Chapter 13:
Indonesia

INTRODUCTION
In 1967, smallpox was endemic in 5 Asian countries, whose total population amounted to 769 million. Four of these —countries Afghanistan, India, Nepal and Pakistan—were contiguous, sharing long borders, which travellers (including people infected with smallpox) crossed with relative freedom. However, the fifth country, Indonesia (population, 112 million), lay some 2000 kilometres south-east of the nearest endemic area on the continent—East Pakistan (after 1970, Bangladesh). Comparatively few people travelled between Indonesia and the other 4 countries. Thus, it seemed logical and opportune to concentrate resources and energies initially in Indonesia in the expectation that on becoming free of smallpox, the country would not be seriously threatened by importations (Wkly epidem. rec., 1969a). WHO resources committed to Indonesia could then be shifted to other programmes in Asia. The fact that smallpox transmission had once been interrupted in Indonesia, immediately before the Second World War, added strength to the belief that the objective could be attained.
As had been hoped, Indonesia was the first of the 5 Asian countries to become free of smallpox. The programme began there in June 1968; the last known case occurred little more than 3 1/2 years later, on 23 January 1972. The achievement of eradication so quickly in such a large and populous country was both a surprise and a stimulus (and to some degree an embarrassment) to health staff in Bangladesh, India and Pakistan, whose programmes had by then been in progress for a decade. That this feat had been accomplished with little more than US$1 million in international assistance made it even more notable.
Success was not easily achieved in the Indonesian programme. Smallpox was tenacious and spread readily even among populations with exceptionally high levels of vaccinial immunity—a marked contrast to the behaviour of the disease in most endemic countries of Africa and the Americas. Full credit for the achievement is due to an imaginative group of Indonesian and WHO staff, who conceived and evolved effective strategies that were later adapted for use in other parts of the world and proved vital to the interruption of smallpox transmission in the Indian subcontinent. Among Indonesia’s contributions to global eradication were the concept of a special programme involving a village-by-village search for cases, the introduction of a reward system for anyone reporting a case of smallpox and the development of the widely used WHO smallpox recognition card (see Chapter 10, Plates 10.29, 10.30).
A number of papers were prepared describing selected aspects of the Indonesian programme, although a book would have been warranted to recount the whole gamut of activities. There was little time available to attempt a detailed narration, however. When eradication was certified in 1973, experienced staff were urgently needed in other countries; key Indonesian staff and the WHO advisers who had been assigned there responded promptly and, in so doing, contributed to the record of achievement compiled in India, Bangladesh and Ethiopia.
THE DECISION TO BEGIN THE PROGRAMME
Originally it had been hoped that the campaign in Indonesia might begin during the first year of the Intensified Smallpox Eradication Programme but its start was delayed until June 1968. In part, this stemmed from doubt and inertia in the WHO Regional Office for South-East Asia in New Delhi, India. The then Regional Director believed that the health resources in the countries of the region were too inadequate to permit eradication to be realized. He frankly and publicly stated his view that the World Health Assembly’s decision to undertake global eradication was ill-advised, and consequently offered little support to the programme. Likewise, the Regional Adviser for Communicable Diseases, the senior technical officer, took little interest . A memorandum of 10 October 1967 from Henderson to his superior in WHO Headquarters, Dr Karel Raska, the Director of the Division of Communicable Diseases, summarized the situation prevailing during much of that year :
“In December [1966] and April [1967], the considerable importance of an early visit to Indonesia to assess Government interest and capability to undertake [smallpox eradication] had been agreed by [the Regional Adviser for Communicable Diseases] and myself. No visit has yet been undertaken and none is contemplated until possibly November. In fact, I gather there was no correspondence with Indonesia on the question of [eradication] until July…No solutions are proposed; no possible courses of action are outlined .”
Subordinate to the regional adviser and ostensibly responsible for providing assistance to countries in developing smallpox eradication programmes was a 2-man intercountry advisory team for epidemiology whose duties then encompassed a range of different activities. During his visit to New Delhi, Henderson had met the team, which had exhibited both an interest and a desire to proceed rapidly in the development of WHO smallpox eradication programmes. Subsequent communication with them by mail proved difficult. All correspondence relating to smallpox eradication between WHO Headquarters and the regional office, as well as between the countries and the regional office, was routed first to the regional adviser. Seldom was it passed to the intercountry team. By the end of November 1967, the intercountry team had been permitted to make only two brief visits, to Afghanistan and Nepal, the only countries in the region in which WHO-supported smallpox eradication programmes were then in progress. In the autumn of 1967, one of the team’s members, Dr Jacobus Keja, prepared a draft plan of operations for Indonesia but was denied permission to visit the country to discuss the plan.
The lack of activity in the South-East Asia Region and its failure to obligate smallpox eradication funds allotted for the calendar year led to important financial ramifications in the global programme as a whole. When the budget for smallpox eradication for 1967 had been approved by the Nineteenth World Health Assembly, several countries had expressed the view that an allotment of US$2.4 million for the first year was too large and proposed instead that a sum of US$1 million should be provided (see Chapter 9). The larger allocation was eventually agreed on, but only after assurances had been given by the Director-General that the full amount was needed and could be spent. In the American and Eastern Mediterranean Regions, activities were progressing sufficiently well to ensure that the funds allotted to them would be obligated. However, US$806 000 had been assigned to the SouthEast Asia Region and little of it had been spent. If these funds were not obligated by the end of the year, not only would they be lost to the programme, but the possibility of questions arising at the next World Health Assembly could be foreseen, conceivably resulting in reductions in subsequent budgets for smallpox eradication. Because of this problem, the Regional Director finally agreed, in November 1967, that the intercountry team should discontinue its other activities and assume primary responsibility for smallpox eradication under a higher-level regional office official, the Assistant Director for Health Services. With this administrative change, the development of a programme in the region became feasible.
Three other events occurred during the autumn of 1967 which were to alter significantly the possibilities for eradication in the South-East Asia Region and in Indonesia in particular. A new WHO Regional Director, Dr Herat Gunaratne, was nominated in September 1967 and took office in February 1968. As President of the Twentieth World Health Assembly, in May 1967, Dr Gunaratne (a former Director-General of Health Services in the smallpox-free country of Sri Lanka) had stated categorically that the eradication of smallpox was wholly achievable, that it was simply a matter of will and determination. As testimony to this belief, he offered his own considerable enthusiasm and support for the programme.
The second event was the appointment in November 1967 of Dr Julie Sulianti Saroso to the post of Director-General for the Control and Prevention of Communicable Diseases in the Indonesian Ministry of Health. This decisive and energetic woman was determined to revivify a discouraged and listless health staff who had received little pay for more than 4 years because of a decision by the previous government that health care costs should be borne primarily by private individuals. Although the health staff were expected to supplement meagre salaries through charges for their services, few were successful in obtaining even subsistence wages. Dr Sulianti promptly asked for help from WHO. The regional office decided that Dr Keja should visit Indonesia en route to an intercountry seminar on smallpox, due to begin in Bangkok on 11 December. He arrived in Jakarta on 7 December 1967.
The third event was the development of epidemic smallpox, beginning in August 1967 with an outbreak in the capital city, Jakarta. By November, more than 50 cases a week were being reported (Fig .13.1).

Plate 13.1. Several national and intercountry seminars on smallpox eradication were held in Indonesia . At the concluding seminar, in September 1972, Julie Sulianti Saroso, Director-General for the Control and Prevention of Communicable Diseases, presented an award to Nyoman Kumara Rai, who had directed the Indonesian Programme since April . Standing behind the Director-General are 2 WHO advisers, G .G .O . Cuboni (for left) and W . L . R . Emmet.
With Dr Sulianti, Dr Keja at once decided to carry out a sample survey of the city to assess vaccinial immunity—the first of many such surveys to be conducted during the global programme. For this survey, 20 field staff from the smallpox and malaria programmes were selected and trained. Each examined 200 children for vaccination scars and the facial pockmarks of smallpox in a house-to-house survey beginning from randomly selected points in the city. In only 4 days, the survey had been completed and the results analysed. From the survey and a review of other available data, it was apparent that there were major problems :
Reporting was incomplete. In all, 1265 cases and 413 deaths had been recorded during 1967, but because so many cases were found during the survey the actual number of cases was thought to be at least twice this figure.
The number of vaccinations given was insufficient to sustain immunity. Jakarta Municipality’s 49 vaccinators had performed 384 000 vaccinations in 1967, but only 35 295 (9.2%) had been primary vaccinations. In a population of 1.4 million, with a birth rate of 40 per 1000, it was calculated that 56 000 primary vaccinations would be required annually simply to protect newborn infants.
The proportion of successful primary vaccinations was unsatisfactory. Take rates of only 60-80% were observed, a phenomenon attributed to the use of vaccine of lower than acceptable titre as well as unsatisfactory vaccination technique.
However, vaccinial immunity, though still not adequate, was found to be far higher than expected. Vaccination scars were seen in 90% of children aged 5-14 years, in 75% of those aged 1-4 years, and in 45% of infants aged less than 1 year. Nevertheless, the situation was clearly disturbing. Smallpox was spreading rapidly throughout a reasonably well-vaccinated urban population; the vaccination campaign was lagging and was further compromised by the use of substandard vaccine; extension of the epidemic into less well vaccinated rural areas was only a matter of time. A programme for smallpox eradication was urgently needed and indeed its development proceeded rapidly.

Plate 13.2. Ignatio F. Setiady (b. 1929), Director of Communicable Disease Control, at the 1967 WHO seminar in Bangkok, Thailand, where plans for the Indonesian programme were worked out.
However, vaccinial immunity, though still not adequate, was found to be far higher than expected. Vaccination scars were seen in 90% of children aged 5-14 years, in 75% of those aged 1-4 years, and in 45% of infants aged less than 1 year . Nevertheless, the situation was clearly disturbing. Smallpox was spreading rapidly throughout a reasonably well vaccinated urban population; the vaccination campaign was lagging and was further compromised by the use of substandard vaccine; extension of the epidemic into less well vaccinated rural areas was only a matter of time. A programme for smallpox eradication was urgently needed and indeed its development proceeded rapidly.
The above-mentioned WHO intercountry smallpox seminar in Bangkok, which, by lucky timing, took place immediately after the Jakarta survey, provided the opportunity for a draft plan of operations to be finalized. Indonesia’s representative, Dr Ignatio Setiady, Director of Communicable Disease Control, met Henderson and Dr Keja, and using the latter’s earlier prepared draft, worked out a plan for the programme and estimated the cost involved and the assistance required.
A critical problem, and one that was never really solved, was that of providing Indonesian staff with high enough salaries to permit them to work virtually full time8. Vaccinators, for example, were then receiving the equivalent of US$2 a month, which was insufficient to buy food for themselves, let alone for their families. WHO’s resources could not deal with the situation in its entirety. Despite this problem, it was apparent from the survey that somehow a large proportion of the population was being vaccinated. With hope rather than confidence that the vaccinators would continue to function, it was agreed that supplementary WHO funds would be provided to a small number of senior Indonesian staff to permit them to carry out full-time supervisory functions; other personnel would necessarily work only part time, and field operations would have to take this into account. WHO also agreed to provide a medical officer and to purchase various items, including 15 vehicles, 135 motor cycles, 1550 bicycles, 23 refrigerators and vaccine production equipment. By the end of December, funds for equipment and supplies had been obligated. Less than a month later, on 24 January 1968, Indonesia’s Minister of Health signed a formal agreement with WHO authorizing the programme. Field operations were scheduled to begin in June 1968.
DEMOGRAPHY AND GEOGRAPHY OF INDONESIA AND ITS HISTORY OF SMALLPOX CONTROL
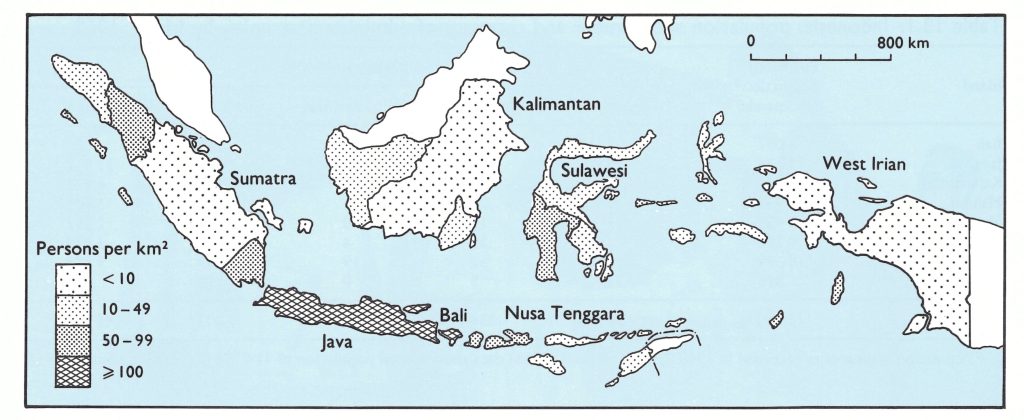
Fig. 13.2. Indonesia: population density, 1968.
The country’s demographic and geographical features, as well as its remarkable history of smallpox control, were determining factors in the development and progress of the programme.
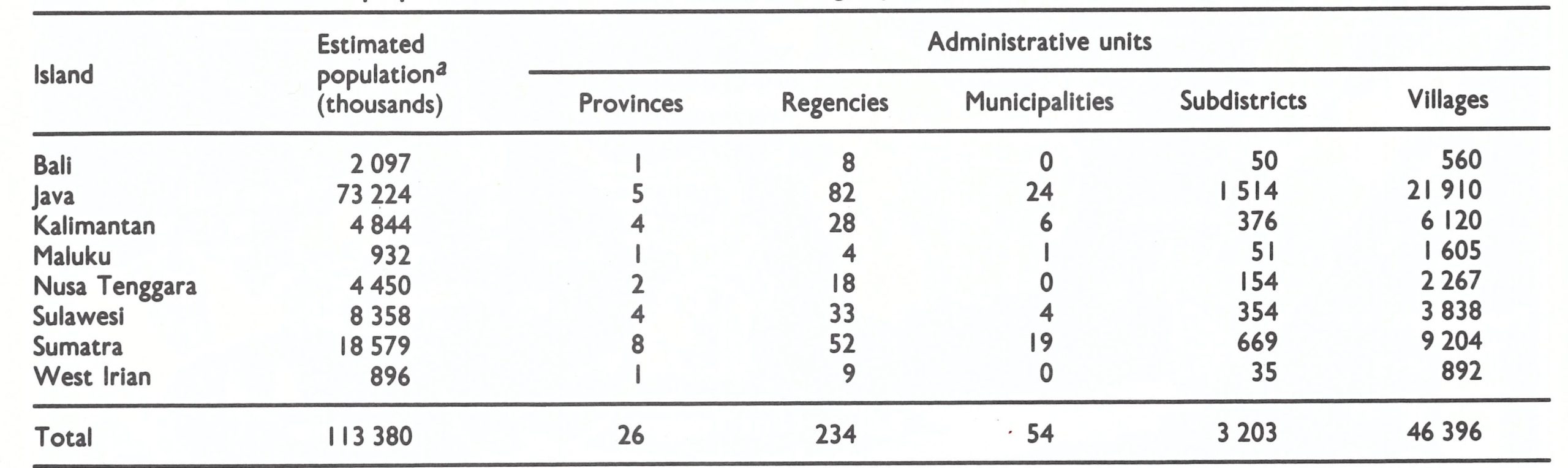
The Indonesian archipelago, extending over more than 4800 kilometres, consists of some 13 000 islands, of which 3000 are inhabited. In 1968, 66% of the country’s 115 million people lived on the densely populated islands of Java and adjacent Bali (Fig. 13.2 ; Table 13.1). Most of them (83%) lived in localities with 5000 or fewer inhabitants or in rural areas . However, it was estimated that fully 60% of the population could be reached by motorized vehicle, 20% by boat and 20% on foot or by bicycle.
Table 13.1: India: political divisions, area and population distribution, 1971a
a Population estimates as recorded in 1968 . United Nations (1985) data show a total population of 114 798 000 for Indonesia in 1968.
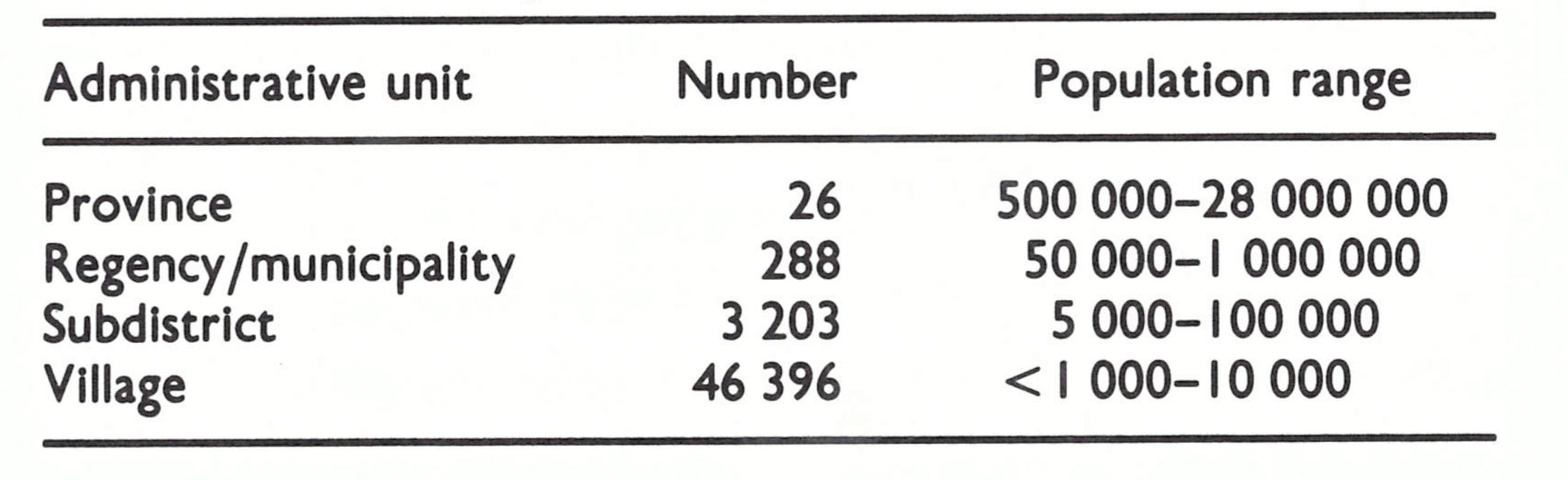
For administrative purposes, Indonesia in 1968 was divided into 26 provinces, which were subdivided into 288 regencies and municipalities (Table 13.2), consisting of 3203 subdistricts . The smallest administrative unit was the village. The size of the population in these administrative divisions varied considerably from one area to another.
Table 13.2: Indonesia: number and population range of administrative units
Although organized vaccination campaigns in Java dated back to 1856, an extraordinarily effective campaign was begun in the 1920s which was successful in interrupting smallpox transmission as early as 1936 (Table 13.3).
Of the 21 cases recorded between 1937 and 1940, 7 were found to be importations and the others were suspected to be either importations or mistaken diagnoses (Polak, 1968). The Second World War intervened and morbidity reporting ceased. After the war, no Of the 21 cases recorded between 1937 and 1940, 7 were found to be importations and the others were suspected to be either importations or mistaken diagnoses (Polak, 1968). The Second World War intervened and morbidity reporting ceased. After the war, no cases are known to have occurred in Indonesia until May 1947. The first cases were reported from the Riau Islands, adjacent to Malaysia, in which smallpox was then endemic. Over the next few years, the disease swept eastwards across the western and central islands of the archipelago, 99 016 cases being reported in 1950. However, smallpox did not spread beyond Sulawesi and West Nusa Tenggara to the numerous but more sparsely populated islands to the east-East Nusa Tenggara, Maluku and West Irian (Fig. 13.3).
Table 13.3: Indonesia : number of reported cases of smallpox, 1924-1940
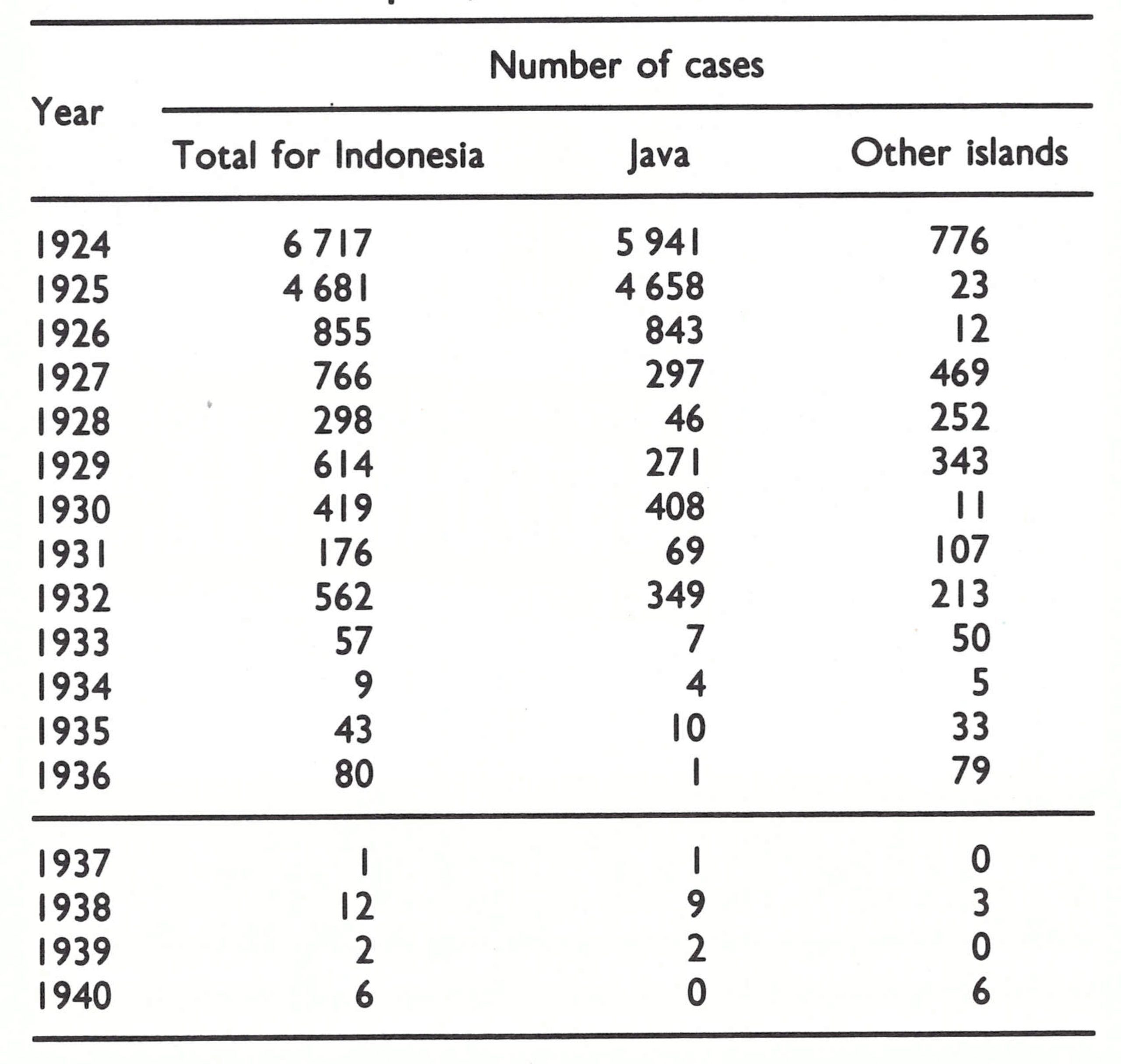
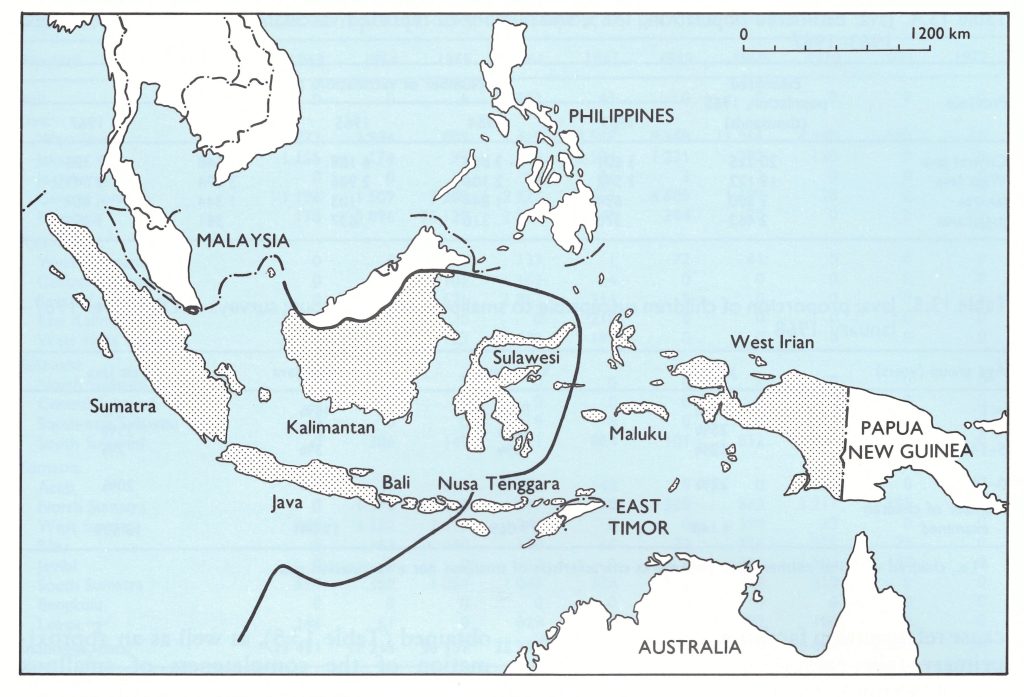
Fig. 13.3. Indonesia and adjacent countries. The heavy line shows the limit of the spread of smallpox after its reintroduction in 1947.
The methodology employed in the vaccination campaign of the 1920s and 1930s is of interest, since the structure and many of the operational components of the campaign still existed in 1968 (Polak, 1968), although the number of staff had diminished and the quality of performance was poorer. A trained vaccinator was assigned a vaccination district of about 100 000 persons. Under the supervision of a medical officer who was responsible for several regencies, he travelled by bicycle and on foot through his assigned district on a strictly prescribed schedule. During each 3-month period, he devoted 8 weeks to primary vaccination and 5 weeks to revaccination. Infants were brought to designated collecting points not more than 6 kilometres from their homes and up to 150 were vaccinated daily. In the case of revaccination, up to 500 persons were dealt with each day. When outbreaks occurred, intensive programmes of vaccination were conducted in the areas infected . Most vaccinators used liquid vaccine, produced by the government-owned quasi-independent Lymph Institute in Bandung (Biofarma), which had opened in 1891. In the more remote districts, a remarkably stable, room-dried and vacuum-sealed vaccine was used which had been first produced in 1926 (Otten, 1932).
In the systematic vaccination campaign, resumed after the Second World War, both liquid and room-dried vaccines and eventually some freeze-dried vaccine were used. High inflation rates and the drastic reduction of salaries of government health staff forced vaccinators and other personnel to take additional jobs. Periodic ad hoc mass vaccination campaigns were also conducted, financed by local merchants and village organizations. The numbers of vaccinations reported by vaccinators in Java from 1963 to 1967 indicate the extent of activity (Table 13.4).
Table 13.4: Java : Estimated population, 1965, and number of reported vaccinations in selected provinces, 1963-1967

In all, 15-25% of the population in the different provinces were reported to have been vaccinated annually by the special vaccinators. Of the total number of vaccinations, 10-15% were recorded as primary vaccinations . In addition, vaccinations were performed in local clinics and maternal and child health units; these were not included in the totals but their number was thought to be large. On the basis of this information, it was difficult to guess the probable extent of vaccinial immunity. Not only were the reports of vaccinations performed considered to be suspect, but primary take rates were reported to range from 33% to 88% . Both high and low rates were recorded during the use of each of the 3 forms of vaccine then being produced : liquid, room-dried, and a small quantity of freeze-dried vaccine . Because refrigeration facilities were limited, low primary take rates with the thermolabile liquid vaccine were understandable. The low take rates with the more stable freeze-dried and room-dried vaccines reflected, in part, the low potency of some batches; moreover, none of the dried vaccine was kept under refrigeration, since the manufacturer claimed that it retained its potency at room temperature for 18 months . Although a few batches attained this degree of stability, most did not.
Special mass vaccination campaigns had been conducted in Jakarta in 1962-1963, in East Java in 1964, in West Java in 1965 and in Central Java beginning in the autumn of 1966. The campaigns were not well supervised or well coordinated and were chronically short of funds to pay vaccinators and to purchase vaccines from the Biofarma laboratory.
Despite the apparently questionable efficacy of the campaign, vaccinial immunity in Java proved to be surprisingly high, although the level of immunity varied widely from one locality to another. Sample cluster surveys, similar to the one conducted by Dr Keja in Jakarta in December 1967, were carried out in January and February 1968 throughout Java. In all, 56 619 children under 15 years of age were surveyed. All the children were examined to determine whether facial pockmarks were present and whether or not they had a vaccination scar. From these studies, an estimate of the level of vaccinial immunity was obtained (Table 13.5), as well as an approximation of the completeness of smallpox notifications.
Table 13.5: Java : proportion of children susceptible to smallpox,a by age group ; surveys of December 1967- January 1968
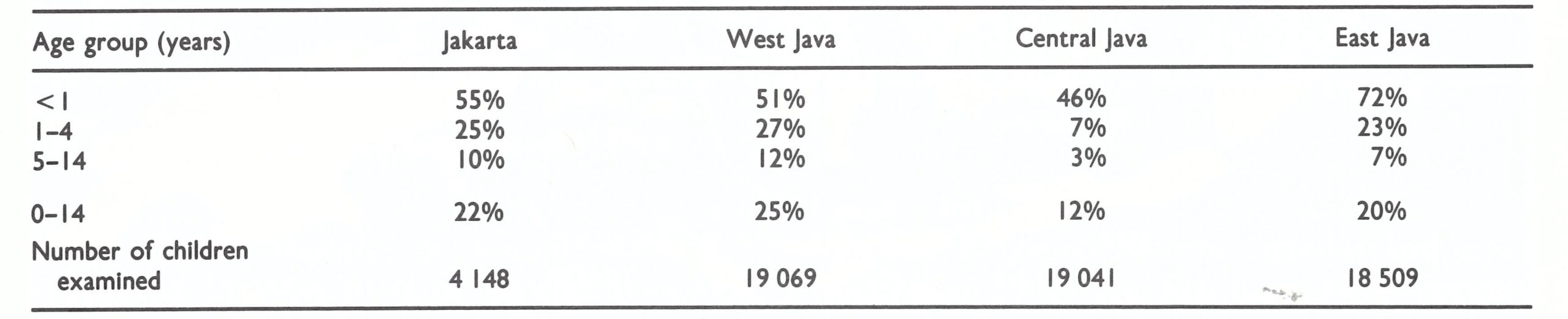 a I.e ., children who had neither facial pockmarks characteristic of smallpox nor a vaccination scar.
a I.e ., children who had neither facial pockmarks characteristic of smallpox nor a vaccination scar.
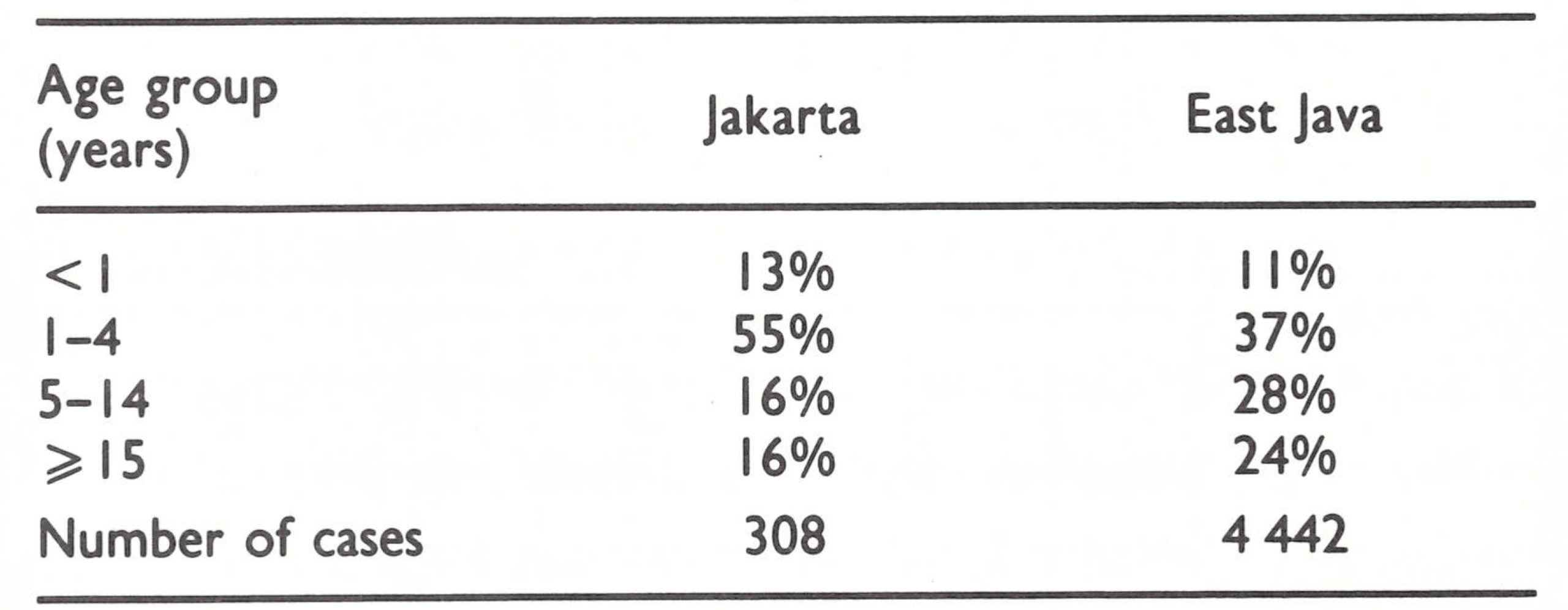
Less than one-quarter of all the children were considered to be fully susceptible to the disease. Only 807 (1 %) had facial pockmarks characteristic of smallpox. Since persons less than 15 years of age constituted approximately half the population and since only a small proportion of those older than 15 were fully susceptible, it was assumed that not more than perhaps 10-15 % of the total population were then susceptible to smallpox. Not surprisingly, at that time more than 75% of smallpox cases were reported to be occurring among children under 15 years of age (Table 13.6) and upwards of 80% of cases occurred among those without a vaccination scar.
Table 13.6: Jakarta and East Java: age distribution of cases of smallpox, 1965-1966
SMALLPOX INCIDENCE, 1963-1967
National data for smallpox prior to 1963 provide little indication as to the incidence or geographical distribution of the disease . Not only did villages and regencies fail to report to provincial authorities, but many provincial administrations submitted no reports to the national authorities. The number of cases officially recorded at the national level varied from 1000 to 10 000 during the period 1952-1962. Better data are available for the years 1963-1967, because smallpox control staff visited each of the provinces during 1968 to compile provincial data from previous years in order to obtain baseline information. In 1963, 17 431 cases were recorded, of which all but 3658 were from West Java (Table 13.7). The most complete data available pertain to the years 1965-1967, and these show a wider dispersion of smallpox throughout the central and western islands of Indonesia.
Major epidemics were reported in 2 areas during the period 1965-1967 (Fig. 13.4). In 1965, East Java reported 36 120 of the 56 359 cases recorded in Indonesia and this epidemic was followed in 1966 by one in neighbouring West Nusa Tenggara. Central and South Kalimantan experienced epidemics in 1965, which gradually subsided over the next 2 years without a planned vaccination campaign. Other provinces of Indonesia also reported significant numbers of cases, but because of inadequate reporting few conclusions can be drawn about the comparative magnitude of the smallpox problem in these areas. That reporting was seriously deficient was shown in the January 1968 survey in Java. In this survey, estimates of recent smallpox incidence were derived from the prevalence of facial pockmarks. The survey revealed that, at most, 10% of all cases were actually being reported. Thus, it was calculated that more than 100 000 cases had occurred in 1967 in Java alone. Reporting from the other islands, in which the health resources were fewer, was much less complete than in Java.
Table 13.7: Indonesia: number of reported cases of smallpox, by province, 1963-1972a
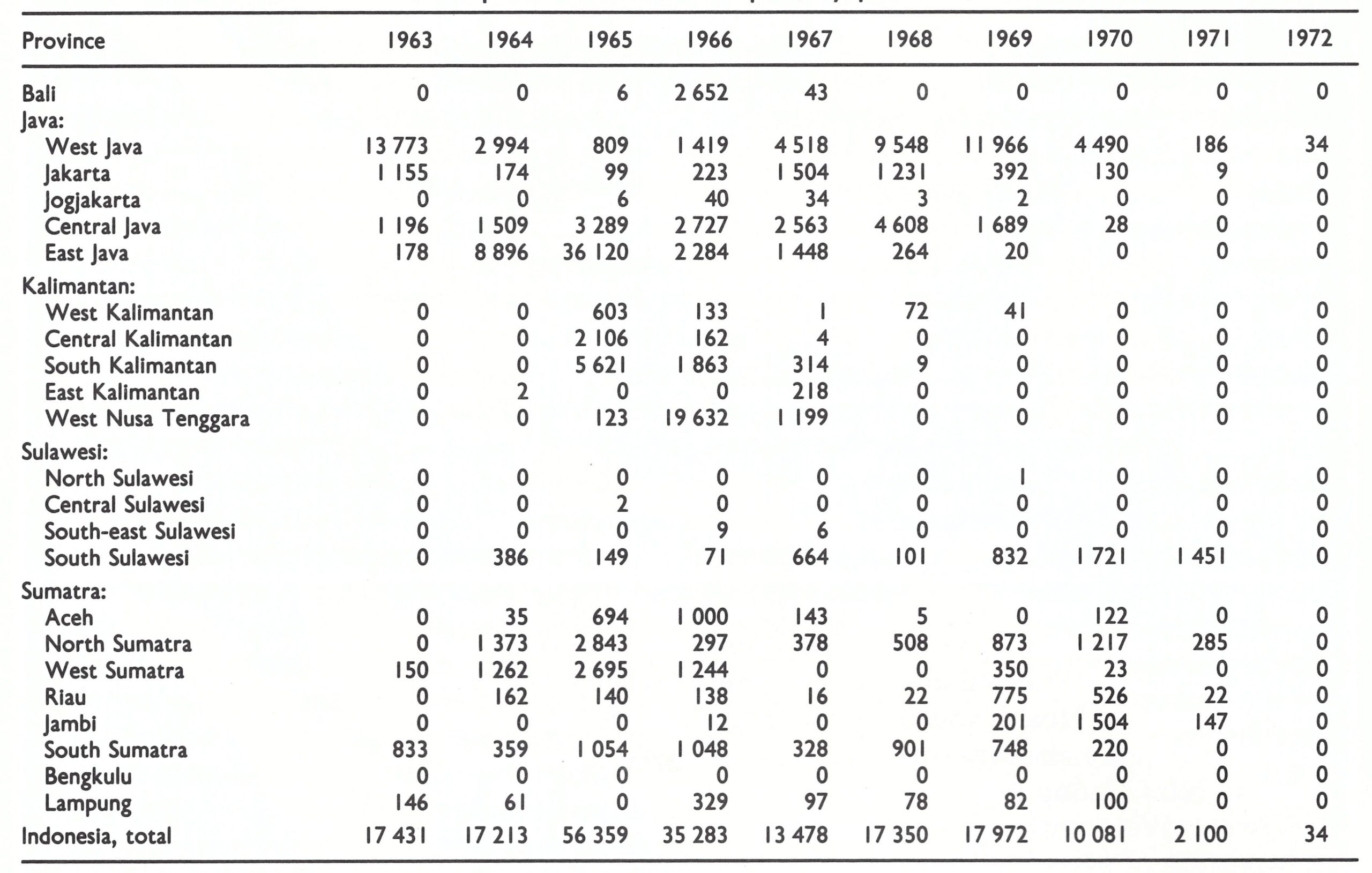
a No cases were reported from Maluku, East Nusa Tenggara or West Irlan during this period.
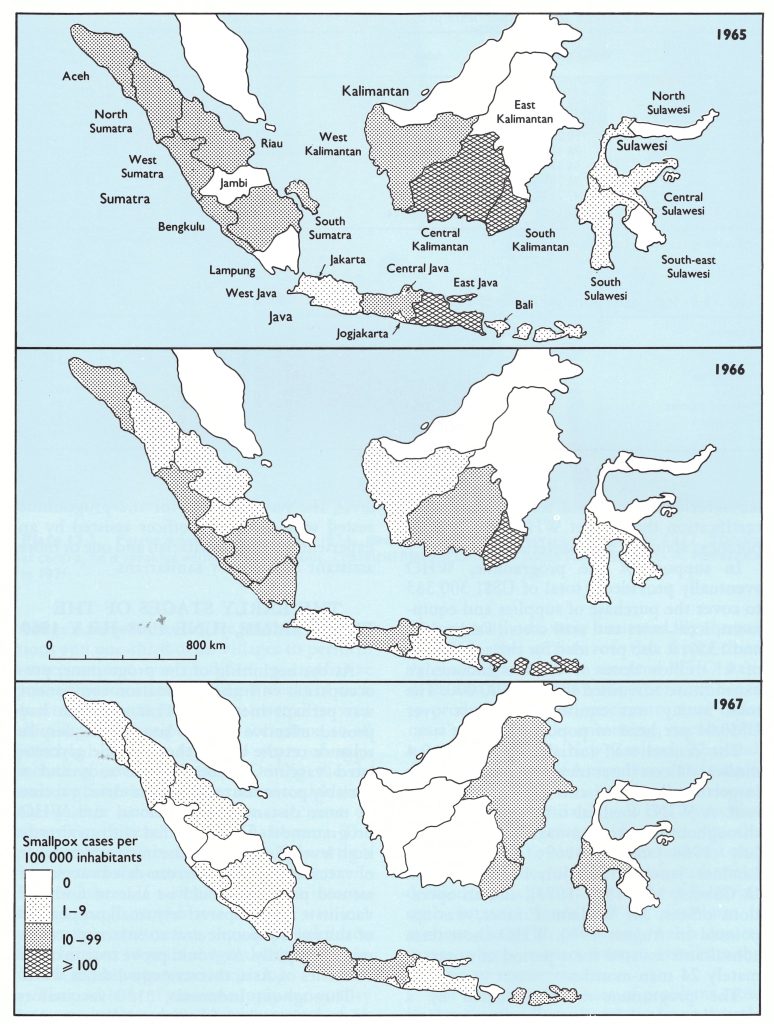
Fig. 12.2. Indonesia: number of reported cases of smallpox per 100 000 inhabitants, 1965-1967
ORGANIZATION OF THE PROGRAMME, JANUARY-JUNE 1968
Dr Sulianti lost no time in setting the eradication programme in motion. As a first step she changed a meeting on tuberculosis vaccination scheduled for February 1968 into a planning seminar for smallpox eradication. It was to be the first of a series of annual national meetings which reviewed the programme’s progress and established specific plans and targets for the succeeding year. Those attending included Dr Sulianti’s staff; senior health officials from the provinces, regencies and municipalities; directors of maternal and child health, school health and malaria control programmes; and representatives from the armed forces, the Ministry of Home Affairs and the Central Bureau of Statistics. The seminar represented a laudable effort to involve a wide range of civil and military authorities in the programme although, in fact, few of those present were to make significant contributions until late in its course.
It was decided to launch the programme in June 1968 in Java and Bali, in which 66% of the population lived, and to extend it to the outer islands a year later. Additional vaccinators would be appointed for each subdistrict (40 000-50 000 population), which would more than double the number then in the field. However, they would work only part time, as did the others, because their pay remained low. A supervisor would be appointed for each regency (500 000-1 000 000 inhabitants) and additional supervisory staff would be provided at provincial and national levels. In each of the 90 regencies and the 6 provinces, a “fire-fighting” team of 3 or 4 persons would be formed from existing staff specifically to contain outbreaks.
Because the vast majority of cases were occurring among the unvaccinated, vaccinators were instructed to concentrate on primary vaccination. The maternal and child health centres were directed to vaccinate all infants attending clinics (estimated to represent about 40% of the total number of infants) and the school health services to vaccinate all schoolchildren (corresponding to about 50% of all children of school age). The newly developed bifurcated needles and the multiple puncture technique of vaccination would be employed by all vaccinators except the members of national surveillance- cold-storage depots would be established at containment teams, who would use jet injec-national, provincial and regency levels, and tors supplied by WHO. It was agreed that only that each batch of vaccine produced by the freeze-dried vaccine would be employed, that Biofarma laboratory would be tested by WHO laboratories and released for use only after certification that it met WHO standards of potency, stability and bacterial content.
In support of the programme, WHO eventually provided a total of US$1 300 363 to cover the purchase of supplies and equipment, local costs and staff costs (Tables 13.8 and 13.9); it also provided for the acquisition of 4.1 million doses of vaccine. Indonesia’s expenditure amounted to US$3 600 000. The total outlay was equivalent to just over US$0.04 per head of population.
The central staff initially consisted of 4 medical officers (later increased to 8), 7 health inspectors (later 10) and 12 administrative staff. A WHO medical officer was assigned throughout the programme (Dr M .F. Polak, July 1968 January 1969; Dr Reinhard Lindner, January 1969 July 1971; Dr G. G. O. Cuboni, May 1971-1973), and an operations officer, Mr William Emmet, was appointed in August 1970. WHO short-term consultants assisted for a period of approximately 24 man-months.
The programme was conducted by a specially created Smallpox Eradication Unit in the Directorate of Epidemic Control under the direction of a motivated and committed physician, Dr P. A. Koswara. This unit, in turn, reported to Dr Sulianti. At the provincial level, there was a smallpox eradication programme section, also headed by a full-time medical officer. At the regency/municipality level, the responsibility for the programme rested with a medical officer assisted by an experienced senior sanitarian and one or more assistant supervisory sanitarians.
Table 13.8: WHO support for the Indonesia programme, 1967-1974 (US$)a
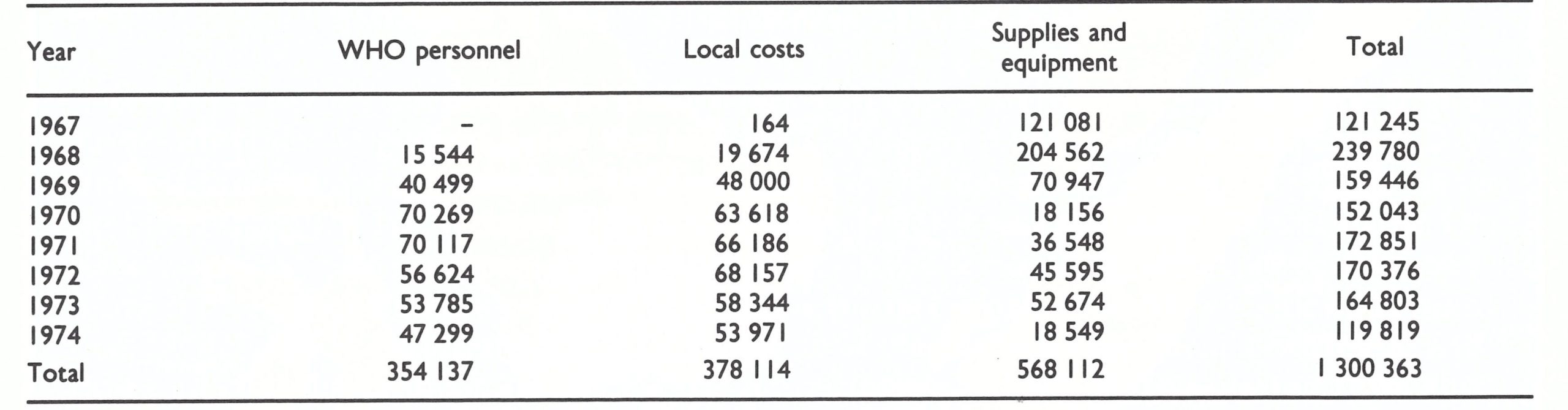
a Excluding the cost of supplies of vaccine.
Table 13.9: Indonesia : principal items of equipment provided by WHO, 1968-1971

THE EARLY STAGES OF THE PROGRAMME, JUNE 1968 JULY 1969
At the beginning of the programme, preoccupation with the vaccination component was perhaps inevitable . This approach had proved effective in the late 1930s, despite reliance on the use of thermolabile glycerolated vaccine in the main islands and a variably potent but stable room-dried vaccine in more distant areas . National and WHO programme staff believed that with an already high level of immunity, the increased number of vaccinators, using a freeze-dried vaccine of assured potency, should be able to find and vaccinate the comparatively small proportion of susceptible people and so interrupt transmission rapidly. As would prove true in other countries of Asia, this strategy did not work.
Throughout Indonesia, 3130 vaccinators—approximately 1 for each subdistrict—and 324 regency supervisors conducted the programme. On average, this amounted to 1 vaccinator for every 39 000 persons, the ratio ranging from 1 to 9000 in sparsely inhabited areas to 1 to 50 000 or more in densely populated regions. The pre-war procedure, according to which vaccinators visited each village 4 times a year to give primary vaccinations and one-third of all villages to perform revaccinations, was modified to emphasize primary vaccination. During 8 weeks of each quarter, vaccinators were instructed to visit all villages to give primary vaccination to all preschool children (up to 4 years of age), including newborn infants. During the remaining 5 weeks, they were instructed to visit one-quarter of all villages to vaccinate or revaccinate all children aged 5-14 years. The programme was modified in Bali, in which vaccination was entrusted to malaria surveillance workers. If well executed, this intensified campaign would have ensured, within 1 year, vaccinial immunity in nearly all children from birth to 14 years of age, the age group in which most cases were occurring.

Plate 13.3. Petrus Aswin Koswara (1931 – 1974), directed the national programme until April 1972. Standing at centre, he is speaking with Dr Hasan Anoez, Provincial Medical Officer in South Sulawesi, and D . A . Henderson in 1971.
The problems of vaccine supply and quality were gradually resolved over a period of 18 months. Biofarma ceased production of the liquid and room-dried vaccines and began to produce freeze-dried vaccine only. UNICEF provided additional vaccine production equipment and WHO recruited consultant assistance for the laboratory. Better methods of quality control, as well as improved production methods, were instituted. By the end of 1968, the quality of the freeze-dried vaccine began to meet accepted WHO standards and, during 1969, the laboratory began to produce sufficient vaccine to meet Indonesia’s needs . In the meantime, vaccine donated to WHO by New Zealand, Thailand, the USSR and the USA augmented the supply. National and provincial cold-storage depots were already available; WHO provided additional refrigerators for use at the regency level. To simplify procurement and distribution, the national health authorities decided to purchase all vaccine from Biofarma with national funds and to distribute it without charge to provincial health departments, which, in turn, were to distribute the vaccine to regencies.
Not surprisingly, a host of problems arose in a programme which was to be so greatly strengthened and executed in such a large population with only 6 months of preliminary planning and organization. One by one, these difficulties were resolved. To cite a few of the more important: deliveries of vehicles, bicycles and other items transported by sea were delayed by months because of customs clearance formalities; government fiscal procedures were cumbersome and payments for vaccine to Biofarma were held up, resulting in the periodic cessation of production in late 1968 and 1969; payments to staff were similarly interrupted from time to time, with a consequent suspension of work; the recording of cases and transmission of data were seriously deficient; and effective supervision at the beginning of the programme was minimal. All these problems had to be dealt with more or less simultaneously and all persisted to some degree or recurred throughout most of the programme.
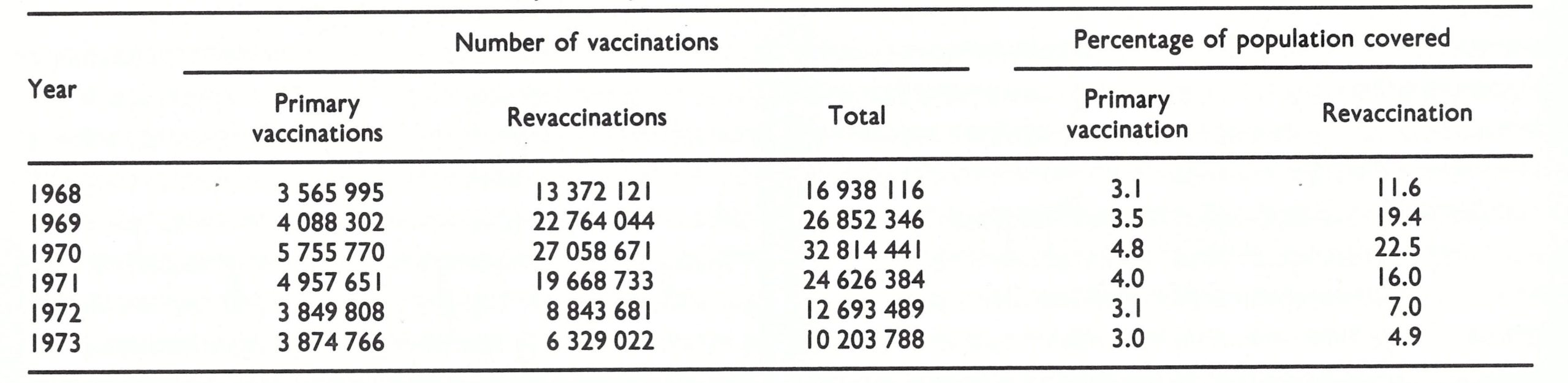
For the vaccination campaign, it was decided to establish an annual target for primary vaccinations equivalent to 6% of the population and one for revaccinations equivalent to 30% of the population . It was an unrealistic expectation, given that the vaccinators worked only part time and that the supervision and planning of vaccinator tour schedules were marred by lack of experience. Vaccinators on average performed only 20-80 vaccinations per day, of which between 2 and 20 were primary vaccinations. The programme never met its targets, although it began to approach them in 1970 (Table 13.10) . A repeat stratified cluster sample survey in June 1969, similar to that performed in January 1968, showed no significant change in the proportion of susceptible persons (Wkly epidem. rec., 1969c).
Table 13.10: Indonesia : number of primary vaccinations and revaccinations, 1968-1973
The plan had called for “fire-fighting teams” at regency level to contain outbreaks, but few of the regency teams functioned well—and most of them not at all—because of lack of interest and motivation. Vaccination to control outbreaks was neither thorough nor systematic; the sources of cases were not traced, and few of the locales of outbreaks were revisited to ensure that transmission had been stopped.
Indonesia, so densely populated, had seemed to be an ideal place to use jet injectors in outbreak containment. The injectors were provided by WHO and, in August 1968, a consultant was recruited to train special vaccination teams in their use and maintenance. As was true in many other areas, the concept was attractive in theory but disappointing in practice. Except in urban areas, the population was not accustomed to gathering in large numbers at collecting points, and unless they did so the considerable capacity of the injectors could not be realized. Maintenance and repair of the injectors and the logistics of providing a flow of spare parts proved to be formidable obstacles. Within a year, the jet injectors had been abandoned in favour of bifurcated needles . Not only did the latter yield far better results in comparison with the old vaccinostyle (as was revealed in a short trial in Ciloto, West Java) but they also proved to be considerably more economical in the use of vaccine. Beginning in March 1969, the bifurcated needle was accepted as the standard equipment for vaccination in the programme. Improvement in the supervision and execution of the programme was needed at all levels and, to effect this, 13 “advance teams” (1 each in Jakarta, Jogjakarta and Bali, 2 in East Java and 4 each in West and Central Java) were established in January 1969. These teams provided a critical link in supervision between the national programme directorate and the regencies and were ultimately instrumental in instituting an effective surveillance-containment programme . They were given a month of special training and sent to the field. Each team was provided with a WHO vehicle and was headed by a physician who was able to work full time in the programme, thanks to a salary subsidy paid by WHO. The initial plan called for the teams to spend two-thirds of their time in surveillance and containment activities and one-third in in improving the supervision of vaccinators.
Despite the chaotic beginning and the numerous problems, remarkable progress was recorded in some provinces (Table 13 .11). East Java had experienced major epidemics in 1964 and 1965 and, in consequence, had conducted mass campaigns. However, the vaccination survey of December 1967-January 1968 (see Table 13.5) showed that vaccinial immunity was no better than in West Java and far lower than in Central Java despite the mass campaigns. In July 1968 a dynamic Provincial Director of Communicable Disease Control, Dr Bahrawi Wongsokusomo, and his assistant, Dr Witjaksono Hardjotanojo, took charge of the programme in East Java and vowed that they would interrupt transmission before January 1969. Vaccination activities were intensified, but—more important—any outbreaks found were energetically contained. During the last 6 months of 1968, only 133 cases were detected in the entire province. Between January and June 1969, only 3 outbreaks occurred, each of which could be traced to importations from Central Java; all were well contained after discovery. It was a remarkable achievement, accomplished almost wholly with provincial resources.
In Jakarta, under the leadership of Dr Guno Wiseso, special teams equipped with jet injectors demonstrated the efficacy of the outbreak-containment strategy. During a 3-month period, they investigated and contained 73 outbreaks, in which 217 cases had been reported (Wkly epidem. rec., 1970a). The teams searched for additional cases, endeavoured to find the origins of the outbreaks and vaccinated the inhabitants of the affected administrative units (about 200 persons in each unit), as well as the people living in the 4 surrounding units. During these activities they discovered an additional 215 cases and vaccinated some 73 000 persons. A subsequent assessment revealed that smallpox transmission had ceased within 2 weeks of containment in two-thirds of the outbreaks (Table 13.12). Although these results would be considered poor by later standards, it was clear that outbreaks could, in fact, be quickly stopped.
No smallpox cases were reported in Bali or in the islands to the east after the programme began, and in February 1969 Jogjakarta recorded its last cases. By June 1969, smallpox in Central Java was being reported from only 4 of 35 regencies but West Java continued to report nearly 1000 cases per month. Meanwhile, the complement of vaccinators and supervisors in Java steadily increased and by June had more or less reached the numbers planned (Table 13.13). In Kalimantan, Sulawesi and Sumatra, the programmes did not officially begin until July 1969, and thus all reports were considered to be suspect.
The number of cases reported in Indonesia between January and June 1969 amounted to 8789, a total not significantly different from the 8847 cases recorded during the same period in 1968. Although the staff believed that there was more complete reporting of cases, it was impossible to measure the extent of improvement. What was certain, however, was that reporting was still incomplete. The reporting of cases to the regency medical officer was the responsibility of village chiefs, but many chiefs completely neglected this task, even though they were aware that cases were occurring. Moreover, some regencies failed to report to the provinces, or, if they did, the reports were greatly delayed. In June, reports from almost one-quarter of all provinces in Java and Bali were overdue by a month or more. Reporting from other provinces was even more delayed and incomplete.
When the programme began, plans had been made for its assessment by a WHOIndonesia team one year later. In June 1969, this was undertaken and recommendations were developed. The team was sharply polarized on the issue of mass vaccination. One group maintained that, with vaccinial immunity so high, the mass vaccination campaign could be said to have been completed already and that all efforts should be directed to surveillance and containment. A second group argued for a special campaign to move rapidly and systematically throughout the country to vaccinate the now very small proportion of people who had no vaccination scars.
A compromise was reached and the teams recommended that: (1) special programmes should be mounted to deal with the backlog of unvaccinated children under 15 years of age in Jakarta and West and Central Java (the number was estimated to be 3.3 million, or 16.6% of a population of 19.9 million children), and (2) surveillance should be strengthened through improved reporting by village chiefs and other health staff, and more active outbreak containment by the special “fire-fighting” and advance teams. It was recognized that the backlog vaccination-campaigns would tax, and perhaps overstrain, available government resources, but the campaign was accepted as a component of the strategy.
Table 13.11: Indonesia: number of reported cases of smallpox by province and month, 1969a
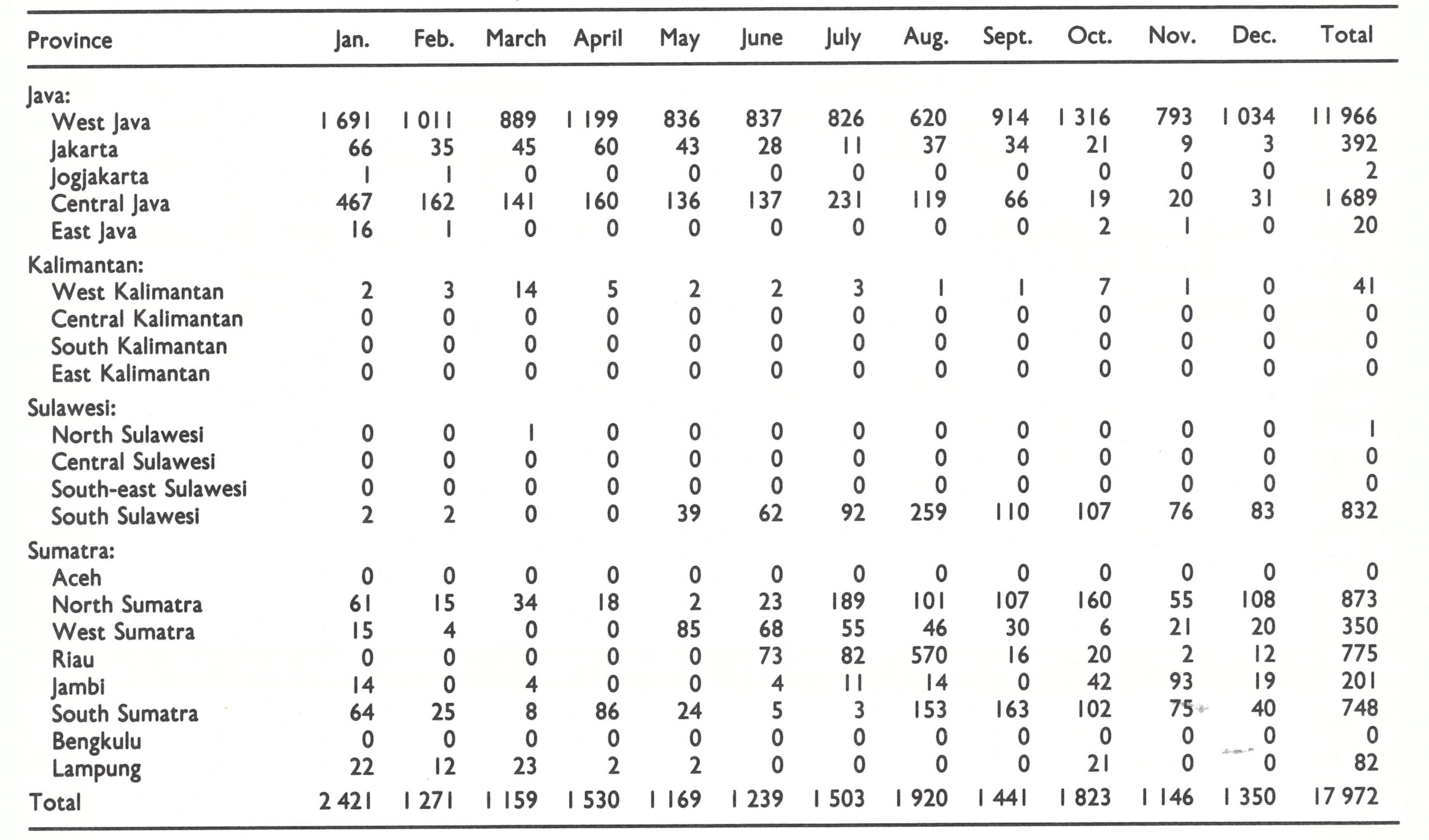
aNo cases were reported in Maluku, Bali, Nusa Tenggara, or West Irian during this period.
Table 13.12: Jakarta : number of weeks after containment in which new cases were detected, 1968

Table 13.13: Java: population and number of vaccination staff and supervisors, June 1969
THE STRATEGY CHANGES, JULY 1969
The resources available did not permit the implementation of backlog vaccination campaigns throughout the whole of Java, and so priorities were defined . In East Java and the islands to the east, in which transmission had been interrupted, efforts were to be directed solely to the early detection and containment of imported cases. In Central Java, lying immediately to the west, smallpox incidence was declining and prospects for the early interruption of transmission appeared good. Thus, the decision was made for vaccination teams (called “backlog-fighting teams”) to begin work in the eastern regencies of Central Java and to move westward in the expectation that smallpox would progressively disappear in an east-to-west direction. Given the probability that the situation in West Java would soon follow the same course, backlog-fighting teams were scheduled to commence operations in the province’s 7 easternmost regencies.
As the backlog-fighting teams began vaccination in Central Java, the 4 provincial surveillance teams started work in the northwest, where smallpox incidence was the highest. Directed by a capable epidemiologist, Dr P. R. Arbani, these teams concentrated entirely on case detection and outbreak containment. Gradually they extended the scope of their operations to include the whole province. The number of cases in Central Java declined dramatically (Fig. 13.5). In December only 31 cases were detected, and by May 1970 the last case had occurred. The advance teams had performed only 54 000 containment vaccinations, a small fraction of the 5 million vaccinations which were being given annually in the province.
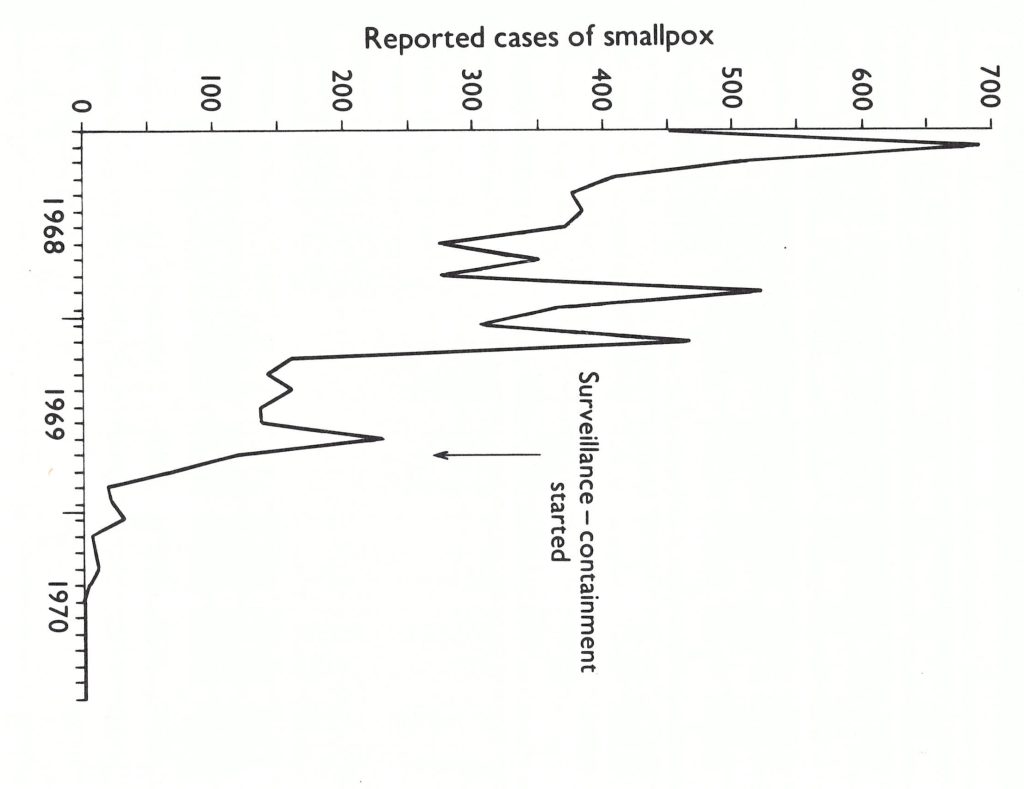
Fig. 13.5. Central Java: number of reported cases of smallpox by month 1968-1970.
West Java presented a more formidable problem. Provincial supervision had been inadequate for many years and this was reflected in the low levels of vaccinial immunity throughout the province. During the first half of 1969, an average of almost 250 cases had been reported weekly in a province whose notification system was the poor est in Java. In July, 4 special teams, each consisting of 5 vaccinators and a team leader, were recruited for each of the 7 regencies bordering on Central Java (Koswara in WHO/SE/71.30). As in Central Java, the teams proceeded house by house and village by village, performing primary vaccinations and containing any outbreaks that were found.
By October 1969, it became apparent that smallpox transmission was continuing in West Java, even in regencies in which backlog fighting had been completed. Although the teams were instructed to intensify surveillance-containment activities, few did so. In one regency, Tjirebon, in which no such activities had been conducted (Wkly epidem . rec., 1970a), a WHO adviser was assigned to undertake surveillance-containment activities only. National staff supervised combined surveillance-containment and vaccination programmes in 3 other regencies, including Bandung, in which smallpox incidence remained high. Two months later, in December, a main focus of smallpox in the province was found to be yet another regency, Bogor, in which so far no work was in progress. Resources were all but exhausted and only a single team could be assigned there to conduct a surveillance-containment programme.
Three different types of programme had therefore developed in an unplanned operational experiment: (1) in Tjirebon, backlog vaccination was followed by an intensive surveillance-containment programme; (2) in Bandung, a combined backlog vaccination and containment programme was directed by national supervisors; (3) in Bogor, a surveillance-containment programme only was conducted. The results of this experiment were to decide the subsequent strategy of the programme in Indonesia.
Plate 13.5. Reinhard R.Lindner (b.1926) was the WHO smallpox adviser to the Indonesian programme from 1969 to 1971.
Tjirebon Regency
The backlog vaccination operation had begun in July 1969 and ended 18 weeks later. During 2025 man-days, the teams visited 188 287 households in 267 villages. In all, 208 smallpox cases were discovered in 24 villages. On completion of the work, a sample survey showed that the proportion of unprotected children below 1 year of age had decreased dramatically, from 83% to 26%; of those aged 1-4 years, from 36% to 11%; and of those aged 5-14 years, from 3% to 2%. The illusion of a highly successful programme was shattered when just 2 days after the programme had been completed, 12 mobile teams from other provinces undertook a 2-day training exercise in Tjirebon. They discovered E that in 7 infected villages transmission was still continuing. By tracing the sources of infection, an additional 118 cases and 3 undetected outbreaks were discovered.
Greater efforts were obviously needed, and a WHO consultant, Mr Michael O’ Regan, was assigned in mid-November. On arrival, he found a frustrated but hard-working staff with a disorganized record system and no dayto-day operational programme. In the yaws and leprosy programmes in which Mr O’ Regan had worked, methods had been developed for the systematic search for cases throughout extensive areas. Applying similar principles in Tjirebon, he obtained reliable maps and lists of villages from the army and, with regency staff, planned a programme consisting of a systematic village-by-village search for cases and house-to-house searches when outbreaks were found. The basic work was performed by 7 search teams each composed of 2 men on bicycles, their work being supervised by 2 search teams with vehicles. In every village, the programme was explained to the village leader and assurances were given that, should he report a case, a team would come to the village within 24 hours. Outbreaks, when discovered, were contained and the locality concerned was revisited weekly until 4 weeks after the last case had occurred. Identification of the source of each outbreak permitted the discovery of other, unreported outbreaks. Each night the staff met, reported their findings and planned the following day’s work. The initial search revealed that, as at 1 December 1970, there were 31 villages with active cases, but within 2 months transmission had been interrupted (Fig. 13.6). Cases continued to occur as a result of importations from other regencies but these were quickly contained. The Tjirebon programme was the first in the Intensified Programme in which teams undertook a systematic area-wide search for cases without simultaneously performing vaccinations. The technique was later to be widely applied throughout Indonesia and was to prove vital in interrupting transmission in the Indian subcontinent.
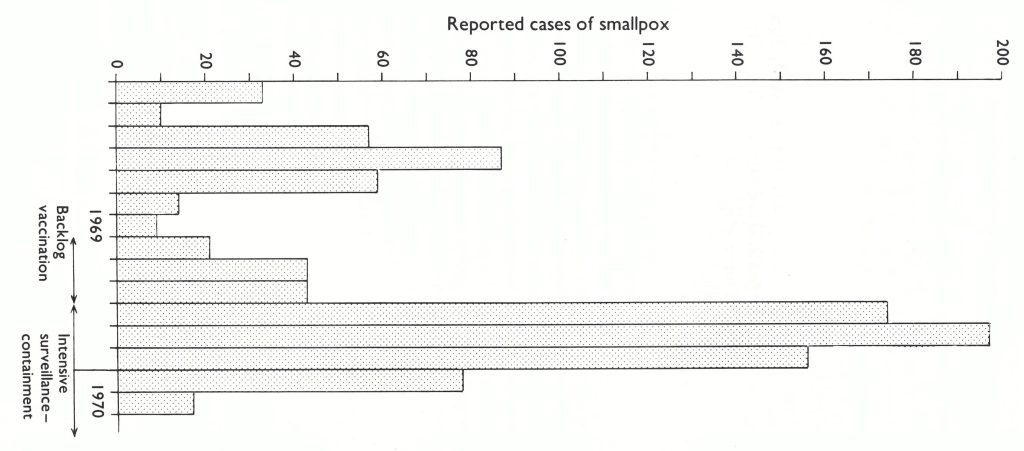
Fig. 13.6. Tjirebon Regency: number of reported cases of smallpox, by 4-week intervals. 1969-1970. The last interval in 1970 includes 6 important and ii Delayed reports of inactive cases.
Bandung Regency
In Bandung, the combined surveillance containment and backlog-fighting operation under the supervision of national staff had begun early in November 1968 and ended 26 weeks later . The teams visited 401 490 households in 242 villages and performed 163 194 primary vaccinations ; 74 outbreaks with 565 cases were detected and contained . Altogether 4020 man-days were required. The resources needed to interrupt transmission were even greater than those expended in the Tjirebon programme.
Bogor Regency
A single surveillance team with a vehicle had been assigned to Bogor in December 1969, after a national team investigating a reported outbreak discovered that not 1 but 18 out of 24 subdistricts were infected. Because no additional resources could be spared, the team continued to work alone. During 42 weeks, active search and containment detected 2101 cases in 101 villages, but transmission was completely interrupted; only 15 175 containment vaccinations were performed. Time was required to interrupt transmission in this densely populated area, but it was achieved at a cost of only 1802 mandays.
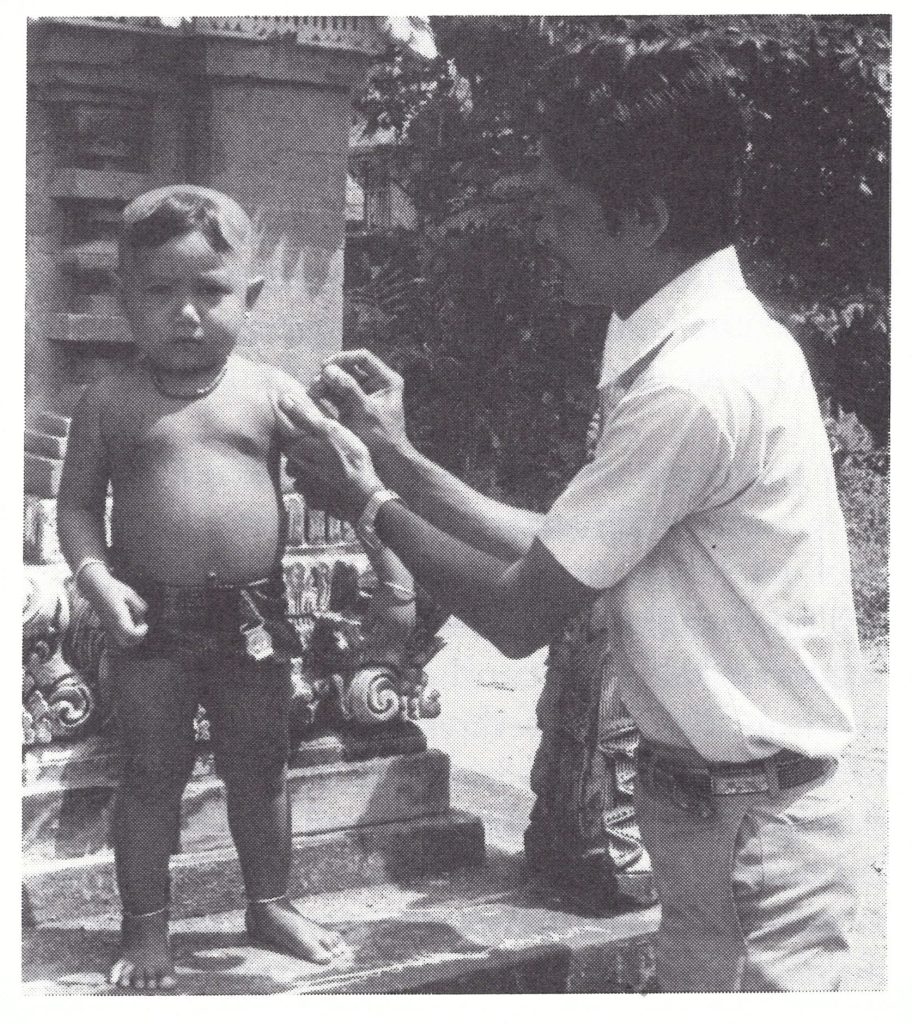
Plate 13.6. Vaccinators in Indonesia moved from house to house, concentrating their efforts on young children and infants who had not been vaccinated previously. For this work, the bifurcated needle was especially valuable.
Factors Affecting Transmission
In October 1970, after transmission had been interrupted in the 3 regencies, surveys were conducted to determine comparative levels of vaccinial immunity (Table 13.14). Smallpox transmission had been rapidly interrupted in Tjirebon once surveillancecontainment measures had been effectively applied, but vaccinial immunity was already high there. Success had also been achieved in Bandung with improved supervision but at a considerable cost in resources. Bogor presented a contrast. There, transmission had also been successfully interrupted with surveillance-containment only, although 2-3 times as many unprotected children remained. The proportion that was unprotected was almost as high in the infected areas—in which containment vaccination had been extensive—as it was in the less endemic areas.
Everyone involved in the programme was surprised by the tenacity of smallpox in these and other regencies of Java despite comparatively high levels of vaccinial immunity and intensive surveillance-containment measures. It was a contrast to the situation in Brazil and western Africa, in which surveillance and containment had quickly stopped transmission, even in less well vaccinated populations (see Chapters 12 and 17). Indonesia, demographically and socially, was different in several respects (Wkly epidem. rec.,1970a). Population density in Java was one of the highest in the world and, traditionally, families carried children who were sick from house to house to visit relatives. The tradition of isolating cases, so often observed in other countries, was uncommon. Thus, many more susceptible persons, on average, were exposed to smallpox cases than in most other areas. Because of high levels of vaccinial immunity and the greater frequency of exposure of susceptible persons, the age distribution of cases was different in Java from the corresponding distributions in Brazil and Pakistan, for example (Table 13.15).
Table 13.14: Tjirebon, Bandung and Bogor Regencies : percentage of children unprotected by vaccination, by age group, October 1970a
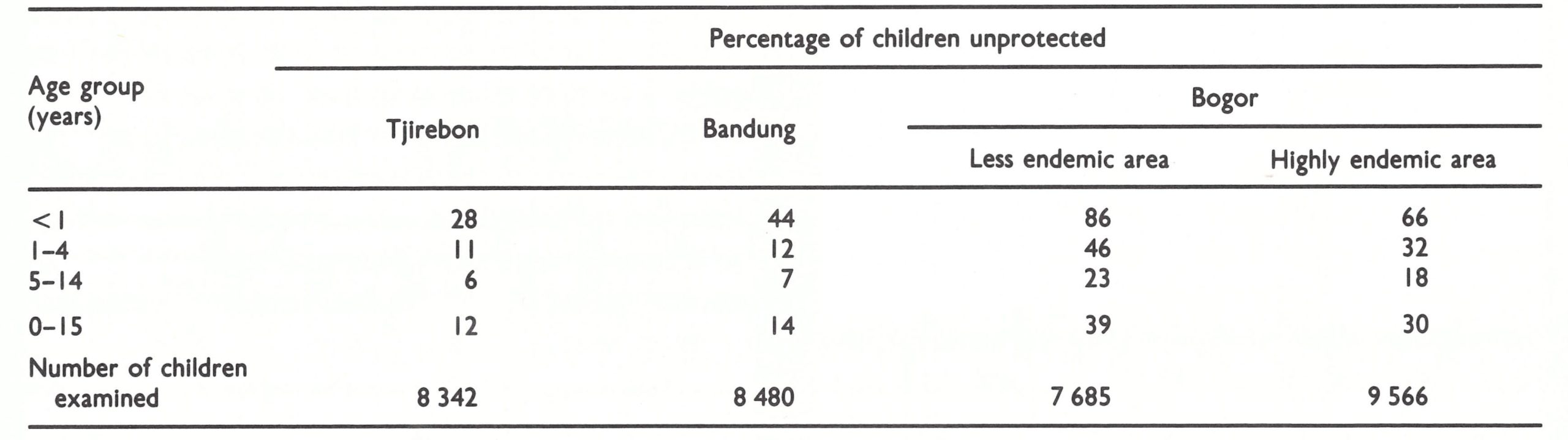
aBased on Koswara
Table 13.15: Comparative percentage distribution of smallpox cases, by age group, 1969a
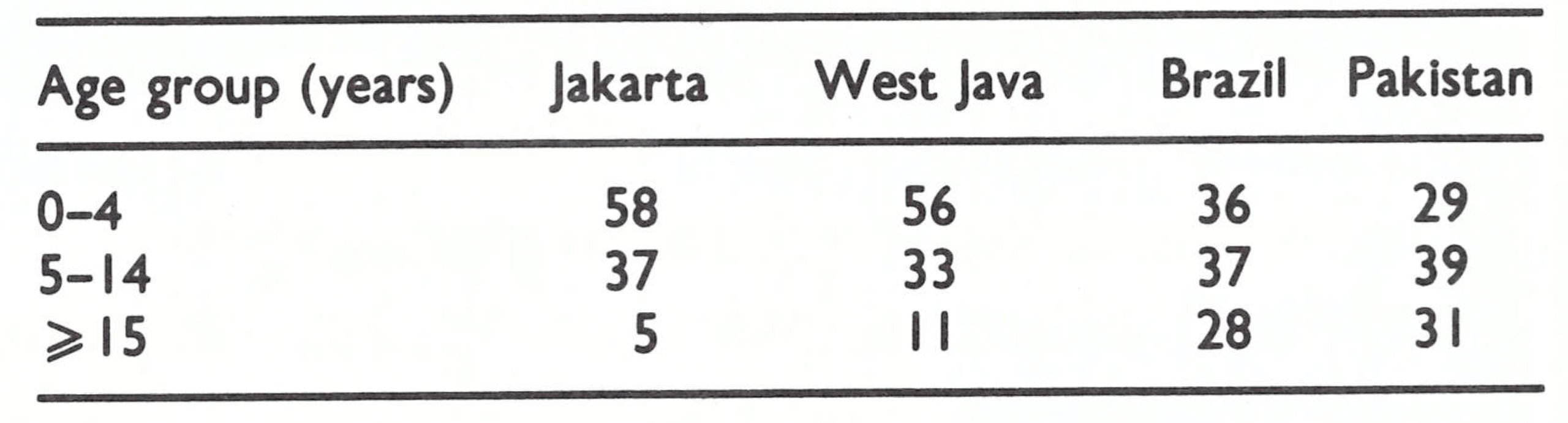
aBased on Hartohusodo (in WHO/SE/71.30).
In Java, more than half of all cases were found in children under 5 years of age; few cases occurred in adults. In Africa, South America and Asia, cases were more evenly distributed among all age groups.
Another factor of importance in smallpox transmission in Indonesia was climatic: smallpox was readily transmitted throughout the year (Fig. 13.7). Indonesia, located between 5°N and 5°S of the equator, did not have the wide seasonal fluctuations in transmission which were characteristic of countries such as Brazil, India and Pakistan (Wkly epidem. rec., 1969a) (see Chapter 4). In these countries, in which transmission rates declined sharply during the summer and early autumn months, many chains of transmission terminated spontaneously and the containment of outbreaks during these periods was comparatively simple. In Indonesia no such circumstances obtained.
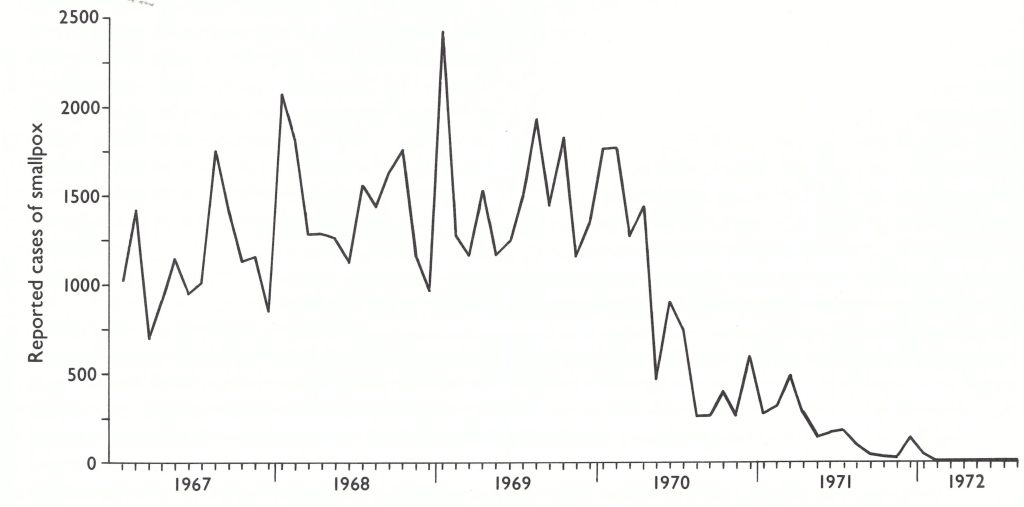
Fig. 13.7. Indonesia : number of reported cases of smallpox, by month, 1967-1972.
Smallpox Transmission in a Well-Vaccinated Area
An outbreak in Passar Minggu (population, 14 376), a densely populated section of Jakarta City, vividly illustrated the ability of smallpox to continue to be transmitted even in well-vaccinated areas. In August 1970, the investigation of a death due to smallpox led to the discovery of a chain of infection involving 20 cases extending over a period of 21 weeks (see the figure below). A scar survey in the area revealed that only 2% of children between 5 and 14 years of age were unvaccinated (see table). Overall, the proportion of susceptible persons in the area was only about 6%, almost none of whom were adults.
Passar Minggu: Vaccination Status of Children and Cases of Smallpox (Emmet in WHO/SE/71.30)
| Age group (years) | Percentage unvaccinated | Number of cases |
|---|---|---|
| <1 | 61% | 2 |
| 1–4 | 20% | 11 |
| 5–14 | 2% | 5 |
| ≥15 | – | 2 |
The cases spread from one house to the next, usually over a distance of no more than 300 metres (see illustration) . Nine of the cases resulted from intrafamilial transmission ; the remainder occurred through the visits of susceptible children to infected households.
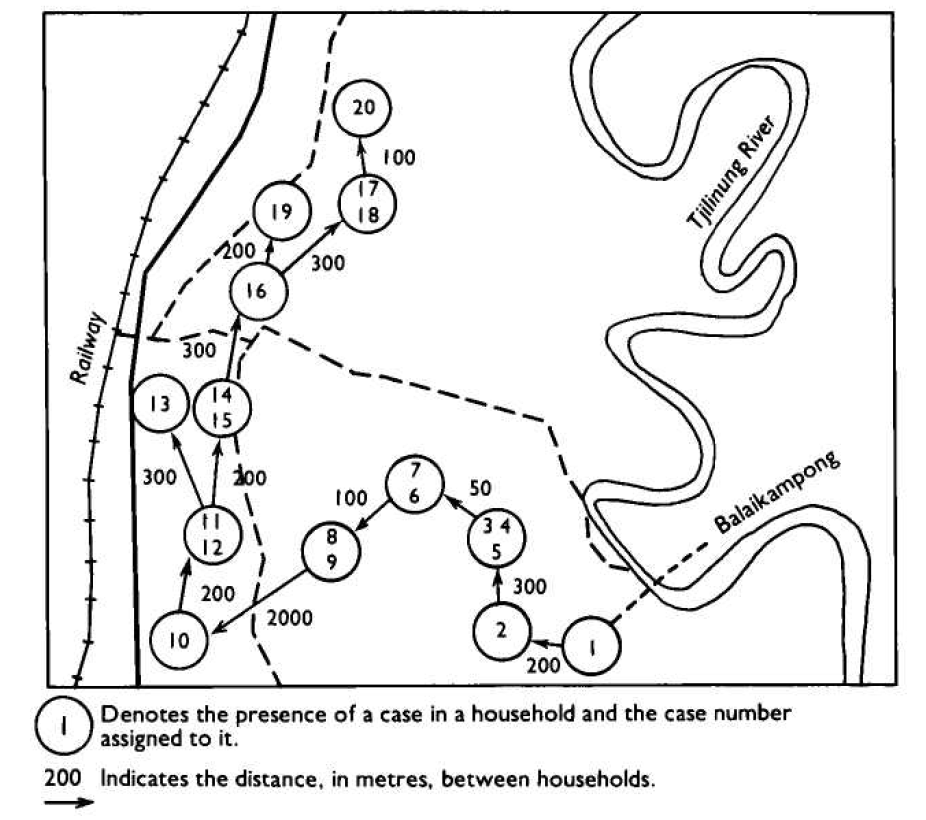
Similiar occurrences of slowly spreading epidemic smallpox in well-vaccinated populations were observed throughout the rural areas of West Java and, to some extent, of Central Java. In the other endemic areas of Indonesia, non of those which experienced smallpox after 1968 was so densely populated and smallpox there was far more easily contained.
THE SURVEILLANCE-CONTAINMENT STRATEGY BECOMES
Despite the problems of the backlog vaccination campaign and the diversion of resources from surveillance-containment activities, progress was made in the “east-to west” strategy in Java (Fig. 13.8). By February 1970, endemic smallpox remained solely in West Java. In Central Java, during 1970, only 28 cases were detected, all of which represented outbreaks due to importations. Meanwhile, programme activities were extended to the outer island.

Fig. 13.8. Java : number of reported cases of smallpox, by regency, January-february 1969 and January-February 1970.
Reporting, which had been so incomplete and greatly delayed, improved markedly in 1970 following the assignment of a full-time medical officer, Dr A. Karyadi, to assume responsibility for surveillance and data collection. Simplified standardized reporting forms were adopted for the weekly reports and a goal was set for the receipt of reports with a delay of no more than 2 weeks from provinces in Java and of no more than 3 weeks from the outer islands (Karyadi in WHO/SE/71 .30). Defaulting provinces were repeatedly contacted by letter, telegram, messenger and personal visits to promote compliance. Cooperation was sought from civil authorities as well. In the absence of an adequate postal service, many methods were utilized for the transmission of provincial reports, including couriers such as bus drivers, businessmen, special messengers and military personnel. Provincial authorities, with assistance from the smallpox eradication staff, sought to obtain promptly the weekly reports from regency medical officers and health units. To simplify reporting, the data requested were limited to the names of infected villages and subdistricts, the numbers of cases and deaths, the ages of cases, and the source of infection of each outbreak. Beginning in May 1970, a national weekly surveillance report was prepared which documented smallpox incidence and progress in the campaign. This was distributed to health authorities throughout Indonesia. In September 1970, Dr Karyadi was able to report that 95% of weekly reports were being received from provinces in Sumatra and Sulawesi within 3 weeks. Just one year previously, only about half as many reports were being received, and then with delays of up to 21 weeks. An increasing number of cases began to be reported from Sumatra, reflecting better notification (Table 13.16). Despite improved reporting, the number of provinces reporting cases began to fall drastically as from the beginning of December 1970 (Fig. 13.9).
Table 13.16: Indonesia : number of reported cases of smallpox, by province and month, 1970a
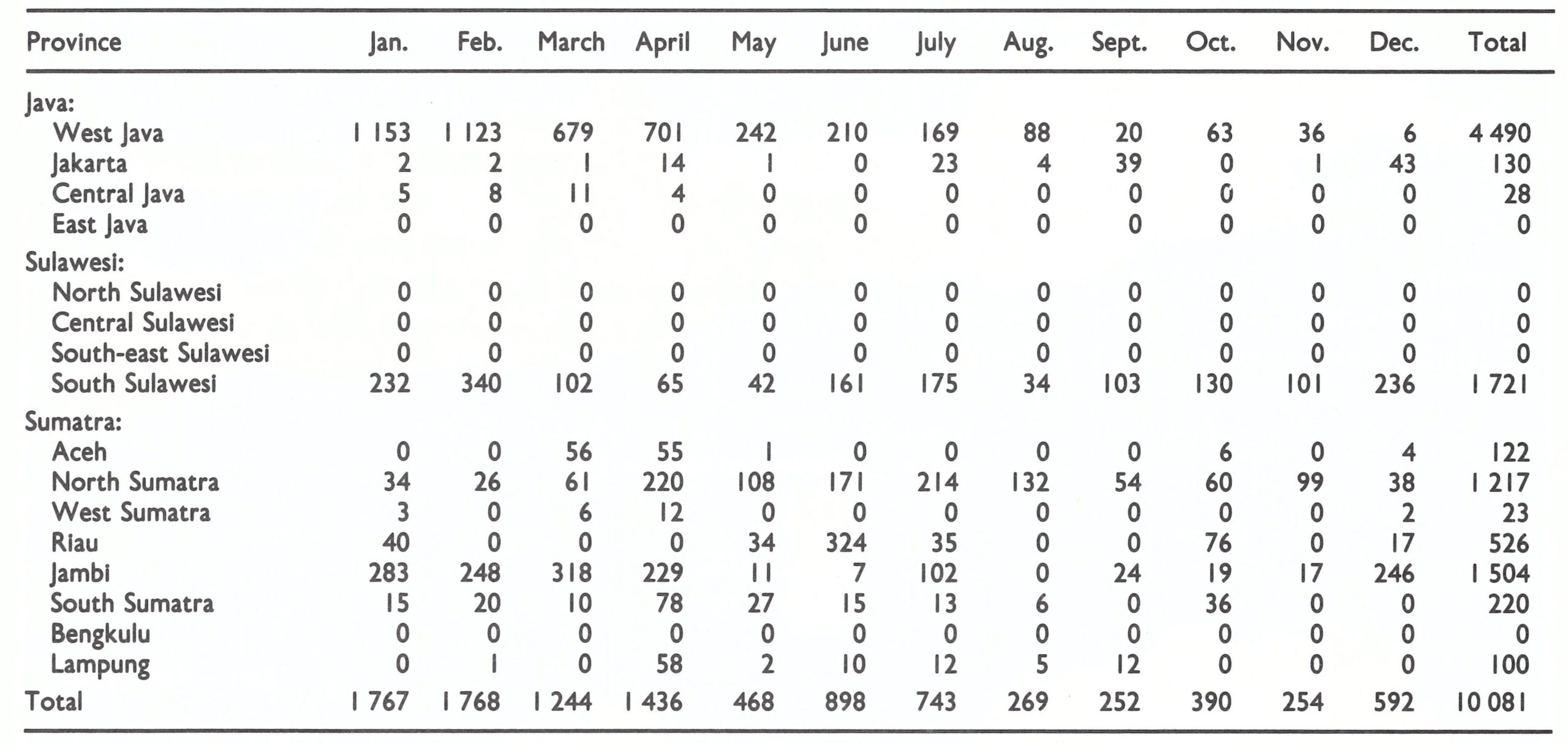
aNo cases were reported in Maluku, Kalimantan, Ball, Nusa Tenggara, West Irian or Jogjakarta during this period.
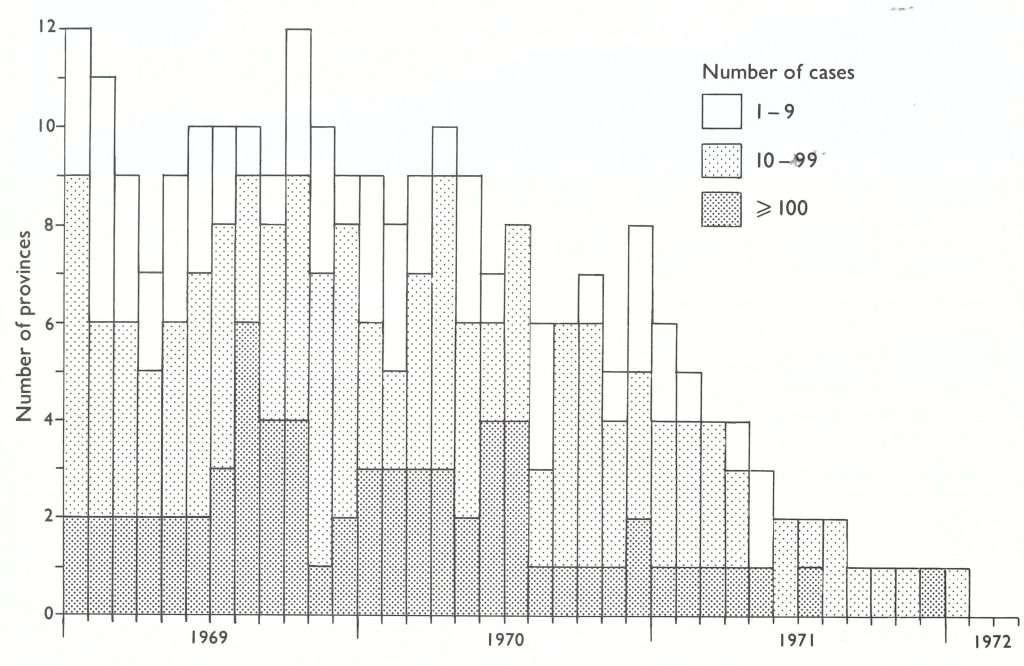
Fig. 13.9. Indonesia: number of provinces reporting cases of smallpox, by month, 1969 -1972.
In West Java, 8 mobile surveillance-containment teams worked with regency teams in carrying out active search operations and outbreak containment. As the year progressed, area vaccinators devoted less time to routine vaccination and more to systematic searches to detect cases and to contain outbreaks, as was done in Tjirebon. Initially, vaccinators were requested to search house by house, but because of the small numbers of vaccinators available, they were subsequently asked to contact specific persons and the staff of various facilities who would be the most knowledgeable regarding the existence of smallpox cases: (1) health units such as clinics, hospitals and aid posts; (2) civil officials, notably village chiefs, who in Indonesia had considerable authority in their designated areas; and (3) schoolchildren and teachers. Maps were prepared for each area, showing the principal sites and persons to be visited. A tour schedule was established to ensure that each was visited at least once a month. It was during these operations in West Java that the concept arose of printing smallpox recognition cards, depicting in colour a case of smallpox, which could be shown to those being contacted. This idea, which was proposed by Indonesian field staff to WHO regional office and Headquarters staff, was adopted and eventually tens of thousands of such cards were printed and distributed widely in Indonesia and other endemic countries throughout the world (see Chapter 10).
Containment activities were ever more rigorously defined and performed. In each outbreak, the “fire-fighting” or advance teams ensured that patients were isolated in their houses; the names of all villagers were recorded and everybody was vaccinated; the source of infection was identified and investigated; and the teams remained in the village at least overnight to ensure more complete vaccination of those working in the fields or absent during the day at the market or in school.
The Development and Use of the WHO Smallpox Recognition Card
Events which led to the development of the WHO smallpox recognition card and the use of schools in the search for cases in Indonesia occurred in Bandung. Among the many vaccinators engaged in search activities, there was one who recorded exceptional success in detecting outbreaks. Supervisors noted that, paradoxically, this vaccinator was considered to be one of the laziest workers—the last to leave for the field and the first to return home. When asked how he was so successful, he admitted that instead of visiting all the houses in a village, as instructed, he was visiting only the schools. There he showed children and teachers pictures of smallpox cases which appeared in a WHO teaching folder on smallpox diagnosis that had been prepared for Africa. Numerous case notifications were obtained with the minimum effort.
The teaching folder contained many different pictures of smallpox in African children. The photographs were small and the smallpox rash on a black skin appeared to differ somewhat from the rash on the skin of Indonesians, which was much lighter in colour. Nevertheless, most children had recognized the disease. Programme staff suggested the preparation of a single large picture of an Asian child with smallpox for use as a recognition card. Thus, the WHO smallpox recognition card was first prepared, encased in plastic for durability, and widely distributed around the world.
STRENGTHENING OF PROGRAMMES IN THE OUTER ISLANDS, 1970
Until 1970, resources and energies were principally directed to the containment of smallpox in the heavily populated island of Java. With the number of cases declining rapidly in Java during 1970 (from 1160 in January to 210 in June and to 49 in December) additional resources could be diverted to the two outer islands still harbouring smallpox—Sumatra and Sulawesi.
Sumatra had the higher priority because of the extensive inter-island boat traffic with Java. The programme in Sumatra had begun in July 1969 with an intensified vaccination campaign conducted by 567 vaccinators and 73 supervisors. As in Java, this had little effect on smallpox incidence. During 1970, more resources were made available to the programme (Wkly epidem . rec.,1970d), notably transport and assistance from national campaign staff, and the strategy shifted from intensive vaccination to surveillance-containment. Smallpox spread less rapidly in the more sparsely populated Sumatra and successful containment was easier, but this advantage was counterbalanced by a less-developed health structure and poorer supervision. In Sumatra, priority was given to the southern provinces, those nearest Java, to minimize the risk of importations. In October 1970, South Sumatra recorded its last cases, but the northern provinces (North Sumatra, Jambi and Riau) did not become smallpox-free until August 1971.
Sulawesi also began its programme in July 1969, with 355 area vaccinators and 38 supervisors. Endemic smallpox, however, was found only in South Sulawesi (population, of 5 million). Progress was slow: the rugged mountainous terrain made travel difficult; communication with villagers was a problem because 15 different dialects were spoken there; and the civil and health infrastructure, after prolonged and devastating civil disturbances, was less developed than in Sumatra or Java. The interruption of transmission in Sulawesi was to require the best skills of experienced national and WHO staff and the most effective application of now well-defined techniques for case search and outbreak containment.
Only 59 vaccination staff worked in South Sulawesi—less than half the number planned. Throughout 1970 comparatively little progress was made. However, early in 1971, with smallpox transmission all but interrupted in Java and with incidence rapidly diminishing throughout Sumatra, senior national staff and WHO advisers transferred to Sulawesi, and additional automobiles, motorcycles and bicycles were assigned to the programme. The WHO smallpox recognition card began to be used in contacts with schools and civil authorities. In March 1971, a planned programme of meetings with village chiefs and other civil administrators was instituted in order to acquaint them fully with the programme and to solicit their help in the prompt reporting of suspected cases. Many conscientiously fulfilled this responsibility through special search programmes which they independently organized. Isolation of patients in their houses, containment vaccination, both by day and by night, search for the sources of outbreaks and identification of exposed individuals who had left infected villages were more rigorously executed. With improved surveillance and containment measures and heroic efforts by national and WHO staff, smallpox transmission came to an end in South Sulawesi in November 1971 (Table 13.17).

Plate 13.7. Schoolchildren parade in support of the national smallpox eradication programme in South Sulawesi, Indonesia.
Table 13.17: Indonesia : number of reported cases of smallpox, by province and month, 1971a
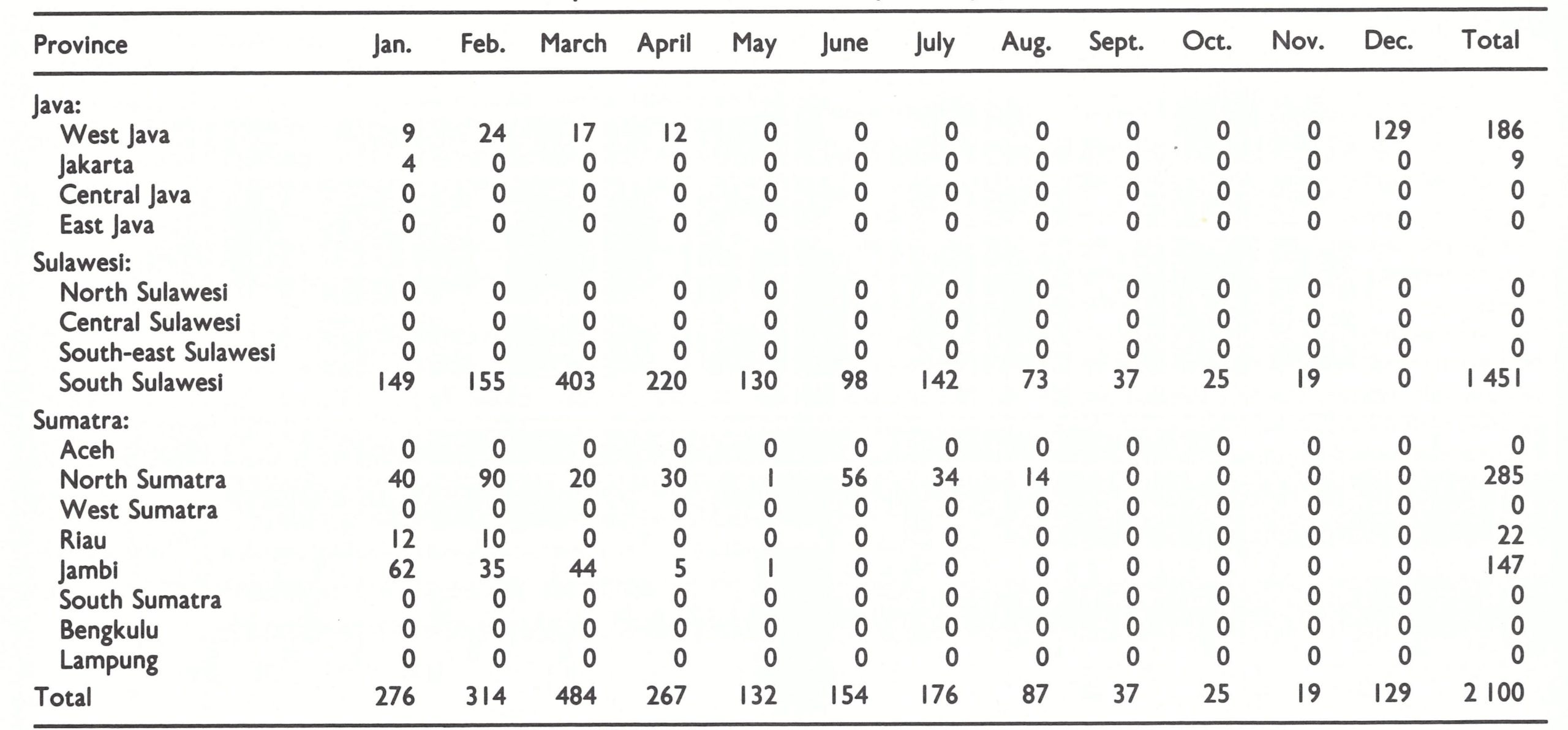
aNo cases were reported in Maluku, Kalimantan, Bali, Nusa Tenggara, West Irian or Jogjakarta during this period.
Immediately after the apparent detection of the last case, the 1208 vaccinators in Sulawesi, Sumatra and Kalimantan searched village by village during a 4-month period, reaching 18 205 (73.5%) of the 24 781 villages in the process. Although 920 suspected cases were examined and 76 specimens were taken, none revealed the presence of smallpox (WHO/SE/74.63, Cuboni et al.).
In the island of Kalimantan (population, 5 million) and in the other provinces of Sulawesi, provincial and local health staff, without significant additional support from national or WHO staff, had unexpectedly succeeded in interrupting transmission as early as November 1969. How this was achieved is not fully documented. Kalimantan had experienced a major epidemic of smallpox, with large numbers of reported cases, during 1965-1967. The epidemic may have begun before 1965, although no earlier data are available. Because reporting was so incomplete, it is probable that the actual number of cases may have been 100 times or so greater than the number recorded.
Programme staff at the time speculated that natural immunity induced by the epidemic, combined with extensive vaccination, had so reduced the number of susceptible persons that transmission was interrupted even though the surveillance-containment programme was much less effective than in other areas. However, a high level of immunity was not the primary explanation for the interruption of transmission in Kalimantan and in Central, South-east and North Sulawesi, as was shown in a February 1974 survey. At that time, Indonesian staff conducted random cluster sample surveys among children throughout these provinces (Table 13.18) (WHO/SE/74.66, Cuboni et al.). In most provinces, more than one-third of all children remained susceptible. Immunity levels were substantially below those in most of Java, in which health services were far more extensive.
Important to the interruption of transmission was the fact that the populations of Kalimantan and Sulawesi were concentrated in discrete areas, primarily along the coast. Communication between these population centres was much more difficult than in Java or Sumatra. In effect, they were more like a series of comparatively small island populations than a land mass over which travel was easily accomplished. Many outbreaks undoubtedly terminated spontaneously and others responded to comparatively perfunctory containment and vaccination activities, as was the case in much of Africa, for example . After transmission had been interrupted in an area, smallpox was reintroduced only infrequently .
Table 13.18: Kalimantan and Sulawesia : percentage of children unprotected by vaccination, by age group, February 1974
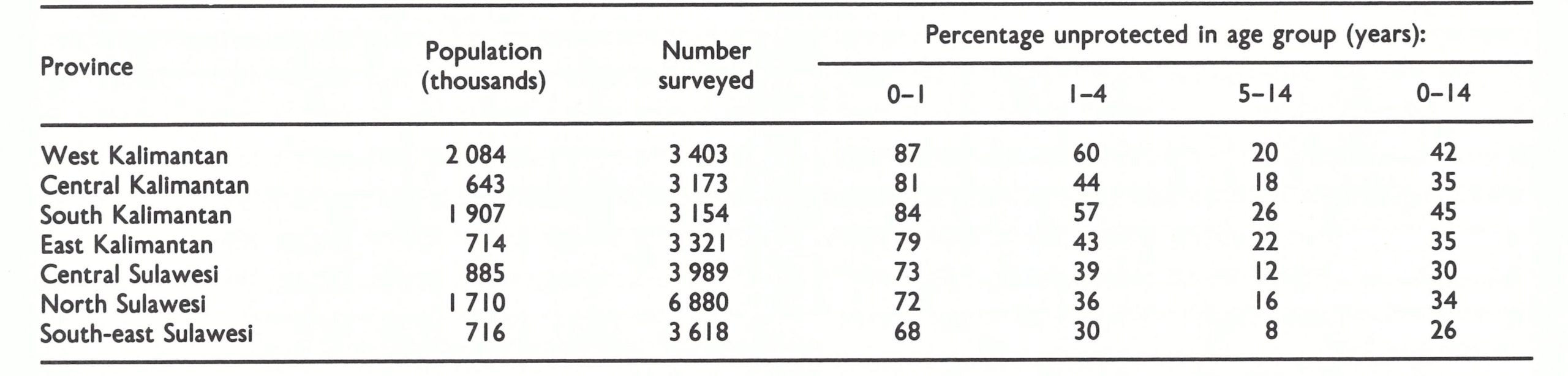
aSouth Sulaswesi excepted.
INDONESIA'S LAST OUTBREAK, 1971
After the last cases occurred in Sulawesi in November 1971, 4 weeks elapsed during which no smallpox cases were reported in Indonesia. It appeared that transmission had been interrupted, but on 14 December 1971, the Director of the Smallpox Eradication Programme received a report from Tangerang Regency (one of the 24 regencies/municipalities in West Java) of 45 cases and 6 deaths in Sepatan Subdistrict, only 28 kilometres from Jakarta. Tangerang (population, I million) had recorded its last cases in February 1971, fully 10 months earlier. A village-by-village search had been conducted in West Java between June and August 1971 in the subdistricts which had reported cases during 1970-1971; lack of personnel had precluded a search in all subdistricts. Sepatan Subdistrict had not reported cases during this period and thus had not been searched.
On investigation, it was found that as early as December 1970, a whole year earlier, many cases in Sepatan had begun to be reported to the health centre by the subdistrict’s vaccinator. The medical officer of the health centre periodically organized ineffectual mass vaccination campaigns to control the outbreaks but deliberately suppressed the reports of smallpox, fearing that he might be punished for incompetence. In mid-December 1971, a provincial mobile surveillance and supervisory team visited the area on routine tour and was informed of the outbreaks by the local staff (Cuboni et al . in WHO/SE/76 .85). Search and containment activities were immediately instituted . In the realization that the suppression of reports might be widely prevalent, the decision was made to offer a transistor radio to any person who reported an active case of smallpox. This, so far as is known, was the first occasion in the Intensified Programme when a reward was offered for case reporting. It proved to be highly effective. Numerous suspected cases with illnesses of all types were reported by people throughout the area. Eventually, 160 smallpox cases with 15 deaths were confirmed in 3 villages (total population, 7982) of Sepatan Subdistrict ; nearly one-third were unprotected when containment vaccination had begun (Table 13.19).
Table 13.19: Sangiang, Sarakan and Gaga villages, Sepatan Subdistrict : number of vaccinations performed during containment operations, 1972

a I.e., those receiving primary vaccination as a percentage of the total vaccinated during the containment phase .
The outbreak had started in Sarakan village in December 1970 (Fig. 13.10), 1 year previously, as a result of an importation from West Jakarta. Smallpox spread slowly, only 14 cases occurring between December 1970 and May 1971. Eventually, the outbreak was contained by a local vaccinator. Meanwhile the disease had spread to Sangiang village in May 1971 and, in September, numerous cases began to occur. In all, 131 persons eventually developed smallpox in this village of 3106 persons. At the end of November the disease was reintroduced into Sarakan village and, in December, it spread to nearby Gaga village. Finally, late in December, an outbreak of cases developed in a village 80 kilometres distant. The last 2 known cases in Indonesia occurred on 23 January 1972, one of them in Gaga village, and the other in Kupahandap village.
Concerned that other hidden foci might be present elsewhere in Indonesia, the programme staff decided in May 1972 to offer a reward of 5000 rupiah (US$12) to anyone reporting a case. This was widely publicized. The following month, teams from throughout Indonesia began an active search programme. Numerous rumours were investigated and many specimens were examined, but no further cases were found. A summary of the numbers of specimens examined in laboratories during 1969-1973 (Table 13.20) indicates the extent of this activity.
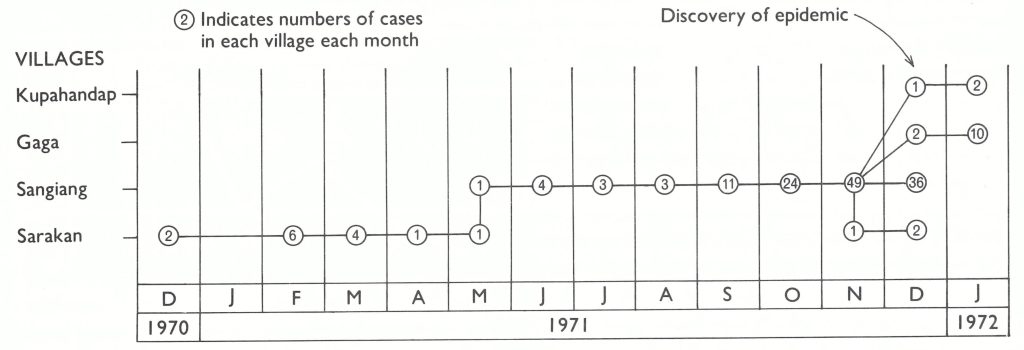
Fig. 13.10. Indonesia: last chain of smallpox transmission, 1970-1972.
Table 13.20: Indonesia : laboratory examination of specimens, 1969-1973

MORBIDITY AND MORTALITY PATTERNS
Smallpox in Indonesia exhibited two unusual features: (1) an exceptionally large proportion of cases among younger children; and (2) case-fatality rates which were often lower than those observed elsewhere in Asia.
In June 1969 the joint WHO-Indonesia Assessment Team analysed the age distribution of 3823 cases in selected areas and during periods when reporting was considered to be reasonably complete (Table 13.21). The age distributions were similar in West and Central Java and Jakarta, in which smallpox was then endemic. Cases in East Java occurred primarily in outbreaks following importations and the patients were generally older, as was the case in other non-endemic areas. Excluding the data for East Java, 68% of cases occurred in children aged 0—4 years, a group which comprised only 18% of the population of the country. A surprisingly high incidence—about 12%—was found in infants under 1 year of age, twice the proportion recorded in India.
Table 13.21: Java: age distribution of 3823 cases of smallpox, 1968-I969a
aIncludes only cases, from parts of regencies and for limited periods, whose precise age was known .
Smallpox spread in Indonesia more readily than in most parts of the world and transmission occurred throughout the year with no apparent seasonal pattern. The facility of spread can be attributed to the high population density and the custom in Indonesia of carrying sick children to visit relatives, thus exposing many more susceptible individuals.
The reported case-fatality rates in many years and during most outbreaks appeared to be lower than those in the Indian subcontinent. This is the converse of what might have been expected, because cases in Indonesia were proportionately more numerous in the very young, among whom case-fatality rates are customarily higher. The question whether case-fatality rates in Indonesia were substantially and uniformly lower than those in the Indian subcontinent was never resolved. The reporting of both cases and deaths was grossly incomplete throughout Indonesia before 1968. The degree of underreporting of cases compared to that of deaths undoubtedly differed from year to year. This probably accounted for such discrepancies as a case-fatality rate of 10% in 1950 and one of 44% only a year later. With the commencement of the national programme, the reporting of cases gradually improved, more rapid progress being achieved in some areas than in others. However, as in other countries, few efforts were made to improve the completeness of the notification of deaths . Since the programme’s goal was to interrupt the transmission of smallpox, it was more important to know where and how many cases were occurring than to be aware of how many deaths had taken place.
In containing outbreaks, especially in 1970-1971, the smallpox eradication staff carefully enumerated cases, and because teams remained in the infected areas, the numbers of deaths (which usually occurred 1-2 weeks after the onset of illness) were also known fairly accurately. In those outbreaks, case-fatality rates of 5-10% were often observed, about half as high as the rates in the Indian subcontinent. Data from Jakarta, however (Fig. 13.11), consistently showed much higher case-fatality rates. Jakarta had had a reasonably complete system for the notification of deaths since 1965 and for the reporting of cases since 1968. The case-fatality rates were twice as high as those of West Java, a province which surrounds it and across whose borders residents moved freely. In other respects, the populations were essentially similar with regard to nutrition and general health. If it is assumed that the virus strain in Jakarta was the same as that in West Java, the obvious explanation for the lower rates in West Java would be incomplete notification of deaths. And yet the case-fatality rates in West Java were similar to those observed later in some well-studied outbreaks elsewhere in Indonesia. The observations were never reconciled.

Plate 13.8. Misah Bin Inang (A), one of the last two smallpox patients in Indonesia, became ill on 23 January 1972. Facial pockmarks are apparent in this picture taken in 1979, but many persons (B) were more severely afflicted.
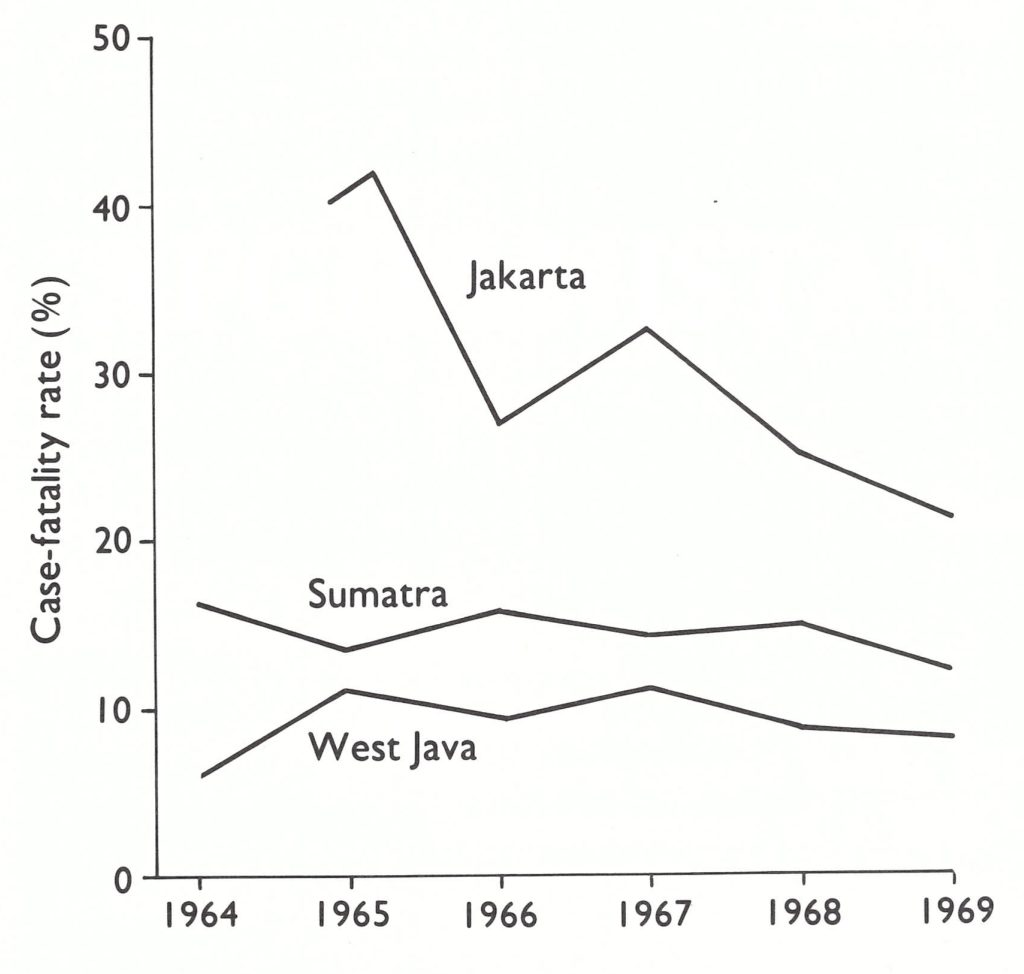
Fig. 13.11. Jakarta, Sumatra, and West Java: smallpox case-fatality rates, 1964-1969.
CONCLUSIONS
Smallpox transmission in Indonesia was interrupted just 3 years and 7 months after the programme began in July 1968 . This was a remarkable achievement considering the country’s size, population and the limited international resources provided . The experience in Indonesia had a profound effect on other programmes during the succeeding years. Among the innovations were the WHO smallpox recognition card, the offer of a reward for reporting a case, a procedure for the systematic search for cases throughout a wide area, and the demonstration of the efficacy of a search based on contact with teachers and schoolchildren. More important, the success of the surveillance-containment strategy was forcefully communicated by Indonesian programme staff to their counterparts in the Indian subcontinent through papers and seminars. Of particular significance was a specially convened WHO interregional seminar in New Delhi in December 1970. One of the papers, contributed by Dr Koswara, the Indonesian programme’s director (Koswara in WHO/SE/71.30), was entitled: “Is Routine Vaccination a Necessity in a Smallpox Eradication Programme?” The author concluded that proper surveillance containment action had brought smallpox under control in a short period, while routine vaccination and mass vaccination campaigns had had little effect in interrupting transmission. Many participants at the conference severely criticized this view, which they considered tantamount to heresy. At that time, Indonesia had not yet stopped transmission in Java, let alone in Sumatra or Sulawesi. Because of this, few of the participants were persuaded by Dr Koswara’s arguments. However, with the occurrence of Indonesia’s last case in January 1972, it was apparent that the 11-year-old programmes in India and Pakistan had much to learn from the Indonesian experience. A strong stimulus for change was provided.
EdgarGlink
September 1, 2025В приложении Telegram появилась функция звезд. Теперь участники могут отмечать важные сообщения. Это позволяет быстро возвращаться нужную информацию. как купить звезды в телеграмме в россии Функция комфортна для ежедневного общения. С использованием звёзд легко оставить ключевые заметки. Такой инструмент бережёт время и делает общение быстрее.
AlvinKah
September 28, 2025Выбор профессиональной техники — серьёзный этап в развитии красоты. Сначала стоит уточнить потребности и направления, которые хотите проводить. Важно изучить документы и качество выбранного оборудования. Комментарии других пользователей помогут сформировать обоснованный выбор. Бьюти Инструмент Также нужно обратить внимание на набор функций и простоту работы. Тестовая проверка оборудования позволяет понять комфорт работы. Важно оценить тарифы и поддержку производителя. Взвешенный выбор аппарата поможет повысить уровень услуг.
MichaelSpisa
October 4, 2025Современное медоборудование играет значительную часть в обследовании и поддержке пациентов. Больницы всё чаще оснащаются передовую технику. Это обеспечивает специалистам ставить правильные заключения. Актуальные приборы создают безопасность и для больных, и для персонала. http://marshallplast.com/forum/index.php?topic=347.new#new Внедрение высоких технологий помогает результативное лечение. Большинство устройства включают возможности для детального наблюдения состояния здоровья. Доктора могут оперативно реагировать, основываясь на данных аппаратуры. Таким образом, современное медицинское оборудование повышает уровень лечебного процесса.
Floydcop
November 12, 2025This website offers a lot of captivating and useful information. On the website, you can explore many topics that broaden your horizons. Everyone will benefit from the materials shared on this site. Each section is thoughtfully designed, making it convenient to use. The materials are presented professionally. You can find recommendations on many areas. Whether your interest is in educational content, this site has everything you need. Overall, this site is a excellent platform for those who love learning. https://tango-city.de/
Floydcop
November 13, 2025The site provides a lot of interesting and helpful information. On the website, you can explore various materials that broaden your horizons. Everyone will enjoy the content shared here. Every category is easy to navigate, making it comfortable to use. The materials are easy to understand. You can find tips on many areas. Whether your interest is in educational content, this site has a lot to offer. All in all, this platform is a great source for those who love learning. https://xevanio.de/