Chapter 17:
Western and central Africa

INTRODUCTION
Progress in smallpox eradication throughout most of Africa was more rapid than in Asia, despite the fact that the majority of African countries had less developed health service infrastructures, poorer roads and communications and proportionately fewer health personnel. The rapidity with which smallpox was eliminated in an area embracing 21 countries of western and central Africa (Fig. 17.1) was especially significant. Programmes in all but one of the countries in this region were supported by the United States 849 Agency for International Development (AID) with technical direction and coordination provided by the United States Communicable Disease Center (CDC), later called the Centers for Disease Control. Most national programmes in this area began early in 1967 and all were fully operational by January 1968. By September 1969, every country except Nigeria had interrupted smallpox transmission, and in May 1970, only 31/2 years after field operations had begun, the last case in this region was detected. Within this brief span of time, smallpox had been eliminated from some of the least developed and most heavily infected countries in the world—from a contiguous area greater in size than the continental USA, inhabited by 111 million people (the estimated population in 1967).
From November 1965, when the USA decided to support the smallpox eradication effort in western and central Africa, this programme played a pivotal role in the ultimate achievement of global eradication. The resolve of the USA to commit substantial resources lent encouragement to the Nineteenth World Health Assembly’s decision in 1966 to embark on the Intensified Smallpox Eradication Programme. Programme staff made important early contributions to the development and improvement of field operations; their observations changed the understanding of the epidemiology of smallpox and served to alter the global strategy. The demonstration that smallpox could be eliminated rapidly throughout such a vast developing area provided a crucial impetus to programmes in other countries and convincingly showed that the goal of eradication was realistic, even in areas in which health services were the least adequate and in which difficult problems-even civil war-had to be surmounted. Finally, many individuals who acquired experience in this regional programme subsequently made important contributions to the development and execution of programmes in other parts of the world.
The activities and decisions leading to the development of this endeavour are thus of particular significance. Interestingly, despite the importance of the programme, the USA’s decision to contribute to it did not result from a considered policy judgement to support the WHO Intensified Programme as such. Rather, it began as an ancillary objective in a multicountry programme for the control of measles in many of the less populous countries of this region.
After the programme had begun, the staff of CDC bore full responsibility for its technical guidance and coordination, although they kept in close contact with WHO staff responsible for the global programme. WHO’s contributions were modest, consisting mainly in the provision of bifurcated needles, an average annual subvention of US$200 000 to cover local costs, technical support to one programme (Mauritania) and the organization of activities pertaining to the certification of eradication in 1976. The remarkable achievements in this part of Africa are therefore primarily those of the national governments and staff, AID and the personnel of CDC.

Fig. 17.1. Western and central Africa: countries that participated in the smallpox eradication and measles control programme, 1967-1972. The bold lines and circled numerals indicate the country groupings under which the national programmes are discussed in the text.
Changes in Political Status and Names of Countries
In 1967, when the AID-supported regional programme began, all but 2 of the 21 countries (Equatorial Guinea and Guinea-Bissau) shown in Fig. 17.1 were independent States. Liberia had enjoyed sovereignty since 1847 but 18 others had become independent between 1957 and 1965. Thirteen had been colonies of France and were commonly referred to as francophone countries. These were the Central African Republic, Chad, the Congo, Cote d'Ivoire, Dahomey, Gabon, Guinea, Mali, Mauritania, Niger, Senegal, Togo and Upper Volta. Cameroon, which had been administered jointly by France and the United Kingdom, was officially bilingual. Four—namely, the Gambia, Ghana, Nigeria and Sierra Leone—had recently obtained independence from the United Kingdom.
Equatorial Guinea (population in 1967, 278 000), a colony of Spain, became independent in 1968 and subsequently received supplies and equipment from the USA for smallpox and measles vaccination. Guinea-Bissau (population in 1967, 525 000), a colony of Portugal, became independent in 1974 after assistance from the USA to the regional programme had terminated.
Two countries changed their names after the programme's conclusion. Dahomey was renamed Benin in 1975, and Upper Volta was renamed Burkina Faso in 1984. In this chapter, which describes activities before 1975, the former names, Dahomey and Upper Volta, are used.
THE REGION OF WESTERN AND CENTRAL AFRICA
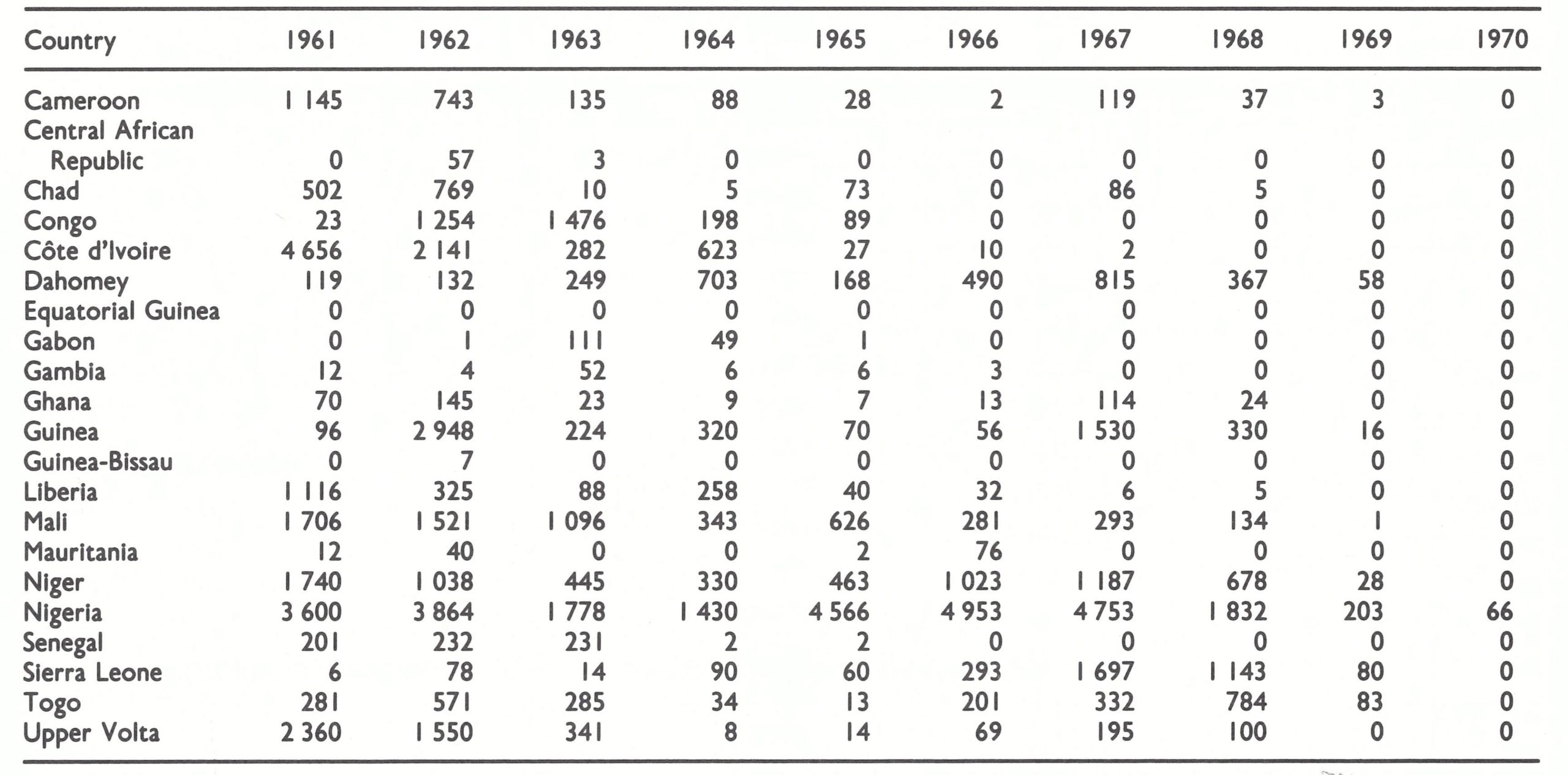
Within the region defined in this book as western and central Africa were 21 countries, of which 14 reported cases of smallpox in 1966 (Table 17.1). The predominant form of smallpox was variola major with a case-fatality rate of 5-15% . Because established health services were few and reporting was very incomplete, the actual geographical extent of smallpox and its true incidence were uncertain when the programme began.
The region was diverse both in ecology and in culture. Rain forests predominated along the coast, giving way to savanna and finally to the Sahara desert. Throughout the region, hundreds of tribal groups speaking their own local language were organized into various tribal and theocratic societies which often transcended national boundaries 9. Road systems were generally poor, communications were difficult, and newly created governments were only beginning to cope with the array of problems associated with the development of education, agriculture, industrialization and health services. Smallpox was but one of many problems for which resources were few and trained manpower was limited.
CDC and WHO staff were in agreement that if smallpox could be eliminated from this entire region, importations would be infrequent and their containment would probably not present a serious problem. To the north lay the Sahara desert and the smallpox-free countries of Morocco, Algeria and Libya and the Spanish province of Western Sahara. To the east was the Sudan, then free of smallpox. To the south-east of the region was the Democratic Republic of the Congo (later renamed Zaire), the only adjacent country infected with smallpox. It bordered on the Central African Republic and the Congo. The latter two countries, in 1966, were thought to be smallpox-free and there were few travellers from the Democratic Republic of the Congo into either of them because of the difficult terrain and political restrictions on travel.
In countries which had formerly been colonies of the United Kingdom, health care was provided primarily through government or mission health centres or dispensaries, some of which performed smallpox vaccination using glycerolated or lanolinated vaccine produced in Nigeria or the United Kingdom, although many offered no immunizations whatsoever. Mobile health units periodically augmented the vaccination effort in Ghana and in parts of Sierra Leone and southern Nigeria. The control of smallpox outbreaks was the delegated responsibility of district or local medical officers and, in some instances, mobile medical field units. As in other countries, the health personnel responded with varying degrees of interest, but even where efforts were made to control smallpox, these were frequently unsuccessful because of the use of the heat-labile, sometimes low-potency vaccine. Of the countries relying on this approach, only Ghana and the Gambia had succeeded in achieving a substantial measure of smallpox control. Ghana’s success could be attributed to its mobile medical field units and to health inspectors who took special care in preserving the thermolabile vaccine and who diligently investigated and contained reported outbreaks by vaccination. The Gambia, too small in area and population to permit long-sustained transmission of smallpox on its own, was partially insulated from importations by the surrounding, comparatively well vaccinated population of Senegal. Liberia, in which a mass vaccination campaign with freeze-dried vaccine had been conducted in 1962, followed by a WHO-supported programme, reported few cases. In northern Nigeria and Sierra Leone, however, vaccinial immunity in 1967 was especially low and smallpox was a serious problem.
Table 17.1: Western and Central Africa: number of reported cases of smallpox, by country, 1961-1970
In the former French colonies, disease control was primarily the responsibility of multi-purpose mobile teams of the local endemic diseases control service (Service des Grandes Endemies), which systematically moved throughout the country endeavouring to reach each village once every 2-3 years (Richet, 1965; Labusquiere, 1967). Government health centres and dispensaries also existed but were less numerous and generally less well supported than in the former British colonies; mission hospitals and health centres were few. The multi-purpose teams administered smallpox vaccine and undertook other preventive measures, such as those aimed at controlling yellow fever, trypanosomiasis, yaws and leprosy. In most of the countries, a French-produced, freeze-dried vaccine had been used since the early 1920s (Fasquelle & Fasquelle, 1971). The degree of potency and stability of this vaccine is unknown, but when freeze-dried smallpox vaccine of reasonably high titre began to be used extensively in the early 1960s, and in areas in which the multipurpose teams continued to function, smallpox incidence declined rapidly; in some countries, the disease had disappeared by 1967. Thus, the numbers of reported cases in 1966 were few or nil throughout the former area of French Equatorial Africa (Cameroon, Central African Republic, Chad, the Congo and Gabon), as well as in Mauritania, Senegal and Upper Volta. In Mali, a WHO-supported programme begun in the early 1960s had markedly reduced smallpox incidence, and in Cote d’Ivoire specially constituted mobile smallpox vaccination teams interrupted transmission in 1966. In the other francophone countries, multi-purpose teams functioned less effectively, and in some of them had ceased to function altogether; in Dahomey, Guinea, Niger and Togo, smallpox continued to be an important problem.
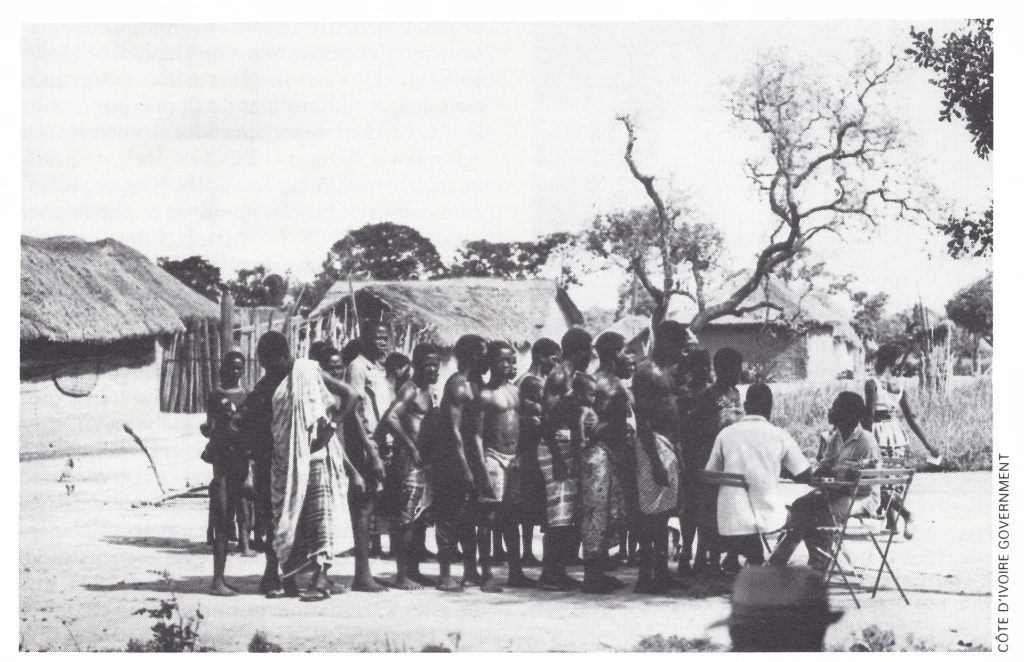
Plate 17.1. Villagers in Cote d’lvoire line up for smallpox vaccination during the campaign that eliminated smallpox from that country in 1966.
ORIGINS OF THE REGIONAL PROGRAMME, 1961-1965
The decision by the USA in November 1965 to support a region-wide programme of smallpox eradication and measles control had its origin in a small-scale field trial of the newly developed Edmonston strain measles vaccine, which was conducted in 1961 in Upper Volta (Meyer et al., 1964a). This vaccine had been found to be safe and effective when given to children in the USA but because it frequently induced high fever, gamma-globulin was given simultaneously to diminish symptoms. Under the difficult field conditions in developing countries, the administration of both the measles vaccine and gamma-globulin was not feasible. Both had to be given subcutaneously, and while a jet injector could be used to administer measles vaccine, a needle with syringe was required for the more viscous gamma-globulin. Expense was another factor, the vaccine and gamma-globulin costing nearly US$2.00 per dose. Most developing countries could not afford to spend scarce foreign exchange on vaccines costing even a small fraction of this amount.
In 1960, Dr Paul Lambin, Minister of Health of the newly independent country of Upper Volta, was told of the new vaccine while visiting the United States National Institutes of Health (NIH). Because of the severity of measles in African children (Morley, 1962; Cantrelle, 1965), the vaccine was of special interest to him. Accordingly, he proposed that a study should be undertaken in Upper Volta to determine whether the measles vaccine without gamma-globulin could be given safely to African children. Concern about its safety was legitimate, since it was feared that the high fever it induced might prove harmful or even fatal to children suffering from such conditions as tuberculosis or malnutrition.
With support from NIH, Dr Harry Meyer and his colleagues studied a group of 600 children in Upper Volta in 1961 (Meyer et al., 1964a). They demonstrated that the vaccine without gamma-globulin could be administered with safety and efficacy. Dr Lambin was impressed by the results and requested the USA to provide support for measles vaccination for all young children throughout the country. This request was granted and between November 1962 and March 1963, the multi-purpose mobile teams of the endemic diseases control service in Upper Volta, assisted by Dr Meyer and his colleagues, vaccinated 731 548 children (Labusquiere, 1967). The number of reported cases of measles declined sharply, and during the next 2 years remained well below previously recorded levels.

Plate 17.3. J. Donald Millar (b.1934), a CDC epidemiologist, directed the AID-supported programme for smallpox eradication and measles control in western and central Africa from November 1966 to March 1970. As Chief of the CDC Smallpox Unit, he had supervised field studies of the jet injector and demonstrated its usefulness in large-scale programmes. He is holding a fetish statue of Sopona, a smallpox deity of some tribes of western Africa.
Information about this campaign was widely communicated by Upper Volta to other member countries of a regional health organization, the Organization for Coordination and Cooperation in the Control of Major Endemic Diseases in West Africa (Organisation de Coordination et de Cooperation pour la Lutte contre les Grandes Endemies en Afrique de l’Ouest-OCCGE), whose headquarters were in Upper Volta. The organization comprised most countries of the former area of French West Africa (Cdte d’Ivoire, Dahomey, Guinea (until 1965), Mali, Mauritania, Niger, Senegal and Upper Volta). At the request of OCCGE, AID agreed to support additional national campaigns, and thus it was arranged for Dr Meyer to conduct training and demonstration projects in 6 of the countries (Cote d’Ivoire, Dahomey, Guinea, Mali, Mauritania and Niger) late in 1963. During the following year, AID allocated US$1 478 000 for the provision of vehicles, jet injectors and measles vaccine to vaccinate 25% of the children between 6 months and 6 years of age. Towards the end of 1964, the measles vaccination campaigns began.
AID staff had assumed that the execution of the campaign would be comparatively straightforward, given the success in Upper Volta and the long experience of the multipurpose mobile teams in each of the countries. The fact that not all the endemic diseases control services were of the same quality as that in Upper Volta was not appreciated. The ensuing difficulties were compounded by the problem of introducing a new technology the jet injector-which at that time required electric power and was difficult to repair and maintain, and a new vaccine, which had to be refrigerated until reconstituted for use. To conduct the mass measles vaccination campaigns, most countries curtailed or stopped the activities of the multi-purpose mobile teams because national resources were too limited to permit the two sets of activities to be continued.
With the beginning of the mass campaigns, it was decided that such technical assistance as might be needed from the USA should be provided by CDC, the agency primarily concerned with the field implementation of disease control programmes. Thus, in December 1964, Dr Lawrence Altman of CDC was requested by AID to spend 6 weeks in the countries to observe the campaigns and to report on progress. He found few of the campaigns to be progressing at all satisfactorily and eventually spent 6 months endeavouring to bring order out of chaos, albeit with little success.
Despite the difficulties, AID decided to offer assistance to an additional 4 countries (Cameroon, Central African Republic, Chad and Togo) to permit them to begin mass measles vaccination campaigns in 1965-1966. The potential scope of the project was even further expanded when, late in June 1965, the manufacturer of the measles vaccine brought the persuasive Dr Lambin to the USA on a special tour. The Director of AID was impressed with Dr Lambin and asked that a plan be drawn up for a comprehensive programme of assistance for measles vaccination in 16 African countries, including all the former French colonies of western and central Africa, as well as the Gambia, Liberia and Sierra Leone. Recognizing that this implied the need for more technical assistance staff than had been foreseen, AID asked CDC whether 9 epidemiologists could be made available in the autumn of 1965, each to serve on temporary duty for periods of 4-6 months in the countries in which campaigns were either in progress or due to begin.
The Addition of Smallpox Eradication as an Objective
Until July 1965, CDC personnel had not been involved in the development of policy or plans for the measles vaccination campaigns. However, if CDC were to provide so many epidemiologists for such extended periods of time, its own programmes would have to be curtailed or substantially altered. Accordingly, an examination of priorities and alternatives was undertaken, a responsibility assigned to Henderson, then Chief of the CDC Surveillance Section, from which most of the epidemiologists would be drawn.
To Henderson and his colleagues, the programme, as then conceived, did not represent sound public health policy. AID foresaw a 4-year programme during which each year all children from 6 months to 6 years of age would be vaccinated against measles in onefourth of each country. At the conclusion of the programme, AID staff reasoned that all children would have been vaccinated and that the country would assume responsibility for continuing to vaccinate children who were born after the programme had terminated. It seemed unreasonable to CDC staff to assume that the impoverished African countries would be able to bear the recurring expenditures, given that measles vaccine then cost US$1.00 per dose; indeed, at that time, few of these countries could afford yellow fever vaccine, which was one-tenth as expensive. Had it been possible to eradicate measles from the area, vaccination conceivably could have been stopped, but this objective appeared unrealistic given the fact that no industrialized country, despite greater health resources, had yet eliminated the disease. At best, the reduction in measles incidence would be transient because almost all cases of measles in Africa occurred among young children and thus, within 3-4 years after vaccination in an area, measles incidence could be expected to approach levels comparable to those observed before the programme had begun. To embark on such a programme implicitly raised public expectations that the vaccine would continue to be made available as a routine preventive measure. If a government were to terminate its use abruptly after 4 years, possible repercussions from the public could be foreseen, particularly in the wake of the measles epidemics that would almost certainly follow.
In July 1965, however, the USA had already undertaken to provide assistance for measles vaccination campaigns in 11 western and central African countries; a proposal from CDC that no programme should be conducted was not acceptable. The combination of this programme with one designed to eradicate smallpox from the region appeared the most logical move, since it would provide an objective which offered hope of longer-term benefits. That the eradication of smallpox throughout a geographical region was feasible had been shown in other parts of the world. If this could be achieved, occasional cases might still be imported into the region and these would have to be contained. Smallpox eradication, however, seemed to be a more reasonable long-term goal than one which called for a continuing campaign of measles vaccination for all children. Moreover, as CDC staff reasoned, WHO and its Member countries were committed to a programme of global smallpox eradication and, although this was not progressing well, it was believed that a successful regional effort in one of the most highly endemic areas would represent an important contribution and perhaps a stimulus to other endemic countries.
Two other considerations—one technical and one political—also lent support to the idea of smallpox eradication. In 1965, CDC had just completed a series of studies which demonstrated the efficacy and practicability of the intradermal administration of smallpox vaccine utilizing a newly developed nozzle for the jet injector (Millar et al .,1969; Neffet al .,1969; Roberto et al .,1969; Millar et al .,1971). The jet injector itself had been redesigned so that it could be powered by a pedaloperated hydraulic pump rather than by electricity; this offered a substantial advantage in field work. A second important consideration was the commitment made by the USA in 1965 at the Eighteenth World Health Assembly to provide support to the Intensified Smallpox Eradication Programme (see Chapter 9). Although the support then envisaged was for the development of a vaccine production laboratory in Kenya and assistance to smallpox eradication programmes in South America, it seemed reasonable to propose a broader initiative.
Plate 17.3. J. Donald Millar (b.1934), a CDC epidemiologist, directed the AID-supported programme for smallpox eradication and measles control in western and central Africa from November 1966 to March 1970. As Chief of the CDC Smallpox Unit, he had supervised field studies of the jet injector and demonstrated its usefulness in large-scale programmes. He is holding a fetish statue of Sopona, a smallpox deity of some tribes of western Afric.
CDC therefore suggested that AID should support a region-wide programme of small pox eradication in western and central Africa, with measles vaccination also being offered in countries selected by AID and where it was agreed by national authorities. This was a much bigger programme than that envisaged by AID, which had anticipated providing support to only 16 countries, with a total population of about 50 million in 1967. Two important countries in the region which were not then included—Nigeria and Ghana—together had a population of more than 60 million (see Table 17.9).
The proposal was strongly endorsed by officials of the United States Public Health Service—Dr Luther Terry, the Surgeon General, and Dr James Watt and Dr Benjamin Blood of the Office of International Health. AID readily accepted the proposal for a programme dealing with smallpox and measles in 16 of the countries but not for the inclusion of Ghana and Nigeria. As noted in an AID memorandum of 19 July 1965:
“The total scope of the African problem is too great for any one donor to undertake its solution . . . With a few exceptions [the 16 countries are among those] in which a modest demonstration of US interest and presence is desired without involving the USA in major dollar or personnel expenditures.”
Despite these reservations, planning by CDC staff proceeded throughout the summer for an 18-country programme of 5 years’ duration which would provide all supplies and equipment, plus a complement of CDC technical staff for work in individual countries, in an African regional office and at CDC headquarters in Atlanta. If accepted, this would be the first AID-supported technical assistance programme to be administered by CDC. On 20 August 1965, after many discussions between CDC and AID staff, the full proposal was formally submitted to AID. At the suggestion of CDC, Mr Milton P. Siegel, an Assistant Director-General of WHO, and Dr Karel Raska, Director of the Organization’s Division of Communicable Diseases, visited Washington to discuss the proposal, and, early in November, the Director-General of WHO, Dr Marcolino Candau, also had meetings with AID and CDC staff. Everyone urged that the plan should be implemented, although a point at issue was whether WHO or perhaps another donor could support the programmes in Ghana and Nigeria. WHO officials stated that the Organization’s resources were inadequate for the undertaking, and on the basis of WHO’s experience with respect to voluntary contributions from national sources, little hope was offered that the necessary support could be found elsewhere.
AID was faced with a dilemma. Commitments had already been made for measles vaccination campaigns in 11 countries for which technical assistance was needed. It was difficult to find the requisite complement of technical staff at short notice except from the Public Health Service, but this the Public Health Service declined to provide unless all 18 countries were included in a programme that provided for smallpox eradication.The issue was settled, partly in response to a memorandum from the Public Health Service (see box), and the offer of assistance was formally announced on 23 November 1965. Thus began the first coordinated regional smallpox eradication programme.
GOVERNMENT AGREEMENTS AND ORGANIZATION OF THE PROGRAMME
The proposal for the regional programme envisaged that it would begin in January 1967, little more than 13 months after the decision had been made to offer assistance to the 18 countries. The schedule was optimistic, given the need to develop plans and obtain agreements with each of the countries, to recruit and train technical staff and to procure and deliver all the necessary supplies and equipment. Surprisingly, these goals were largely achieved, although not without problems.
Discussions in Africa began with the governments concerned immediately after the formal announcement. From 23 November to 17 December, a team composed of Henderson, Dr Clayton Curtis of AID, Dr Henry Gelfand of CDC and Dr Warren Winklestein, a CDC consultant, held meetings with health staff and discussed the programmes with officials of 16 of the 18 countries—at the ministerial meeting of OCCGE countries; at a technical meeting of a counterpart organization for former French colonies in central Africa, OCEAC, comprising Cameroon, Central African Republic, Chad, the Congo and Gabon (the Organisation de Coordination pour la Lutte contre les Endemies en Afrique centrale, or Organization for Coordination in the Control of Endemic Diseases in Central Africa); and in special visits to Guinea, Liberia, Nigeria, and Sierra Leone. Time constraints precluded visits by the team to the Gambia and Ghana, but government officials there communicated to the respective United States embassies their willingness to participate. Discussions were also held with staff of the WHO Regional Office for Africa attending the OCCGE and OCEAC meetings and by Henderson with the Director-General of WHO and his staff in Geneva.
The only one of the countries noted above for which assistance was not foreseen was the Congo, with which the USA then had no formal diplomatic relations. However, AID agreed to include the Congo, when confronted with the decision by OCEAC leadership that either all or none of its member countries would participate in the regional programme. With this addition, the number of countries increased to 19; when Equatorial Guinea became an independent country in 1968, it too, was included, bringing the number of countries assisted by AID to 20.
The national staff in each country enthusiastically welcomed the proposal for a programme of smallpox eradication and measles control, the latter being the principal attraction to countries in which smallpox was not a significant problem. The inclusion of Nigeria was vital to the success of the programme, since that country accounted in 1965 for nearly three-fourths of all reported smallpox cases and almost half the population of the region. It was most encouraging to learn that a senior health officer in the Nigerian Ministry of Health, Dr G. Adeyemi Ademola, had already elaborated a detailed plan for smallpox eradication which the government had approved and which he was about to dispatch to WHO and AID with a request for assistance.
During the visits in Africa, it became apparent that many United States officials assigned to the countries were not enthusiastic about the programme. As a matter of policy and personal conviction, they attached the highest priority to economic development programmes. Bilateral and multilateral assistance agencies generally considered at that time that improvements in health would follow naturally on economic development and that special programmes in the health sector would serve only to divert resources from the primary objective. Apart from this broader policy issue, the officials concerned anticipated that meeting what were termed “local costs” would present insurmountable difficulties. During the visits of the CDC team the belief was repeatedly emphasized that most countries did not have adequate resources and that AID, as a matter of policy, did not provide for such local costs as the purchase of petrol and vehicle maintenance and repair. This policy had been adopted to ensure that, as far as possible, national governments would cover these recurrent costs by drawing on their own budgets, thereby fostering the continuity of programmes. For many governments, however, the resources available were so severely constrained that many fully equipped and fully staffed projects were unable to function for lack of comparatively small sums of money needed to buy petrol, for example. This potentially serious problem for the smallpox eradication-measles control programme was averted when the DirectorGeneral of WHO pledged to make WHO funds available to cover local costs when required. It was a decision about which he was politically uncomfortable since it meant that petrol purchased by WHO would be used to operate vehicles provided by the USA in a bilateral assistance programme. However, he abided by the commitment, and such support was eventually provided to 13 of the countries.
Memorandum of 10 November 1965 [Condensed from the original]
TO: Chief, office ofInternational Health Through: deputy Chief, Bureau of State Services
From: Donald A.Henderson, M.D.
SUBJECT: Scope of the Proposed West African AID-CDC Vaccination Program
The principal scientific objectives of the West African vaccination program, as discussed in repeated meetings between ourselves and AID officials have been two: (1) the eradication of smallpox and (2) the control of measles as a significant health problem in the countries under consideration. Since our earliest meetings, it has been noted repeatedly that smallpox eradication was not a realizable goal unless conducted on a comprehensive regional basis.
We have sensed reluctance on the part of AID to include Nigeria and Ghana in the total scheme. The concept that WHO or the United Kingdom might wish to support the Nigerian program in concert with the AID effort in the other countries in this area has been propounded. From knowledge of WHO plans and programs, Dr Henderson can state categorically that it will be difficult for WHO to assign a high level of priority to a Nigerian project for the next few years. Whether the United Kingdom could and would undertake a Nigerian programme reasonably promptly and aggressively is a moot question. The probability that they would, however, is recognizably slight.
It must be reiterated that any multi-country West African smallpox eradication program in West Africa must from its inception include Nigeria in its development and planning. Short of so doing, the program is a control program only. As stated at the end of August in meetings with AID officials and Dr Karel Raska of WHO, the Communicable Disease Center does not feel that it is indicated nor does it wish to divert skilled personnel to assume full-time responsibility and direction of a program for smallpox and measles in West Africa limited to control only.
The problem of decision and timing with respect to this program is a second major consideration. To recruit capable medical staff . . . commitments to them must be made in the fall of the year for employment beginning the following July. This has been firmly and clearly expressed in every meeting conducted with AID officials since early in the summer.
In the proposed program prepared in mid-August it was stated that, "It is important that this PASA [Participating Agency Service Agreement] be negotiated by mid-September 1965, in order that the USPHS may make the necessary staff commitments." We were later informed, however, that October 15 would be more realistic for a firm AID commitment. Postponement of the decision was again requested by AID to November 1 and then November 5. These dates have passed without decision.
In the meantime, a meeting of the Ministers of Health of the OCCGE countries has been scheduled for late November. It was felt by AID and PHS that Dr Henderson and Dr Gelfand should attend to initiate with the attending countries necessary discussions for programs next year. It was agreed, however, that such a trip would be essentially fruitless unless a commitment on the part of AID for full support to a West African program were forthcoming prior to the meeting. Since Dr Henderson and Dr Gelfand would have to depart about November 15, such a decision would have to be reached almost immediately.
Prospects of success for this program are already fading as a firm decision to undertake this activity is deferred . If decisions on the part of AID for full support to the 18-country program cannot be reached by November 15, the Public Health Service would be forced to withdraw such implied commitments as have been made and when AID decisions have been reached, discussions regarding the technical feasibilities would have to be re-explored from the beginning.
CDC staff had hoped that the overall regional programme could be phased in during a period of 2 years, some countries beginning operations in 1967 but as many as possible delaying them until 1968 to permit the necessary planning. For various reasons, however, such a delay was possible only in Guinea, Liberia and Sierra Leone. A programme in Nigeria was essential from the beginning of the regional effort, because of the size of the country and the fact that its central location made it the most logical site for the programme’s regional office. Programmes had also perforce to be introduced in 1967 in the OCCGE and OCEAC countries because of commitments already made by AID for measles vaccination campaigns. Because of these and other political considerations, it was decided that programmes would have to begin in 1967 in 16 countries and in 1968 in the other 3.
The direction of the regional programme at CDC was yet another problem. A Smallpox Unit had been created in the CDC Surveillance Section in 1962 which, under the direction of Dr J. Donald Millar, had ably conducted studies on the use of the jet injector for smallpox vaccination and on the frequency of complications following vaccination. It was logical that he should assume direction of the regional programme but, in August 1965, he departed for a year’s postgraduate study. In December 1965, with Dr Millar temporarily absent and no other suitable leadership available, Henderson relinquished his post as chief of the Surveillance Section to assume direction of the programme until Dr Millar returned. He was joined by his deputy, Mr Leo Morris, as well as by Dr Bernard Challenor, Dr Gelfand and Dr Ralph Henderson, and an administrative officer, Mr Billy Griggs—all CDC staff.
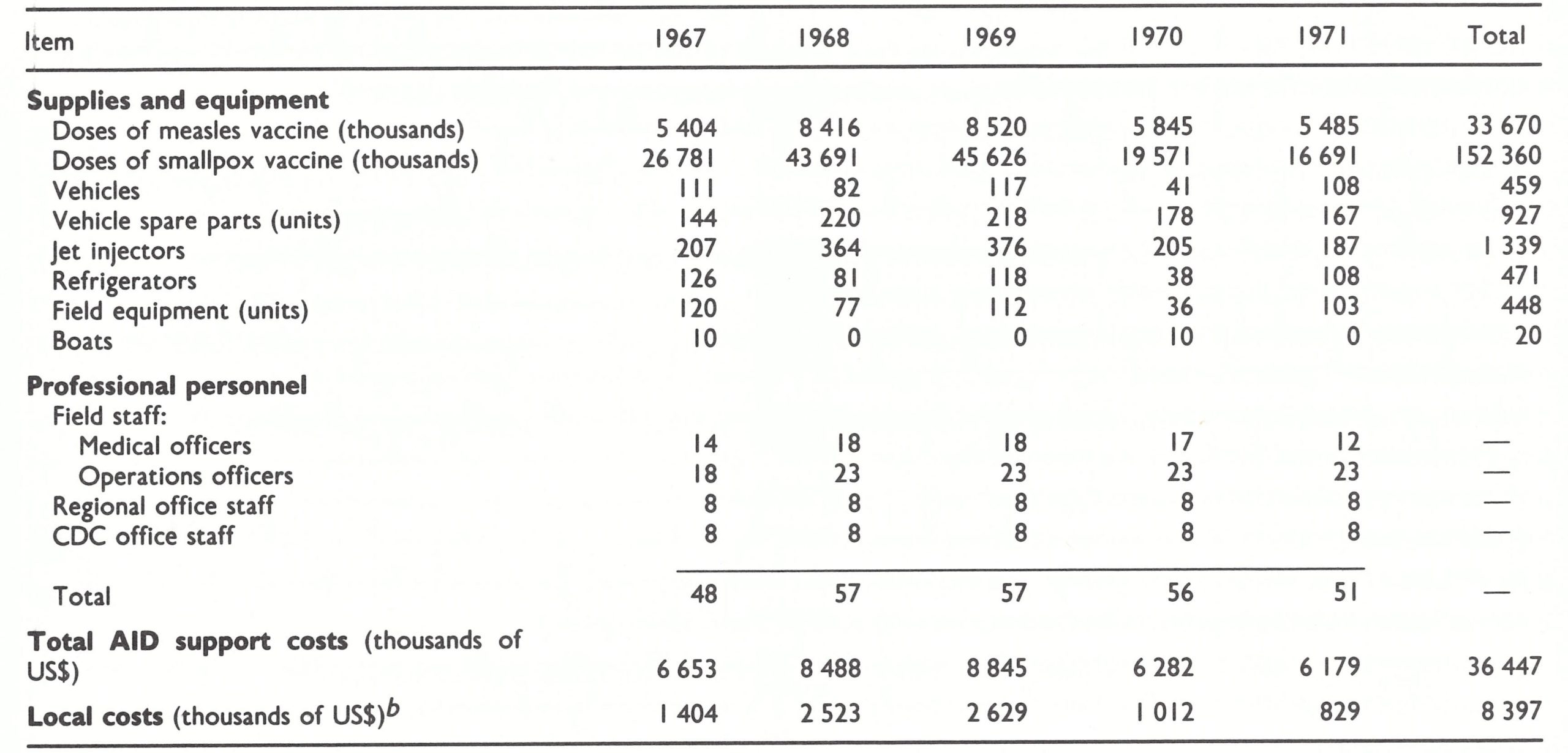
Within a month of the initial discussions with African health leaders, a 60-page document had been prepared which specified objectives and activities and identified needs and costs for personnel and commodities by country (Table 17.2). With minor modifications, this compilation was accepted by AID. The total cost of United States assistance was estimated to average about US$7 million per annum, of which approximately 40% was associated with the measles vaccination component, including storage refrigerators and jet injectors. It was anticipated that, on average, an additional US$1.7 million would be needed annually from WHO for local costs, a figure which, if correct, would have required 70% of all the WHO regular budget funds subsequently appropriated for smallpox eradication. Fortunately, the countries themselves eventually bore most of these local costs—WHO providing US$1.1 million to 13 countries from 1967 to 1972, or about US$200 000 per annum.
Table 17.2: Western and Central Africa: number of reported cases of smallpox, by country, 1961-1970
 a From a document prepared by CDC, 21 January 1966; estimates did not include requirements for the Congo.
b Expected to be met mainly by WHO.
a From a document prepared by CDC, 21 January 1966; estimates did not include requirements for the Congo.
b Expected to be met mainly by WHO.
The projected size of the staff in the programme’s regional office in Lagos and the central office in Atlanta, comprising about one-third of the total personnel, requires comment, as it was considered by some to be excessive and was accepted only with reluctance. The requirements, as outlined, arose from observations of other field programmes by CDC staff. It was believed that such programmes had regularly underestimated the need for central support and, indeed, this proved to be WHO’s experience in establishing the Intensified Smallpox Eradication Programme. The regional office in Lagos was expected to exercise broadly delegated responsibilities for administration and field supervision. The personnel concerned were expected to travel extensively to effect coordination and to provide short-term emergency technical support, as well as to assist the Lagos laboratory in the development of vaccine production . The document proposed the recruitment of 2 medical officers, 2 administrative officers, an equipment specialist, a health educator and a virologist. The CDC staff in Atlanta would be responsible for liaison with AID staff in Washington and with other agencies, for the recruitment and training of staff, for the development of instructional manuals, for the procurement and shipment of supplies and equipment, for the provision of longer-term emergency assistance in problem areas, and for the conduct of special studies pertaining to the programme. Although practical realities eventually required a redefinition of the respective roles of the two offices, experience demonstrated that the proportionately large staff in the central and regional offices, and the flexibility in assigning personnel which this implied, were vital to the rapid progress ultimately achieved.
In the programme document, the primary goal was specifically stated to be the eradication of smallpox, with measles control as a secondary objective, but longer-term objectives were envisaged:
- The establishment or, in some countries, improvement of mobile disease control services capable of administering vaccines or other preventive medications efficiently, economically and on a mass scale throughout the country.
- 2. The establishment in each country of a system of disease surveillance broadly applicable to a variety of communicable disease problems. a From a document prepared by CDC, 21 January 1966 ; estimates did not include requirements for the Congo. b Expected to be met mainly by WHO.
- The development of highly simplified statistical sampling techniques applicable in these developing countries which will permit rapid assessment of disease problems.
- The establishment of elementary virological laboratories . . . for the diagnosis of smallpox. [This objective was soon abandoned, as it was in other areas, when it became clear that the clinical diagnosis of smallpox was usually sufficiently accurate for surveillance purposes, and when it was discovered that laboratory diagnosis by the more sophisticated electron microscopy offered substantial advantages over traditional methods.]
- Improvement of the existing smallpox vaccine production laboratory in Nigeria such that it [can produce] vaccine of the multiple puncture type in quantities sufficient for Nigeria and other countries in the area.”
PREPARATION FOR THE CAMPAIGN, JANUARY-DECEMBER 1966
As might be expected in the development of a new programme of this magnitude, the preparatory phase, during January-December 1966, was characterized by hectic activity and administrative frustration. A director for the CDC regional office to be established in Lagos, Dr George Lythcott, was recruited early in 1966. He, with Dr Gelfand and Dr Ralph Henderson, travelled throughout western and central Africa drawing up programme agreements for each country. Such agreements, however, could not be formally signed nor could the procurement of supplies and equipment begin until the United States Congress had passed the act which appropriated the funds. Although this had been expected before 1 July, when the government’s fiscal year began, the Foreign Assistance Act of 1966 was not signed until 19 September. The difficulties in launching the programme were compounded by the fact that, within AID, the interval between the decision to implement field programmes and their actual commencement was usually 3 years, and the Agency’s procedures were geared to this pace. As time progressed, it became apparent that the single year allotted for preparation was unrealistic unless special measures were taken.
Fortunately, the recruitment of staff had been authorized and training could begin early in July 1966. Two basic categories of staff were recruited: medical officer-epidemiologists to provide overall assistance in programme development and execution, and non-medical personnel, termed “operations officers”, who would deal with logistics—including the maintenance and repair of vehicles and jet injectors, the distribution of supplies and equipment and the handling of financial matters. Priority was given to persons in their twenties and thirties, who were considered to be more likely than older individuals to have the stamina and interest required for extended work in the field. This also reflected the view of African health officials, who argued that they had a very limited need for advisers, in the usual sense of the term, but required, instead, individuals who were willing to participate actively in field operations. One operations officer was recruited for each country and 1 for each of the 4 regions in Nigeria. One medical officer was recruited for each Nigerian region, 1 for each of the larger countries, and 1 for every 2 or 3 of the smaller countries—i.e .,1 for Dahomey and Togo, 1 for Cameroon and Gabon, 1 for Chad and the Central African Republic, and 1 for the Gambia, Mauritania and Senegal.
The medical officers were primarily epidemiologists who had worked in the USA with CDC or who had had international health experience. The operations officers included 4 with experience as United States Peace Corps volunteers, the rest having played an important role in CDC’s domestic disease control programmes. The latter group, all of whom were university graduates, had received shortterm training in epidemiology and disease control and had proved their merit in field control programmes . Their experience in programme management and field investigations was to prove invaluable . Although the operations officers were initially not well accepted by some senior government health staff because they lacked a medical degree, they rapidly earned respect and, in many areas, eventually served as senior advisers. So impressive was their performance that WHO increasingly recruited such persons for smallpox eradication and other programmes.
During the spring and summer of 1966, a manual for field operations was prepared from which the WHO Handbook for Smallpox Eradication in Endemic Areas (SE/67 .5 Rev.1) was eventually adapted; other manuals dealing with the repair and maintenance of the jet injectors were prepared and tested in the field by Mr Morris; and orders were drawn up for the procurement of the necessary supplies and equipment.
Numerous problems were resolved during this period but a few of the more important and unexpected deserve mention. The licensing of smallpox vaccine for use in the jet injector caused one, wholly unexpected difficulty. CDC staff had assumed that the inoculation of vaccinia virus into the superficial layers of the skin by the jet injector’s highpressure spray achieved the same result as the administration of the vaccine by the scratch of a needle. However, in 1966, the agency in the USA responsible for biologicals—the Division of Biologics Standards—asserted that the vaccine specially produced for the jet injector had to be treated as a new product and because it was intended for parenteral inoculation, it must be sterile. Vaccinia virus, however, was then being grown—as it always had been—on the flank of a calf, and when harvested it inevitably contained some bacteria. Subsequent steps in manufacture diminished the number of bacteria to very low levels, and tests were performed to ensure the absence of pathogenic species. It was impossible, however, to produce a vaccine which could be stated with certainty to be free of all bacteria unless it were grown in tissue culture. Vaccinia virus could be grown in tissue culture, but at that time no laboratory had succeeded in producing such a vaccine which met WHO’s heat-stability requirements. The debate as to whether the vaccine for jet injection had to be sterile spread from the USA to WHO, where those concerned with biological standards also proposed that vaccine intended for jet injection should be sterile. Although there was agreement that the issue was one of principle rather than perceived risk, those concerned with biological standards insisted that principle should take precedence over all other considerations. Faced with the prospect of having a thoroughly evaluated method for vaccination which was vital to the new programme, but no vaccine, CDC staff carried the debate to higher administrative levels within the United States Public Health Service and the World Health Organization and finally were able to gain agreement that, in this case, principle would not prevail. However, considerable time and effort were spent on resolving the problem—at the expense of other urgent activities.
The vehicles and their spare parts presented a second problem. CDC decided that standard model pick-up trucks rather than customdesigned vehicles were preferable and less costly, and that the refrigerators required for the transport of measles vaccine could simply be bolted to the bed of the truck. The most desirable were British or French vehicles, which were in common use throughout western and central Africa. Spare parts for such vehicles were already widely available and local mechanics were familiar with their necessary maintenance and repair. AID procurement policies, however, required the purchase of vehicles made in the USA, and efforts by CDC to obtain a waiver of this requirement were unsuccessful. To alleviate the problems of repair, arrangements were made with the manufacturer for all of the programme’s professional staff to take intensive training in vehicle maintenance and repair. Spare parts had to be procured and specially stockpiled in all countries, but which spare parts and in what quantities was another question, since, curiously, neither the manufacturer nor the various agencies working in Africa, including WHO and UNICEF, had compiled a list of needed spare parts based on field experience. There was no option but to make a “best-guess” estimate of which spare parts to stock and, as might be expected, requirements only roughly approximated available stocks. Over time, and with special assistance from the manufacturers, the design of the vehicles was improved, special repair facilities were established and an effective transport system was ensured.
One of the most contentious problems related to the question of which of two measles vaccines should be procured the Edmonston strain vaccine, which was produced by one manufacturer and which had been used since the 1961 campaign in Upper Volta, or a more recently licensed, more attenuated product, the Schwarz strain vaccine, produced by another manufacturer. The Schwarz strain vaccine resulted in less frequent and less marked febrile responses, but the initial antibody levels induced were lower (Krugman et al .,1965). The available evidence indicated that the two vaccines conferred comparable immunity but some investigators suggested that immunity following the use of the Schwarz vaccine might not be so long-lasting. Investigators in Senegal and Nigeria (Hendrickse et al .,1965) had evaluated the Schwarz strain vaccine and argued that it was the more desirable, given the fact that it would be administered to ill and malnourished children among whom the higher fevers caused by the Edmonston strain vaccine might be harmful. A number of African countries, however, encouraged by the manufacturer’s travelling sales representative, requested the Edmonston strain vaccine. Even the New England journal of medicine (1965) entered the dispute, stating in an editorial,” . . . it may be wise, at least under circumstances such as exist in these countries [of western Africa], not to adopt other vaccines [other than the Edmonston strain vaccine] until the results of future studies become available”. The manufacturer translated the editorial into French and circulated it widely in Africa, and eventually obtained support for the product from many United States legislators. One alternative for CDC was to permit each country to decide for itself which strain of vaccine would be used. However, CDC staff not only considered the Schwarz strain to be preferable, but for logistic reasons believed it important to employ only one type of vaccine. Eventually, the issue was decided by the United States Surgeon General, and ultimately all countries were persuaded to accept the use of this strain (which became routinely used). As with the standards for smallpox vaccine for use in the jet injector, the issue was satisfactorily resolved, but again at the expense of considerable time and energy.
The training programme began in July 1966. A month-long course in basic field epidemiology and biostatistics was followed by a month of specialized training which covered subjects ranging from the history and socio-cultural characteristics of western and central Africa to the maintenance and repair of vehicles and jet injectors. To foster collaboration with WHO, the WHO advisers in Africa, Ladnyi and Dr Hans Mayer, were invited to participate during the first month of the course. When the course ended, however, the staff had to remain in Atlanta, housed in temporary and crowded quarters, because none of the national agreements had yet been signed.
Many discussions with governments about the programme had been conducted during the spring and summer of 1966 but, as has been noted earlier, formal agreements could not be signed at least until September. Nigeria was of the highest priority because of its size and because it was to serve as the site of the regional office. Nearly half the complement of technical staff were expected to live there. Nigeria, however, was then on the brink of civil war. A military coup in January 1966 had displaced the existing civilian authority, and 7 months later, a second coup coincided with an army mutiny in the north, during which thousands of Ibo tribesmen were killed. The Ibos, whose tribal home was eastern Nigeria, threatened to secede and to establish an independent nation. The signing of an agreement for a smallpox eradication-measles control programme was not high on the list of the government’s priorities. For many weeks, it appeared that the regional programme might well be doomed, as the United States Ambassador and the WHO Representative endeavoured, unsuccessfully, to obtain the agreement of the Nigerian government. Finally, Dr Lythcott flew to Nigeria to ascertain what might be done. The documents had been approved by the Minister of Health and awaited only the signature of the head of state. During a 6-week period, Dr Lythcott, too, was unsuccessful in working through conventional channels but, at a social function, he was introduced to the President’s fiancee. He explained the programme and the nature of his mission to her, and on the following day, the agreement was signed.
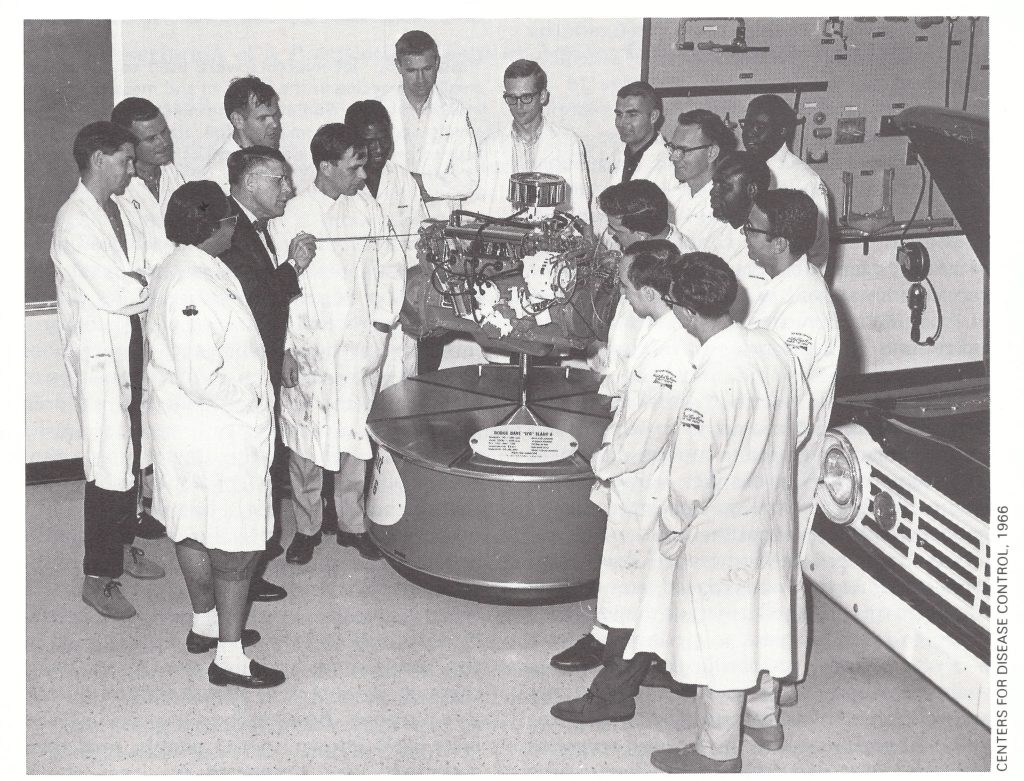
Plate 17.4. CDC field staff received training in the maintenance and repair of vehicles in Atlanta before taking up assignments in western and central Africa. Clockwise from lower left: Margaret E. Grigsby, Ralph H. Henderson, Gordon E. Robbins, a vehicle maintenance instructor, Stanley O. Foster, Thomas Drake, E. Ademola Smith, William H. Foege, David Thompson, Donald Moore, Deane L.Hutchins, Hillard Davis, unidentified, Arlen Rosenbloom, Pascal Imperato, Bernard Lourie, Christopher D’Amanda.
Nigeria’s agreement, though it was crucial, was only one of 16 which were needed. In other countries, various problems delayed the signing of the programme agreements, and not until March 1967 was the last of these finalized. Agreement in principle to undertake a programme of smallpox eradication and measles control was more readily achieved than agreement on specific operational plans. CDC staff had envisaged a similar type of programme in all countries in principle, an elaboration of the special mass vaccination campaign against measles. Mobile teams would use jet injectors in the administration of smallpox vaccination to everyone in the population, while measles vaccine would be given to children between 6 months and 4 years of age (Henderson, 1967). Expectations as to the extent of coverage to be achieved were modest—80% of the population in urban areas and perhaps 60% in peripheral areas. Important additional components, not then familiar to any of the countries, were the provision of independent assessment as a quality control measure to determine vaccine coverage and the success of vaccination, as well as a surveillance system utilizing detection sites such as hospitals and aid posts to measure progress in eliminating smallpox.
In countries in which mobile teams had previously been little used, or in which such teams had largely ceased to function, the plan was adopted with few changes. In most of the former French colonies, however, multipurpose mobile prevention units, often referred to as “prospection teams”, were well established. As the teams moved from village to village on a planned itinerary they endeavoured to reach all parts of a country over a 2-3 year period, vaccinating the inhabitants against smallpox and sometimes tuberculosis and yellow fever and examining an average of 400-500 persons a day for leprosy, trypanosomiasis, yaws and (where the disease was present) onchocerciasis. The programmes, as well as many of the mobile units, were usually directed by French military medical officers. In these countries, separate programmes for smallpox and measles vaccination were seen to be wasteful of petrol and trained personnel. CDC staff, however, considered that the integration of the two programmes would present a problem because it would compromise the speed and efficiency of operations afforded by the jet injectors. In a population of 500, for example, fewer than 100 children would be of a suitable age to receive measles vaccine, a number barely sufficient to warrant the use of the injectors. A second problem was that the health officials in these countries saw no need to provide special teams to assess the results of the programme. Participation in the multi-purpose programmes was encouraged in most countries by giving individual certificates to persons examined and vaccinated by the teams, and by subsequently requiring these documents to be shown for administrative purposes. Because the prospection teams were well known to the people, and their activities were supported by local chiefs, health officials believed that no assessment was required other than to compare the numbers vaccinated by the teams with the estimated population in the area. A third problem was the reluctance of most authorities to divert resources to improve reporting or to investigate cases of smallpox. This was considered to be wasteful because of the common view that the best that could be achieved was the control of smallpox as well as of measles; if a few cases of smallpox did occur they were thought of little consequence in the total context of health problems.
Compromises in the basic strategy were required. Support from the Secretaries-General of OCCGE and OCEAC—Medecin-General Pierre Richer and Colonel Rene Labusquiere, respectively-helped to resolve many problems. In the OCEAC countries, the smallpox eradication and measles control programmes were eventually fully integrated into the activities of the prospection teams (see box). In Upper Volta, the prospection teams continued to give smallpox vaccine but different mobile teams were created to give measles vaccine. In Cote d’Ivoire, separate measles vaccination teams and smallpox vaccination teams were formed (Table 17.3). In the other OCCGE countries, it was decided that special teams would conduct both smallpox and measles vaccination.
Few of the countries at first agreed to accept the provision of special teams to conduct independent assessments of smallpox vaccination coverage and takes. By the end of 1967, only 6 countries had created such teams—Dahomey, Ghana, Mali, Niger, Nigeria and Togoalthough eventually 4 others did so—Chad, Gambia, Guinea and Sierra Leone. At the start, there was even less interest in smallpox surveillance, which fell by default to CDC advisers until late in 1968. Fortunately, assessment and surveillance were best accepted in the countries in which smallpox was the greatest problem.
Plate 17.5. Jet injectors were used to administer smallpox vaccine in the left arm and measles vaccine in the right arm. Sometimes the injections were given simultaneously. Aluminium foil covers the vaccine vials to prevent the inactivation of virus by exposure to light.
Table 17.3: Western and central Africa : smallpox vaccination team operations in the attack phase (as at May 1969), by countrya
a Based on Millar & Foege (1969).
b ..=data not recorded.
c Smallpox vaccine only administered by prospection teams.
When the first programme plan had been developed, in January 1966, it had been projected that “smallpox cases should cease by the end of the fourth year of the programme”—i.e.,by December 1970. In the autumn of 1966, projections were made as to the numbers of reported cases of smallpox which might be expected up to the end of the programme. This was done in the expectation that, with better recording, the reported incidence might actually rise during the first year of operations, thus generating concern on the part of the responsible administrators as to the effectiveness of the programme. Anticipating this problem, Henderson and his colleagues prepared a graph depicting the expected numbers of reported cases throughout the duration of the programme (Fig. 17.2). The graph is of interest, since the predicted incidence up to the end of 1968 was surprisingly close to what was actually fund, but thereafter the results were substantially better than expected, one of the few occasions in which progress in the Intensified Smallpox Eradication Programme exceeded expectations.
One by one the programme agreements were signed, and personnel, supplies and equipment gradually began to arrive in western and central Africa. By March 1967, 16 months after the USA’s decision to offer assistance, pilot projects had begun in 11 of the countries and a total of 2.5 million smallpox vaccinations had been recorded.
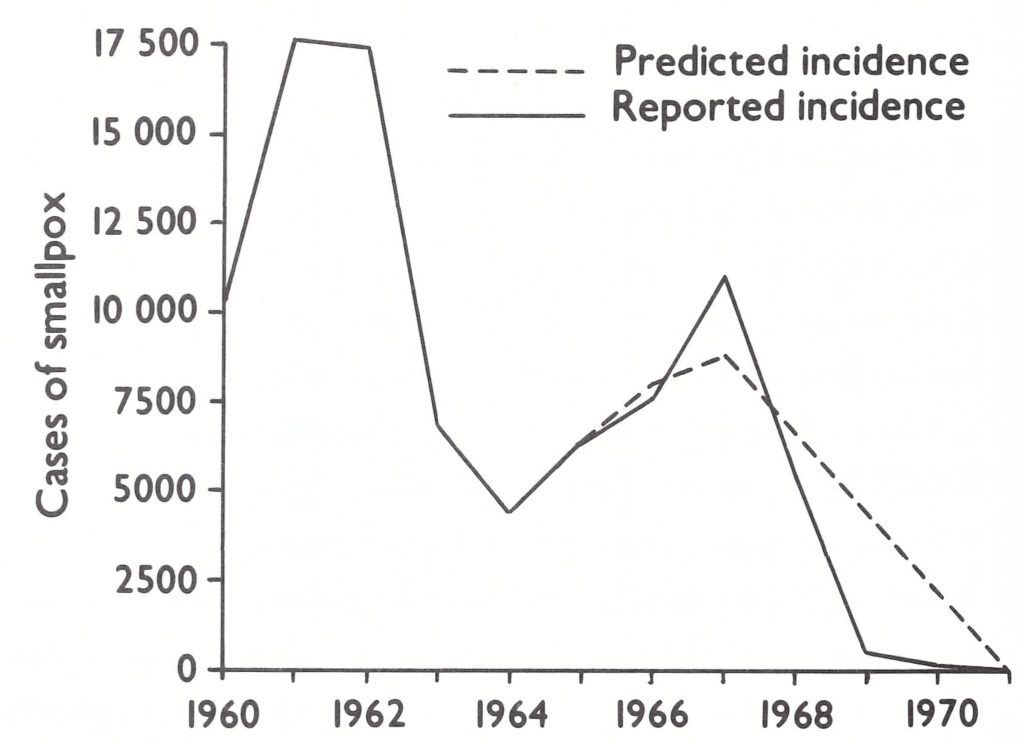
Plate 17.2. Western and central Africa: number of reported cases of smallpox compared with the numbers predicted in September 1966.
Description of a Prospection Team in Action, Central African Republic
From a 1967 field report by Dr Ralph Henderson and Mr Neal Ewan :
"The team began its activities around 7.30 a.m. Zinga and an adjoining village were to be prospected' that morning. First, all the children between 6 months and 4 years of age were formed into a line and given measles vaccinations. They were tallied by age and sex as they received their shots. This procedure required about one-half hour and took place with minimal difficulty.
"The team leader then requested the village to form into a line of males and a line of females. Each line then passed in front of a recorder, who tallied age and sex, and handed each person a metal tag from a box containing tags consecutively numbered from 1 to 1000. The line then moved through a small tent where a nurse performed a screening physical examination, particularly looking for trypanosomiasis, onchocerciasis, leprosy, and yaws. After passing through the tent, the line passed in front of the smallpox vaccination station, where everyone except infants under 3 months and pregnant women was vaccinated using the scratch technique. The line next moved to a table where each metal tag was collected, and yellow OCEAC cloth health certificates were given out, stamped with rougeole (measles) and/or variole (smallpox) and the date, and filled out with the person's name. People were then either dismissed or proceeded to one or more of three additional sites. Blood, sputum and stool specimens were obtained from suspects referred by the nurse performing screening physicals. The nurse concerned prepared slides to be read by one of two microscopists. Trypanosomiasis and onchocerciasis suspects were referred directly to the microscopists, who made their own slides from fluid and tissue obtained by placing a clean needle into suspected cysts or ganglions and wiggling it.
"The team leader then requested the village to form into a line of males and a line of females. Each line then passed in front of a recorder, who tallied age and sex, and handed each person a metal tag from a box containing tags consecutively numbered from 1 to 1000. The line then moved through a small tent where a nurse performed a screening physical examination, particularly looking for trypanosomiasis, onchocerciasis, leprosy, and yaws. After passing through the tent, the line passed in front of the smallpox vaccination station, where everyone except infants under 3 months and pregnant women was vaccinated using the scratch technique. The line next moved to a table where each metal tag was collected, and yellow OCEAC cloth health certificates were given out, stamped with rougeole (measles) and/or variole (smallpox) and the date, and filled out with the person's name. People were then either dismissed or proceeded to one or more of three additional sites. Blood, sputum and stool specimens were obtained from suspects referred by the nurse performing screening physicals. The nurse concerned prepared slides to be read by one of two microscopists. Trypanosomiasis and onchocerciasis suspects were referred directly to the microscopists, who made their own slides from fluid and tissue obtained by placing a clean needle into suspected cysts or ganglions and wiggling it.
CHARACTERISTICS OF WESTERN AND CENTRAL AFRICA
The estimated 110 million population of the 19 countries included in the programme in 1967 inhabited a diverse ecological area ranging from humid tropical coastal areas with prolonged rainy seasons to rolling savanna and eventually to the vast, sparsely populated and arid Sahel, whose vegetation consisted of thorny scrub and stunted trees (Plate 17.6). Subsistence farmers formed the largest proportion of the population. Christians and animists lived primarily in the coastal areas; Muslim herders inhabited the Sahel. Tribes numbering from less than 100 000 persons to many millions, each with its own language, culture and customs, had traditional boundaries, often overlapping one or more national frontiers. In the process of evolving into nation-states, most countries experienced clashes between the new and the established and between religious, traditional, military and civilian leaders. Changes of government occurred frequently.
Paved roads provided limited links between coastal cities and some inland towns, but few connected the major capital cities. In the savanna, most unpaved roads were made of laterite, with a washboard surface that took a heavy toll of vehicles; in the coastal areas, there were clay roads, which were dusty during the dry season and a morass of mud during the rains. Railways were few and frequently out of order. Air transport connected many of the major cities and towns but schedules were followed erratically. Travel between one capital and another was sometimes more readily accomplished by flying by way of London or Paris. Similarly, telephone and telegraph links were generally few, and it was often easier to communicate with other countries through London or Paris.
The inhabitants of western and central Africa were inveterate traders and, despite poor roads, many travelled long distances to buy and sell cattle, textiles, salt, gold and other products. Local markets played an important role in commerce and as social centres. Some were held weekly, others at intervals of 4, 5 or 8 days. Herdsmen moved regularly across the Sahel seeking grazing areas and migrant labourers from the Sahel moved seasonally to coastal and savanna areas to harvest crops. Rapidly increasing urbanization characterized the entire area, the population of Abidjan (Cote d’Ivoire), for example, growing from 5000 in 1921 to 180 000 in 1966 and the population of Lagos (Nigeria) from 100 000 to 665 000 during the same period.
National administrative structures largely reflected the legacy of the previous British and French colonial administrations. In the former British colonies, the authority of the tribal chiefs had been supported and fostered within a decentralized civil structure ; in the former French colonies, however, the power of the traditional chiefs was largely subordinated to that of the civil service and a strong centralized government. For the smallpox eradication-measles control programme, the support of the principal chiefs in the former British colonies was therefore as vital as that of the civil authorities; in the former French colonies, the civil service and village leaders provided the essential link with the people. The governmental structure was different in Guinea and Mali, where the authority of a national political party superseded that of traditional leaders. In both countries, the parties greatly facilitated contact with the villagers.
Approaches to the provision of health services also differed, depending on the colonial tradition. In the former British colonies, rural dispensaries operated by African personnel provided basic drugs and sometimes vaccine, but they were rather few and far between and their efforts were devoted primarily to curative medicine. The establishment of mission clinics and hospitals was encouraged, however, and in some areas these were quite numerous. In the former colonies of France, in contrast, health services were more widely available, through the use of mobile multi-purpose prospection teams. The system, conceived during the 1920s by Dr Eugene Jamot, had first been used to control trypanosomiasis in Ubangui-Shari (later the Central African Republic), but the teams’ duties were gradually expanded to include the prevention and treatment of other diseases; in time, similar teams were organized throughout French West Africa and French Equatorial Africa (Richet, 1965; Cohen, 1971). The Service des Grandes Endemies, as the mobile service was called, provided basic health services in rural areas, supported by dispensaries, which served as treatment centres for patients referred by the mobile teams. The establishment of mission clinics and hospitals had not been encouraged and therefore not many existed . After the colonial period, health services continued to be supported in most countries by French bilateral assistance. Mobile teams were also used in some of the former British colonies for yaws control and occasionally for smallpox vaccination, but, except in Ghana (Waddy, 1956), they did not operate throughout the entire country.
Thus, in a number of the countries of western and central Africa, a structure and/or tradition existed for executing large-scale vaccination campaigns. Systems for the notification and investigation of cases, however, were poorly developed.
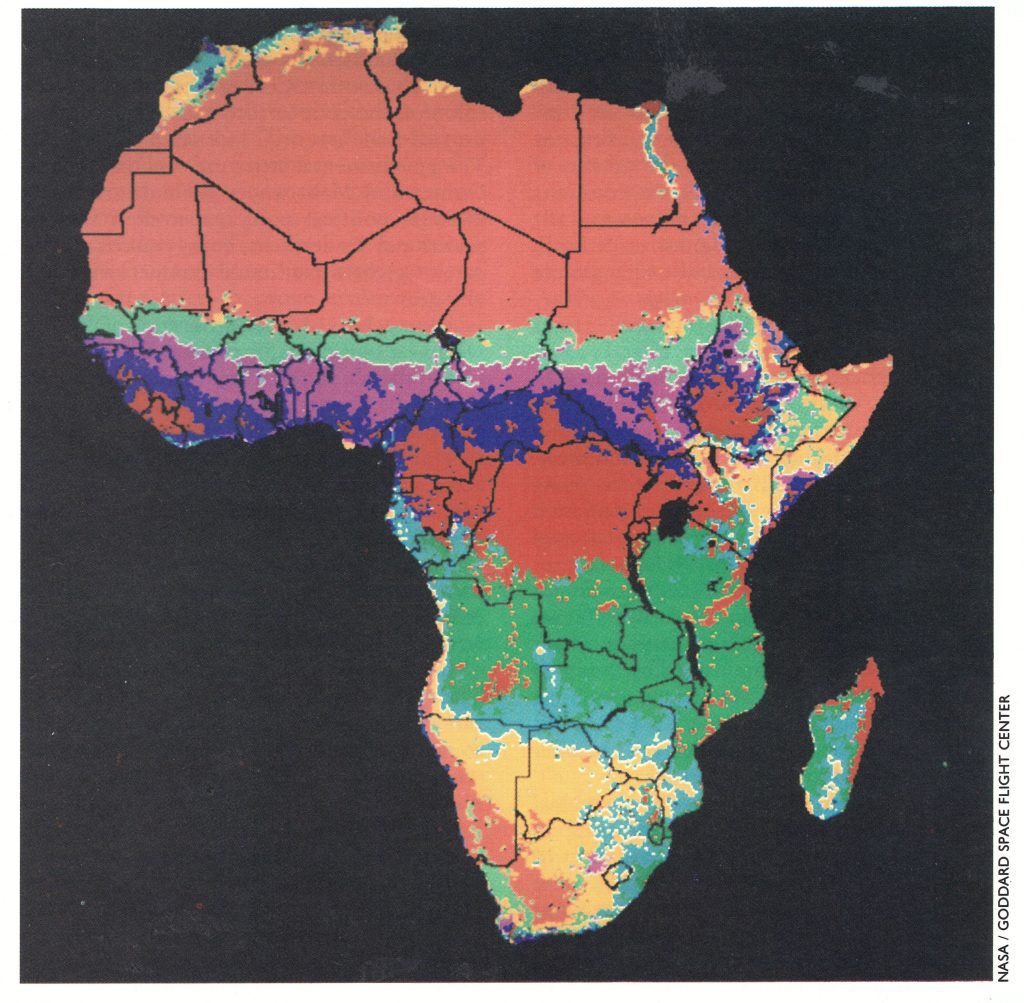
Plate 17.6. Principal land cover components of Africa. The types of vegetation present in different parts of Africa were important in population distribution. Maps developed from satellite observations using very high-resolution radiometer sensors were prepared in 1982 (Tucker et al ., 1985); the situation they show was probably not significantly different from that in 1967. The tan areas are desert and semi-desert, the light green are semi-arid wooded grassland, and the light blue are bushland and thicket; all these areas were sparsely populated. The purple areas are woodland and grassland, the dark green are woodland and the yellow are wooded grassland and thicket. The dark blue areas are interspersed tropical forest and grassland, and the red are tropical rainforest and mountain forests; the latter areas were more densely populated.
PLANS FOR THE PROGRAMME
With only 13 months allotted before the commencement of field operations, and with available personnel fully committed to working out the logistics, CDC staff had had no time to undertake feasibility studies, pilot projects or field reconnaissance to determine the extent of vaccinial immunity or to assess the epidemiology of smallpox or measles. A number of assumptions were made, some of which were later to prove erroneous. For example, it was assumed that vaccinial immunity was uniformly low throughout the region but, in fact, urban populations were later found to have been moderately well vaccinated, as were the inhabitants of large rural areas in some francophone countries. Especially low levels of vaccinial immunity were observed, however, throughout northern Nigeria, in many parts of Sierra Leone and in the more isolated rural villages in most countries. It was also believed that cases of smallpox would be found to be widely dispersed in all countries but, in fact, 10 out of the 21 countries in the region were found to be free of smallpox or nearly so by 1967. Where smallpox incidence was high, cases and outbreaks tended to be concentrated in specific geographical areas. It was also assumed that, as in Asia, the densely populated cities and market towns would constitute the major reservoir for the sustained transmission of disease, with spread occurring from these foci to rural areas (Henderson, 1967). It was discovered, however, that comparatively few cases occurred in urban areas but rural areas were found to be capable of sustaining transmission over surprisingly long periods.
CDC staff viewed the eradication of smallpox as a feasible objective given its epidemiological characteristics, but less was known about measles, since it was not routinely reported in most countries. However, control rather than eradication was foreseen because of the greater communicability of measles, especially in Africa (Morley, 1962; Senecal et al.,1962), the greater difficulty of clinical diagnosis and the fact that the disease had not been eliminated in any country, as of 1967, even in those with well-developed health services. Whether the objective of the programme should be defined in terms of the control of measles or its eradication had been debated at length. AID staff thought it preferable to establish eradication as an objective, believing that even if it was not achieved, more substantial progress would be made. CDC staff were concerned lest the enunciation of a goal which might prove to be unrealistic, as had been the case with malaria eradication (see Chapter 9), would only serve to erode further the credibility of public health professionals. Eventually, the CDC position prevailed and so the programme bore the somewhat clumsy title of “smallpox eradication-measles control” rather than the simpler “smallpox and measles eradication.” As the programme was to demonstrate, effective measles control, let alone eradication, was a formidable task (United States National Communicable Disease Center, 1970; Foege & Eddins, 1973).
The planning process would unquestionably have benefited if more information had been available regarding the incidence of both smallpox and measles and the capacities of each of the national health services, but the seeking of such information would have caused a delay of perhaps 12-18 months. With many commitments already made, so long a delay was not acceptable. Moreover, because of possible changes of government staff and of priorities, there was no guarantee that a better-defined project would subsequently be approved for funding. Thus, with the resources at hand, there was a need to act. Consequently, the project began without preparatory studies, employing such information as was available; a great many assumptions were made in the hope that an able and energetic staff would solve problems as they arose.
It was recognized that the different characteristics of the administrative, health and social structures in each of the countries would dictate somewhat different types of programme. Therefore, instead of a highly prescriptive plan, four principles were formulated for the execution of the national programmes in the expectation that during the first year they would evolve by trial and error (1) the programmes would be coordinated as a regional effort because of the ready movement of people across national borders; (2) freeze-dried vaccine would be administered by mobile teams employing jet injectors in order to economize on scarce resources; (3) independent assessment of the vaccination campaign would provide a quality control mechanism; (4) a workable surveillance programme would be developed on the basis of regular reporting from case-detection sites, because, as had been stated, “The goal of the project is a specific one, the reduction of smallpox to the level of zero cases” (Henderson, 1967).
Surveillance, as a principle, was a characteristic which differentiated this from previous smallpox eradication programmes and eventually proved to be critical to its success. It was a concept that had been fostered by Dr A. D. Langmuir at CDC (see Chapter 9); since 1961, CDC’s surveillance programme had been under Henderson’s direction. With respect to smallpox, it was defined in the following terms (United States Communicable Disease Center, 1966) :
- The routine, systematic collection of data, amplified appropriately by special field investigations and studies.
- The analysis and interpretation of reported data and studies on a concurrent basis.
- The initiation of appropriate definitive action, including field investigation, epidemic control, modification of operational campaign procedures, and recommendations regarding vaccination.
- Widespread dissemination of the compiled and interpreted data to principal reporting sources and to others concerned with disease control activities.
As has been noted earlier, the concept of surveillance was unfamiliar to health staff in western and central Africa and it was thought that not less than 2 years of sustained effort would be required to develop a surveillance system. The CDC Manual of Operations (United States Communicable Disease Center, 1966) pointed out the need to begin the development of a notification system from the inception of the programme but did not then envisage the obligation to investigate and contain all the outbreaks that were detected. As the manual stated:
“In countries with a high endemic occurrence of disease, field investigation activities may focus on comparatively few of the many outbreaks. As systematic vaccination programs progress, the importance of small outbreaks and individual cases becomes increasingly important. As the numbers of cases diminish, the field investigation and control procedures should be instigated for an increasing proportion and, ultimately, for all cases.”
Three stages in the development of the surveillance programme were envisaged:
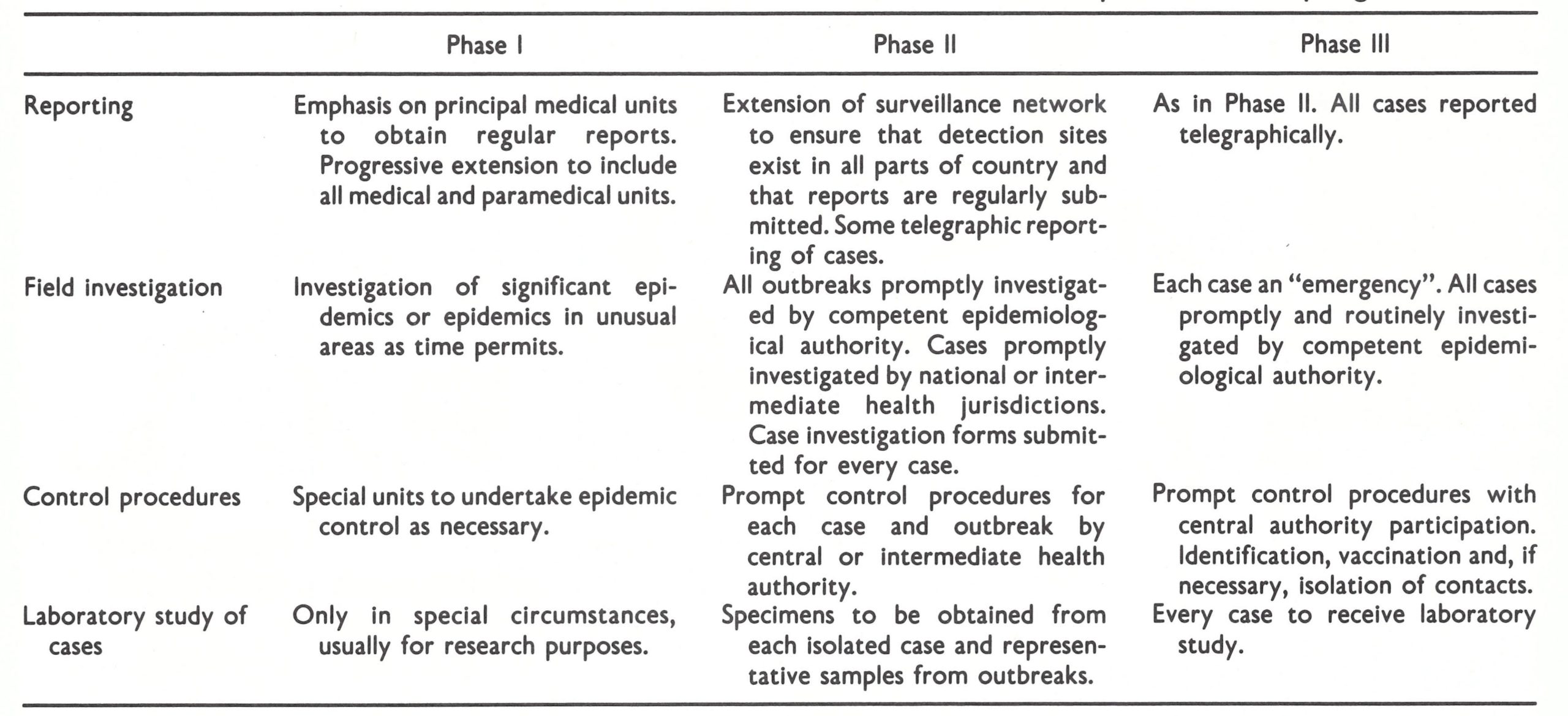
PHASE I—Referring to endemic areas with a sustained or frequent high incidence of smallpox as indicated either by official reports or by educated estimates. This would include all countries with a rate of perhaps 1 or 2 cases or more per 100 000 population per year.
PHASE II—Referring to countries with a low continuing incidence of smallpox.
PHASE III—Referring to areas rendered non-endemic by systematic vaccination. No country or subdivision would be classified in Phase III until it had been covered by the attack phase of systematic mass vaccination.
Strategically, surveillance and containment activities in most countries were initially considered as subsidiary to mass vaccination, serving primarily to identify problems or weaknesses in the mass vaccination campaign. When the number of cases had been substantially reduced by the vaccination campaign, surveillance and containment would become essential to eliminate residual foci. The activities deemed appropriate for each phase of the programme are listed in Table 17.4. On the basis of the reported incidence in 1966, Phase I activities were called for in at least 6 of the countries—Dahomey, Mali, Niger, Nigeria, Sierra Leone and Togo.
Table 17.4: Western and central Africa: surveillance activities at different phases of the programmea
 a From United States Communicable Disease Center (1996).
a From United States Communicable Disease Center (1996).
EXECUTION OF THE PROGRAMME
The first year of the programme was to be devoted to formulating logistic plans, training national staff, and evaluating methodologies for adaptation by both national and CDC personnel. Although it was inevitable that the development of a programme of this magnitude would encounter substantial problems, their extent had not been anticipated. The solution of these problems by CDC ultimately became the responsibility of Dr Millar, who returned from study leave in the summer of 1966 and assumed direction of the programme on 1 November, when Henderson went to Geneva to head WHO’s Intensified Smallpox Eradication Programme.
By September 1966, the recruitment and training of staff had been completed as scheduled, but little else was proceeding as planned. The procurement of supplies and equipment lagged far behind schedule and formal agreements with countries were slow to be concluded. Two countries refused to sign programme agreements until they had been formally assured that WHO would provide funds for fuel supplies and travel; several objected to the requirements for surveillance; another expressed concern about budgetary obligations; in Upper Volta, in which the measles control programme had first been successfully conducted, the director of the endemic diseases control service refused to endorse the programme on the grounds that smallpox eradication could not be a Phase III 871 As in Phase II. All cases reported telegraphically. Each case an “emergency”. All cases promptly and routinely investigated by competent epidemiological authority. Prompt control procedures with central authority participation. Identification, vaccination and, if necessary, isolation of contacts. Every case to receive laboratory study. achieved. Continuing discussions eventually led to the signing of 3 agreements in October, 4 in November and 3 in December. The last to be signed were those in the Gambia, Senegal and Upper Volta, in March 1967.

Plate 17.7. Health workers of Dahomey’s endemic disease control service at a training course on the use of jet injectors, March 1967.
Each national programme experienced different types of problems and each had to be adapted to the health structure and social context of the country concerned. As programmes progressed, epidemiological observations and useful techniques for field operations were communicated from one to another through annual meetings of national directors and CDC advisers, through the travel of staff based in Lagos and Atlanta and through periodic surveillance reports which were sent to programme staff in all countries. To attempt to present events throughout the region in chronological order is difficult and confusing, given the number of different national programmes. Accordingly, we shall first describe progress in the programme as a whole before commenting on the salient features of individual national programmes.
In most of the countries, field operations commenced between January and June 1967; in the others, for which assistance had been postponed for a year—Guinea, Liberia and Sierra Leone—these operations had all begun by January 1968.
The proposed method of operation in each of the vaccination campaigns drew extensively on the experience of Dr Harald Frederiksen, a United States adviser to an earlier successful smallpox vaccination campaign in Bolivia (Frederiksen, 1962). It called for vaccination of the population at assembly points. This was achieved through preparatory meetings with local chiefs and civil auth-‘orities to explain the programme and to solicit their help. Such meetings took place 1 to 7 days before the vaccination team arrived. The assembly points were usually selected so that no one would have to walk more than 8 kilometres, although, in some areas, even this distance was found to be too great and it was decreased to 3 kilometres. The teams usually E consisted of 5 or 6 persons—as many as could o 60-conveniently ride in one vehicle. They vaccinated all persons against smallpox and o children between 6 months and 4 years old a 40-against measles. Although on some days as many as 10 000-14 000 persons could be vaccinated, on average the teams administered between 750 and 3000 smallpox vaccination daily (Millar & Foege, 1969) and about one-fifth of this number of measles vaccinations. The teams usually worked for a consecutive 3-week period, camping out or staying in the villages. As experience demonstrated, living among the local population fostered cooperation and improved vaccination coverage. At the end of the 3 weeks, 7-10 days were set aside for rest and recuperation.
Jet injectors were used for most vaccinations, but in small villages and among special groups, smallpox vaccine was administered by bifurcated needle. Most people readily accepted vaccination, although resistance was encountered in Dahomey, Togo and south-western Nigeria, where an animist cult was active among some small groups, and in scattered, remote areas. In each instance, special efforts were made to persuade village and religious leaders of the benefits of vaccination-usually, but not always, with success.
In urban settings, the vaccination campaign required special planning and the provision of many more vaccination assembly points. In Nigerian towns, it was calculated that one assembly point would be required for every 8000 persons and that arrangements would have to be made for vaccination in the early morning and late afternoon (Smith et al .,1970). The most intensive urban campaign was that conducted in Ibadan (Nigeria), in which, over a 10-day period, 12 teams administered 757 308 smallpox vaccinations and 69 069 measles vaccinations. People connected with the university, local churches and private voluntary organizations, as well as members of the police force, assisted in the effort.
The pace of the vaccination campaign gradually accelerated. By January 1968, a special ceremony in Ghana marked the 25 millionth vaccination and by the summer of 1968 (Fig. 17.3), the numbers vaccinated had reached the optimistic estimates of January 1965.
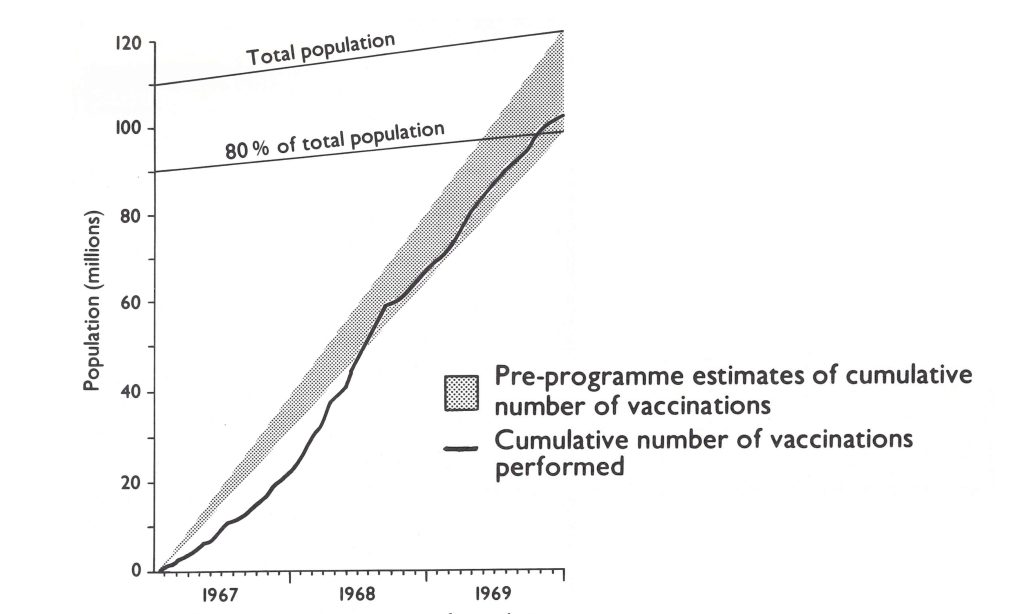
Plate 17.3. Western and central Africa: cumulative number if vaccinations performed compared with pre-programme estimates. (From Foege et al.,1975).

Plate 17.8. William Stewart, Surgeon General of the United States Public Health Service, attended a special ceremony in Ghana, in January 1968, to celebrate the 25 millionth vaccination given. George Lythcott (b .1918), with sunglasses, was Director of the CDC regional office in Lagos from 1967 to 1972. An able and diplomatic administrator, Lythcott played an important role in sustaining the momentum of the programme through many political and logistic crises.
The concurrent assessment of coverage, although deemed essential, was conducted in only 9 of the countries. The principal objection to assessment was that it wasted resources. Where it was performed, teams of 2 or 3 persons visited a random sample of 5-10% of the villages whose inhabitants had been vaccinated 4 10 days previously to ensure that the proportion of successful vaccinations was satisfactory and that coverage was adequate. Where coverage was found to be low, a repeat vaccination campaign was organized. Assessment data showed that good coverage was achieved in most countries (Table 17.5).
To ascertain the overall efficacy of the vaccination campaign, special surveys were conducted in 1968 in 5 areas Dahomey, Niger, northern Nigeria, western Nigeria, and Togo under the direction of Dr Ralph Henderson, then deputy director of the Lagos regional office (Henderson et al .,1973). With Mr Donald Eddins and Dr William Foege, he devised for the purpose of this survey a practical method of cluster sampling based on principles elaborated by CDC statisticians for immunization surveys in the USA (Serfling & Sherman, 1965). (The method was later adapted for use in WHO’s Expanded Programme on Immunization, in nutrition surveys and in other health status assessments.) “The survey revealed a generally satisfactory performance in most programmes. Nearly 80% of the people questioned reported having been vaccinated with jet injectors (Table 17.6). The low rates among those under 1 year of age could largely be accounted for by children born after the mass campaign ; lower rates among those over 45 years were attributable to the fact that a number of older people had declined to be vaccinated, believing (correctly, in most instances) that they were already immune owing to previous disease or repeated vaccinations. The best results were obtained in northern Nigeria, in which cooperative, authoritarian emirs and district chiefs directed their subjects to accept vaccination; the lowest rates were found in western Nigeria, which lacked the tradition of authoritarian leadership and in which no concurrent assessment had been conducted.
Special comment is called for regarding the results obtained among children aged 0-4 years in Niger and northern Nigeria. In these areas, the proportion with a vaccination scar acquired at any time was lower than the proportion reported to have been vaccinated with the jet injector. This paradox can be partly explained by the possibility that some of the vaccinations by jet injector might have been unsuccessful or that parents might have reported that vaccinations had been performed when they had not. Because the surveys were conducted many months after the campaign, it proved impossible to determine the cause or to remedy the situation.
Of particular interest was the much higher proportion of persons in northern Nigeria with facial pockmarks, confirming a growing suspicion that this was the principal endemic focus of smallpox in western and central Africa.
Table 17.5: Western and central Africa: selected coverage figures for countries carrying out systematic assessment, 1969, by agea,b,c
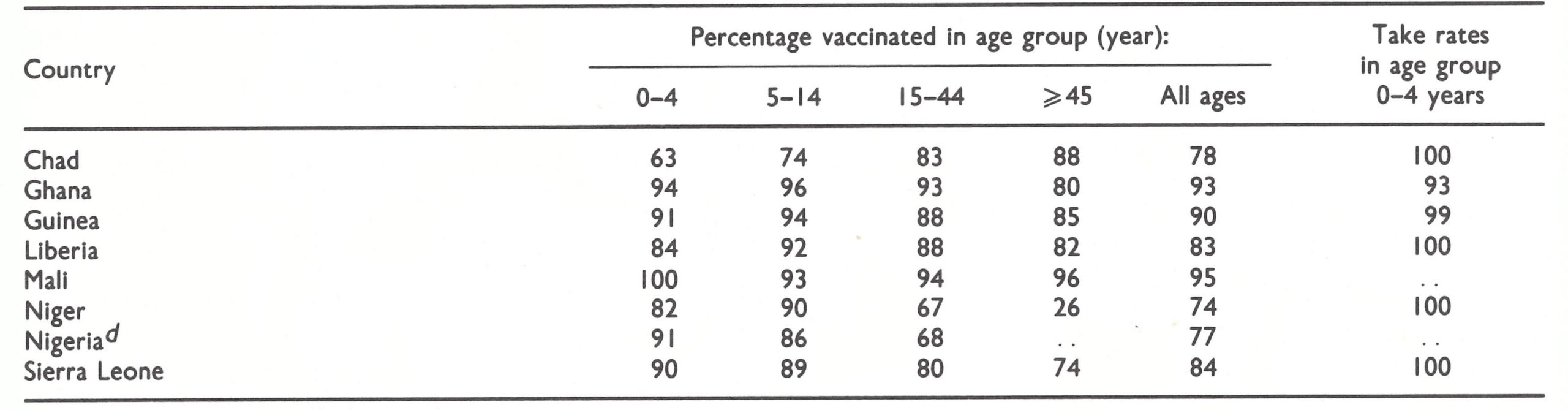 a Based on Milar & Foege (1969).
a Based on Milar & Foege (1969).
b ..=data not recorded.
c Assessment was also carried out in Togo, butno data are avaiable.
d Data for Gombe town, North-eastern State, in age groups 0-3, 4-14, and > 15 years.
Table 17.6: Western and central Africa: results of cluster sample surveys in five areas, 1968-1969: (A) by age; (B) by country or area
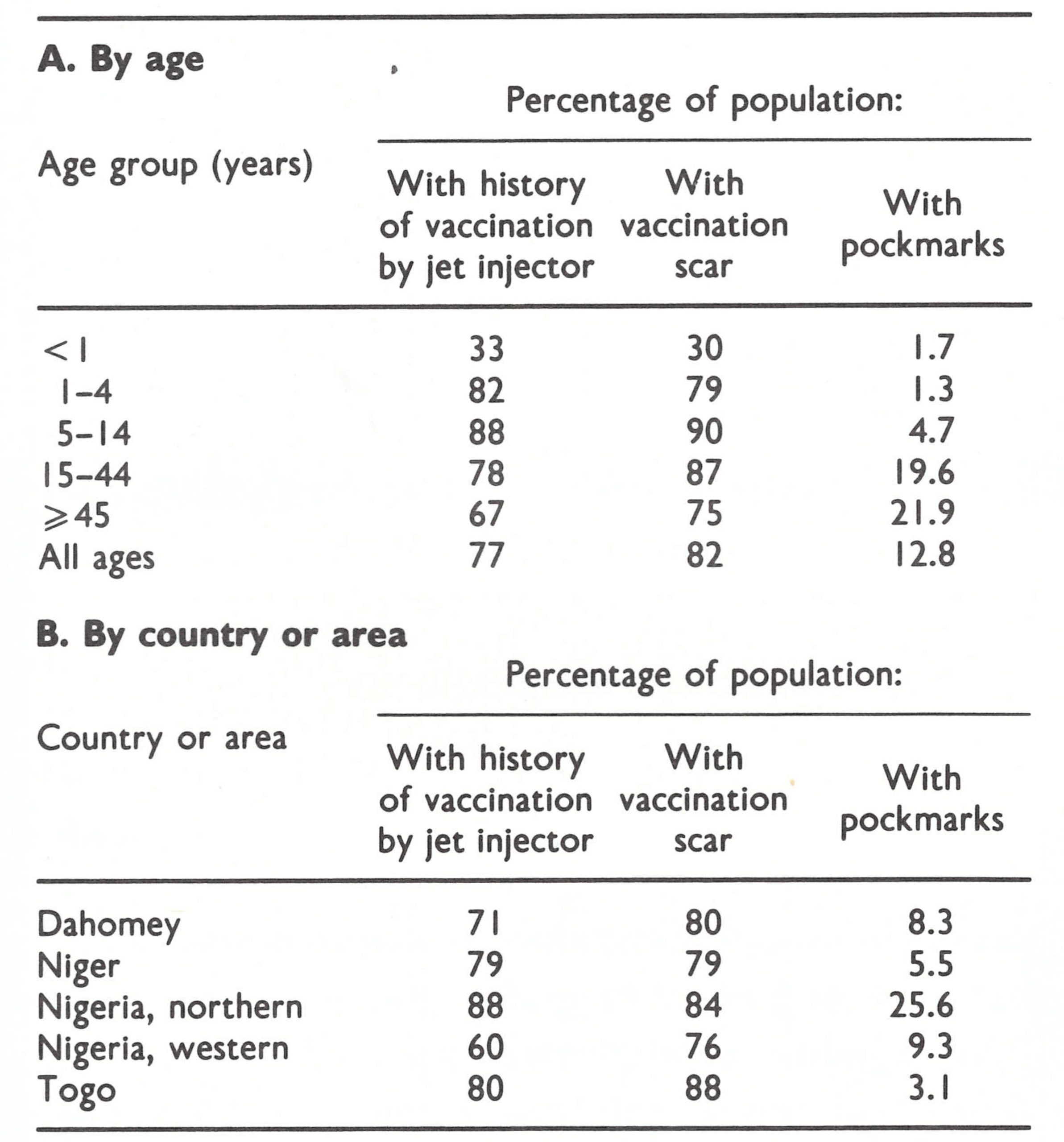
Coordination With International Organizations
Throughout the course of the programme, beginning with the initial planning visits, efforts were made by CDC staff to develop a collaborative working relationship with WHO through its Regional Office for Africa, the WHO representatives in the respective countries and two WHO smallpox advisers based in western Africa—one in Mali and the other in Liberia. These attempts were less successful than had been hoped, partly because the WHO regional adviser in Brazzaville who had been assigned responsibility for smallpox eradication had many other duties and could devote little time to the programme. Dr Mayer, the WHO adviser in Liberia, was WHO’s intercountry adviser for all smallpox programmes in western and central Africa, but he could rarely travel. In 1968, he was transferred to Mauritania, where he served as the smallpox eradication programme adviser, the CDC adviser having had to leave Mauritania when diplomatic relations between that country and the USA were severed. The WHO adviser assigned to Mali rarely left the capital and in 1968 his post was discontinued. In response to requests from Member governments, the WHO Regional Office for Africa provided funds to cover local costs, 13 countries receiving in all a total of US$1 110 675 over the period 1967-1972. However, apart from processing these requests, the regional office and the WHO country representatives had little contact with the CDC programme.
From Geneva, Henderson maintained close contact with the CDC staff in Atlanta. They and selected national counterparts contributed to WHO interregional and intercountry smallpox seminars in Africa, South America and Asia; some WHO staff from the regions participated in the CDC smallpox eradication training programme in Atlanta in 1967 and 1968; and accounts of the progress made in western and central Africa were regularly published in the WHO Weekly epidemiological record and in special reports of the smallpox eradication programme. From 1968, supplies of bifurcated needles began to be shipped from Geneva, and in 1969 a jointly sponsored WHO/AID/CDC conference on smallpox eradication was organized in Lagos. The extensive proceedings, which documented many important observations on smallpox eradication (United States National Communicable Disease Center, 1970), were distributed to WHO and national staff throughout the world.
Collaboration with OCCGE and OCEAC was effective and useful. These organizations, both supported by France, kept abreast of events through written reports and discussions at their semi-annual meetings, which dealt with the progress and policies of this and other regional programmes. The directors of these organizations also participated actively in solving problems of implementation and communication arising in programmes conducted by their member governments. In addition, OCEAC served as an intermediary for the transmittal of national reports and the receipt of supplies and equipment for the Congo, with which the USA did not then have formal diplomatic relations; beginning in 1968, OCCGE performed a similar function with respect to Mauritania.
Measles Control
From a 1967 field report by Dr Ralph Henderson and Mr Neal Ewan :
Many valuable observations were made during the course of the programme with respect to the epidemiology and control of measles (Foster & Pifer, 1971), a disease which presented quite different problems from those of smallpox. Case-fatality rates associated with measles were customarily 4-5%, sufficient to identify it as second only to malaria as a cause of death among children. In contrast to smallpox, measles spread rapidly and widely. Studies in urban and in the more populous rural areas revealed that 50% of cases occurred in children less than 15 months of age (Smith & Foster, 1970a). Only in remote villages, where visitors were infrequent, did substantially higher proportions of cases occur among older children (Millar, 1970). In densely populated urban areas, morbidity decreased by about half for only 1 year following a mass vaccination campaign; in more sparsely populated areas, this decrease persisted for 2 years, but the incidence then returned to pre vaccination campaign levels (Smith & Foster, 1970b). In the hot and humid densely populated coastal areas, there was no apparent seasonal change in the frequency of transmission.
The prevention of measles infection was, and continues to be, a difficult problem. Essentially all children are born with circulating maternal antibody, which prevents infection. In some the protection is lost within 5 months, but in others it persists for up to 12 months of age. However, immunization is successful only after maternal antibody is lost, this antibody serving to protect against the attenuated infection induced by the measles virus vaccine. To prevent infection, therefore, it is necessary to administer the vaccine during the brief period between the time the child has lost the protection conferred by maternal antibody and his exposure to infection—in Africa, usually between 6 and 18 months. In a mass campaign in which vaccinations are given, for example, every 2-3 years to preschool children, much of the vaccine has no effect, these children being protected by maternal antibody or having already had the disease. Thus, the effect of a mass campaign on measles incidence is a transitory one. Efforts were made to vaccinate at more frequent intervals in urban areas of western Africa, but usually this had little effect unless the campaigns were conducted every 6 months, a prohibitively expensive strategy. Vaccination at conveniently located health centres was an alternative but in most areas there were few of these and most were not equipped with refrigerators. Thus, although the number of measles cases and deaths could be reduced, sometimes substantially for short periods of time, long-term control was not achieved.
Changing Roles of the CDC Atlanta Office and the Lagos Regional Office
Flexibility in the management structure was no less important than in field operations. The Lagos regional office had been expected to serve as the principal point of contact for operations and as the conduit for reports and requests from all the national programmes; the CDC Atlanta office was expected to bear primary responsibility for recruitment, training, procurement of supplies and equipment and liaison with AID. This management relationship had originally appeared to be the most logical because of the geographical proximity of the Lagos office staff to field operations and of the less elaborate procedures that would be needed to obtain United States government approval for travel by persons stationed abroad. What had seemed logical during the planning stage, however, proved less functional in practice. It soon became apparent that communication between the individual countries and Atlanta was usually easier than between them and Lagos. When a protracted civil war broke out in Nigeria in 1967, the difficulties became greater as cable traffic increased. Because messages concerned with the smallpox eradication-measles control programme were given low priority, a cable from a national capital sent through Lagos took as long as 1-2 weeks to reach Atlanta. Shipments of supplies by air freight or diplomatic pouch were also delivered more promptly when dispatched from Atlanta than from Lagos. Although it was a major transport centre, Lagos had few direct flights to many of the African capitals, especially those of the francophone countries. In consequence, field staff and personnel in Atlanta, faced with an increasing array of problems, found it necessary to communicate direct with each other. Towards the end of the first year, responsibilities and relationships were redefined to centralize direction in Atlanta, the Lagos office assuming a support role in contacts with national authorities and undertaking special investigations and assessments. In practice, the revised system worked well : new approaches were identified as experience accrued, and alternative methods and systems found useful in one country were applied with little delay throughout the region.
Surveillance and Containment Activities
It had been thought at first that surveillance and containment activities would be most crucial to interrupting transmission during the concluding phases of each of the national mass campaigns, but experience quickly showed that they could play a vital role from the beginning of a programme, irrespective of smallpox incidence. This was first shown in eastern Nigeria, just as the regional programme began.
The Nigerian programme agreement was signed on 6 October 1966 and field staff soon began to arrive. Operations were, however, initially confined to 2 of Nigeria’s 4 regions because special agreements had to be finalized with each of the semi-autonomous regions before work could begin. The Eastern Region was the first to commence operations. In November 1966, Dr Foege with Dr David Thompson and Mr Paul Litchfield, began a programme of staff training while awaiting delivery of vehicles and other commodities . Early in December, they were informed by a missionary of smallpox cases in a small village and decided to use this opportunity to train vaccination teams in containment activities. Using borrowed transport, they vaccinated people in the village and along nearby roads ; an outbreak of 19 cases was stopped in 4 weeks (Foege et al., 1975). Missionaries in the southern part of the Eastern Region, who had their own radio network, were approached for help in notifying other outbreaks. Two further outbreaks were soon identified, one of 14 cases and one of 5 cases. Both were contained within 3 weeks, again simply by vaccinating household and village contacts. With the limited resources available, the programme staff had expected to do little more than control a few of an anticipated large number of outbreaks, but surprisingly no further outbreaks were reported in this area . On investigation, the staff discovered that the last epidemic to be recorded in the area had occurred in 1950, despite the fact that comparatively few persons, except those living near roads, had been vaccinated since then. The first case in the 1966 outbreaks had come from the Northern Region of Nigeria fully 5 months before; subsequently, smallpox had spread slowly southwards with as many as 4 generations of cases occurring in a single compound. The finding of so few outbreaks, all in nearby villages, along with the discovery that they could be rapidly contained even where vaccinial immunity was low, was impressive. A review of data from earlier years suggested that outbreaks normally began along the northern borders of the region and spread progressively towards the south, an observation which suggested that persistent endemic transmission did not occur in most of the Eastern Region.
The programme staff decided to concentrate their resources in areas in which smallpox was known to be present. Accordingly, a new reporting system was devised . In each of the 3 provinces of the Eastern Region, a reporting officer was designated to obtain weekly reports from all government and missionary health establishments and transmit them by radio directly to Enugu, the regional capital. The data quickly revealed that most of the known cases were occurring along the northern boundaries, and a pilot vaccination campaign was therefore begun in the northern urban area of Abakiliki (WHO/SE/68.3, Thompson & Foege). Within a week, 46 500 people were vaccinated and gradually the campaign moved to adjacent areas in the savanna. Numerous unreported cases of smallpox were discovered and, by May 1967, 754 cases with 180 deaths had been documented.
Meanwhile, political turmoil steadily increased throughout the Eastern Region and on 30 May the predominantly Ibo tribal population seceded from Nigeria, proclaiming the independent Republic of Biafra. It became increasingly difficult to continue with the programme; travel was restricted to those with special passes, and petrol became scarce. Nevertheless, during June 1967, a mass vaccination campaign was conducted in and around Enugu the only remaining endemic focus. By the end of the month, transmission appeared to have ended, after only 6 months of activity, during which only 750 000 of the 12 million inhabitants had been vaccinated (Foege et al .,1971). Programme operations in eastern Nigeria were interrupted almost immediately thereafter but the idea had been planted that it might be desirable to give precedence to the discovery and containment of outbreaks over the execution of the mass vaccination campaign.
By June 1968, vaccination teams were active in 19 countries; some 40 million persons had been vaccinated about 35% of the estimated population . In each programme, priority was given to vaccination campaigns in the areas reporting the most cases of smallpox, although this strategy was not pursued with the same vigour as in eastern Nigeria. Less than half the countries had independent assessment teams but in most of them documentary or other evidence indicated that the vaccination coverage was high. The impact of the vaccination campaign was already apparent, only 2312 cases being reported by the end of May compared with 4071 during the same period of the preceding year. Although reporting systems were still inadequate, many cases which would not otherwise have been reported were being detected by vaccination teams, and some during outbreak investigations, where these were being undertaken.
In June 1968, Dr Foege, who had joined CDC’s Atlanta staff, proposed to participants at the annual CDC Regional Programme Conference a change in strategy to hasten eradication namely, to give priority to the detection and containment of outbreaks (Foege et al.,1971). Originally, there had been doubt that simple containment measures could be effective because of the common belief that smallpox was comparatively easily and rapidly transmitted through the population (Felsenfeld, 1966; Top, 1968), especially where vaccinial immunity was low. The experience in eastern Nigeria and a study in Dahomey in 1967 (Henderson & Yekpe, 1969) contradicted this. Moreover, epidemiological studies of smallpox in East and West Pakistan in 1966-1967 (Thomaset al.,1971 a, b, 1972; Mack et al .,1972a,b) also showed that smallpox spread slowly, that outbreaks tended to be clustered in an area rather than widely dispersed and that at the low point of seasonal incidence very few villages were infected. These observations were also confirmed in India in a study conducted in a district classified as heavily infected but in which it was found that at no time were more than 1 % of all its villages infected with smallpox (India National Institute of Communicable Diseases, 1968).
Dr Foege reasoned, as had the investigators in Pakistan, that intensive efforts to detect and contain outbreaks, if begun at the low point of seasonal incidence (September-October), should readily contain the few outbreaks then present. This would serve to avert major epidemics later in the year, when smallpox spread more rapidly. He proposed that each of 8 countries which then had endemic smallpox should undertake an intensive and continuing programme of surveillance and containment. The programme was given the name E 2, for “eradication-escalation” (Foege et al., 1971). The strategy was formally adopted in July 1968 by all countries except Nigeria, which decided that because of a widening civil war, it would give priority to completion of its mass vaccination campaign . However, in areas of Nigeria in which mass vaccination had been conducted, specially assigned short-term CDC epidemiologists would undertake outbreak investigation and containment.
For the detection of cases, the usual reporting mechanism was augmented by the cooperative efforts of other special health service programmes (e.g., leprosy and malaria control), government personnel, village leaders and non-governmental bodies such as missions. Outbreaks were investigated and vaccination was performed in a “geographically or socially contiguous area around each patient”, as determined by epidemiological investigation. The area was not defined more explicitly, as was later done in Asia, nor was an attempt made to enumerate contacts and village populations to ensure that all had been vaccinated.
The increase in surveillance activity led to the discovery of many additional cases, with the result that the number of reported cases rose from 197 in August to 289 in September ; from then on, it fell steadily (Table 17.7).
By January 1969, endemic smallpox remained only in Dahomey, Nigeria, Sierra Leone and Togo. The last cases in Sierra Leone and Togo were detected in May of that year, and the last case in Dahomey was found in September ; thereafter no further cases were notified for 6 months (Table 17.8). In March 1970, however, a persistent endemic focus was discovered in northern Nigeria, but 2 months later the last known case in Nigeria, the last in western and central Africa, was detected, only 9 months after “eradicationescalation” had begun.
The vaccination campaign continued throughout the “eradication—escalation” operation, 33 million persons being vaccinated during 1969 and 22 million in 1970 (Table 17.9). Contrary to expectations, the pace of the vaccination campaign did not diminish during this period ; indeed, more vaccinations were given each week, on average, than before the special programme began. By the end of 1970, the number of vaccinations performed in 12 of the countries was equivalent to, or greater than, the estimated population.
During 1971—1972, the programme was modified in order to give priority to the vaccination of those who had been missed during the initial mass campaign and of those born after it. By the end of 1972, 153 484 000 smallpox vaccinations and 28 163 000 measles vaccinations had been performed. The cost of smallpox eradication in the region was estimated to be US$0.138 per head of population (Foege et al .,1975).
In 1972, as the 5-year programme drew to a close, CDC staff proposed to AID that other types of vaccine and support for other preventive measures should be provided in order to strengthen the health services in the countries of western and central Africa. Although the proposal was endorsed by all the ambassadors of the USA in the region, as well as the respective health ministers, the programme was terminated at the end of 1972. CDC sought to sustain surveillance and a maintenance vaccination programme by assigning epidemiologists to OCCGE and OCEAC, but because of the large number of countries and the lack of supplies and equipment to replenish the programmes, vaccinial immunity steadily declined thereafter as did the quality of surveillance. By 1976, when precertification activities had to be undertaken, special programmes had to be initiated in all the countries of the region to document what had been accomplished and to verify, through pockmark surveys, that no further cases had occurred.
Table 17.7: western and central africa: number of cases of smallpox reported and detected in 9 countries,2 1968b
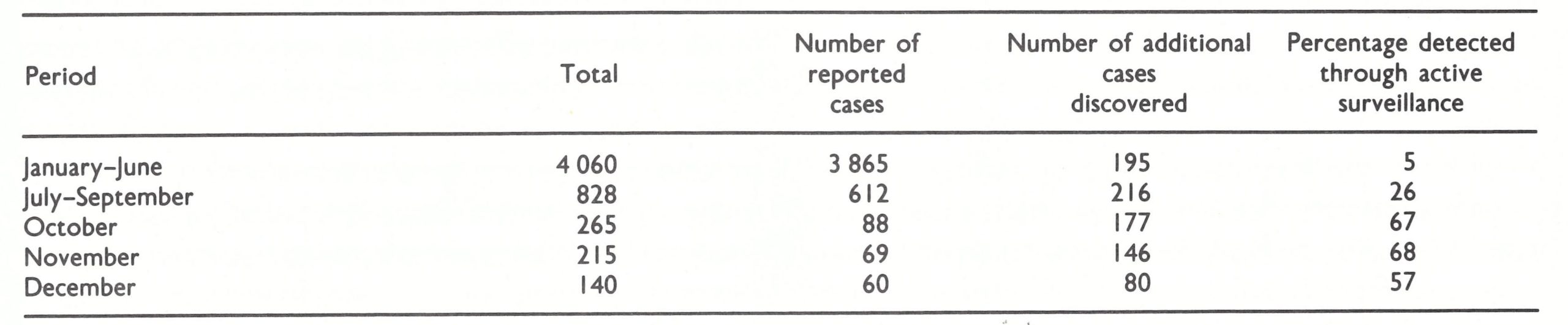 NOTE: These data, taken from field records, differ somewhat from the figures given in official reports, from which for example Table 17.1 was compiled.
NOTE: These data, taken from field records, differ somewhat from the figures given in official reports, from which for example Table 17.1 was compiled.
a Cameroon, Dahomey, Guinea, Mali, Niger, Nigeria, Sierra Leone, Togo and Upper Volta.
b Bases on Foege et al. (1971).
Table 17.8: Western central Africa: number of reported cases of smallpox by countrya and by month, 1969-1970
 a No other countries in western and central Africa reported cases after 1968.
a No other countries in western and central Africa reported cases after 1968.
b Figures in parentheses denoted cases recorded by date of onset rather than by date of notification; these cases were discovered on 21 March and during succeeding weeks.
c Cases reported in January 1969; the onset of the last case was in december 1968.
d Cases reported in May 1969; the onset of the last case was in April 1969.
Table 17.9: Western and central Africa: number of reported smallpox vaccinations (thousands), by country, 1967-1972a
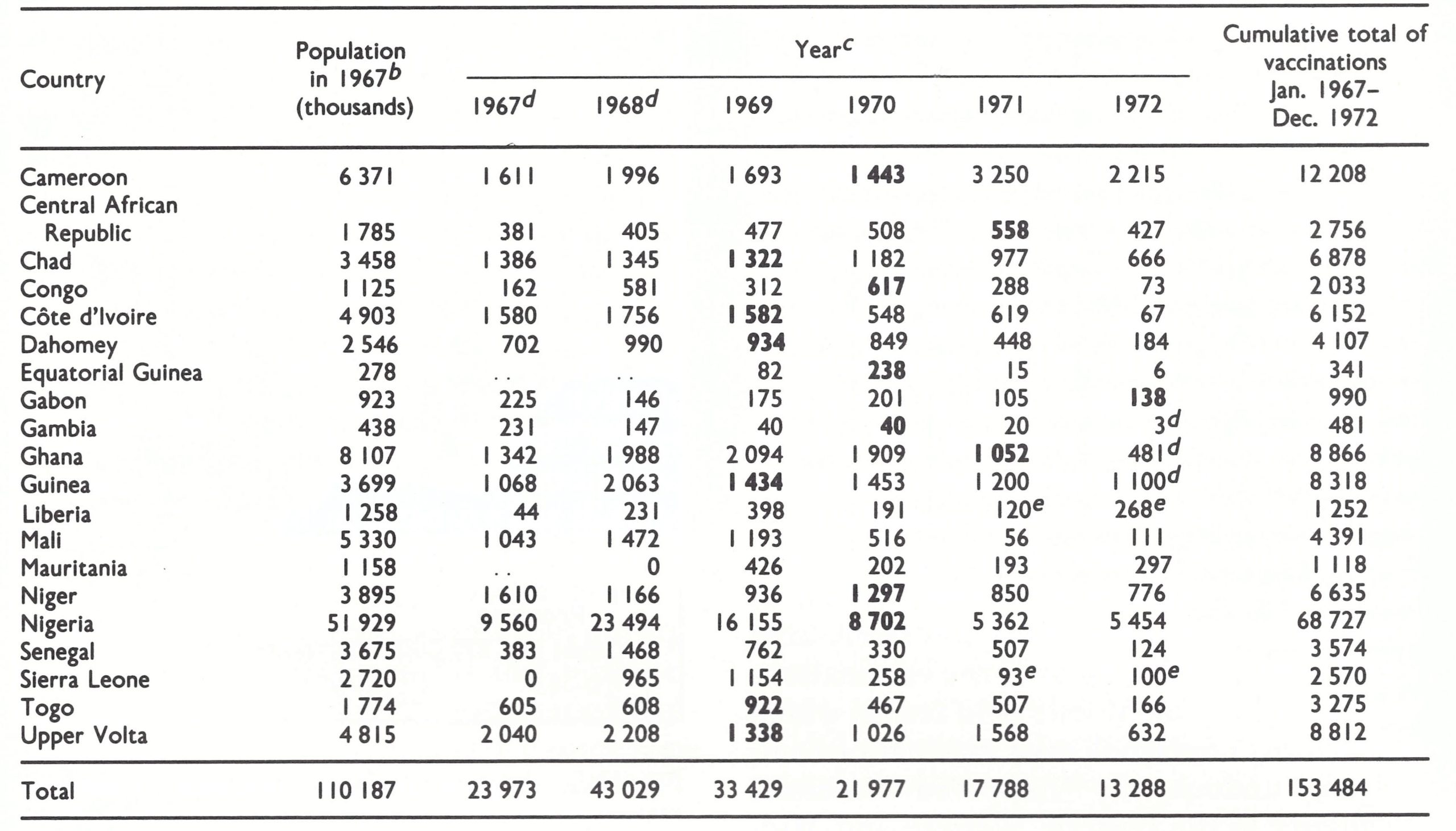 a Based on Foege et al.(1975).
a Based on Foege et al.(1975).
b Population data from United Nations (1985).
c ..=data not recorded.
d Incomplete and/or provisional data.
NATIONAL PROGRAMMES
Each of the national programmes had different characteristics and encountered different types of problems, some of which are summarized and discussed below. For ease of presentation, the countries are dealt with in 7 groups (shown in Fig. 17 .1) : (1) Nigeria—the most populous country, which, between 1967 and 1970, reported 6854 (40%) of the region’s 17 106 cases; (2) Dahomey and Togo—2 small adjacent coastal countries, in which smallpox incidence was high, and in which there was resistance to vaccination because of fetish practices; (3) Mali, Niger and Upper Volta—3 inland Sahelian countries, in which there were many nomads and frequent trans-humance; (4) Guinea and Sierra Leone—2 highly endemic countries, in which programmes were launched nearly a year later than in the other groups but which succeeded in interrupting transmission within 18 months; (5) Cote d’Ivoire, Ghana and Liberia-3 adjoining countries on the southern coast of western Africa, which experienced few cases of smallpox after 1966; (6) the Gambia, Mauritania and Senegal-all of which were free of smallpox when the programme began, and remained so ; and (7) the OCEAC countries-only 2 of which (Cameroon and Chad) detected cases of smallpox after 1966, mostly imported from Nigeria . GuineaBissau’s status is summarized in the accompanying box; activities in Equatorial Guinea, which remained free of smallpox and in which no special programme was conducted, are not further described.
Nigeria
Nigeria (population in 1967, 51.9 million) was the crucial country for the smallpox eradication programme, being centrally located and heavily endemic (Fig. 17.4) and having a population totalling nearly half that of the entire region. The largest number of CDC technical staff were therefore assigned to Nigeria and the CDC regional programme office was located there.
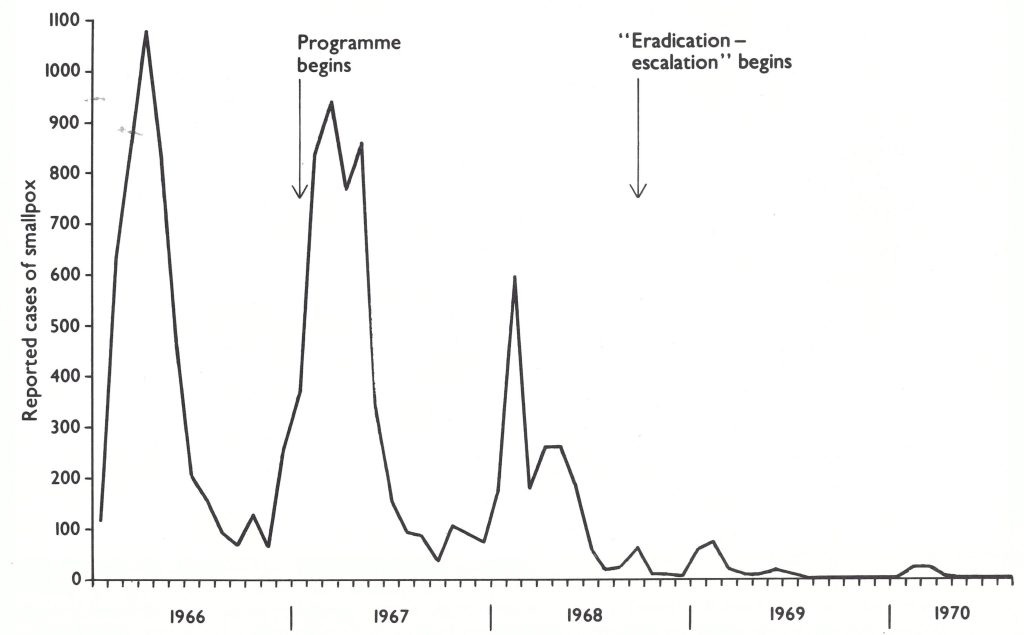
Plate 17.4. Nigeria: number of reported cases of smallpox, by 4-week period, 1966-1970.
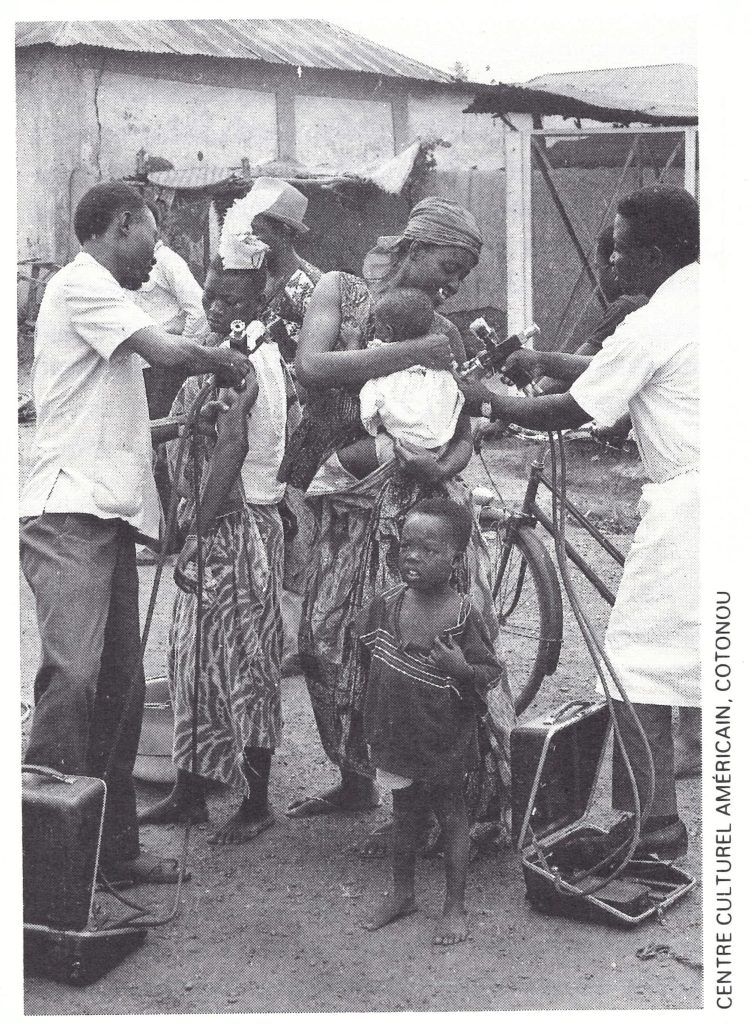
Plate 17.9. A vaccination team at work in Dahomey in 1967.
When the programme began, Nigeria was a federal republic consisting of 4 regions and the federal district of Lagos . Because responsibility for health matters was delegated to the regions, programme policies and plans had to be worked out and agreed on not only at the federal level but with each regional authority as well. Each region, in turn, dealt with traditional tribal authorities, which, in the Northern Region, had substantial powers. The National Council on Health had decided in 1962 that the eradication of smallpox should be an objective of national policy (Foster & Smith, 1970) and plans for such a programme were developed by the Principal Medical Officer of the Ministry of Health of Nigeria, Dr G. A. Ademola. Implementation of the programme, however, had to be delayed until 1967, when resources were made available by AID. Meanwhile, thermolabile lanolinated vaccine, produced in a government laboratory in Lagos, was provided for use in health centres, but because it was rarely kept under refrigeration, many of the vaccinations were unsuccessful. Mobile field teams, which periodically undertook mass vaccination campaigns, undoubtedly improved vaccinial immunity in the Eastern, Western and MidWestern Regions. However, nowhere was the level of immunity high, and in the Northern Region, vaccination coverage was especially poor.
Pockmark surveys conducted after the AID-supported programme began revealed that smallpox had been widely prevalent throughout Nigeria during the early 1960s, an estimated 100 000 or more cases having occurred annually. Survey data, as well as morbidity data compiled in 1967 (Fig. 17.5), showed the Northern Region to be the most heavily afflicted. In this region, which consisted mainly of savanna and arid scrub, the highest incidence occurred in the dry season, from January to May; in coastal areas, seasonal changes were less marked. The case-fatality rate was probably about 10%, although the only available data pertain to persons admitted to hospital—usually those who were the sickest and among whom deaths would have been more frequent (Table 17.10).
Early in 1967, Nigeria was on the brink of civil war. As major tribal groups vied for power, a military government displaced civilian rule, and an army mutiny occurred in the north, accompanied by extensive riots. The Eastern Region of the country threatened to secede. Despite these serious problems, the government supported the smallpox eradication programme. Pilot activities, each with its own programme unit, began in Lagos and in the Eastern and Western Regions during the spring of 1967 and in the Northern and MidWestern Regions during the summer. Because of the widespread prevalence of smallpox and concern as to the continuing stability of the country, Dr Ademola and Dr Stanley Foster, the CDC senior adviser, decided to devote all available resources to the mass vaccination campaign, giving first priority to the areas with the highest incidence in each region.
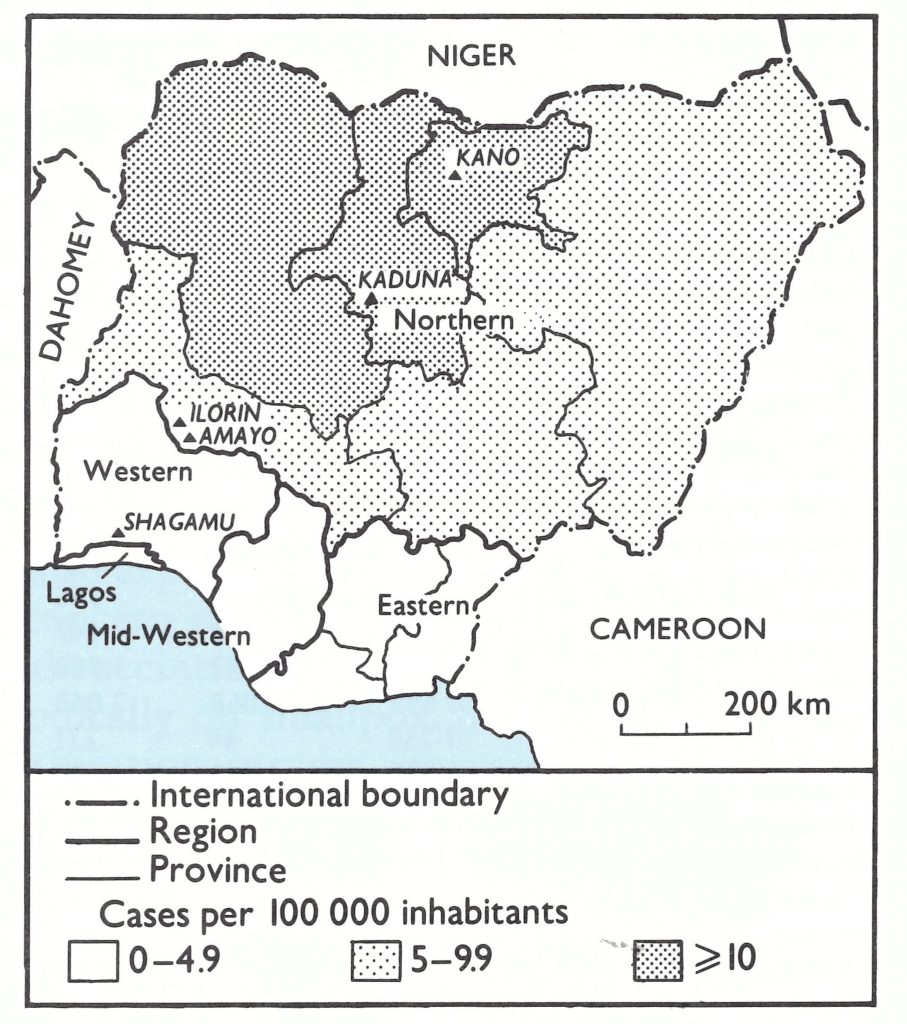
Plate 17.5. Nigeria: smallpox incidence by administrative region and province, 1967. Early in 1967, Nigeria was made up of 4 regions and the federal capital territory of Lagos. The map also shows the provincial subdivisions in the Northern and Eastern Regions.
Table 17.10: Nigeria: number of cases of and deaths from smallpox, and case-fatality rate, in Kano Infectious Diseases Hospital, by age, 1967-1970
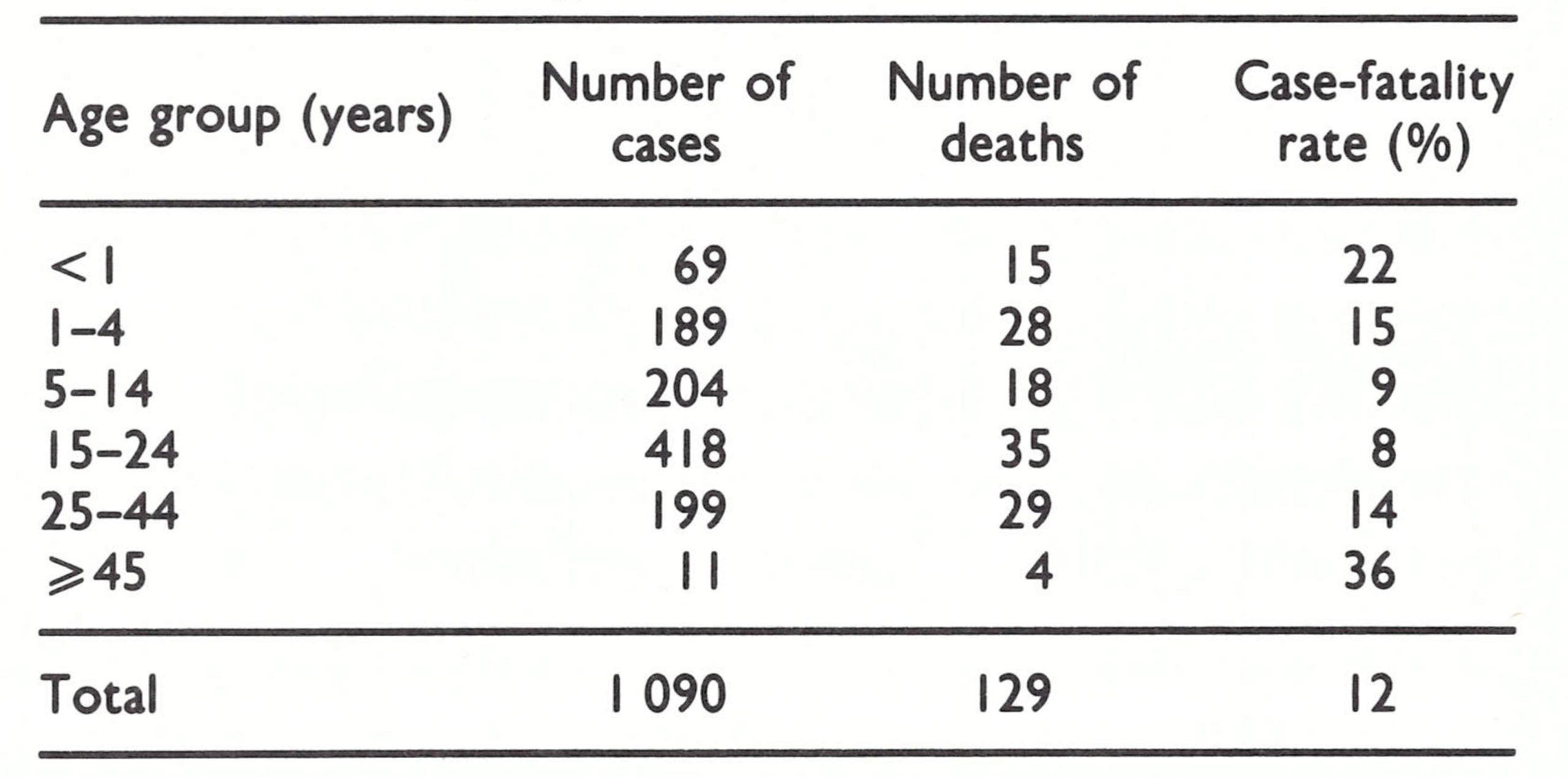
The responsibility for outbreak control was left to local health authorities, to which the government continued to issue lanolinated vaccine despite advice to the contrary by CDC staff.
In the Eastern Region, smallpox was eliminated with surprising rapidity . Mass vaccination in the north of that region, in which cases were concentrated, concluded in June 1967, simultaneously with the occurrence of the last known smallpox cases . In July, the Eastern Region having declared itself the independent Republic of Biafra, fighting between the Nigerian and Biafran armies began along its borders . The vaccination campaign decreased in intensity but did not stop immediately, and for many months vaccine continued to be transferred from Nigerian to Biafran health authorities during cease-fire periods arranged for this purpose. By the end of 1967, however, vaccination had ceased, and in 1968 widespread famine developed in Biafra, accompanied by epidemics 17. WESTERN AND CENTRAL AFRICA 88 3 of measles with high case-fatality rates . In October, the government of Biafra appealed for help and the International Committee of the Red Cross (ICRC) and the World Council of Churches responded with technical assistance and provided measles and smallpox vaccines, the latter coming from WHO stocks in Geneva. A vaccination campaign began again on 27 December 1968, organized by Dr A. E. Ifekwunigwe, a senior lecturer in paediatrics at the university in Enugu, Dr Nicole Grasset of the Institut Pasteur (Paris) and Dr A. T . C . Bourke, consultant to the ICRC. Despite serious shortages of petrol and staggering problems of transport and communication, 11 teams succeeded during the following year in giving an average of 100 000 smallpox vaccinations and 3500 measles vaccinations each week. Suspected cases of smallpox were investigated and specimens sent to Geneva for examination by WHO reference laboratories, but none contained smallpox virus.

Plate 17.10. The secession of the Eastern Region of Nigeria and the civil war that ensued resulted in extensive famine throughout that area. Despite formidable problems and great personal danger, national and international staff undertook extensive smallpox and measles vaccination campaigns, with special attention to refugees in camps.
Vaccine Production in Nigeria
From 1967 onwards, both CDC and WHO provided support to a government vaccine production laboratory at Yaba, near Lagos, in the hope that it might be able to manufacture sufficient high-quality freeze-dried vaccine to meet the needs of Nigeria and perhaps of other countries in western Africa. A CDC virologist, Mr Nathaniel Rothstein, was appointed to the laboratory in 1967 and, later, a WHO expert in vaccine production, Mr Ronald C. Kent, was assigned there and remained until 1976. Nigerian laboratory staff, assisted by WHO fellowships, received training in the United Kingdom, and the necessary laboratory equipment was provided by WHO. Batches of freeze-dried vaccine began to be produced in 1968, but the vaccine did not meet international standards until 1974, and then only briefly. Frequent transfers of technical personnel and management problems hampered work throughout this period. Nevertheless, the vaccine was routinely distributed for use in health centres, the vaccination teams using vaccine supplied by the USA. After 1973, the laboratory supplied all the vaccine required in Nigeria.
Meanwhile, by the beginning of May 1967, a pilot project in Lagos had been completed during which 1 million persons were vaccinated against smallpox; in February, the Western Region began its programme and in July more than 750 000 were vaccinated in Ibadan, the capital. Assessment showed that 90.8% of the population had been vaccinated. In the Northern Region, however, problems in reaching agreement about the conduct of the programme delayed its start until July. The vaccination campaign began in the western part of the region, in which the reported smallpox incidence was highest, and moved progressively eastwards, achieving substantially higher levels of coverage than in other parts of the country. The better coverage was achieved as a result of the edict of tribal leaders that people accept vaccination or be fined if they refused. As one programme officer commented: “In the south, a health education programme had to reach all the people to convince them to participate in a health activity, whereas in the north, a health educator only had to convince the emirs.”
By the end of 1967, some 9.5 million smallpox vaccinations had been performed in Nigeria. A monthly mimeographed “Nigerian Smallpox Eradication—Measles Control Surveillance Report,” which first appeared in April of that year, informed health staff throughout the country about the efforts being made. The number of cases reported in 1967 (4753) differed little from the 1966 figure (4953), most of the cases being reported during the first half of the year, primarily from the Northern Region.
Although the national programme had proceeded at a slower pace than planned, it was remarkable that so much progress had been made in a country engaged in full-scale civil war. There were problems in the delivery of supplies by air and sea, serious impediments to travel, shortages of petrol and other supplies and considerable personal risk to the teams working near the areas bordering on Biafra. Imagination, persistence and courage were required of national staff and CDC advisers alike: Dr Ademola and Dr Emmanuel A. Smith, the national programme director; Dr J. I. Adetosoye, Dr I. S. Mebitaghan and Dr P. O. Adeoye, Nigerian directors of programmes in the west, mid-west and north, respectively; and their CDC counterparts, Dr Margaret Grigsby (succeeded by Mr Lloyd Wade), Mr Warren Jones (succeeded by Mr Paul Bond) and Dr Deane Hutchins (succeeded by Mr Robert Hogan) . The age distribution of cases of smallpox for which ages were recorded closely resembled that of the general population (Table 17.11), suggesting that where outbreaks occurred, primarily in rural areas, immunity was low throughout the population.
Problems in northern Nigeria continued to be substantially greater than in other regions, partly because of its size, the lack of roads and the relative paucity of health facilities, and partly because many of the senior administrative and technical staff, including mechanics, had been Ibos from the Eastern Region who had fled with the onset of war. Only 3 CDC technical staff had originally been assigned to assist, but in April 1968 their number was increased to 6 and the CDC regional office equipment specialist was transferred to Kaduna to train new mechanics in the repair and maintenance of some 60 vehicles and jet injectors. Operations were further complicated, however, by the government’s decision to divide the region into 6 states, a move which required many modifications in the programme, including the reassignment of supervisors and field personnel, the restructuring of the reporting system, and changes in the budget and payment systems.
As 1968 advanced, the programme in Nigeria became fully established and during the year almost 24 million persons were vaccinated against smallpox by 60 mobile teams. In the Northern Region, assessment teams, visiting areas 7-14 days after the population had been vaccinated, usually found coverage levels of 95% or higher. For assessment elsewhere, the authorities decided to use the less satisfactory method of comparing the number of vaccinations performed with the population census figure. Although the personnel of the Western Region programme regularly estimated the coverage to be 90% or greater, later surveys showed levels of 80% in towns of more than 5000 inhabitants and levels as low as 45-65% in the villages.
Table 17.11: Nigeria: number and percentage distribution of cases of smallpox by age and percentage distribution of general population by age, 1967-1968
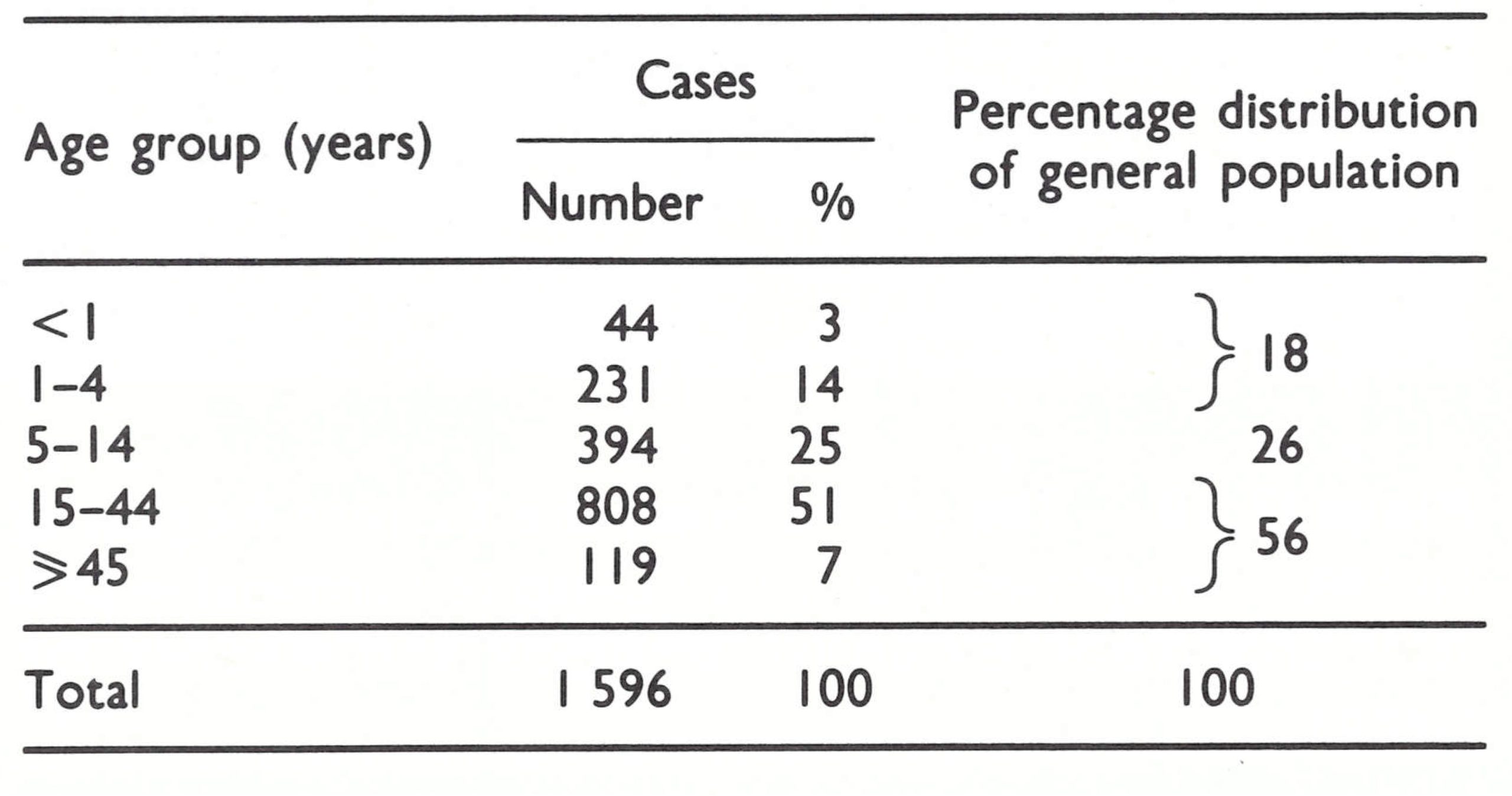
In September 1968, with the introduction of the regional “eradication-escalation” programme, efforts were made in Nigeria to improve the reporting system, which was complex and functioning poorly, some reports being delayed for weeks or even months—if they were sent at all. The system required the responsible village heads to report suspected cases to a district superintendent, and although some complied, many did not. The district superintendent, in turn, was expected to inform the superintendent for health, who was supposed to institute control measures and to forward his report to an area medical officer, who in turn reported to the regional government. Such outbreak control measures as were undertaken were largely ineffective, since the lanolinated vaccine continued to be distributed to the local health authorities. In the hope of improving reporting, efforts were made to persuade teachers, missionaries, foreign volunteers and others to report cases by recording the details on stamped addressed postcards, which had been duly supplied. In practice, however, this activity had little effect.
Although the epidemiological observations in eastern Nigeria had generated the “eradication-escalation” strategy, Nigerian staff and their CDC counterparts decided not to divert resources to this undertaking. As they assessed the situation, surveillance in northern Nigeria, in which virtually all cases were then occurring, could be established only with difficulty and over time because health centres were few, experienced personnel were lacking and the population was widely dispersed. In view of the continuing war, it was uncertain whether vaccination teams would have access to many areas in the future. Because the mass vaccination campaign was progressing well, with high levels of coverage, it seemed to the personnel concerned that the most prudent course would be to complete the campaign as rapidly as possible. That being accomplished, resources could be diverted to the investigation and containment of outbreaks. Limited surveillance activities were begun, however, towards the end of 1968, using short-term CDC epidemiologists in areas in which mass vaccination had been completed. At that time cases were found to be occurring in small outbreaks primarily among semi-nomadic Fulani herders. Having no special allegiance to the principal tribal leaders, these groups had largely been missed by the vaccination teams and by assessment teams as well (WHO/SE/68.5, Pifer & Adeoye).
The mass vaccination campaign continued to progress rapidly, concluding in the autumn of 1969. Meanwhile, the number of reported cases of smallpox declined sharply, only 5-16 cases being recorded each month from March to the end of July 1969. After July, no further cases were detected that year although an average of 10 rumours were investigated each month (WHO/SE/71.30, Foege). Transmission appeared to have been interrupted and, with the last cases occurring in Dahomey in September 1969, national and CDC staff scheduled a celebration for the end of March 1970 to mark the eradication of smallpox from western and central Africa. On 21 March, just as the staff were preparing to depart for the celebration, a 14-year-old girl was admitted to the infectious diseases hospital in Kaduna (Fig. 17.6) with unmistakable smallpox (Wkly epidem. rec.,1970b). She had fallen ill shortly after arriving from the town of Amayo (population, 1400), Kwara State, some 400 kilometres away. The outbreak was discovered almost simultaneously by a state senior health superintendent . Intensive house-to-house vaccination and search for cases revealed 48 additional cases in the town (WHO/SE/71.30, Foege) and 12 other cases in neighbouring villages, the first cases in the outbreak having occurred in October 1969. Further investigation revealed that smallpox transmission had persisted in the area since early 1969, primarily in communities of up to 300 persons, the cases being hidden by their families from the health authorities. The search was extended to Ilorin, the capital of Kwara State (population, 300 000), only 11 kilometres away. Nine additional cases were found—the last on 22 April 1970.
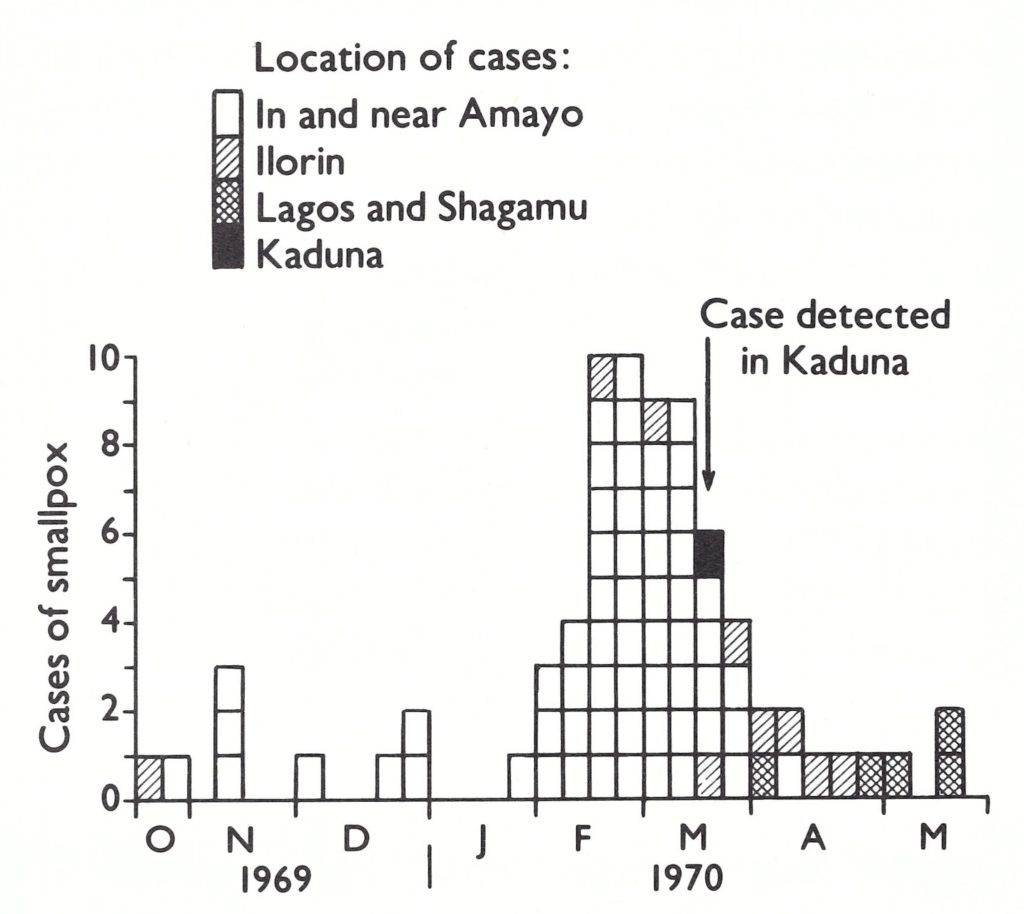
Plate 17.6. Nigeria: number of reported cases of smallpox, by week of onset and by area, October 1969-May 1970.
Northern Nigeria: the Role of Traditional Leaders
In northern Nigeria, strong traditional tribal leadership both helped and hindered programme implementation. One adviser recalled his surprise when attending the first mass vaccination campaign in a town to find 6000 persons already in a line at 6 o'clock in the morning. As the day progressed, he proposed to the chief that a vaccination team should move to the market area to begin work there. The chief forbade this, indicating that if all vaccinations were performed in front of him, everyone would comply, but if he were not present at the vaccination assembly point, people would report they had been vaccinated when they had not. Vaccination in this and other largely Muslim northern cities continued until long after dark, as women were not allowed to leave their homes until nightfall.
On the negative side were such problems as those encountered during the investigation of the outbreaks in 1970 in and around Amayo. A village chief, when questioned about rumours of smallpox cases, denied all knowledge of them until, during the course of interrogation, his granddaughter emerged from the house with evident smallpox lesions. Because of fear that he would be deposed from his chieftaincy if it were found that he had been hiding cases, he had suppressed information about the outbreaks.
Vaccination in Kwara State had been conducted between December 1968 and July 1969. However, the reassignment of personnel, which accompanied the division of the Northern Region into states, had left Kwara with fewer resources than other states, and the supervision of the programme had been poor. Teams had concentrated their efforts in the major villages and towns, but even there coverage was poor because villagers resisted vaccination. During assessment, it had been found that coverage was only 70% in rural areas and 60% in the town of Ilorin; a repeat campaign had therefore been conducted in the course of which 97 000 additional vaccinations had been performed. Despite this effort, a survey in April 1970 showed that only 77% of the population had vaccination scars; in some peripheral areas of the city, the proportion was only 35%. Following the discovery of the outbreak in April 1970, a repeat house-to-house vaccination campaign was conducted, and road-blocks were established around the city to vaccinate any person who entered or left. Subsequently, special teams conducted village-by-village searches and vaccinated the inhabitants of the surrounding districts; special district search teams continued work during the following 12 months . The last known case in the area, however, occurred during the second week of April, 3 weeks after containment operations had begun.
just as the outbreaks in the Amayo-Ilorin area began to come under control, a more alarming discovery was made: 2 cases had occurred in Lagos, 150 kilometres to the south, the patients having become ill during April. Three further cases, with onset of illness in May, were discovered in Shagamu, a town to the north of Lagos. The source of infection in both outbreaks was suspected to be Ilorin, but this could not be confirmed. Intensive search and vaccination were extended in ever-widening areas around these 2 foci but no further cases were found.
The occurrence of new, widely scattered outbreaks in Nigeria was profoundly disturbing to staff throughout western and central Africa, since the cases were discovered more than 6 months after it had been thought that transmission had been interrupted and more than a year after the intensified surveillance scheme had been launched. Optimism and complacency were quickly replaced by doubt and a redoubled surveillance effort. No celebrations were in fact held until more than a year later. Although the cases in Shagamu proved to be the last, the intensified search that their presence had stimulated gave grounds for confidence that transmission had indeed been interrupted.
Dahomey and Togo
In 1967, Dahomey (population, 2.5 million) and Togo (population, 1.8 million),former colonies of France lying on the Bight of Benin between Nigeria and Ghana, were impoverished and politically unstable. Together, they cover an area between 250 and 500 kilometres from east to west and 650 kilometres from north to south. In both countries, the population was concentrated in the south. Travel from one to the other and to neighbouring countries was unrestricted and frequent because the presence of tribal groups extended across national borders. In contrast to most of the former French colonies in Africa, traditional tribal leadership remained strong and the civil governments were comparatively weak and unstable. Togo experienced 2 coups d’etat in the 4 years immediately preceding the smallpox eradication-measles control programme; and Dahomey 6 coups d’etat between 1960 and 1970, its first decade of independence.
Preventive medical services in both countries had all but ceased to function by 1967 because of political upheaval and lack of funds . Dahomey had had a reasonably effective mobile endemic diseases control service, which had functioned like its counterparts in other former French colonies. As recently as 1965, it had had a complement of 237 staff, operating from headquarters posts in the southern, central and northern parts of the country. The number of vaccinations given each year had been equivalent to 20-25% of the population. The activities of the service had, however, gradually diminished, and by 1967 little field work was being done. Togo had also had a mobile endemic diseases control service, which was less well supported and had effectively been disbanded in 1964- 1965. The number of vaccinations performed and the type of vaccine used are not recorded.
In both countries, substantial numbers of smallpox cases were reported every year (Table 17.12), primarily from southern areas. There, as in parts of western Nigeria, resistance to vaccination had been widespread, especially in the more rural areas. The resistance was attributed to the cult worship of a smallpox fetish (see Plate 17.11) called VoduSakpate, or Sopona, the major earth god of the Fon tribe. Hereditary fetish priests (feticheurs), who were thought by the people to have the power to prevent or to induce the disease, had traditionally performed variolation by the inoculation of pulverized scabs on the forehead, at the base of the nose or on the underside of the wrist (Glokpor, 1970). Customarily, large numbers of persons were variolated in an affected village some 3-4 weeks after the onset of illness in the first case, in a ceremony which was said to “free the patient” of illness. For thefticheurs, there were economic disincentives to cooperate in vaccination campaigns, since they were customarily given all the possessions of a patient who died of smallpox. Concern about the problem was reinforced by information that a vaccination team in Dahomey had been killed by fetish worshippers in the early 1960s.
Table 17.12: Dahomey and Togo: number of reported cases of smallpox, 1962-1969
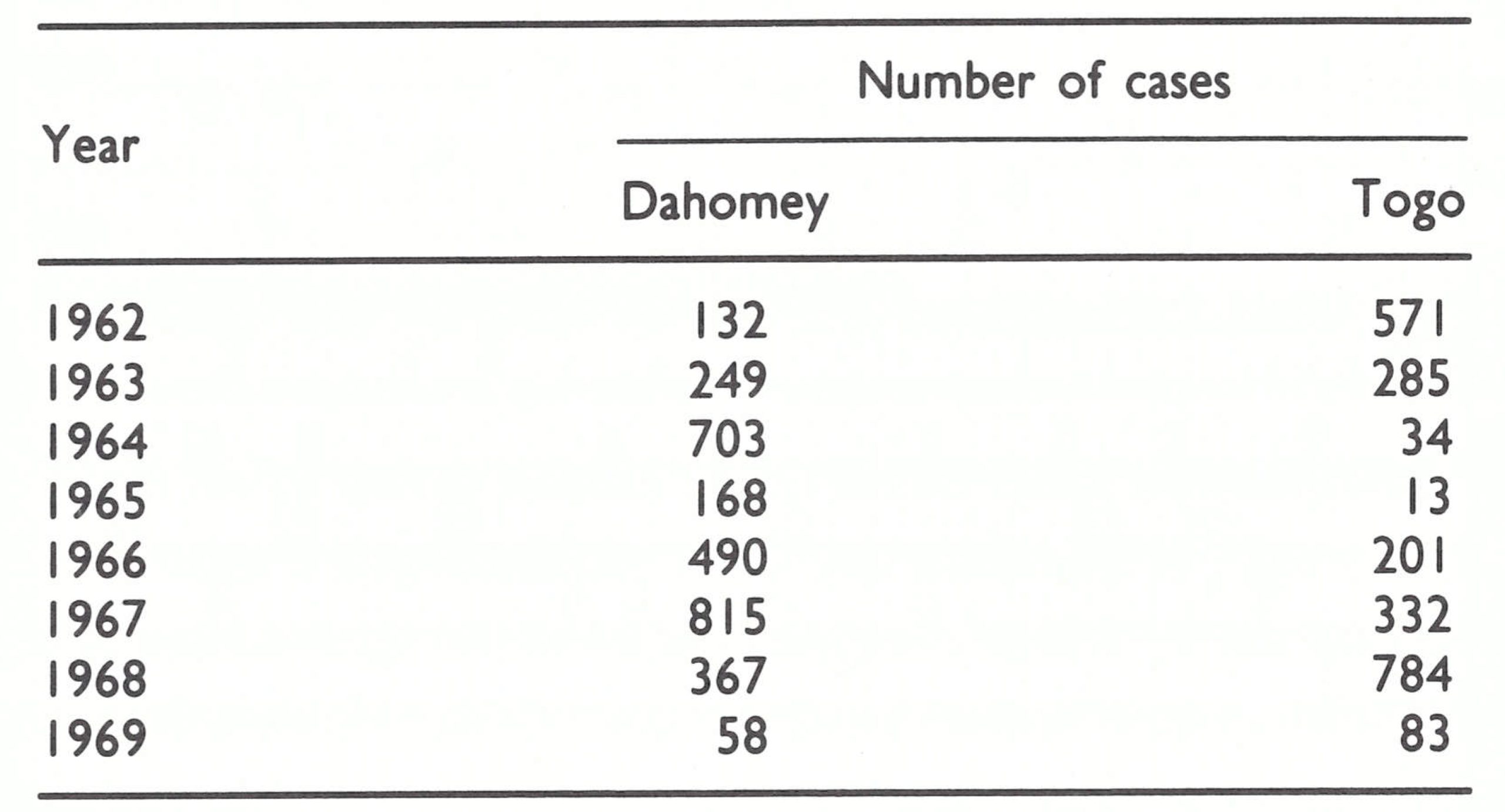
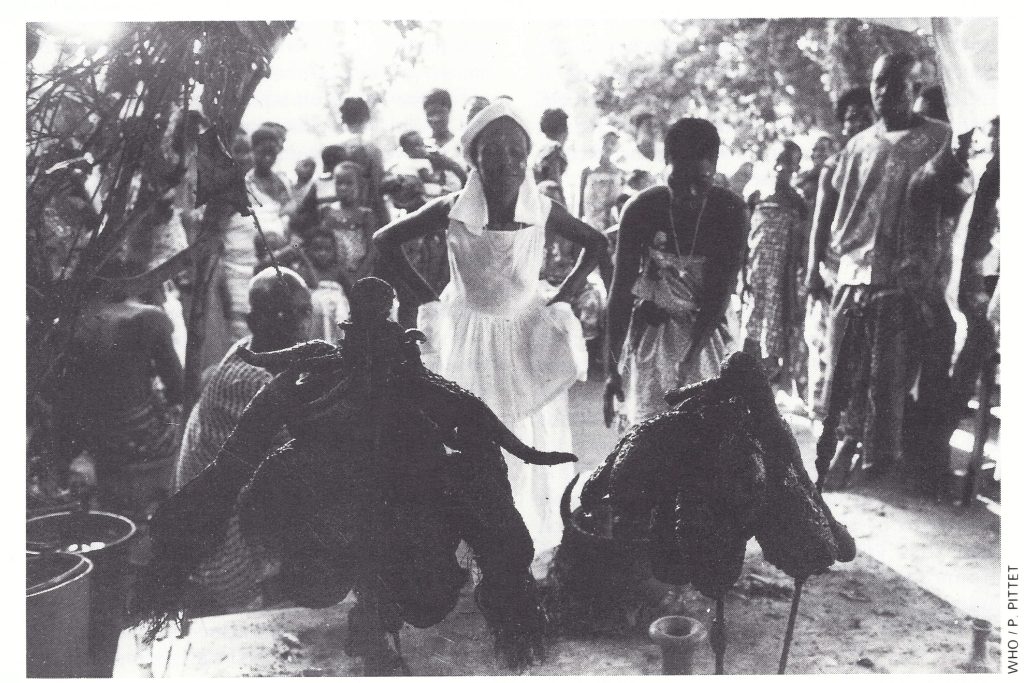
Plate 17.11. The practice of variolation and resistance to visits by vaccination teams were both associated with fetish worship. At a celebration in Dahomey, a priestess dances in front of the smallpox fetish until she goes into a trance.
In Dahomey, personnel from the endemic diseases control service were again employed for a mass vaccination campaign, which commenced simultaneously in April 1967 in the northern, central and southern zones of the country. At the beginning, progress was discouragingly slow, since by government decision smallpox vaccine and measles vaccine were given by separate teams. Ultimately, however, the practice was changed and each team gave both kinds of vaccine, which resulted in a considerable improvement in programme efficiency and a reduction in cost. Better progress was also made when it was realized that tribal chiefs, especially in the southern areas, were more influential than the civil authorities. Accordingly, meetings began to be arranged with tribal authorities to explain the programme’s goals and method of operation and to discourage variolation.
In August 1967, soon after the programme had begun, a special study of a small outbreak revealed quite a different epidemiological picture of smallpox in this area from that which had been anticipated (Henderson & Yekpe, 1969), a finding which contributed to the formulation of the 1968 “eradicationescalation” strategy. The investigation began 10 weeks after the occurrence of the first case, but only 28 cases were found in the village of 300 inhabitants, despite the fact that only 15% of the children and 54% of the total population had vaccination scars. Surprisingly, the outbreak had terminated spontaneously, notwithstanding the many remaining susceptible persons. The study, which was conducted by Dr Ralph Henderson and Dr Maximilien Yekpe, chief of the southern sector of the endemic diseases control service, showed, moreover, that the patients were geographically clustered within the village itself despite the frequent movement of the population throughout the village. These observations reinforced the belief that smallpox in Africa spread slowly and that transmission occurred primarily as a result of intimate personal contact in households and rarely through casual contact in market-places or elsewhere. Given this pattern of spread, outbreak control was clearly more feasible than had been expected.
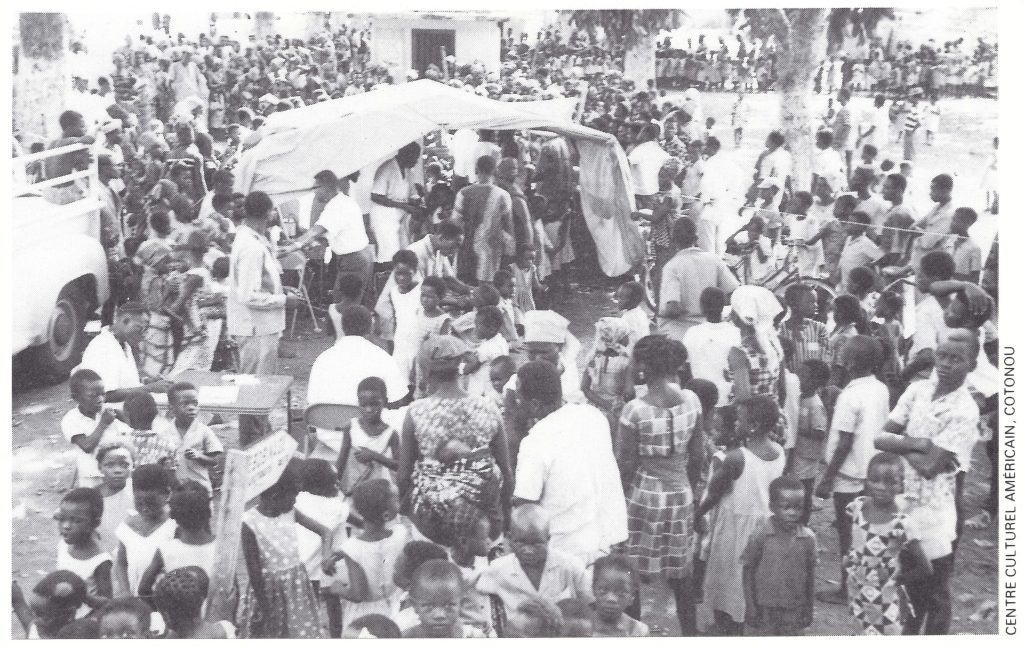
Plate 17.12. Residents of the principal urban areas in Dahomey were vaccinated during mass campaigns conducted between May and July 1967.
Assessment of the vaccination programme in Dahomey during 1967 revealed that only 28% of the population were being vaccinated by the teams and that the more remote, less accessible villages and hamlets were being missed; in some of these, smallpox outbreaks occurred after the teams had left the area. To complement the work of mobile teams who vaccinated only at assembly points, a group of 12 young health workers, called “les douze,” was recruited, trained and given motorcycles. They worked in areas in which coverage was poor, performing house-to-house searches and vaccinating, by means of bifurcated needles, all children under 5 years of age and anybody without a vaccination scar (Yekpe, 1970).
The programme in Togo likewise got off to a slow start in 1967. The vaccination teams consisted of staff from a yaws control programme, who had continued to receive their pay but had not worked for more than 2 years. They were unenthusiastic about performing the requisite field work and made a poor showing until threatened with suspension. For political reasons, the vaccination campaign began in the north but, after a coup d’etat and a change of government, it shifted to the south, where most cases were being reported and where villagers were both resistant to vaccination and suspicious of the government teams. The problems encountered may be illustrated by the description of an outbreak investigation conducted in November by the CDC advisers, Dr Bernard Challenor and Mr Andrew Agle. On checking a rumour of smallpox cases in a village whose inhabitants had been vaccinated twice, in January 1967 and again in October of that year, they found 8 patients, 7 of whom were hidden in the bush. The director of the medical zone, who was disturbed by these observations, decided to obtain help from the police and to take village chiefs into custody until the inhabitants of their villages had all been vaccinated. As in most areas in which police or military force was used, the result was even less satisfactory than before, since chiefs and villagers fled the area or fought with the police. That approach was soon abandoned.
Despite all the difficulties, 605 000 vaccinations were recorded in Togo in 1967 and 702 000 in Dahomey, which approximated to the projected targets. In that year the number of cases reached 815 in Dahomey and 332 in Togo, an incidence in each country which was among the highest in the world.
During the course of 1968, both countries significantly improved their reporting systems and gradually the proportion of people vaccinated in each area increased. Programme staff in both countries enlisted the help of personnel in health clinics, other health workers, foreign volunteers and tribal authorities to report cases. In south-eastern Togo, 15 health workers, comparable to “les douze” in Dahomey, were assigned to visit each house monthly in designated problem areas to vaccinate residents and to detect cases. In both countries, surveillance systems gradually improved and by late 1968 were well established, effective national programme leadership being provided by Dr G. F. Glokpor, Chief of the Division of Epidemiology in the Ministry of Health in Togo, and by Dr Yekpe in Dahomey. The number of vaccinations in 1968 rose to 990 000 in Dahomey but remained almost at the same level as in 1967 in Togo. In 1968, the number of reported cases decreased to 367 in Dahomey but rose to 784 in Togo—mainly owing to more complete notification.
The continuing high incidence of smallpox in Togo and reports that the entire population of villages had fled from the teams led to two studies in January 1969, one to determine what role fetish worship played in resistance to vaccination and what could be done about it, and the other to ascertain overall levels of vaccinial immunity. Mr Gordon Robbins, the health education adviser from the CDC regional office in Lagos, conducted the fetishism study (Robbins, 1970). He discovered that the resistance to vaccination had less to do with fetish practices and attitudes than with the concern of villagers about government teams in general, many of which were then engaged in tax collection and military conscription. As he learned, many of the feticheurs themselves, as well as their families, had been vaccinated. To measure overall levels of immunity, a national cluster sample survey was conducted. The survey showed that immunity was surprisingly high in all age groups, except among infants under 1 year of age (Table 17.13). From these findings, it seemed unlikely that smallpox transmission could persist for long, especially with the greatly strengthened systems for case detection and containment then operating. Indeed, the last case in Togo occurred in May and the last in Dahomey in September.
Table 17.13: Togo: levels of smallpox immunity by age, January 1969
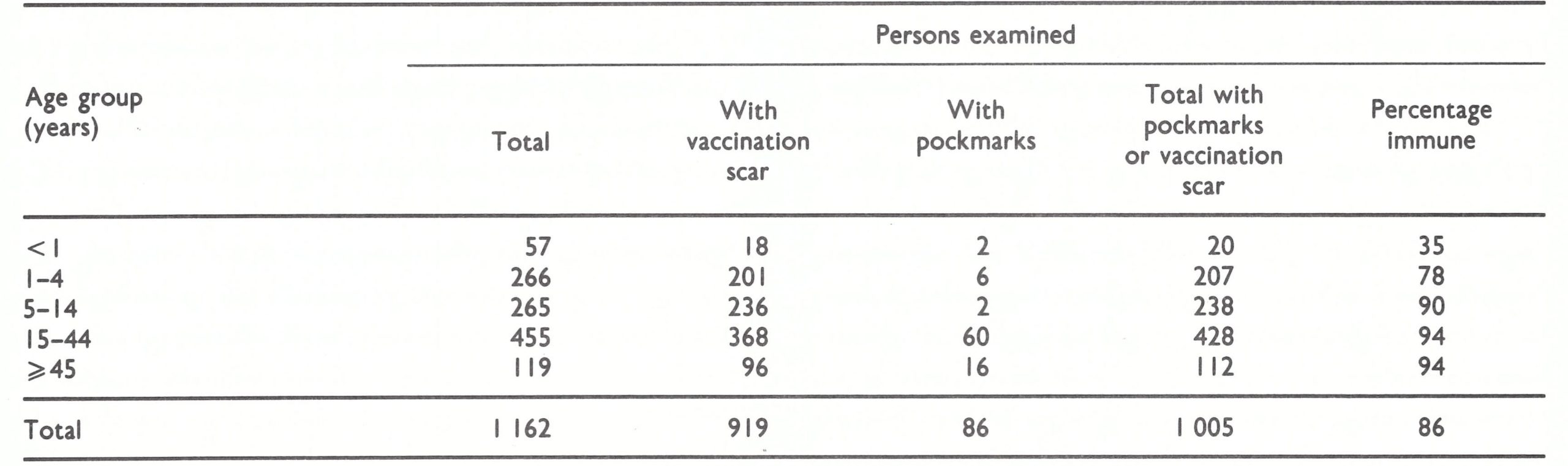
Observations made during the surveillance programme in Togo during 1969 are of interest (WHO/SE/70 .21, Glokpor & Agle). In that year 45 outbreaks were reported, of which 17 were notified by the routine report ing centres, comprising 190 dispensaries and polyclinics and 15 hospitals; 9 were found by smallpox teams in the field; and 19 were reported by other sources. The other sources included a radio-club president, village chiefs, a civil administrator, a social worker, an employee of the social welfare bureau, and members of malaria control spraying teams. Twenty-five of the 45 reported outbreaks were confirmed to be smallpox; two-thirds of the outbreaks and more than half the cases were in generally remote and isolated villages of less than 200 inhabitants. In these places vaccination coverage was usually found to be lower than 50%.
The differences between the number of smallpox cases routinely notified and the number actually confirmed are shown in Table 17.14. If routine notification data had been accepted, 21 cases would have been recorded in 1969, the pattern of occurrence suggesting that smallpox had been transmitted continuously throughout the year. During the investigation of these 21 cases, as well as that of 64 other suspected cases reported by other sources, a total of 215 cases of fever with rash were identified, of which only 83 were smallpox. All occurred between January and May.
Of the 61 cases discovered in Togo during April and May 1969, all but 2 were in riverine areas, difficult of access, in the south-east near the border with Dahomey. There, resistance to vaccination had been the greatest and, despite two intensive vaccination campaigns, only 60% of the population had vaccination scars (Table 17.15). Early in April, programme staff were notified of suspected cases by a health centre and, on investigation, they discovered 8 outbreaks with a total of 47 case. The first of the cases had occurred 2 months before but neither these nor subsequent cases had been reported by the responsible health worker, who, as was later discovered, had vacated his post in January. With transmission apparently close to being interrupted, the President of Togo requested the army to form a cordon sanitaire around the areas, and police accompanied teams to lend authority to the effort; markets were closed and public gatherings forbidden. Personnel drawn from other regions vaccinated 45 420 persons in April, a figure which, by September, had grown to 248 854. The last 2 cases in this series of outbreaks occurred towards the end of April, less than 3 weeks after the initial discovery of cases. A survey in September showed that vaccinial immunity had increased from 60% to 93%.
Togos last 2 outbreaks, numbering 6 cases in all, were discovered in May 1969 in isolated but reasonably well vaccinated fishing villages near the border with Dahomey. These were apparently the last cases of a major epidemic which had occurred throughout the area late in the preceding year.
Table 17.14: Togo: number of cases of smallpox by month, 1969
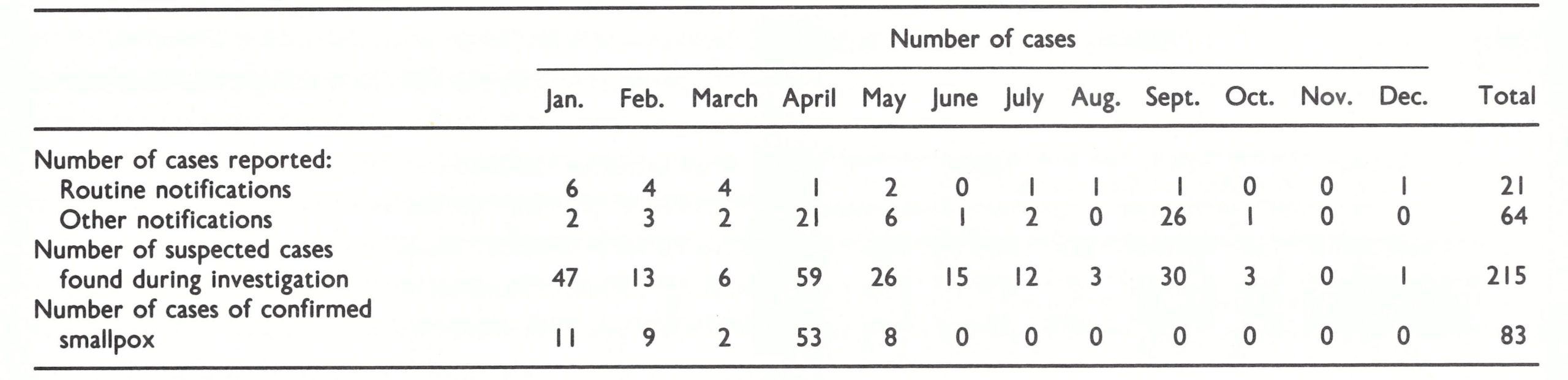
Table 17.15: Amecho-Vogan area, Togo: vaccinial immunity by age before and after April 1969, as ascertained by survey in September 1969
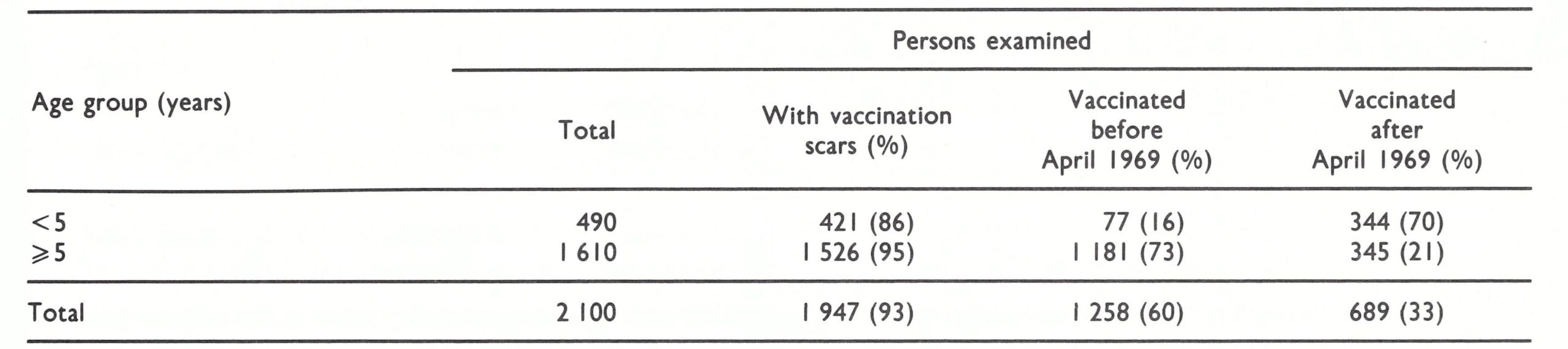
Transmission appeared to have been interrupted in Dahomey in January 1969, but in July an infant from Dahomey was diagnosed as a smallpox patient in a dispensary in Togo near the border. Teams from the two countries converged on the area in a coordinated search and vaccination operation on both sides of the border. In all, 55 further cases occurred in Dahomey over the next 2 months but in September 1969 the last case was detected. Until March 1970 (see the section on Nigeria, above) this was thought to have been the last case in western and central Africa.
Programme staff in Togo collected data regarding the age distribution of most smallpox cases occurring between 1967 and 1969; these are presented in Table 17.16. It is of interest that each year 40-50% of all cases occurred among persons aged 15 years and over. This finding reflected the occurrence of the disease in isolated rural villages which experienced smallpox only infrequently and whose inhabitants were poorly vaccinate.
Although programmes in Dahomey and Togo had only limited resources, they began to function reasonably well after little more than a year, and only 18 months later transmission was interrupted. Resistance to vaccination in the southern areas of the countries proved to be a problem, although variolation, associated with fetish practices, was observed only once during the course of the programme.
Table 17.16: Togo: number and percentage distribution of cases of smallpox by age, 1967-1969a
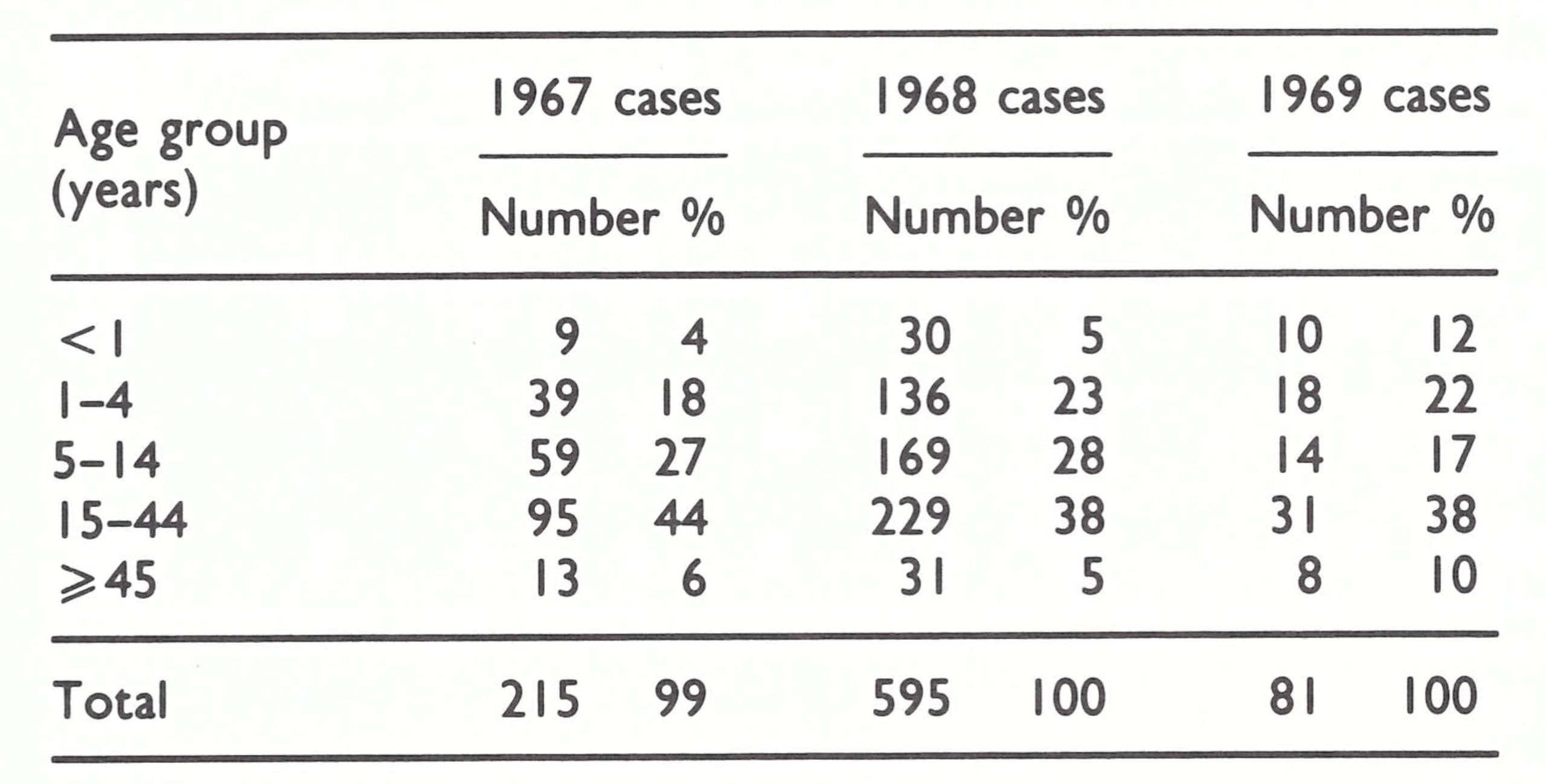 a Details are not available for 3085 other cases reported during this period.
a Details are not available for 3085 other cases reported during this period.
Mali, Niger and Upper Volta
The third of the 7 groups of countries are 3 inland states, which extend over 2.8 million square kilometres in the central part of western Africa—Mali (population in 1967, 5.3 million), Niger (population, 3.9 million), and Upper Volta (population, 4.8 million). Topographically, the area encompassed by these countries consists of desert in the north, giving way to the semi-desert areas of the Sahel and then to savanna in the south. In Upper Volta the population was evenly dispersed throughout the country, but in Mali and Niger the northern areas were very sparsely populated, virtually all of Mali’s population living in the southern half of the country and 90% of Niger’s being concentrated along the western and central segments of the Niger river, near the country’s southern border, in a belt less than 250 kilometres wide. Thus, although both Mali and Niger were far larger than Upper Volta, the areas with a significant concentration of population in these countries were only slightly greater than in Upper Volta. As in most parts of western and central Africa, roads were few and communications difficult.
The majority of the population were sedentary agriculturalists living in villages of fewer than 1000 inhabitants. Large numbers of pastoral nomads, however, were to be found in all 3 countries, being especially numerous in Mali and Niger. They were predominantly Tuareg and Peuhl tribal people, who moved along well-defined routes seeking pasturage for their animals. During the May—October rainy season, the nomads worked on farms or congregated in pasture areas, but during the October-April dry season, they migrated over great distances. During this period, smallpox spread extensively.
OCCGE had its headquarters in Upper Volta and the country’s endemic diseases control service, directed by a French military medical officer, was perhaps the best supported and most effective of such services in western Africa in 1967. In Niger, a similar service existed, but its performance was much less satisfactory. In Mali, which had ceased to receive financial support from France, the multi-purpose teams no longer functioned, having been replaced in 1962 by 2 mobile smallpox vaccination teams.
In these countries, in which health services were traditionally provided by mobile teams, there was both interest in and a structure for a large-scale combined smallpox and measles vaccination campaign. As has been described earlier, Upper Volta had, in fact, completed a national measles vaccination campaign in 1962. However, the assessment of vaccination coverage and surveillance were unknown practices, and government officials considered them unnecessary. Moreover, views differed within each of the countries as to whether separate teams should conduct the measles and smallpox vaccination campaigns or whether they should, in some manner, be incorporated into the scope of work of multipurpose teams. Because of these problems, there were delays in the signing of programme agreements, although all the programmes became operational by April 1967. In the end, none provided for ongoing assessment of vaccination coverage; surveillance activities, although originally intended to be conducted by national teams, became, by default, the responsibility of CDC advisers.
In Mali, a special smallpox vaccination campaign had been in progress since December 1962 with 2 teams, each composed of 15 persons, administering freeze-dried smallpox vaccine provided by the USSR and yellow fever vaccine produced in Senegal. Mali was handicapped by a lack of trained personnel, transport and petrol and requested assistance from WHO, which began to be provided in 1964; a WHO medical officer was assigned to the programme in December 1965.
A WHO team which assessed the Mali programme in February 1965 described the prospects for eradication there as “bleak” (World Health Organization, 1965b). In the campaign, vaccinators were expected to average 140 vaccinations a day, but even this modest target was not being met. At that rate of work, the WHO team estimated that it would take at least 8-10 years to complete one round of vaccination. Such vehicles as were available were old and frequently out of order, and refrigerators did not function. The vaccine was stored at ambient temperatures of up to 50°C, which caused it to deteriorate and the take rates to decline as a result. The vaccination campaign did not improve materially during 1965-1966, but the number of reported cases decreased significantly, reaching, in 1966, the lowest total ever recorded in Mali (Table 17.17).
With the offer of AID assistance, government health officials in Mali decided to reconstitute the multi-purpose mobile teams, 8 such teams being created to administer yellow fever vaccine, as well as smallpox and measles vaccine, and to examine and treat patients for onchocerciasis, trypanosomiasis and leprosy. The problems involved in drawing up plans and in training teams for this more complex set of activities delayed the launching of the programme. Further delays resulted from the government’s insistence that each trip the CDC advisers (Dr Pascal Imperato and Mr Jay Friedman) made outside the capital should be authorized weeks in advance. Although this requirement applied to all foreign advisers at the time, it was apparent that this policy would seriously handicap the necessary training of staff and all but preclude the establishment of surveillance and containment measures. The problem was compounded by a lack of collaboration between the smallpox eradication adviser assigned by WHO and the CDC staff, which resulted in the government’s receiving contradictory advice. In view of the many constraints and frustrations, senior CDC smallpox eradication staff proposed suspending assistance until the problems could be sorted out. When confronted with this possibility, the government decided to give the advisers full freedom to travel; a new Chief Medical Officer, Dr Ousmane Sow, was appointed; and the WHO smallpox eradication officer completed his assignment and returned home. The campaign proceeded to gain rapid momentum. The complex logistics and problems of conducting a vaccination campaign in areas such as Mali have been described by Dr Imperato in his book, A Wind in Africa (Imperato, 1975).
Table 17.17: Mali, Niger and Upper Volta: numbers of reported cases of smallpox and vaccinations performed, 1962-1969
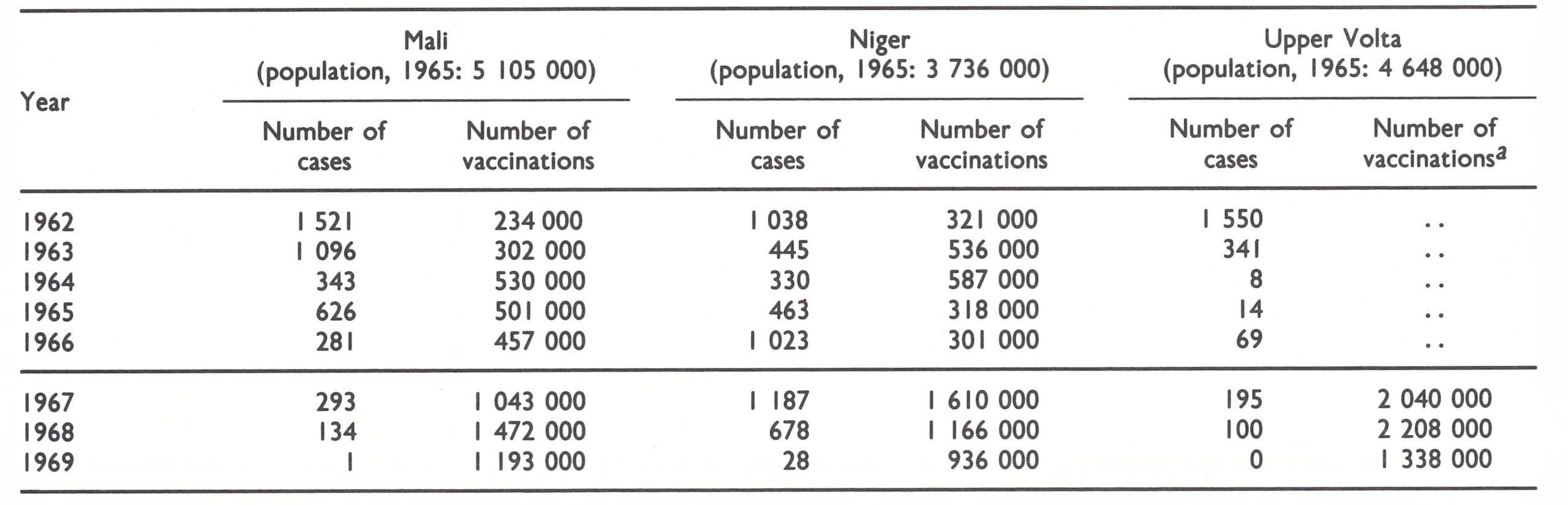 a..= data not recorded.
a..= data not recorded.
The teams began work in areas in the eastern part of the country, in which most cases of smallpox were then being reported. The cases were mainly among nomads and in remote rural areas (Imperato et al., 1972), a distribution attributed to the great distances separating the vaccination assembly points established during the 1962-1966 campaign. Early surveys in the more accessible areas revealed that 93% of the farmers, but only 54% of the nomads, had vaccination scars. In some areas, the inhabitants of entire villages, far from the assembly points, remained unvaccinated, as were many young children and elderly persons, who could not easily walk or be carried over long distances. Assembly Plate 17.13. Mass vaccination in Mali, using jet injectors. points continued to be used, as in the earlier campaign, but they were more numerous, requiring the villagers to travel less far.
In April 1967, the CDC advisers began to investigate some of the outbreaks. The first were in east-central Mali, in which mass vaccination had been completed in 1965 but, as was discovered, less than half the population had a vaccination scar. Smallpox transmission, nevertheless, was not rapid, even in the season of highest incidence. In one outbreak, for example, only 71 cases were found to have occurred over a 4-month period (Imperato, 1970). As the programme moved towards the border with Upper Volta, the teams began to encounter a large number of persons who refused vaccination and found that many women and children were hidden when the teams arrived. Vaccination continued throughout the east-central area, 521 000 people being vaccinated over a 2-month period beginning in October 1967. Although programme staff had expected to find epidemic smallpox occurring widely throughout the country, only 293 cases were discovered during 1967, most of which were in areas bordering on Upper Volta, in which a mass vaccination campaign was in progress. Of the total, 145 cases occurred in a cluster of 5 villages whose aggregate population was only 3700. Variolation was responsible for some of the cases—the only occasion on which variolation was observed in Mali.

Plate 17.13. Mass vaccination in Mali, using jet injectors.
Following the mass campaign in the endemic border areas, 2 further outbreaks, of 12 and 28 cases, were discovered in March 1968 among unvaccinated children who had been hidden from the teams (Imperato et al .,1973). Repeat vaccination in the respective villages quickly terminated the outbreaks, and for 6 months no further cases were found or notified in the entire country. It appeared that smallpox transmission in Mali had been interrupted by the time the vaccination campaign was little more than a quarter of the way towards completion.
On 6 November 1968, however, programme staff in Mali received a telegram from Upper Volta informing them that the first case in an outbreak near the border had come from a village in Mali. The Upper Volta outbreak—the last in that country—had begun in May 1968 and although 6 months had elapsed since the first case had entered Upper Volta from Mali, programme staff from the two countries agreed that a joint search should be undertaken . This began on 14 November. The village from which the initial case had come was 10 kilometres from a road and could be reached only by a narrow footpath through a mountainous rocky area . On arrival, the teams discovered that the village consisted of 8 widely separated groups of huts with a population of about 1350 people. During the vaccination campaign, which had concluded 1 year previously, the villagers had been directed to visit an assembly point 10 kilometres away, but few had done so. An outbreak had begun in late 1967 and spread progressively from one of these groups of huts to another.
Despite the fact that this was then Mali’s only known focus of smallpox, the containment measures were surprisingly incomplete: only 541 villagers (40%)were vaccinated and only 16% of them were found to have vaccination scars . Pockmarks indicative of recent smallpox were observed in 65 of the 541 people examined, the last person to contract the disease having become ill in October 1968, a month before the team’s arrival.
Only 1 further case was discovered in Mali, in February 1969; it occurred in a migrant tribal group believed to have been infected in Niger. This was the last of 9 known outbreaks, comprising a total of 370 cases, which had originated among migrant Tuaregs and Peuhl nomads between 1967 and 1968, and accounting for more than three-fourths of all cases recorded in Mali (Sow, 1970).
In Upper Volta, smallpox vaccination had been a routine activity of the mobile multipurpose teams, and the director wanted to continue this practice. He believed, correctly, that smallpox was then substantially under control and saw no reason to mount a special effort, since he did not consider eradication of the disease to be achievable. However, he decided to create special teams to administer measles vaccine, much as had been done in the 1962 campaign.
Smallpox incidence in Upper Volta had diminished greatly after 1962, as it had in Mali. Because there were comparatively few cases and responsibility for the smallpox vaccination campaign had been assumed by the endemic diseases control service, the CDC advisers, Dr Christopher D’Amanda and Mr William White, devoted substantial time to the improvement of reporting and the investigation and containment of outbreaks. In 1967 they discovered 195 cases, mainly along a north-south route used by pastoral nomads. In 1968, however, the epidemiological pattern changed. Only 100 cases were found, all of them in small villages near the border with Mali or Niger (D’Amanda, 1970). One outbreak of 19 cases in a village only 3 kilometres from the border with Niger led to a joint vaccination campaign by teams from Niger and Upper Volta. In October 1968, the last outbreak in Upper Volta was discovered by one of the multi-purpose teams in a village of 650 persons situated in a rocky mountainous area near the border with Mali. Forty cases had occurred between May and October, the first being infected in Mali; only 2 patients remained with active disease. Thorough vaccination in this and neighbouring villages quickly stopped transmission.
The concentration of cases along the frontier areas, in which health dispensaries were the most scarce, led to changes in the programme strategy in 1969. The schedule of the multi-purpose teams was altered to achieve a thorough coverage of the frontier areas, and the 604 mobile and established health units, as well as members of mobile teams giving leprosy treatment, were asked to supply weekly reports. The new system elicited many additional rumours of smallpox cases, but transmission had ceased by then and no importations were detected.
For Niger, smallpox was a much greater problem than for Mali or Upper Volta. In all, 1023 cases were recorded in Niger in 1966 and 1187 in 1967. Until 1967, the numbers of smallpox vaccinations given by mobile teams, in proportion to population, were comparable to those in Mali, but the campaign in Niger had not achieved effective smallpox control. In part, the failure could be attributed to the high ambient temperature and the inactivation over time of improperly stored freezedried vaccine. This was apparent from studies conducted in early 1967 which showed primary take rates of only 20-25%. Another contributory factor was Niger’s proximity to northern Nigeria. Most of the population lived within 250 kilometres of the Nigerian border, and many travellers crossed it. Mali and Upper Volta, in contrast, were at a considerable distance from the heavily endemic coastal areas of neighbouring countries
Of special concern to the CDC advisers, Dr Donald Moore and Mr Anthony Masso, as well as to the national programme staff, were the nomads, estimated to number about 530 000. They travelled widely throughout Niger and to neighbouring countries and were, therefore, considered to constitute a special risk in the spread of smallpox. Moreover, they were said to practise variolation when outbreaks did occur, thereby amplifying the outbreaks and increasing dissemination.
The vaccination campaign, utilizing teams devoted solely to giving smallpox and measles vaccine, began well and, by the end of 1967, 1.61 million people-equivalent to 41 % of the population had been vaccinated. A component of the programme during its first year was a special campaign aimed at vaccinating nomads, some 150 000 of whom gathered annually in a pasturage area 600 kilometres from the capital. Although the strategy was sensible, it proved to be a far more difficult endeavour than had been expected when the rains turned the few dry roads into a quagmire which could scarcely be traversed even with 4-wheel-drive vehicles. A sand storm ripped the tents and scattered the camping equipment, and the nomads sought to evade the teams, fearing that they were also engaged in tax collection. Ultimately, as was revealed by assessment, only 45% of the population were vaccinated.
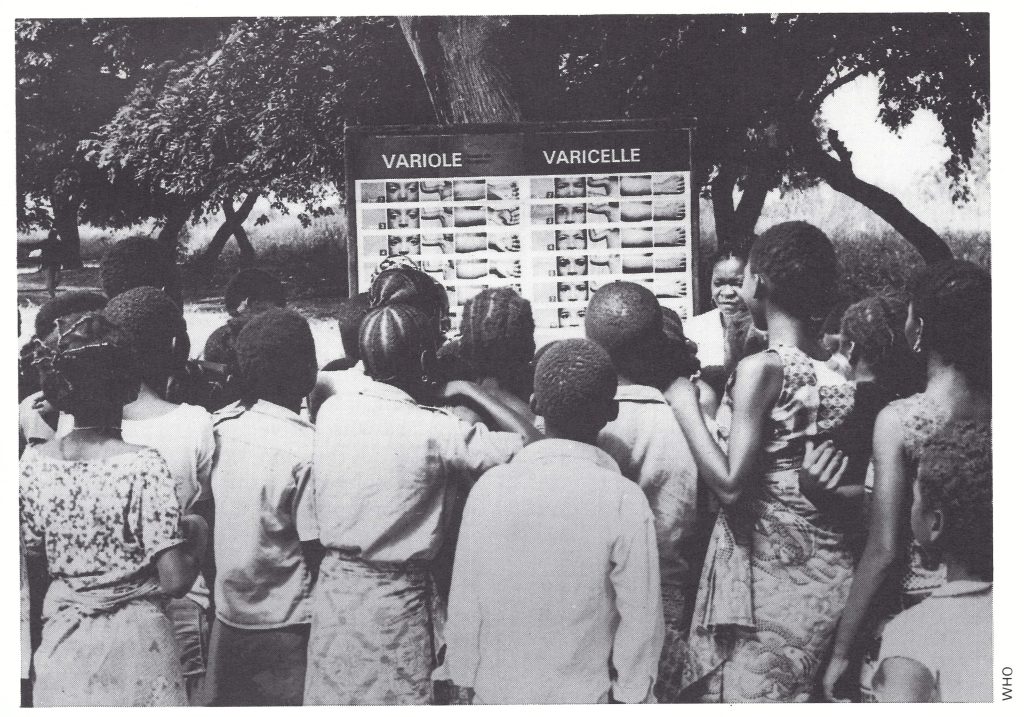
Plate 17.14. In Niger, a health worker uses the WHO diagnostic wall chart to explain the difference between smallpox and chickenpox, an important educational activity in the surveillance phase of the programme.
In 1967 and the early months of 1968, some outbreaks in Niger were investigated and containment vaccinations performed, but the principal effort was directed to the difficult logistics of the vaccination campaign. During the first 6 months of 1968, an additional 725 000 persons were vaccinated, following which—and coincidentally with the beginning of the seasonal rains—smallpox incidence declined sharply and did not increase again. Only 24 cases were recorded during the last 6 months of 1968 and another 28 cases in 1969. Although they were not fully documented, all the cases in 1969 are believed to have resulted from importations from Nigeria.
Despite the concern of programme staff, nomads in Niger—unlike those in Mali and Upper Volta were found to play only a minor role in transmitting smallpox from place to place, even in the more densely populated areas. In the vast but sparsely populated northern regions of Niger, in which an estimated 150 000 nomads lived, only 1 case was discovered. That smallpox did not spread through this area was welcome but unexpected, and was probably partly due to a comparatively high level of immunity induced by vaccination as well as variolation (Masco, 1970). In a survey conducted in 1969, 38% of the nomads examined were found to have vaccination scars, but an additional 29 had the scars of variolation. Evidence of past variolation was frequently observed—in different parts of Niger, and although the practice was originally believed by health staff to be important in sustaining transmission, only a single instance of recent variolation was observed—in October 1967 in a village near the Nigerian border.
The transmission of smallpox in Mali, Niger and Upper Volta was interrupted more rapidly than had been foreseen, but the problems of logistics and vaccination proved greater than expected. In Mali and Upper Volta, previous vaccination campaigns had been successful in sharply reducing the incidence of smallpox, and in less than 2 years—in November 1968—transmission was interrupted in both countries. In Niger, smallpox incidence was high at the outset of the programme, but the vaccination campaign progressed rapidly and transmission was interrupted at about the same time as in the other countries.
Guinea and Sierra Leone
The fourth of the 7 groups of countries to be discussed consists of 2 neighbouring coastal countries, Guinea and Sierra Leone. Programmes in both countries began in December 1967, nearly 12 months after the regional programme had started. As has been noted earlier in this chapter, the reason for the delay was that the CDC staff wanted to phase in activities over a 2-year period. When this decision was made, the fact was not recognized that cycles of epidemic smallpox had recurred in these countries at intervals of 10-12 years. Major epidemics had occurred in Sierra Leone in 1956-1958, and in Guinea in 1955-1957, although in the latter country nearly 3000 cases occurred only 5 years later, in 1962. In both countries, epidemic smallpox recurred early in 1967 (Table 17.18). Sierra Leone (population, 2.7 million) recorded 1697 cases and Guinea (population, 3.7 million) 1530 cases, giving incidence rates for that year which were among the highest in the world. In aggregate, the total number of cases represented nearly a 10-fold increase in incidence over 1966.
The launching of both campaigns in December 1967 coincided with the advent of the dry season-the season of highest incidence-and the beginning of the second year of the epidemic. Smallpox being a matter of much concern at the time, Guinea and Sierra Leone gave their full support to the programme and developed plans to complete the mass vaccination campaign within 16 and 24 months, respectively. In the summer of 1968, case detection and outbreak containment were given special emphasis. Smallpox incidence declined rapidly, and the last cases were recorded in January 1969 in Guinea and in May 1969 in Sierra Leone. Benefiting from experience in the other countries of western and central Africa, these programmes were the best executed and the best documented. An account of the programme in Sierra Leone has been given by Dr Evelyn Cummings, the Chief Medical Officer, and Dr Donald Hopkins and Mr James Thornton of CDC, and their colleagues (Hopkins et al .,1971a,b,c) . Guinea’s programme has been described by Dr A. B. Alecaut, the director of the country’s endemic diseases control service, and Dr Joel Breman, the CDC medical epidemiologist, and their colleagues (Alecaut et al .,1970; Breman, 1971; Breman et al .,1977a,b).
The population in both countries consisted primarily of sedentary farmers living in villages of less than 1000 inhabitants, most of which were not readily accessible by motor vehicle. The most densely populated part was the coastal area from Freetown, the capital of Sierra Leone, to Conakry, the capital of Guinea. In the more sparsely populated area comprising north-eastern Guinea and northeastern Sierra Leone, cattle herders moved freely between the two countries. Work in the diamond mines of eastern Sierra Leone attracted many farmers during the dry season.
In 1967, neither country had a continuing special programme for smallpox vaccination. Vaccinations were performed by the established health units and, in Sierra Leone, by a mobile unit of the endemic diseases control service, which periodically conducted smallscale mass vaccination campaigns. Approximately 700 000 persons were reported to have been vaccinated each year in Guinea and 300 000 in Sierra Leone. In Guinea, freezedried vaccine from Switzerland and the USSR began to be used in the early 1960s. Sierra Leone, like Nigeria, employed the thermolabile lanolinated vaccine purchased from the United Kingdom or Nigeria. Surveys in Sierra Leone when the programme began revealed vaccination scars in only 26% of those under 15 years of age and in 60% of older persons. Overall, almost half the population of Sierra Leone was considered to be susceptible to smallpox. Comparable data from Guinea are not available.
Smallpox incidence began to increase in Sierra Leone in 1966 (Table 17.18); in 1967 the disease became endemic throughout the country, the eastern areas being the most affected. In Guinea, the incidence started to increase a year later, the most heavily afflicted areas being the coastal districts bordering on Sierra Leone (Fig. 17.7.). Because of the spreading epidemic, an emergency mass campaign was conducted in Conakry in February and March 1967, during which 180 000 of the city’s 250 000 inhabitants were vaccinated.
In Guinea, the AID-supported vaccination campaign began in December 1967, utilizing, as supervisory personnel, senior staff of the former endemic diseases control service, which, by 1967, had ceased to function owing to a lack of vehicles and of funds for petrol and equipment. Vaccination was conducted by 8 mobile teams of 6 persons each: a team leader, 2 vaccinators, a recorder, a driver and an “advance man”. The last-named visited leaders of the well-organized political party in each area and village prior to the team’s arrival, in order to acquaint them with the programme and to obtain their support. To simplify the logistics of providing supplies, all teams worked together in a given region of the country, vaccinating at assembly points situated so that villagers had to walk no more than 2-3 kilometres. Local costs, which amounted to US$10 000 per annum, were covered by WHO.
Table 17.18: Guinea and Sierra Leone: number of reported cases of smallpox, 1960-1969
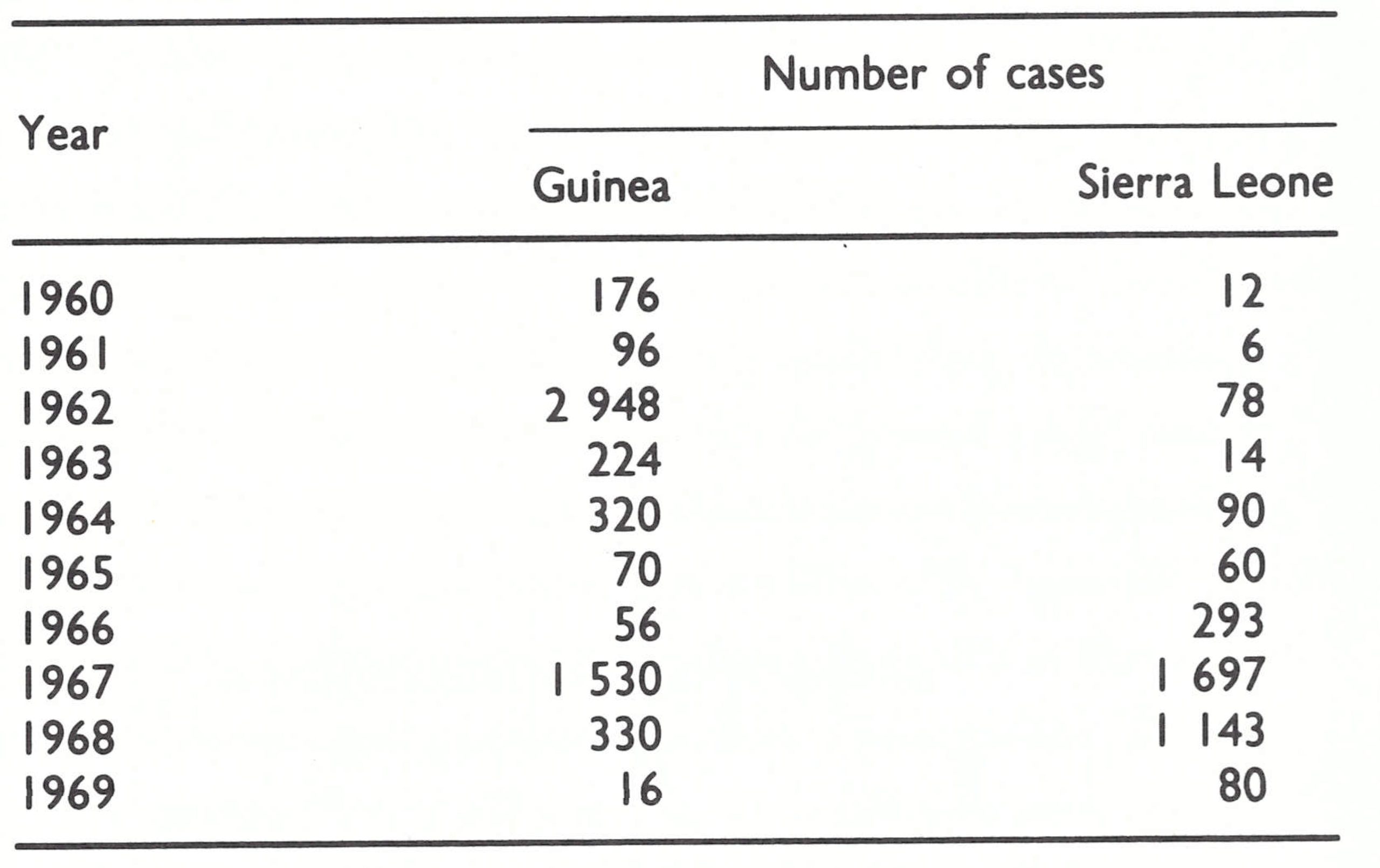
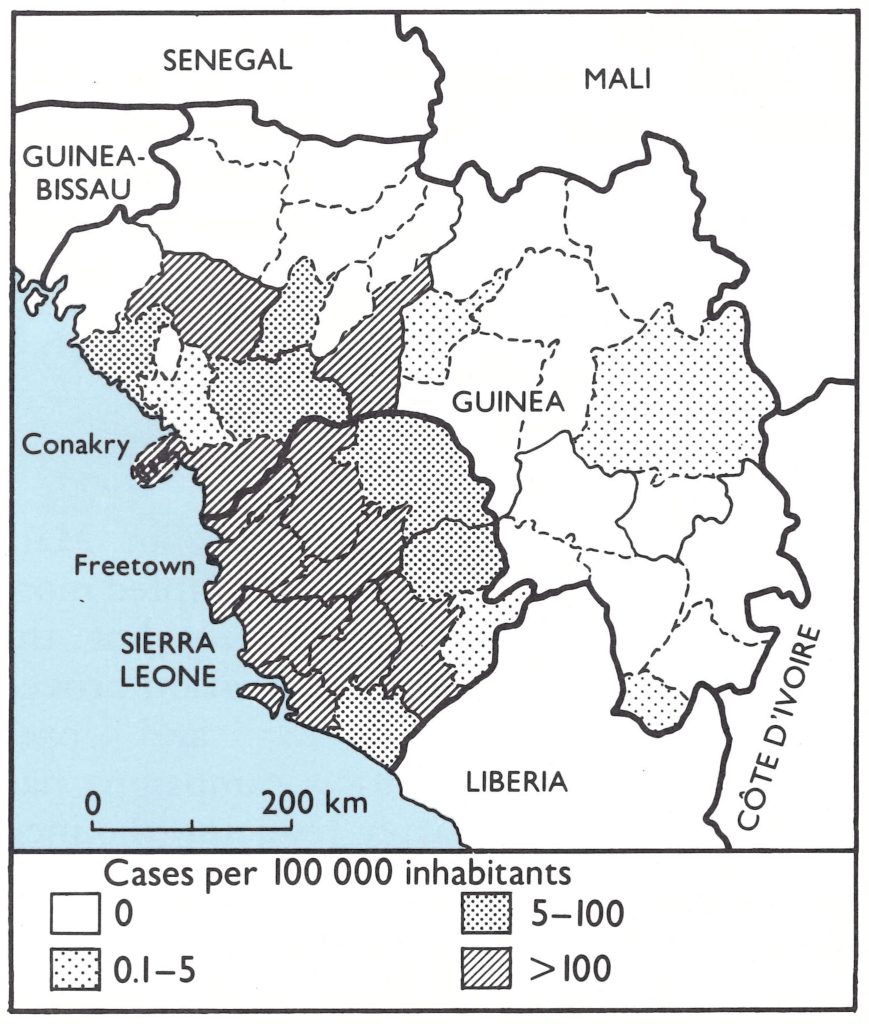
Fig. 17.7. Guinea and Sierra Leone: smallpox incidence, by province, 1967.
From the beginning, vaccination coverage in Guinea was carefully assessed. Two methods were used. The first, performed when the teams were working in the village, consisted simply in comparing the numbers vaccinated with the population census. If the numbers vaccinated seemed to be low, local party officials were asked to search for those who had been missed, and send them for vaccination. Where vaccination coverage was particularly low, a special team was assigned to conduct repeat mass vaccination and vaccine was sometimes left with regional officials, who were asked to vaccinate the people who had been missed.
The second form of assessment, conducted a week later by a senior technical officer of the programme and an assistant, utilized the modified cluster sample technique devised by Dr Ralph Henderson (Henderson et al., 1973); this required the examination of a number of persons sufficient to ensure, with 95% confidence, that the results obtained were within 10% of the true value. Although this was a more sophisticated survey method than that routinely employed in other programmes, it was well executed. As the programme progressed, it was found that the results of the two types of assessment usually corresponded well, due primarily to close supervision of teams and the availability of unusually accurate census data.
With the active cooperation of party leaders, the levels of vaccinial immunity achieved usually exceeded 80% and more often 90%. The teams themselves averaged 2000 smallpox vaccinations a day and, in addition, provided measles vaccination to all children between 6 months and 4 years of age.
From January to October 1968, the end of the rainy season, the residents of Conakry and of all districts bordering on Sierra Leone were systematically vaccinated (Fig. 17.8). These areas included most parts of the country then known to be infected with smallpox.
The investigation and containment of outbreaks began within months of the start of the mass vaccination campaign . In June 1968, a special surveillance team was assigned this responsibility and asked to make a village-byvillage search for cases in high-risk areas. By then, owing to the decrease in incidence during the rainy season and the high levels of vaccinial immunity in previously infected areas, smallpox had all but disappeared. From July 1968 to the end of January 1969, only 8 outbreaks, with a total of 75 cases, were discovered, almost all in villages of less than 500 inhabitants. All were in western Guinea, near the border with Sierra Leone, and 5 of the 8 were thought to have originated in that country. In each instance, information regarding the source of infection was cabled promptly to Sierra Leone. The last known case in Guinea was reported and investigated in January 1969, though it actually occurred in December 1968.
The first phase of the systematic vaccination campaign continued until June 1969. In all, 3.1 million smallpox vaccinations were given during the 18-month period, another 2.6 million during a subsequent 2-year cycle, and a further 2 million in a third 2-year vaccination cycle. Meanwhile, weekly reports from each of the 29 regions were being received with increasing regularity. In 1968, 33 % of the expected reports were received a proportion which increased to 60% in 1969, and to 87% in 1970.
The smallpox problem in Sierra Leone differed from that in Guinea in that the disease was widespread throughout the country. The campaign, which began in January 1968, utilized the staff of the endemic diseases control service, which had previously been responsible for 43 treatment centres for yaws and trypanosomiasis. Six teams performed the vaccinations and one the assessment. The composition of the teams and their methods of work were similar to the system operating in Guinea. Priority was given to eastern Sierra Leone, in which smallpox incidence was the highest, presumably because of a large population turnover associated with diamond mining and the migration of cattle herders. Because of the epidemics, attention was initially concentrated on vaccinating as widely and as rapidly as possible before the end of the rainy season in 1968 and the commencement of the expected seasonal increase early in 1969.
The help of tribal chiefs in the 146 chiefdoms was necessary to obtain the cooperation of villagers. Although the chiefs were generally receptive, they proved to be less effective than Guinea’s political party leaders. Efforts were made to achieve a vaccination coverage of 80% or more in all areas, but assessment showed that it was usually no greater than 75%.
A few outbreaks were investigated between January and August 1968, but a concerted effort to investigate and to contain all reported outbreaks did not begin until August, when the regional “eradication-escalation” activity commenced. Vaccination teams were assigned in rotation to this duty. As in Guinea and in other countries at this time, outbreak containment consisted primarily of 1-2 days of intensive vaccination in the infected village, in neighbouring villages and in nearby markets. Patients were isolated in their houses, a traditional practice in most of this part of Africa. Nearly all the cases (94.5%) in Sierra Leone occurred in villages of less than 1000 inhabitants and although containment measures were less rigorous than in the later phases of the Intensified Smallpox Eradication Programme, most outbreaks ended quickly . Studies by the programme staff showed that no secondary cases occurred in villages in which coverage was greater than 80%, and 1-9 secondary cases in those in which vaccinial immunity was less than 70%.
An unusual feature of smallpox transmission in Sierra Leone was the occurrence of outbreaks associated with special funeral ceremonies for smallpox victims. In two documented outbreaks (Hopkins et al., 1971c), cases occurred among members of secret societies who washed the corpse of the smallpox victim and among others who attended special funeral services. One of the outbreaks gave rise to 33 cases among contacts at the funeral and an additional 97 cases due to further spread ; the other resulted in 10 contact cases and 2 cases due to secondary spread. While secret societies were prevalent throughout western Africa, and other such outbreaks were believed to have occurred in Sierra Leone, these were the only ones which could be documented.
Plate 17.15. Donald R. Hopkins (b. 1941), a CDC epidemiologist, served as the senior adviser to the programme in Sierra Leone. Although the incidence of smallpox in Sierra Leone was among the highest in the world in 1967, it was possible to interrupt transmission in only 16 months. Hopkins later wrote a history of smallpox, Princes and Peasants.
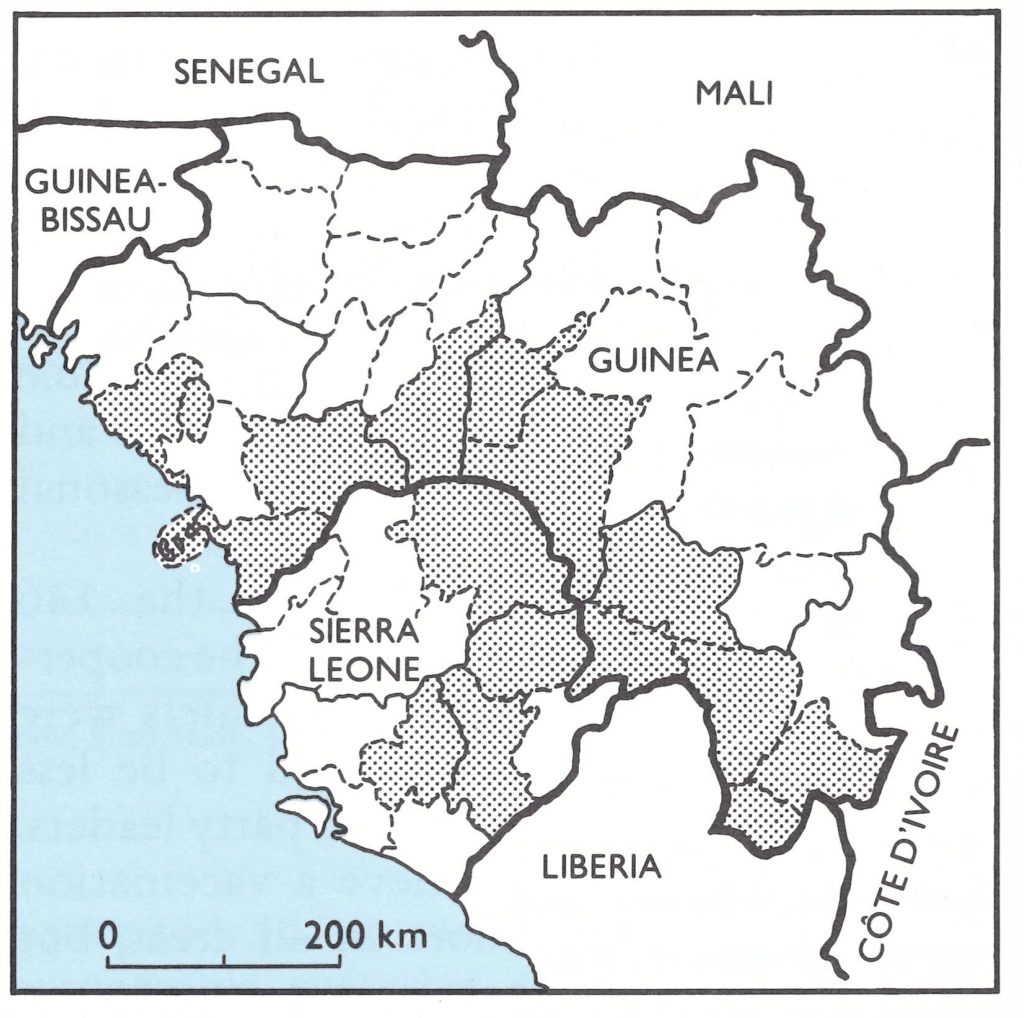
Fig. 17.8. Guinea and Sierra Leone: areas (shaded) in which mass vaccination was completed before the end of the rainy season, October 1968.
From August 1968 onwards, the number of cases in Sierra Leone decreased steadily and from January to the end of April 1969, only 12 outbreaks, with a total of 80 cases, were found, all but one situated in coastal areas in which mass vaccination had not yet been conducted. On 5 April, the last case occurred, in Freetown; it was not officially reported until May and the source of infection was not discovered.
An important contribution to the success of the programme was the monthly publication of a mimeographed bulletin, The Eradicator, which was distributed widely to programme staff, medical officers, dispensers, civil officials, paramount chiefs and other interested persons. It reported on the programme’s progress, paid tribute to effective health workers and local officials and announced the schedule of activities for the coming month. When the intensified surveillance programme began in August 1968, the bulletin served to stimulate reporting throughout the country.
Data on the age distribution of cases and case-fatality rates in Guinea and Sierra Leone were more complete than in most national programmes, and it is pertinent to include them here, since they are probably representative of the situation in other countries of the region (Table 17.19).
In proportion to population, cases were more numerous among children than adults, but there was, nevertheless, an unusually large percentage of adult cases in what were considered to be endemic countries. Most of the cases, however, occurred in rural areas, in many of which smallpox had not been present for several decades. The low levels of vaccinial immunity in these areas, coupled with the infrequency of variolation, ensured the presence of many susceptible adults when outbreaks occurred. Because of the nature of data collection, the case-fatality rates probably understate the severity of the disease. Since in most of the fatal cases of smallpox, the patients did not die until the second or third week of illness, some who were acutely ill at the time of outbreak investigation may have died later but their deaths were not recorded. An overall case-fatality rate of perhaps 10-15%, depending on the age distribution of cases, would probably be more correct.
The programmes covering the comparatively small populations of Guinea and Sierra Leone, both highly endemic at the start, are of interest because of the rapidity with which they succeeded in interrupting transmission. Guinea’s last case occurred only 12 months, and Sierra Leone’s only 16 months, after the inception of their respective programmes. This achievement in two countries which were so lacking in health services, transport, and communications greatly encouraged regional and global smallpox eradication programme staff and, to some extent, a Data are not available for 41 cases in Guinea and 43 cases in Sierra Leone; in addition, the age distribution of 85 cases In Sierra Leone is unknown though their outcome was recorded. generated an unwarranted confidence that comparable successes could be achieved as readily in other parts of the world.
Table 17.19: Guinea and Sierra Leone: number of cases of and deaths from smallpox and case-fatality rate, by age, 1968-1969
 a Data are not available for 41 cases in Guinea and 43 cases in Sierra Leone ; in addition, the age distribution of 85 cases In Sierra Leone is unknown though their outcome was recorded.
a Data are not available for 41 cases in Guinea and 43 cases in Sierra Leone ; in addition, the age distribution of 85 cases In Sierra Leone is unknown though their outcome was recorded.
Cote d’Ivoire, Ghana and Liberia
In the adjoining countries of C6te d’Ivoire, Ghana and Liberia, smallpox had largely been brought under control by 1967; C6te d’Ivoire, in fact, had succeeded in interrupting transmission (Table 17.20). Each had achieved this status in a different manner: C6te d’Ivoire by mass vaccination, with little external assistance; Liberia through a mass vaccination campaign supported by a private voluntary organization; and Ghana by a remarkably effective programme of surveillance and containment.
Ghana is of special interest, being one of the few countries in which an effective programme of case investigation and outbreak control all but interrupted smallpox transmission despite a comparatively low level of vaccinial immunity in the population and the use of a thermolabile smallpox vaccine. Ghana was the second most heavily populated country in the western and central African region (population in 1967, 8.1 million), and in the 1950s and 1960s had one of the best-organized health services and networks of all-weather roads . A moderately extensive morbidity reporting system had been established, and a compulsory mortality registration scheme covered approximately half the population. Between 500 000 and 1 million persons were vaccinated annually in hospitals, health centres and health posts and by mobile rural health service teams (originally called medical field units). The thermolabile lanolinated vaccine produced in the United Kingdom was used exclusively until 1964, when freeze-dried vaccine began to be purchased from Switzerland. However, on the basis of field observations by a WHO adviser in 1965, and outbreak investigations in 1967, it can be assumed that overall vaccinial immunity was probably not greater than 50% when the programme began. Despite this, no more than 251 cases had been notified in any year since 1953—that is, during a period when many countries in western and central Africa with smaller populations reported 1000 or more cases every year. The explanation can be found in the existence of a corps of well-trained sanitarians who took special care to keep the vaccine refrigerated, investigated all outbreaks, isolated patients in a hospital or in separate quarters, vaccinated those living in the area and recorded the daily temperature of household contacts in order to detect additional cases as early as possible. Only 7 cases of smallpox were notified in 1965 and 13 in 1966.
The mass vaccination campaign began in February 1967 in the capital, Accra, utilizing the mobile health service teams to give both smallpox and measles vaccine. At the same time, senior Ghanaian programme staff, Dr Frank Grant and Dr V. de Sario, with the CDC advisers Dr Challenor, Dr David Melchinger and Mr James Lewis worked with local sanitarians in the investigation and containment of outbreaks. In all, 17 outbreaks, with 114 cases, were found in 1967. Two of these, with a total of 21 cases, were in Accra and affected only 7 households in an area populated by immigrants from Togo; 5 others, with 27 cases, were in southern Ghana, the Accra outbreaks being the source of one of them and Nigeria another; 10 outbreaks, with 66 cases, occurred in a cluster of small villages within a few kilometres of the point where the borders of Ghana, Togo and Upper Volta meet (WHO/SE/69.8, de Sario). The last group of outbreaks occurred in a tribal area in which no cases had been seen for 6 years but in which smallpox was well recognized by its name naba, which means “the chief of all the other diseases”. A source of infection in Togo or Upper Volta was suspected but not proved. Although the sources of infection could not be traced for all outbreaks, it is apparent that there was little endemic disease and few chains of transmission. During 1968, 24 additional cases in 6 outbreaks were discovered, all of which could be traced to importations from Togo, 2 of the outbreaks occurring very near the border, while the others were at a distance of more than 100 kilometres from it (Grant, 1970).
The mass vaccination campaign progressed steadily but more slowly than in most other countries of the region, being completed in 1970, 4 years after it had begun. Coverage levels, based on concurrent assessment, were consistently over 90%.
In Cote d’Ivoire (population in 1967, 4.9 million), smallpox had been an important problem in the early 1960s, 4656 cases having been reported in 1961. In August of that year, the government decided to embark on a special 3-year mass vaccination campaign using a freeze-dried vaccine produced in France and 5 mobile teams comprising 50 health staff. The responsibility for its execution was entrusted to the Institute of Hygiene in Abidjan and its director, Medecin-Colonel Gaston Binson. During the next 3 years, 3.6 million persons were vaccinated; a repeat 3-year campaign, lasting from 1964 to 1966, succeeded in vaccinating another 3.7 million. Smallpox incidence fell precipitously and by 1965, only 27 cases were notified, followed by 10 cases in 1966.
When assistance was provided by the USA, the government decided to undertake a third national smallpox vaccination campaign under the same leadership as before; other teams from the Ministry of Health, working independently, administered measles vaccine. The smallpox vaccination campaign differed somewhat from those in other countries in that the vaccine was administered by scarification rather than by jet injector. Dr Binson saw little virtue in speeding up the rate of vaccination by using the jet injector, since this was offset by the time-consuming process of preparing for each person vaccinated a signed personal vaccination certificate giving the individual’s name, the date of vaccination and the batch number of vaccine used. The preparation of a vaccination certificate was traditional in Cote d’Ivoire, as in many of the other francophone countries and, while most countries soon abandoned the practice or simply distributed certificates without the holder’s name inscribed, the traditional approach continued to be used in Cote d’Ivoire . Assessment of coverage was not performed. In November 1969, at the conclusion of the third national mass smallpox vaccination campaign, measles vaccination teams were merged with the smallpox teams, the practice of issuing vaccination certificates was abandoned and jet injectors began to be used for both antigens.
Table 17.20: Cote d'lvoire, Ghana and Liberia: number of reported cases of smallpox, 1961-1968
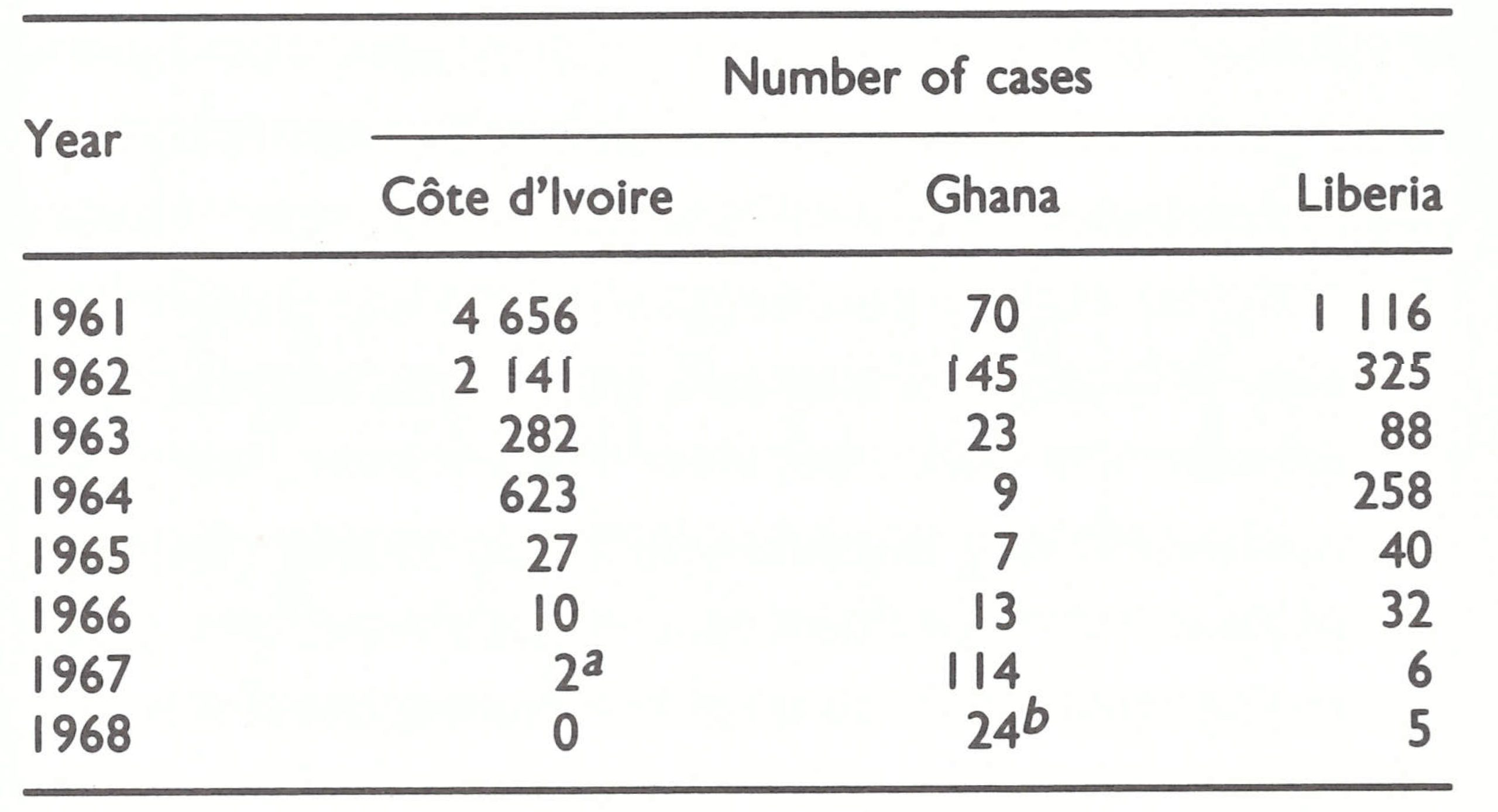 a Imported from Upper Volta.
a Imported from Upper Volta.
b Imported from Togo.
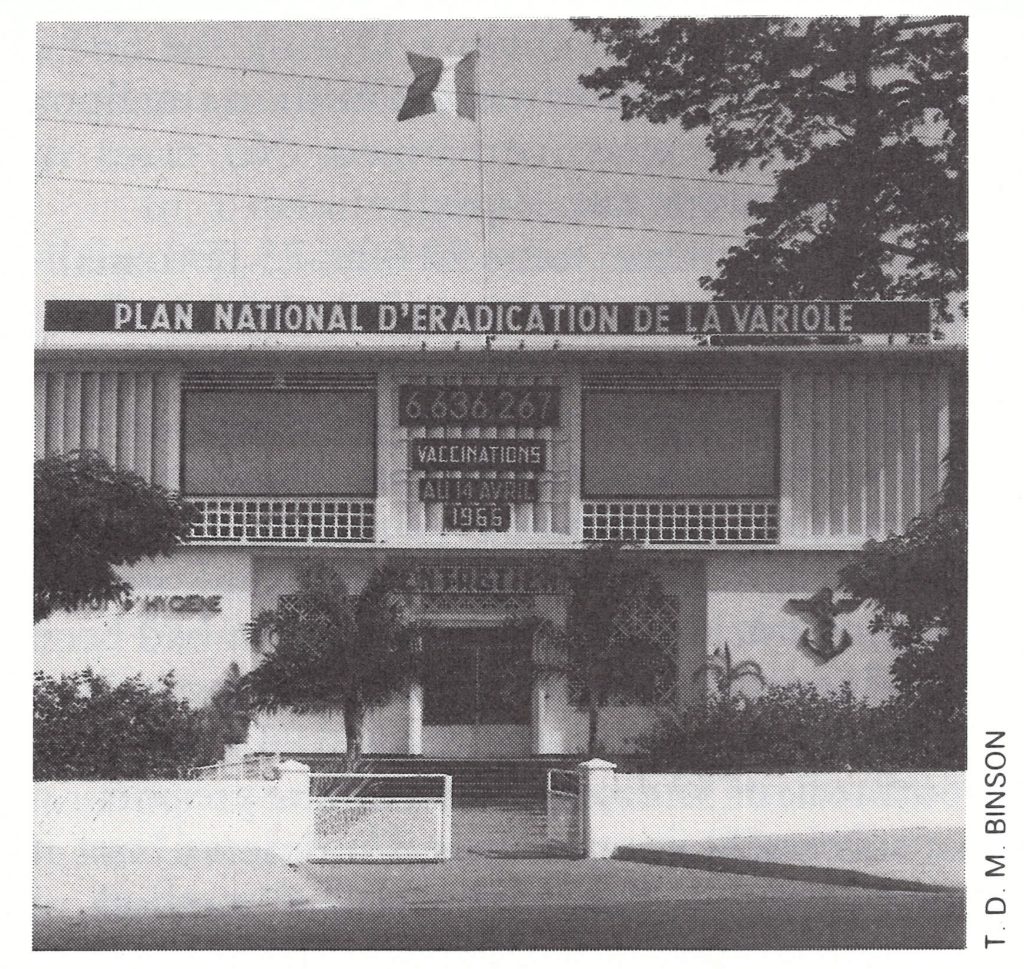
Plate 17.16. Headquarters of the national smallpox eradication programme at Abidjan, Cote d’Ivoire.
After the regional programme had commenced, only 2 cases of smallpox were discovered in Cote d’Ivoire, in March 1967, both of which were importations from Upper Volta. The cases did not appear in the official records, however, until 2 years later; the director of the programme, proud of its accomplishments, believed that the country’s record should not be blemished by 2 cases for which he did not feel responsible. Liberia (population in 1967, 1.3 million), which abutted on Cote d’Ivoire in the west, reported more than 1000 cases in 1961, and the following year began a smallpox vaccination campaign. It was directed by a religious organization called Brother’s Brother, which undertook mass vaccination through out the accessible, populated areas (Bryant, 1968). Over a 5-month period, some 775 000 vaccinations were reported to have been given, using jet injectors of a different type from those subsequently employed by CDC, and a freeze-dried vaccine, which was diluted approximately 15-fold owing to a lack of supplies. Neither vaccination take rates nor coverage was assessed.
After the 1-year mass campaign, WHO provided an adviser, Arita, and enough freeze-dried vaccine to permit a more systematic programme which utilized undiluted vaccine administered by scarification. That this was needed became apparent when Arita found that only 60-70% of persons had had successful primary vaccinations when vaccinated in accordance with the procedure used by the Brother’s Brother group. Progress in the WHO-supported programme was slow, but smallpox incidence continued to fall. Although the number of reported smallpox cases had averaged more than 1000 per annum from 1958 to 1962, only 325 cases were reported after the first mass campaign in 1962. The figure dropped to only 40 cases by 1965, to 32 by 1966 and to 6 by 1967.
The AID-supported campaign, which began early in 1968, progressed little more satisfactorily than had the campaigns in 1962-1967. Even with 7 vaccination teams, nearly 4 years were required to complete the operation. Assessment was seldom conducted and reporting remained almost as unsatisfactory at the conclusion of the programme as at the beginning. Nevertheless, a system which had notified hundreds of cases in previous years reported only 5 cases in 1968, all of which occurred during the first 3 months of that year. Nothing is known of these cases, since no reports of cases were investigated until April 1968. Some—perhaps all—may have been erroneously diagnosed, or they may have been importations. No further cases of smallpox were discovered by vaccination teams as they advanced systematically across the country, but in 1970 they did detect the first cases of human monkeypox outside Zaire (see Chapter 29).
The Gambia, Mauritania and Senegal
The Gambia, Mauritania and Senegal, 3 contiguous countries comprising the westernmost part of the region, recorded no cases of smallpox after 1966 (Table 17.21). The cessation of reported smallpox that year followed many years of effective control measures, especially in Senegal, which accounted for 70% of the area’s population (in 1967) of 5.3 million and which was economically the most developed. The Gambia, a strip of land 16 kilometres wide and 320 kilometres long, entirely surrounded, except for the coastal section, by Senegal, had a population of 438 000, which moved freely back and forth across the border. Not surprisingly, its experience with smallpox reflected that of Senegal. Mauritania, although 6 times larger than Senegal, was mostly desert. Because its predominantly nomadic population of 1.2 million was widely dispersed throughout the country, the transmission of smallpox was not easily sustained. After 1962, Mauritania reported 78 cases of smallpox—2 in 1965 and 76 in 1966. Government reports, however, note that the 1966 cases, all in a confined area, had never been confirmed by a physician and, in retrospect, chickenpox was thought to have been a more probable diagnosis.
In Senegal, the endemic diseases control service had been in operation for many years and had a personnel of 292 in 1967. With a reasonably extensive network of all-weather roads, the multi-purpose mobile teams were able to move comparatively easily throughout the country. Vaccinations, equivalent in number to about 20% of the population, were administered annually. Since the early 1960s, a good-quality freeze-dried vaccine produced in France had been used, a factor which undoubtedly contributed to the interruption of smallpox transmission. No surveys were performed either before or during the programme to assess the level of vaccinial immunity, but it was believed to be reasonably high. For the AID-supported programme, the government decided that the supplies and equipment provided should be utilized by its mobile teams, which endeavoured to visit all villages once every 3 years. During the first 3 years of the programme, 2.6 million smallpox vaccinations were performed. No cases of smallpox were discovered.
In the Gambia, some 50 000-75 000 smallpox vaccinations had been administered annually at health centres and dispensaries, using lanolinated vaccine produced in Nigeria. Few of the health units, however, had refrigeration equipment ; supplies of vaccine were distributed monthly and kept in wet cotton until used. Mass vaccination had been conducted only once during the preceding decade—in a localized area in 1963, when an outbreak of 52 cases occurred. The proportion of successful vaccinations is unknown, but it was probably not high, as the method of storage would not have preserved the thermolabile vaccine for more than a few days . Despite the presumably low levels of vaccinial immunity and the fact that 10% of the population was migratory, few cases of smallpox were recorded, the immune barrier provided by Senegal undoubtedly playing an important role in protecting the Gambia.
With assistance provided by the USA for smallpox and measles vaccination, 3 mobile teams were created, each consisting of 2 vaccinators, a tally clerk and a driver; a health superintendent, Mr Kebba A. M. Sanneh, supervised field activities. The mass vaccination campaign began in June 1967 and was completed in 10 months (167 working days), during which 350 000 people were vaccinated against smallpox and 81 000 against measles, an average of 2580 vaccinations a day. This far surpassed the expected average of 1500 vaccinations a day (see box). The continuing programme of maintenance vaccination was no less successful. Concurrent assessment regularly showed coverage rates of more than 90%, which were sufficiently high to interrupt measles transmission for more than 2 years. No cases of smallpox were discovered after the programme had begun.
Mauritania presented a set of problems quite different from those encountered either in the Gambia or in Senegal. Like Senegal and other former French colonies, Mauritania had had an endemic diseases control service, which consisted of 7 mobile teams, each composed of 5 health workers. About 125 000 people were being vaccinated annually against smallpox with a freeze-dried vaccine produced in France. However, in 1962, most senior staff of the service left Mauritania, and thereafter team activities diminished sharply, only penicillin and aspirin being distributed
during the period 1962-1967.
Table 17.21: Gambia, Mauritania, Senegal: number of reported cases of smallpox, 1961-1967
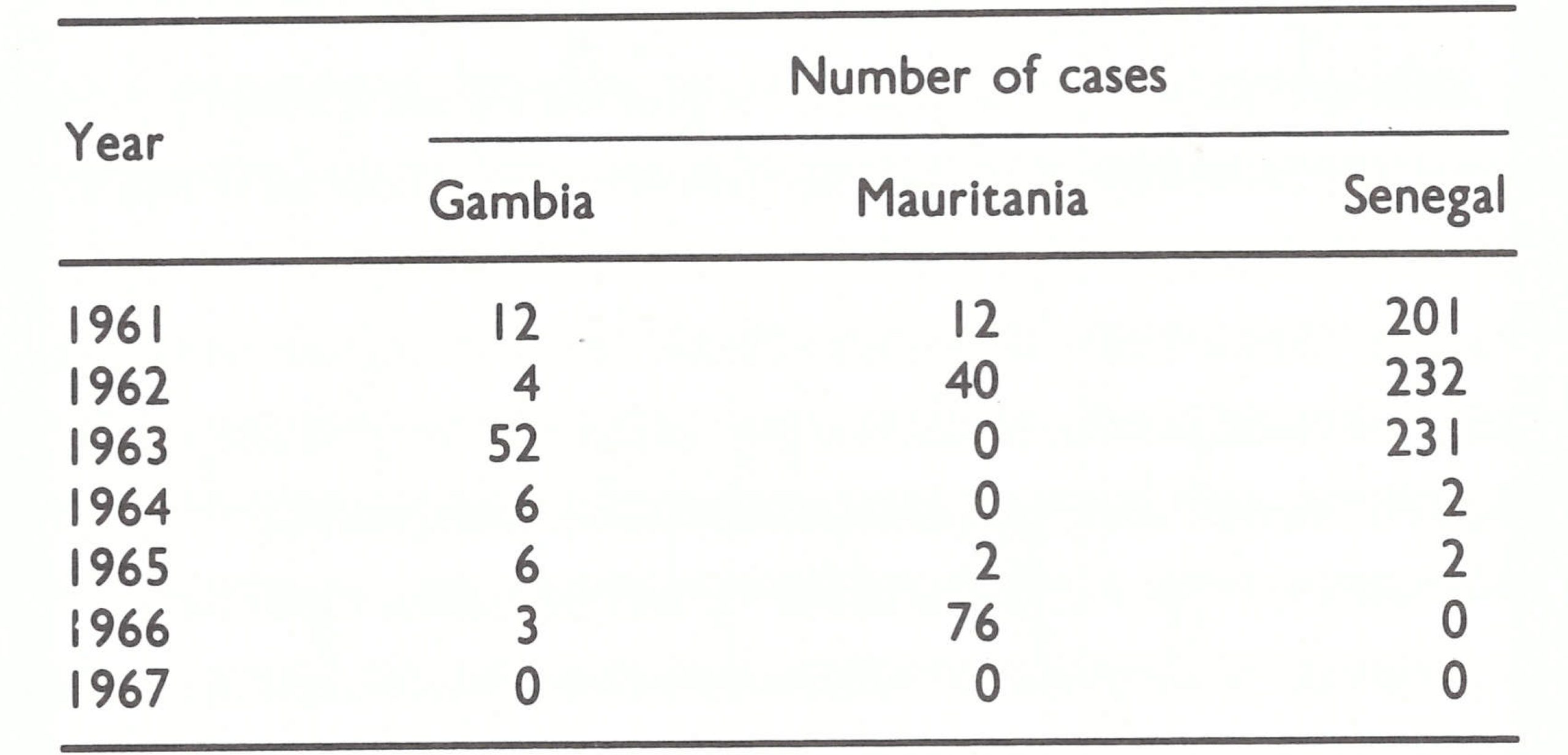
With the provision of assistance from the USA, it was decided to reconstitute the endemic diseases control service and to add smallpox and measles vaccination to its tasks. For ease of supervision it was decided that the teams would work in two separate groups, progressing from one region to the next, rather than assigning one team to each of 6 regions. However, in 1967, following the outbreak of hostilities between Egypt and Israel, Mauritania severed diplomatic relations with the USA. The United States adviser left the country and field activities ceased after only one week, not to be resumed until 1969.
In March 1968, Dr Mayer, the WHO intercountry smallpox adviser for western Africa, visited Mauritania and, with government officials, developed a plan of operations which provided for the assignment of a WHO medical officer and an operations officer, as well as a vehicle, some items of equipment and funds to cover local costs. The USA agreed to provide vaccines and other supplies and equipment, using OCCGE as an intermediary. The arrangement was similar to that which was devised to support the programme in the Congo.
At government insistence, two basic changes were made in the original plan: BCG vaccine (provided by UNICEF) would also be administered, and the teams would work simultaneously in 6 rather than 2 regions. In a country of 1.2 million square kilometres with few, poorly maintained roads, the dispersal of teams created difficulties in communication as well as in supervision and supply. Air transport was of little help since scheduled weekly flights served only a few of the larger towns and were frequently cancelled owing to the breakdown of equipment and to sandstorms.
Dr Mayer moved from Liberia to Mauritania in May 1968 and shortly thereafter conducted a scar survey among village children in the north of the country. Vaccinial immunity was found to be poor: among the children up to 14 years old only 45% had vaccination scars and these were almost all in the 5-14-year-olds. After 7 months of preparation, pilot field activities were resumed in January 1969, and full operations commenced in April. The programme progressed slowly, owing to difficulties in supervision and supply and to mechanical problems with vehicles. In 1969, 426 000 smallpox vaccinations were given and about one-fourth this number of measles and BCG vaccinations. In 1970, the number of vaccinations decreased by half and remained at about this level until June 1976, when the programme came to an end. However, no cases of smallpox were detected after 1966.
Although the need for smallpox vaccination in the 3 countries was questionable, since all of them had remained free of smallpox after 1966, the campaigns also provided measles vaccination and the vaccinators, in their systematic travels through the countries, were able to ensure that no foci of smallpox had been missed.
Factors in the Success of the Programme in the Gambia
In a detailed paper (unpublished), the Gambian field supervisor, Mr Kebba A. M. Sanneh, enumerated the factors which he considered to be of importance in the success of the programme.
Training: The field supervisor was trained first and actively participated in training the teams, all of whose members (vaccinators, recorders and drivers) were trained together. This created a special team spirit. Included in the training were 5 stand-by vaccinators who could replace any who became ill. After several days of classroom training, a 3-day field exercise was conducted in a large village to work out practical problems.
Publicity and scheduling: Before the programme began, it was given wide publicity through the local press and radio, and through letters to all medical and health personnel, as well as to Divisional Commissioners, and through them to district chiefs. In each district, the field supervisor met each seyfo (chief) to discuss the programme and to obtain a list of all villages and hamlets. The seyfo was asked to inform each alkalo (village head) of the programme and assign a "badge messenger" (a type of policeman) to work with the teams. One day before the teams vaccinated in a village (the population of as many as 20 villages were vaccinated each day), a team member met the alkalo and requested him to ask each family head to bring his family to the vaccination assembly point .The field supervisor was given wide latitude in planning the programme, but once a village had been informed that the teams would be present on the following day, every effort was made to reach it even if this meant working for 12 hours or more.
Support of teams: Team morale was enhanced by support given to them by headquarters staff and other government personnel. If transport was sent on a Sunday to obtain vaccine and petrol, these would be supplied, although Sunday was not a normal working day. In addition, teams were paid promptly whenever they returned to the capital. They were given priority at ferries by Marine Department personnel, and priority in vehicle repair by the Public Works Department. The CDC advisers, Dr Thomas Drake and Mr Robert Helmholz, gave help wherever this was required, sharing with the teams the hardships of field living conditions.
Local customs: Public support was actively sought but no compulsion was used and no attempt was made, at any time, to foreshorten the traditional greetings required in the Gambia before any matter could be taken up for discussion. Where teams encountered the initiation ceremonies for circumcision, which necessitated the isolation of the boys and girls concerned from others in the village, the boys were vaccinated "in the bush", and the girls were vaccinated privately in a compound.
With good support from local government and villagers alike, the morale and enthusiasm of the teams remained high, permitting a programme scheduled to last 260 working days to be completed in 167 days, with an independently assessed rate of coverage of more than 90%.
The OCEAC Countries : Cameroon, Central African Republic, Chad, the Congo and Gabon
Of the last group of countries to be dealt with in this chapter, all were members of OCEAC, then directed by Medecin-Colonel Labusquiere. The 5 countries (population in 1967, 13.7 million) comprised an area of almost 3 million square kilometres, which, until 1960, had been known as French Equatorial Africa. In the provision of health services, each country relied primarily on the well-established multi-purpose mobile teams of the endemic diseases control service, directed by French medical advisers who were usually military officers. The programmes in these countries all followed the same pattern, which had been agreed on in the meetings of OCEAC.
The method of operation has been described by Dr J . M. Roux, the Chief Medical Officer of Chad (Roux, 1970). A typical team consisted of 12 male nurses, 2 drivers with vehicles and 2 labourers. They administered smallpox, BCG and yellow fever vaccines; examined each person for leprosy and trypanosomiasis as well as other common endemic diseases; conducted simple routine tests on specimens of blood, faeces and urine; and prescribed appropriate treatment. For every individual examined, a special certificate documenting each procedure was prepared and retained by the person concerned. Two or three years were required for the teams to visit all parts of the country.
A freeze-dried smallpox vaccine of good quality, produced in France, began to be used in the early 1960s, and soon thereafter the number of reported cases of smallpox declined sharply, only 2 cases being recorded in the 5 countries in 1966 (Table 17.22).
Table 17.22: OCEAC countries: number of reported cases of smallpox, 1961-1969
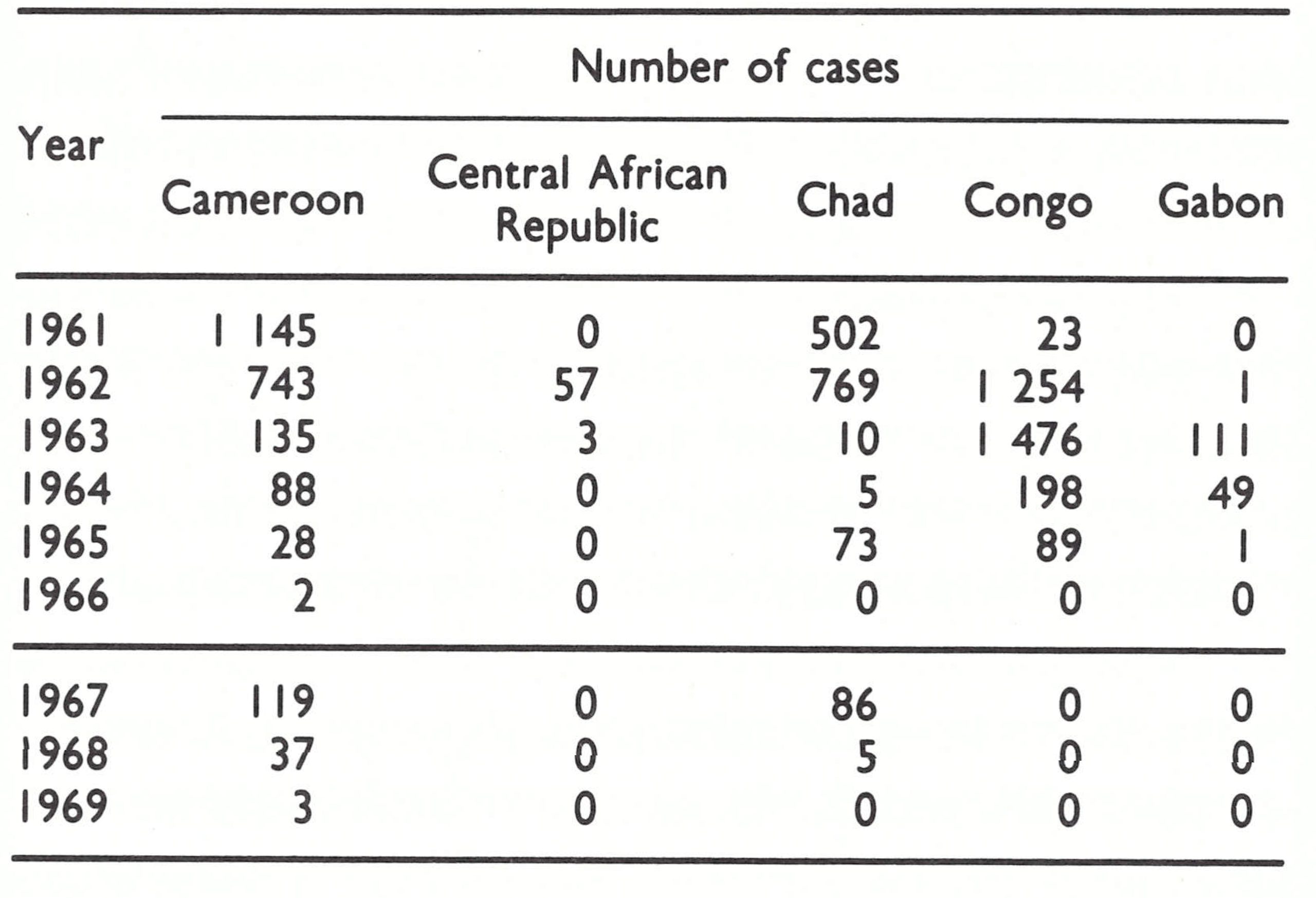
In the initial planning for the regional programme, CDC staff had not been fully aware of the scope and extent of activities already being carried out in these countries, and had envisaged the need to create special teams for measles and smallpox vaccination such as had been done during the earlier AID supported measles vaccination campaigns. However, OCEAC and government officials decided to incorporate the new vaccination activities into the work of the multi-purpose mobile teams, and to utilize the vehicles and equipment to strengthen existing efforts. Although this was advantageous to the execution of the vaccination campaign, the prescribed operations provided for neither concurrent assessment of the work by sample surveys nor a surveillance team to investigate suspected cases of smallpox.
OCEAC officials decided that the provision of separate assessment teams would be too costly and that it was basically unnecessary, since assessment in the OCEAC countries was conventionally done by the vaccination teams, who compared the numbers vaccinated with the estimated population in the area served. In most countries, such assessments proved misleading, partly because of inaccurate census data, but the OCEAC programmes were generally well conducted, and independent assessments, when performed, usually revealed that at least 80% and often more than 90% of the population had vaccination scars. By late 1969 and early 1970, the total numbers of smallpox vaccinations administered in each country during the course of the regional programme were almost equivalent to or exceeded the estimated population.
The investigation of suspected cases was generally undertaken by the CDC advisers, with assistance from local officials. After 1966, all smallpox cases in the OCEAC countries were discovered in Cameroon and Chad, in areas bordering on Nigeria. The outbreaks in Chad were traced to importations from Nigeria, as were most of those in Cameroon.
In Cameroon, during 1967-1969, 21 outbreaks, with 159 cases, were detected among tribal peoples who lived in widely scattered settlements in the rugged Mandara mountains adjacent to Nigeria. The villagers frequently crossed into Nigeria and some, in fact, maintained houses in both countries in order to escape taxes. Many villagers resisted vaccination, and because of the difficult terrain, the multi-purpose teams had not vaccinated extensively throughout the region. When surveys showed that 40% of the inhabitants had never been vaccinated, special smallpox vaccination campaigns were conducted in 1967 throughout the area, primarily in the crowded market-places. By March 1968, the last of the large outbreaks had been contained (Delas, 1970). Over the next year, however, 9 additional outbreaks of 1-7 cases occurred among visitors to Nigeria, then still heavily endemic and in which neither vaccination nor surveillance had yet begun.
The outbreaks in Chad occurred among villagers living on thousands of floating islands on Lake Chad, a shallow lake some 250 kilometres long and 25-100 kilometres wide. The islands, inhabited by fishermen, consisted of matted networks of papyrus reeds and other weeds, which often drifted for miles over the surface of the lake. Cases were reported from the area by a missionary physician in June 1967—the first cases known to have occurred in the lake area for more than 2 years . To investigate the outbreak, Dr Bernard Lourie, the CDC adviser, chartered an aeroplane with pontoons, and using a medical service boat and 4-wheeldrive vehicles, he and Chadian staff eventually identified more than 100 cases, not all of which were officially reported. The first had occurred in April among fishermen returning from Nigeria. Smallpox then spread from one small village to another in an area in which only 20-30% of the population bore the scars of vaccination. A special vaccination campaign was conducted in markets and villages throughout the area. The floating islands presented a special problem, because when pressure was exerted on the pedal of the jet injectors, they tended to sink through the surface. The difficulty was solved by laying mats on the island. In all, some 80 000 people were vaccinated in an area thought to have a population of about 150 000. Transmission was interrupted within a matter of weeks, although importations resulted in 5 further cases in 1968.
Throughout the OCEAC countries, roads were few, the distances were great and communications were limited. Secessionist groups, who were active throughout the central and northern parts of Chad, compounded the problems there and taxed the skills of the able director of the mobile disease control service, Dr Pierre Ziegler. Rebel groups, in fact, ambushed a team, killing a labourer, wounding a driver and setting fire to one of the vehicles. Efforts to contact the secessionists to ensure safe passage proved futile, since the different groups acted independently and assurances provided by one leader did not obligate others. Accordingly, vaccination in these areas had to be restricted to the major towns and cities which had military garrisons. Neither surveillance nor vaccination was possible in rural areas of the north, but the population was sparse there, and smallpox transmission did not persist as it did under similar conditions in the Ethiopian Ogaden in 1975-1976.
Plate 17.17. A health worker in Gabon repairs a jet injector. jet injectors made it possible to vaccinate large numbers of people very quickly, but they frequently malfunctioned and their daily maintenance was essential.
CONCLUSIONS
The elimination of smallpox in 1970—little more than 3 years after the inception of the Intensified Smallpox Eradication Programme—from the vast region of western and central Africa provided enormous encouragement to the remaining endemic countries. The fact that many countries of the region were among the world’s poorest, with the least developed infrastructures of health, transport and communication, increased confidence that global eradication could eventually be accomplished. The valuable early insights into the epidemiology of smallpox and the methods for its control were no less important. Subsequently, the experience acquired by both national and CDC staff was to prove invaluable when many of them served with programmes in other parts of the world.
The regional programme was also important in that the USA provided sufficient support to make eradication feasible in this vast region; WHO did not then have resources of this magnitude available for programmes in other endemic areas. The fact that CDC staff assumed full responsibility for technical assistance permitted WHO Headquarters staff to direct their efforts and attention elsewhere. Indeed, in view of the formidable administrative problems that WHO encountered in implementing smallpox eradication programmes in other countries of Africa, it is problematic whether eradication in Africa could have been achieved without this support. At the same time, WHO’s own modest but vital contribution to many of the countries by meeting the “local costs” of items such as petrol and vehicle maintenance and repair must be acknowledged.
This programme is identified with the first effort to implement, as national policy, a strategy which accorded priority to the discovery of outbreaks and their containment, even if these activities meant some compromise in the pace of execution of the mass vaccination campaign. An important change of emphasis in the global strategy took place as a result, and, in supporting this change, WHO staff frequently cited the successful experience of the regional programme. In retrospect, however, when the relative contributions made by mass vaccination and surveillance-containment (“eradication-escalation”) are weighed, the importance of surveillance-containment to the western and central Africa programme itself is less certain. When such measures were actually implemented late in 1968, the mass vaccination campaign had already reached some 60 million persons, more than half the population of the region, and a much higher proportion of those in the known endemic areas, to which the campaign had given priority. Endemic smallpox then remained in only a few of the countries, and where surveillance teams actively sought to discover and to contain outbreaks—as in Dahomey, Guinea, Sierra Leone and Togo—smallpox transmission had practically ceased, the remaining outbreaks being small and in isolated rural areas. The strategy was not employed in northern Nigeria, then the principal focus of smallpox. There, programme staff undertook to contain outbreaks only in areas in which the mass vaccination campaign had been completed. Thus although the rapid demise of smallpox in western and central Africa was impressive, and the success of the programme attributed to the new strategy, the well-executed mass vaccination campaign using freeze-dried vaccine probably played the more decisive role.
In this region, as well as in most of Africa south of the Sahara, the interruption of smallpox transmission proved to be more straightforward and less difficult than in Indonesia and the Indian subcontinent. In contrast to the Asian countries, the population density in Africa was lower, population movement was less, vaccination was usually more readily accepted, and many villagers, by tradition, isolated smallpox patients. When the comparatively simple surveillance-containment methods used in Africa were employed in Asia, the results proved disappointing. In Bangladesh, India and Pakistan, in particular, whose populations had generally higher levels of vaccinial immunity than those of African countries, surveillance and containment measures failed to make a significant impact on the disease until the methods were substantially modified and strengthened.
As had been hoped, the programme in western and central Africa served to strengthen the foundation for disease reporting and preventive services in all the countries concerned, but with only 5 years of operational experience the endeavours could not be fully institutionalized. Thus, in 1976, when it became necessary to certify that eradication had been achieved, special programmes had to be organized to permit certification (see Chapter 25).
Subsequent chapters describe eradication programmes in other countries of Africa, which, with some notable exceptions, consisted largely of mass vaccination campaigns but which succeeded in eliminating smallpox with surprising rapidity.