Chapter 26:
Certification of 29 countries of Africa and Asia: 1978-1979

INTRODUCTION
By June 1977 international commissions had already visited or were preparing to visit all the previously endemic countries and countries at special risk. However, as has been explained in Chapter 24, there was a need to determine what measures should be taken in order to certify that the transmission of smallpox had been interrupted for at least 2 years in other countries, in several of which the staff of the WHO Smallpox Eradication Programme needed outside advice on how best to deal with the situation. In addition, advice on whether global eradication could be certified needed to be, and to be seen to be, independent of the special interests of WHO personnel who were intimately involved in the global eradication programme.
These problems could be solved by establishing a global commission of respected scientists which, as one of its functions, would advise the staff of the WHO Smallpox Eradication unit as to what data should be collected, for clearly this was a matter of judgement. Eventually, when these experts were fully satisfied that global eradication had been achieved, this conclusion would have been reached, not by WHO itself, or on the basis of the reports of a series of international commissions each dealing with one or a few countries, but by an international group of senior scientists and administrators capable of taking a global view of the problem. For this reason, the Consultation on the Worldwide Certification of Smallpox Eradication was set up in October 1977 and subsequently converted into the Global Commission for the Certification of Smallpox Eradication. This chapter and the next deal with activities undertaken at the suggestion of the Consultation and the Global Commission throughout 1978 and 1979; it was hoped that these would provide data on which the Global Commission could ultimately base its opinion that the transmission of smallpox had been interrupted everywhere in the world.
In this chapter, various operations carried out in 29 countries situated in widely separated parts of Africa and Asia (Fig. 26.1) are described. Not all were certified by formal international commissions such as those referred to in Chapter 25 ; other procedures—a visit by a WHO-designated expert or consultant and subsequent report, or the provision of a detailed country report—had to be used for some countries (Fig. 26.2).

Fig. 26.1. The 29 countries of Asia and Africa (including Lesotho and Swaziland) in which certification was carried out in 1978 or 1979 by international commissions, by visits by a WHO-designated expert or by the provision of a detailed country report (see Fig. 26.2).
In Africa, by mid-1977, formal certification had been successfully completed in 24 countries in western and central Africa (Chapter 25). At that time, smallpox was still occurring in Somalia, so that certification of the Horn of Africa lay in the future (Chapter 27). There remained 14 countries requiring certification, extending from the Sudan in the north to South Africa in the south, and from Angola in the west to Madagascar in the east. The strategy of certification by international commissions, as recommended by the 1977 Consultation, was followed for 10 of them (Fig. 26.2, No. 1-10), but for political and logistic reasons it was not possible to follow the Consultation’s recommendations for South Africa, Namibia or Southern Rhodesia (Fig. 26.2, No. 13-15). Instead, certification by the Global Commission was based on reports prepared by Global Commission members and WHO consultants after visits arranged by the Smallpox Eradication unit. As recommended by the Consultation, eradication in Madagascar was certified by the Global Commission after receipt of a detailed country report, followed up by a visit by a WHO staff member.
For 11 countries in south-western Asia, certification by various procedures was recommended. Democratic Yemen, Yemen, Iraq and the Syrian Arab Republic (Fig. 26.2, No.11, 12, 18 and 19) were visited by international commissions. Iran was visited by experts and certified by the Global Commission on the basis of their reports. The 6 Arab countries of the Gulf area (Fig. 26.2, No. 20-25) were required to submit a country report. At their request a more searching inquiry was made; each country carried out an intensive surveillance programme designed and supervised by a WHO epidemiologist.
For 5 countries in eastern Asia, the Consultation had recommended special certification activities. China, because of its vast size and population and its lack of contact with WHO for many years, required the special measures described in Chapter 27. There remained Thailand and the wartorn countries of Democratic Kampuchea, the Lao People’s Democratic Republic and VietNam. The fact that there had never been a WHO-sponsored smallpox eradication programme in the 3 last mentioned countries, and that their health systems had been compromised by prolonged warfare, made it difficult to collect data or arrange visits by WHO consultants or staff members. Thailand was visited by a member of the Global Commission; for the other countries reliance had to be placed on reports compiled from a variety of sources.
In this chapter, the certification of 14 countries in Africa is first described, then that of the 11 countries in south-western Asia and finally that of Thailand, Democratic Kampuchea, the Lao People’s Democratic Republic and Viet Nam. All these operations were undertaken while, at the same time, the most intensive search activities of the whole eradication programme were being carried out in the Horn of Africa. The operations mounted to certify eradication in Ethiopia, Somalia, Djibouti and Kenya, and in China, are described in Chapter 27.
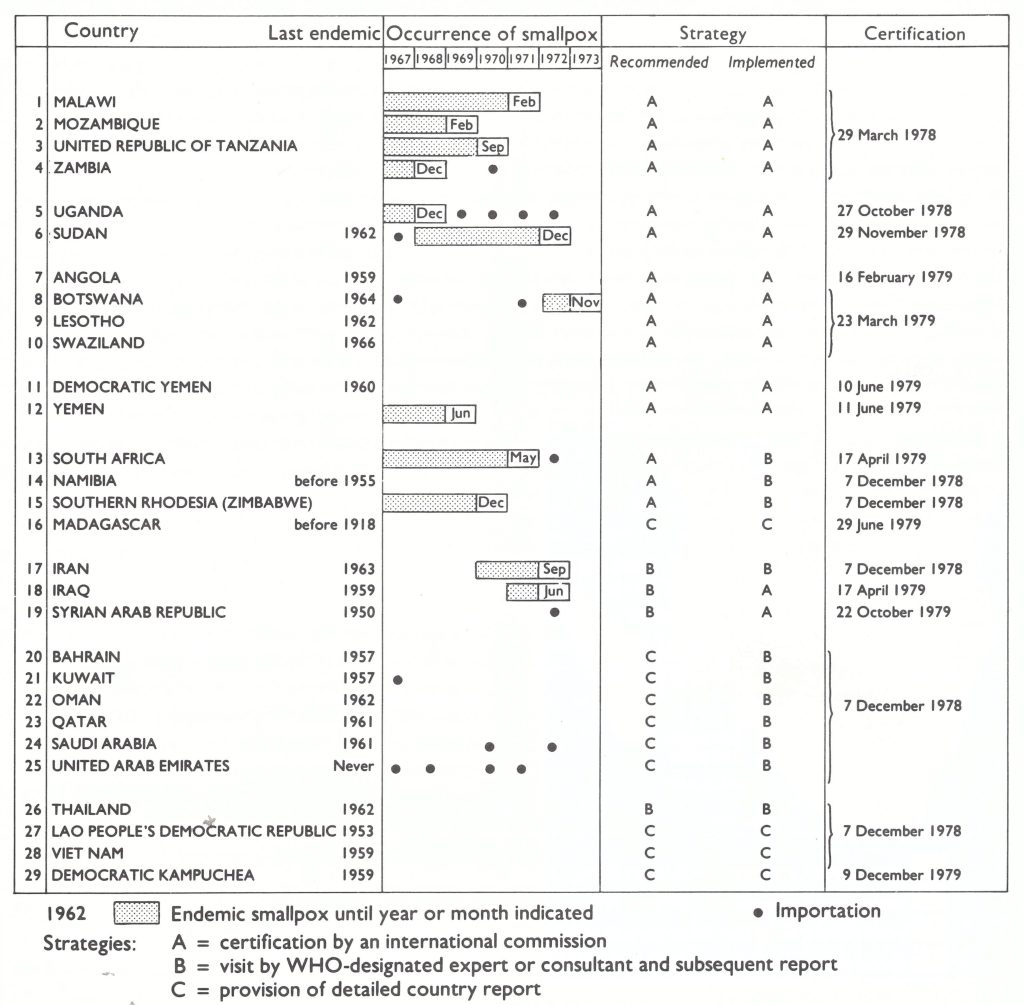
Fig. 26.2. Year of the last case of endemic smallpox and of importations of smallpox, and dates of certification of 14 countries in Africa and I5 countries in Asia according to the strategies recommended by the Consultation on the Worldwide Certification of Smallpox Eradication, October 1977. and as implemented.
SOUTHERN AFRICA
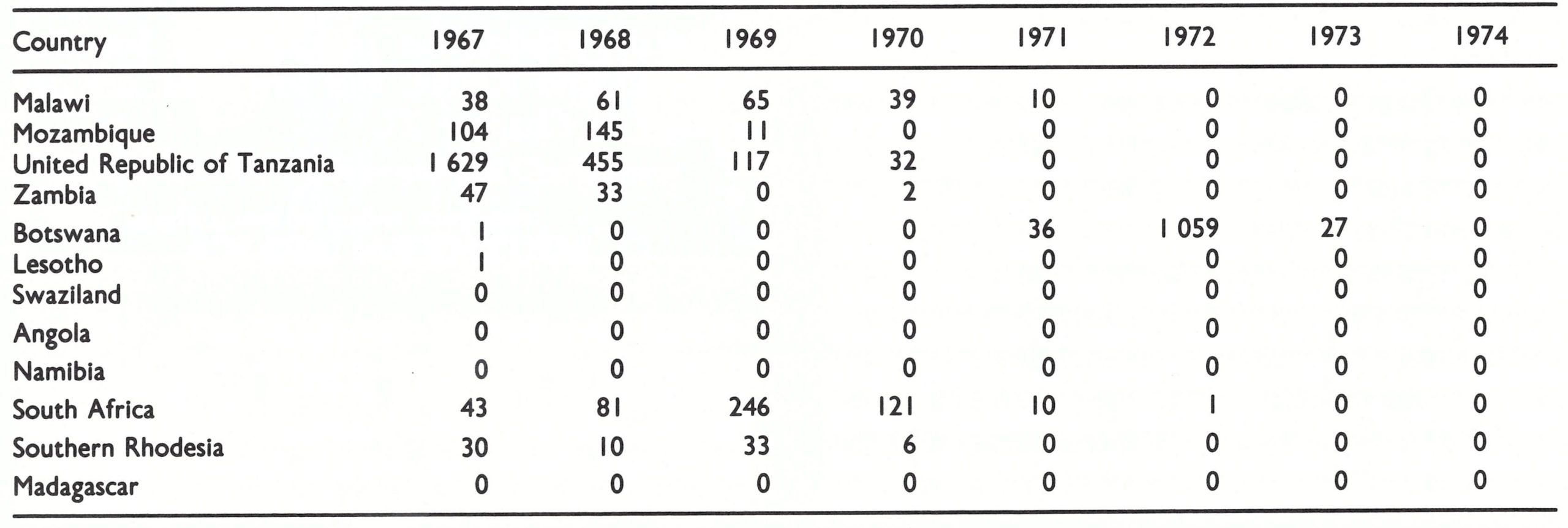
The progress of certification in the 12 countries of southern Africa (Angola, Botswana, Lesotho, Madagascar, Malawi, Mozambique, Namibia, South Africa, Southern Rhodesia, Swaziland, the United Republic of Tanzania, and Zambia) is shown in Fig. 26.3. No smallpox had been reported in any of these countries since 1972, except for an outbreak of variola minor in Botswana in 1971-1973, following an importation from South Africa late in 1971 (Table 26.1).
Civil unrest and, indeed, open warfare had been occurring in Angola, Mozambique and Southern Rhodesia since the mid-1970s. South Africa, Namibia (which was controlled by South Africa) and Southern Rhodesia (then regarded by the United Nations as a British colony) were not represented at the World Health Assembly. This complicated the organization of certification by international commissions. Eventually such commissions were able to visit Angola and Mozambique, where they met with no difficulties. However, there were political difficulties in organizing WHO-sponsored international commissions to certify smallpox eradication in Southern Rhodesia and Namibia, and attempts to arrange for an international commission to visit South Africa (which provided the only route of entry to Namibia) were thought unlikely to be successful or at best unduly time-consuming, owing to political factors. The recommendation of the Consultation on the Worldwide Certification of Smallpox Eradication that an international commission should visit these 3 countries (see Chapter 24) was therefore not followed. Instead, arrangements were made to obtain country reports and other necessary data by organizing visits by a Global Commission member and WHO consultants who were acceptable to the respective national governments. This proved to be quite straightforward in Southern Rhodesia and Namibia, but several visits to South Africa were needed before the requisite data could be obtained.
Fig. 26.3. Countries of southern Africa certified free of smallpox by international commissions or visited by a member of the Global Commission or WHO-designated expert before certification by that Commission
Table 26.1: Numbers of reported cases of smallpox in I2 countries of southern Africa, 1967-1974
Logistics
Experience in western and central Africa had shown clearly the difficulties faced by the small staff of the Smallpox Eradication unit and the relevant personnel in the WHO Regional Office for Africa in arranging simultaneous precertification activities in many countries. Furthermore, it was impossible to find experts of sufficient experience to form the international commissions if members were required to travel too often and to too many different countries. To simplify certification, 2 groupings were therefore made of small numbers of countries, as follows: (1) Malawi, Mozambique, the United Republic of Tanzania, and Zambia; and (2) Botswana, Lesotho and Swaziland. The remaining 5 countries were dealt with separately. Angola, in particular, was a large country in which there had been serious civil disturbances both before and after it achieved independence in 1975 so that it was uncertain whether commission members would be able to travel extensively enough for certification to be possible. For this reason, a separate international commission was established for Angola so as not to prejudice the certification of any other country that might be grouped with it. The political problems associated with Namibia, South Africa and Southern Rhodesia have already been mentioned, while Madagascar, as an island, was a special case.
For the first time since certification in South America in 1973, the problem had to be faced that the variety of smallpox most recently present in some of these countries was mainly variola minor. In this situation, pockmark surveys, which had proved so useful in the countries of western and central Africa, were much less likely to reveal recent transmission of smallpox, because facial scars persisted in less than 10% of patients. To supplement such pockmark surveys as were performed, intensive surveillance for cases of chickenpox was carried out, and specimens were collected for laboratory examination-a procedure which reached its apogee in certification operations in the Horn of Africa (see Chapter 27). Surveillance for cases of chickenpox provided a measure of the sensitivity of the reporting system and permitted specimens to be collected from cases and outbreaks over a wide area. If cases had mistakenly been diagnosed as chickenpox instead of variola minor, this would be revealed by laboratory studies. Moreover, by obtaining material from outbreaks in which a patient had died, presumably of chickenpox, the likelihood of detecting smallpox, if it were present, was increased.
Time Schedules for Certification
Since there were so many countries for which certification was required by the end of 1979, all certification activities had to meet a strict time schedule. Further, if one of a group of neighbouring countries failed to achieve certification, none of the countries in that group could be certified. Various measures were taken to accelerate certification and maintain uniform progress —e.g., countries were requested to send information on the progress made in preparations for certification to the WHO Regional Office for Africa by cable every month. An example of such a request is reproduced below. Although formal communications were with the Regional Office, it was important that the epidemiologists in Nairobi and the Smallpox Eradication unit in Geneva should be kept informed of the situation; hence a copy of the cable was sent to each of them.
Outgoing cable:
“Reference progress SME [smallpox eradication] certification activities from now onwards please deliver to AFRO [Regional Office for Africa] a monthly cable to monitor status commission preparation including AAA cumulative totals pockmark surveys since surveys began BBB total number localities chosen for field surveys ccc total number localities visited by teams DDD total number of persons seen in schools or elsewhere EEE number of persons with facial pockmarks FFF number of specimens collected for laboratory study stop Please begin this cable report thirty October and forward thereafter on day thirty of subsequent months to AFRO with copy SME HQ [Smallpox Eradication unit] and ICP ES 005 [Epidemiological Surveillance of Diseases Intercountry Project] epidemiologists Nairobi and Maputo.”
Malawi, Mozambique, United Republic of Tanzania, and Zambia
Precertfication activities
These countries had recorded their last cases of smallpox between 1969 and 1971 (Table 26.1). Dr Ziaul Islam, a WHO epidemiologist based in Nairobi, who had worked on both the western and central African certification programmes, took the major role in precertification activities in this group of countries.
The preparation of country reports started early in 1977 while the certification of central Africa was in progress. In July 1977, a coordination meeting attended by WHO regional and Headquarters staff was held in Brazzaville, Congo, to assess progress. It was decided at this meeting that, in addition to pockmark surveys, a programme for the surveillance of chickenpox cases, with emphasis on the collection of specimens for laboratory examination, should have a high priority in the preparations for certification. It was proposed that at least 100 specimens from chickenpox patients should be collected in each country, from outbreaks separated in both space and time. By October 1977, Dr Islam had visited Malawi, the United Republic of Tanzania, and Zambia at least once to assist with the pockmark surveys and chickenpox surveillance. It was estimated that by December 1977 all the preparations for visits by an international commission would be completed.
Pockmark surveys. As part of the preparations for certification, pockmark surveys were carried out in each country, covering 3.2% of their combined population of 38.2 million (Table 26.2). No pockmarked children were seen among 70 621 children of preschool age, nor had any person with facial pockmarks suffered from smallpox later than 1970.
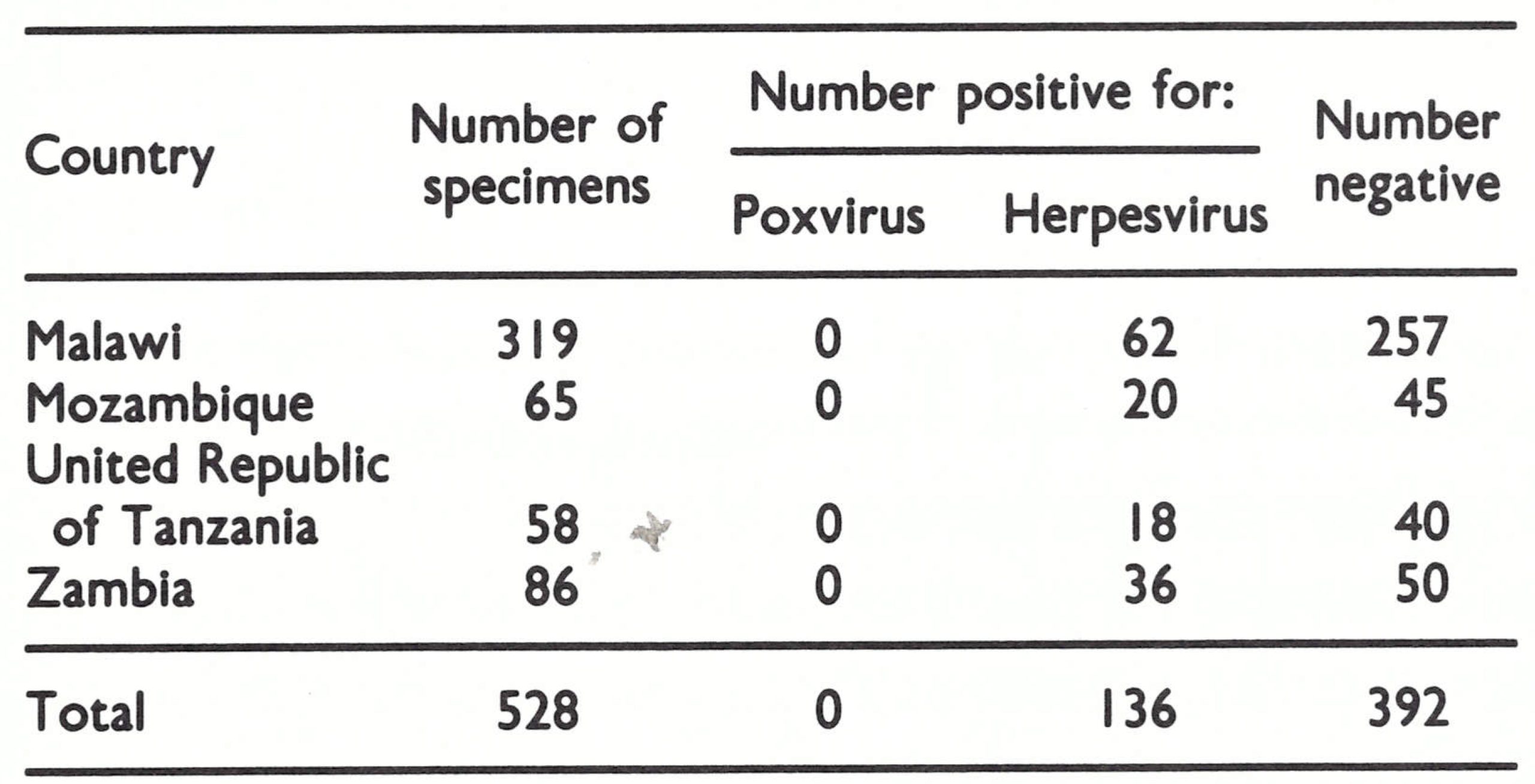
Chickenpox surveillance. In accordance with the decision made at the coordination meeting at Brazzaville in July 1977, all countries had collected a number of specimens from cases clinically diagnosed as chickenpox (Table 26.3). When examined at the WHO collaborating centres, no specimens showed poxvirus particles by electron microscopy and cultures for orthopoxviruses were uniformly negative. Herpesvirus particles were seen in 26% of the specimens.
Continued transmission in Malawi. During preparations for certification in Malawi, evidence was obtained which showed that smallpox transmission had continued for a long period of time without being recognized by the health services. The last reported case occurred in December 1969. In April 1972, Dr Islam discovered in a remote part of southern Malawi 48 individuals with facial pockmarks who had contracted their infections between April 1970 and February 1971—i.e., up to 14 months after the last reported case (see Chapter 20). Subsequently, during the precertification surveys, a joint Malawi-WHO team discovered a pockmarked girl and 2 other possible cases in the same area who gave a history of having been infected in September 1972. The exact status of these cases was never determined, but it was eventually concluded that, among the illiterate rural population, information given as to the year of illness was unreliable, and that the last case in Malawi had occurred in an outbreak that terminated spontaneously in 1971 without being detected by health staff.
Table 26.2: Malawi, Mozambique, United Republic of Tanzania, and Zambia: results of facial pockmark surveys conducted during precertificatlon activities, 1977-1978
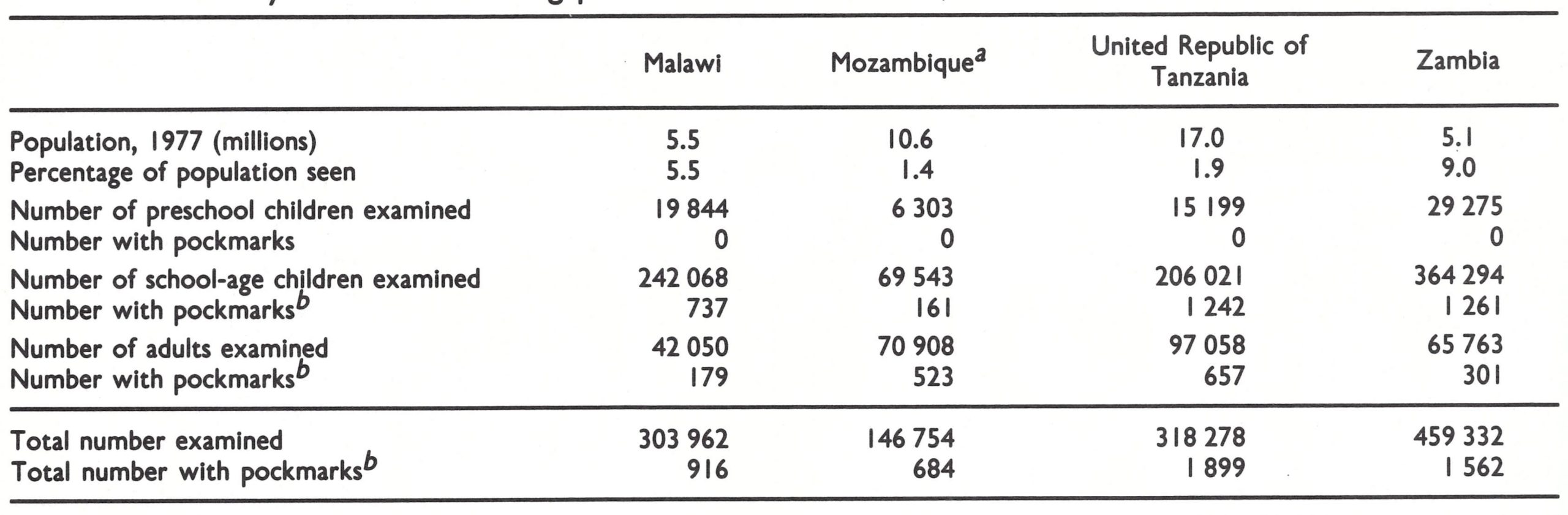 a In addition, in surveys carried out during the national mass vaccination campaign (June 1976-February I978), 35 589 persons were found with facial pockmarks among 7 379 265 persons examined. None of them had contracted smallpox after 1969.
a In addition, in surveys carried out during the national mass vaccination campaign (June 1976-February I978), 35 589 persons were found with facial pockmarks among 7 379 265 persons examined. None of them had contracted smallpox after 1969.
b Due to smallpox contracted before 1971.
Table 26.3: Malawi, Mozambique, United Republic of Tanzania, and Zambia: laboratory examination of specimens from cases clinically diagnosed as chickenpox, 1977-1978
Difficulties in precerttfication activities. WHO-assisted national smallpox eradication programmes had operated in Malawi, the United Republic of Tanzania, and Zambia, but the sensitivity of the surveillance system for smallpox had diminished in each of these countries since 1974. WHO had not been involved in smallpox eradication work in Mozambique. The precertification surveys just described were made possible only by detailing a WHO epidemiologist to work with designated national health workers in each country. Some logistic problems arose—e.g., in Mozambique, in which available resources were insufficient to permit the carrying out of a pockmark survey and extra funds had therefore to be provided to cover petrol costs and living allowances. Three new vehicles were also needed, but only for 2-3 months, so that it would have been wasteful to purchase them. Furthermore, they could not have been obtained in time, since procurement usually took 12 months. This problem was solved when the vehicles were made available by the WHO Expanded Programme on Immunization and money to cover local expenses was provided by WHO.
Visit Ly the International Commission, 6- 29 March 1978
An International Commission for the Certification of Smallpox Eradication met in Maputo, Mozambique, from 6 to 9 March 1978. After reviewing the data from all 4 countries, the Commission set up 4 teams, one for each country, and reassembled for its final meeting in Lusaka, Zambia, 27 to 29 March.
After extensive travel throughout each country and examination of the reporting networks and of the data provided in the country reports, the Commission decided that, if smallpox transmission had continued after the date of the last known case, it would have been detected. The circumstances of the missed outbreak in Malawi were carefully scrutinized, but the epidemiological evidence indicated that the last case had occurred in 1971. The Commission noted that, even if the disease had persisted until September 1972, this was over 5 years ago, and the local situation had been examined in detail both by the joint Malawi-WHO team in precertification activities and by the Commission member during his visit. At its final plenary meeting in Lusaka the Commission agreed that the 4 countries should be certified to be free of smallpox.

Plate 26.1. Participants in the final meeting of the International Commission for the Certification of Smallpox Eradication in Malawi, Mozambique, the United Republic of Tanzania and Zambia, held in Lusaka, Zambia, 29 March 1978. Left to right: I.H. Chu (WHO), A.H. Abou-Gareeb (WHO), Z.M. Dlamini (Swaziland), I. Arita (WHO), J. Moeti (Botswana), J.A. Espmark (Sweden), M. Davies (Sierra Leone), J.G. Breman (WHO), M. Altmann (WHO), P. Dordevic (WHO), I. D. Ladnyi (WHO), F. Fenner (Australia), Z. Islam (WHO), C. Algan (WHO). The names of the Commission members are in bold type.
Botswana, Lesotho and Swaziland
Coordination meeting
During the International Commission’s visit to Lusaka in March 1978, mentioned above, a coordination meeting was held to discuss strategies for the certification of the remaining countries in southern Africa. It was attended by Dr Celal Algan and staff from the WHO Regional Office for Africa, Dr Joel Breman, formerly of the Center for Disease Control, Atlanta, USA, who had recently joined the Smallpox Eradication unit, and Arita. Apart from the Horn of Africa, where smallpox remained endemic until 1977, the last case in Africa had been reported in Botswana in November 1973. The small landlocked countries of Lesotho and Swaziland had experienced their last outbreaks in 1962 and 1966 respectively.
Although the 6 adjacent countries of Botswana, Lesotho, Namibia, South Africa, Southern Rhodesia and Swaziland formed an epidemiological unit (see Fig. 26.3), the coordination meeting decided that it would be very time-consuming and perhaps politically difficult to arrange for simultaneous precertification surveys and the certification of these countries by one or even several international commissions. Botswana was the only one of them in which WHO had been involved in a smallpox eradication programme when, after the outbreak there in 1971, a WHO team had assisted an augmented national programme. It was decided that arrangements should be made for the visit of an international commission to Botswana, Lesotho and Swaziland in March 1979, and that preparations for precertification activities in those 3 countries should begin immediately. Other measures were to be taken to obtain the information necessary to certify smallpox eradication in Namibia, South Africa and Southern Rhodesia (see below).
Precertification activities
The last outbreak of smallpox in the region had been due to very mild variola minor in Botswana in 1971-1973 (see Chapter 20), and variola minor was the predominant variety of smallpox recently prevalent in South Africa, by which Lesotho was completely and Swaziland almost completely surrounded. However, outbreaks of variola major had occurred in all these countries in the past, and it was decided to carry out both pockmark surveys and chickenpox surveillance. Dr Moises Altmann, a WHO epidemiologist stationed in Maputo, Mozambique, assisted the national health authorities in their preparations for the commission’s visit. Progress was initially rather slow, but by January 1979 all 3 countries had prepared country reports and completed pockmark and chickenpox surveys.
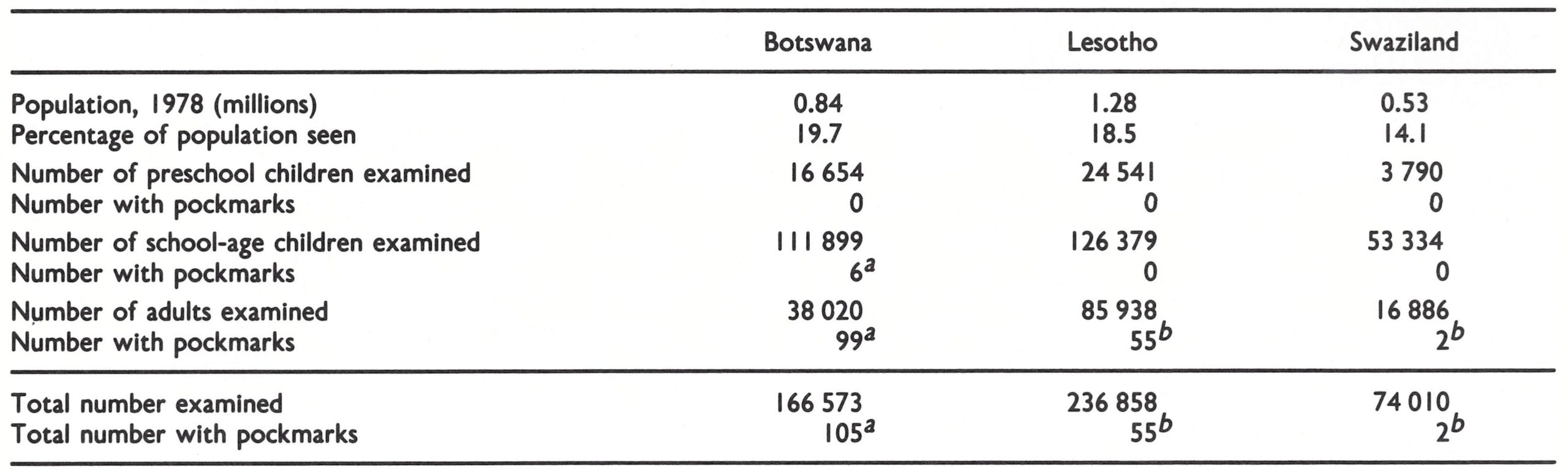
Pockmark surveys. The pockmark surveys covered a large proportion of the small populations of the 3 countries (Table 26.4). No facial pockmarks were seen in 44 985 children of preschool age and only 6 cases (all in Botswana) were found among 291 612 schoolchildren. Pockmarks were somewhat more common in adults, being seen in 0.26% in Botswana and a smaller proportion in Lesotho and Swaziland, and heavy facial scarring was found only in adults, reflecting the outbreaks of variola major in the 1950s and 1960s.
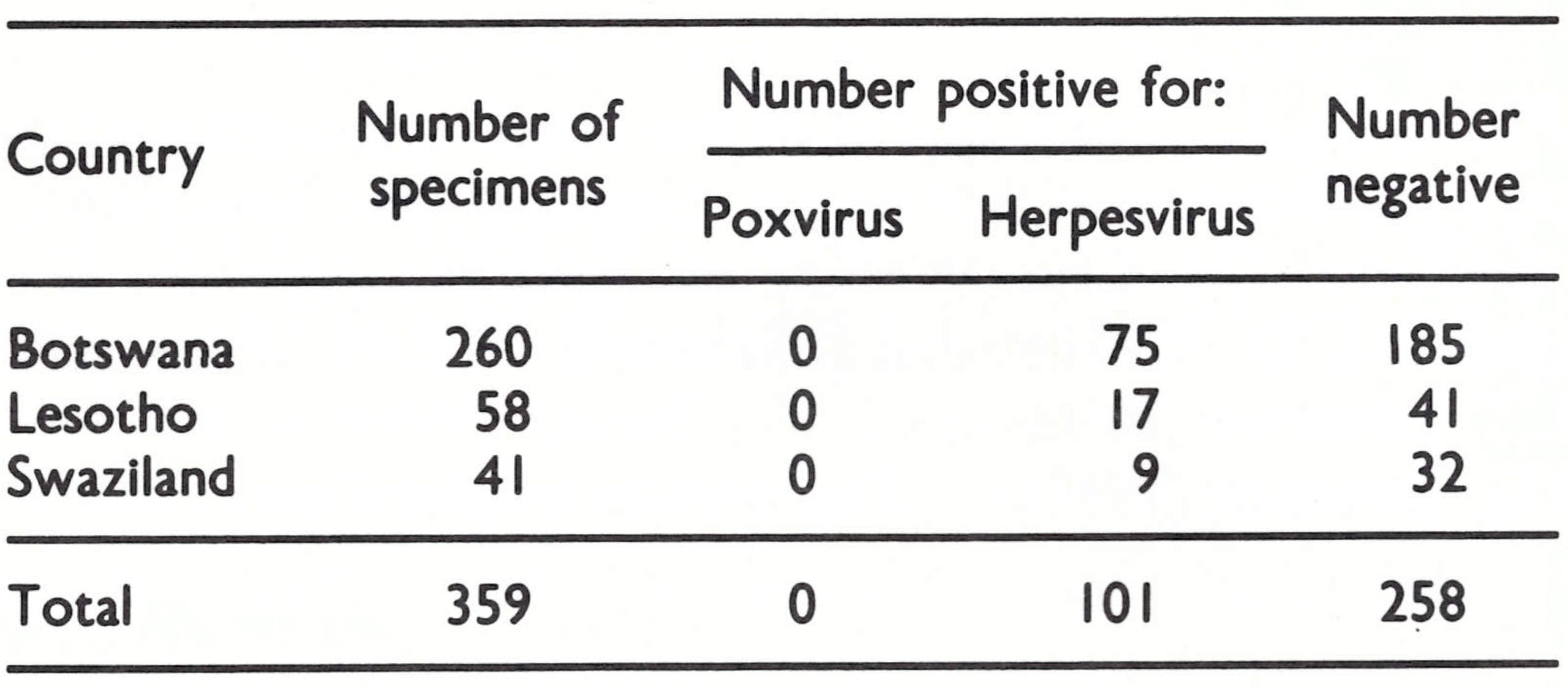
Chickenpox surveillance. Specimens were collected from cases of chickenpox during precertification surveillance, care being taken to obtain specimens from as many separate outbreaks as possible. They were examined at WHO collaborating centres. None contained poxvirus, but herpesvirus particles were seenwith the electron microscope in 28% of the specimens (Table 26.5).
Table 26.4: Botswana, Lesotho and Swaziland: results of facial pockmark surveys conducted during precertification activities, 1978-1979
 a Due to smallpox contracted before 1974.
a Due to smallpox contracted before 1974.
a Due to smallpox contracted before 1971.
Table 26.5: Botswana, Lesotho and Swaziland: laboratory examination of specimens from cases clinically diagnosed as chickenpox, 1978-1979
Visit by the International Commission, 5-23 March 1979
The first meeting of the International Commission was held in Gaborone, Botswana, from 5 to 7 March 1979. In addition to examining the country reports for these 3 countries, the Commission reviewed the data available at that time on smallpox eradication in the 3 neighbouring countries, Namibia, South Africa and Southern Rhodesia, because these 6 countries formed an epidemiological unit. The Commission then divided into 3 groups, which visited Botswana, Lesotho and Swaziland respectively, and reassembled for final discussions in Mbabane, Swaziland, between 21 and 23 March.
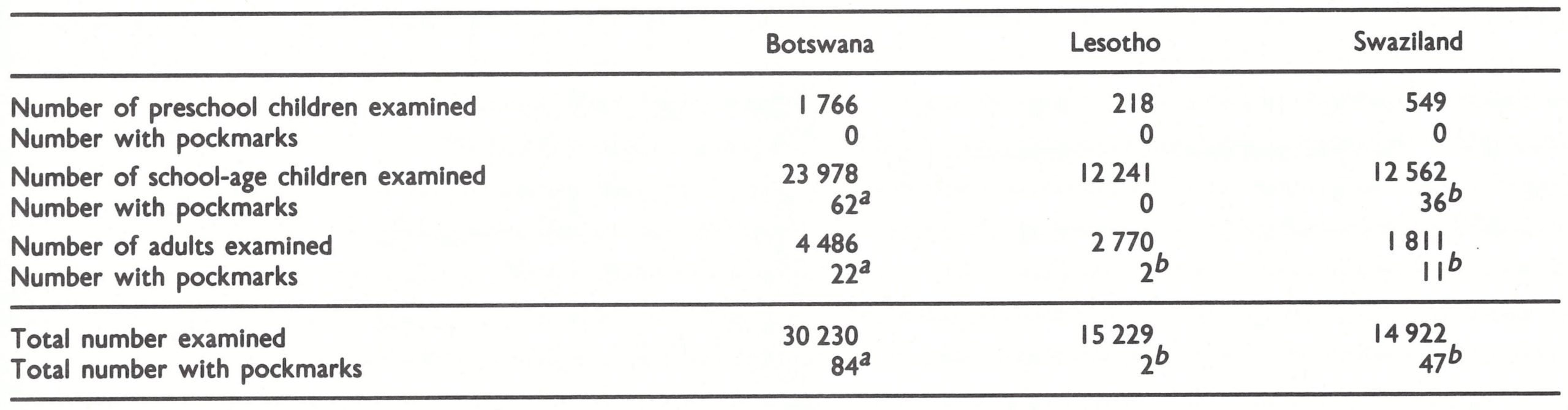
During their visits, Commission members themselves carried out pockmark and vaccination scar surveys, though necessarily on a much smaller scale than in the national surveys (Table 26.6). They discovered a higher proportion of pockmarked schoolchildren and adults than had been found in the national surveys in Botswana and Swaziland, but fewer in Lesotho. In any case, even these higher frequencies were quite low (0.26% and 0.29%, in schoolchildren in Botswana and Swaziland respectively) and no pockmarked children under the age of 6 were found, out of a total of 2533 examined.

Plate 26.2. Participants in the briefing meeting of the International Commission for the Certification of Smallpox Eradication in Botswana, Lesotho, and Swaziland, held in Gaborone, Botswana, 7 March 1979. Left to right, front row: I.H. Chu (WHO), M. Altmann (WHO), G. Meiklejohn (USA), W. Koinange (Kenya), 1. Tagaya (Japan), D. Chilemba (Malawi), P.E.M. Fine (USA); bock row: R.A. llbor (WHO), J.P. Sibiya (Botswana), L.T. Lesetedi (Botswana), V. Chinien (WHO), A. Deria (Somalia), B.C. Dando (WHO), A. Sunde (Botswana), J.G. Breman (WHO). The names of the Commission members are in bold type.
Table 26.6: Botswana, Lesotho and Swaziland: results of facial pockmark surveys carried out by members of the International Commission in March 1979
 a Due to smallpox contracted before 1974.
a Due to smallpox contracted before 1974.
b Due to smallpox contracted before I97 I.
There was some doubt among Commission members in Botswana whether smallpox transmission there had been interrupted in 1973 or had extended into 1974. Two suspected cases of smallpox in children had occurred in 1974, but it was impossible to confirm or disprove the diagnosis.
The vaccination scar survey conducted by Commission members revealed a high vaccination coverage of the population in all 3 countries; in the age group under 15 years, for example, it was 96% in Botswana, 85% in Swaziland and 7204 in Lesotho. In Botswana, refugees, bushmen and a religious sect whose members objected to vaccination on principle were considered as high-risk groups among whom the transmission of smallpox was more likely to continue. However, national vaccination surveys and visits by Commission members showed satisfactory vaccination coverage in each of these groups.
Because the variety of smallpox most recently prevalent in these 3 countries had been variola minor, the absence of pockmarks in children was less significant than in the majority of other countries, but the absence of variola virus in specimens taken from cases diagnosed as chickenpox and the high level of vaccinia1 immunity were persuasive. Noting that there had been no evidence of confirmed smallpox since 1973 or of suspected cases since 1974, the Commission certified that smallpox had been eradicated from Botswana, Lesotho and Swaziland.
South Africa
With a population of 22.8 million in 1970, South Africa was the most populous country in southern Africa. Variola major and variola minor had been endemic up to the Second World War, but thereafter only variola minor had persisted as an endemic disease, and was not regarded very seriously by the health authorities. Apart from a visit to South Africa in 1972 by Henderson (see Chapter 20), the country had had no contact with the WHO smallpox eradication campaign and had not established a national smallpox eradication programme. Smallpox was regarded as one of the diseases for which vaccination should be provided, but was considered to be of minor importance compared with poliomyelitis, measles, diphtheria, and other diseases.
Arrangements for certification
Following the Consultation on the Worldwide Certification of Smallpox Eradication in October 1977, the Director-General of WHO wrote to the South African Minister of Health and Welfare to propose that the South African government should participate in the global certification of smallpox eradication. In his letter he suggested that a visit early in 1978 by Fenner, who had been the chairman of the Consultation, would be a useful way to begin this activity. Within 10 days of the dispatch of this letter, South Africa informed WHO by cable of its willingness to participatein these certification activities and to provide every assistance during Fenner’s visit.
Visit by Fenner, 19 January-19 February 1978. The purpose of the visit was threefold: (1) to advise South African health officials on how to prepare a country report for submission to the Global Commission ; (2) to emphasize the importance of chickenpox surveillance and make arrangements for the collection of specimens for laboratory examination by WHO collaborating centres; and (3) to obtain an impression of the recent history of smallpox and rural health services in South Africa (including some of the “black homelands”). Fenner’s itinerary is shown in Fig. 26.4. With the help of the South African government, the trip was extended to include Namibia (see below). He was cordially received by government and provincial health officials (see box) and visited infectious disease hospitals, university medical schools, diagnostic laboratories in Johannesburg and Cape Town, and rural health centres in northern Transvaal and 3 of the “black homelands”, Bophuthatswana, Lebowa and Transkei.
The laboratory services were found to be of high quality and a network of diagnostic laboratories covered most of the country. However, their practice of testing for orthopoxviruses by growth in tissue culture rather than on the chorioallantoic membrane, and reporting positive results as indicating a “member of the vaccinia-variola group” was confusing (see Chapter 20). Variola virus stocks were held in the National Institute for Virology, but the South African Director General of Health would not agree to a request by Fenner that they should either be transferred to a WHO collaborating centre or destroyed. In fact, it was not until December 1983 that they were finally destroyed (see Chapter 28).
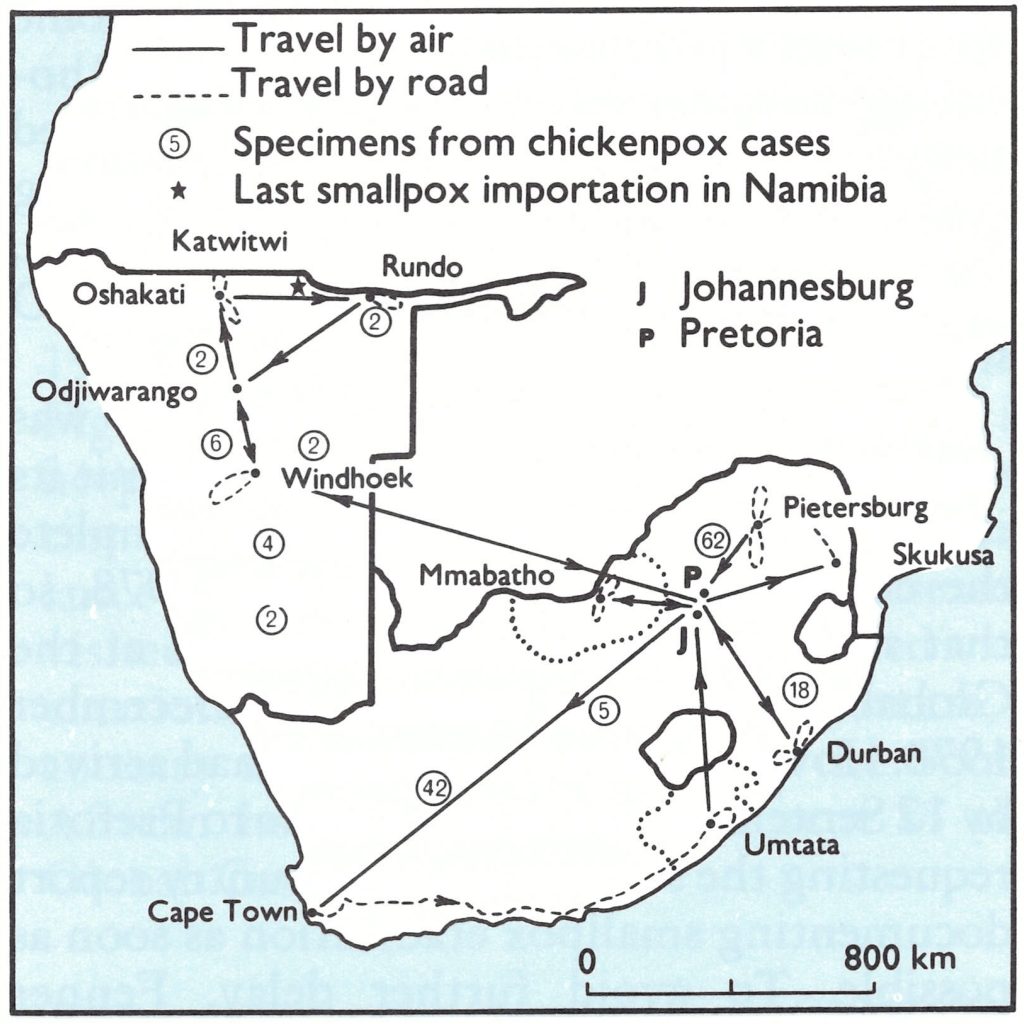
Fig. 26.4. Itinerary of the visit to South Africa and Namibia by the chairman of the Global Commission, Dr F. Fenner, 19 January-19 February 1978, and numbers of specimens from cases of chickenpox from each of the provinces of South Africa and various parts of Namibia.
Collaboration between South Africa and WHO on Smallpox Eradication
The following note prepared by Fenner on his return from South Africa illustrates that country’s willingness to cooperate with WHO’S global certification activities:
“Everywhere I went I was received with great cordiality, and there were frequent expressions of satisfaction that WHO had arranged the visit. No effort was spared to enable me to see what I regarded as the ‘vulnerable’ areas, the more heavily populated parts of Namibia near the Angolan border and the northern parts of Transvaal (Lebowa) and Bophuthatswana, near Botswana.
“I was driven around the countryside and to clinics and hospitals by senior health officials, health inspectors or nursing sisters over a distance of more than 3000 km, and a chartered plane was made available for 3 days. Such travel afforded opportunities for extensive informal discussion of the health conditions and the complex politics of these parts of Africa, as well as observation of the countryside and living conditions in the rural areas, and the rural hospitals and clinics.”
Vaccine was produced in a laboratory in Cape Town for use locally and in some neighbouring countries—e.g., Southern Rhodesia. Tests on freeze-dried vaccine carried out in 1970 by the WHO Collaborating Centre for Smallpox Vaccine in Bilthoven, Netherlands, showed that it met WHO standards.
Preparation of the country report. It was suggested that South Africa should submit its country report by 1 June 1978 and complete the chickenpox survey in October 1978, so that the situation could be reviewed at the Global Commission meeting in December 1978. However, when no material had arrived by 12 September, Arita sent a cable to Pretoria requesting the submission of a country report documenting smallpox eradication as soon as possible. To avoid further delay, Fenner revisited South Africa briefly in mid-October, and Dr Nicole Grasset, formerly the regional smallpox adviser in the WHO South-East Asia Region, who had lived in South Africa in her youth, visited the country in November and brought data and a draft report back to Geneva, where it was finalized by staff of the Smallpox Eradication unit.
The delay in sending the results of the chickenpox surveys was due to the seasonal character of the disease; outbreaks occur in spring and, in the Southern Hemisphere, this starts in September, so that, by October, there had been too few to enable the stipulated 100 specimens to be collected.
Review of country report by the Global Commission, December 1978
The country report and the results of an incomplete chickenpox survey were presented to the Global Commission at its meeting in Geneva from 4 to 7 December 1978. The Commission noted that South Africa had relatively well developed health services, as shown by the overall doctor to population ratio of 1:1806 and registered nurse to population ratio of 1:573. In addition, 5660 health stations were responsible for reporting communicable diseases. After the last known outbreak in 1971, when special efforts were made to achieve high vaccination rates in the northern Transvaal (see Chapter 20), smallpox vaccination was being performed as part of a well-organized immunization programme which also provided poliomyelitis, BCG and diphtheria-pertussis-tetanus vaccination.
The results of facial pockmark and vaccination scar surveys carried out in widely separated rural and urban areas during 1978 are shown in Table 26.7. An additional survey of 17 064 children under 15 in Bophuthatswana and Transkei revealed none with facial pockmarks and 67.6% with vaccination scars. Four adults with facial pockmarks gave histories of attacks of variola major many years earlier.
Table 26.7: South Africa: results of facial pockmark and vaccination scar surveys in 1978, by age group and type of locality
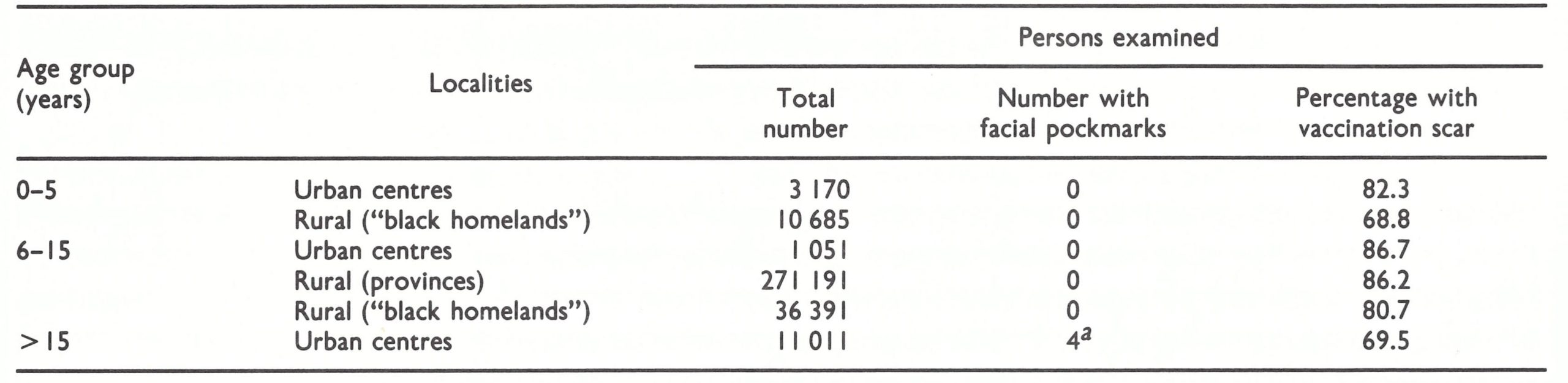 a Due to smallpox contracted many years earlier.
a Due to smallpox contracted many years earlier.
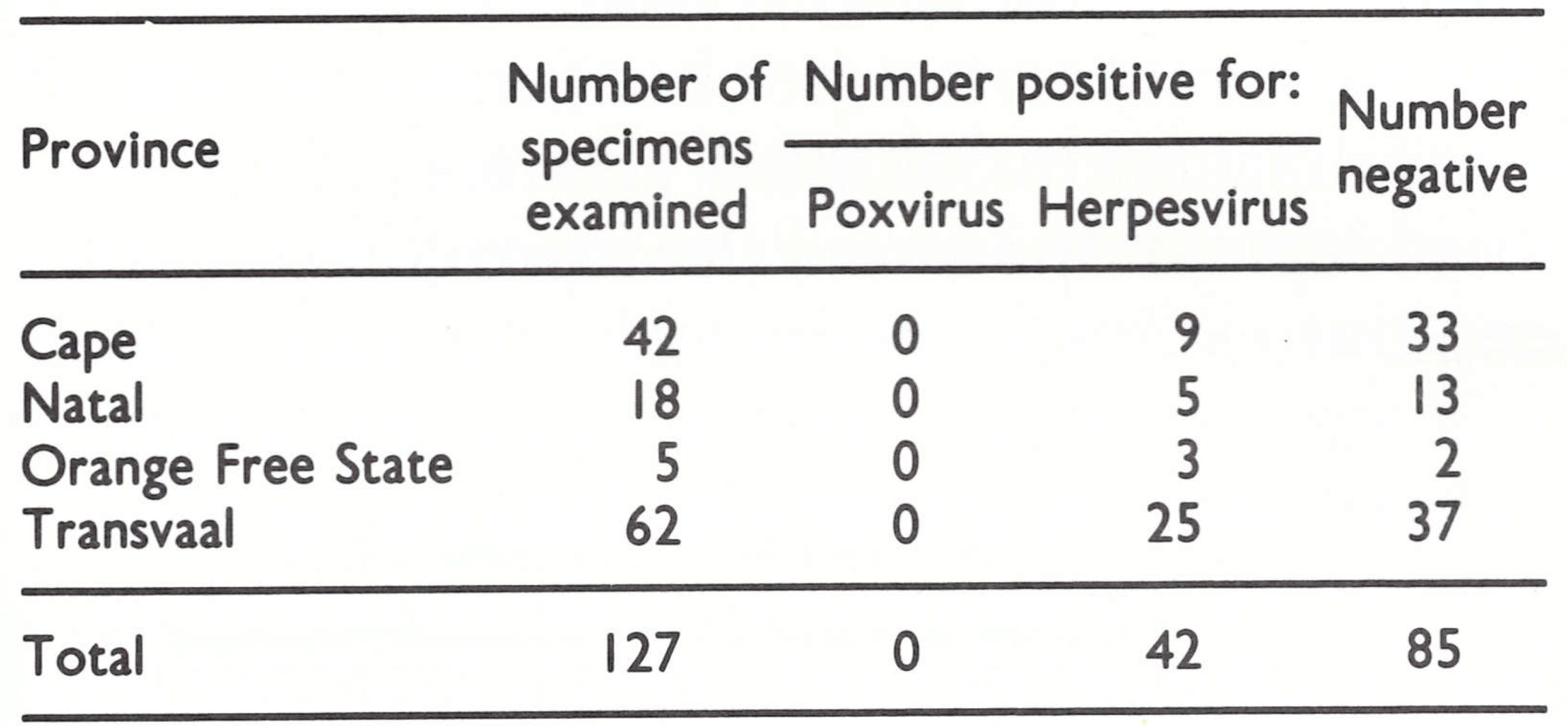
When the Global Commission met in December 1978, no data were available on the laboratory examination of specimens from cases of chickenpox, and it was therefore decided to delay certification pending the arrival of the results of this survey. By June 1979, 127 specimens had been submitted for examination, the majority coming from the northern Transvaal (see Fig. 26.4), where the last outbreak of smallpox had occurred in 1971. All were negative for poxvirus, but herpesvirus particles were seen in 33% of the specimens (Table 26.8).
After receipt of the results of the examination of the first 100 specimens, Arita wrote to members of the Global Commission, who, on the basis of their review of the situation in December 1978 and the results of the chickenpox survey, agreed on 17 April 1979 that smallpox eradication had been achieved in South Africa.
Table 26.8: South Africa: results of examination by WHO collaborating centres of specimens collected from cases clinically diagnosed as chickenpox
Namibia
Although the United Nations had terminated the South African mandate over Namibia in 1966 and the South African presence there had been declared illegal by the International Court of Justice in 1971, the country was in fact controlled and administered by South Africa, under the name “South West Africa”. In this sparsely populated country, the highest population density being 7.5 persons per square kilometre in Ovamboland, adjacent to the border with Angola, endemic smallpox was said never to have been present, though there had been occasional importations from Angola, most recently in 1956. Endemic smallpox had been eliminated from Angola in 1959 (see below) and although cases had occurred as recently as 1973 in Botswana, these were in the eastern part of that country, separated from Namibia by the Kalahari desert. The South African Institute for Medical Research operated a branch laboratory in Windhoek, the capital, and small laboratories in some other towns in Namibia.
Visit by Fenner, 5-9 February 1978
During his trip to South Africa early in 1978, Fenner also spent 5 days in Namibia (see Fig. 26.4). He met health officers and staff in hospitals and laboratories, obtained information on health services, especially the surveillance and control of communicable diseases, visited schools and conducted a limited vaccination scar survey. After his departure, a country report was prepared by the South African health authorities and sent to the Global Commission.
Review Of the country report ly the Global Commission, December 1978
The country report was considered at the meeting of the Global Commission in December 1978. It followed the usual lines, describing the geography and demography, health administration, history of smallpox and records of vaccination activities. Between 1969 and 1978, 10 specimens had been examined for suspected smallpox at the National Institute for Virology in Sandringham; all were negative. Pockmark and vaccination scar surveys had been conducted throughout the country in April-November 1978 (Table 26.9). The 3 pockmarked adults found were Angolans who said that they had suffered from smallpox in childhood.
During 1978 and 1979, 18 specimens collected from cases clinically diagnosed as chickenpox (see Fig. 26.4) were examined in a WHO collaborating centre; none contained poxvirus but 9 showed herpesvirus particles.
On the basis of the history of smallpox in Namibia, the low probability of importations from adjacent countries during the previous decade, the results of the facial pockmark surveys and the high vaccination rate in individuals over 5 years of age, the Global Commission certified that smallpox had been eliminated from Namibia.
Table 26.9: Namibia: results of facial pockmark and vaccination scar surveys in April-November 1978, by age group
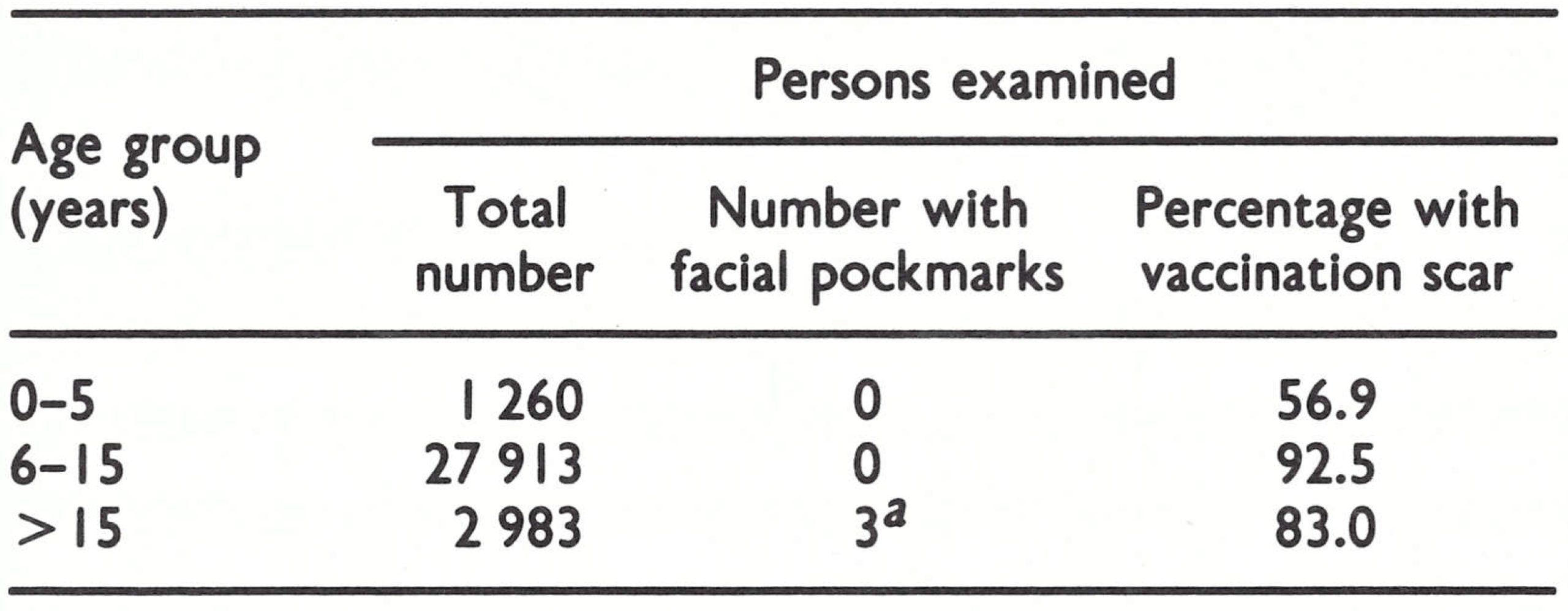 a Angolans who had had smallpox in childhood.
a Angolans who had had smallpox in childhood.
Southern Rhodesia (Zimbabwe)
Southern Rhodesia was a British colony until 1980, when it attained independence and was renamed Zimbabwe. In 1965 the white colonists had made a unilateral declaration of independence and since then the country had been in a state of civil war. Legally, in 1978, it remained under the jurisdiction of the United Nations Sanctions Committee. In order to obtain information on the smallpox situation, the Director-General of WHO wrote to the Southern Rhodesian authorities requesting that 2 WHO consultants should be allowed to visit the country to assess whether smallpox had been eliminated. A favourable reply having been received, Dr Nicole Grasset and Dr Gordon Meiklejohn, both highly experienced in smallpox eradication activities, visited the country in January 1978.
Visit Ly Dr Grasset and Dr Mezklqohn, 10-30 Januay 1978
Since Southern Rhodesia was a much smaller country, the objectives of this visit differed from those of Fenner’s visit, mentioned above, to South Africa and Namibia. The consultants’ aim was to obtain enough information, by travel and inquiry, and supported by subsequent investigations by local personnel, to be able to submit to the Global Commission a definitive report on the smallpox situation in Southern Rhodesia.
The consultants were warmly received by the local authorities (see box) and after initial consultations in Salisbury (Harare), theytravelled separately around the 5 provinces, carrying out extensive pockmark and vaccination scar surveys as well as evaluating the level of surveillance of infectious diseases by health personnel. Subsequently, national health personnel carried out further and more extensive studies. The consolidated results of all these surveys are shown in Table 26.10.
In their inquiries, the consultants observed that there was a remarkable lack of knowledge about smallpox among persons under 25 years of age. Almost without exception they failed to recognize the smallpox pictures on the recognition cards and stated that they had never seen or known of the presence of the disease. On the other hand, many older persons knew about smallpox from their childhood, and 0.26% of adults surveyed had facial pockmarks, the most recent being said to date from an illness in 1966.
In addition to their field survey, the consultants commented on the health services, which they described as extensive, well planned and supported by excellent communications. There was a medical school in Salisbury; the health personnel included many European nurses and physicians, a large proportion of whom had undergone training in public health and tropical medicine; and an extensive network of 83 mission hospitals existed. Because of the civil war, health staff were working under extremely difficult circumstances, often at the risk of personal injury or death. Although smallpox was at the top of the list of notifiable diseases, the country had never set up a separate smallpox eradication programme. Mobile vaccination teams sought to vaccinate the entire population against smallpox in a 3-year cycle, using liquid smallpox vaccine purchased from South Africa. There were no systematic search operations and, apart from reporting during an outbreak, no routine “nil” reports. Reliance was placed on the extensive and well distributed network of health units and on the alertness of staff in high-risk areas. This approach appeared to have been reasonably successful in detecting almost all outbreaks, and transmission was interrupted in 1970. The instability in some border areas raised doubts as to the ability of this health structure to detect outbreaks rapidly in those areas if there should be an importation, but the neighbouring countries—Botswana, Mozambique, South Africa and Zambia—had been free of smallpox since 1973 or earlier.
Table 26.10: Southern Rhodesia: results of facial pockmark and vaccination scar surveys in January-April 1978, by age group
 a Due to smallpox contracted before 1967.
a Due to smallpox contracted before 1967.
The consultants found no evidence of smallpox transmission within Southern Rhodesia or of importations since the last reported outbreak there in 1970. It was their opinion that, because the health units were numerous, geographically well distributed and staffed with well-trained and alert personnel, any case of smallpox that might have occurred after 1970 would have been detected. Facilities for laboratory diagnosis, including electron microscopy, were available in Salisbury and many specimens had been tested between 1970 and 1977, all with negative results. After the consultants’ visit, a further 23 specimens obtained from patients with what was diagnosed clinically as chickenpox were examined in a WHO collaborating centre. Herpesvirus particles were found in 10 of them but poxvirus in none.
Review by the Global Commission, December 1978
At its meeting in December 1978 the Global Commission reviewed the consultants’ report and the results of the pockmark and vaccination scar survey supplied by the government, and certified that Southern Rhodesia was free of smallpox.
Angola
The only countries remaining for assessment in southern Africa were Angola and the island of Madagascar. At the coordination meeting held in Lusaka in March 1978, it had been decided that the certification of Angola should be carried out by an international commission in February 1979.
The last reported cases of smallpox in Angola had occurred in 1966. Although the country had suffered from political instability since 1961, there had been a good vaccination programme, in which freeze-dried vaccine had been used, until 1975. Variola minor was endemic up to 1959, and outbreaks of variola major had occurred following importations from Zaire during the 196Os, the last taking place in 1966. Each of these was investigated by state epidemiologists and confirmed by virus isolation at a laboratory in Luanda. The extensive national vaccination campaign extended through 1974 but was then sharply curtailed because of the civil war, which culminated in national independence in 1975. By then, more than 3 years had elapsed since the last outbreak in Zaire, which had been the source of earlier importations. However, in 1978 many areas were regarded as inaccessible and it was thought that it would be difficult to carry out pockmark surveys and obtain specimens from cases of chickenpox in those parts of the country.
Precertification activities
Dr Joel Breman of the Smallpox Eradication unit helped to plan the precertification programme and Dr Renir F. M. Collas, a WHO epidemiologist, and Mr Josk F. Verani, a WHO technical officer, who were stationed in Angola in connection with other WHO projects, assisted the national health officials. In August 1978 Dr Clovis H. Tigre, a Brazilian epidemiologist, visited Angola to review the progress of field surveys and the preparation of the country report. He found that little had been done.
In November 1978, at Arita’s request, Dr Francisco J. C. Cambournac, a former resident of Angola who had been Director of the WHO Regional Office for Africa but had retired to Portugal, provided valuable data on smallpox in Angola before 1975, the year of independence. The country report was finally prepared later that month, by which time 79 specimens had been collected from chickenpox patients. However, the field survey had been delayed because of poor communications and lack of resources, and it was doubtful whether all the data would be available for the visit of the International Commission scheduled for February 1979. Early in December, after a meeting at the Ministry of Health between government officials and the WHO programme coordinator in the country, the survey proceeded more rapidly and by early January 1979 all preparations had been completed.
Pockmark survey. The pockmark survey carried out by the national health authorities covered all the provinces (Fig. 26.5) and 11 yo of the total population. About 0.8% of the adult population and 0.04% of school-age children had facial pockmarks, but only 1 pockmarked child was found in the preschool age group (Table 26.11), and it was decided that the scarring had been caused by chickenpox.
Chickenpox surveillance. Variola minor had virtually replaced variola major in Angola in the 1950s and had been present together with variola major in neighbouring countries (Zaire and Zambia) until the late 1960s. A total of 122 specimens collected from outbreaks of chickenpox occurring in various provinces (Fig. 26.6) were examined in a WHO collaborating centre; none contained poxvirus but 12 were found to contain herpesvirus particles. This unusually small proportion of herpesvirus-positive specimens was due to a breakdown of the electron microscope during the period concerned, so that much of the material had only been cultured.
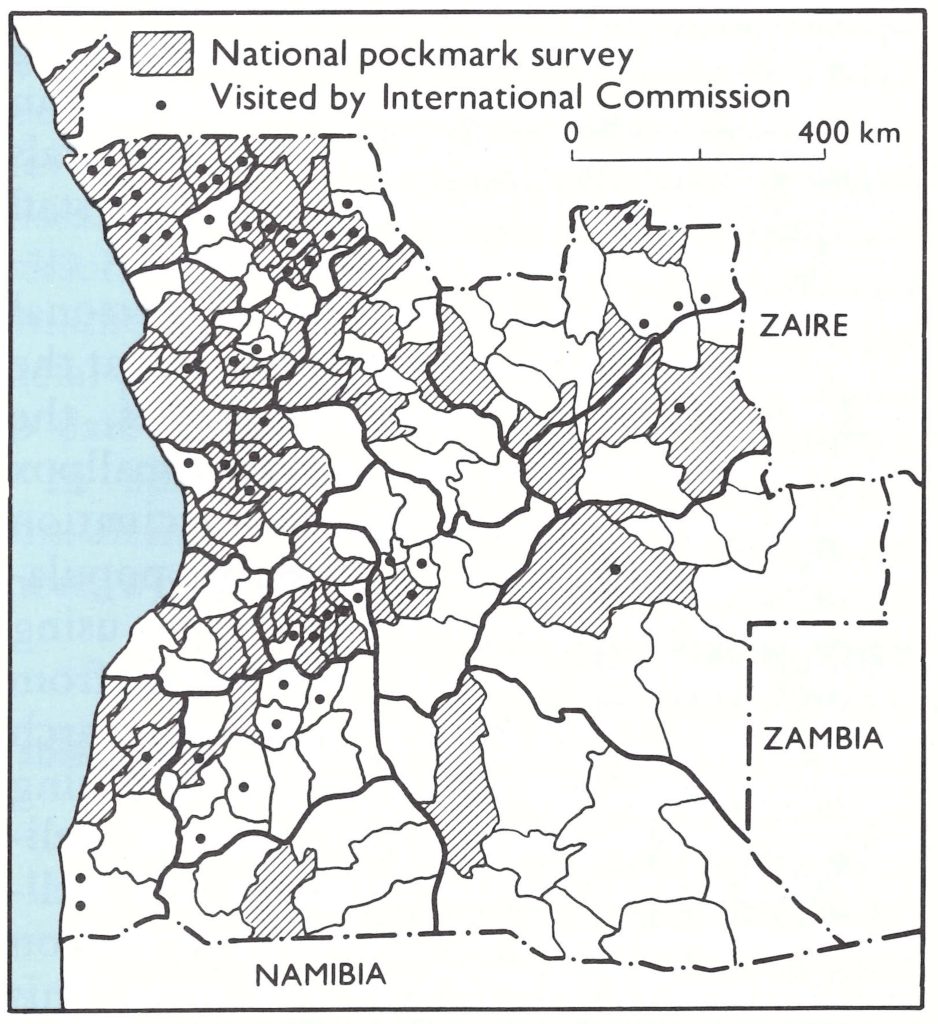
Fig. 26.5. Certification activities in Angola: municipalities covered by the national pockmark survey, July-December 1978, and those visited by members of the International Commission for the Certification of Smallpox Eradication in Angola, 5-16 February 1979.
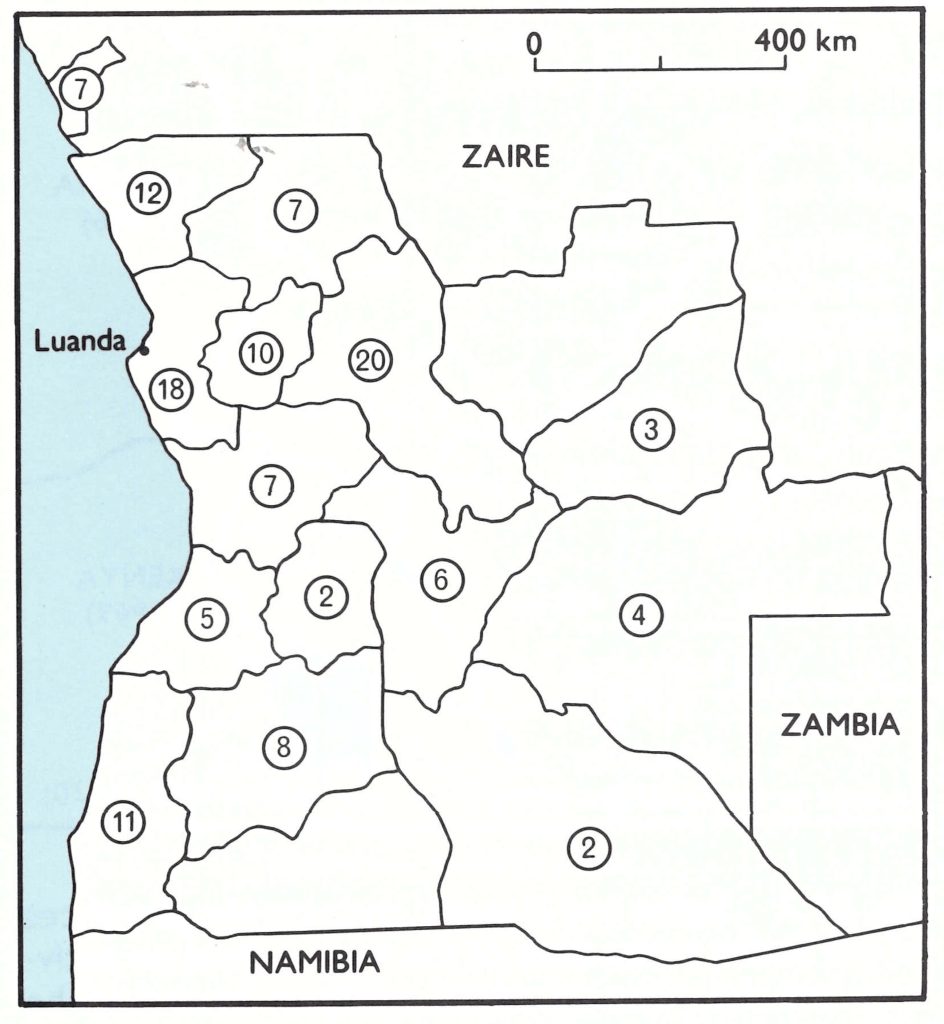
Fig. 26.6. Numbers of specimens collected from chickenpox cases in various provinces of Angola between July 1978 and February 1979.
Table 26.11: Angola: results of facial pockmark survey in July-December 1978, by age group
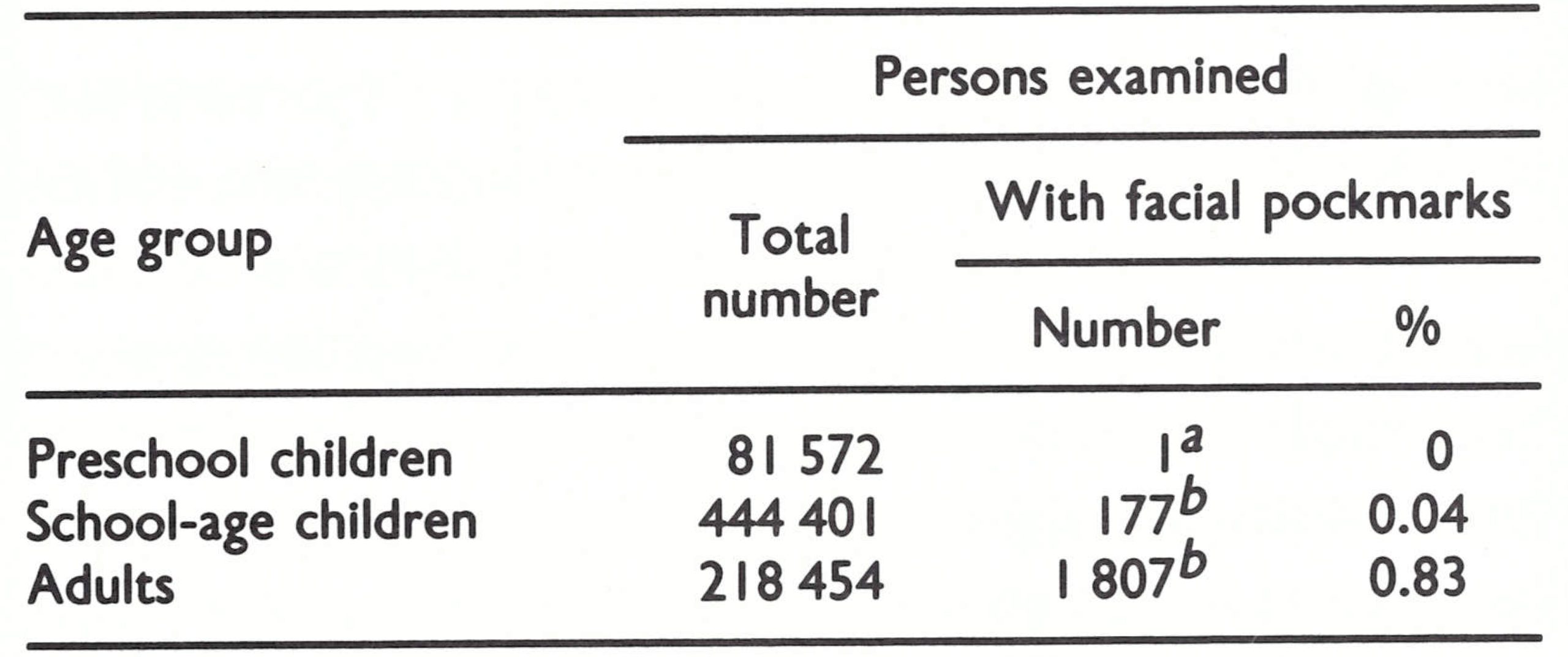 a One child had facial scarring which resembled pockmarks caused by smallpox, but after further examination it was decided the scarring had been caused by chickenpox.
a One child had facial scarring which resembled pockmarks caused by smallpox, but after further examination it was decided the scarring had been caused by chickenpox.
b Due to smallpox contracted before 1974.
Visit of the International Commission, 5-16 February 1979
After reviewing the data supplied by the Angolan authorities in Luanda, the Commission formed 5 teams, which travelled widely throughout the country (see Fig. 26.5) before meeting again in Luanda on 15 and 16 February to review the situation. Contrary to the opinion prevailing earlier, members were able to visit most parts of Angola, except the south-east, which bordered on Namibia, a country that had been free of smallpox for decades. During their visits they conducted a facial pockmark survey that covered 28 167 persons, of whom 495 had pockmarks; these were all persons of school age or older and all had contracted the illness causing the pockmarks prior to 1966.
Between 1966 and 1974 there had been a good vaccination programme, 1.5-2.8 million people out of a population (in 1974) of about 6.3 million having been vaccinated annually with freeze-dried vaccine of good quality purchased from a number of European countries. There were 144 reporting units in the 16 provinces and, on average, one-third of them were sending in monthly epidemiological reports. Taking into consideration the absence of smallpox from Angola since 1966 and from neighbouring countries since the late 196Os, the field investigations carried out by the Angolan authorities, and the results of the chickenpox survey, the International Commission certified Angola to be free of smallpox.
Madagascar
Because Madagascar was an island with a relatively small population, it had been possible to interrupt smallpox transmission there during the First World War, and to control effectively the few importations that occurred between 1925 and 1931 (see Chapter 8). The Consultation on the Worldwide Certification of Smallpox Eradication, meeting in October 1977, decided that all that was needed from Madagascar was a country report, which was presented by the government to WHO in December 1977.
An unusual feature of this report was the large number of recorded deaths from chickenpox (Table 26.12). The data for 1972-1975 were supplied in the country report, the other figures by correspondence. These data could have been interpreted as the result of an unrecognized importation of variola major into Madagascar in 1974 and its subsequent spread and misdiagnosis as chickenpox during 1975 and 1976. The likelihood that this was so was increased when the data by province for 1976 showed that the casefatality rate for “chickenpox” in the province of Antananarivo was almost 1% (8572 cases; 83 deaths). Correspondence between the Smallpox Eradication unit and health officials and the WHO programme coordinator in Madagascar failed to elicit a satisfactory explanation for the reported high death rates from chickenpox, and in December 1978 the Global Commission deferred certification pending the provision of further information.
It was arranged that Dr Ziaul Islam should visit Madagascar and investigate the situation. Working there from 26 February to 9 March 1979, he checked the original records for 1972-1978 and discovered that measles deaths had sometimes been attributed to chickenpox, typing errors had been made, and confusion had resulted from using reporting forms for mortality when those intended for reporting morbidity had run out; sometimes no explanation for the figure reported could be found. His final assessment of the numbers of deaths from chickenpox, also shown in Table 26.12, is consistent with the occurrence of chickenpox only.
Dr Islam’s report, which also provided some additional information on the health structure and vaccination programme in Madagascar, was distributed to members of the Global Commission on 10 May 1979. They accepted the explanation that the high mortality attributed to chickenpox was due to reporting and/or recording errors and eradication in Madagascar was certified by correspondence on 29 June 1979. Had the Global Commission not made such a decision, arrangements between the Smallpox Eradication unit and the government of Madagascar were in hand to carry out an intensive pockmark survey in the areas in which large numbers of chickenpox deaths had been originally reported, but this did not prove necessary.
Table 26.12: Madagascar: number of reported cases of and deaths from chickenpox, 1972-1978
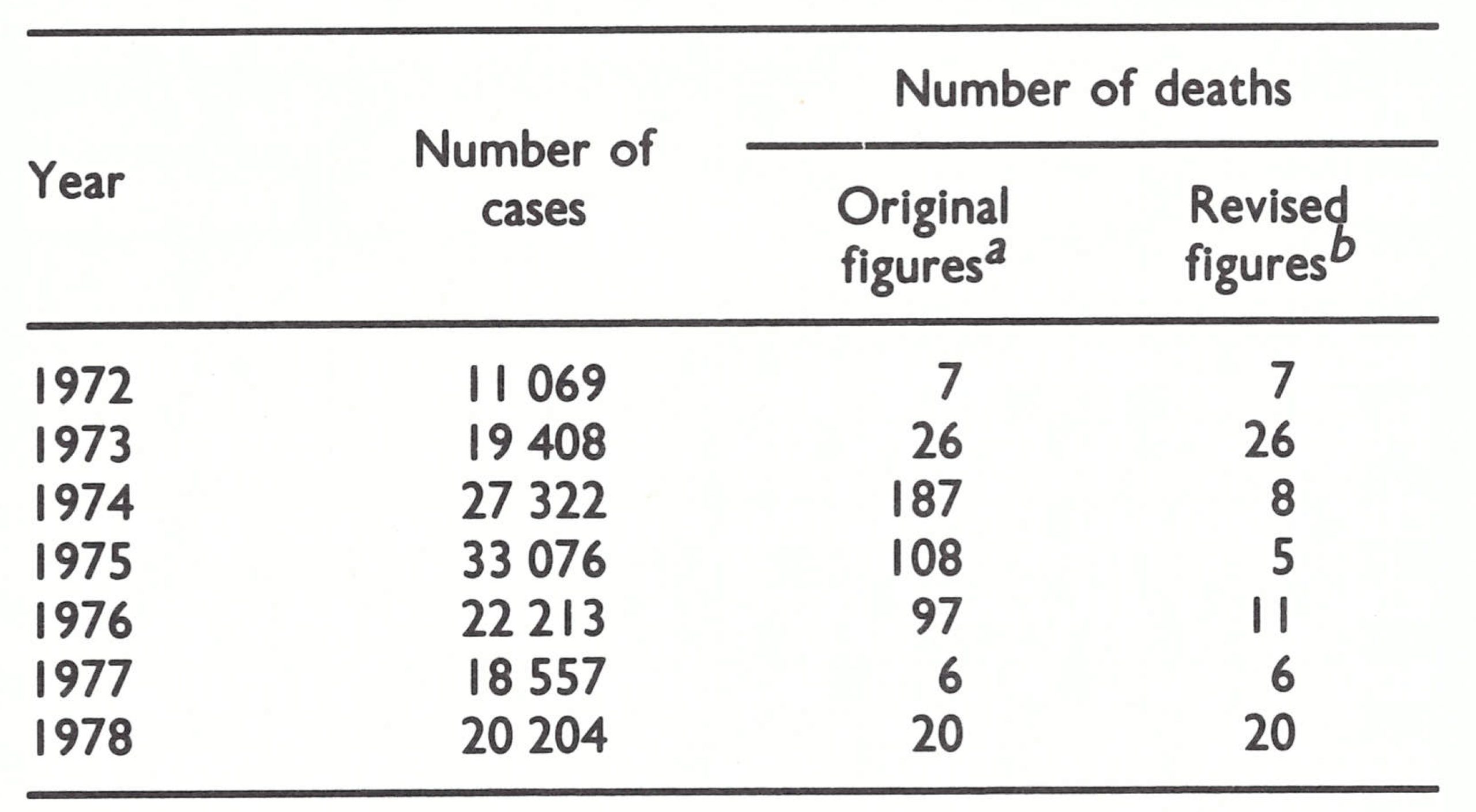 a From the Ministry of Health of Madagascar.
a From the Ministry of Health of Madagascar.
b After Investigations by Dr 2. Islam In March 1979.
UGANDA AND THE SUDAN
In parallel with the certification activities in the countries of southern Africa, arrangements were made for international commissions to visit the 2 African countries (other than those of the Horn of Africa) for which certification was still required—namely, Uganda and the Sudan. Uganda had reported its last endemic case of smallpox in 1968, but imported cases had occurred each year between 1969 and 1972, originating from the neighbouring Equatoria Province of the southern Sudan (Fig. 26.7), in which there had been civil disturbances until 1972. The certification of eradication in Uganda was therefore dependent on that in the Sudan. However, certification could not be undertaken in the Sudan until 1978 because of the risk of importations from Ethiopia, in which smallpox remained endemic until August 1976. Plans were therefore made for the certification of the Sudan and Uganda in October-November 1978, by separate international commissions.
Fig. 26.7. Sudan and Uganda, showing the provinces of the Sudan at the time of the precertification activities and the years in which smallpox ceased to be endemic in neighbouring countries. Uganda was visited by an international commission from II to 27 October 1978 and the Sudan by another international commission from IS to 29 November 1978.
Uganda
Precertification activities
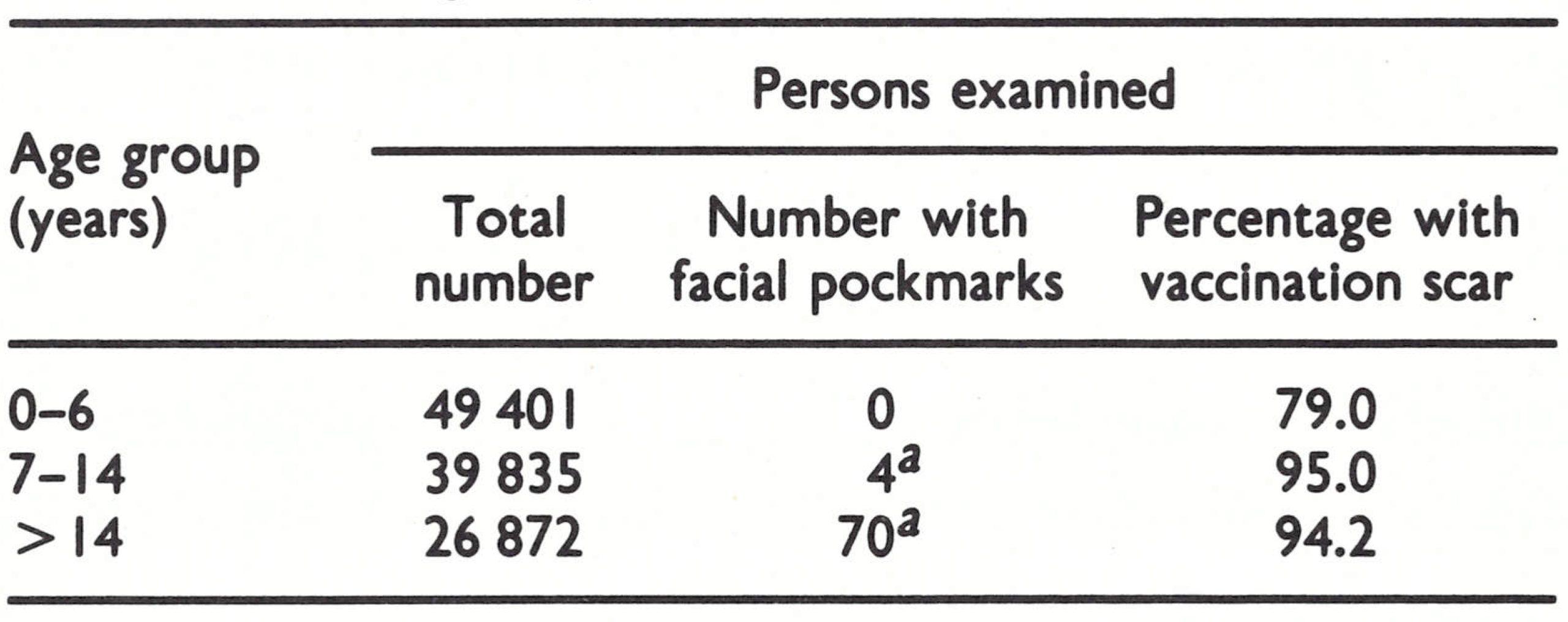
Preparations for certification in Uganda followed the pattern that had been developed in western Africa, where a similar long interval had occurred between the last reported case and certification (see Chapter 25). Dr Chu In Ho, a WHO epidemiologist stationed in Kampala, assisted the Ugandan health authorities in the preparation of the country report and in conducting pockmark surveys and chickenpox surveillance. For the pockmark survey (Table 26.13), 622 localities widely dispersed over Uganda’s 10 provinces were selected and over 1.5 million persons, representing 12.2% of the total population of Uganda, were examined. Most of the more recent outbreaks of smallpox in Uganda had been due to variola minor (see Chapters 8 and 19), so it was not surprising that facial pockmarks were rare, being found in only 0.005% of persons of school age or older. None was ascribed to smallpox infection contracted after 1970.
A WHO-supported virus laboratory in Entebbe had confirmed diagnoses of smallpox in 1970 and 1972, but thereafter had gradually ceased to function. In preparation for certification, 118 specimens were collected from cases of chickenpox occurring in all provinces during the period April-September 1978. On examination at WHO collaborating centres, none was found to contain poxvirus particles.
Plate 26.3. The President of Uganda took a personal interest in the certification of smallpox eradication in his country. The eradication programme transcended personal and political barriers in a global effort towards a common goal.
Visit of the International Commission, 11-27 October 1978
After an initial 3-day meeting in Kampala, the Commission was divided into 3 teams, which between them visited all the provinces. As well as inspecting health units and the reporting system, they carried out facial pockmark surveys (see Table 26.13) which confirmed the results of the larger national survey.
Before certifying that smallpox transmission had been interrupted in Uganda, members of the Commission made a special visit to the Virus Research Institute in Entebbe and confirmed that all stocks of variola virus previously held there had been destroyed on 27 July 1976, after receipt of the letter dispatched from the Smallpox Eradication unit earlier that month (see Chapter 30).
Table 26.13: Uganda: results of facial pockmark surveys by national authorities, April-September 1978, and by International Commission members, October 1978, by age group
 a Due to smallpox contracted before 1971.
a Due to smallpox contracted before 1971.
Sudan
A WHO-assisted smallpox eradication programme had been carried out in the Sudan, geographically the largest country in Africa, from 1969 onwards but was not very effective until 1972 (see Chapter 18). The last endemic case of smallpox had occurred in Bahr El Ghazal Province in December 1972. The requisite 2-year surveillance period after the last known case had been completed by the end of 1974, but the eradication of smallpox was not certified in the Sudan by an international commission until November 1978.
Certification was delayed because the Sudan was at the crossroads of movements by seasonal agricultural workers and pilgrims, some of whom came from western Africa on their way to Mecca, and some from Ethiopia, in which smallpox had been endemic until 1976 (see Chapter 18, Fig. 18.6). The movement of refugees from Ethiopia into the southern Sudan also caused problems. The certification of smallpox eradication in the Sudan could be undertaken with confidence only after transmission had been interrupted in Ethiopia.
The delay in certification caused considerable problems for the Sudanese health authorities, since they had to maintain surveillance for a further 5 years after the last case. However, the fact that they had done so meant that smallpox eradication in the central and eastern parts of the African continent could be certified with much greater confidence. In addition to Ethiopia, the Sudan had borders with the Central African Republic, Chad, Kenya, Uganda and Zaire, from which cases had regularly been imported in the 1950s and 1960s. The absence of importations from these countries into the Sudan between 1972 and 1978 provided additional assurance that transmission had ceased in these countries as well.
Precertification activities
After the last case occurred in December 1972, surveillance continued in the Sudan, more than 600 staff being employed for the purpose, including 48 supervisors, 18 assessors and 369 vaccinators, who were distributed throughout the 13 provinces. During this period 1 or 2 WHO epidemiologists or consultants assisted in developing and implementing surveillance. The smallpox eradication staff who contributed in this way included Dr Abdel Hamid el Sayed, as the national director of the programme, and the WHO epidemiologists Mr David Bassett, Dr Donald P. Francis and Dr Satnam Singh.
While the reporting system was being strengthened, programme staff conducted a systematic search for hidden foci of smallpox, particularly in the southern provinces and the areas bordering on Ethiopia. Active searches were conducted in villages, health establishments, schools, police stations and markets to seek information on cases of diseases with a rash, and a reward was offered. The vaccination programme was also maintained.
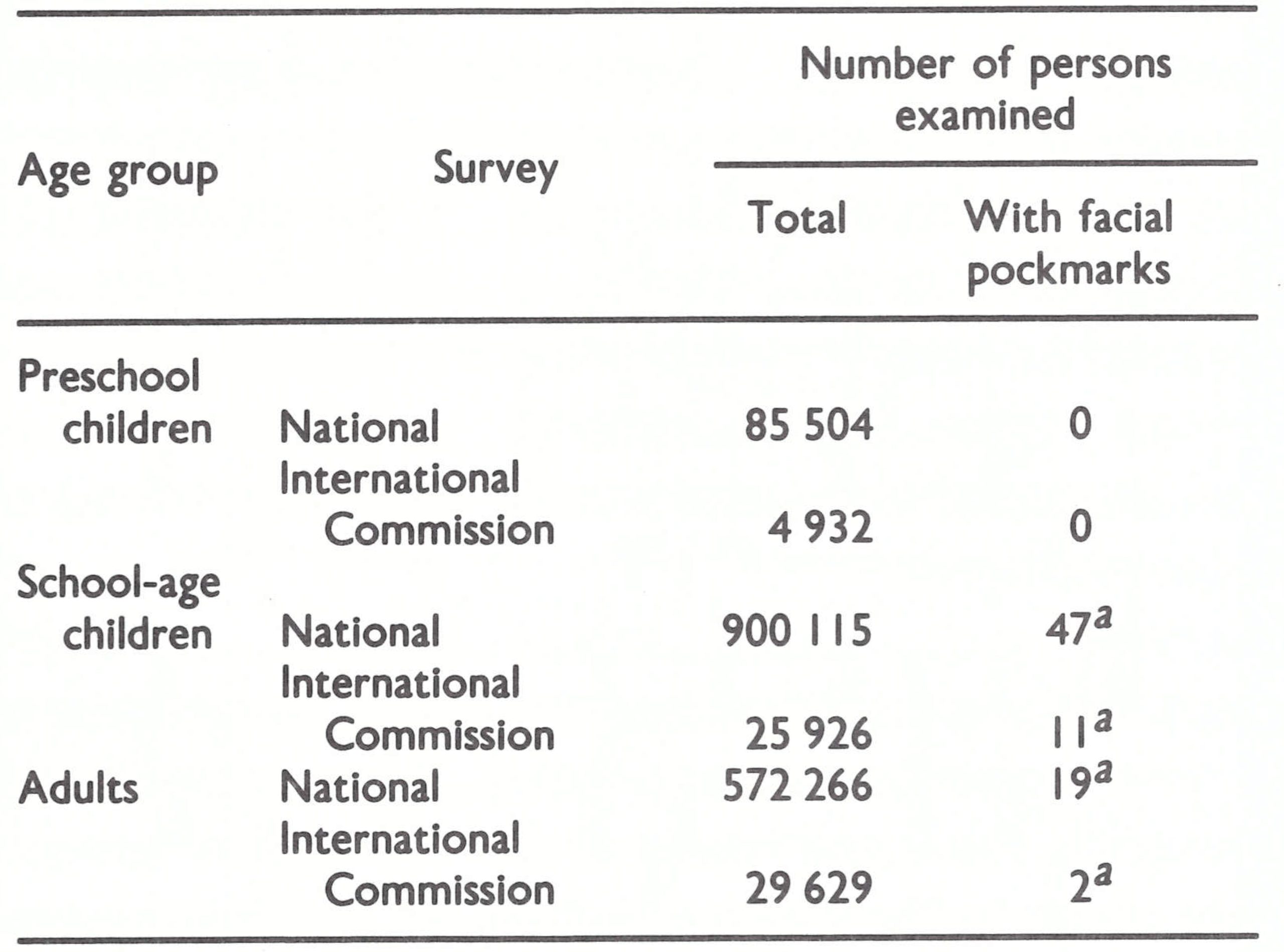
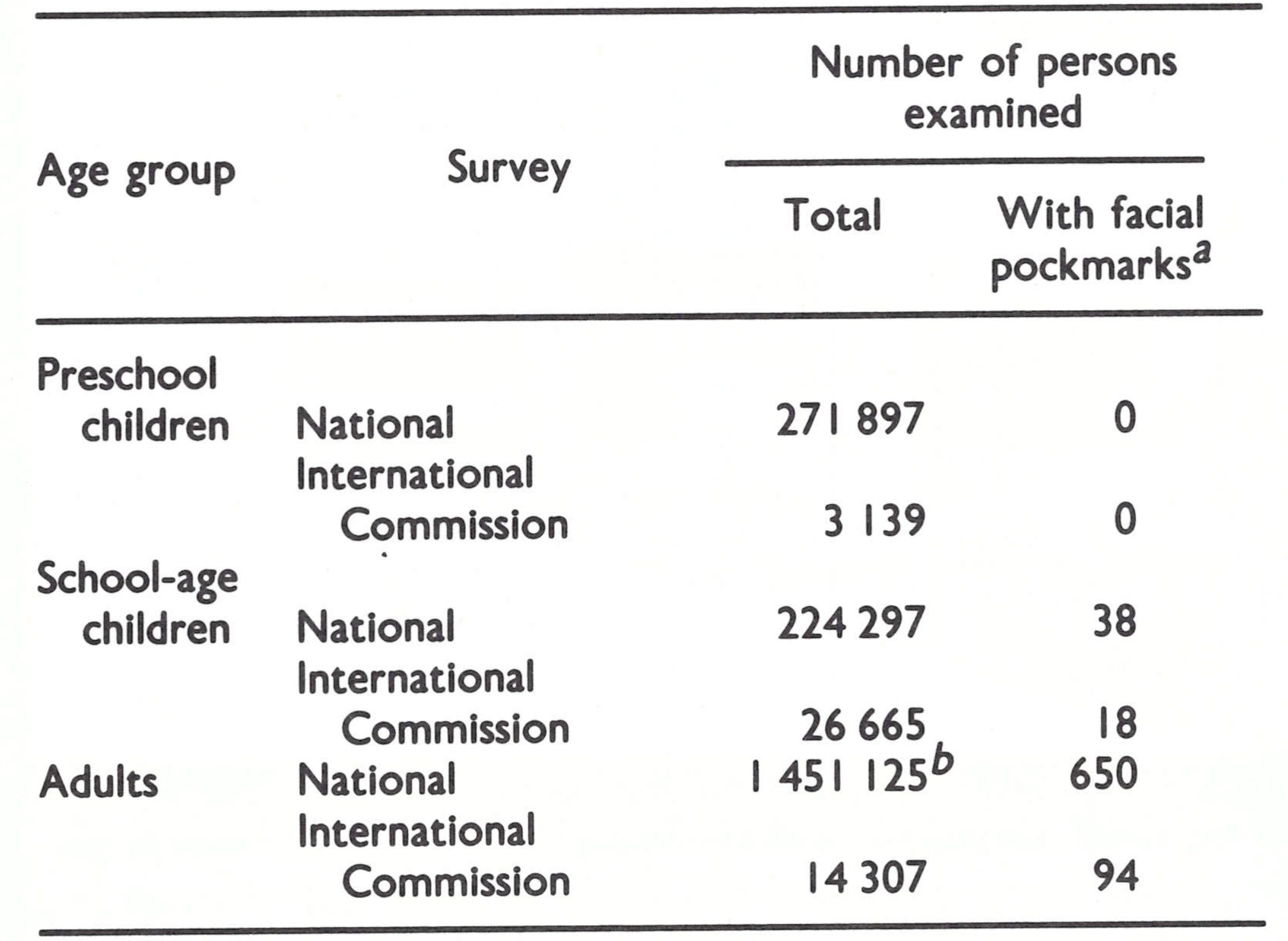
Pockmark survey. Between 1975 and 1977 smallpox eradication programme staff examined a total of nearly 2 million persons, out of a total population of 14 million, for facial pockmarks (Table 26.14). The few people found with them (0.04% of those examined, all of school age or older) had contracted smallpox before 1972.
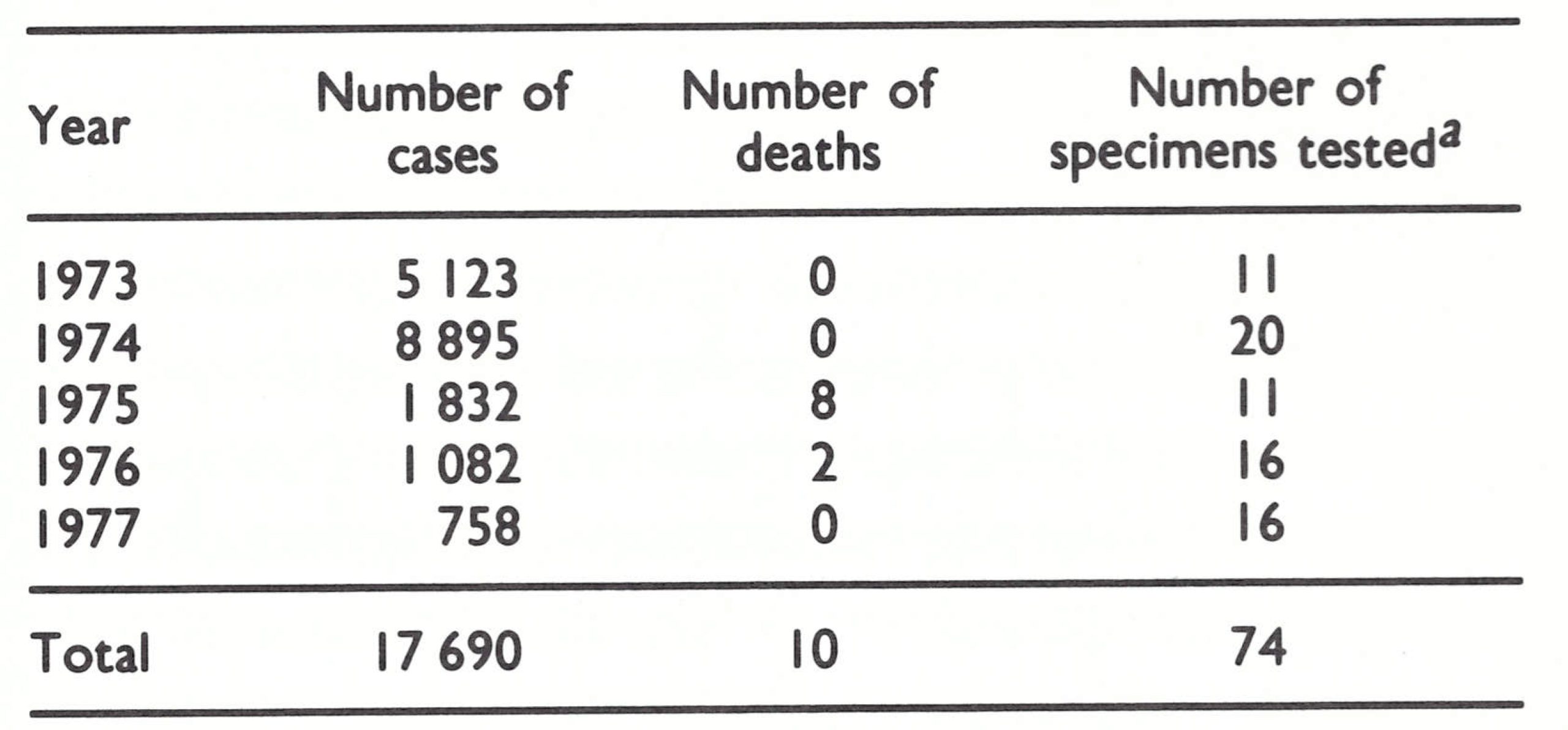
Chickenpox surveillance. Because of possible diagnostic confusion between variola minor and chickenpox, the latter was made a notifiable disease and, wherever possible, outbreaks were investigated by smallpox eradication programme staff. Between 1973 and 1977, 17 690 cases, including 10 deaths, were reported (Table 26.15). Each year, specimens for laboratory investigation were taken from a number of cases, usually those with unusual features. Of 74 specimens examined in WHO collaborating centres none contained poxvirus.
Special searches in the southern provinces. Because of the difficulties of access before 1972, special searches were conducted in Upper Nile and Equatoria Provinces. During two searches in Upper Nile, in 1972 and 1974, 718 000 out of 798 000 inhabitants of the province were vaccinated. A vaccination scar survey revealed a coverage of 85 o/o in the age group 0-4 years and 98% in the age group 5-14 years.
Table 26.14: Sudan: results of facial pockmark surveys conducted by smallpox eradication programme staff between 1975 and 1977, and by members of the International Commission in November 1978, in all provinces, by age group
 a Due to smallpox contracted before 1972.
a Due to smallpox contracted before 1972.
b Examined at check-points, mostly adults.
Table 26.15: Sudan: number of reported cases of and deaths from chickenpox between 1973 and 1977 and number of specimens tested
 a None contained poxvirus.
a None contained poxvirus.
Plate 26.4. The collection and testing of material from skin lesions in cases of fever with rash, especially in countries where variola minor had recently been endemic, provided assurance that the surveillance system would have detected smallpox if it had occurred.
In Equatoria Province, the special surveillance team operating in January 1974 discovered evidence of possible smallpox transmission as late as November 1973. The last confirmed case in the province had occurred in November 1972, in the most densely populated part of Kapoeta District, some 80-100 kilometres from the Lafit mountains, where evidence of possible continued transmission was discovered. Intensive investigations suggested that there had been a number of cases, the last in a 15-month-old boy with facial pockmarks. However, it was impossible to determine precisely the date of onset of the disease. The surveillance team revisited the Lafit mountains 3 times in 1974, and repeatedly thereafter, but failed to find any further evidence of smallpox. During a visit to the area in 1976 evidence was obtained suggesting that the supposed last case in the focus had been infected late in 1972, not late in 1973.
Special surveillance in areas on the Ethiopian border. In September 1973, an interregional WHO smallpox eradication programme seminar was held in Addis Abeda. Border surveillance was discussed, and the Ethiopian and Sudanese governments made arrangements after the seminar for surveillance teams from each country to investigate rumours of smallpox on the other side of the border (see Chapter 21). For example, at the request of Ethiopia in November 1973 and February 1974, a Sudanese team investigated smallpox rumours and vaccinated the inhabitants in the Gabba and Metabel areas of Gojam Province in Ethiopia, which were not easily accessible from the Ethiopian side of the border.
Visit by a WHO consultant. In AugustSeptember 1977, Dr Gordon Meiklejohn, a WHO consultant, visited Khartoum and assisted in documenting the work of the smallpox eradication programme and subsequent surveillance activities. In May 1978, a further stimulus was given to the discovery of cases of smallpox by the announcement by the World Health Assembly that a reward of US$lOOO would be offered to any person who reported a smallpox case which was confirmed by laboratory investigations in a WHO collaborating centre.
Visit of the International Commission, 15-29 November 1978
After a brief meeting in Khartoum, field visits were made by 9 separate teams over a period of 12 days. Because of the large size of the Sudan, an aeroplane was made available by the United Nations Development Programme to help to cover critical areas in the northern and eastern provinces (Fig. 26.8). During their visits, Commission members carried out facial pockmark (see Table 26.14) and vaccination scar surveys.
The International Commission found nothing to cause them to doubt the claim that smallpox transmission had been interrupted in the Sudan at least 5 years earlier, and certified the country to be free of smallpox.
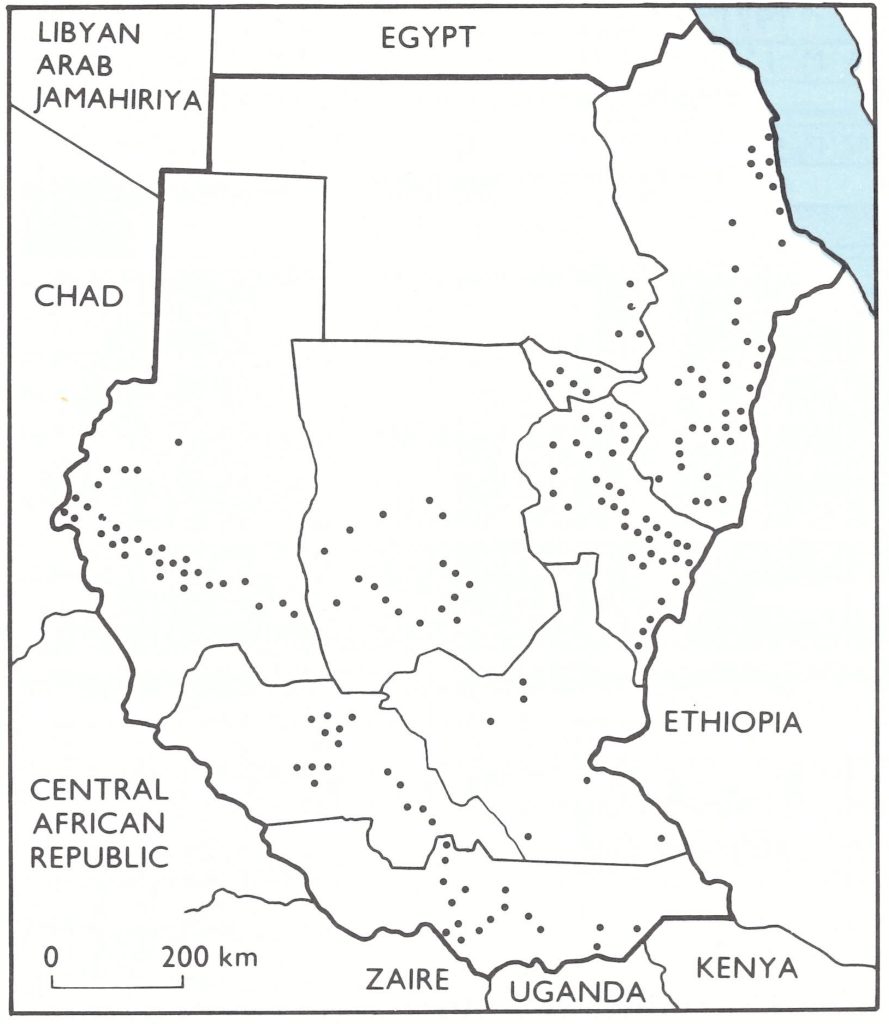
Fig. 26.8. Localities in the Sudan visited by members of the International Commission for the Certification of Smallpox Eradication, 15-29 November 1978.

Plate 26.5. Some of the participants at the meeting of the International Commission for the Certification of Smallpox Eradication in the Sudan, 29 November 1978. Left to right: R.A. Khan (WHO), C. Lerche (Norway), W. Koinange (Kenya), Yemane Tekeste (Ethiopia), A.H. El Sayed (Sudan), J.G. Breman (WHO). The names of the Commission members are in bold type.
SOUTH-WESTERN ASIA
Several countries in south-western Asia required certification by international commissions or other special measures (Fig. 26.9). They fell into 3 groups. Yemen and Democratic Yemen were geographically close to the last remaining endemic countries in the world, Ethiopia and Somalia, and certification activities were delayed there until nearer the time when the Horn of Africa would itself be visited by international commissions. Because of political differences between the two countries, they were visited by separate international commissions in June 1979.
To the north-east lay Saudi Arabia and the Gulf states of Bahrain, Kuwait, Oman, Qatar and the United Arab Emirates. Because of the intensity of the traffic between these countries and the Indian subcontinent and the vast annual pilgrimages to Mecca, the Consultation on the Worldwide Certification of Smallpox Eradication had recommended in October 1977 that WHO should obtain special country reports from each of them for review by the Global Commission in December 1978.
Iran, Iraq and the Syrian Arab Republic were not included in the Intensified Smallpox Eradication Programme in 1967 because they had eliminated endemic smallpox in 1963, 1959 and 1950, respectively. However, it was known that a major epidemic of variola major had spread through these countries in 1970- 1972, after an importation from Afghanistan (see Chapter 23). Few of the many cases which occurred had been reported to WHO-29 from Iran in 1971 and 2 in 1972,37 from Iraq, all in 1972, and 54 from the Syrian Arab Republic in 1972 (Fig. 26.10). Unofficial reports suggested that there was good reason to believe that transmission had persisted for almost 2 years in Iran, 8 months in Iraq and 4 months in the Syrian Arab Republic, with many more cases than had been reported.
Fig. 26.9. Countries of south-western Asia and the Arabian Peninsula and the methods by which they were certified.
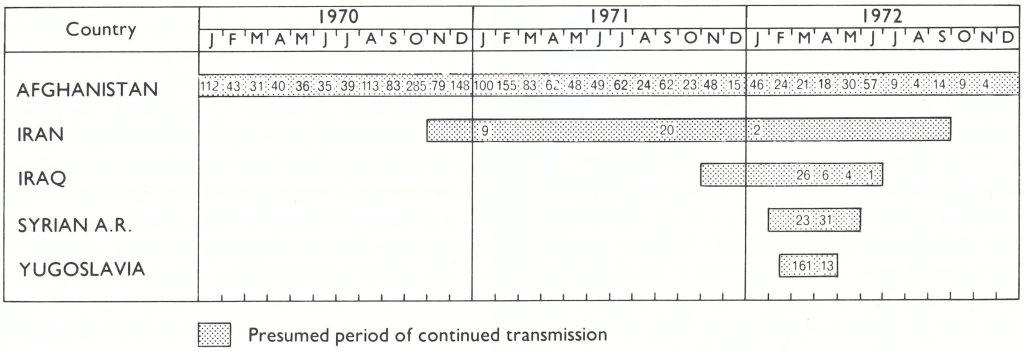
Fig. 26.10 Smallpox in Afghanistan, 1970-1977, and the 1970-1972 outbreak of smallpox in Iran. Following an importation from Afghanistan. The disease spread to Iraq and the Syrian Arab Republic, and from Iraq to Yugoslavia. Numbers indicate the cases officially reported to WHO by month. In both Iran and Iraq, the numbers of cases which actually occurred and were known to the respective governments were far larger (see Chapter 23).
The last cases of smallpox in these countries were believed to have occurred in 1972, some 5 years earlier but the Consultation believed that it was important to confirm with greater certainty that smallpox was not persisting in any of them and had not been present for at least the last 2 years. It therefore recommended that visits should be made to Iran, Iraq and the Syrian Arab Republic by Global Commission members, consultants and/or WHO staff, to verify and document smallpox eradication and present their findings to the meeting of the Global Commission in December 1978.
Certification did not proceed exactly as suggested by the Consultation. Iraq and the Syrian Arab Republic were visited and certified in succession by an international commission, of which the chairman, Dr Robert Netter, was a member of the Global Commission. In Iran, however, although extensive precertification activities were conducted, political events made it impossible to arrange the planned visit of an international commission to that country.
Yemen
A WHO-assisted smallpox eradication programme had been initiated in Yemen in 1969 in the course of which the primary vaccination of 0.7 million children and the revaccination of 1 million persons, out of a population of 4.8 million, were carried out. Surveillance activities had discovered 23 possible smallpox cases between 1970 and 1977, but when specimens from these cases were examined in WHO collaborating centres no poxvirus particles were found.
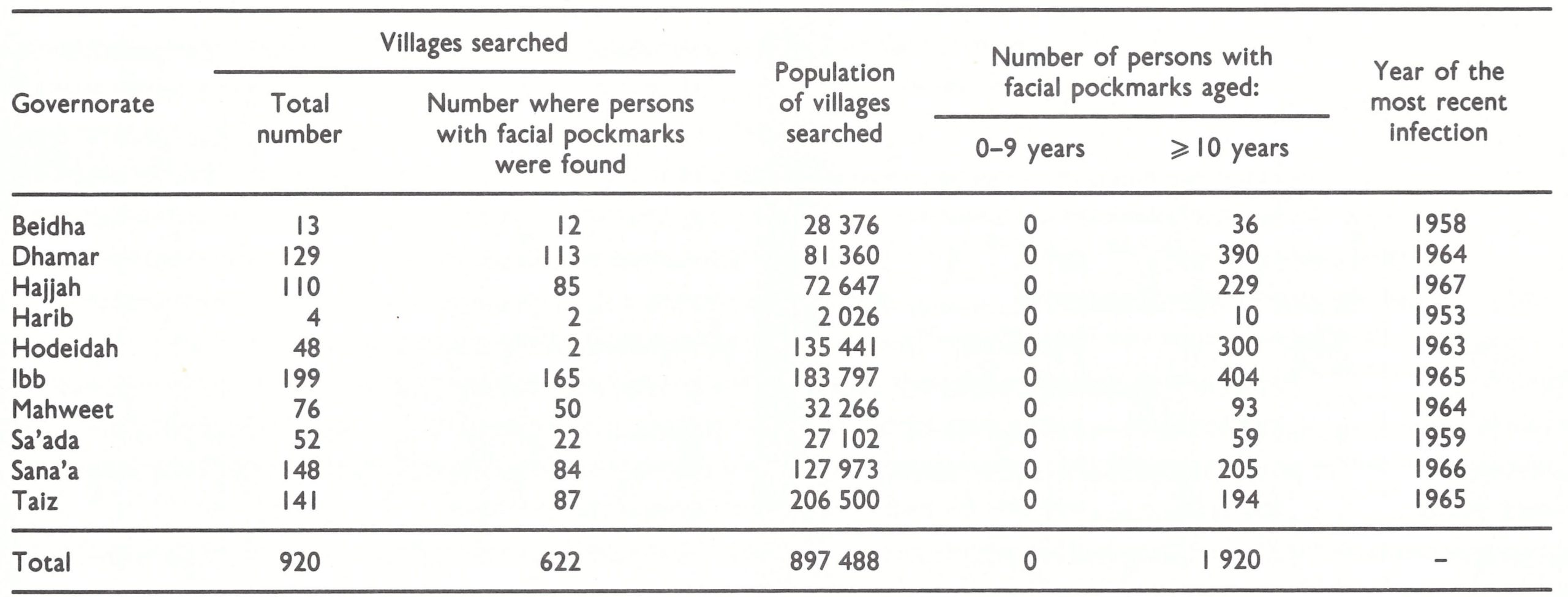
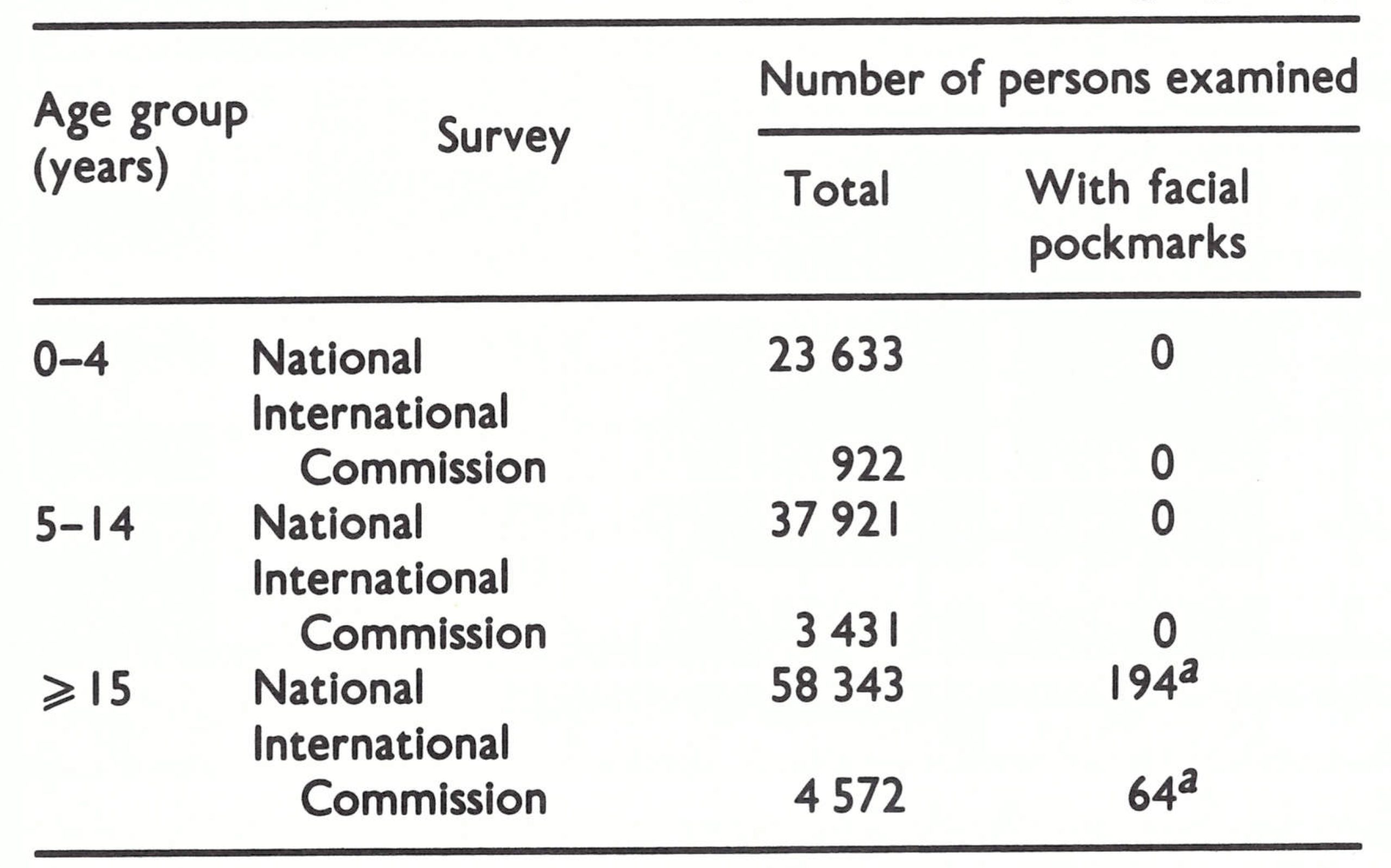
In 1978 and 1979, a special search was conducted with the assistance of Mr Robert C. Steinglass, a WHO operations officer. This included the investigation of suspected cases of smallpox, the collection of specimens from every chickenpox outbreak discovered in the country, and facial pockmark and vaccination scar surveys in a large number of selected localities. Altogether 920 localities were visited in 146 of the 162 districts. The WHO reward of US$lOOO for information on new smallpox cases that could be confirmed was widely publicized to stimulate the reporting of suspected cases. In contrast to African countries, in which variola minor had been most recently endemic, variola major had been the prevalent form in Yemen, and a facial pockmark survey covering some 20% of the total population revealed 1920 pockmarked persons, all of whom were over 10 years of age (Table 26.16). None of them had had smallpox more recently than 1967. None of the 42 specimens collected from cases of fever with rash was found by WHO collaborating centres to contain poxvirus.
A vaccination scar survey revealed that only 22.9% of children aged 0-4 years had vaccination scars, a proportion that rose to 65.6% among those aged 5-9 years.
Table 26.16: Yemen: results of facial pockmark survey during active searches, 1978-1979
Visit of the International Commission, 2-10 June 1979
After preliminary discussions in Sana’a, the Commission members formed 3 teams and travelled widely throughout the country, except in the sparsely populated eastern desert area of the Marib, which was closed for political reasons. The results of the surveys confirmed those presented in the country report, and the Commission concluded that there was no evidence that there had been any endemic cases of smallpox since the last recorded cases in 1969. Accordingly, Yemen was certified to be smallpox-free.
Democratic Yemen
Although Democratic Yemen had not reported a confirmed case of smallpox since 1961, the government undertook a smallpox eradication programme, beginning in 1970. In a mass vaccination campaign combining smallpox and BCG vaccinations, 4 mobile vaccination teams had performed 1.7 million smallpox vaccinations between 1970 and 1977, among a population of 1.7 million; 578 000 were primary vaccinations, and the take rate was over 90%.
Precertification activities
Special search operations were carried out between February 1978 and February 1979, with the assistance of a WHO epidemiologist, Dr Mohamed El Naggar. The offer of a reward of 50 Yemeni dinars (approximately US$l50) for the notification of a case of smallpox was publicized by newspapers, radio and television. During a year-long operation, active searches were conducted in 55 of the 83 subdistricts in the country, including 2 subdistricts on the island of Socotra. Dr R.N. Basu and Dr Holger Lundbeck, members of the Global Commission, visited the country in November 1978 to study and advise on preparations for certification.
Pockmark survey. Facial pockmarks were seen only in persons over 14 years of age (Table 26.17). From the replies to questions put to those with pockmarks, it emerged that the most recent infection among them in Democratic Yemen had occurred in 1958. A vaccination scar survey recorded 59.8 yo with scars in the age group 0-4 years, the corresponding proportion reaching 96.9% in the age group 5-14 years. Of 36 specimens collected from cases of fever with rash during 1978-1979 and examined by WHO collaborating centres, 8 showed herpesvirus particles and none poxvirus.
Visit by the International Commission, 3-11 June 1979
After a briefing meeting in Aden, 3 teams, each including a Commission member, a WHO consultant and a national representative, visited 18 districts and carried out limited surveys for facial pockmarks (Table 26.17) and vaccination scars. The results obtained corroborated the evidence presented in the country report.
The Commission concluded that there was no evidence that the endemic transmission or importation of smallpox had occurred in Democratic Yemen since the smallpox eradication programme had begun there in 1970. It certified the country to be free of smallpox.
Table 26.17: Democratic Yemen: results of facial pockmark surveys by national teams, February 1978-February 1979, and by members of the International Commission, June 1979, by age group
 a Due to smallpox contracted before 1959.
a Due to smallpox contracted before 1959.
Arab Countries of the Gulf Area: Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates
The health services of these 6 countries had been greatly strengthened since the increase in income from oil production in the early 1970s. Indigenous transmission of smallpox was thought to have ceased in all of them in the 1960s, but there were numerous opportunities for importations to occur (see Chapter 23, Table 23.10) and the inadequacy of the surveillance system at that time meant that a report of zero incidence of smallpox could not be regarded as completely reliable. The 1977 Consultation on the Worldwide Certification of Smallpox Eradication had therefore requested that detailed country reports should be supplied to the Global Commission (see Chapter 24).
One of the members of the Consultation, Dr Jalal M. Aashi, who was at the time Secretary-General of the Secretariat-General of Health for the Arab Countries of the Gulf Area, arranged for a member of the Smallpox Eradication unit, Dr Ehsan Shafa, to attend the meeting of the Secretariat-General in Riyadh, Saudi Arabia, from 30 October to 2 November 1977. Dr Aashi and Dr Shafa had drawn up a plan of action for the Gulf states, to be implemented during 1978, and this was approved by the assembled ministers of health. In fact the plan was more thorough than the Consultation’s suggestions had indicated. Under its terms each country was requested: (1) to carry out chickenpox surveillance and collect specimens from selected cases; (2) to establish and maintain rumour registers of suspected cases of smallpox; (3) to carry out facial pockmark surveys; and (4) to prepare a country report. Specimen collection kits and forms for each section of the plan of action were provided.
Dr Arcot G. Rangaraj, a veteran of the smallpox eradication campaign in Afghanistan, was appointed as a WHO consultant for 6 months (1 March-31 August 1978) to help to implement the plan of action. He visited each country 3 times, contacting public health laboratories, hospitals, health centres and clinics, medical officers of oil companies, missionary and other private institutions, and private practitioners.
The results of the special investigations are shown in Table 26.18. There was no evidence that smallpox had been present in any of the 6 countries since 1971.
After reviewing the excellent data provided in the reports of these countries, the Global Commission, meeting in December 1978, had no hesitation in certifying all of them to be free of smallpox.
Table 26.18: Arab countries of the Gulf area: results of precertification investigations, January-July 1978
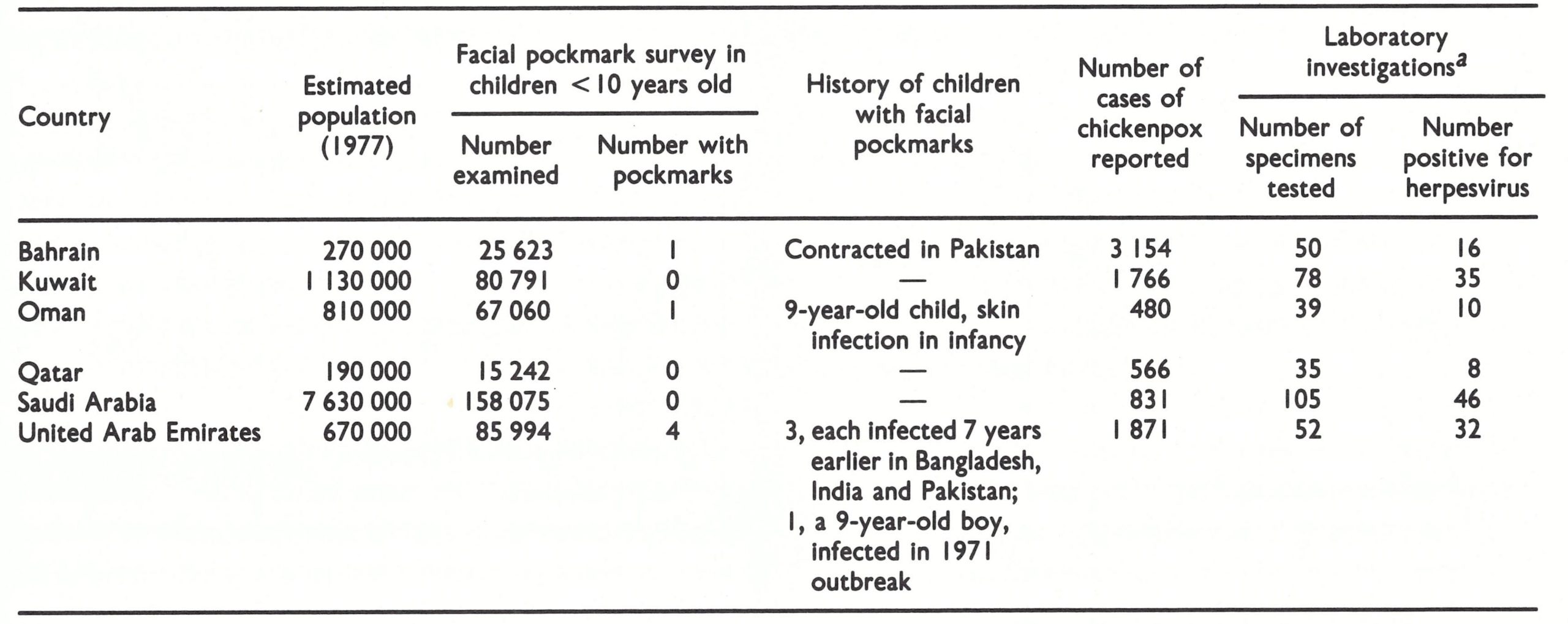 a 5pecimens examined at WHO collaboratlng centres; all were negatlve for poxvirus.
a 5pecimens examined at WHO collaboratlng centres; all were negatlve for poxvirus.
Iran
Preparations for certification
Shortly after the Consultation in October 1977, Dr Shafa visited Iran from 2 to 14 December 1977, during which time, in collaboration with the health authorities, a plan of operations for the confirmation of smallpox eradication was prepared. In view of the large epidemic of smallpox in Iran in 1970-1972 (see Chapter 23), government health officials agreed to carry out a comprehensive programme. This was to last for 6 months, starting on 21 March 1978 (the Iranian New Year), and include: (1) chickenpox surveillance with the compulsory reporting of cases, and epidemiological and laboratory investigation of chickenpox outbreaks associated with deaths; (2) the maintenance of a rumour register and reports on the investigation of suspected cases of smallpox; (3) facial pockmark surveys; and (4) the preparation of a comprehensive country report.
Dr Parviz Rezai, Deputy Director-General of Communicable Diseases Control and Malaria Eradication, was put in charge of the programme, and by the end of February 1978 sanitary inspectors from every province in Iran, who were responsible for specimen collection, had attended a seminar in Teheran and been issued with specimen collection kits. A seminar was also held, attended by the chiefs of the communicable disease departments of all the provinces, to discuss the plan of action and their role in its execution.
Activities went on until 23 September. Dr Shafa continued to follow their progress closely and visited Iran again in August 1978. In October, he and Dr Lawrence Brilliant, who had worked as a WHO staff member in the smallpox eradication programme in India, visited Iran to assist in the analysis of the data and the preparation of the final report for the Global Commission. They also paid brief visits to the provinces of Ilam, Fars and Isfahan. It had been planned that Dr Aashi and Henderson, members of the Global Commission, would visit Iran between 1 and 15 November, during which time they would be provided with a supplementary report giving epidemiological details of the 1970-1 972 outbreak. However, their visit had to be cancelled owing to increasing civil unrest, which culminated in the deposition of the Shah and the proclamation of an Islamic Republic on 1 April 1979.
Pockmark survey. The object of the facial pockmark survey was to confirm the absence of smallpox during the previous 5 years (1973-1978); hence only children under 5 years of age were examined. The areas to be surveyed were selected in the following order of priority: (1) the environs of the last known smallpox outbreaks; (2) districts in which deaths from chickenpox had been reported; (3) districts in which suspected cases of smallpox had been reported; and (4) border territories and remote areas.
Of 72 337 children examined (1.2% of all those under the age of 5 years), 15 were reported to have apparent pockmarks. On investigation, the scarring was found to be due to chickenpox in 11 cases, to boils in 3 cases, and to the secondary infection of chickenpox vesicles in 1 case. The survey was conducted in 160 of the 162 districts, in all 23 provinces. Dr Brilliant visited the provinces of Fars and Isfahan during October 1978 and confirmed that the facial pockmark survey was well designed, the sampling frame was carefully chosen, and the survey procedures were understood by the health workers.
Chickenpox surveillance. Weekly reporting of chickenpox from each district by telegram was made compulsory for the 6-month period 21 March-23 September 1978. In all, 4076 cases were reported, giving an incidence of 12.2 per 100 000 population over a 6-month period, which was similar to incidence rates in other countries in which extensive chickenpox surveillance programmes had been undertaken. Of these reported cases, 88% were verified by senior health officials and epidemiologically analysed; 85% of the persons in question had vaccination scars. Laboratory specimens were taken from 46% of the 459 cases in unvaccinated subjects and from 140 chickenpox cases which, although the persons concerned had been vaccinated, were either severe or atypical or had occurred in an adult. Specimens were collected from every province except Boyer Ahmadi-ye Sardsir va Kohkiluyeh, Kerman, Ilam, and Lorestan. Ilam Province, which had reported the poorest chickenpox surveillance, was visited and checked by Dr Shafa in October 1978. All 349 specimens tested by WHO collaborating centres proved negative for poxvirus.
Special investigation of suspected smallpox cases. Four unusual cases of skin disease were investigated by physicians from the Communicable Disease Unit in Teheran. Two were found to be cases of molluscum contagiosum and the other 2 were severe chickenpox. Routinely, all cases of fever with rash were regarded as suspected cases of smallpox until proved otherwise by clinical, epidemiological and laboratory findings. Between 1973 and mid-1978, 309 such cases were investigated. All proved negative for variola virus on laboratory examination by the Pasteur Institute in Teheran, an establishment which had demonstrated a good laboratory capability for smallpox diagnosis in 1971-1972.
Review by the Global Commission, 7 December 1978
Dr Rezai presented a detailed country report entitled Smallpox Eradication in Iran, and Dr Brilliant an additional document, The Special Programme to Confrm Smallpox Eradication in Iran. In addition, 2 confidential reports-Smallpox in Iran 1970-72, prepared by the Iranian government, and Smallpox in Fars Province, Iran, 1970-72, prepared by Dr Brilliant-were made available to a special group of Commission members. These 4 reports provided very comprehensive data on the smallpox situation in Iran. The confidential government report gave details of 1996 cases of smallpox that had occurred in 400 outbreaks between November 1970 and September 1972 (see Chapter 23, Fig. 23.4), of which 1349 had been confirmed as positive for variola virus in the laboratory in Teheran.
The epidemic had originated from an importation from Afghanistan and was eventually controlled by mass vaccination. Its long duration (23 months) was due to the use of poor-quality liquid vaccine, and it was rapidly controlled as soon as potent freeze-dried vaccine became available (see Chapter 23). The political decision not to report the actual number of cases to WHO did not prevent the health services from being fully operational within the country and from being committed to eliminating the disease. There was no reason to believe that any cases had occurred after September 1972.
As has been mentioned above, political circumstances had led to the cancellation of the planned visit to Iran in November 1978 by members of the Global Commission, as recommended by the October 1977 Consultation, but on the detailed evidence before it the Global Commission had no hesitation in certifying that Iran was free of smallpox.
Iraq
Smallpox had been eliminated from Iraq in 1959, so that there had been no WHO-assisted smallpox eradication programme in the country. Vaccination, and subsequently certification activities, were undertaken by the regular health services. Late in 1971, smallpox had spread from Iran to Iraq (see Fig. 26.10) but, as in Iran, the authorities had been reluctant to report it. Evidence obtained subsequently suggested that there had been at least 800 cases (see Chapter 23), but that the outbreak had been finally contained by June 1972.
Preparations for certification
In May 1978 Dr James Tulloch, a consultant with the Smallpox Eradication unit, visited Iraq to assist with the preparation of a country report and the organization of a facial pockmark survey. The basic report was prepared in collaboration with Dr Felix Jurji, the national Director of Epidemiology and Quarantine. In June, the Director-General of the Public Health Administration sent forms to all departments in the school health administration with a request that all schoolchildren should be examined for pockmarks and that the forms should be returned by mid-September for presentation to members of the International Commission, which planned to visit Iraq in October.
Visit by the International Commission, 5-15 October 1978
Because of the reluctance of the government to discuss the 1971-1972 epidemic, members of the Commission concentrated on determining whether Iraq had been free of smallpox for at least the previous 2 years. After a briefing meeting in Baghdad, Commission members and their colleagues formed 2 teams, which travelled widely through the country. They checked the quality of the reporting system, and visited hospitals, health units and the diagnostic laboratory in Baghdad. The general impression everywhere was one of competence. In the laboratory, 162 specimens collected between 1972 and 1978 from patients with a rash had been tested; all had proved negative for variola virus. Of these, 27 collected in January 1978 and 11 collected in March-June 1978 were tested in WHO collaborating centres, all with negative results.
Four out of 3825 children aged between 4 and 12 years who were examined had pockmarks, all due to smallpox contracted before or during 1972. Vaccination coverage was between 75% and 100% in primary-school children, depending on the area, and between 50% and 80% in preschool children.
The Commission concluded that there was no evidence that smallpox had occurred in Iraq since 1972 and that the health services were sufficiently reliable from the point of view of detecting, recording and reporting communicable diseases to ensure that, if a case of smallpox had occurred, it would have come to the notice of the central public health authorities. However, between their visit in October and the meeting of the Global Commission in December, the results of the facial pockmark survey had been received; these showed that 17 out of 195 665 schoolchildren had “facial pockmarks”. No details were provided of the children’s ages or of the dates on which they had suffered from smallpox. Certification was therefore delayed pending clarification of the situation. Subsequently, it was reported that, of these 17 children with “facial pockmarks”, 16 had good primary vaccination scars, 15 cases were of chickenpox, 1 had had boils, and 1 had had another kind of skin infection. This information was sent to all Global Commission members in March 1979 and Iraq was certified to be smallpox-free by correspondence on 17 April 1979.
Syrian Arab Republic
Because endemic smallpox had been eliminated from the Syrian Arab Republic in 1950, there had never been a smallpox eradication programme in the country. All vaccinations were carried out by the regular health services. The Iran-Iraq epidemic had spread to the Syrian Arab Republic in February 1972, but appeared to have been contained by May of that year (see Chapter 23).
Preparations for certification
After his visit to Iraq, Dr Tulloch proceeded to the Syrian Arab Republic in May 1978 to help to arrange the preparation of a country report, a facial pockmark survey and the collection of specimens for laboratory testing. Dr Nouri Ramzi, Vice-Minister of Health, arranged for Dr Tulloch to visit the area of the last outbreak, in which there were 54 reported cases around Meyadin in the south-eastern part of the country, along the Euphrates River, and on the main road from Baghdad (see Chapter 23, Fig. 23.5). A survey of 507 schoolchildren in this area found 15 with facial pockmarks due to smallpox, which made it clear that more cases had occurred than were notified in 1972, as well as revealing an unreported outbreak in the period 1966-1 967. For the purposes of certification, it was not considered worthwhile to make a major effort to clarify events which had taken place over 6 years before, but the government was asked to undertake a facial pockmark survey of the 6-year-old children entering school in September. If no pockmarks were found among them, that would be considered good evidence that no cases had occurred since 1972. Surveys carried out on 28 072 6-year-old children in 197 schools in Damascus and 11 320 children in 207 schools in Deir-ez-Zor failed to find any pockmarks. The vaccination coverage was good in schoolchildren in the higher grades—namely, 80-95%—and 50-60% among those in the first grade.
Since 1972, when 3 specimens taken from cases were found to contain variola virus by the WHO collaborating centre in Atlanta, USA, 1 specimen tested in 1974 had proved negative, as had 6 specimens tested by WHO collaborating centres between August and October 1978.
Visit by the International Commission, 15-22 October 1978
After reviewing data with the health authorities in Damascus, Commission members visited health centres and primary schools. Of 3873 children then examined, one had facial scarring reportedly due to smallpox contracted in Haffe in 1971. Four other persons with pockmarks were adults who had suffered from smallpox some 30 years previously. Commission members reviewed the reports and concluded that the detecting, recording and reporting of communicable diseases in the country were sufficiently reliable to ensure that, if an outbreak of smallpox had occurred since 1972, it would have come to the notice of the central public health authorities. Their recommendation that the Syrian Arab Republic should be certified to be free of smallpox was accepted by the Global Commission in December 1978.
SOUTH-EASTERN ASIA
At the other side of the Asian land mass were several countries in which WHO assisted smallpox eradication programmes had never been operative because the disease had been eliminated in 1962 or earlier. The largest country, China, is the subject of detailed consideration in Chapter 27. Malaysia had eliminated endemic smallpox by the end of 1949 and effectively controlled a large outbreak that had occurred after an importation in 1959 and continued into 1960. Singapore had reported no cases since ‘a small outbreak following an importation in 1959. Both countries had had stable governments since 1960 and the Consultation did not recommend that any special investigation should be undertaken. The remaining 4 countries were Democratic Kampuchea, the Lao People’s Democratic Republic, Thailand and Viet Nam; the numbers of reported cases of smallpox in these countries during the period 1952-1963 are shown in Table 26.19.
The October 1977 Consultation had recommended that, because of the prolonged hostilities and the possibility of breakdowns in the public health services, country reports should be obtained for Democratic Kampuchea, the Lao People’s Democratic Republic and Viet Nam. The authorities of each of the countries concerned were to be asked to endorse these reports and, in so doing, to certify that no cases of smallpox had occurred in their country for the past 2 years. In view of the intense traffic between Thailand and India and Bangladesh, it was recommended that a member of the Global Commission or a WHO consultant should visit Thailand.
Plate 26.6. James Tulloch (b. 1949), an Australian epidemiologist who served as a consultant to the smallpox eradication programme from 1976 to 1980. He participated in the final stages of the eradication programme in Bangladesh and played an active role in preparations for certification in many countries
Table 26.19: Thailand, Democratic Kampuchea, Lao People’s Democratic Republic and Viet Nam: numbers of reported cases of smallpox, 1952- 1963
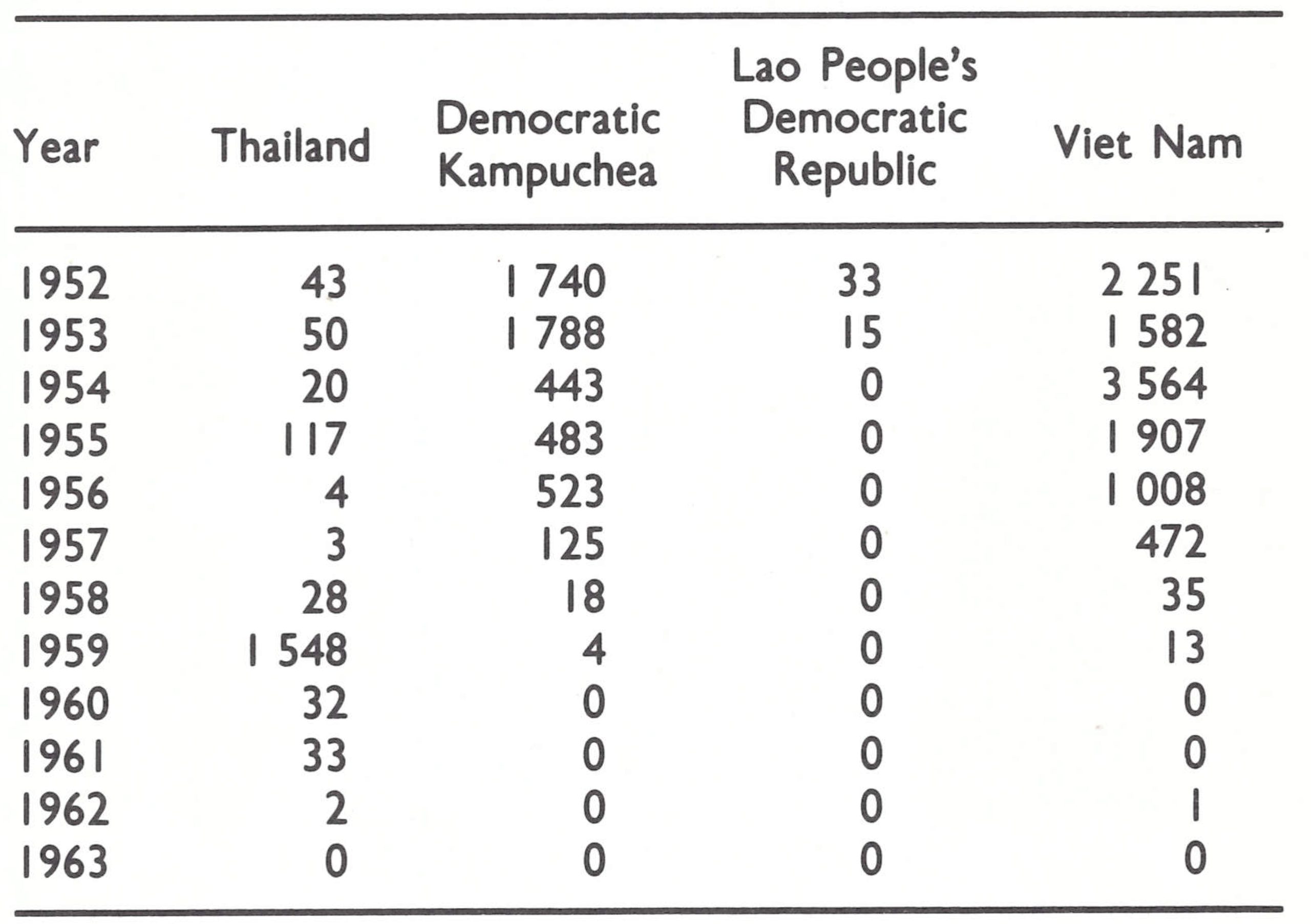
Lao People’s Democratic Republic and Viet Nam
In recommending that country reports should be obtained from Democratic Kampuchea, the Lao People’s Democratic Republic and Viet Nam, the Consultation had taken a cautious attitude, for there had been only 1 reported case (in Viet Nam in 1962) since 1959. Because of the fighting there during the 1960s and 1970s, large numbers of foreign soldiers had been present in these countries, but no reports of the occurrence of smallpox had been received. Furthermore, smallpox had been absent from neighbouring countries for many years, and over the past decade there had been little communication with the endemic countries of the Indian subcontinent.
Much of the available information on Democratic Kampuchea, the Lao People’s Democratic Republic and Viet Nam was in the files of the WHO Regional Office for the Western Pacific in Manila, which requested these countries in March 1978 to provide additional information. However, by August of that year no reports had been received at WHO Headquarters in Geneva. To accelerate matters, Dr Bert van Ramshorst, a medical officer in the Smallpox Eradication unit, was sent to Manila on 4 October 1978 to prepare country reports, based on the data available in the regional office, for the Global Commission meeting early in December. These were sent to the respective governments for endorsement, which was eventually received in Geneva from Viet Nam on 28 November and from the Lao People’s Democratic Republic on 29 November. Thus the Lao People’s Democratic Republic and Viet Nam were certified by the Global Commission on the basis of the reports prepared from the documentation available in the regional office and the official statements by their respective governments that the countries were smallpox-free. However, the certification of Democratic Kampuchea had to be deferred, because government endorsement of the country report had not been received.
Democratic Kampuchea
Formal endorsement by the government of Democratic Kampuchea of the country report prepared by the Smallpox Eradication unit proved to be very difficult to obtain because of the political turmoil in that country. Briefly, the situation was that, after a prolonged civil war, the Kampuchean National United Front for National Salvation took power in January 1979, overturning the Khmer Rouge government under Pol Pot and calling the country the People’s Democratic Republic of Kampuchea. The Khmer Rouge fled, but continued to fight a guerrilla war against the new government, at the same time setting up, together with other groups, a rival coalition government. The latter was recognized by the United Nations, so that official contact with the authorities who were actually running the country, necessary in order to obtain endorsement of the country report, was not possible.
In accordance with the decision that official government endorsement of the report was essential, the Global Commission, meeting in December 1978, deferred certification. During the succeeding months WHO took a number of steps designed to break the deadlock. These included attempting to make contact with the Ambassador of Democratic Kampuchea in Beijing and approaches via Dr Robert Netter, a member of the Global Commission resident in Paris, since at that time two French groups were working in Democratic Kampuchea, as were UNICEF and the International Committee of the Red Cross.
In early autumn news came that Dr My Samody from Phnom Penh was attending a meeting at the International Committee of the Red Cross in Geneva. He was contacted and given a copy of the report. At the same time an urgent request for the endorsement of the report was addressed to the government recognized by the United Nations through its mission in Geneva, but no reply was received.
On 8 November, a letter dated 25 October 1979 was received from Dr Nu Beng, Minister of Health of the People’s Democratic Republic of Kampuchea in Phnom Penh, endorsing the country report and containing a declaration of the smallpox-free status of the country. This was accepted by the Global Commission, and together with China (see Chapter 27), Democratic Kampuchea was the last country in the world to be certified, on 9 December 1979.
Thailand
In accordance with the recommendation of the October 1977 Consultation, Dr R. N. Basu, then Assistant Director-General of Health Services in India and a member of the Global Commission, visited Thailand from 8 to 27 May 1978 for an initial appraisal, field visits and the preparation of documentation. He visited Bangkok and 4 provinces, where he interviewed personnel in health offices, hospitals, clinics and schools, and also visited 2 refugee camps on the Laotian border. In the camps, he examined people for vaccination scars, and by questioning them found that none had ever seen a case of smallpox either in the camp or in their country of origin. Dr Basu observed the way in which the communicable disease surveillance system operated in hospitals, in the 4 regional epidemiological offices, in the regional communicable disease control offices, and in remote areas, where mobile units were used for this purpose; he also evaluated the performance of the health volunteers scheme for providing primary health care at village level.
Documentation provided for the Global Commission included a comprehensive country report prepared by the government of Thailand and a paper presented by the government at the 1967 interregional seminar on smallpox eradication, which gave epidemiological details of the eradication of the disease in Thailand. The last case occurred in 1962—an importation from Calcutta, which did not give rise to any secondary cases.
On the basis of the country report and the evidence presented by Dr Basu, the Global Commission in December 1978 certified that smallpox had been eliminated from Thailand.
CONCLUSIONS
This complex series of operations, involving 29 countries in Africa and Asia over the brief period of 24 months, completed the certification of smallpox eradication in all the countries of the world in which the disease had been endemic in 1967, or countries otherwise regarded as at high risk, except for China and the countries of the Horn of Africa. Many different procedures were adopted, depending mainly on the prior history of smallpox and a variety of political considerations. There remained only the certification of China, the Horn of Africa and the adjacent country, Kenya, and the receipt from other Member States of WHO of certificates denoting freedom from smallpox for at least the preceding 2 years. These matters are discussed in the next chapter.