taken from a boil on the back of one of the WHO advisers contained variola virus. A technique which had worked well in the laboratory had failed when used in the field, and was soon stopped (Tarantola et al., 1981).
Plate 16.13. Smallpox eradication programme offices in the field were simple but functional like this one in Chandpur Thana.
THE LAST OUTBREAK
When the conflicting laboratory and clinical data had been resolved, it became clear that smallpox transmission had apparently been terminated—the last known case having occurred on 14 September. Over the succeeding weeks, 8 previously undetected outbreaks were discovered in Patuakhali, Barisal and Dhaka but in none had cases occurred after 14 September. The monthly programmes of systematic search continued and, except in these three districts, independent assessement showed excellent results. At the beginning of November, civil disorder erupted, with local fighting breaking out in three different parts of the country. The United Nations was sufficiently concerned to recall its personnel to Dhaka. Only the WHO smallpox eradication staff remained in the field. But no additional cases could be found.
The progress of the smallpox campaign in Asia had been followed closely by the press, which believed, as did the personnel involved, that eradication of smallpox from Asia was the most formidable obstacle to global eradication. Early in November, 6 weeks after the onset of the last case, the only active outbreak in Asia was scheduled to be removed from the list. It was agreed, however, that caution was required and an additional 2 weeks should be allowed to elapse before an announcement was made. No cases occurred, and on 14 November 1975 WHO announced at a press conference that 2 months had passed since the onset of the last case in Bangladesh; and while the intensive search for cases would continue in Bangladesh and other countries, there was at that time no known patient in the whole of Asia, indeed in the world, with variola major. On the following day, 15 November, the eradication programme’s telex control room received the following cable from the densely populated Bhola Island, off the southern coast:
“ONE SUSPECT SMALLPOX CASE DETECTED VILLAGE KURALIA [UNION COUNCIL SOUTH DINGALDI [POLICE STATION BHOLA DATE OF DETECTION 14/11/75 DATE ATTACK 30/10/75 CONTAINMENT STARTED DETAILS FOLLOW”.
(The date of onset was later confirmed to be 16 October 1975.)
A team of epidemiologists immediately left Dhaka for Bhola Island expecting to find a misdiagnosed case of chickenpox. They reached the infected house only after a 24- hour journey by speedboat, steamer, jeep, motor cycle and finally on foot. The diagnosis was not in doubt: it was smallpox, and this was confirmed days later by the laboratory. Everyone was concerned. It was November, the monsoon was over, and the season when smallpox was most rapidly transmitted was at hand. If there was one case, there had to be others in the chain of transmission.
Bhola Island, located at the mouth of the Ganges, had a population of 960 000 and an area of approximately 2600 square kilometres. Regular ferries connected the island with the mainland and other islands and these were heavily used.
In 1970, Bhola had been devastated by a tidal wave, which was followed by a relief operation that included a smallpox vaccination campaign. Because of this, the proportion of persons with a vaccination scar was higher than in most of the country. During 1974 and 1975, few smallpox cases had been reported. However, in August 1975, it was discovered that a medical officer had failed to report known outbreaks. Subsequently, surveillance had been reinforced, and since the beginning of August 141 cases and 33 deaths had been detected. All but 2 of the outbreaks, one of 43 cases and one of 44, had ceased before discovery. Once again, investigation revealed the suppression of reports and so, early in October, an additional surveillance team had been sent from another area, the Bhola surveillance team reorganized, and an epidemiologist posted to the island for fulltime work.
On 6 November 1975, while conducting a search of markets, the Bhola surveillance team received information about an outbreak in Kathali village. During the course of investigating and tracing the sources of infection, the team discovered outbreaks in 3 other villages with cases extending back to 2 March. A search began within a 5-mile (8-kilometre) radius of each of these villages. During a tea break in one of the markets, the surveillance team obtained information about the death of a person with rash in the village of West Joynagar, 5 kilometres to the south.
The death had been reported to the thana smallpox eradication officer, who had sent a family welfare worker to investigate. His conclusion had been that the death was caused by measles. On investigation, the surveillance team was in no doubt that it was due to smallpox. A search revealed an outbreak of 7 cases and 3 deaths. One of the patients was a heavily pockmarked 8-year-old girl who informed the team that there were other cases in Kuralia village, some 200 metres to the west of her house. Investigation there revealed 2 cases, one of which was in a 10-year-old boy whose onset of illness was on 6 October and the other in a 3-year-old girl, Rahima Banu, who had become ill on 16 October.
By the time of investigation, Rahima Banu was the only known patient with active smallpox in all of Asia. Accordingly, extraordinary efforts were begun immediately to contain the outbreak and to discover other possible cases. The surveillance team which had detected the outbreak was soon joined by teams of epidemiologists from Dhaka and other areas. A launch brought vaccine, light transport (motor cycles and bicycles), speedboat engines, drums of petrol, kerosene lanterns, loudspeakers and other equipment. The patient, who still had a few scabs on her legs, was isolated at home. House guards were posted 24 hours a day; food and money were supplied to the family so that no one would have to leave the house. Vaccination of the 18 150 people living within a radius of 12 miles (2.4 kilometres) of the infected house was begun immediately. This task included day and night house-to-house vaccination, the enumeration of every household member, the checking of vaccination results, and the vaccination or revaccination of any newcomers to the village.
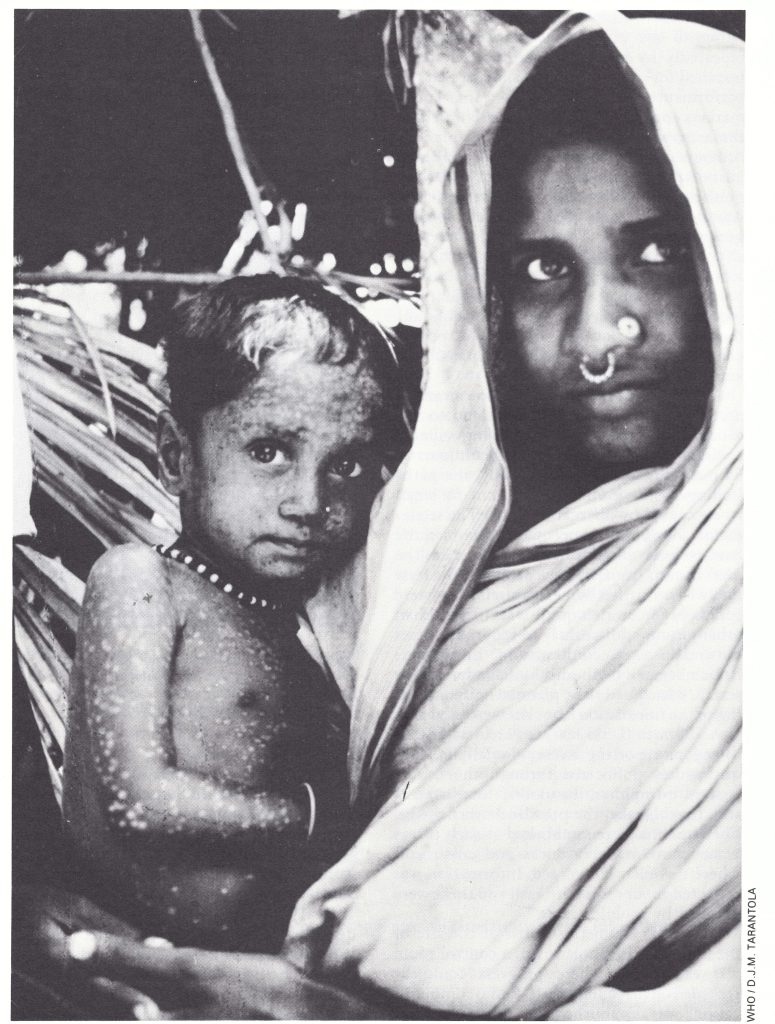
Plate 16.14. Rahima Banu, a 3-year-old girl from Bhola Island, Bangladesh, was the last case of smallpox in Asia and the last naturally occurring case in the world of variola major, the more virulent form of the disease. Her illness began on 16 October 1975, approximately 3 weeks before this picture was taken. The depigmented areas of her skin are sites where lesions were present. eradication programme offices in the field were simple but functional like this one in Chandpur Thana.
The area within a 5-mile (8-kilometre) radius of the infected house was searched repeatedly by successive teams; each team searched for cases with fever and assessed the performance of the preceding team. The 7 markets and 9 schools, as well as all healers in the area, were visited repeatedly to pick up rumours of other cases. Each house on Bhola Island was searched by health staff under the guidance of epidemiologists and surveillance teams, which had been allocated specific geographical areas. This search also covered all public meeting-places such as markets, schools and tea-shops. Whenever it was reported that a member of any household in the outbreak area had left, the responsible authorities were notified so that the person concerned could be found, vaccinated and kept under surveillance.
A difficult problem was the poor means of access from the centre of the island to the shore, where most of the outlying villages could be reached only after a difficult journey by bicycle or on foot. Frequently, the paths leading to these villages were cut by small rivers caused by fluctuating tides. The settlements along the shore were occupied by landless peasants or fishermen, who were the most distant from health centres and the least likely to be visited by health staff. They were generally much less well vaccinated than other groups and unlikely to report any cases of smallpox. Accordingly, a dispensarylaunch began a methodical village-by-village search, which had to be planned daily according to the tides. Local launches were used also.
A 500-taka (US$33.00) reward was offered to anyone reporting a case of smallpox. This was widely publicized through the use of posters, pamphlets, handbills, loudspeakers and, from Dhaka, the press and other media. Check-points were established at such places as bus stations, ferry docks and crossroads, where travellers converged. Information was collected about cases with rash and these were checked by mobile teams.
About 10 kilometres north of the site of the outbreak, in Bhola town, a control room was established where progress could be recorded on maps and charts. Radio communication was established to permit regular contact between the control room, the dispensary-launch travelling along the shore areas, and Dhaka.
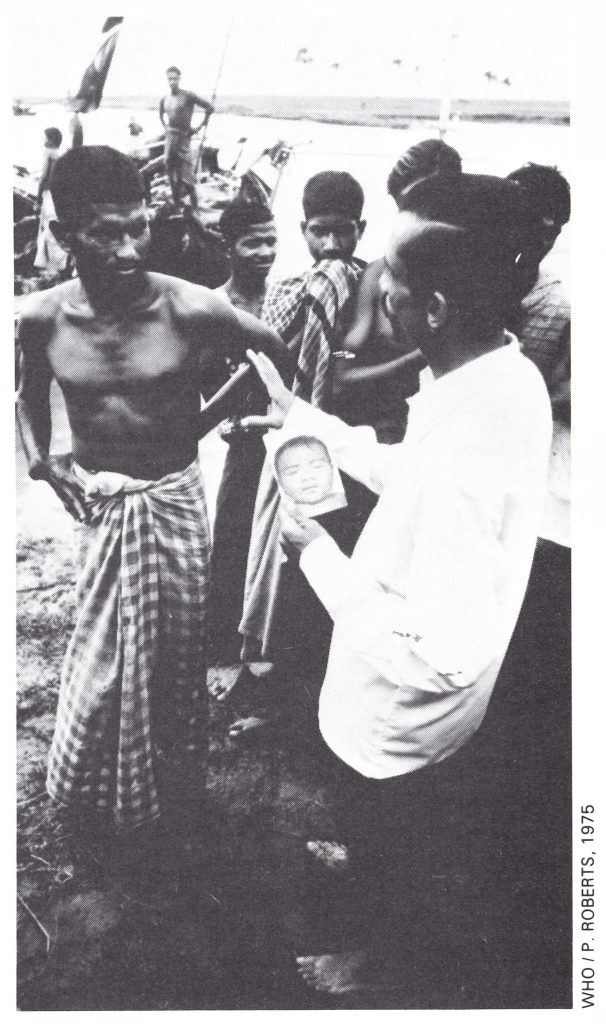
Plate 16.15. Mohammed Matiur Rahman (b.1932), a medical officer with the national programme in Bangladesh, questioning villagers about possible smallpox cases during the search on Bhola Island.
The health staff engaged in this outbreak alone (within a 5-mile radius) consisted of 3 epidemiologists and more than 40 health staff and temporary workers. For the rest of the island there were 3 epidemiologists, and 180 specially deputed health workers to assist the subdivisional staff in the house-to-house searches. In addition, 16 emergency field workers worked at check-points and conducted municipal searches.
By 19 November, the fifth day after the discovery of the outbreak, the first round of vaccinations within the 12-mile radius of the infected house had been completed. A second round was begun, covering the same area, and was completed 8 days later. Of a listed population of 18 150, 16 295 were vaccinated. A later assessment showed that 100% of the residents living within a half-mile radius and 95% of those living within a 11/2-mile radius of the infected house had been vaccinated.
Meanwhile, 2 consecutive house-to-house searches within the 5-mile radius were completed by 8 December. Among the 120 000 population, 52 individuals with fever and rash were found, including 17 with chickenpox and 11 with measles, but there were no cases of smallpox. During the following 2 months, 2 additional house-to-house searches of Bhola Island were conducted. During these operations, 2 more unreported smallpox outbreaks were discovered: one had occurred in 1974 and had resulted in 18 cases and 6 deaths; the second involved 1 person, who had become ill in July 1975.
At the end of December, the additional staff who had been sent to Bhola began to be recalled to their respective districts. Kuralia was declared smallpox-free and the 2-year post-epidemic surveillance period commenced.
MORBIDITY AND MORTALITY DATA
To obtain precise data on the age distribution and case-fatality rates for smallpox, special studies were undertaken in 1976 to enumerate all cases and deaths in 165 outbreaks, including 115 that constituted the last outbreaks in the country, and 46 others, which were investigated in northern Bogra District. In all, 1127 cases were recorded (Table 16.17).
Cases occurred among all age groups but the youngest were the most heavily afflicted. Of the total, 55% occurred among children under 10 years of age, a group that made up only 34% of the population. Overall, the casefatality rate was 18%, comparable to that in India. The much higher case-fatality rate among males over 20 years than among females in the same age group was notable but no explanation was found for this disparity.
Table 16.17: Bangladesh: cases of and deaths from smallpox and case-fatality rates in 165 outbreaks, by age and sex, 1975
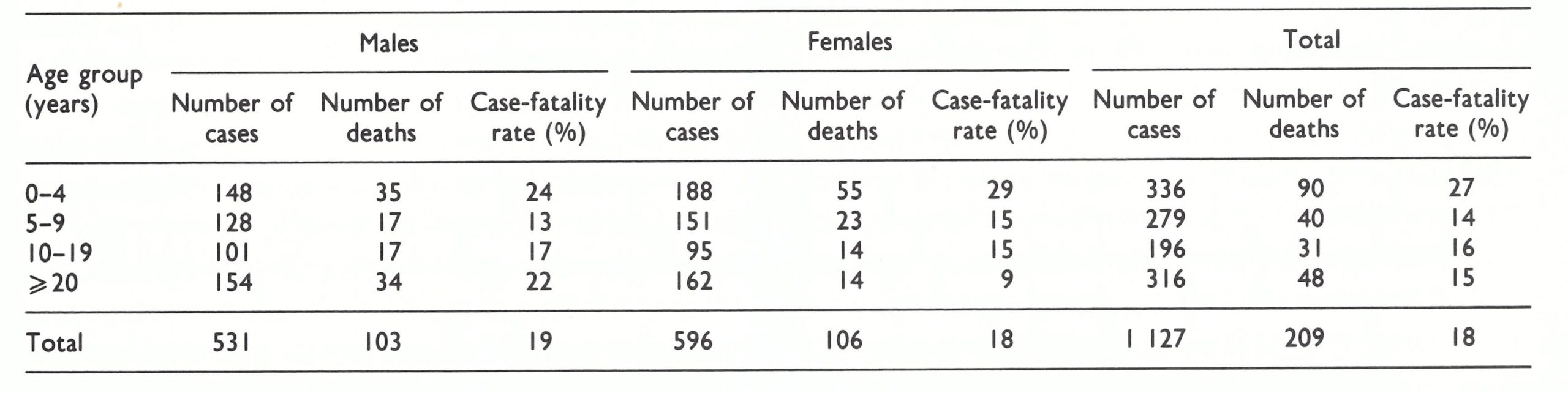
CONCLUSIONS
The programme in Bangladesh was uniquely distinguished by extremes with peaks of optimism and success alternating with catastrophic setbacks resulting from natural disasters of flood and famine and man-made disasters inflicted by civil war and the disruptive reorganization of the health services. The frustration and pessimism of the programme staff during the spring of 1975 were matched only by the feelings of their counterparts in Bihar State, India, 6 months earlier and are vividly depicted in the book Quest for the Killers (Goodfield, 1985).
The successful application of a surveillance-containment programme in the spring of 1970 had so rapidly and so easily interrupted transmission that it was difficult to believe that the success could not be repeated in 1972 or in the 2 succeeding years. In retrospect, the 1970 experience in Bangladesh to some extent paralleled events in India, where, for example, transmission was so rapidly interrupted in Tamil Nadu State (population, 41 million) in 1968 and in Gujarat State (population, 27 million) in 1971. These successful programmes engendered unwarranted confidence that transmission could be quickly interrupted in a population already reasonably well vaccinated and with so numerous a health staff available. What was not appreciated was the dearth of supervision of the host of health workers in many parts of India and in Bangladesh. Given optimum conditions of population stability, vigorous and enlightened senior programme leadership and the application of surveillance-containment measures at a declining or low point in the long-term periodicity of smallpox, a modest surveillance-containment programme was rapidly and dramatically successful. When natural or man-made disasters created hordes of refugees, when leadership was deficient or when smallpox was at the height of its periodic wave, it became apparent that the health structure had little in reserve with which to cope with the situation.
Progress in programmes in the northern and eastern states of India had been disappointing and frustrating, but within little more than a year after the special intensified national programme began in September 1973, transmission was interrupted. In Bangladesh, however, the interruption of transmission, once successfully achieved, was frustrated in each of 3 successive years by unexpected disasters. With courageous confidence, bolstered by material support from Sweden and other countries, a remarkably diverse national and international staff made one more heroic effort in 1975 and succeeded in attaining their goal. If civil war had broken out in August 1975, following the assassination of Sheik Mujibur Rahman, transmission would probably have persisted for at least another year and might perhaps still be occurring. History records, however, that Rahima Banu was the last victim of variola major—on 16 October 1975.
Robneb
September 1, 2025In today's fast-paced world, staying informed about the latest advancements both domestically and globally is more crucial than ever. With a plethora of news outlets competing for attention, it's important to find a trusted source that provides not just news, but perspectives, and stories that matter to you. This is where [url=https://www.usatoday.com/]USAtoday.com [/url], a top online news agency in the USA, stands out. Our dedication to delivering the most current news about the USA and the world makes us a key resource for readers who seek to stay ahead of the curve. Subscribe for Exclusive Content: By subscribing to USAtoday.com, you gain access to exclusive content, newsletters, and updates that keep you ahead of the news cycle. [url=https://www.usatoday.com/]USAtoday.com [/url] is not just a news website; it's a dynamic platform that empowers its readers through timely, accurate, and comprehensive reporting. As we navigate through an ever-changing landscape, our mission remains unwavering: to keep you informed, engaged, and connected. Subscribe to us today and become part of a community that values quality journalism and informed citizenship.