Chapter 21:
Ethiopia, Yemen and Democratic Yemen

INTRODUCTION
The execution of successful eradication programmes was a challenge to all countries, but for those which in 1967 had only just begun to develop national infrastructures for health, transport and communication it presented a staggering problem. Ethiopia, with a population of 25.5 million (in 1970), was by far the largest and most populous of countries in this category. Across the Red Sea lay the much smaller states of Yemen (population, 4.8 million) and Democratic Yemen, with its sparse population of 1.5 million (Fig. 21.1). The problem was complicated by civil strife, which was present in all 3 countries either at the beginning or during the course of the Intensified Smallpox Eradication Programme.
In 1967, smallpox was considered to be endemic in both Ethiopia and Yemen; Democratic Yemen, which had reported no cases since 1961, was provisionally categorized as smallpox-free. Because health services were sparse and so few persons were routinely vaccinated, it was feared that the incidence of smallpox in Ethiopia and Yemen might be among the highest in the world; also, the smallpox-free status of Democratic Yemen had to be regarded with some scepticism.
Recognizing that effective national eradication programmes would take time to establish, WHO began to explore the possibility of developing such programmes in each of the 3 countries as soon as the Intensified Programme was launched in 1967. Four years elapsed, however, before eradication activities had been established in all 3 countries. Plans for a programme in Yemen had been discussed by government and WHO staff as early as 1959, a plan of operations had been signed in 1961 and some vaccine had been provided. However, a civil war broke out which lasted 5 years, and little could be achieved until 1969, when a revised plan of operations was agreed on and a special smallpox eradication unit created within the Ministry of Health. Democratic Yemen embarked on a programme in 1970 and, finally, in 1971, Ethiopia followed suit—the last of the countries which had endemic smallpox in 1967 to participate in the Intensified Programme.
The programmes were each very different in character and operated independently of one another. Epidemiologically, they were also distinct. Despite their geographical proximity, none of the 3 countries is known to have imported cases from either of the others after 1967.
Yemen began a systematic vaccination campaign in 1969 in urban districts and areas accessible by road. After little more than a year, during which 1 million vaccinations were performed, the campaign quickly deteriorated to the point that 5 years elapsed before another million persons were vaccinated. After the programme had begun, only 29 poorly documented cases were recorded in 1969, and none thereafter. From 1971 to 1977, specimens were obtained from 26 suspected cases but none showed evidence of variola virus. Although WHO provisionally reclassified Yemen as a nonendemic country in 1970, this decision was grounded primarily on the absence of reported cases; little other information was available. Because the reporting system was poor and surveillance all but nonexistent, the true status of smallpox remained uncertain until 1978. In that year, a carefully conducted national survey confirmed the absence of smallpox during recent years and suggested that the disease had indeed been absent since 1969.
Between 1970 and 1972, Democratic Yemen conducted an extensive vaccination campaign in and around Aden, the capital city, and in 1973 extended it to other parts of the country. Surprisingly, only 1 case of smallpox was reported, in 1968, but this report was subsequently retracted, it being alleged that the case had been one of misdiagnosed chickenpox.
Ethiopia’s participation in smallpox eradication did not begin until 1971, and up to 1975 the government gave it limited support. Two factors were primarily responsible (1) national and international malaria eradication programme staff had initially opposed undertaking a programme which they believed would adversely affect their own activities; and (2) when the smallpox eradication programme finally began, it was discovered that only the mild variola minor form was present in Ethiopia, and among the many health problems confronting the government, this disease was not of major consequence. During the first 4 years of the programme, fewer than 100 Ethiopian health personnel, WHO staff and international volunteers, travelling mainly on foot and on muleback, struggled desperately to contain widespread and persistent smallpox. The task was made more difficult by the wide dispersal of the population, more than half of whom lived more than a day’s walk from any sort of road in extraordinarily rugged terrain; by a rudimentary governmental infrastructure ; and by a dearth of health facilities and manpower. Continuing civil war, hostile groups who resisted vaccination, famine and flood further complicated the effort. Yet, surprisingly good progress was made with the limited resources available. However, smallpox persisted stubbornly throughout vast rural areas, in contrast to the situation in Yemen, in which control measures in the few urban areas were quickly succeeded by the interruption of transmission in the country as a whole. Following the eradication of smallpox in Asia in 1975, greater resources could be made available to Ethiopia, and the new revolutionary government gave substantial additional support. An intensified programme with more adequate resources succeeded in interrupting transmission in August 1976.
The 3 national programmes are described in this chapter in chronological order of commencement, beginning with a brief account of activities in Yemen and Democratic Yemen and concluding with a more detailed description of the Ethiopian programme, which was one of the most difficult, complex and imaginative of any national eradication campaign. In this chapter, the spelling of Ethiopian geographical names adopted by the Ethiopian Mapping Agency in 1978 has been followed (Tekeste et al.,1984).
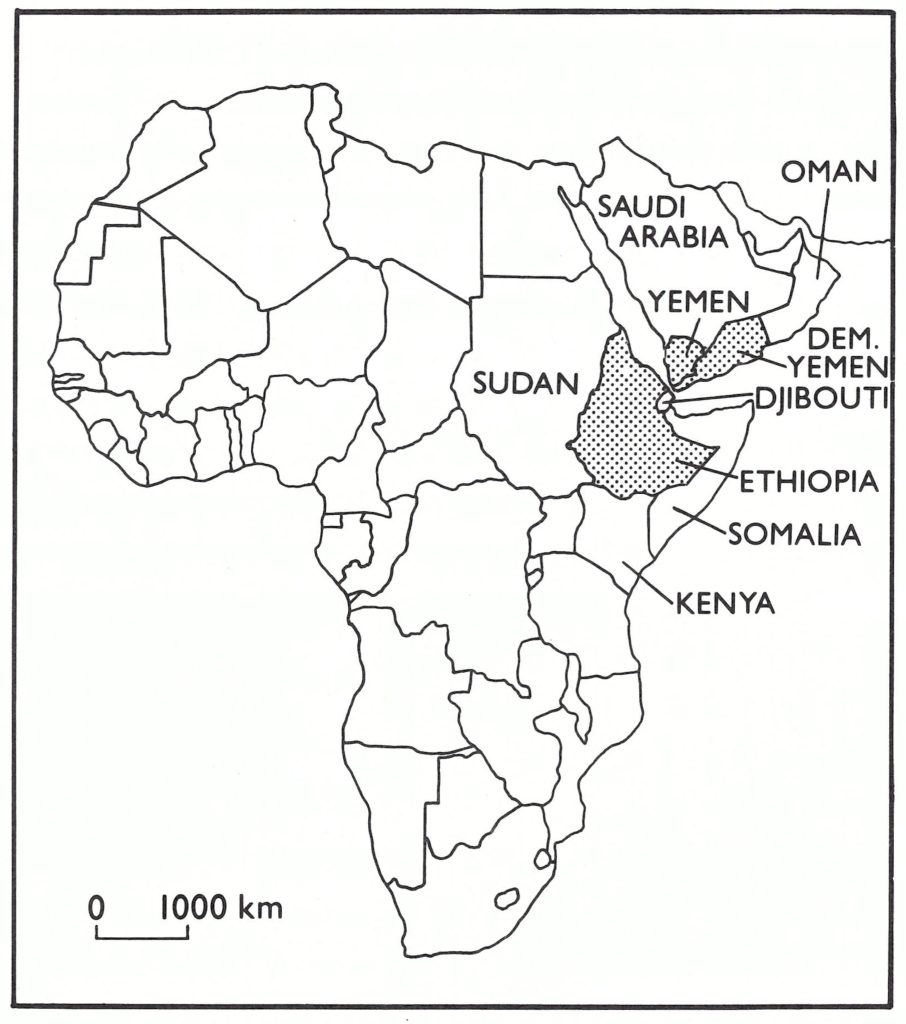
Fig. 21.1. Horn of Africa and adjacent countries.
YEMEN
Yemen, the most densely populated country in the Arabian Peninsula, is situated on an ancient route used by pilgrims, many of them from Asia and some from Africa. After travelling by sea to the port of Aden, 100 kilometres to the south of Yemen, or to other ports on the Arabian Peninsula, or overland, many pilgrims passed through Yemen on their way to Mecca.
The country has an area of 195 000 square kilometres and consists of 3 different geographical regions. The first is a hot arid semidesert strip, 30-70 kilometres wide, extending along the shores of the Red Sea and inhabited, in 1967, by perhaps 20% of the population, many of African origin. The second area, inhabited by 75% of the population, is a high plateau, about 100 kilometres wide, with densely populated river valleys and scattered villages among rugged mountains. The third area, in the east of the country, is a sparsely populated arid desert in which, in 1967, not more than 5 % of the population lived.
Until 1962, when it became a republic, Yemen had been ruled by feudal tribal leaders and was largely isolated from the outside world. According to the first census, taken in 1975, 5.2 million persons were living in the country, and an estimated 1.2 million were working abroad, mainly in Saudi Arabia. Less than 1000 kilometres of roads connected the 3 main towns, Sana’a (population, 100 000) and Taiz (population, 30 000) in the mountains and Hodeida (population, 50 000) on the coast. Most of the population lived in an estimated 15 000 villages, the majority of which could be reached only on foot or on muleback.
During the rule of the tribal leaders, neither health nor educational facilities had been widely developed and such facilities as did exist were primarily confined to the 3 main towns. When the country became a republic in 1962, efforts were made to introduce a modern form of central government, but they were severely hampered by 5 years of civil war. In 1967, more than 90% of the population was illiterate and few people had access to either curative or preventive health services. As recently as 1978, 70% of the 162 districts in the country had no health facilities whatsoever.
Little is known about smallpox in Yemen, there having been no national reporting system until 1975. However, because of the relative isolation of the population, outbreaks were probably infrequent in much of the country. Data from what had been the Protectorate of South Arabia, which included the port of Aden, now the capital of Democratic Yemen, show few or no cases and very few deaths in recent decades, until 1957, when 65 cases with 19 deaths were recorded. The source of infection was reported to have been Pakistan. Outbreaks continued in the Protectorate between 1957 and 1961, and smallpox may well have spread from Aden to Yemen, in which an epidemic started in 1957 or 1958 and continued for several years. It was said to have resulted in not less than 30 000 cases and 18 000 deaths. Assistance from WHO was requested and a team was sent to investigate in June 1959. The team found no active cases in Sana’a, the capital city, but noted large numbers of persons with facial pockmarks. A report from a village of 800 inhabitants stating that only 200 of them had survived the epidemic was indicative of its severity. The evidence, such as it is, suggests that a severe epidemic of variola major had occurred among a population which had experienced little smallpox in recent decades.
During succeeding years, some vaccine was provided by WHO and through bilateral assistance. Vaccination was made available in hospitals in the 3 major towns and at the 20 or so health centres when outbreaks occurred. However, not more than 15 000 or 20 000 individuals were vaccinated each year. In 1962, with assistance from WHO, a national vaccination campaign commenced. Forty vaccinators were recruited and trained; the population of Sana’a was vaccinated in a house-to-house campaign, but thereafter these activities diminished with the gradual intensification of civil strife. Reports obtained during the certification procedure in 1978 suggest that the epidemic of variola major subsided in 1963. WHO was officially notified by Yemen of the occurrence of 5 cases of smallpox in 1964, of 1 case in 1966 and of 3 in 1967, but nothing more is known of these cases or where exactly they occurred. Reporting at that time was not good and Table 21.2. Yemen: number of vaccinations per WHO did not endeavour to elicit more com-formed and number of reported cases plete information about cases until the of smallpox, 1967-1975 Intensified Programme was well under way.
In 1967, Yemen was provisionally classified by WHO as an endemic country with the expectation that an effective surveillance programme would probably reveal many hundreds, if not thousands, of cases. Because one of the principal routes of the Mecca Pilgrimage passed through it, Yemen constituted a potential focus for the spread of smallpox to Africa and other countries of Asia. The early initiation of an eradication programme was therefore thought to be vitally important. However, a coup d’etat in 1967 and continued fighting between republican and royalist forces delayed the start of the work.
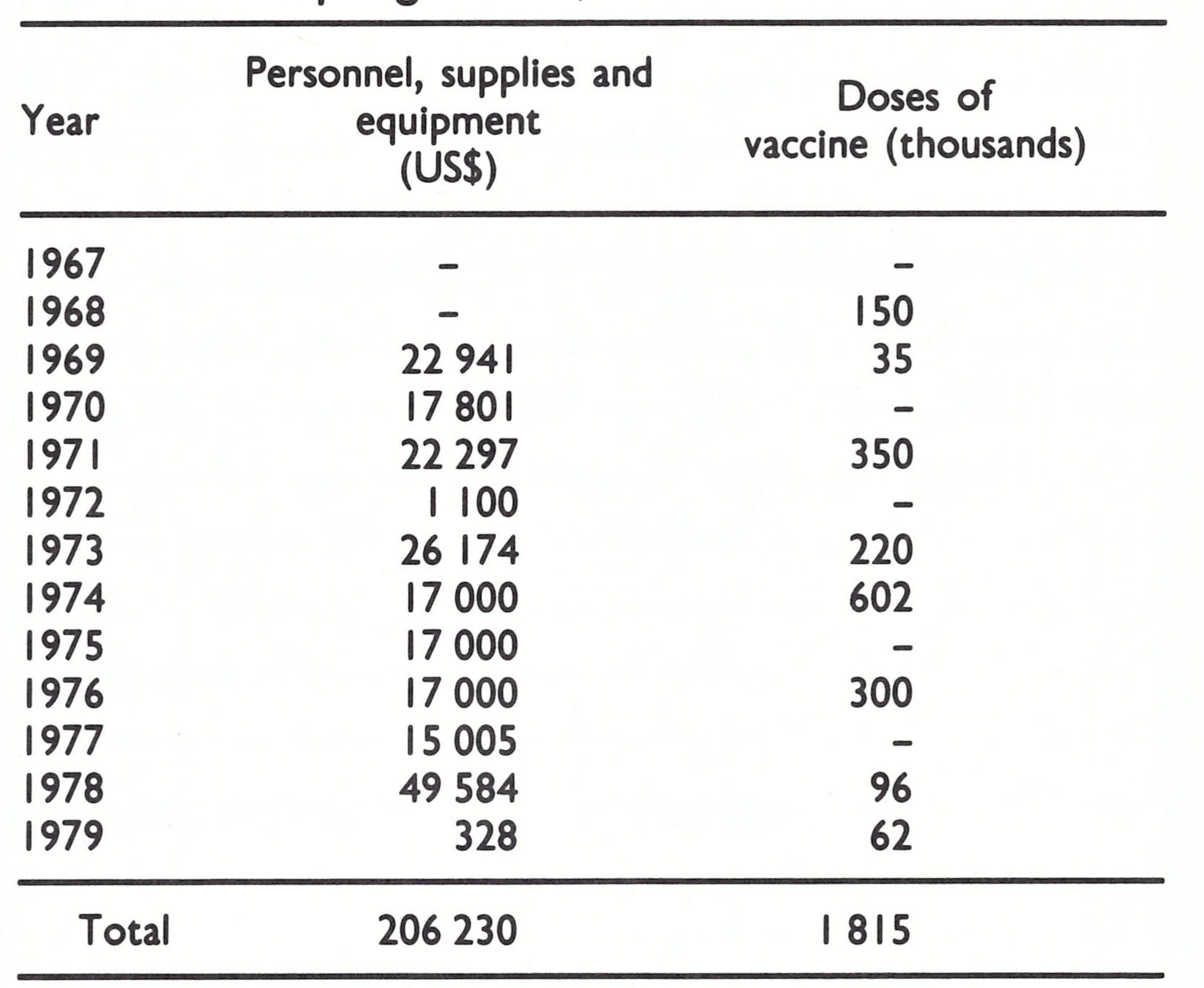
In 1968, discussions with government officials led to the approval of a plan of operations for a WHO-supported programme, to begin in July 1969. WHO agreed to provide a medical officer, vaccine, vehicles and a per diem allowance for national staff travelling in the field. In the course of the following decade WHO provided some US$313 000 in support of the programme (about US$0.06 per head of population), as well as 3 million doses of vaccine (Table 21.1). The government agreed to provide a counterpart medical officer, 53 vaccinators and 20 auxiliary staff for a 3-year national vaccination campaign during which it was planned to vaccinate 4 million persons (Table 21.2). The development of surveillance was considered an essential component of the plan although it received little attention from the programme staff.
Table 21.1: Yemen: WHO support provided to the smallpox eradication programme, 1967-1979
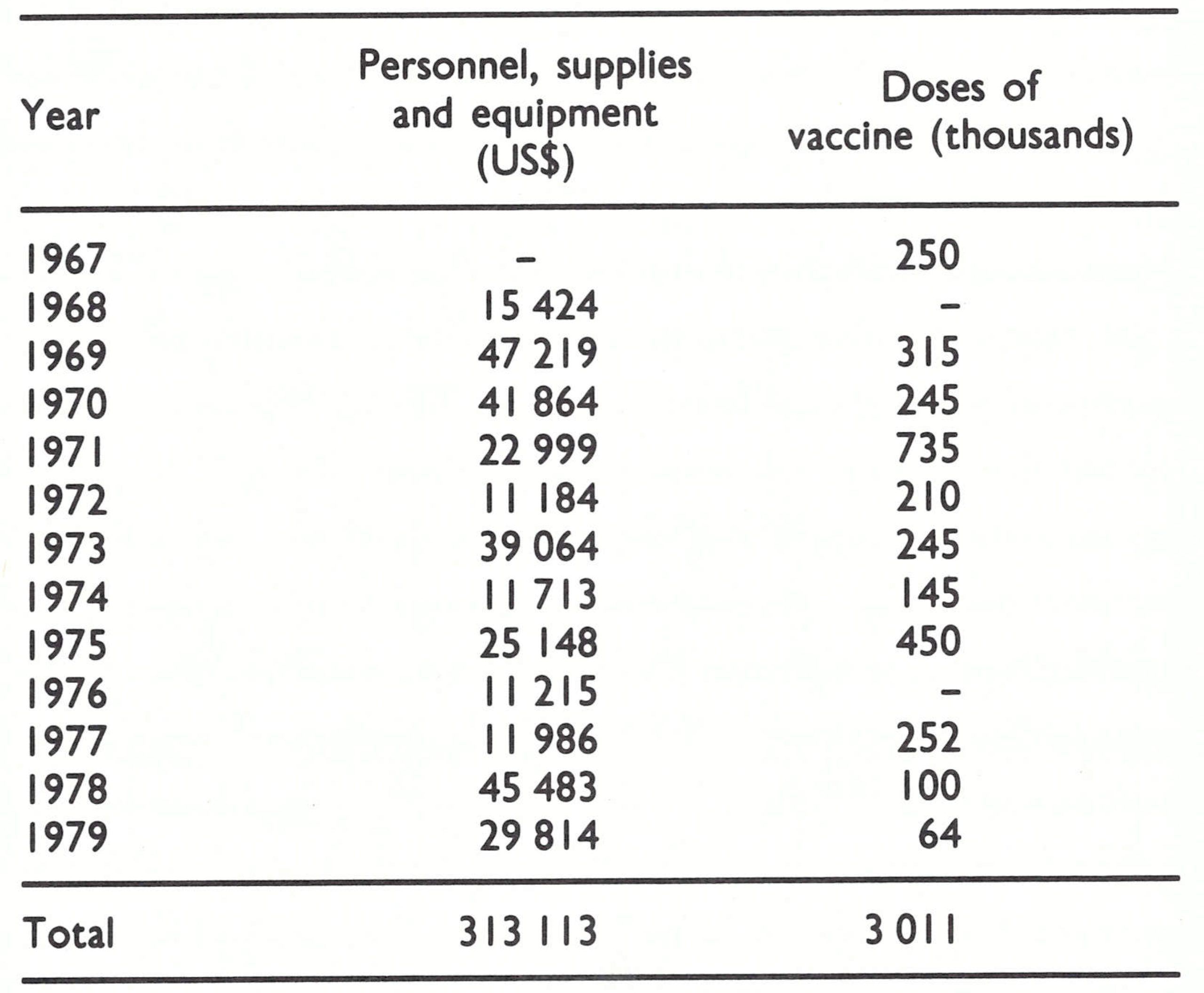
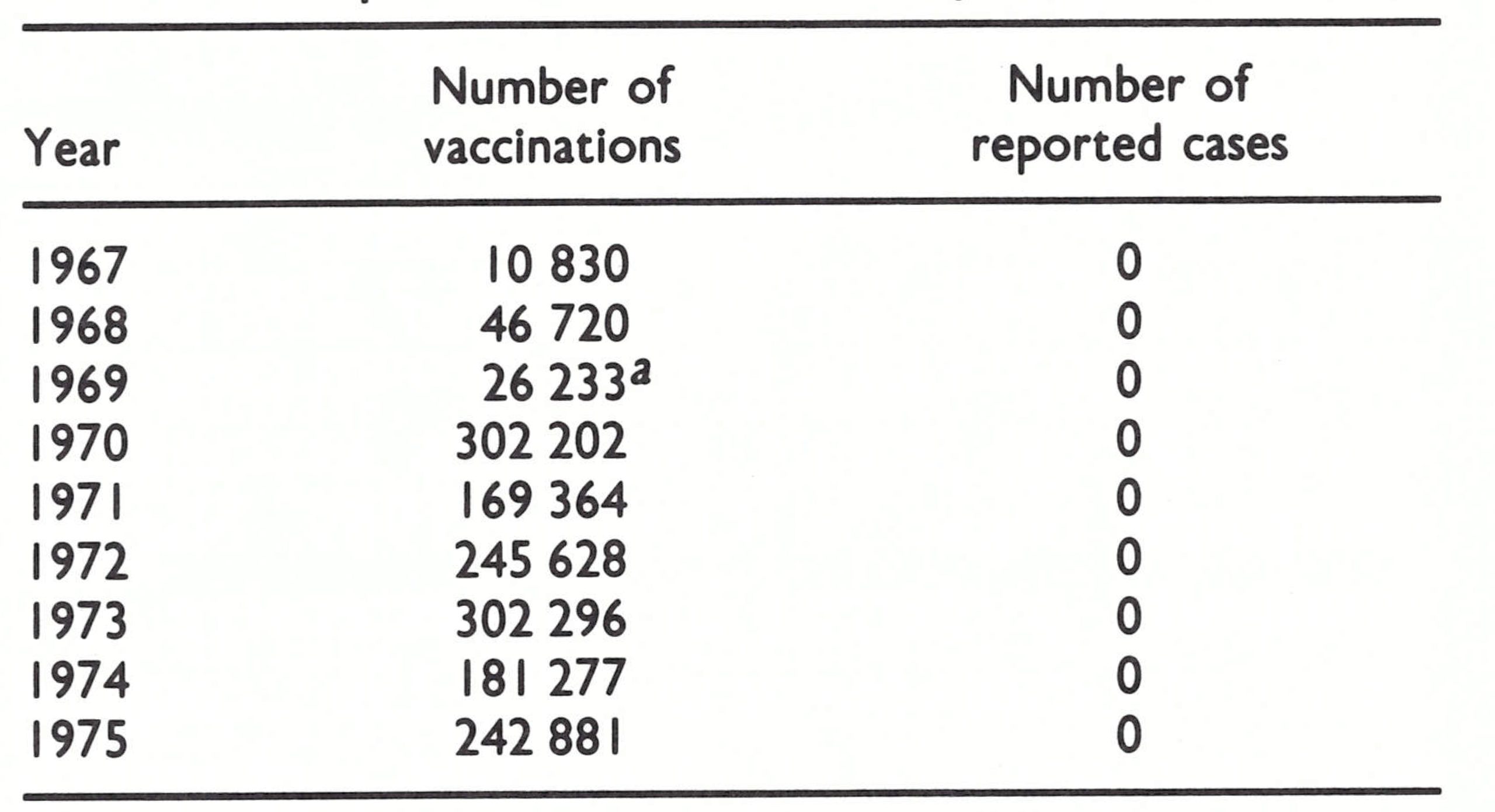
Table 21.2: Yemen: number of vaccinations performed and number of reported cases of smallpox, 1967-1975
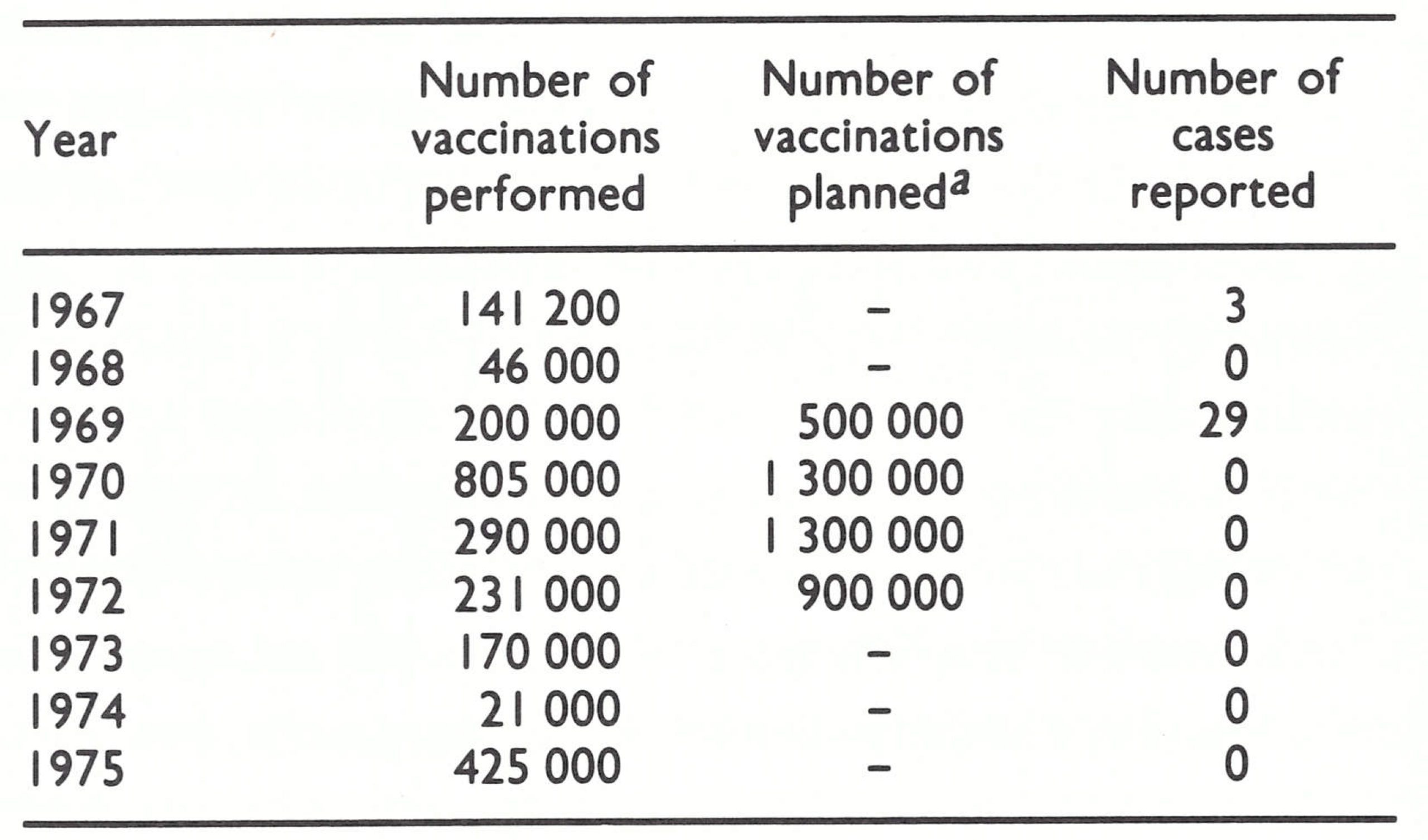 a According to plan of operations (1968) for madd campaign.
a According to plan of operations (1968) for madd campaign.
Headquarters were established in Sana’a under the national programme director, Dr M.K. Al Aghbari, and in July a WHO epidemiologist arrived. Because of the paucity of health staff and facilities, the smallpox eradication programme was envisaged as one which would lay the foundation for other national communicable disease control activities.
A house-to-house vaccination campaign began in October 1969 and at first progressed reasonably well, with assessment showing more than 90% coverage. By the end of the year, 119 752 residents of Sana’a and 192 surrounding villages had been vaccinated, 25% of them for the first time; 80 000 people were vaccinated in other parts of the country. In 1969, 29 cases of smallpox were officially reported by the government to WHO, although at a WHO regional smallpox eradication seminar held in November of that year, the government submitted a report indicating that 47 smallpox cases had occurred. The WHO smallpox adviser in Yemen was asked to investigate and confirm these cases; he merely reported that he thought they were all cases of chickenpox. It was not long before the reliability of his observations was called into question when, in a quarterly report, he stated that, having examined the staff of the smallpox eradication programme, he had been able to ascertain that none were “carriers” of the disease. The quality of surveillance in Yemen did not improve materially thereafter.
In January 1970, when vaccination could be more readily performed than during the intolerably hot summer months, the vaccination campaign shifted to the coastal strip (Fig 21.2). Three vaccination units, each equipped with a vehicle and consisting of a national supervisor and 8 vaccinators, proceeded systematically through the area performing house-to-house vaccination. Staff from the local health services, where such existed, worked with the teams in the expectation that they would continue maintenance vaccination after the teams had left. Each vaccinator averaged about 140 vaccinations a day. An assessment team checked vaccination takes and coverage 1 week later. By the end of the year, more than 800 000 people had been vaccinated.
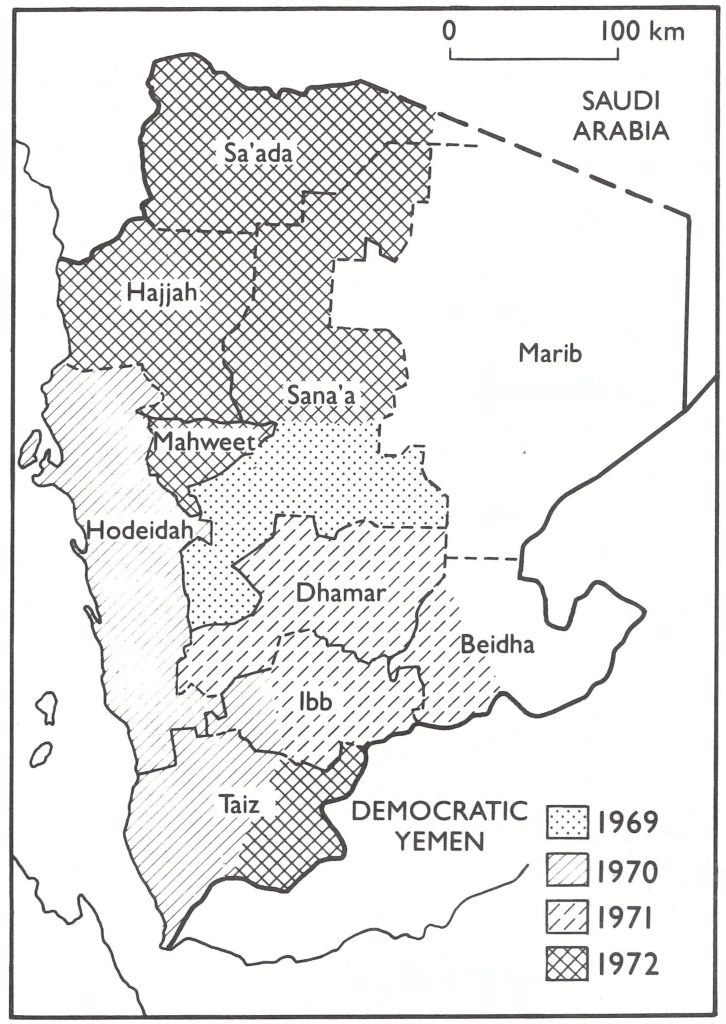
Fig. 21.2. Yemen: progress of the smallpox vaccination campaign, 1969-1972.
Towards the end of 1970, the vaccination campaign began to deteriorate. Dr Al Aghbari was asked to assume direction of all preventive services for the Ministry of Health and was therefore obliged to spend less time in the field; project vehicles broke down more often and the field staff began to take increasingly frequent and extended holidays. The WHO adviser rarely left the capital city, and in March 1971 his assignment was terminated.
During the whole of 1971, only 290 000 persons were vaccinated; the level of coverage was unknown because assessment had ceased. The few reports of smallpox received were seldom investigated; the cases that were examined were diagnosed as chickenpox or dermatitis. The vaccination campaign was gradually extended to most other areas of the country and finally concluded in April 1973, although the inhabitants of most rural areas throughout the north and east remained unvaccinated. Only 231 000 persons were vaccinated in 1972, 45% of them for the first time. From the campaign’s inception to its conclusion, the staff succeeded in vaccinating only about 2 million persons—less than half the estimated population. Of this number, nearly 300 000 were vaccinated by teams of the Swedish Save the Children Foundation, who were then providing health services in coastal areas of the country.
The government was dissatisfied with the programme and repeatedly requested the WHO Regional Office for the Eastern Mediterranean to assign another full-time WHO epidemiologist. This request was not met until April 1973, when the former WHO smallpox adviser in the Sudan, despite an unsatisfactory performance there, was transferred to Yemen. In addition to dealing with smallpox, he was made responsible for developing a preventive medicine section in the Ministry of Health and creating a health statistics unit.
About the time of his arrival, the systematic vaccination campaign was terminated and the teams were disbanded. Vaccination continued to be offered through existing health facilities. However, of the 170 000 recorded vaccinations in 1973, 60% were reported to have been given to adults who required international certificates of vaccination in order to leave the country.
None of the health units provided weekly or monthly reports of smallpox cases nor did they submit reports on other diseases. When suspected cases of smallpox were notified, national staff or the WHO epidemiologist investigated them and sent specimens to one of the WHO reference laboratories. In all, 26 specimens were submitted during the 7-year period 1971-1977. None contained poxvirus.
In 1975, a monthly communicable diseases reporting system was at last introduced and reports of smallpox and chickenpox were carried by hand to the capital. This was intended to facilitate investigation by the newly created Department of Preventive Health Services, consisting of a national medical officer, the WHO epidemiologist and a clerk. Most of the reports received were from the 3 major towns. Five suspected cases of smallpox and 79 cases of chickenpox were reported in 1975 and 2 suspected cases of smallpox and 88 cases of chickenpox in 1976. None of them was confirmed to be a case of smallpox.
From 1970 to the end of 1977, neither WHO Headquarters staff nor the WHO regional smallpox adviser had devoted much attention or effort to the programme in Yemen. Smallpox eradication in other parts of the world commanded a higher priority. Because no confirmed cases of smallpox had been reported from Yemen since 1969 and none was being detected among the numerous pilgrims or Yemeni workers who travelled to Saudi Arabia and to other countries, WHO staff were cautiously hopeful that smallpox transmission had been interrupted.
By the autumn of 1977, when smallpox had been eliminated in Ethiopia (see below) and its interruption in Somalia was imminent, a more detailed appraisal of the situation in Yemen was considered to be essential. A WHO smallpox consultant who visited the country in September 1977 found large numbers of refugees from Ethiopia and some from Somalia living in villages along the coastal desert strip. Few had vaccination scars. An extensive vaccination campaign and search for cases were subsequently initiated in this area, but no cases were found.
In December 1977, another WHO consultant travelled through the highland areas, and, although he found no cases, he discovered that only people living in the larger towns and along the principal roads had been vaccinated during the campaign. Many of the more remote villages had not been visited by programme staff or vaccination teams for 6-8 years. If variola minor had been imported-from Ethiopia, for example-he believed that it might still be present, spreading slowly through sparsely settled areas, as had been the case in Ethiopia. Accordingly, it was deemed essential to conduct a thorough country-wide search for cases.
From June 1978 to the end of March 1979, a search programme under the direction of an experienced WHO epidemiologist, Mr Robert Steinglass, was conducted by Yemeni staff assisted by personnel of the Swedish Save the Children Foundation and Peace Corps volunteers from the USA, who were engaged in other health programmes in Yemen at that time . Three surveillance teams, each consisting of a team leader, 1 or 2 surveillance workers, a driver and locally hired temporary staff searched 146 of 162 districts and 920 villages and towns with a population of more than 500 persons . In all, 116 184 persons were examined in villages and towns whose total number of inhabitants amounted to 897 488-i.e .,13% of Yemen’s resident population. Four hundred and eighty reports of illness with rash and fever were investigated ; 43 specimens were submitted for laboratory examination, but none showed evidence of smallpox.
Vaccinial immunity was low, as had been expected. Only 23 % of children under 4 years of age and only 63% of the population as a whole had vaccination scars (Table 21.3).
Table 21.3: Yemen: results of vaccination scar survey, by governorate and by age, 1978-1979
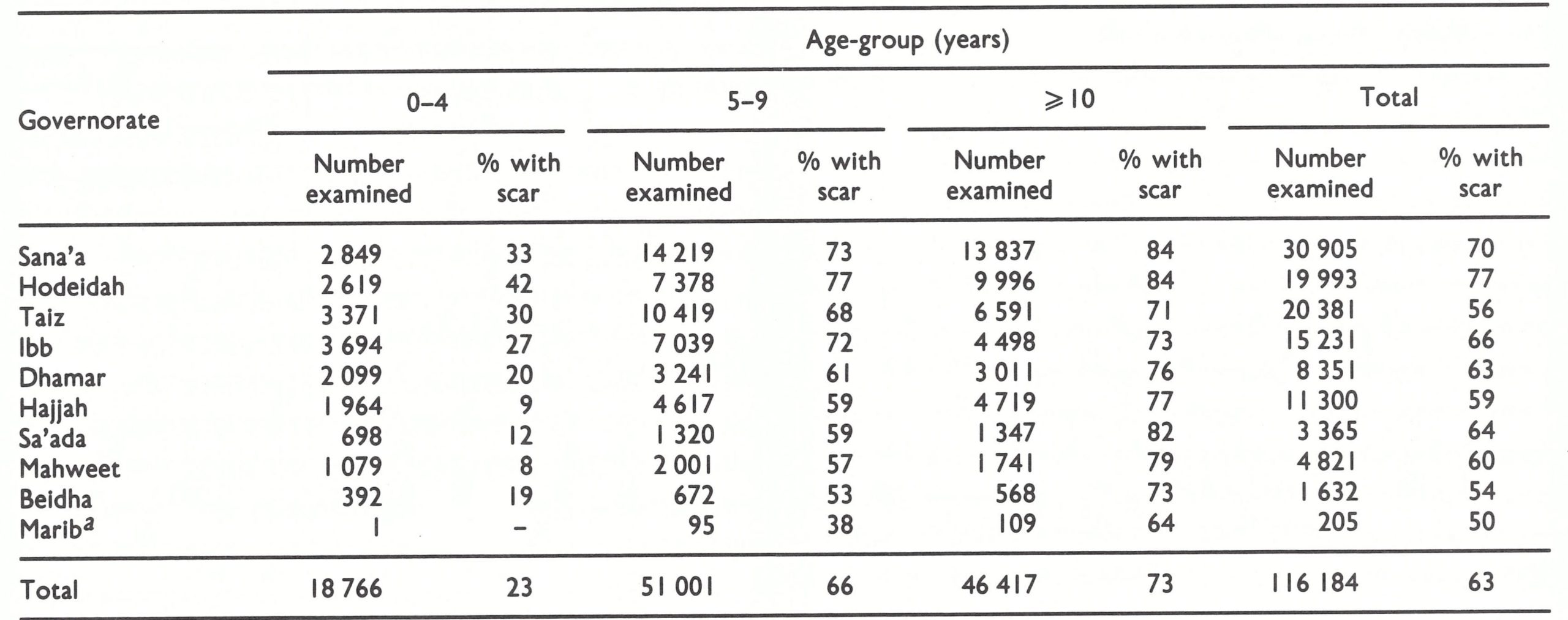 a The Governorate of Marib (population 40 896) was not accessible to government staff and thus area-wide search was not possible.
a The Governorate of Marib (population 40 896) was not accessible to government staff and thus area-wide search was not possible.
Of 2514 persons with the facial pockmarks of smallpox none was younger than 11 years of age and none had experienced smallpox after 1969. Persons with facial pockmarks were found in 95% of the 146 districts and in 72% of the villages. More than 60% had contracted the disease during the 1957-1963 epidemic.
It had been feared that smallpox eradication in Yemen would present a formidable problem; ironically, the last known cases had occurred just before the mass vaccination campaign began in October 1969. Natural immunity conferred by the extensive epidemic of variola major in 1957-1963, coupled with the practice of variolation, apparently served to reduce the number of susceptible subjects to a sufficiently low proportion of the population that transmission ceased. It is possible that undetected importations, notably from Ethiopia, Yemen’s nearest endemic neighbour, may have occurred, but if so they terminated spontaneously. Whatever its problems, the programme served eventually to foster an infectious disease reporting system and provided an impetus to a broader immunization programme, which commenced in 1977.
DEMOCRATIC YEMEN
Democratic Yemen occupies a vast barren area in the south-western part of the Arabian Peninsula, but as was revealed in its first census in 1973, 55% of the country’s population of 1.6 million lived in 12% of the land area in and around Aden, the capital. In 1967, Democratic Yemen was considered to be free of smallpox, the last endemic case having occurred in 1960. However, it was thought to be at high risk of importations. Ships carrying Mecca pilgrims from Asia and Africa regularly called at Aden ; and travellers as well as refugees, especially from areas of Ethiopia with endemic smallpox, were numbered in the tens of thousands. Accordingly, a WHO-supported programme was planned for Democratic Yemen.
Until it achieved independence in 1967, the area constituting Democratic Yemen consisted of the British crown colony of Aden and a large number of loosely federated independent sultanates and sheikdoms, known as the Protectorate of South Arabia. Over past decades, occasional small outbreaks of smallpox, usually attributed to cases imported by pilgrims, had been reported from Aden. The last officially notified outbreaks occurred between 1957 and 1961, during which 341 cases with 105 deaths were recorded, primarily in the western part of the country. The outbreaks were said to have resulted from a series of different importations from India, Pakistan and Yemen. They were controlled by mass vaccination. Twentyfour cases of variola minor, which were not officially reported to WHO but were nevertheless recorded in a government document, occurred in 1965 in the eastern part of the country. As in other countries, there were undoubtedly other unreported cases, but in this very sparsely settled area it was difficult for smallpox transmission to be sustained; any importations that may have occurred ceased spontaneously.
Vaccination with liquid vaccine had been fairly extensively practised in the British crown colony of Aden for many decades. In the less populated areas to the east, protection against severe smallpox was more frequently achieved by variolation. The outbreaks of 1957-1961 had occasioned an extensive vaccination campaign in Aden, some 338 000 vaccinations having been recorded between 1957 and 1959. In 1960, freeze-dried vaccine was first made available by UNICEF for a vaccination campaign, but until 1970, it was uncommon for more than 50 000-75 000 persons to be vaccinated each year.
In September 1969, WHO agreed to support an eradication programme, basically a village-by-village campaign to administer smallpox vaccine to all persons and BCG vaccine to those under 15 years of age. WHO supplemented the salary of the national programme director, paid the national staff a per diem, provided vehicles, vaccine and other supplies and equipment, and made funds available for petrol and vehicle repairs. WHO eventually provided about US$206 000 and more than 1 .8 million doses of vaccine in support of the programme (Table 21.4).
Table 21.4: Democratic Yemen: WHO support provided to the smallpox eradication programme, 1967-1979
The national staff comprised 48 persons, including 32 vaccinators who worked in 4 operational groups, each with 4 vaccination teams consisting of 2 men. The vaccination campaign proceeded on a house-to-house basis and was regularly assessed by a special team. Because of security problems, operations were initially restricted to 3 of the country’s 6 governorates that were located in the immediate vicinity of Aden. In September 1971, one of the programme vehicles, carrying 10 vaccinators and the driver, was destroyed by a land-mine, which killed 4 of the vaccinators and injured the others. Understandably, the staff feared to venture too far from the capital. Not until 1973 did civil disorder subside sufficiently to permit the extension of vaccination activities into all governorates.
As is shown in Table 21.5, the number of vaccinations performed annually from 1970 onwards ranged between 169 364 (1971) and 302 296 (1973). Productivity was not high, each vaccinator averaging about 50 smallpox vaccinations and 10-20 BCG vaccinations a day. This was partly attributable to the difficulty of travelling through the generally rugged mountainous country, with few roads. Assessment figures indicated that the coverage achieved was consistently about 90%, but it took 7 years for a total of 1.5 million vaccinations to be performed, a number approximately equivalent to the population. During this time, some 514 000 BCG vaccinations were also administered.
Despite the strategic location of Democratic Yemen and the apparent risk of importations, no cases were confirmed after 1967. A single case in Aden was reported to WHO in 1968 but the report was later retracted in the belief that the illness had been chickenpox. The absence of known importations can be explained in part by diminished maritime traffic associated with the closure of the Suez Canal from 1967 to 1975’and in part by restrictions on travel imposed by the government after independence in November 1967. Conceivably, outbreaks may have been overlooked since neither a surveillance nor a morbidity reporting system was ever developed. However, extensive surveys conducted during the country’s programme in 1978 to certify the absence of smallpox failed to detect any person who had been infected with the disease since 1966. These surveys also showed that, in the different governorates, between 76% and 90% of the population had vaccination scars—a high level of vaccinial immunity.
Contrary to expectations when the programme began, Democratic Yemen did not experience problems with smallpox; in retrospect, a special vaccination programme may have been unnecessary. However, the combined smallpox and BCG vaccination campaign did provide a basis for the establishment of a national immunization programme.
Table 21.5: Democratic Yemen: number of vaccinations performed and number of reported cases of smallpox, 1967-1975
 a Six months only.
a Six months only.
ETHIOPIA
Ethiopia was 6 times larger in area (1.2 million square kilometres), with a population (25.5 million in 1970) more than 5 times greater than that of Yemen, but the problems of geography and population dispersion were similar. Most of Ethiopia’s population was widely distributed in small groups of huts scattered across the central highlands (Fig. 21.3) at 1500-3000 metres above sea level. Rugged mountains and deep ravines made travel extremely difficult throughout this area, and impossible during the rainy season, from June to September. At the periphery of the country were lowland areas in the west and south-west, with a fertile and more populated savanna grassland. Nomads roamed the vast Danakil and Ogaden deserts to the east, moving freely across the unmarked borders with Somalia and the French Territory of the Afars and the Issas (later Djibouti). Less than 10 000 kilometres of all-weather roads connected the few scattered cities and towns. Health facilities and trained health staff were few ; vaccination was all but unknown to most of the population, but variolation was widespread. Several hundred cases of smallpox were reported each year, but in 1967 it was surmised that thousands of cases must be occurring.
Throughout the world, experience had shown that smallpox transmission was not readily sustained in sparsely settled areas. Elimination of smallpox from urban centres and the accessible, more populated rural areas usually resulted in the disease dying out spontaneously in the more remote parts of a country. In Ethiopia, this did not happen. Here, among a dispersed, thinly settled population, the global eradication of smallpox came nearest to being thwarted, as an unparalleled array of problems and catastrophes continually hampered the programme. Nearly 6 years elapsed after the campaign had begun before the last outbreak was finally discovered and contained, in August 1976.
A detailed account of the programme is presented in the book Smallpox Eradication in Ethiopia by Tekeste et al.(1984), from which most of the data in this chapter are drawn.
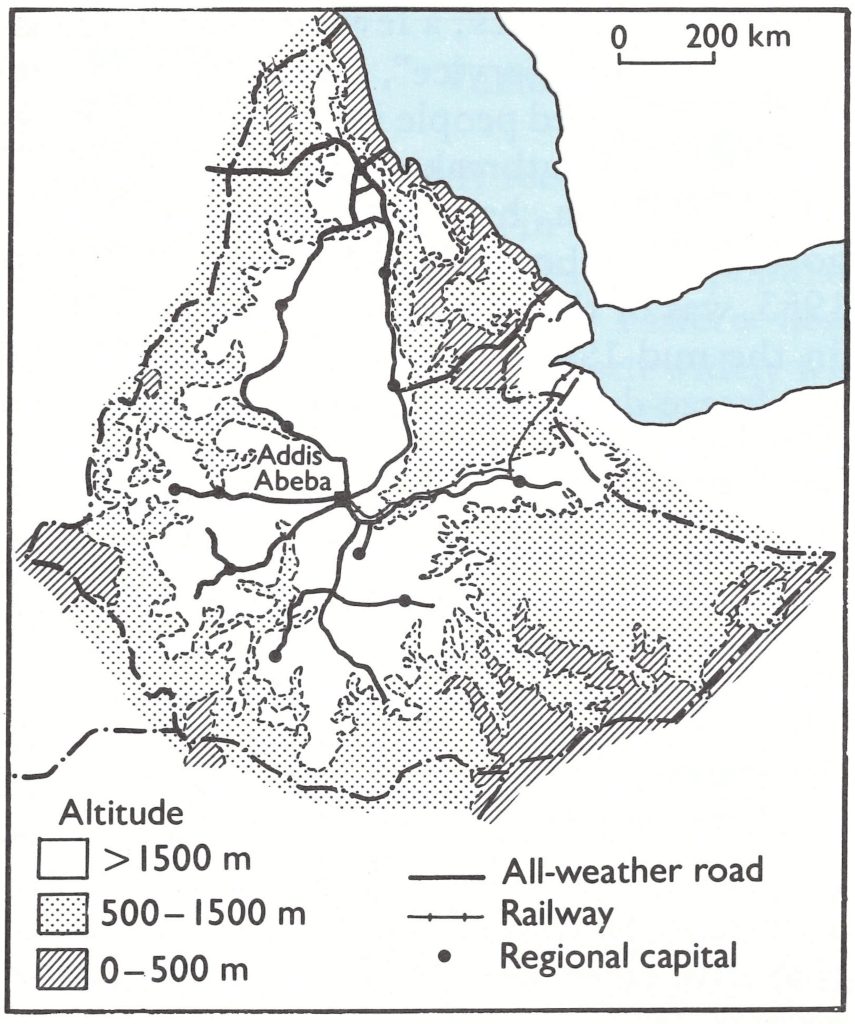
Fig. 21.3. Ethiopia: topography and road system.
Background
Ethiopia, in 1967, was one of the world’s least developed countries, and until 1974 it was a monarchy with numerous feudal landlords. The infrastructure of services for health, education, transport and communications was rudimentary except in the northern province of Eritrea, in which a number of roads and health centres had been built during the Italian and British administrations.
Administratively, the country was divided into 14 provinces (which, after the 1974 revolution, became 15 regions), each with a governor, who was usually a member of the royal family. Each province was subdivided into awrajas (102 in the country as a whole) and these, in turn, into woredas (539 all told), each with its appointed governor or administrator. At the local level, the feudal, often absentee, landlord was the acknowledged headman, but he was frequently indifferent and sometimes hostile to higher government authority. To obtain assistance with the programme at each administrative level a special letter requesting cooperation had to be prepared by a superior and taken by messenger to the official concerned.
No census had ever been taken but it was thought that no more than 2 million of the estimated 25.5 million population lived in about 200 towns and villages of 500 or more persons. In the rural areas of the plateau, the houses were widely scattered. There, the smallest traditional unit, sometimes referred to as a village, was the mender, consisting of up to 100 houses occupied by one or more related families. Fifty or more menders comprised a deber, which included the membership of a single church. After the 1974 revolution and nationalization of the land, workers’ cooperatives, called “farmers’ associations” or “urban dwellers’ associations”, were created and village areas were defined. The villages, however, were unlike those in most other countries in that they usually extended over large areas, the distance between houses often ranging from a few hundred to a thousand metres. In the extensive eastern and southern scrub desert areas, which comprised half the country, nomadic groups with ethnic ties to the neighbouring French Territory of the Afars and the Issas and Somalia wandered freely, not infrequently crossing open borders between the countries. In the south-west were tribal groups whose way of life was little more advanced than that of a Stone Age culture.
Roads of any type were few; more than 85% of the population lived further than 30 kilometres away from the nearest all-weather road (Ayalew, 1982). Travel from place to place during the dry season was largely on horse- or muleback or by foot. When torrential rains occurred in the highlands, between June and September, large areas became completely inaccessible. Communications were poor: an unreliable, frequently unusable, telephone service linked the capitals of provinces, and the postal service was deficient.
Language presented a further problem. The people of Ethiopia consisted of 10 major ethnic groups speaking 70 languages and dialects. Frequently, programme staff had to communicate successively through two or three different interpreters to question villagers about the existence of smallpox and to explain the unfamiliar practice of vaccination. Some people were reasonably receptive, but refusal and sometimes active resistance were encountered among many who lived in the highland areas in the north and central parts of the country. Not surprisingly, smallpox proved to be particularly tenacious in those areas.
Health personnel and facilities in 1967 were concentrated in Addis Abeba, the capital, and in Eritrea. The largest proportion of the government’s health budget was allocated to curative services, to which not more than 5 % of the population had access. Government records for 1967 show a census of 84 hospitals and 64 health centres and a total of 362 physicians and 2800 other health staff. For 40% of the population, a journey of 3 days or more, and for another 30%, a journey of 1-2 days, was required to reach the nearest health unit. Personnel engaged in the administratively separate malaria eradication programme were far more numerous than the national health services staff. In all, 8000 malaria eradication staff were distributed over about one-third of the country. They were concerned only with malaria and were supported under a bilateral assistance programme.
Protection against smallpox was often provided through variolation. This was usually performed by the head of a household among family members after cases began to occur in the vicinity. The Afghan type of professional variolator, who travelled widely and preserved scabs and pustular material over long periods of time, was uncommon. Data on the number of smallpox vaccinations performed annually before 1971 are not available but estimates indicate the total to be less than 500 000. Most of them were performed in hospitals and clinics; a few were given by an “Anti-epidemic Service”, a small mobile unit which vaccinated people in and around Addis Abeba when outbreaks were reported . The vaccine, which had been produced at a government laboratory in Addis Abeba since 1953, was of the thermolabile liquid variety. In the mid-1960s, however, the preparation of a freeze-dried vaccine began, but this could not be tested for potency owing to a lack of fertile eggs. When it was eventually examined by a WHO reference laboratory, it was found to be unsatisfactory. In 1970, freeze-dried vaccine was provided by WHO and vaccine production in Addis Abeba ceased.
Little is known about the prevalence, extent and severity of smallpox before 1971. Epidemics with high mortality were said to have occurred every 10-30 years during the 19th century. Annual statistical compilations that date from 1931 show as many as 2832 cases in 1956 but comparatively few in most years. The cases that were reported were among hospitalized patients in the few urban centres. There is no information on the number of deaths. After 1971, when the eradication programme began and more complete data became available, only the mild variola minor form of smallpox was found. Variola major had disappeared, but it is not known when this occurred. Variola minor was documented as early as 1958, but as recently as 1964 a smallpox outbreak with a high case-fatality rate typical of variola major was reported by a health officer in the central highlands.
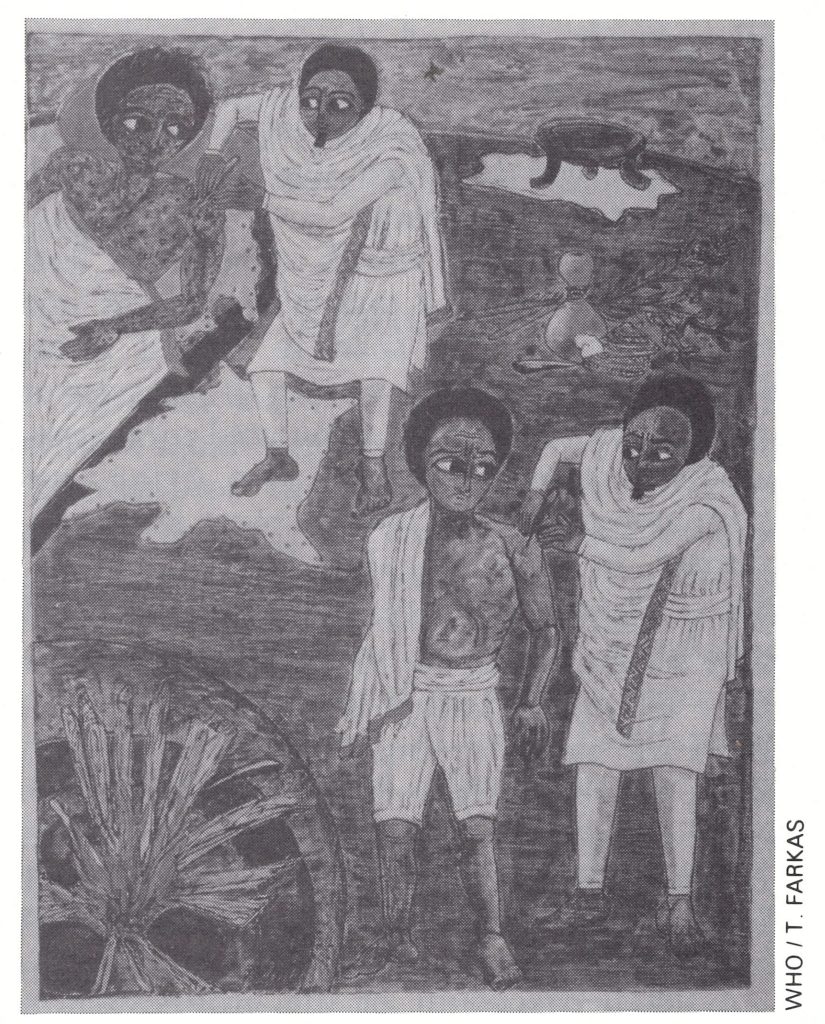
Plate 21.1. A variolator in Ethiopia obtaining pustular material from a patient (lying) and inoculating it into the arm of a healthy recipient (standing). Variolation was usually performed by one of the elders in a family and was widely practised throughout Ethiopia. The last known patient in Ethiopia (August 1976) developed illness following variolation. (Detail from a painting by Zerihun Yetmgeta presented to WHO by the Government of Ethiopia.)
Variolation and Receptivity to Vaccination
Smallpox was widely recognized and feared by the different ethnic groups throughout Ethiopia, each of which, in the absence of vaccination, dealt with it in a different manner. Among the Amharas, who largely populated the central zone provinces and Shewa, and among the nomads of the eastern desert areas, protection was obtained through variolation, which was practised widely when outbreaks occurred. Many Amharas resisted vaccination in favour of variolation and religious ceremonies that consisted in decorating the dwelling of a patient with fresh green leaves, grasses and flowers and in burning incense. Sheep, goats and hens of different colours were sacrificed, and ritual play-acting and singing were performed to induce the disease to take a mild form. Other groups had other practices and rites. When smallpox occurred, the Nuers, a Nilotic tribe living near the Sudanese border, performed a ceremony in which a prophet would lead the people to a river where goats were sacrificed to the "mother of gods", who was thought to live in the river; in a ceremony of joy, the assembled crowd would then bathe in the river.
For reasons which are unclear, most ethnic groups in the south and east of the country readily accepted, indeed actively sought, vaccination whether or not they performed variolation. Among Galla groups, who inhabited large areas of provinces in the south-west and south-east, people returned many times for vaccination, and many villages reported falsely that outbreaks were occurring in order to induce the teams to visit. In this area, it was not uncommon for teams to discover crudely scribbled notes left along trails requesting visits to villages as distant as 40-50 kilometres.
Delays in Launching an Eradication Programme
At the inception of the Intensified Smallpox Eradication Programme in 1967, Ethiopia was considered to be strategically important as an endemic country. The neighbouring areas of the French Territory of the Afars and the Issas, Somalia and the Sudan were thought to be free of smallpox. Kenya, with an extensive network of health services and a more complete notification system, was reporting fewer than 200 cases a year. If reinfection of adjacent countries was to be averted, a programme would have to be started in Ethiopia as soon as possible.
Government officials stated, however, that they were not interested in undertaking a smallpox eradication programme and could not do so because so many resources were already committed to malaria eradication . They reasoned that one eradication programme must be as expensive as another, a belief encouraged by expatriate malaria advisers . Given that the Ethiopia malaria eradication programme was then disbursing more than US$8 million a year, primarily from bilateral contributions, and that it employed 8000 workers, their apprehension was understandable. The government authorities did not appreciate that a smallpox eradication programme was far simpler, cost much less and required far fewer personnel than a malaria eradication programme . Moreover, WHO staff believed that smallpox eradication in Ethiopia might be combined successfully with other health activities then being considered, including a BCG vaccination programme in urban areas and a proposed yellow fever vaccination campaign which the Federal Republic of Germany was expected to support. The most extensive resources available were those of the malaria eradication programme itself. It was felt that much could be accomplished if its directors would permit the thousands of malaria workers to serve as smallpox surveillance agents and to vaccinate those encountered during their regular house-to-house visits. In addition, several projects staffed by United States Peace Corps volunteers were then in operation in Ethiopia and it was understood from United States government officials that they would be receptive to a request to provide manpower to health-related projects.
WHO smallpox eradication staff believed that a suitable, economically feasible and acceptable plan for at least a control programme, if not for eradication, could be developed. To do so would require appraisal and discussion in Addis Abeba of potentially available resources and of the cost and options for the conduct of such a programme . Repeated proposals were made to the government that WHO regional and Headquarters staff should make an exploratory visit, but for nearly 3 years these proposals were firmly declined . Initially, this reaction was difficult to understand because most governments were more than willing to discuss possible options, whether or not they were inclined to undertake a programme. Gradually, however, it became known that the United States malaria eradication programme adviser and his Ethiopian counterpart had persuaded the Minister of Health that a smallpox eradication programme would fatally compromise the malaria eradication campaign, which was then making little progress. They advised that, under the circumstances, his best approach would be to refuse to receive WHO smallpox eradication staff, even for exploratory discussions.
The impasse was not readily resolved. The strategy and the projected order of magnitude of needs for smallpox eradication were discussed in Geneva at the World Health Assembly with Ethiopian government officials and malaria advisers from the USA, with bilateral assistance staff in Washington and with malaria staff at the United States Center for Disease Control—all to no avail. An indirect approach to the government was planned when Dr George Lythcott, senior adviser to the United States-aided western and central African smallpox eradication programme, was invited to speak about that programme at a meeting of the Organization of African States in Addis Abeba . Having been briefed by WHO staff and being prepared to hold informal meetings with Ethiopian government officials, he was about to leave for Addis Abeba when United States officials abruptly and without explanation cancelled his trip.
Nearly 3 years had elapsed when, inexplicably, in October 1969, the government responded favourably to yet another proposal for an exploratory visit. Dr Ehsan Shafa, then Regional Adviser on Smallpox Eradication at the WHO Regional Office for the Eastern Mediterranean, and Henderson flew immediately to Addis Abeba. The response to the proposed visit had been sent by a subordinate when the Minister and Secretary of Health were absent on a trip abroad. They were not pleased, on their return, to find the WHO team awaiting them; they made it clear that Ethiopia’s attitude had not changed. They did agree, however, that Henderson and Dr Shafa could devote 2 weeks to the preparation of a plan which the government would consider. In view of WHO’s budgetary limitations and the obvious antipathy of the government, it was apparent that whatever programme might be devised would have to be a modest one. The malaria eradication programme’s considerable resources in manpower and transport offered a potential building block, but its director declined to cooperate in any way. There were no other immunization programmes and little assistance could be expected from the few existing health units. However, tentative offers to provide volunteers were made by the USA and Japan. Among the many officials to whom Henderson and Dr Shafa spoke was Dr Kurt Weithaler, then serving as director of the hospital for the Emperor’s Imperial Guard. Dr Weithaler, an Austrian, had been employed by the government for more than a decade, was widely known in government and medical circles, served as a member of the Health Minister’s advisory panel—the General Medical Board—and was a friend of the Emperor. He expressed considerable enthusiasm for the programme and intimated that he might be persuaded to serve as WHO’s senior adviser. The draft plan of operations was presented to the Minister on a Saturday for consideration that weekend and a decision on Monday. He expressed little interest. Meanwhile, unbeknownst to the WHO team, Dr Weithaler showed the plan to the Emperor, who agreed that it should be initiated and ordered the Minister of Health to support it.
Plate 21.2. Kurt L. Weithaler (b. 1919), an experienced health administrator, served as the senior WHO adviser to the Ethiopian smallpox eradication programme from 1970 to 1976.
The Programme Begins, 1971
The draft plan of operations envisaged: (1) a search for outbreaks and their containment to the extent possible with the available manpower; (2) the development of a simple surveillance programme for the reporting of cases and vaccination by the staff of existing health facilities; and (3) mass vaccination in Ethiopia’s few centres of population. It was hoped that, with the limited personnel and equipment that could be provided, smallpox transmission might be successfully interrupted in the accessible areas. It was to be hoped that the disease would then die out spontaneously in at least some of the rural areas. However, since a relatively small proportion of the population lived in accessible areas and since vaccinial immunity was undoubtedly as low as anywhere in the world, the proposition was uncertain. All the same, a less than fully effective control programme was better than no programme at all.
A staff of about 70 was envisaged. The government requested that a senior WHO medical officer should be appointed as “the responsible executive authority”, and the energetic Dr Weithaler was recruited to fill the post. It was exceptional in most countries for a person assigned by WHO to serve in this capacity but, in Ethiopia, in which trained personnel were in short supply, such an appointment was considered essential. A WHO epidemiologist was to be appointed for surveillance, and Dr Ciro de Quadros, who had served previously on the national staff of the Brazilian smallpox eradication programme (see Chapter 12), was selected for this post. The government assigned as the senior national professional Ato Tamiru Debeya, a respected and able person who retained this responsibility through 1975. His title was that of sanitarian but, in Ethiopia at that time, such persons had a broad public health training and served as administrators for many public health programmes. Twelve other workers were to be assigned to the headquarters office—3 drivers, 8 office staff and a most competent locally recruited WHO administrative officer, Ato Tefari Seyoum. For assignment to the field, the government agreed to provide 21 staff, health officers or sanitarians, who would work with volunteers from the USA. The health officers played an exceptionally important role; they were graduates of a recently established 4-year course of study in the health sciences which was designed for students who had completed secondary school.
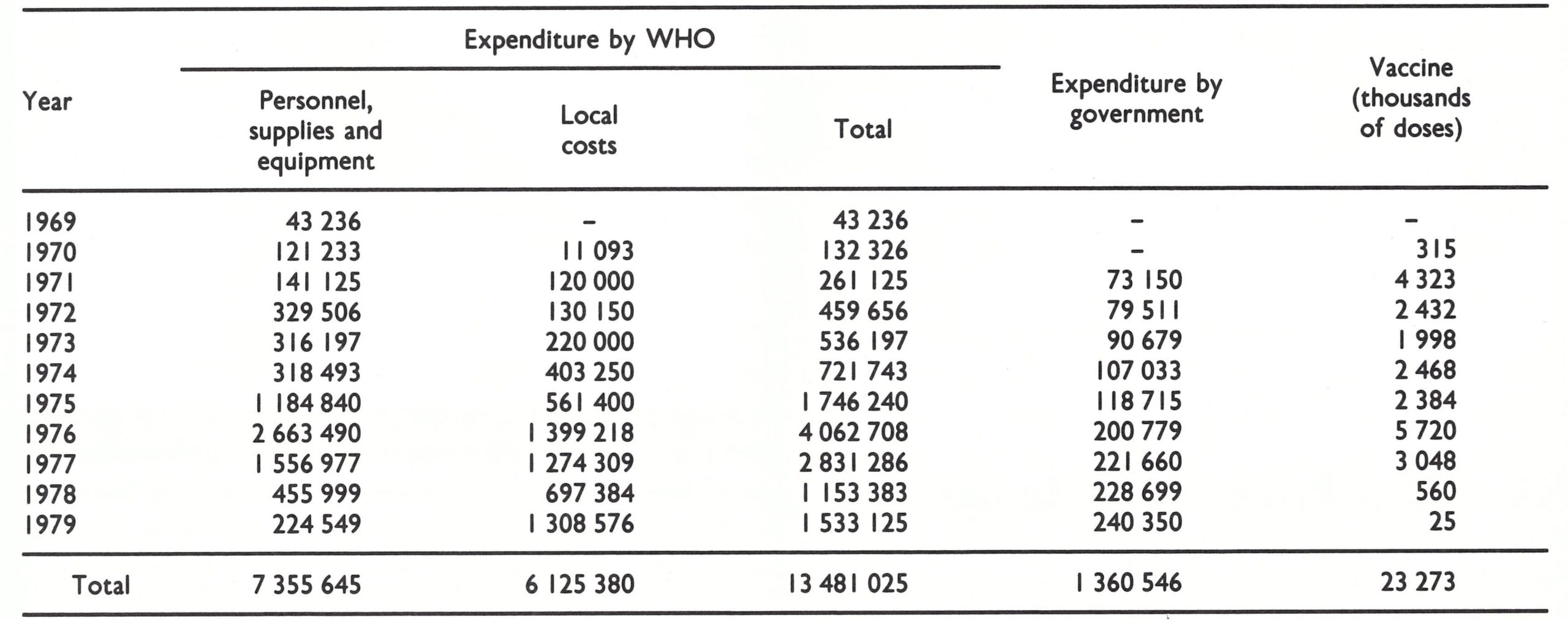
Ethiopia’s financial commitments consisted only in paying salaries of its health officers and sanitarians, all of whom were transferred from other programmes, and meeting the cost of office accommodation. WHO provided all supplies and equipment and covered the cost of transport, as well as the per diem allowances of Ethiopian staff and the salaries of the central office staff. The salaries and expenses of the volunteers were borne by their respective governments. WHO provided, in all, US$175 562 in 1969-1970, in addition to supplies of vaccine (Table 21.6). Eventually, the Organization was to spend nearly US$13 500 000 from its regular budget and from contributions made by numerous governments to the WHO Voluntary Fund for Health Promotion and to contribute more than 23 million doses of vaccine. The Ethiopian government spent US$1 360 546. Additional support, amounting to about US$1 390 000 was provided, in cash and in kind, through bilateral contributions from Austria, the Federal Republic of Germany, Japan and the USA. The total support to the programme amounted to about US$0.57 per head of population.
Table 21.6: Ethiopia: WHO and goverment support to the smallpox eradication programme, 1969-1979 (US$)a
 a An additional US$1 390 213 were provided through bilateral assistance.
a An additional US$1 390 213 were provided through bilateral assistance.
During the autumn of 1970, personnel were recruited, the volunteers from the USA arrived, equipment was delivered, a central office was established, training programmes were conducted, and by mid-January 1971, field operations began. At that time, there were only 3 other countries in Africa in which smallpox remained endemic—the Sudan, Zaire and South Africa. The latter 2 succeeded in interrupting transmission in 1971 (see Chapters 18 and 20).
For a programme in one of Africa’s last endemic countries-one of its largest and least developed-the available resources were few indeed. Over the first 6 months, the entire field staff consisted of only 39 persons—the 2 WHO advisers, 2 health officers, 19 sanitarians and 16 United States volunteers. They had only 6 Land Rovers between them, although 11 more were scheduled for delivery that summer. In the interim, it was hoped that vehicles might be borrowed from the malaria eradication programme’s large reserve pool of vehicles, which were parked at a training centre south of Addis Abeba. A request was made, but the vehicles mysteriously vanished. The request was denied on the grounds that all vehicles were in use. (It was later learned that they had been transferred to a motor pool in a remote desert area.)
It was decided to concentrate personnel and vehicles in the 4 provinces of the southwestern zone: Gamo Gofa, Kefa, Ilubabor and Welega (Fig. 21.4 ; Table 21.7). Besides being epidemiologically important because they bordered on the Sudan, these provinces had a better health service structure than most, and the people’s acceptance of vaccination was generally good. Two additional vehicles and teams were assigned for work in Addis Abeba and the surrounding Shewa Province. One sanitarian was assigned to each of the other provinces to establish a smallpox eradication programme office in or near the office of the provincial medical officer. His duties were to report weekly any cases of smallpox that were discovered, to compile a list of health facilities, and to visit them, by bus or mule, in order to provide vaccine and to encourage them to report cases and to vaccinate. In the 4 priority provinces, these functions were to be undertaken by the teams, which were also expected to carry out an active search for cases and to contain by vaccination any outbreaks that were found.
Fig. 21.4. Ethiopia: zones and provinces, 1970.
Table 21.7: Ethiopia: demographic data, by zone and province and number of health facilities, 1971a
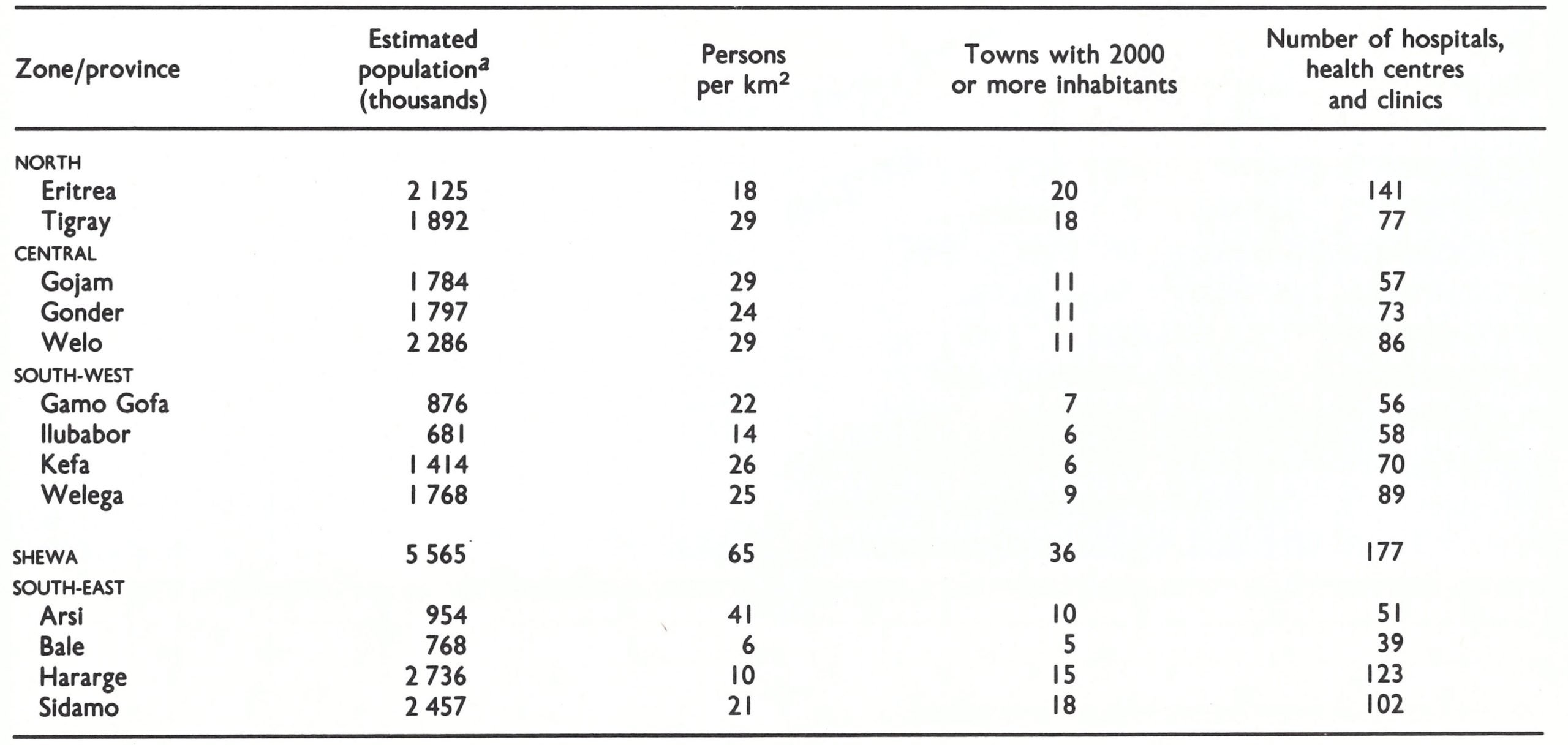 a Ethiopian government estimate for 1971. United Nations (1985) data show a total population of 26 133 000 for Ethiopia in 1971.
a Ethiopian government estimate for 1971. United Nations (1985) data show a total population of 26 133 000 for Ethiopia in 1971.
To provide encouragement and guidance to the smallpox eradication staff and other health personnel throughout the country, Dr de Quadros, in January 1971, inaugurated the publication of a surveillance report which documented smallpox incidence and conveyed important information and instructions. The report was at first distributed monthly to health personnel and relevant government officials throughout the country; late in 1974, weekly publication began. The report proved of inestimable value in securing cooperation and support and also served to sustain morale among the widely distributed smallpox eradication staff, who could contact each other only infrequently.
The number of cases that might be discovered when the teams reached the field was a subject of intense speculation. Ethiopia had reported only 197 cases in 1969 and 722 cases in 1970. It was recognized that smallpox was greatly underreported, but the extent of the underreporting was unknown. Although few vaccinations were being performed, variolation had been extensively practised throughout the country and had undoubtedly rendered many persons immune. To obtain some idea of the possible extent of smallpox, Henderson and Dr Shafa, during their visit in 1969, had questioned many health officers, mission health personnel and others, both in Addis Abeba and on a field visit to Welega Province. Surprisingly, few persons reported having seen many cases of smallpox recently and some reported having seen no cases whatsoever for many years. Although the survey was brief and incomplete, it fostered the hope that smallpox might be uncommon in the sparsely settled rural areas and that continuing endemic transmission might be confined primarily to the comparatively few populous areas.
Whatever the smallpox situation may have been in 1969, it differed greatly in 1971 from what had been expected. The teams began work in mid-January and discovered 278 cases in only 2 weeks; 1493 cases were found in February and 3434 cases in March. This amounted to half the cases being reported throughout the world at that time. Henderson was sceptical that so few field staff could discover and investigate so many cases; he therefore cabled Dr Weithaler and Dr de Quadros, cautioning against recording rumoured outbreaks without due investigation. They were justifiably indignant and replied by cable and letter that the only cases reported were those individually confirmed by the smallpox eradication staff. Dr de Quadros had established a reporting system which was similar to that used in Brazil. A form was completed for each household in which a case was discovered. The form included the name, age, sex and past history of smallpox and vaccination of each household member. Only the cases seen by the surveillance teams and recorded on the forms were reported. The Ethiopian programme, in fact, had the most comprehensive data collection system of any national eradication programme and was the only one in which data were collected from the outset.
Smallpox Surveillance and Containment in the South-west Zone in 1971
One volunteer, Mr Vincent Radke, has described his own initial surprise at the magnitude of the smallpox problem and the necessary adaptations in procedures which field staff had to make. During the training programme, the surveillance teams had been instructed to undertake a planned series of trips through the province for which they were responsible. They were to visit health centres and schools, where these existed, as well as village leaders and, in showing the WHO smallpox recognition card, were to inquire about possible smallpox cases. Any reports were then to be investigated. In the first classroom Mr Radke visited in Kefa Province, he obtained so many reports of cases in so many different villages that he did not bother to visit the other classrooms but went immediately to investigate. Village after village throughout many parts of this and other south-western provinces were found to be so heavily infected with smallpox that he and his fellowworkers decided that for some areas, even village-by-village containment vaccination was futile. Instead, they began to try to define the outer limits of the spreading epidemic and to concentrate on vaccination in populations at the circumference of the outbreak area, much as one would fight a forest fire.
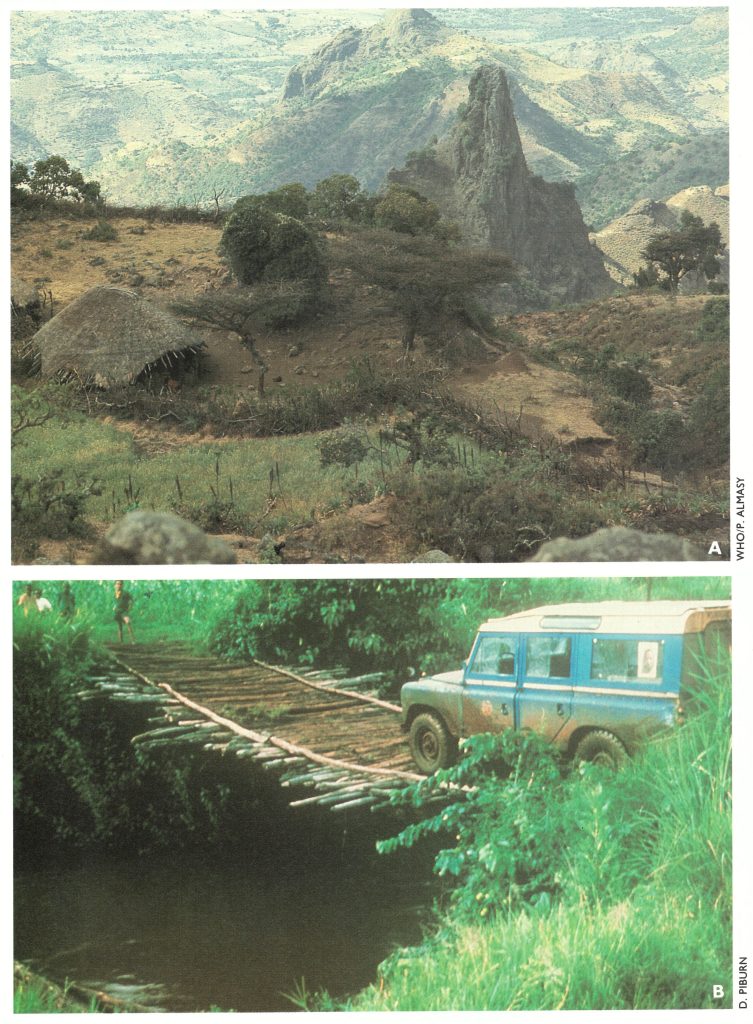
Plate 21.4. Ethiopia. A: The rugged terrain required extensive travel on foot and muleback and eventually necessitated the use of helicopters. B: Roads were few and sometimes impassable, but the bridge shown here was crossed 4 times in 1974.
Since vehicles were available only to the teams in the south-western zone and Shewa during the first 6 months, it was not expected that the health officers and sanitarians assigned to other provinces would undertake much field work. However, most of them exhibited extraordinary ingenuity in getting from place to place by bus and borrowed vehicles, by foot and by mule. They, too, discovered and investigated numerous cases of smallpox.
Up to the end of June 1971, the field staff of only 39 persons documented 13 447 cases, more than had been recorded in the whole of India during the preceding year. Meanwhile, the threat that Ethiopia represented to its smallpox-free neighbours became manifest in March, when an outbreak of 46 cases of smallpox, introduced by an Ethiopian cattle herder, was discovered in Kenya. The now evident epidemic smallpox and the concern shown by neighbouring countries served to alarm the government, and from then on the programme began to receive somewhat greater support.
Seasonal torrential rains began throughout the highlands in June and, until September, forced the surveillance teams to restrict activities to populations living along the few all-weather roads. There, in addition to a search for cases, extensive systematic vaccination campaigns were conducted in the towns and cities. In Addis Abeba itself, smallpox eradication staff, with help from the Antiepidemic Service and 12 secondary-school students, vaccinated 154 000 people over a 2-month period.
It was apparent that the problem in Ethiopia was a major one, requiring far greater resources than were available. Efforts were intensified to find such support. The government agreed to provide some additional staff but, in fact, had few available who could be mobilized except for personnel of the malaria eradication programme, but a request for the transfer of some of these staff was refused. Programme funds previously destined for countries in the WHO African Region were transferred to Ethiopia, as well as what little remained for smallpox eradication in the WHO Voluntary Fund for Health Promotion. Other Headquarters funds for 1972 were earmarked for the recruitment of another WHO epidemiologist, Dr P.A. Koswara, formerly the director of Indonesia’s successful programme. Continuing discussions with the government of Japan led to its commitment to provide 30 transceivers as well as 5 vehicles and 12 volunteers to serve as radio and automobile mechanics. The Austrian government agreed to provide 4 volunteers, and the USA to increase the number of its volunteers.
Plate 21.5. A: An Ethiopian sanitarian, Assefa Gobeze, records information about atypical cases of smallpox. B: Dimo village, Bale Region, was the site of the last outbreak of smallpox in Ethiopia in August 1976.
The end of the seasonal rains and the return of the teams to the field were eagerly awaited. During the rainy season in other parts of the world, smallpox was transmitted much less easily, and with travel restricted, the disease often died out in large areas. Moreover, the number of susceptible individuals was clearly lower than in the previous year because of the extent of the epidemics and the large-scale vaccination-containment activities that had been conducted in urban areas during the rainy season and in rural areas earlier in the year. Any hope that the smallpox problem might soon become more manageable vanished, however. The number of cases discovered totalled 2113 in September and rose each month, reaching 3322 in December.
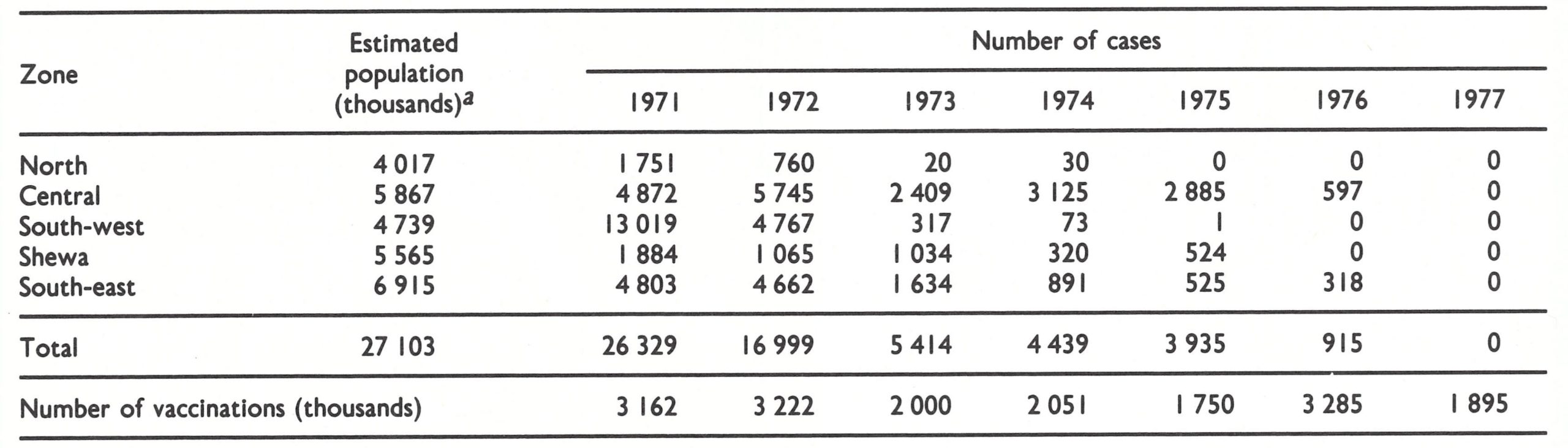
In 1971, 26 329 cases were recorded, more than half in Shewa and the 4 provinces of the south-west zone, in which reporting was the best (Table 21.8). Cases were detected in 146 of the country’s 539 woredas in the first half of the year, and in 160 woredas in the latter half (Fig. 21.5). In all, 3.1 million vaccinations were performed, nearly 15 times the number given during the preceding year, yet this figure represented no more than one-eighth of the population. It was clear that a long and difficult task lay ahead.
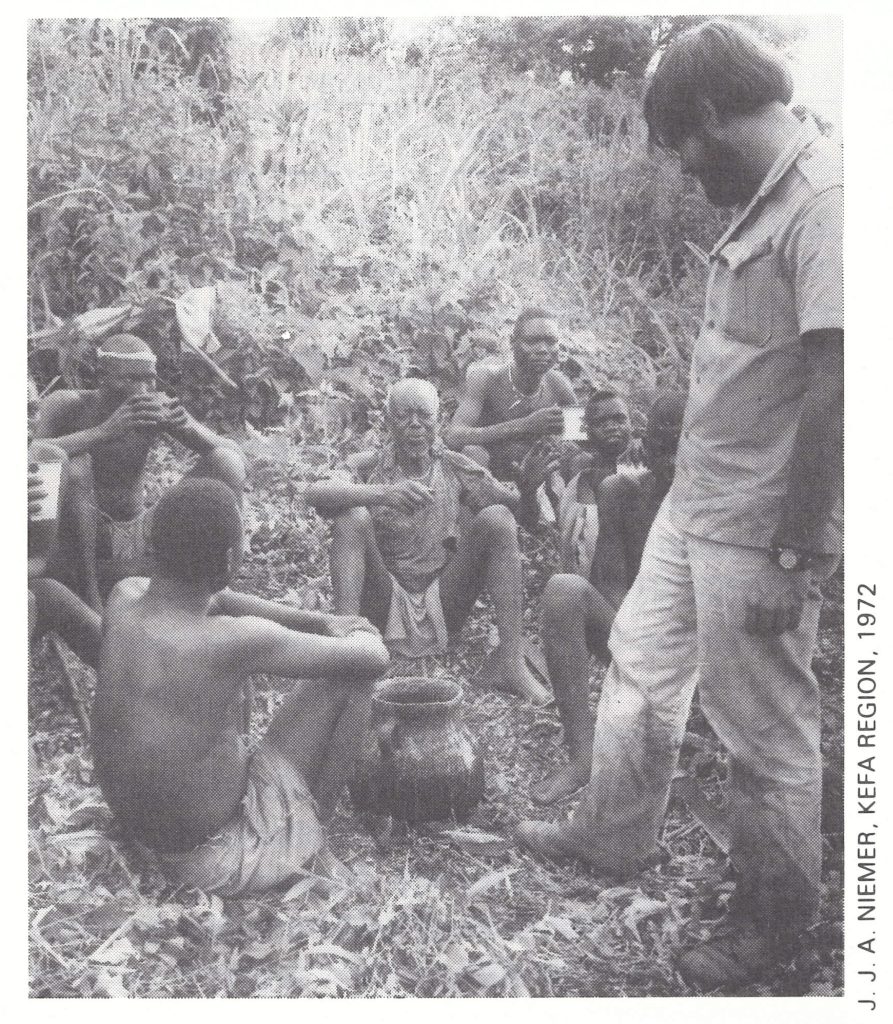
Plate 21.6. Vincent J. Radke (b. 1948) was one of 16 United States Peace Corps volunteers recruited in 1970. He worked for the eradication programme in Ethiopia for 4 years.
Table 21.8: Ethiopia: number of reported cases of smallpox and numbers of vaccinations performed, 1971-1977
 a See footnotea,Table 21.7
a See footnotea,Table 21.7
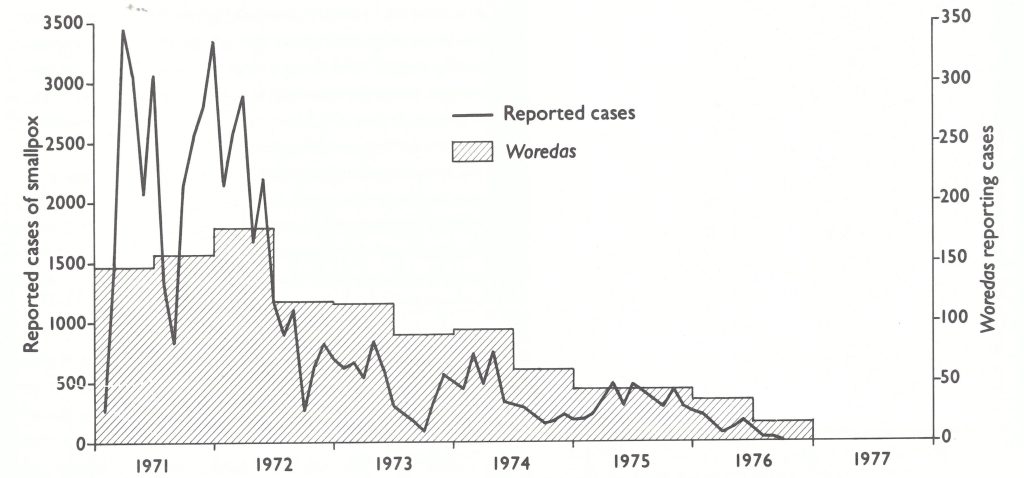
Fig. 21.5. Ethiopia: number of reported cases of smallpox, by month, and number of woredas reporting cases, by 6-month period, 1971-1977.
The Second Year, 1972
In 1972, more resources became available (Table 21.9). A staff which had grown to 67 by January 1972 rose to 82 by the end of the year as additional volunteers from Austria, Japan and the USA joined the programme. In November 1971, a special meeting was held with the provincial medical officers to explain the programme to them and to solicit their support. Gradually they, as well as staff attached to health centres, took an increasing interest in the programme and made substantial contributions. WHO assigned an additional epidemiologist—Dr G. P. Marchenko, who was transferred from the programme in Pakistan. A fleet of vehicles numbering 27 in January increased to 49 by the end of 1972, making the surveillance staff far more mobile. The transceivers, of which half were based at provincial capitals and the other half mounted on vehicles, greatly facilitated communication. Dr Weithaler and Dr de Quadros sought additional help wherever it could be found. Thus ensued, in successive years, a large number of cooperative undertakings with private and public sector groups, including the personnel of a leprosy control programme, mission groups, scientific expedition staff and emergency relief workers, all of whom were supplied with vaccine and asked to report cases of smallpox and to perform vaccinations. Volunteers were also found among visiting health professionals, a number of whom served the programme for many months without salary, receiving the same per diem as Ethiopian staff.
Table 21.9: Ethiopia: staffing patterns, 1971-1979a
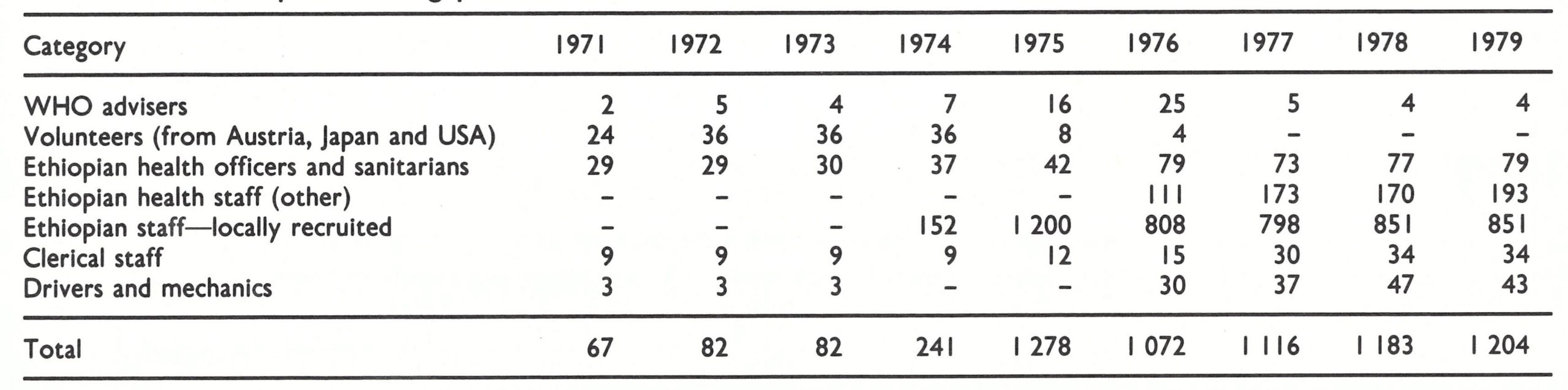 a See footnotea,Table 21.7
a See footnotea,Table 21.7
Major difficulties had, however, become more apparent. Only variola minor was found and mortality was low: in 1971, for example, only 530 deaths were recorded (a case-fatality rate of 2.1%). Even in the acute phase of illness, patients experienced so few symptoms that they were able to travel easily, spreading the disease to contacts. A second problem was widespread resistance to vaccination among the two ethnic groups, the Amhara and the Dorsey, which constituted most of the population of the central zone, northern Shewa and some adjoining areas. A third problem was the widespread practice of variolation, to which, in 1971, more than 3000 cases (12% of the total) were attributed. Many more persons than this were known to have been variolated but, as was the practice in Afghanistan (see Chapter 14), only those who developed a generalized rash in addition to a lesion at the site of inoculation were counted as cases. Lastly, it had become apparent that such maps as were available were very incomplete and often erroneous. Accordingly, the teams found it necessary to prepare their own sketch maps of each awraja and its subdivisions, the woredas, in order to identify the locations of outbreaks.
By the summer of 1972, the control of smallpox had begun to improve. During the first 6 months of 1972, the number of reported cases had remained as high as in 1971, with one-third of the 538 woredas notifying cases. During the rainy season, the number of reported cases fell steeply, as it had in the same period of the previous year. Thereafter, the number of cases recorded monthly remained below 1000 despite an increasingly comprehensive surveillance system. The total number of cases reported in 1972 was 16 999 nearly 10 000 fewer than in 1971. Most of this decrease was accounted for by a sharply diminished incidence in the last 4 months of the year, 2363 cases being reported in this period compared with 10 725 in 1971. During 1972, 3.2 million additional persons were vaccinated.
Progress in the 4 provinces of the southwest zone was highly encouraging, although not unexpected because resources had been concentrated there. Containment vaccination throughout this zone had been extensive because of the widespread outbreaks and was readily accepted, indeed actively sought, by most of the population. There were, however, some tribal groups which caused difficulties. As was reported by some of the smallpox eradication staff,”. . .many workers were suffering at one time from human bites” (WHO/SE/72.48, Tilahun et al.). By the end of 1972, vaccinations equivalent in number to more than half the estimated population had been performed in the 4 provinces and the number of reported cases of smallpox in 1972 fell by nearly two-thirds. In 2 provinces, Ilubabor and Welega, transmission was interrupted by the end of the year.
A rapidly declining incidence in Eritrea and Tigray Provinces was most unexpected, however. These provinces, whose population was nearly as large as that of the 4 provinces in the south-west, had each been assigned only one sanitarian-Ato Tadesse Fissehaye and Ato Worku Gebre Selassie, respectively. Both were dedicated and imaginative workers and proved successful in overcoming extraordinarily difficult problems. Eritrea, although endowed with substantially more extensive health facilities, communications and roads than other provinces of Ethiopia, was torn by civil war. Large areas were periodically cut off so far as road travel was concerned, while other areas were completely inaccessible to government authorities. On assuming responsibility for the programme, Ato Tadesse Fissehaye, contacted all health units to establish a reporting network and to encourage them to vaccinate both patients and nearby inhabitants. As a native Eritrean, he was able to contact dissident groups to explain the programme and obtain their cooperation . Accordingly, he was usually able to travel throughout the province, despite the civil war, to investigate and contain outbreaks. He contained 65 outbreaks with 487 cases in 1971, and 10 outbreaks with 86 cases in 1972. The last endemic case in Eritrea occurred in December 1972. Only 2 importations, resulting in 3 cases, were subsequently discovered in 1973. Tigray, which was more mountainous and had fewer resources, presented a different type of problem. There, Ato Worku Gebre Selassie persuaded the able and widely respected governor to lend his personal support to induce health and other civil authorities throughout the province to cooperate in a search for cases and their containment. Travel was not then hampered, and by the end of 1972 transmission had been interrupted in this province also. Importations were to occur in 1973 and 1974, resulting in 17 and 30 cases respectively, but both outbreaks were effectively contained. Except for these imported cases, the northern provinces remained free of smallpox after 1972. The early interruption of transmission in Eritrea and Tigray was fortunate because the intensity of civil strife in this area heightened significantly in later years, making it far more difficult to travel freely and to obtain the cooperation of the population.

Plate 21.7. Smallpox staff in Addis Abeba, 1972. Left to right: James Lepkowski (a United States Peace Corps volunteer), Ashagre Hailemariam, D. A. Henderson, Tadesse Fissehaye, and Tarekegn Hailu
A Year of Hope, 1973
In only 2 years the smallpox eradication staff, few though they were, had made remarkable progress, and the programme gained such momentum in 1973 that by the end of the year expectations were high that transmission might be interrupted within the next 12 months. The staff had become more experienced and, during twice-yearly seminar training programmes, had steadily modified and improved surveillance techniques. The staff at health centres were increasingly cooperative and participated more actively in reporting and in vaccination campaigns. In fact, 20% of all cases in 1972 were reported by the regular health services. Problems of transport and radio maintenance and repair were fewer, thanks to the Japanese volunteers; adequate supplies were available for camping and the arduous treks on foot or on muleback.
Surveillance methodology had been evaluated in June 1972 in an imaginative study which provided additional confidence in the approaches being adopted. A surveillance officer, Mr James Siemon, accompanied by a vaccinator, undertook a 14-day search in a remote mountainous awraja covering an area of 48 000 square kilometres and with a population of 275 000 (Quadros et al.,1973). No cases had been reported for 6 months. The 2-man team travelled extensively through the awraja, mainly on foot, making inquiries about smallpox cases among administrative officials and at the sole health centre and 4 health stations, at 8 schools, and at weekly markets. None of the administrative officials, village leaders or health staff knew of any cases. However, 5 different persons, at 3 markets and 2 schools, identified a single small outbreak of 8 cases in 3 households. Mr Siemon investigated the outbreak, which was 2-9 hours’ walk from each informant, and discovered it to have been caused by an importation from another province. From follow-up surveys, it was confirmed to be the only outbreak then present in the whole awraja.
A description of surveillance activities as practised at this time is helpful to an understanding of the programme and how it functioned. In most provinces, 2 surveillance teams were assigned, each team being responsible for an area with a population of 500 000 to 2 million. The team leader prepared a sketch-map and drafted a rough tour plan so that each awraja could be visited regularly. In some provinces, this often meant a walking tour of 3 or 4 weeks in just one awraja as the team progressed from valley to valley. A team of 2 workers was found to be the most practical because its members could be more readily accommodated locally. For ease of travel, they carried minimal supplies but were given letters by administrative officials to local leaders requesting that they should be provided with food and accommodation. By staying overnight with local leaders, they became better acquainted with the local people and were often able to obtain assistance from them in searching for cases and performing vaccinations. As the programme gradually began to concentrate on the more mountainous central and northern areas, vehicles were less often used because travel by foot and by mule proved more practical and permitted access to more difficult areas. Accordingly, the vehicles available to the programme staff began to be used primarily for transporting teams and supplies to points accessible by road and picking them up again at an arranged rendezvous point after 2-4 weeks. On arrival in the awraja, the team visited the offices of the awraja and then the woreda administrators to inquire whether they were aware of smallpox cases. Because there was little contact between officials and villagers at that time, this procedure was rarely useful in finding cases. However, official letters from the awraja and woreda officials helped in making contact with village leaders. The team then visited each market, clinic, school and church. Weekly markets were a feature of both rural and urban Ethiopia, and although most of the people attending lived within 3 hours’ walking distance, some travelled for as long as 3 days. For market surveillance, careful planning of the tour was required because markets were held on different days in different villages. Clinics and schools were comparatively rare but, where present, they were often a helpful source of information. Coptic churches, a prominent feature of the mountainous plateau area, convened adults for Sunday services from distances of up to 15 kilometres. Other persons encountered on tour were also questioned about smallpox.
Because the population was sparsely settled, most of the team’s time was devoted to travel. When groups were questioned about possible smallpox cases, vaccination was offered but no attempt was made to persuade those unwilling to be vaccinated or to vaccinate all persons in an area except where there was an outbreak. Outbreak containment consisted only in vaccinating those in geographical proximity. With so few staff, it was impossible for the team to remain at an outbreak site to ensure the isolation of the patient or the vaccination of absent contacts or of visitors who later came to the village. Not surprisingly, some outbreaks persisted for many weeks after the team’s departure, and some resulted in the spread of smallpox to other villages.
During the first 6 months of 1973, an average of only 590 cases was discovered each month; 115 woredas reported cases—64 fewer than during the same period of 1972. With fewer cases and fewer outbreaks, surveillance staff were able to devote more time to search, and additional manpower could be concentrated in problem areas. From April to September the number of cases decreased steadily, reaching a low of only 71 cases in September. Areas known to be infected were few in number and widely scattered except in the central zone (Fig. 21.6).
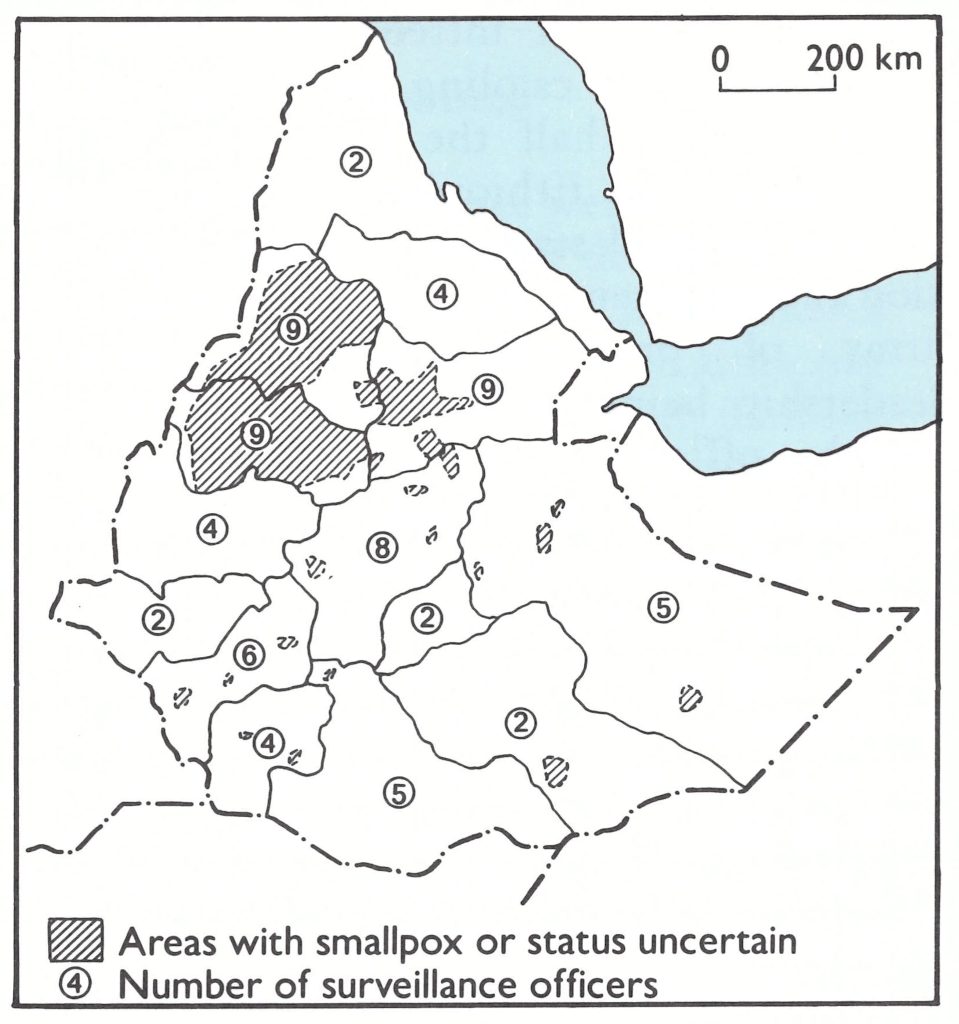
Fig. 21.6. Ethiopia: areas with endemic smallpox and number of surveillance agents assigned to each province, as of 30 September 1973.
In preparation for what was hoped might be the last smallpox season, an international seminar was convened in Addis Abeba at the end of the rainy period to which were invited representatives from the French Territory of the Afars and the Issas, Kenya and the Sudan. All these countries by this time were smallpox-free, the Sudan having been the last to eliminate the disease (at the end of 1972). Plans were coordinated for continuing surveillance along border areas and the possibility was explored for teams from these countries to undertake surveillance programmes within Ethiopia in areas adjacent to their borders. The remaining endemic areas, principally in Gojam, Gonder and Welo, were comparatively small but they posed enormous problems. The population was predominantly Amhara, many of whom adamantly refused vaccination despite the persuasive efforts of government leaders, village chiefs and priests. Meanwhile, variolation continued to be widely practised, performed by the heads of households when cases occurred in the vicinity. The terrain was the most mountainous and rugged in all of Africa and throughout much of the area security was a problem. In some areas, there was no government presence and smallpox eradication staff were forbidden to enter. It was apparent that helicopters would be invaluable for surveillance, but they were costly; appeals at this time to donor agencies as well as to the Ethiopian army met with no response.
To persuade villagers to accept vaccination sometimes required the teams to remain in an area for extended periods. The overcoming of resistance to vaccination required a somewhat different approach in each village. Some people accepted vaccination only if it was performed on the wrist (the site normally used for variolation); some would accept it only if it was administered by jet injector; in other areas, additional medications had to be provided first. Not infrequently, weeks of A Year of Turmoil, 1974 inducement and cajoling were required to vaccinate even half the population of an infected village. Ethiopian and WHO staff showed unusual stamina, courage, imagination and persistence in solving the formidable array of problems, especially notable leadership being provided by 3 Ethiopian health officers—Ato Bono Hora, Ato Wassihun Woldetensie and Ato Zein Ahmed. Time and manpower were required, however, both of which were in short supply. Because of the special problems in these provinces, 2 additional WHO epidemiologists were recruited to permit the assignment of one to each of the 3 provinces, leaving 2 advisers to work with Ethiopian coordinators throughout the remaining 11.
In the autumn of 1973, an unforeseen disaster occurred. The eastern and northeastern parts of Ethiopia experienced an extremely severe drought, followed by famine, during which an estimated 200 000 persons died. This was accompanied by an unprecedented migration of nomads into the highland areas and by a large-scale migration of the population from the endemic areas of Welo Province into other provinces. Many cases were imported into smallpox-free areas and into the neighbouring country of Somalia and the French Territory of the Afars and the Issas.
Because of the extensive movement of refugees, the number of cases increased to 542 in November and 508 in December, almost as many as had occurred during these same months in 1972. For the year as a whole, however, the 5414 recorded cases represented a decrease of nearly 70% from the 1972 figure of 16 999 cases. Ninety percent of the cases were from only 5 provinces, in which half the smallpox staff were concentrated. During 1973,2 additional provinces, Gamo Gofa and Arsi, succeeded in interrupting transmission, bringing the number of smallpox-free provinces to 6. Much had been achieved, but it was becoming apparent that the eradication of smallpox from Gonder, Welo and especially Gojam was anything but a certainty. Resistance to vaccination in these areas was reflected by the proportion of the population that had been vaccinated. By the end of 1973, 8.3 million people in Ethiopia as a whole had been vaccinated, a total equivalent to one third of the population, but in the central zone provinces, the corresponding proportion was only 20%.
A Year of Turmoil, 1974
The optimism and high expectations of early 1973 that a rapid interruption of transmission might be achieved had given way to the recognition that an arduous task lay ahead which would require the utmost persistence and imagination. Greater support from the government and the involvement of more Ethiopian staff were essential in order to cope effectively with uncooperative populations. Increased financial support from international sources was also required but was difficult to obtain. At this time, WHO considered the eradication of the severe variola major in Asia to be of higher priority, and such discretionary funds as were made available to the Organization had to be directed to the programmes in Bangladesh and India. Possible bilateral support for Ethiopia, meanwhile, remained in suspense as increasing civil strife began to envelop a country beset with economic crises, famine and rebellion against the traditional feudal system of government.
The programme’s resources were primarily concentrated in the central zone provinces but the working conditions there became increasingly difficult. Because of armed conflict, woredas and sometimes entire awrajas were declared by the army to be too dangerous to permit work to continue. In other areas, the teams had to travel with a security escort. In Welo and the south-east, in which outbreaks accompanied refugees, the teams sought and obtained assistance in reporting and vaccination from relief workers distributing food supplies.
Special assistance to the programme was provided during the early months of 1974 by health staff from the French Territory of the Afars and the Issas, Kenya and the Sudan in an exceptional display of international cooperation. It was beyond Ethiopia’s capacity to contend successfully with the outbreaks among nomads and refugees in the huge eastern desert areas. Here, with the full approval of Ethiopia, the authorities of the French Territory of the Afars and the Issas responded by providing 5 teams, comprising 46 persons supported by 20 vehicles and 3 helicopters for a 6-week programme of search and vaccination. This operation extended up to 300 kilometres inside the Ethiopian border in the eastern part of Welo and Hararge. To support the effort, Ethiopian staff established petrol depots at key points and accompanied the French teams, coordinating the overall work through the transceiver network . Meanwhile, a Sudanese team of 12 persons with 3 vehicles undertook a 2-month programme of search and vaccination throughout the western third of the difficult Gojam Province. In the south, Kenyan teams began a continuing programme of search and vaccination in Ethiopian awrajas adjacent to Kenya.
The Sudanese Search in Western Gojam Province
Search and vaccination in the difficult area of western Gojam Province were undertaken by a Sudanese team in a journey characterized by great ingenuity and determination. Travelling in 3 Land Rovers, 12 persons required 2 months to traverse some 250 kilometres through Gojam Province from the Sudanese border to the town of Bahir Dar in Ethiopia. Led by a Sudanese sanitarian, Mr Abdul Gadir El Sid, the team had to carry with it all the petrol and most of the supplies needed. Sudanese pounds were acceptable currency for the purchase of food over half the distance; for the last part of the journey, the team members needed Ethiopian dollars, and to obtain them they sold a supply of blankets which they had brought with them just for this purpose. The "roads" over which they travelled had not been traversed for years. It was necessary for them to construct bridges and in many areas to walk ahead of the vehicles, clearing a path with large knives. In some places, the underbrush was so dense that it had to be burnt (on one occasion the flames nearly consumed one of the vehicles). Mechanical breakdowns, poisonous snakes, wild animals and insects were daily problems. Nevertheless, they persisted in their journey, during which they contacted and vaccinated some 20 000 people but found no smallpox. They were gratefully received in Bahir Dar by Ethiopian staff, provided with Ethiopian dollars and, after a brief rest, returned home by the same route.
Every possible effort was being made to augment the capacity of the programme through cooperative work with the regular health services staff, relief workers and others. Even the malaria eradication staff began to participate after several cases of smallpox had occurred among the malaria workers themselves. The coordination of such disparate groups and activities was difficult, however; it became even more so when, because of the intensifying civil war, a number of foreign volunteers left the programme. Ethiopian health officers and sanitarians served to fill the gap, their efforts being augmented by students who were hired as temporary staff during an extended holiday from the university, which was closed owing to the civil unrest.
Despite the chaos and obstacles, progress continued to be made. Transmission was interrupted in April in Kefa Province, leaving the entire south-west zone smallpoxfree. In the northern zone provinces of Eritrea and Tigray, only one importation occurred and this was contained. In the south-east zone, the outbreaks were contained in the populous areas of northern Hararge by midyear. Smallpox continued to spread among desert nomads, but few of the staff believed that transmission could be long sustained in this sparsely settled area. Gonder, Gojam and Welo remained the principal areas of concern.
More resources were required for the central zone provinces and, in June, came the welcome announcement that the Surgeon General of the United States Public Health Service had arranged to make available US$220 000 from his domestic health budget allocation specifically for the lease of 2 helicopters. Planning began immediately to mount a special search programme, to commence in late 1974, as soon as the helicopters, pilots and mechanics had arrived. A Canadian company, under contract to WHO, arranged to fly the helicopters to Ethiopia and recruited Canadian pilots and mechanics, under the leadership of Mr Robert Lavack and Mr William Waugh . Meanwhile, it was decided to make intensive efforts to continue the programme throughout the rural areas despite the difficulties of travel created by the advent of the rainy season. The challenge of keeping the programme in operation was already enormous, but in 1974 the situation was exacerbated by the beginning of a major revolution. The Emperor was deposed and a new government with a different administrative structure began to take shape. An important tenet of the new government was the abolition of the feudal system of land tenure, an action welcomed in most areas but forcefully resisted in others. At the same time, the long-standing revolt in Eritrea intensified; violence increased among the Amharic peoples of the central zone; and the traditional antagonisms between Ethiopians and ethnic Somalis throughout the Ethiopian portion of the Ogaden desert erupted into sporadic open warfare as armaments began to be supplied to guerrilla forces calling themselves the Western Somalia Liberation Front. These problems persisted over the succeeding years, never completely subsiding. Some of those engaged in hostilities were supportive of the smallpox eradication programme and arranged for the staff to work in areas otherwise inaccessible to government authorities. Others, however, attacked smallpox eradication teams, kidnapped some of them, and on one occasion killed 2 of the Ethiopian vaccinators. Nevertheless, programme staff continued their work, both Ethiopian and international workers often serving in areas in which no other government staff could operate.
The Death of Dr Petrus Aswin Koswara
The emotional and physical strain associated with field work in Ethiopia was especially great in 1974; it cost the life of one WHO smallpox eradication programme adviser, Dr Petrus Aswin Koswara. He was the only WHO adviser to die while actively engaged in the programme. After serving brilliantly as the director of the successful programme in Indonesia, Dr Koswara joined the Ethiopian programme in 1972. In 1974, he was working in Welo Province, where he was responsible for the planning and logistics associated with the new helicopter-assisted search programme. On returning from Welo one afternoon after weeks of exhausting strenuous field work, he experienced severe chest pain and died that night of a heart attack. He was only 43 years old. His wife and their two children returned to Jakarta, where Dr Koswara was buried. He was decorated posthumously by the President of Indonesia and given a state funeral.
Plate 21.8. P. A. Koswara (1931-1974) seated (centre) with 2 Ethiopian colleagues, Endale Alemayehu and Tedla Tegegn, shortly before his death.
The special campaign employing helicopters began, as planned, in mid-November 1974 with the object of searching the more inaccessible highland areas. This took careful preparation as fuel depots had to be established and a scheduled programme of search elaborated for areas of which existing maps, at best, only approximately represented the actual terrain. Camping equipment and food were also necessary because supplies in the drought-stricken areas were scarce. The helicopters, operating from base camps, ferried teams into the most difficult and remote areas. Thereafter, the teams proceeded by foot and on mules to an arranged pick-up point over a period of 7-10 days. The helicopters provided logistic support and were used to transport staff to confirm rumours of outbreaks. The teams searched for cases and performed vaccinations. Where resistance to vaccination was encountered, administrative officials were flown in to help to persuade the villagers. As these operations progressed, the staff were surprised to find that, in many areas, resistance to vaccination was less of a problem than it had been before. This phenomenon was attributed in part to the dramatic appearance of teams by helicopter.
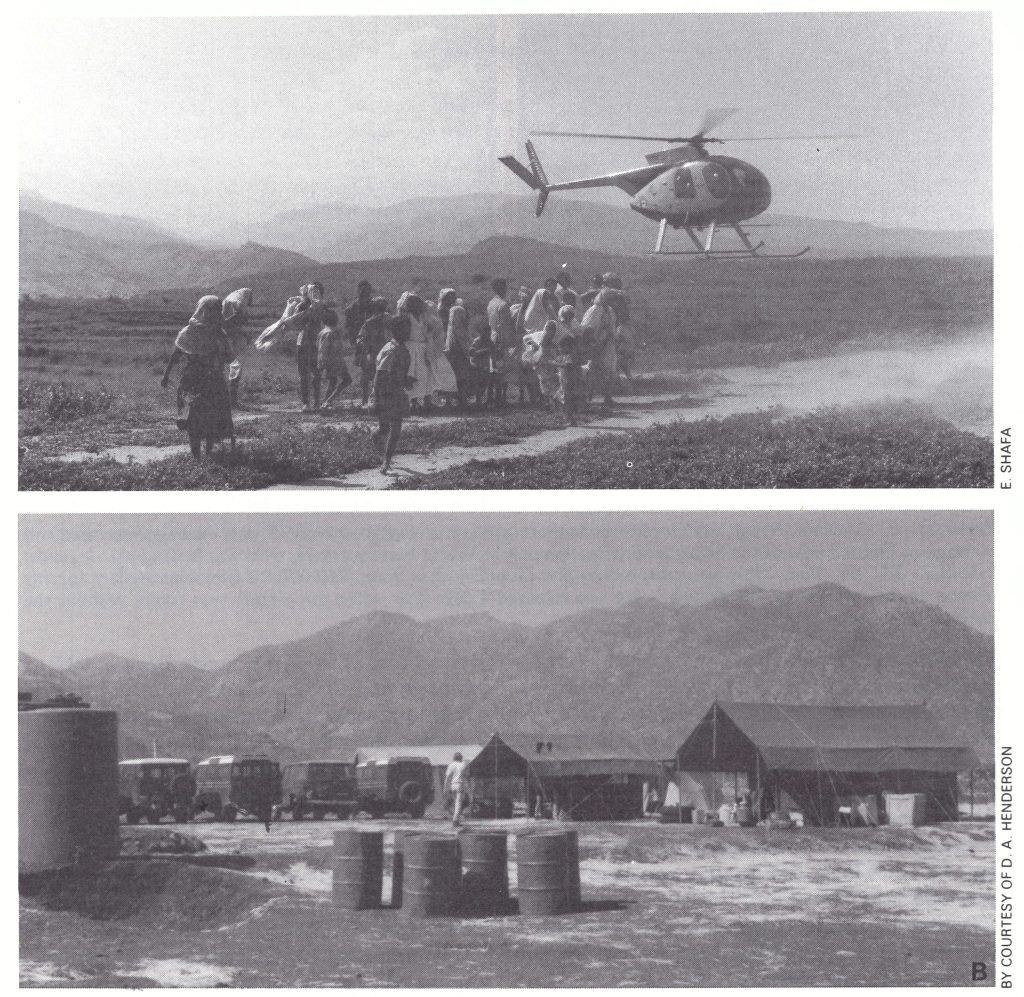
Plate 21.9. A: Helicopters were used in the Ethiopian programme from 1974 for smallpox searches in inaccessible areas. Although they could carry 4 passengers at sea level, they could not transport more than 3 persons at the high altitudes of the vast central mountainous area. B: The limited flight range made it necessary to establish depots of fuel drums in camps.
The helicopters greatly facilitated efforts but an operation such as this was costly and was attended by other problems. One hour of flying cost about US$250 and thus careful planning of use was mandatory. Moreover, the 4-passenger helicopters did not have a great range and at the high altitudes of the central plateau could not transport heavy loads. Thus, fuel depots had to be carefully sited and accessible by the heavy trucks required to transport the drums of fuel from Addis Abeba. Serious delays in the schedule occurred when helicopters experienced mechanical failures or other events took place. Such incidents included the destruction of one helicopter by a hand grenade shortly after a team’s arrival in a village; a second was hit by a bullet which penetrated the fuel line, causing a fire and a forced landing. On another occasion, a helicopter lost its bearings, made a forced landing when fuel ran out, and was not found for 2 days. And on yet another occasion some years later, rebel forces captured a helicopter and pilot and held them to ransom (Plate 21.10). Although nobody was injured or killed as a result of these incidents, some of the pilots returned home within days of arriving in Ethiopia. Most were undaunted and became as expert in the diagnosis of smallpox and the strategy of the programme as the senior programme staff.
The helicopter-supported operation detected fewer smallpox outbreaks than had been expected; most of those discovered were rapidly contained. In Gonder, few cases were found and by December the persistent focus in one awraja, which was responsible for 60% of cases in the area, had been eliminated, leaving only one seriously affected awraja. In Welo, fewer smallpox cases were discovered in the northern area than had been expected, although continuing transmission in the south remained a problem. In Gojam, by the end of the year, smallpox appeared to be limited to only 24 of the province’s 1800 debers.
By the end of 1974, 4439 cases had been discovered, 20% fewer than during the previous year; the number of provinces in which transmission had been interrupted had risen from 6 to 8 as both Kefa and Sidamo in southwestern Ethiopia became smallpox-free. Search continued in both of these provinces but the few cases that were found could be identified as importations and were quickly contained.
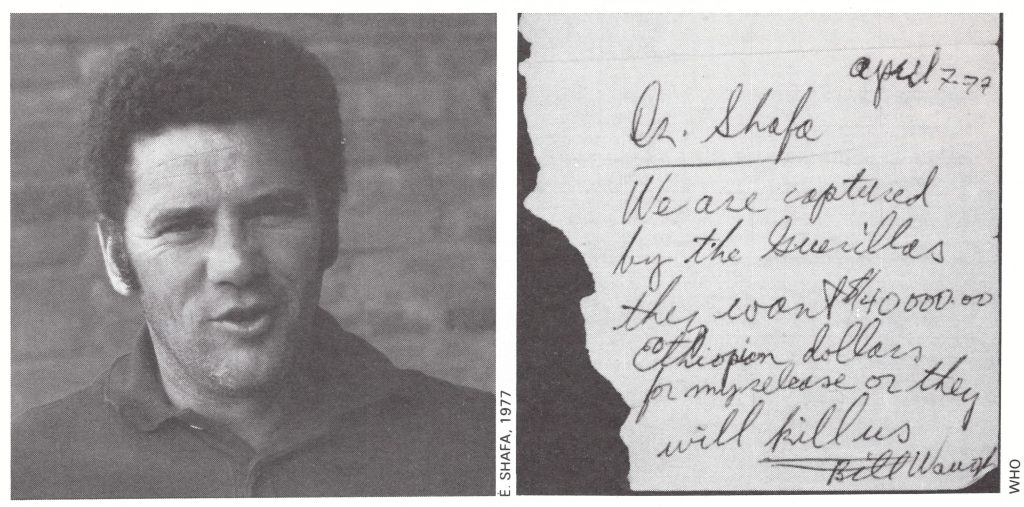
Plate 21.10. William Waugh, a Canadian helicopter pilot, was captured in 1977. He managed to send this message to Ehsan Shafa, of the Smallpox Eradication unit at WHO Headquarters, who was in Ethiopia. It reads: “April 7-77 Dr. Shafa We are captured by the Guerillas they want $40 000 .00 Ethiopian dollars for my release or they will kill us, Bill Waugh”. He was released 4 days later when this picture was taken, without the ransom having been paid.
The Final Phase, 1975-1976
At the beginning of 1975, with mounting civil disorder and with increasingly large areas in the endemic provinces inaccessible to the programme staff for long periods of time, it seemed more and more questionable whether adequate resources could be deployed sufficiently quickly and effectively to interrupt transmission. In fact, it seemed possible that the degree of control that had been achieved was at risk of being lost, which would permit smallpox to spread widely through Ethiopia and into other countries. If additional resources were to be made available, however, they would have to be drawn from other programmes. But eradication of the severe variola major in Asia continued to have priority, and although excellent progress was being made in India and Nepal, in the early months of 1975 Bangladesh experienced major epidemics (see Chapter 16) associated with famine and extensive movements of refugees. Not until the summer of 1975 was it reasonably certain that smallpox could be eliminated from Asia. When smallpox transmission was interrupted in India in May 1975 and in Bangladesh a few months later, it was possible to divert resources and energies to Ethiopia—then the world’s last remaining country with smallpox. At this favourable turn of events, Ethiopian and international staff alike renewed their endeavours to attain what had once seemed such a distant target—”Smallpox Zero”.
Throughout the summer of 1975, the staff, still numbering less than 100, continued the struggle with smallpox in the highlands of the central zone and adjacent areas of Shewa, as well as in the Ogaden desert area of Hararge (Fig. 21.7). Unexpectedly, additional manpower became available when the authorities decided to send 60 000 students into villages throughout the country in a special campaign to improve literacy. The government agreed that some could also work with the smallpox eradication teams, and thus many were trained in techniques of case search and vaccination. The students proved to be especially valuable, since they were natives of the area in which they were working and could both identify persons with political influence and induce the villagers to accept vaccination.
Progress in Asia eventually came to be measured in terms of the number of currently “active outbreaks” in a village or sector of a town—i.e., those in which a case had occurred during the preceding 6 weeks. This system of measurement was introduced into the Ethiopian programme in 1975 but it was difficult to apply. An epidemiologist was required to revisit the site of an outbreak after 6 weeks to confirm that transmission had ceased and that the site could be removed from the list of “active outbreaks”. Because of the paucity of staff and the periodic prohibitions on travel in large areas, such visits were sometimes unavoidably delayed. Moreover, it was no easy matter to deal with an Ethiopian “village”, a collection of houses often dispersed over many square kilometres. Nevertheless, the staff began to define the smallpox problem in this way and by mid-year had evolved a reasonably effective data collection system. By the end of July 1975, there were only 131 known active outbreaks occurring in 13 clusters. The clusters were spread over about 15 360 square kilometres, little more than 1 % of the country’s total area (Table 21.10). Many of the outbreaks in Gojam, Shewa and Gonder, however, had occurred in areas which the teams had been forced to leave because of civil strife, thus precluding their removal from the list of active outbreaks.
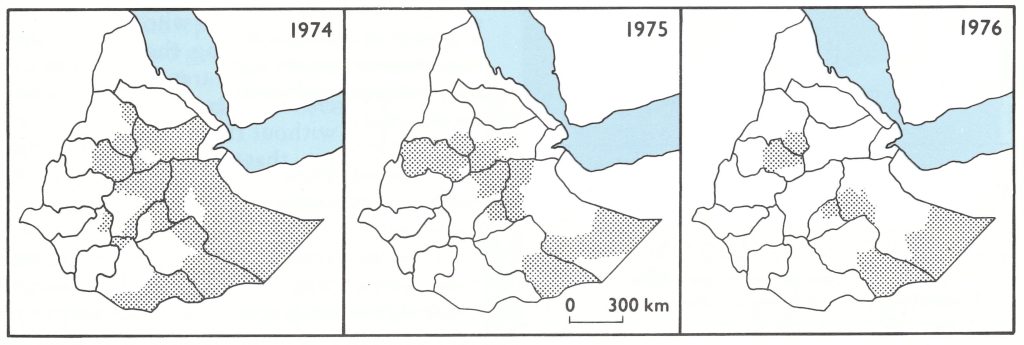
Fig. 21.7. Ethiopia: Awroja areas (shaded) in which cases of smallpox were reported, 1974-1976.
Table 21.10: Ethiopia: status of smallpox as at 23 July 1975a
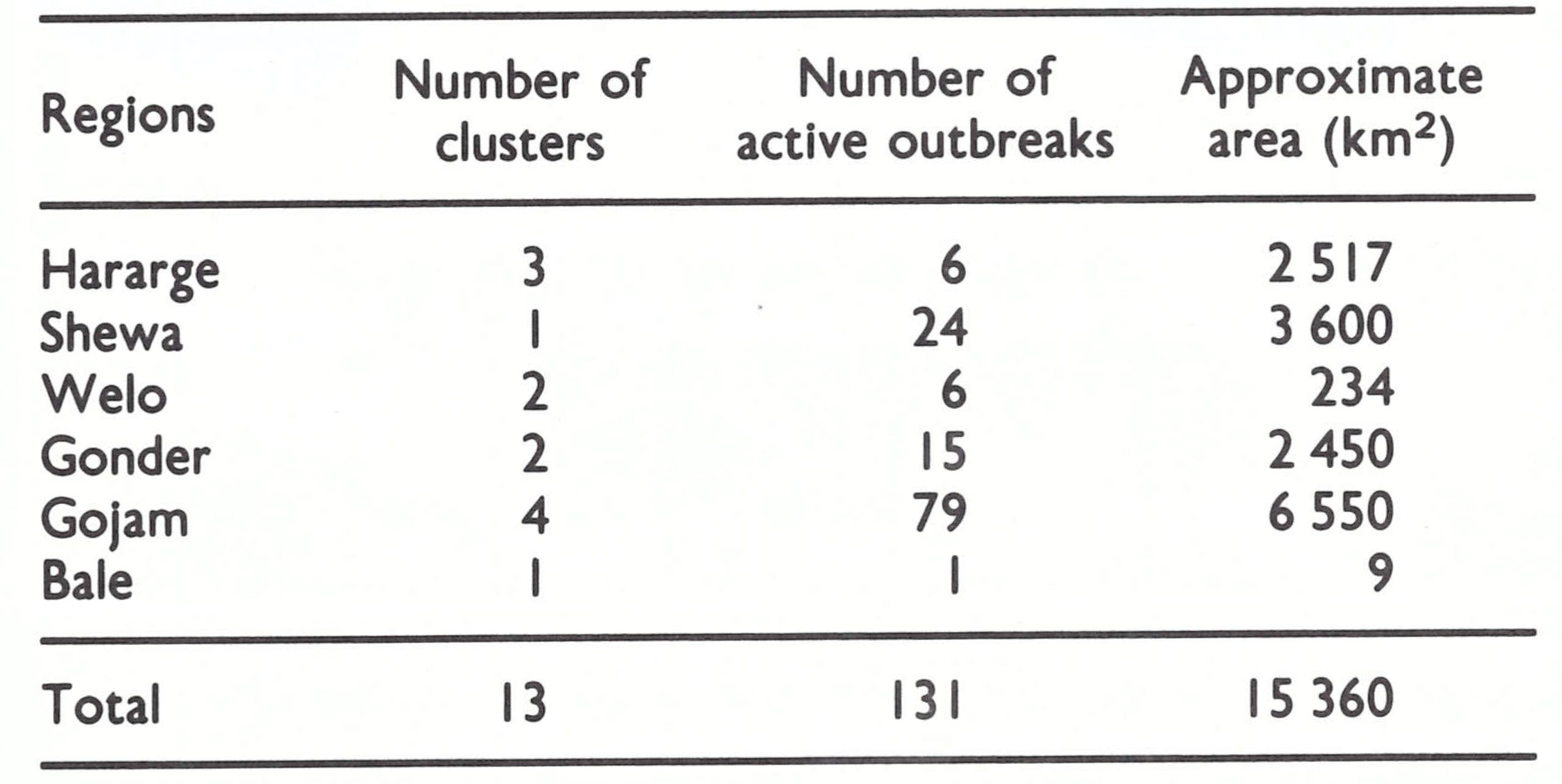
As civil disorder was so widespread, some enbassies decided that effective work in the countryside was impossible and too dangerous and so terminated the assistance of their countries; the remaining volunteers from Austria and the USA were withdrawn, although those from Japan continued to work. The smallpox eradication staff, however, believed that they might yet be successful if conditions did not deteriorate further. In fact, the problems became more acute. Petrol for vehicles, which had been in short supply, was brought to the capital by truck in an armed convoy from the coast. In June, because of the destruction of a major road bridge, the supply line was interrupted and rationing was imposed in Addis Abeba. In many parts of the country, no petrol at all was available. However, the Acting Resident Representative of the United Nations Development Programme, Mr John Phillips, who in 1971-1972 had been instrumental in initiating the smallpox programme in Botswana (see Chapter 20), worked out an imaginative scheme with the French government and an oil company to ship petrol by train from the city of Djibouti to Addis Abeba. From there it was distributed to the regions by truck and by a chartered DC-3 fixed-wing aircraft. Fortunately, there remained a large residual stockpile of aviation fuel in Addis Abeba which the government made available to the programme, thus permitting continued helicopter operations.
In July 1975, Henderson held meetings with Ethiopian and WHO staff to plan an intensified programme extending to the end of 1976. It was hoped to utilize monetary contributions from Canada, the Netherlands and the USA, vaccine from the USSR and additional support from the WHO regular budget. The revolutionary government agreed to issue a proclamation declaring the programme to be of the highest priority. The new plan provided for 85 Ethiopian surveillance officers, 16 WHO advisers and as many as 1200 temporary field staff; the number of helicopters was increased from 2 to 4; additional vehicles and considerable quantities of camping equipment were also provided.
In October, more ample facilities were made available for the programme’s headquarters, including an automotive repair shop. At the end of the year, an exceptionally able Ethiopian health officer, Ato Yemane Tekeste, was named director of the programme; Dr Weithaler continued to serve as its senior WHO adviser.
Activities steadily intensified, especially in the highland plateau areas, to which the most able Ethiopian and WHO staff were assigned. With additional locally recruited staff available, it became possible to assign teams to search for cases more widely and more frequently and to remain in outbreak areas until transmission had ceased. However, areas in which organized operations could not be undertaken because of the lack of security continued to be a problem. In many of these areas, locally recruited staff who were known to the dissidents opposing the government were sometimes able to travel quite extensively to search for cases and to vaccinate, although not without risk. It was during this period, in Gojam, that one worker was killed and a second captured and presumably killed by dissident groups.
By the end of 1975, smallpox transmission had been interrupted in 2 more regions, Shewa and Welo. No cases were detected in Gonder between July and December 1975, but because of the extent of the areas that could not be searched, the staff remained uncertain as to the true situation in the province. The main problem was presented by Gojam, in which 4 contiguous woredas in and adjacent to the Blue Nile gorge, all heavily infected, could not be entered, and from this source cases were repeatedly exported to other areas. The teams sought to contain this focus through the surveillance and vaccination of the population of adjoining areas, but many individuals resisted vaccination.
The other principal focus of smallpox was in the vast Ogaden desert. Smallpox among the nomads had spread slowly but steadily from the highlands of the north-west into the Ogaden desert area of south-eastern Hararge, with occasional spread into Bale and Arsi Regions. From the initial reports of smallpox eradication staff in the area, there appeared to be few problems in containing this focus. They guessed that the affected population was not more than 300 000, of whom a third lived along a river, readily accessible by vehicle. As a result of the vaccination of people settled along the river, of refugees receiving food at shelters, of nomads when they stopped at water-holes and of other individuals contacted during search operations, the WHO epidemiologist estimated that at least 60% of the population had been protected. In a population so sparse and scattered, and so well vaccinated as this, everyone agreed that continuing transmission should cease quickly. However, the possible spread of smallpox into the part of the Ogaden desert that lay within Somalia was also a source of concern . Accordingly, periodic border meetings were arranged between Ethiopian and Somali staff. The Somali programme director reported at one of these border meetings in August 1975 that 85% of the nomads in Somalia had been vaccinated and assured everyone that surveillance in Somalia was most thorough. Only much later did it become evident that both Somali and Ethiopian staff assigned to the Ogaden area had greatly overestimated their achievements and underestimated the size of the population and the severity of the problem.
The early months of 1976 were characterized by far more intensive efforts but increasing organizational turmoil. The arrival of additional WHO epidemiologists and the acquisition of more vehicles, 2 more helicopters and a small fixed-wing aircraft, as well as the employment of many more local staff, overtaxed the capacity of the administrative structure. The helicopters began to be scheduled for as many as 8-10 flying hours a day, which exceeded safety limits and created difficulties in providing the requisite maintenance. Close field supervision of the increased staff became more difficult; the provision of field supplies was increasingly delayed; and the effective management of funds for the field payment of temporary staff and the purchase of supplies deteriorated. On a field visit in late February 1976, Henderson found a well-organized operation in progress throughout Gojam, Welo and Gonder under the overall supervision of Dr de Quadros and directed at regional level, respectively, by Ato Bono Hora and the WHO epidemiologists, Dr P. R. Arbani from Indonesia and Mr Gary Urquhart from the USA. In other areas the situation was less satisfactory. In northern Hararge, Henderson discovered that 5 outbreaks of chickenpox had been misdiagnosed as smallpox by inexperienced field staff. The most disturbing observations were made in the Ogaden, where supervision and organization were seriously deficient. At a wateringplace only 20 kilometres from the Somali border, a smallpox isolation hut, located in the middle of a nomad camp, had no watchguard and was frequently visited by people from the camp; many unvaccinated persons were found in the area. At another camp, 2 individuals were encountered who had been infected in the office of the camp physician by patients summoned for examination from the smallpox isolation facility. It was apparent that the optimism of the field staff in the Ogaden was unfounded.
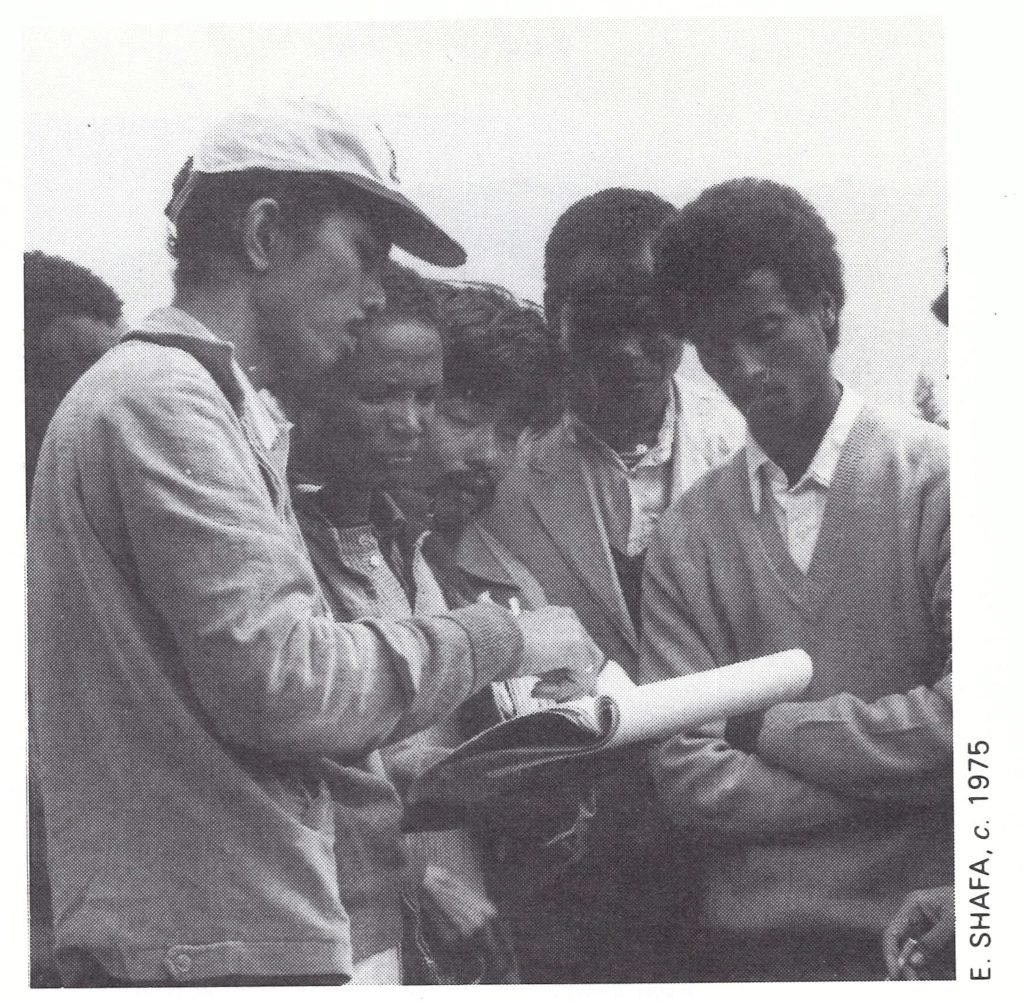
Plate 21.11. Poerwokoesoemo R. Arbani (b. 1941) was a WHO epidemiologist in Ethiopia, 1975-1979, having previously served in the same capacity in Pakistan since 1973. Before that, he had played an active role in the eradication of smallpox from Indonesia.
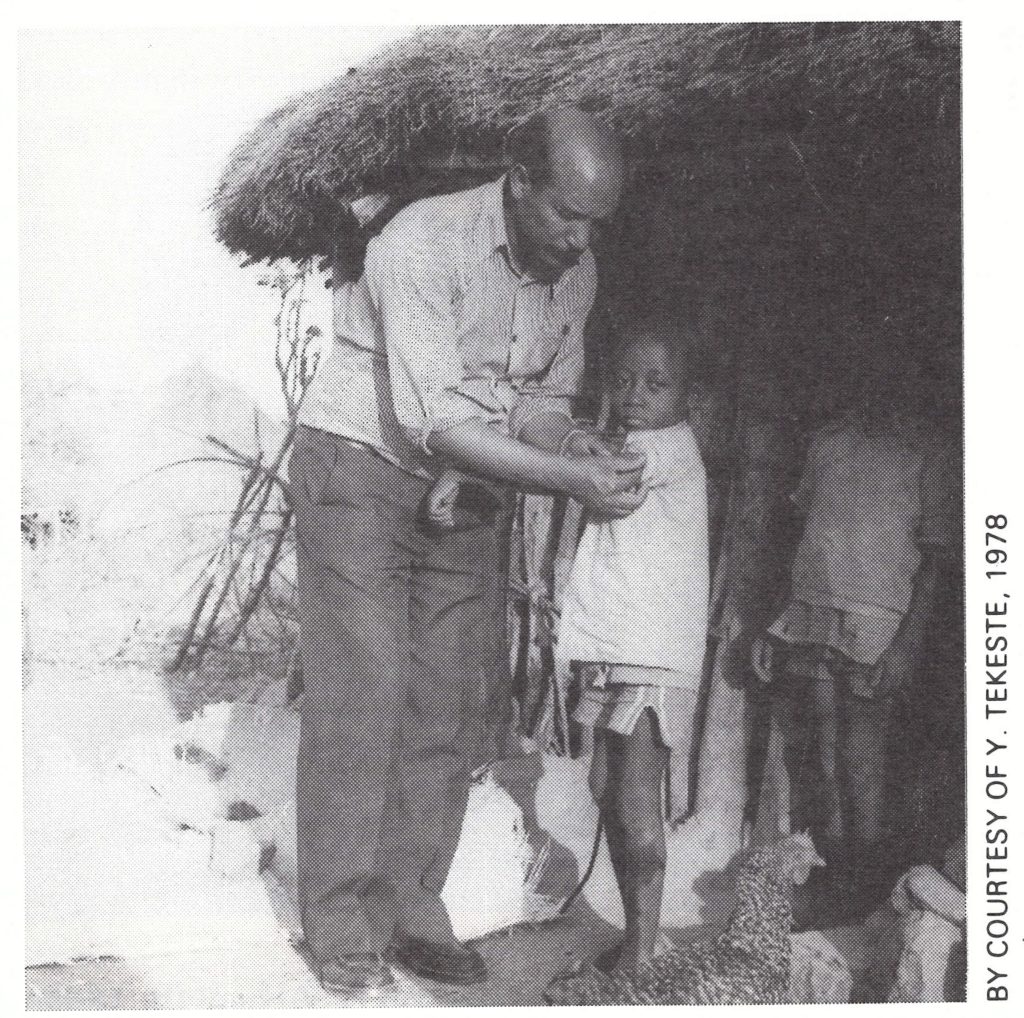
Plate 21.12. PYemane Tekeste (b. 1944), the director of the Ethiopian smallpox eradication programme, 1976-1979, checking the vaccination scar of a chickenpox patient in Gamo Gofa Region.
The management of the programme was reorganized on 5 March 1976, and from then on rapid progress was made. A special task force for the endemic regions was created, with Ato Yemane Tekeste as programme director, Dr de Quadros as chairman, Mr Lavack as director of helicopter support operations, and Mr John Copland, administrative officer for smallpox at WHO Headquarters, as finance officer. Dr Weithaler was assigned to coordinate activities in the nonendemic areas; Ato Tesfaye Temelso and the WHO epidemiologist Dr Bert van Ramshorst assumed responsibility, under the direction of the task force, for operations in the Ogaden.
The tempo of activities increased in 1976 as both government authorities and WHO staff sought desperately to contain the world’s only remaining focus of smallpox. It was possible to employ additional local staff through the use of funds made available by a special contribution from the USA of US$3 million in May of that year. New outbreaks continued to occur, however, until August (Fig. 21.8). The focus in Gojam was eventually contained by using armed civil guards who accompanied teams moving through the area; the last case occurred at the end of March. In Gonder, however, in January, after nearly 6 months without any cases having been detected, search teams were able to penetrate an awraja in the Blue Nile gorge which had been inaccessible for nearly a year, but in which fighting had recently diminished. There the teams discovered that smallpox had continued to spread (Table 21.11). Although this focus was near the outbreak area in Gojam, the two were unrelated. An intensive surveillance-containment programme was conducted, again employing civil guards, but transmission was stopped only with difficulty. As the search was extended around this area, another focus of 24 outbreaks with 140 cases was discovered 120 kilometres to the north. An itinerant musician had introduced the disease in December 1975 from the Blue Nile gorge. Fortunately, the population in the infected area proved to be receptive to vaccination, and on 29 June the last outbreak in the central zone provinces was discovered and contained.
Meanwhile in the Ogaden desert areas of Hararge and Bale, smallpox outbreaks continued to occur among the nomads, but the sources could rarely be traced because of the frequent movements of the different nomadic bands. Additional resources were deployed there in March and a better organized, more systematic pattern of search was developed employing more than 200 locally recruited staff.
In addition to helicopters, fixed-wing aircraft were chartered by WHO, and others were provided by the Netherlands and the Norwegian Save the Children Foundation. Search activities were compromised by sporadic fighting and the occasional kidnapping of staff and WHO advisers, who were taken to Somalia but eventually released through the intervention of United Nations officials. In addition, during this period 9 of the programme’s vehicles were seized and taken across the border. The Somali guerrilla forces sometimes hampered operations, but more often than not took steps to protect the teams. In one town, to which a team had been brought by helicopter, notice was given by guerrilla forces that an attack had been planned and that the team should leave. As the helicopter took off, fighting immediately broke out. On other occasions, guerrilla forces attacked government buildings, killing the occupants, but did not molest the personnel of smallpox camps in the same town. For Ethiopian and WHO staff alike, working in the Ogaden was a trying experience. Many participated in the operation but special credit must go to the dedicated Ethiopian staff, to the helicopter pilots, and to Ato Tesfaye Temelso, Dr van Ramshorst (Netherlands), Dr do Amaral (Brazil), Dr M. N. El Naggar (Egypt), Dr Alexander Gromyko (USSR), Mr Carl Hasselblad (USA) and Dr J.-P. Ryst (France).
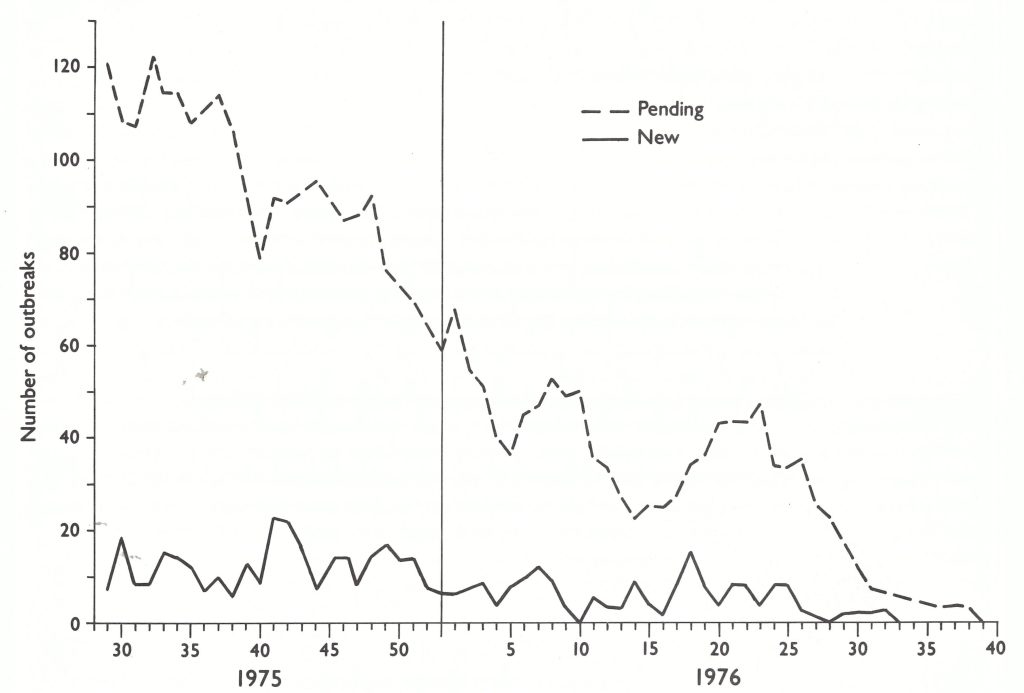
Fig. 21.8. Ethiopia: number of outbreaks pending and newly detected, by week, 1975-1976.
Table 21.11. Ethiopia: number of active outbreaks at month's end, january-September 1976
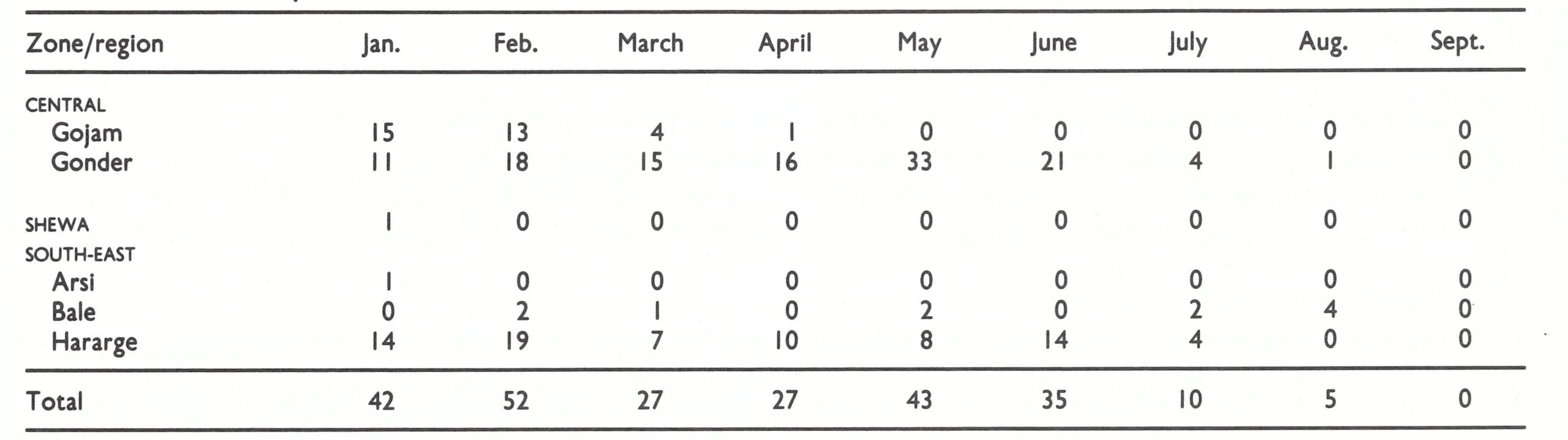
Gradually, it became apparent that in the Ogaden desert, smallpox was persisting primarily as a result of transmission back and forth between desert nomads and agriculturalists settled along the Shebele river, which divided Hararge and Bale. Efforts to control the spread, however, were severely hampered in the summer by the most serious flood in decades, which destroyed roads and river crossings and displaced numerous villagers. Across the river in the southern half of Bale, fighting between Ethiopian and guerrilla forces had greatly intensified and not until the middle of July was it possible for teams to enter this area. On 22 July, one of the teams discovered an outbreak in the small nomad village of Dimo in Bale, the first case having occurred on 5 June. Containment vaccination was immediately instituted. In all, 16 cases occurred, 9 of the persons concerned having been variolated. The Dimo outbreak proved to be the last in Ethiopia, (Table 21.11) and for many weeks it was thought to have harboured the world’s last case of smallpox—that of a 3-year-old girl who had become ill on 9 August. She had been variolated as well as vaccinated during -the incubation period of the disease.
Active search continued and intensified throughout the country, on the assumption that in a country so large and with so many inaccessible areas, smallpox must be present somewhere. In many areas, especially in the south, the task of search was greatly facilitated by the new farmers’ cooperatives and urban dwellers’ associations. Through contact with the leaders of such organizations, it was possible to explain the objectives of the programme and to enlist the assistance of the population in reporting suspected cases. To encourage such reports, a reward was offered, a practice first initiated in January 1975 in Gonder.
Surprisingly, week after week passed with no additional smallpox foci found anywhere in Ethiopia. Except for the cases found in late July and early August in the nomad village at Dimo, none occurred in the Ogaden with an onset of illness after July; in the highlands the last case had occurred on 5 July. Search teams, posted in each awraja, were able to intensify their efforts in September and October as the seasonal rains ended, but still no cases were found.
Plans were made to hold a press conference at the end of October 1976 in the expectation that an announcement could be made that 10 weeks had elapsed since the onset of what was believed to be the world’s last case of smallpox. Confirmation of eradication would require 2 full years of search, but week by week it appeared increasingly certain that no further cases would be discovered. Television crews flew to Dimo to take pictures of the village and of the last known patient, Amina Salat.
In late September plans were abruptly changed when cases of smallpox were reported from Mogadishu, the capital of Somalia. Initial disappointment that a few last imported cases had necessitated delay of the announcement turned to despair as it gradually became apparent that Somalia had endemic smallpox. Despite assurances to the contrary, neither surveillance nor vaccination activities had been well conducted. It had been anticipated that the last chapter of the global eradication of smallpox would be written in Ethiopia—but it was not to be.
A Missing Team — Chronology of Events
Work in the Ogaden was difficult enough. Guerrilla forces made it even more problematic.
Events as experienced by Ethiopian staff:
4 June 1977
Early morning—Surveillance Officer Ato Metiku reported to Addis Abeba by radio from Warder (a town in the Ogaden) that the WHO epidemiologist Dr. Claudio do Amaral and a team comprising an assistant surveillance officer, 2 interpreters, and a driver had not returned as expected on the previous evening. They had gone by Land Rover some 120 kilometers away to check on a rumoured smallpox case.
07.00 hours—The helicopter with Ato Metiku searched without success and returned to base.
10.00 hours—A fixed-wing aircraft joined in a second unsuccessful search.
15.00 hours—The two planes began a third search and at 17.50 hours, the vehicle was sighted. Because dusk had fallen it was decided to send the helicopter the following morning.
5 June 1977
06.00 hours—The helicopter flew to the site and many people were seen gathered around the vehicle waving white cloths. Fearing gunfire, the helicopter had to remain at a distance. From there, no team members could be identified.
12.00 hours—The helicopter returned to the site; this time a truck was observed parked next to the vehicle, again with many people surrounding it but no one waving.
15.00 hours—Two locally recruited Ethiopian staff volunteers were dropped near the site (about 3 kilometers away) to obtain information. Special signals were arranged for them to identify themselves to the helicopter, which would keep watch from a distance and pick them up on 6 June at a site 30 kilometers away, on signal.
16.00 hours—The helicopter returned to the site but the vehicle was gone and the volunteers could not be seen. On returning to base, the truck seen previously was spotted. As the helicopter flew closer 2 individuals jumped from the truck and began firing at it.
Evening—At a special meeting, it was decided to bring in a second helicopter for search; 2 additional Ethiopian staff volunteered to be dropped at the site on the following morning hoping to learn something of the fate of their colleagues and of the team.
6 June 1977
07.30 hours—The volunteers were dropped at the site; helicopter search continued over a widening area.
14.00 hours—A flight over the original area revealed no sign of the volunteers.
16.00 hours—The helicopters flew to the pick-up site; one volunteer was seen but did not signal. Pilot returned to base at 19.15 hours.
Evening—Ato Metiku arranged in secret with the town-dwellers' association for a group of villagers to walk to the site.
7 June 1977
It was decided that all the aircraft should undertake a final area-wide search and then await instructions. Arrangements were made for a DC-3 fixed-wing aircraft to fly additional fuel to the area. The volunteers were located and retrieved by the helicopter; they had been unable to obtain any information.
8 June 1977
The Director-General of WHO sent a telex from Geneva to the Minister of Health of Somalia requesting assistance from the Somali border guards. Daily telex and telephone contact was established by Geneva with Addis Abeba and Mogadishu.
9 June 1977
A surveillance officer from Warder reported that a villager had told him that he had seen Dr. do Amaral and the team on 6 June being taken by guerrilla forces to Deghbur, another area in the Ogaden.
Ato Yemane Tekeste and another high-ranking Ethiopian official left for Deghbur to be available to participate in negotiations should the captors make contact with the government.
11 June 1977
A telex was received in Geneva from the WHO Representative in Mogadishu with the message that the team was in Hargeisa, Somalia.
3 June 1977
We left Warder at 07.00 hours to investigate a rumoured smallpox case 120 kilometers to the north. About 80 kilometers from Warder, 2 men with sub-machine-guns started shooting at us and ordered us to stop. Within minutes, they were joined by many others who ordered us out of the car, took everything we had and made us lie on our backs with our arms up. At that moment, I thought it was the last day of my life! Suddenly, one of their leaders appeared and took us to a village 300 meters from where we had been captured. He identified the group as being soldiers of the Western Somalia Liberation Front. We talked about the smallpox eradication programme and what we were doing, but he said that we had no right to be in the area, and emphasized that they could release us or kill us as they chose. We were given Somali dress and provided with goat meat and camel milk. We slept that night in the open air guarded by 2 men with sub-machine-guns.
5 June 1977
In the morning, we again saw the helicopter and with a gun at my head, I was told to contact the pilot by radio to request him to land. I convinced our captors, however, that radio contact was not possible. The leader then ordered me to take off my shirt so that they would see my white skin and be persuaded to land. Again, I refused, persuading him that the pilot could not recognize color from such a great distance. Fortunately, neither plane tried to land. Surprisingly, in the late afternoon, a vaccinator appeared who was from the village to which we had intended to go. He reported that the case we had intended to see was chickenpox, not smallpox! We were then driven to another village, where, we were told, we should be informed as to what would be done with us.
8 June 1977
After 2 days when nothing appeared to be happening, we were driven to yet another village, 120 kilometers further away, where we met a more senior leader. Once again, I showed my passport, explained I was Brazilian and described the smallpox eradication programme. To my great surprise, he knew all about our movements as well as the names of all the epidemiologists and where they were stationed. The leader said they would hand us over to the Somali authorities. That night they gave us a small hut and blankets for sleeping.
11 June 1977
We were handed over to the National Somalia Security authorities and arrangements were made for me to fly to Mogadishu on 18 June and to Addis Abeba on 22 June. The vehicle, after repair, was to be returned to Ethiopia.
Morbidity and Mortality Data
From the time the programme began, data collected from all households in which cases occurred included the name, age and sex of all residents and their past experience with regard to smallpox, vaccination and variolation. Data from Ethiopia are, in fact, more complete than those from any other country which experienced extensive endemic smallpox. Information on the age and outcome of illness are available for 54 991 of the 58 031 cases reported from 1971 to 1976 (Table 21.12). One-fourth of all cases (26%) occurred among persons aged 15 years and over who comprised 57% of the population The large proportion of cases among adults is characteristic of an area in which the presence of smallpox was infrequent among much of the population. The proportion of cases among those less than 1 year of age (2%) is almost certainly understated because, in many areas, very young children with smallpox were often hidden from investigators.
Only variola minor was observed. No outbreaks were discovered with case-fatality rates comparable to those in Asia or western Africa. The overall case-fatality rate was calculated at 1.5%. The true figure may, however, be somewhat higher because outbreaks that occurred in the early years of the programme were not observed throughout their course and the deaths of some patients during the second or third week of illness may have been missed. Nevertheless, it is doubtful that the actual rate was much higher than 2%, a rate characteristic of variola minor.
Cases occurred almost exclusively among the “never vaccinated” group, only 961 of 49 106 persons of known vaccination status having previously been vaccinated. Even some of those listed as “vaccinated” had been vaccinated too late in the incubation period of the disease to be protected. Of the total number of cases, 7.3% occurred among persons who had been variolated.
Secondary attack rates among susceptible individuals within families were comparable to those measured elsewhere. Nearly 80% of children under 15 years of age who were exposed in households contracted the disease. Lower secondary attack rates among adults (43.6%) may reflect diminished levels of exposure, but they may, in part, be understated because of the failure of adults to recall past infection (Table 21.13).
Comparatively few children under 15 years of age were immune because of previous smallpox, which suggests that the disease had not been widely prevalent for a number of years. Among household contacts of cases as a whole, approximately equal numbers were immune as a result of variolation and vaccination. Three times as many had previously experienced smallpox.
Finally, data regarding the source of infection of outbreaks (if known) revealed that the disease rarely spread over long distances. Of 6957 outbreaks analysed, a source of infection was ascertained for 4565. Of these, the source of 3956 (87%) was from contact in the same woreda and of another 362 (8%) in the same awraja. Only 1 in 20 originated in another awraja.
Table 21.12. Ethiopia: number of reported cases of and deaths from smallpox and case-fatality rates, by age, 1971-1976
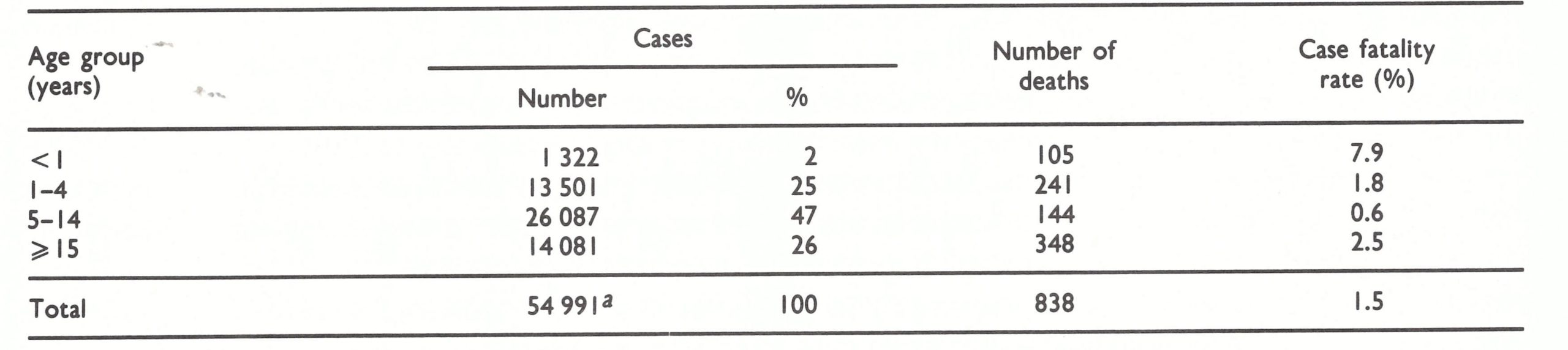 a Data unavailable for an additional 3040 cases occurring In this period.
a Data unavailable for an additional 3040 cases occurring In this period.
Table 21.13. Ethiopia: secondary attack rates among susceptible household contacts, by age, 1971-1974
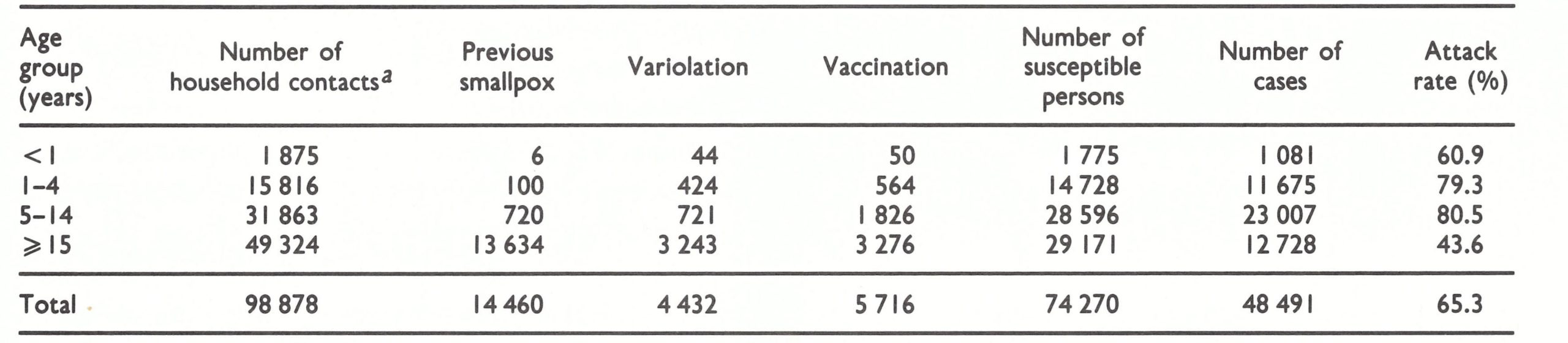 a In 20 398 households.
a In 20 398 households.
Plate 21.13. National and international staff planning search strategy around the last foci of smallpox in Ethiopia. Left to right: Zewde Besha, Muchie Kidanu, Mitiku Haile, C. do Amaral.
Exportation of Cases
Ethiopia, as had been feared, was a source of infection for neighbouring countries. The Sudan, which had been smallpox-free in 1967 (see Chapter 18), was reinfected by cases from Ethiopia in 1967-1968 and the disease subsequently became endemic there. One additional importation occurred in the Sudan in December 1972 but was quickly contained. Kenya experienced 2 imported cases in 1970-1971 with 44 secondary cases; 2 imported cases and 2 further cases in 1973; and 1 imported case with 5 further cases in 1976 (see Chapter 19, Fig. 19.4).
The French Territory of the Afars and the Issas and Somalia were the most subject to importations. The former, in December 1971, recorded an outbreak of 104 cases following an importation; in 1973, 10 separate importations occurred with 4 secondary cases; and in March 1974,12 cases were reported following 1 or possibly 2 importations. Somalia, from 1962 to 1972, recorded only 2 cases of smallpox (1966); the origin of these was unknown. However, from December 1972 to the end of August 1976, when Ethiopia detected its last case, 42 cases were reported, of which 38 were said to have been importations, the last of these occurring in March 1976, 5 months before Ethiopia interrupted transmission. No further cases were reported from Somalia until October. Those cases were said to have originated in Ethiopia but in fact, as was later discovered, endemic smallpox had by then become re-established in Somalia and the official reports of field investigations, at least during the latter part of 1976, were unreliable.
CONCLUSIONS
Ethiopia proved to be as formidable a challenge to the Intensified Smallpox Eradication Programme as any country in the world, and at every stage. For nearly 3 years, the government not only declined to discuss a possible eradication programme, but actively opposed it. The idea of a national programme was eventually accepted, with reluctance, and, when it was launched in 1971—the fifth year of the Intensified Programme—little support was given by the government either in resources or in commitment. For more than 3 years, a staff proportionately smaller in number than in any other endemic country struggled valiantly, but with remarkable success, to contain the disease in one of the most rugged and difficult terrains in the world and among hostile populations to whom vaccination was all but unknown. Escalating civil war and famine further confounded the endeavour. The fact that the disease was of the mild variola minor variety increased the difficulty, because the population was not particularly eager to be vaccinated; many who were ill with smallpox were able to travel widely, spreading the disease as they went. Adequate resources could not be made available until late in 1975, but with much of the country then smallpox free, less than a year elapsed before transmission was interrupted. Subsequently, search activities to certify the absence of smallpox were well supported by the government and resources for the task became available. But less than a year later, in 1977, the Somali-Ethiopian war broke out, rendering inaccessible a large portion of the area in which the last cases had occurred. Only through a surveillance programme conducted from bases in Somalia was it possible to continue activities in the troubled Ogaden desert and to confirm the absence of smallpox.
It is a tribute to a dedicated WHO staff and a small band of extraordinarily capable Ethiopian health officers and sanitarians that programme activities were continued at all during several years in many parts of the country. For many years and in many areas, smallpox eradication was virtually the only health programme in operation in the field, and WHO smallpox staff were almost the only expatriate workers who ventured outside the major cities.
Global smallpox eradication was in jeopardy on numerous occasions and in many countries, but nowhere was the outcome so greatly in doubt, and for so long, as in Ethiopia.
Prospects for the successful interruption of smallpox transmission in Yemen had not originally appeared to be much more encouraging than in Ethiopia, and indeed the programme, such as it was, was reasonably well executed only during its first year. Yemen, however, was far smaller in size and population; variola major, rather than variola minor, had predominated but apparently had spontaneously died out before the programme began. In Democratic Yemen, whose population was even smaller than that of Yemen, the WHO-supported programme was better executed, but its achievement primarily consisted in confirming the absence of smallpox.
In retrospect, it would have paid rich dividends strategically if, in Ethiopia, greater attention had been paid to smallpox in the Ogaden desert area at an earlier stage. The most competent staff and the larger proportion of resources were initially assigned to the difficult mountainous plateau areas of the north in the expectation that smallpox transmission would soon terminate—for the most part spontaneously—among the desert nomads. Until March 1976 the programme in the Ogaden was modest and, as became evident, not well organized. When a fully effective programme did take shape, it was soon discovered that vaccinial immunity was far lower than had been recorded, reporting was poor and containment ineffective. Smallpox continued to spread among nomads, but in August 1976 the last known outbreak was finally contained. This would have marked the end of smallpox if the WHO-supported programme in Somalia had been conducted as well as it was reported to have been. However, uncontained importations into Somalia set the stage for yet one more major programme in a country that had previously been free of smallpox. These events are the subject of the next chapter.