Chapter 1:
The clinical features of smallpox

INTRODUCTION
As this book went to press, endemic smallpox had been eradicated from Europe and North America for almost half a century and from the populous countries of China and India for some 25 and 10 years respectively. The majority of people-including the majority of physicians-now living have never seen a case of this once-dreaded disease. What was it like? For the physician, what were it.s clinical features and its complica tions? What factors influenced the prog nosis? What diseases ent.ered into its differen tial diagnosis? Nowhere is there a better answer to these questions than in the book written by Ricketts and illustrated by Byles over three-quarters of a century ago (Ricketts, J 908).
Since then, however, long series of carefully studied cases of both variola major (Rao, J972) and variola minor (Marsden, 1936) have been documented, and laboratory investigation has become a powerful tool for
confirmation of the diagnosis in puzzling cases. Further, during the global smallpox eradication programme a large number of WHO epidemiologists and their national counterparts had extensive experience of smallpox as it occurred in the field in urban and rural areas and among nomads, as distinct from the hospitals from which Ricketts’s, Rao’s and Marsden’s material was drawn. However, only limited clinical studies were possible in rural situations, outside of hospitals. The most comprehensive clinical study of variola major in a non-hospital setting is a series of 539 cases seen in their houses in Pakistani Punjab in 1966-1967 (Mack et al.,1970). Where relevant, data from this study will be used to supplement the description of hospital-based cases described by Rao (t972 An attempt has been made to interpret the symptoms in the light of current understanding of the pathogenesis and immunology of orthopoxvirus infections, as outlined in Chapter 3.
The plan of the present chapter follows Ricketts in that the account of the clinical features of smallpox consists mainly of a description of the rash, based on photographs of patients, most of which were prepared during the global smallpox eradication pro gramme. Because smallpox is now extinct, we have to take the unusual step, in the clinical description of a human disease, of referring to it in the past tense; this was previously the case only)1 with diseases that apparently disappeared and could be identified only by con temporary descriptions, such as the “English sweat”, or the “sweating sickness”.
Plate 1.1. Thomas Frank Ricketts (1865-1918). Medical Superintendent of the Smallpox Hospitals and of the River Ambulance Service of the Metropolitan Asylums Board, London. His book on the clinical features of smallpox was based on the personal examination of many thousands of cases of variola major.
VARIETIES OF SMALLPOX
From the time it was first recognized as a distinct disease until about the end of the 19th century, smallpox was regarded as a uniformly severe disease, associated with a high case fatality rate, in every part of the world. Mild cases and even mild outbreaks of smallpox were occasionally mentioned in the old literature, but they were the exception; nowhere did endemic mild smallpox occur. Smallpox was designated by many names in various languages, but no one saw a need to distinguish different varieties of smallpox, al though the existence of different clinically (see below) was recognized from the time of Thomas Sydenham (1624-1689) in Europe and much earlier in India and China.
The situation changed when Korte (1904) described a very mild smallpox-like disease, with a case-fatality rate of 1% or less in unvaccinated persons, that had occurred in South Africa for several years and was known locally as kaffir-pox, or “amaas”, a “‘word of uncertain origin, possibly a corruption of the Dutch word masels or mazelen (measles) (Dix on, 1962). Subsequently, Chapin (1913, 1926) recognized that a similar mild disease had been occurring in North America since about 1896, and had subsequently been exported from there to South America, Europe, and Australia. There was controversy about the relationship of this disease to smallpox until the mid-1950s (Jong, J 956), but virological studies (see Chapter 2) showed that there was no doubt that “amaas” and “alastrim” (from the Portuguese alastra, something which “burns like tinder, scatters, spreads from place to place”), as it was called in South America was indeed mild varieties of smallpox. Al though many other names were used, this clinic-epidemiological variety of smallpox has come to be called “variola minor”, a designation that led to the use of ·the term “variola major” for “classical” smallpox.
Recent studies of viral strains recovered from outbreaks of variola minor in various countries have shown that they fall into two groups distinguishable by biological proper ties, one consisting of strains derived from outbreaks in South America or traceable to an American source (which we shall call “alas trim” virus) and the other comprising most strains from Africa (see Chapter 2).
During the first half of the 20th century all outbreaks of smallpox in Asia and most of those in Africa were due to variola major (with case-fatality rates of 20% or more in the unvaccinated). Variola minor (with case fatality rates of 1% or less) was endemic in some countries of Europe and of North and South America and, together with variola major, in many parts of Africa. With the more careful study that began after global eradication had been proclaimed as a goal of WHO in 1959, it was recognized that some outbreaks of smallpox in western, central and eastern Africa and in Indonesia were associated with a lower case-fatality rate than classical variola major, in the range of 5-15% instead of over 20%, Some of these lower figures resulted from aggregating all reported cases in places where both varieties of smallpox were endemic (see Chapter 8), but there were other places where this was not the explanation. The clinical picture of smallpox with a case fatality rate of 5-15% was indistinguishable from that of variola major, both haemorrhagic and Aat types of the disease occurring with about the same frequency as in classical smallpox. Preliminary tests suggested that certain laboratory characteristics of some of the strains recovered from these outbreaks were intermediate between those of variola major and variola minor (see Chapter 4), but later studies failed to support the differentiation of a separate “intermedius” virus. In this book, all outbreaks of smallpox will be categorized as either variola major, with case-fatality rates of 5-25% and occasionally more, or variola minor, with case-fatality rates of about 1% or less.
THE CLASSIFICATION OF CLINICAL TYPES OF VARIOLA MAJOR
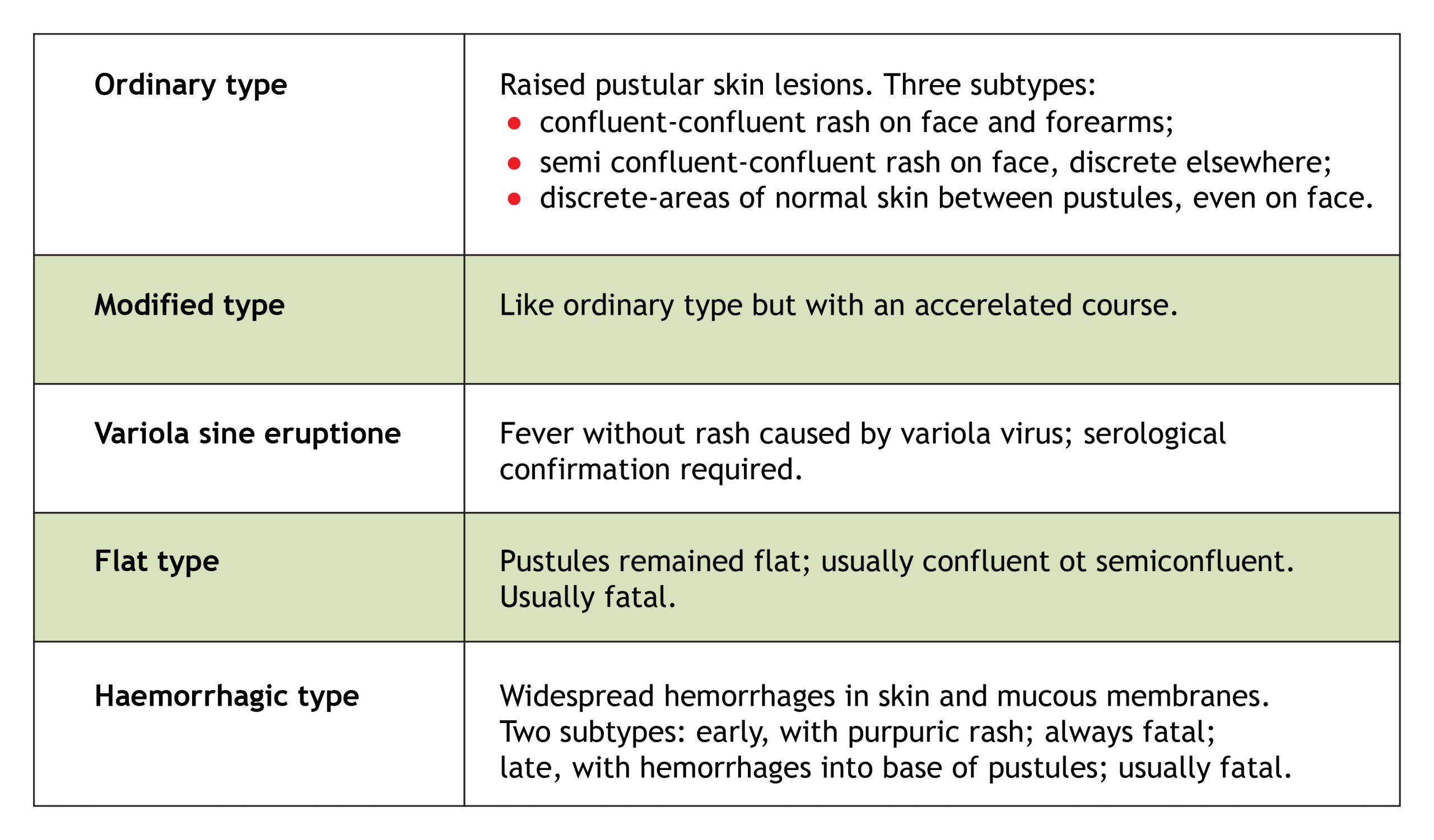
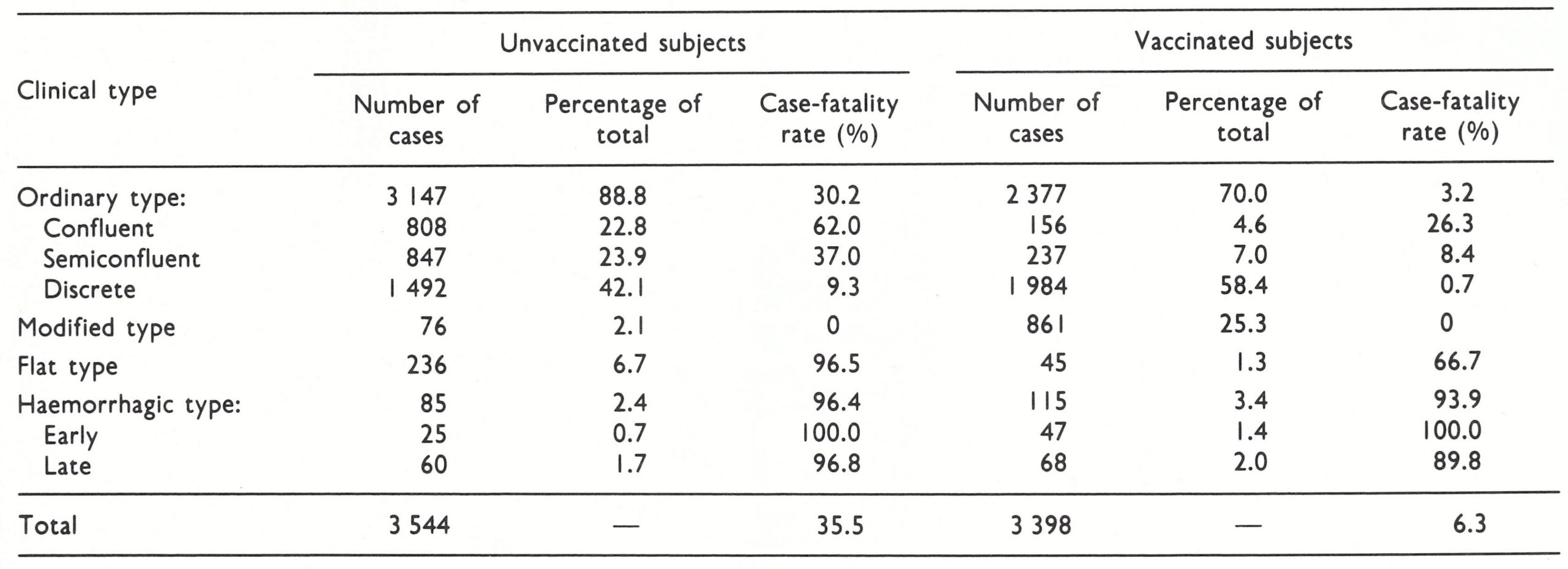
It has long been recognized that several clinical types of variola major could be distinguished which differed in prognosis, differential diagnosis and transmissibility. The old subdivision according to the density of the focal eruption was shown by Dixon (1962) and Rao (1967) to have less prognostic value than a classification based on the nature and evolution of the rash. For this reason, a WHO Scientific Group on Smallpox Eradication {1968) adopted the classification pro posed by Rao and fully described in his book on smallpox (Rao, 1972). A WHO Expert Committee on Smallpox Eradication (1972) reaffirmed its acceptance of this classification (Table 1.1), according to which the commonest clinical type (ordinary-type smallpox) is subdivided in relation to the density of the rash, since this had prognostic significance. The great majority of cases of variola major seen in hospitals among both unvaccinated and vaccinated persons—88.8% and 70% respectively in Rao’s series of 6942 cases (Table 1.2)—were ordinary-type smallpox (and other reported series confirm this); the case-fatality rates in unvaccinated cases with confluent, semiconfluent and discrete rashes were 62%, 37% and 9.3% respectively. Although its use was suggested by Rao, such a subclassification is hardly justified for modified-type or flat-type cases, but it is useful to consider early and late haemorrhagic-type cases separately since they were probably the results of different pathophysiological processes.

Plate 1.2. A. Ramachandra Rao (b. 1917). Formerly Superintendent of the Infectious Diseases Hospital, Madras, India. His book on smallpox was based on the personal study of nearly 7000 hospitalized cues of variola major. He also made important contributions to the understanding of the epidemiology of smallpox in India (see Chapter 15).
A special comment is required on the designation of cases as vaccinated by both Rao (1972) and other investigators. Until freeze dried vaccine became available and regular assessment was made of the results of vaccination, many vaccinations, especially in tropical countries, were performed with vaccine of less than the required potency (sec Chapter 11). The categorization of a subject as “vaccinated” was made on the basis of the presence of what was regarded as a vaccination scar. The presence of such a scar was, however, not certain evidence of successful vaccination. The rotary lancet, used for vaccination on the Indian subcontinent, was attended by considerable trauma, and sometimes bacterial infection alone could produce scarring. On the other hand, vaccination by the jet injector sometimes resulted in a very small scar which might be overlooked on the skin of subjects bearing many scars of traumatic origin. In spite of these short. comings, the vaccination scar provided a more easily determined and reliable index of an individual’s immune status vis-à-vis smallpox than was possible with other infectious diseases.
ORDINARY-TYPE SMALLPOX
The incubation period
The incubation period is the interval between the implantation of infectious virus and the onset of the first symptoms, which in smallpox were fever and constitutional disturbances. Determination of the length of the incubation period is discussed in detail in Chapter 4; in exceptional instances, the duration, from the time of infection until the onset of fever, was as short as 7 days or as long as 19 days, but in the great majority of cases the period extended over 10-14 days, usually 12 days.
Symptoms of the Pre-eruptive Stage
The incubation period in smallpox was a period of intense activity in terms of viral replication and spread within the body and the development of the immune response (see Chapter 3), of which there was at that time no clinical evidence. It ended when the patient became feverish and ill (Fig. 1.1). The onset of fever and malaise was sudden, the temperature usually rising to between 38.5°C and 40.5°C. Other symptoms varied in frequency (Table 1.3). Patients suffering from variola major usually complained of a split ting headache, sometimes frontal but usually generalized, and many complained of severe backache (Rao, 1972). A small proportion of children had convulsions, and some adults were delirious at this stage. Vomiting occurred in about half of all patients, and diarrhoea in about 10%. Some suffered abdominal colic, which could lead to a diagnosis of appendicitis. The patient was usually ill, with an appearance of general toxaemia. By the 2nd or 3rd day (rarely the 4th) the temperature had fallen, and the patient felt somewhat better; at this time the macular rash appeared.
Figure 1.1: Time after infection (days)
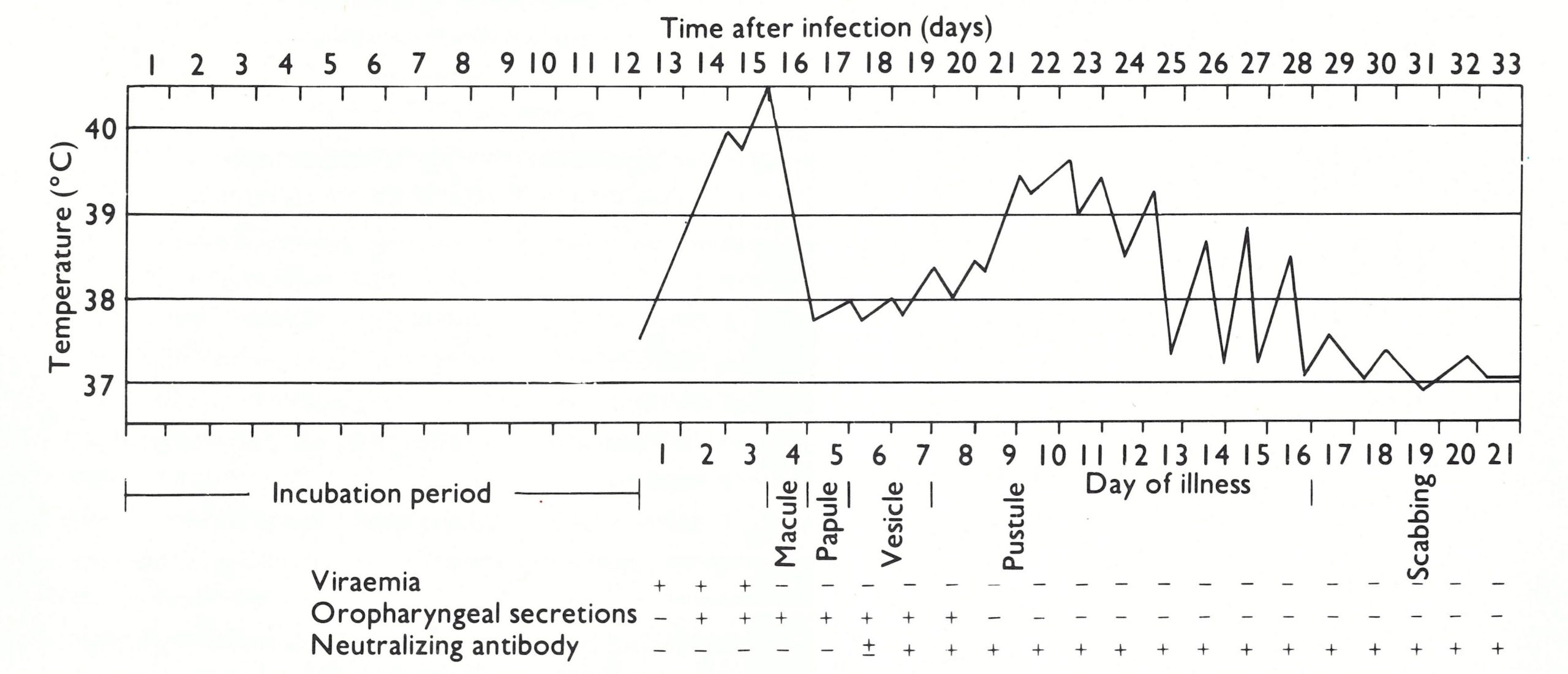
Fig. 1.1. The clinical course of moderately severe ordinary-type smallpox in an unvaccinated subject: the temperature chart, the development of rash, the presence of virus In the blood and oropharyngeal secretions and the time of appearance of neutralizing antibody in the serum. (Data from various sources.)
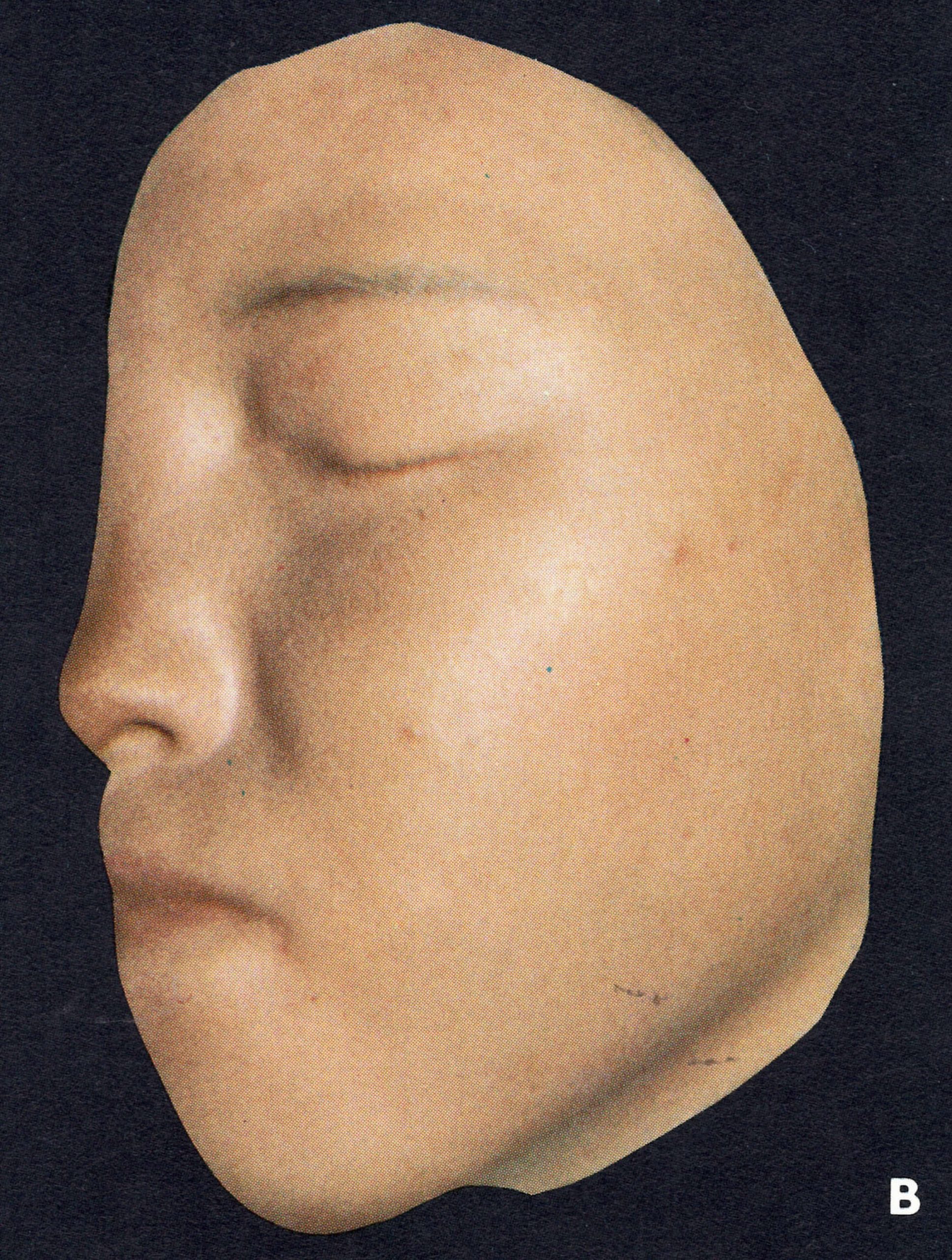
In older writings (e.g., Ricketts,1908) there was often reference to the occurrence of an erythematous rash during the pre-eruptive phase (prodromal rash), best seen in fair-skinned subjects (Plate 1.3A and B). Some authors (Dixon, 1962; Rao, 1972) have cast doubt. on its occurrence in unvaccinated subjects, but all agree that a fleeting “allergic” rash sometimes occurred in vaccinated individuals, most readily visible around the vaccination scar (see Plate 1.3), in the axillae, behind the knees and in the inguinal region. The erythematous rash common in the early stages of hemorrhagic-type smallpox had to be distinguished from the prodromal rash of ordinary-type or modified-type smallpox.
Table 1.3: frequency of symptoms (percentage of cases) In the pre-eruptive stage in variola major and variola minor

a..= data not recorded


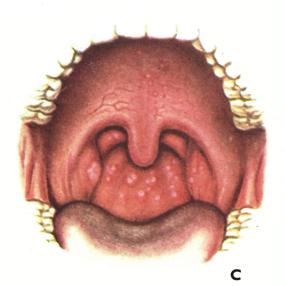
Plate 1.3. A and B: Prodromal rashes. These were best seen in fair-skinned persons (for example, Caucasians and Japanese) and were more common in those previously vaccinated. A: Erythematous prodromal rash on the upper arm, near the sites of vaccination performed 8 days earlier but sparing the skin immediately adjacent to the vaccination lesions. B: Measles-like prodromal rash on the lateral side of the trunk on the ‘4th day of illness. C: The enanthem. Lesions occurred throughout the oropharynx and in the nasal cavity, as well as on the tongue. The lesions on the palate were usually smaller than those on the posterior pharyngeal wall and tonsil. (From Uchida, 1955.)
Day 1

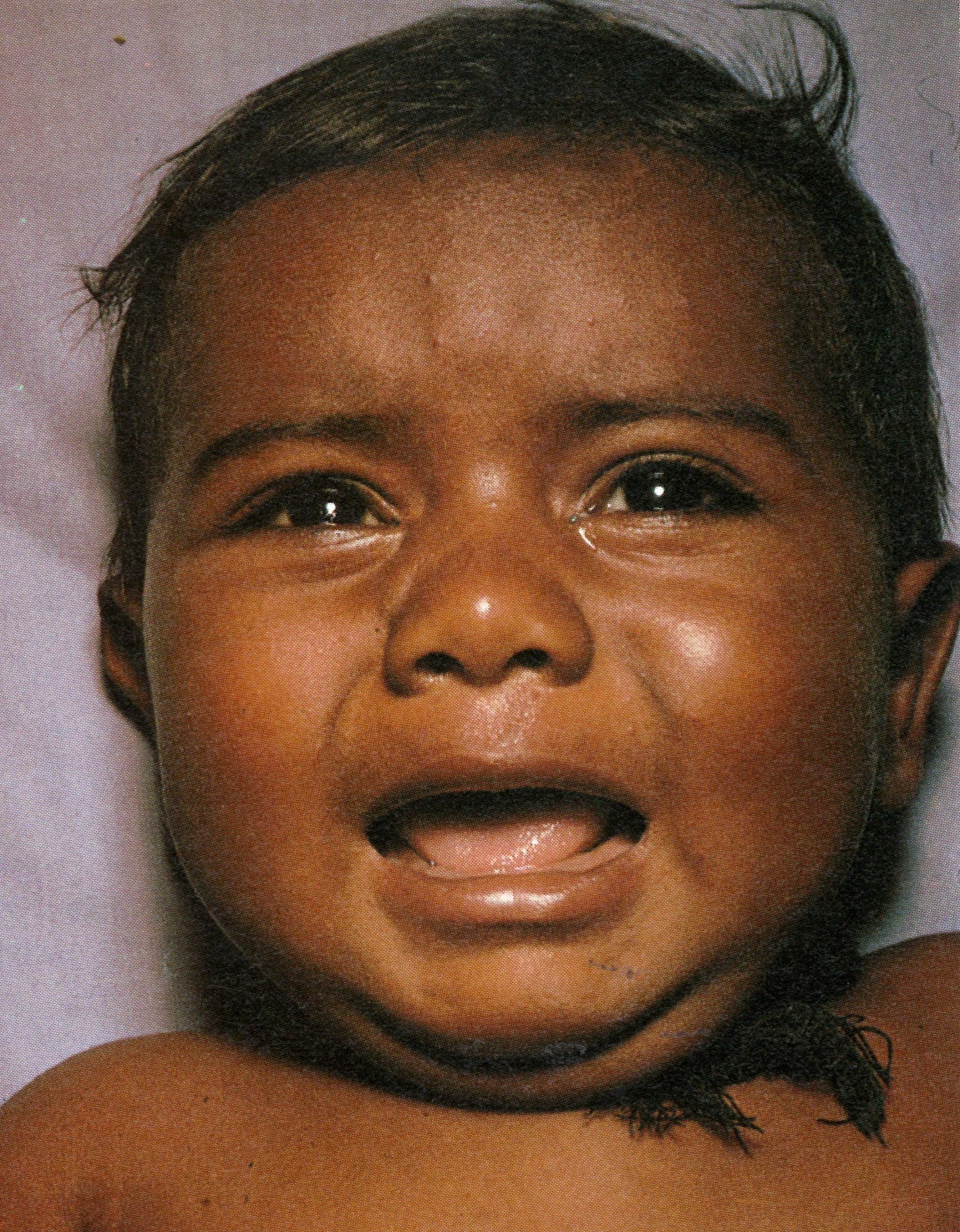
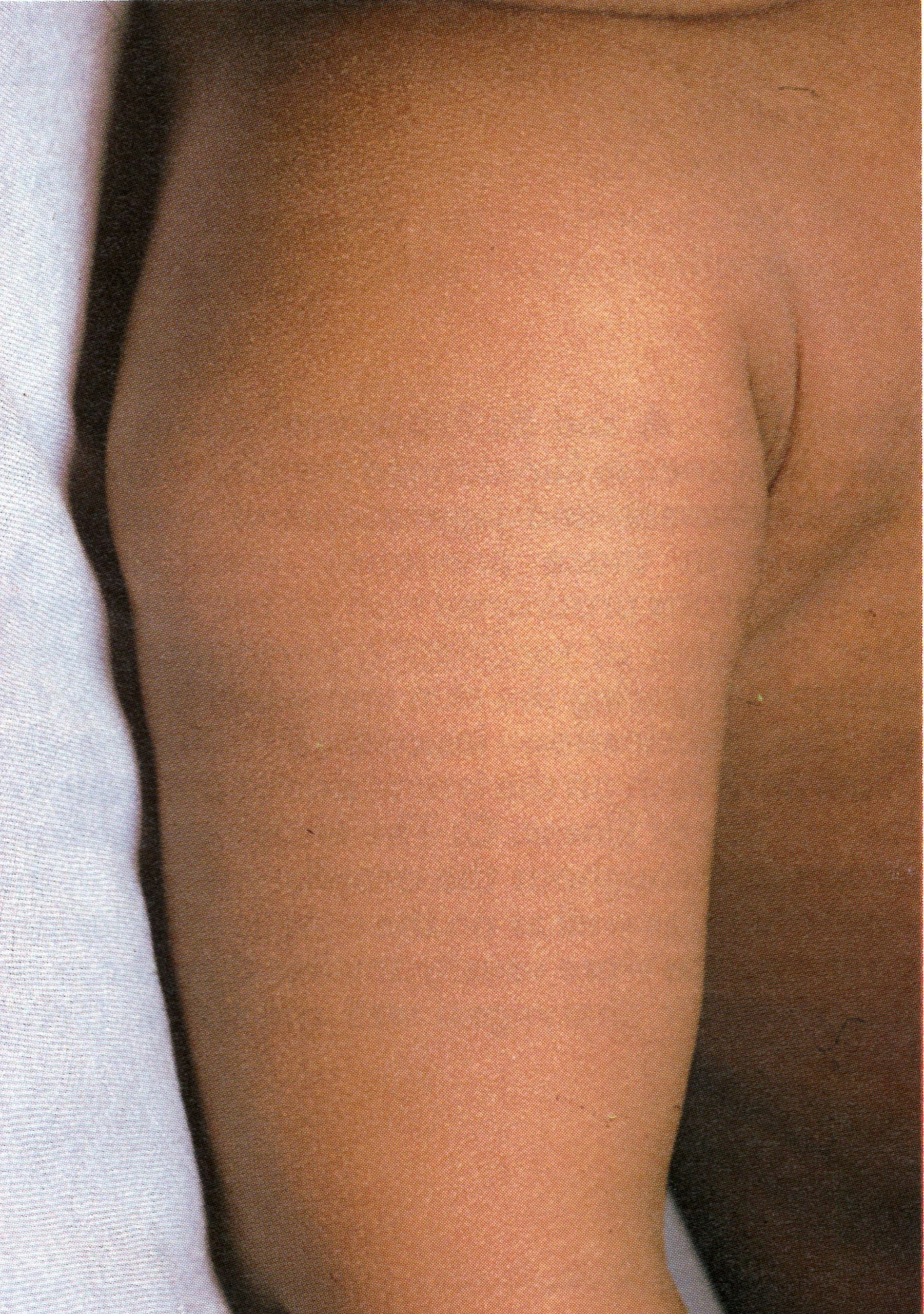
Plate 1.4. This and the next 10 colour plates illustrate the evolution and subsequent healing of the skin lesions in a 9-month-old unvaccinated Pakistani child. The rash appeared I day after the onset of fever, and the illustrations are categorized in terms of the day of rash. Each plate shows the ventral surface of the full body, the face, and the upper arm. This plate illustrates the first day of the rash. A few small papules are visible on the face and upper arm. An enanthem would usually have been present in the oropharynx at this time. but cannot be seen in this photograph (see Plate 1.3C)
Day 2

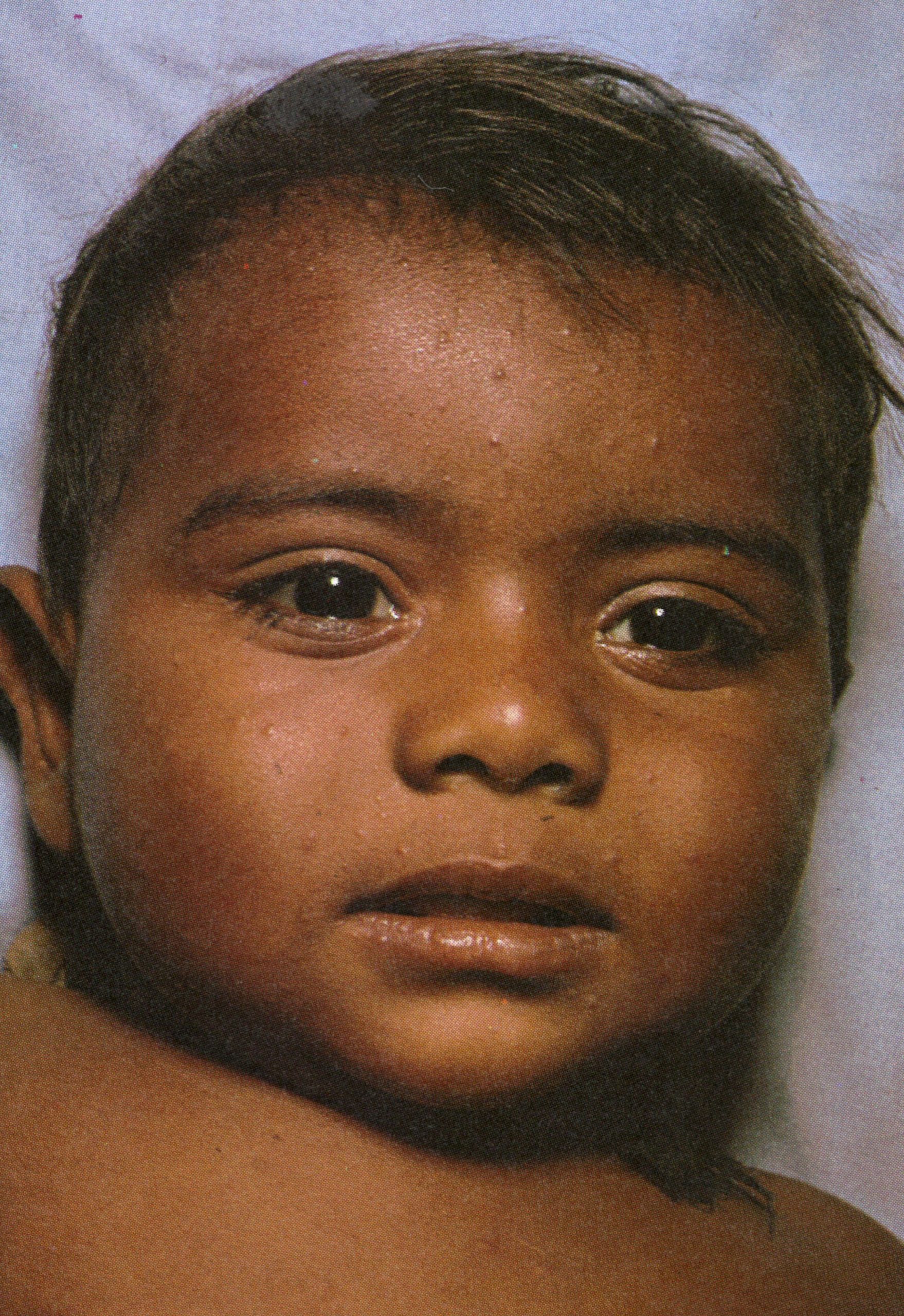

Plate 1.5. Second day of rash. More papules are present, having appeared first on the face and the upper part of the extremities.
Day 3



Plate 1.6. Third day of rash. Additional lesions continue to appear and some of the papules are becoming obviously vesicular.
Day 4

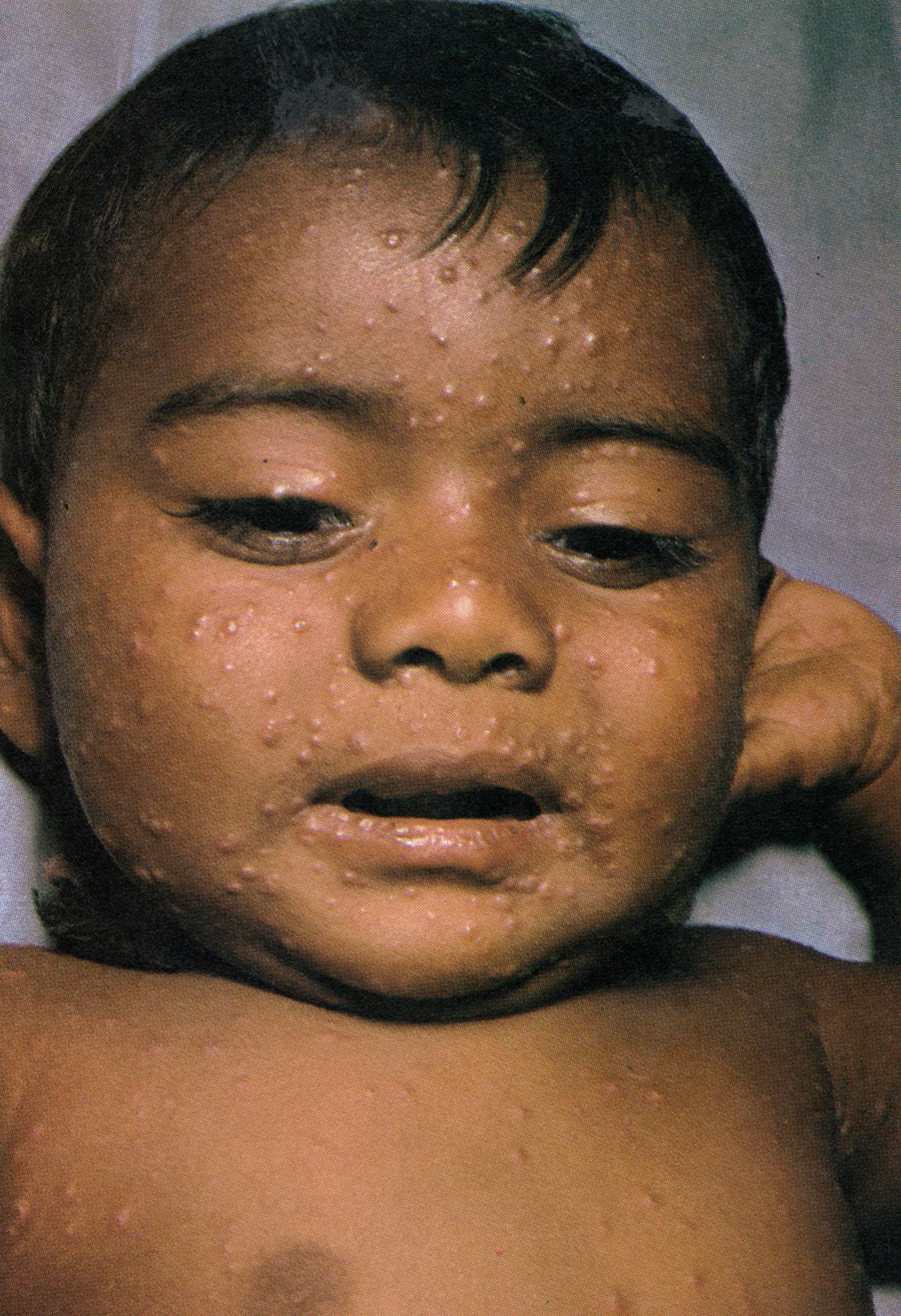

Plate 1.7. Fourth day of rash. All lesions had usually: appeared by this time. Those that appeared earliest, on the face and upper extremities, are somewhat more mature than those that appeared later on other parts of the body. but on any specific area of the body, all lesions are at approximately the same stage of development. Lesions are present on the palm of the hand.
Day 5



Plate 1.8 Fifth day of rash. Almost all the papules have now become vesicular or pustular, the truly “vesicular” stage usually being very brief. Some of the lesions on the upper arm show early umbilication.
Day 6



Plate 1.9. Sixth day of rash. All the vesicles have now become pustules that feel round and hard to touch (“shotty”). like a foreign body.
Day 7



Plate 1.10. Seventh day of rash. Many of the pustules are now umbilicated and all lesions now appear to be at the same stage of development.
Day 8



Plate 1.11. Eighth day of rash. This case is now clearly classified as discrete ordinary-type smallpox. In the confluent subtype of ordinary-type smallpox, the lesions would have been confluent on the face and forearms (see Plate 1.18); in the semiconfluent subtype, they would have been confluent on the face but not on the forearms.
Day 9
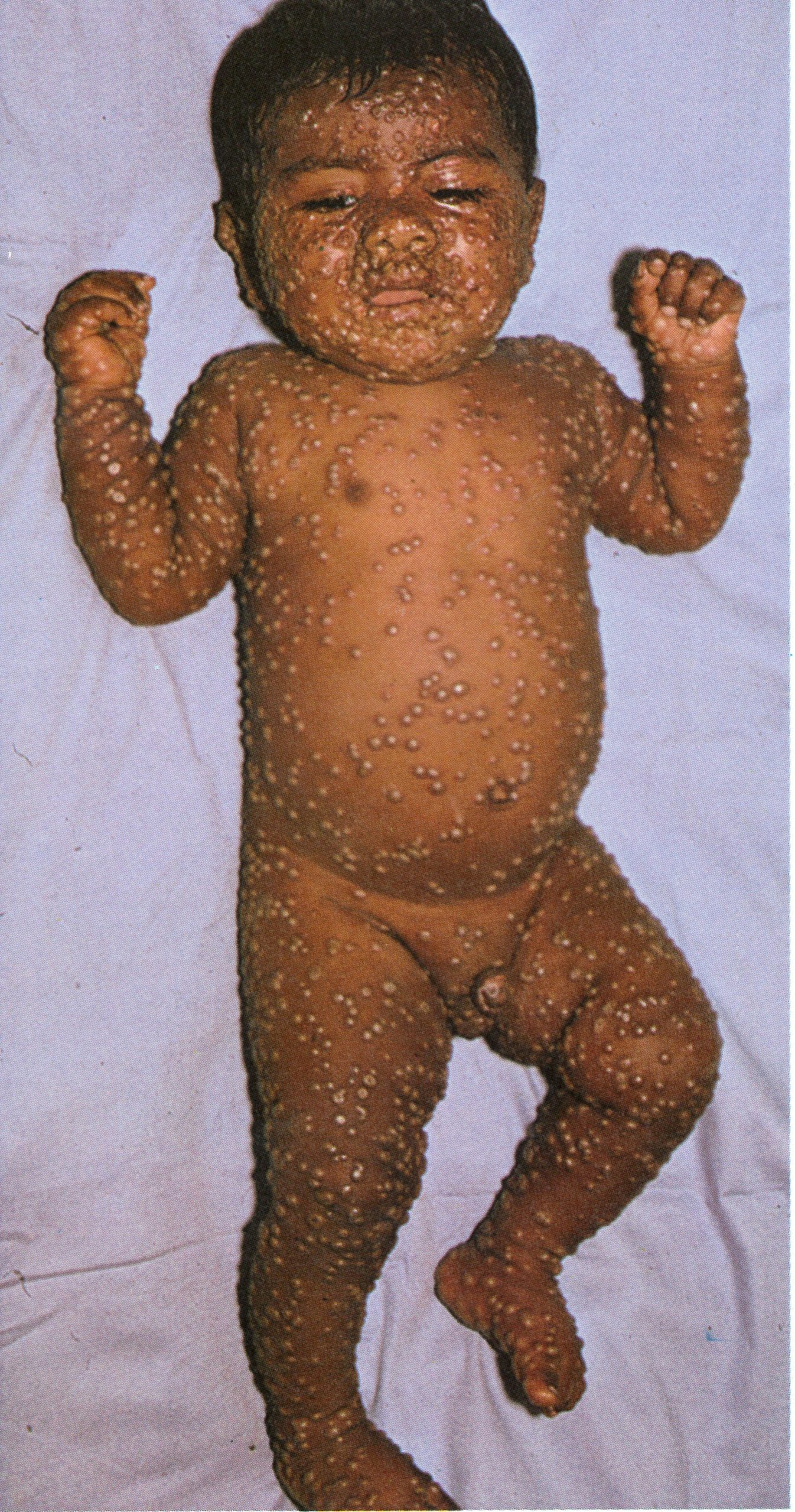


Plate 1.12. Ninth day of rash. The pustules have reached their maximum size and are becoming flattened.
Day 13



Plate 1.13. Thirteenth day of rash. The lesions are now scabbing, but the eyelids are more swollen than at earlier times. There is no evidence of secondary bacterial infection of the skin lesions.
Day 20



Plate 1.14. Twentieth day of rash. The scabs have separated except on the palms of the hands and the soles of the feet, leaving depigmented areas.
The Eruptive Stage
Chapter 3 concludes with an integrated picture of the pathogenesis of smallpox, which was a generalized viral infection with no recognizable primary lesion but with a viraemia whose onset was manifested clinically by the pre-eruptive fever, followed a few days later by the development of a focal eruption on the mucous membranes and skin. Following the example of Ricketts (1908), our description of the clinical features of smallpox is in large part based on illustrations, using a series of colour photographs taken for WHO during the smallpox eradication programme in Pakistan. The subject was a 9-month-old unvaccinated male infant in whom the onset of fever was recorded 1 day before the rash first appeared. He suffered from the commonest form of smallpox—discrete ordinary-type—and recovered without complications. Daily photographs were taken, until recovery was complete, of the entire subject and of face, trunk, arms and legs. Only a limited selection of these can be reproduced here, but they serve to illustrate the nature, evolution and distribution of the rash of smallpox. The temporal succession will be described in terms of the day of rash.
Order of appearance of the focal lesions
The lesions on the mucous membranes (the enanthem—Plate 1.3C) were the first to appear, and they were visible on the tongue and palate, as minute red spots, about 24 hours before the appearance of rash on the skin. Lesions also occurred at this time lower down in the respiratory tract, and some patients, who complained of sore throats during this stage, had an enanthem on the pharynx.
The rash usually appeared between 2 and 4 days after the onset of fever as a few small macules (“herald spots”) on the face, especially on the forehead (Plate 1.4). In a few cases the rash was first seen on the forearms or some other part of the body. Lesions then appeared on the proximal portions of the extremities, on the trunk, and lastly on the distal portions of the extremities. However, the lesions appeared in such quick succession that it was difficult to follow the timing of their occurrence on the different parts of the body, and only rarely did a patient notice this order of appearance and give such a history. Usually, the rash had appeared on all parts of the body within 24 hours. Additional lesions often appeared during the next one or two days (compare Plates 1.4, 1.5 and 1.6) but normally no fresh lesions appeared after that (Plate 1.7).
In a particular area of the body surface all the lesions were at about the same stage of evolution, although of different sizes, because the rash developed essentially as a single “crop”. However, up to the 3rd day, because of the order of their appearance, there were sometimes papules on the face and macules on the legs and similarly, after scabbing had started, lesions might be scabbing on the face and still be pustular on the legs. By the 11th day many of the scabs had come off the face, the temperature had fallen and the patient felt much better. Separation of the scabs proceeded in the same order as the macules and vesicles had appeared, from the face and scalp to the trunk, arms, hands, legs and feet. By the 17th day, only the lesions in the thick-skinned palms of the hands and soles of the feet remained (Plate 1.16).
Evolution and distribution of the enanthem
The enanthem evolved rapidly, because of the absence of a horny layer in the stratified epithelium of the pharynx. The minute macules became papular and vesicular and then broke down before the 3rd day (Plate 1.3C), liberating large quantities of virus into the saliva. By the 10th day they had almost healed.
The visible parts of the oropharynx most likely to show lesions were the hard palate, the tip and edges of the tongue and the pillars of the fauces. Different patients showed remarkable variations in the extent of the enanthem; in cases of equal severity the lesions were sometimes few or absent, or the mouth and throat might have been covered by a confluent enanthem that extended to the larynx and trachea. Although not as spectacular as the rash, the pharyngeal lesions were of great importance epidemiologically, as they constituted the major source from which virus was transmitted to other persons (see Chapter 4).
Evolution of the skin lesions
By the 2nd day of rash the macules were raised and usually described as “papules”. Reference to the histopathology indicates that this term was really a misnomer; they were raised above the skin surface because of the effusion of fluid into the tissue spaces and were in fact early vesicles (Plates 1.5 and 1.6). By the 4th or 5th day they were obviously vesicular, containing at first an opalescent fluid, which became opaque and turbid in another 24-48 hours (Plates 1.7-1.9).
By the 7th day all the skin lesions were pustules (Plate 1.10) and between then and the 10th day they matured and reached their maximum size (Plates 1.11 and 1.12). By about the 11th day resolution started, and the lesions flattened (Plate 1.13). The fluid was slowly absorbed, and by the end of the 2nd week the central portion hardened and finally a scab or crust formed, which later separated, leaving a depigmented area (Plate 1.14).
The palms of the hands and the soles of the feet, because of the very thick stratum corneum, were characterized by the persistence of lesions long after these had scabbed elsewhere. On the soles of the feet especially they had a very characteristic appearance (Plate 1.16). The thick cuticle lay over them and they did not protrude from its level surface, through which the disc-like scabs could be clearly seen. These lesions were called “seeds” and were often artificially removed with a needle in attempts to hasten discharge from the hospital, where patients were usually held until the last scab had separated.
The evolution of the rash can best be appreciated by scanning the series of colour plates provided, which show the lesions daily from the 1st until the 9th day (Plates 1.4- 1.12), and then on the 13th (Plate 1.13) and 20th days (Plate 1.14).
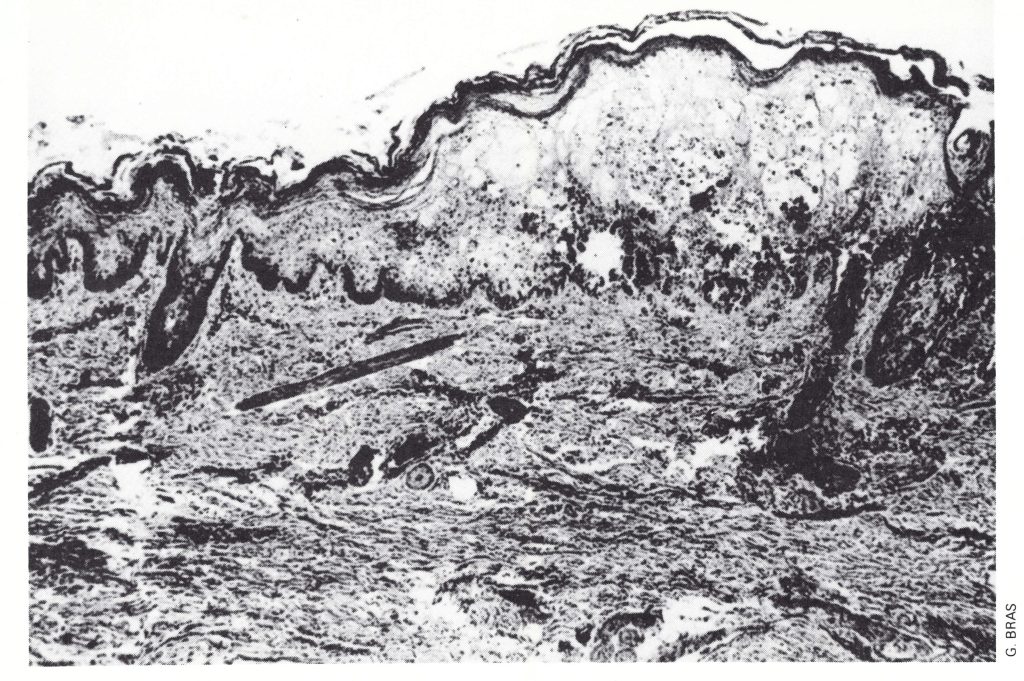
Plate 1.15. Section of a skin lesion on the 6th day of rash. Ballooning degeneration of the cells of the lower part of the epidermis has produced a loculated vesicle which is becoming pustular. The keratohyalin and horny layers form the roof of the vesicle; at the base the dermis is undamaged-there will be no scarring after healing. The central depression associated with the hair follicle on the extreme right would produce loculation of the lesion. (Haematoxylin and eosin, x 50.)
Histopathology of skin Lessions
In order properly to appreciate the clinical features of the skin lesions it is necessary to consider their histopathology. This is described in detail in Chapter 3, but it is convenient to summarize the main features of the lesions here. Plate 1.15 represents a section of part of a skin lesion in which vesiculation was beginning. The lesion occupied the whole depth of the epidermis, the deeper layers of which provided the Aoor and the cuticle (stratum spinosum, keratohyalin layer and horny layer) the roof. At the centre the Aoor was thin and as the lesion grew the deeper layer of basaJ cells Jyscd and the dermis then formed the base of the vesicle. But ordinarily (except in the face, where the numerous sebaceous glands complicated the picture) the lesion was contained within the epidermis. As infected cells became necrotic and Auid accumulated, the tissue split, the columns of epidermal cells being forced apart irregularly, so that the fissures were usually perpendicular to the surface and the vesicle consisted of several separate compartments or loculcs. As cellular necrosis and polymorphonuclear cell infiltration proceeded the Auid became turbid and the lesions pustular, but their turbidity was due to the extensive tissue destruction by the virus and a leukocytic reaction to this; the pus was not associated with bacterial infection.
Characteristics of the individual lesions
Variolous skin lesions, which usually had only a barely perceptible erythematous areola around them, were traditionally held to have three distinctive characteristics: loculation of the cavity of the vesicle, its umbilication, and the solidity and hardness of the lesion.
Loculation. The reasons for loculation are clear from a consideration of the histopathology (Plate 1.15); it used to be determined in cases of smallpox by piercing the vesicle and observing that the fluid contents could not be completely emptied through the wound. However, this was a rather inefficient clinical test, in that it was readily demonstrable in cases in which there was little doubt about the diagnosis but equivocal in cases in which doubt might arise because the vesicles were small or soft. It was rarely used for differential diagnosis by workers engaged in the global smallpox eradication campaign.
The “feel” of the lesion. The skin lesions of smallpox were usually described as “shotty”. Although as papules they projected little above the surface, they could be rolled between the thumb and forefinger and felt like hard round foreign bodies embedded in the epidermis.
Umbilication. This term refers to the central depression, of varying size, that was often seen in the distended vesicle. It is well illustrated in Plate 1.8. Umbilication often persisted into the pustular stage, but as the lesion progressed the fibrinous threads within it were destroyed and its surface usually became flattened because of absorption of fluid (Plates 1.11 and 1.12).
Distribution of the rash
The rash of smallpox had a characteristic centrifugal” distribution pattern. This is apparent in the series of full-body photographs of the Pakistani infant (e.g., Plate 1.11), but is better shown in Plate 1.17. The rash was most dense on the face; more dense on the extremities than on the trunk; and, on the extremities. it was more dense on the distal parts than on the proximal, on the extensor than on the flexor surfaces and on the convexities than on the concavities. The apex of the axilla was relatively free of lesions compared with the folds; this was known as Ricketts’ sign. The palms of the hands and the soles of the feet were involved in a majority of cases (Plate 1.16).
On the face, the rash was more profuse on the upper than on the lower half, but in a small proportion of cases it was more uniformly distributed. On the trunk, it was usually denser on the back than on the front, and, on the front, it was more dense on the chest than on the abdomen. On the abdomen, the upper half usually exhibited a more profuse rash than the lower half.
Ricketts (1908) described at length the fine details of the distribution of the rash, which he regarded as a feature of great value in differential diagnosis. Such minute consideration was no longer necessary when laboratory confirmation of a tentative diagnosis became possible. Ricketts also provides several illustrations of the way in which irritation or friction could produce a local concentration of skin lesions. His suggestion that the “centrifugal” distribution of the rash was due to exposure of the face and forearms in habitually clothed persons was not supported by the universal observation of the same characteristic distribution in habitually scantily clothed patients made by workers in several countries during the global smallpox eradication programme.
Clinical Course
The appearance and evolution of the rash in ordinary-type smallpox have already been described and illustrated. In such cases, the fever, which had fallen somewhat on the 2nd or 3rd day after the onset of the disease, when the rash first appeared, usually rose again by the 7th or 8th day and continued to remain high throughout the vesicular and pustular stages, until scabs had formed over all the lesions (see Fig. 1.1).
If secondary pyogenic infection of the skin occurred, the fever usually remained elevated. Respiratory complications, which sometimes developed on about the 8th day of the disease, were either viral or bacterial in origin. In fatal cases, death occurred between the 10th and 16th days of the illness. Among survivors, scabs separated by the 22nd-27th days, but “seeds” in the palms and soles remained much longer unless artificially removed.
Grades of Severity
Grades of Severity As has been pointed out earlier, so many cases of variola major belonged to the ordinary type, covering a wide range of severity, that some subdivision that was related to prognosis was found useful, That commonly employed related to the extent of the rash, and the terms “confluent”, semiconfluent” and “discrete” were used by Rao (1972) and others. However, it is important to point out that such grades were part of a continuous spectrum; the numbers of pustules in individual cases could vary from a few to several thousand.
As has been pointed out earlier, so many cases of variola major belonged to the ordinary type, covering a wide range of severity, that some subdivision that was related to prognosis was found useful. That commonly employed related to the extent of the rash, and the terms “confluent”, “semiconfluent” and “discrete” were used by Rao (1972) and others. However, it is important to point out that such grades were part of a continuous spectrum; the numbers of pustules in individual cases could vary from a few to several thousand.
Confluent ordinary-type smallpox
This subtype encompassed cases in which the pustular skin lesions on the extensor surfaces of the extremities as well as those on the face were confluent (Plate 1.18). In such cases the temperature, which had fallen on the 4th or 5th day after the onset, rose again 2 days later and remained elevated until scabbing was complete. Sometimes the toxaemia did not abate, and the temperature did not fall even after scabs had formed over all lesions; when this occurred, the prognosis was poor. In Rao’s series the case-fatality rate of confluent ordinary-type smallpox in unvaccinated subjects was 62%.
Semiconfluent ordinary-type smallpox
This was distinguished from confluent ordinary-type smallpox by an arbitrary criterion: the rash was confluent on the face but discrete on the body, including the forearms. A secondary fever often developed during the pustular stage, but the temperature and toxaemia were less marked than in the confluent subtype and the temperature subsided as soon as the scabbing had started. In Rao’s series the case-fatality rate in unvaccinated subjects was 37%.
Discrete ordinary-type smallpox
This was the commonest clinical type in variola major (4201 of cases in unvaccinated subjects and 58% of those in vaccinated subjects in Rao’s series). Plates 1.11 and 1.17 illustrate such cases. The lesions were fewer in number and discrete (i.e., separated by normal skin) on the face and elsewhere. In some cases, although the lesions were less numerous, the course of the disease was the same as in the other two subtypes; sometimes there was no secondary fever during the pustular stage. The overall case-fatality rate was much lower than in confluent or semiconfluent ordinary type smallpox—about 9% in unvaccinated subjects in Rao’s series.
MODIFIED-TYPE SMALLPOX
In 1908 Ricketts wrote:
“By the use of the terms `modified smallpox’ and abortive lesions’, no assumption is made as to the state of the patient with regard to vaccination. All that is implied is that he exhibits lesions which, in certain particulars, differ from the type most common among unvaccinated patients. The papules, instead of developing into the large vesicles and pustules of natural smallpox, are transformed into lesions which are generally smaller and often of a different conformation, which do not form pustules of the usual size or wholly fail to suppurate, and which hasten through their course of evolution more quickly than is natural.”
This was written before variola minor became endemic in Great Britain. In reviewing data on 13 686 cases of variola minor, Marsden (1936) suggested that:
“… the end results of the action of any of the factors which produce modification are indistinguishable in the individual patient…for example, “variola major” in a vaccinated subject.



Plate 1.16. Lesions on the sole of the foot on the 14th day of rash.Band C: Palm of the hand and sole of the foot of a 2-year-old Zairean boy on the 21st day of rash. Elsewhere on the body the scabs had separated; on the palms and soles they remained as dark disc-like scabs (“seeds”).

Plate 1.17. Distribution of the rash in smallpox. Dorsal and ventral views of a 3-year-old unvaccinated girl from Zaire, on the 5th day of rash. The case would be classified as mild discrete ordinary-type smallpox. The pustules were characteristically most numerous on the face, arms, and legs and rather sparse on the trunk.

Plate 1.18. Confluent ordinary-type smallpox in an unvaccinated woman in her twenties, on the 9th day of the illness. Pustules were confluent on the face, forearms and legs but discrete on the trunk. (From Stojkovic et al., 1974.)
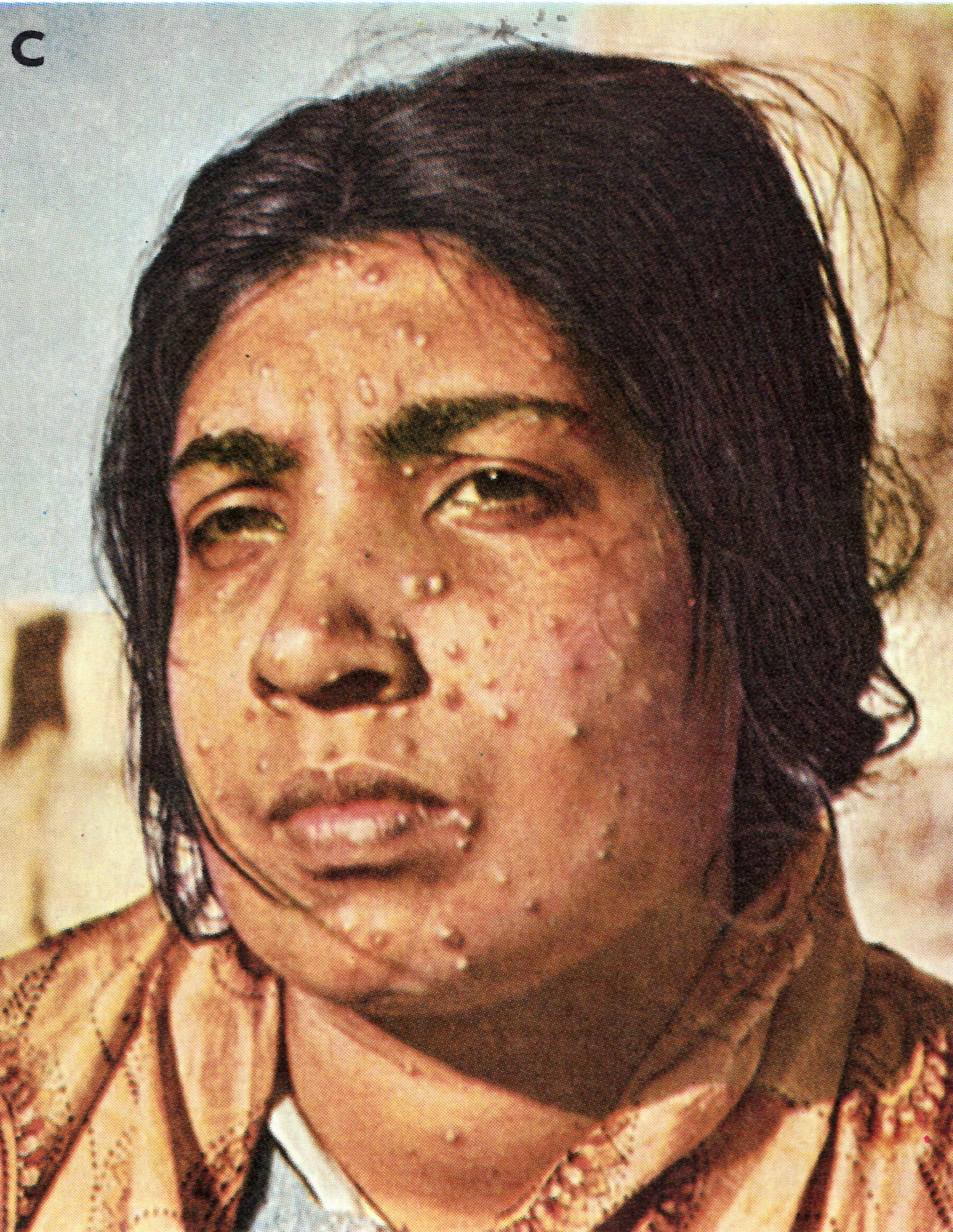
Plate 1.19. Modified-type smallpox. A: Vaccinated Japanese ma11 aged ’42 years, on the 10th day of the illness. Note the varying size of the lesions and their rapid evolution. B: Vaccinated Japanese woman aged 19 years. Very mild case. C: Adult female. Delhi, India. Note lack of toxaemia and diversity in size of lesions. (A and B from Uchida, 1955; C from Herrlich et al., 1967.)
Impressions of Smallpox in Bombay in 1958
"The majority of patients had fully developed smallpox in the suppurative stage, with confluent pustules covering the entire body. The head was usually covered by what appeared to be a single pustule; the nose and the lips were glued together. When the tightly filled vesicles burst, the pus soaked through the bedsheet, became smeared on the blanket and formed thick, yellowish scabs and crusts on the skin. When the pulse was taken tags of skin remained stuck to the fingers ... When secondary haemorrhage appeared, the affected area of skin formed a single black mass.
"All the gravely ill patients were also tortured by mucosa! symptoms. The tongue was more or less swollen and misshapen and hindered breathing through the mouth. The voice was hoarse and faltering. Swallowing was so painful that the patients refused all nourishment and, in spite of agonizing thirst, often also refused all fluids. We saw patients with deep invasion of the respiratory passages ... Wails and groans filled the rooms. The patients were conscious to their last breath.
"Some ... just lay there, dull and unresponsive. They no longer shook off the flies which sat on purulent eyelids, on the openings of mouth and nose, and in swarms on the inflamed areas of the skin. But they were still alive, and with touching gestures they lifted their hands and begged for help." (Translated from Herrlich, 1958.)
naturally immune, may be indistinguishable at the bedside, as in the laboratory, from ‘variola minor’. Furthermore, it is affirmed that the sole method of determining with certainty the primary factor responsible for modification in the individual patient is continued observation of the character of the disease in other patients infected by him or from a source in common with him; and, similarly, that, variola major is to be distinguished from variola minor only by epidemiological study of the course of the outbreak; for the clue is to be sought in the fact that, when the infective agent is of a persistently degraded virulence (variola minor), modification of attack is invariable, because it is independent of the patient’s immunity.”
Following Rao, a WHO Scientific Group on Smallpox Eradication (1968 ) defined modified-type smallpox in much the same way as had Ricketts:
“In this clinical type, which occurs mostly in, vaccinated patients, the modification relates to the character and development of the focal eruption; crusting is complete within 10 days. The pre-eruptive illness may be severe and is not necessarily of short duration, but secondary fever during the evolution of the eruption is usually absent. The skin lesions tend to evolve more quickly, are more superficial, and may not show the uniformity characteristic of the more typical smallpox eruption. The lesions are often few in number, but even when they are numerous they show some pleomorphism and involve rapidly.” by relating modified-type smallpox specifically to smallpox in vaccinated persons.
When preparing this book, we debated this aspect of the definition at some length and eventually agreed to adhere to the older convention—namely, that the term “modified type” connoted smallpox that was accelerated in its clinical course, compared with the expected evolution of ordinary-type variola major, rather than smallpox whose course was modified by vaccination. By far the commonest reason for an accelerated course in variola major was vaccination some years earlier (Plate 1.19), although Mack et al. (1970), who did not categorize any cases as modified-type smallpox, noted that in their series the rapidity of maturation was not associated with either vaccination status or lesion density. In Rao’s series, 25% of the cases in vaccinated subjects were classed as modified type, but only 2% of those occurring in unvaccinated subjects were so categorized. No fatal cases occurred in modified-type smallpox. Plate 1.20 illustrates the way in which even confluent lesions could progress much more rapidly than usual. However, modified type smallpox was usually manifested by fewer lesions as well as by an accelerated clinical course.
VARIOLA SINE ERUPTIONE
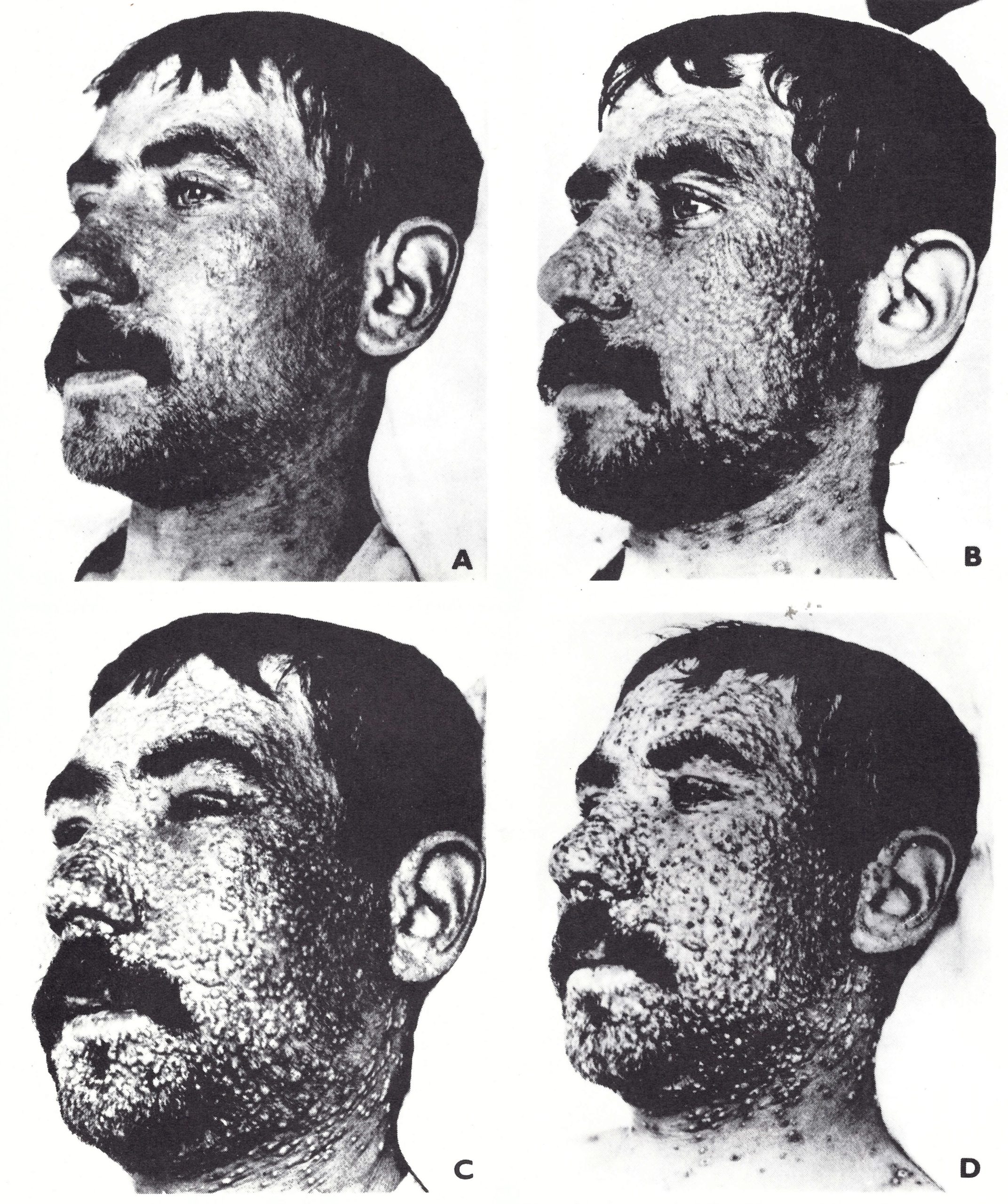
Plate 1.20. Confluent modified-type smallpox in a vaccinated adult male. A: In the papular stage but profuse. B: Early vesicles were confluent and suggested a severe attack, but although the face became swollen (C) the lesions did not increase in size and many became prematurely pus-capped. D: At a stage when the constant rash of ordinary-type smallpox would have been approaching its maturity, the lesions had become encrusted and the swelling of the features had subsided. Individual lesions were small. with fleshy deep-seated bases. (From Ricketts. 1908.)
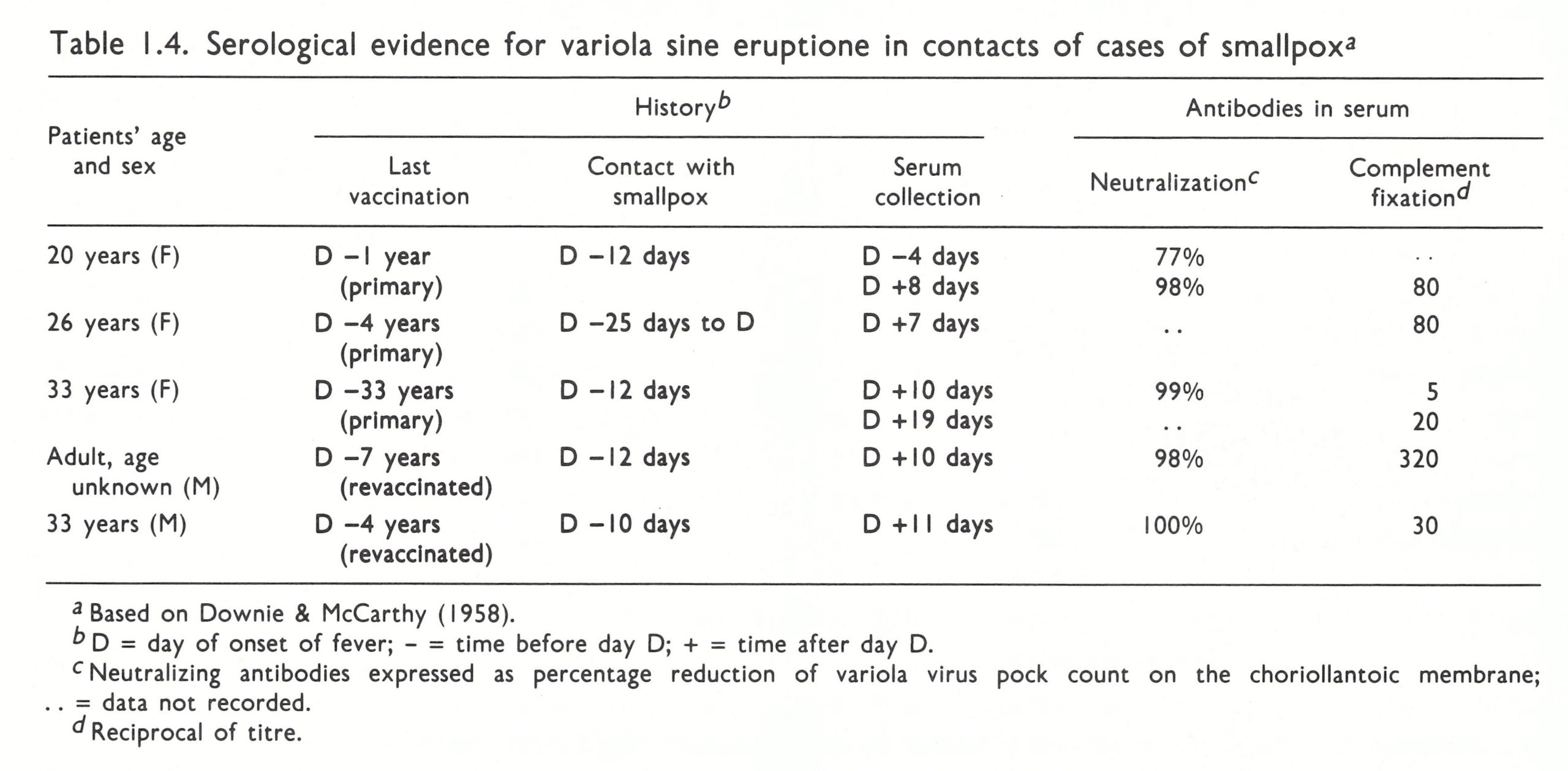
Febrile illness sometimes occurred among vaccinated contacts of cases of smallpox, with a temperature of about 39 °C, headache and sometimes backache. Within 48 hours or often less the attack had subsided, and the temperature was normal. Without laboratory tests it was impossible to determine whether these symptoms had been due to infection with variola virus, but the finding of high complement-fixing antibody in such patients (see Chapter 3), or a rise in antibody titres between the first and second bleeds, indicated that the fever had indeed been due to infection with the variola virus; such cases have been called variola sine eruptione (Table 1.4).
Occasionally viral isolations have been made from oropharyngeal swabs or washings from such patients. Marennikova et al. (1963) mention one such case; virus was recovered day of illness from a patient who did not get a rash. Subsequently, Shelukhina et al. (1973) reported the isolation of variola virus from the throat swab of a recently vaccinated child who had been in close contact with a case of smallpox and who was feverish when the specimen was taken, but who did not develop a rash. Verlinde & Tongeren (1952) reported positive results in 2 out of 13 contacts with cases of variola major from whom pharyngeal washings were taken. One of them was a vaccinated woman from whom, virus was recovered on the 14th day after contact, at a time when she had fever and constitutional symptoms. No rash developed. The other person apparently had a subclinical infection (see below).
Sometimes conjunctivitis was the only clinical manifestation of smallpox infection. Dekking et al. (1967) recovered variola virus from the tear fluid of 7 women, all thought to have had smallpox in infancy, who had signs of conjunctivitis after nursing children who died of smallpox. In a study directed at the possibility of conjunctiva! infection in smallpox contacts, Kempe et al. (1969) reported that conjunctivitis, but no other illness developed in 21 out of 55 close family contacts of smallpox patients. Variola virus was recovered from the conjunctival exudate of 12 of them. Four of these 12 patients on whom serological tests were carried out showed antibody rises compatible with recent smallpox.
Medical attendants who had been vaccinated and revaccinated but had not often been exposed to smallpox cases sometimes suffered from what appeared to be an allergic pneumonitis (“smallpox-handler’s lung”). Fever, constitutional symptoms and signs of pneumonia developed between 9 and 18 days after exposure to cases of smallpox, and X-rays showed diffuse mottling of the lungs (Howat & Arnott, 1944; Leroux et al., 1955; Evans & Foreman, 1963). None developed a rash and attempts 10 recover variola virus from throat washings were unsuccessful.
Table 1.4: Serological evidance for variola sine eruptione in contracts of cases of smallpoxa
Contract Fever
"Variola major was introduced into Durban from India in 1943 and spread widely in South Africa. I was personally involved with one of the patients admitted to Baragwanath Hospital. The physician-in-charge phoned to say that a patient had developed a profuse rash which he felt was probably due to a virus infection. One look at the patient convinced me that she had virulent confluent smallpox. The patient coughed in my face as I was examining her.
In spite of having been revaccinated many times, indeed each time I saw a patient with smallpox and again on this occasion and each time responding with an immune reaction, I developed a high fever 12 days later, beginning with chills, muscle pain, especially in the small of the back, and headache and photophobia. My throat became sore and intensely itchy and a white membrane formed on the tonsils and pharynx, presumably an outward sign of an immune reaction taking place at the virus-blood junction. Also of interest was a marked erythematous reaction which developed at the site of the inoculation of the vaccine, presumably an immunological reaction against the antigen deposited at the site in the skin. This reaction became apparent at the time of defervescence. At the same time, two vesicles, one on my ankle and one on my wrist, appeared and went through the typical stage of vesicle, pustule, and scab.
My infection seems to have been a case of 'contact fever', a condition which had been recognized as occurring in fully vaccinated individuals many years ago. One of the sisters and the physician attending this patient developed a similar illness also, in spite of vaccination immediately after the diagnosis was made."
(J. H. S. Gear, personal communication, 1983.)
SUBCLINICAL INFECTION WITH VARIOLA MAJOR VIRUS
There was no easy distinction between variola sine eruptions and subclinical infection, especially among persons living in circumstances in which malaria was endemic and feverish illnesses, from that or other causes, were so common as to be taken for granted.
Evidence from Viral Isolations
Only a few virological studies of smallpox contacts have been carried out (see above and Chapters 3 and 4). Variola virus was occasionally recovered from the throat swabs of such subjects, sometimes for several days in succession, but most of them had been vaccinated and never developed symptoms. Their infections would thus have to be classified as subclinical.
Evidence from Serological Studies
Serological diagnosis of past infection with variola virus depended on the fact that certain serological tests, such as the complement fixation test, gave positive results (with high titres) for relatively short periods while others remained positive for a prolonged period, both after vaccination and after overt smallpox (Chapter 3).
Heiner et al. (1971 a) carried out a detailed study of subclinical infection in villages and individual houses in West Pakistan in 1968- 1969, in which overt smallpox had occurred in 68.8% of the unvaccinated and 3 .2% of the vaccinated household or compound contacts. Retrospective positive serological diagnoses probably included some cases of smallpox with very few lesions and variola sine eruption (misdiagnosed or ignored) as well as truly subclinical infections, but the figures obtained give an indication of the frequency of unrecognized smallpox as it occurred in endemic regions.
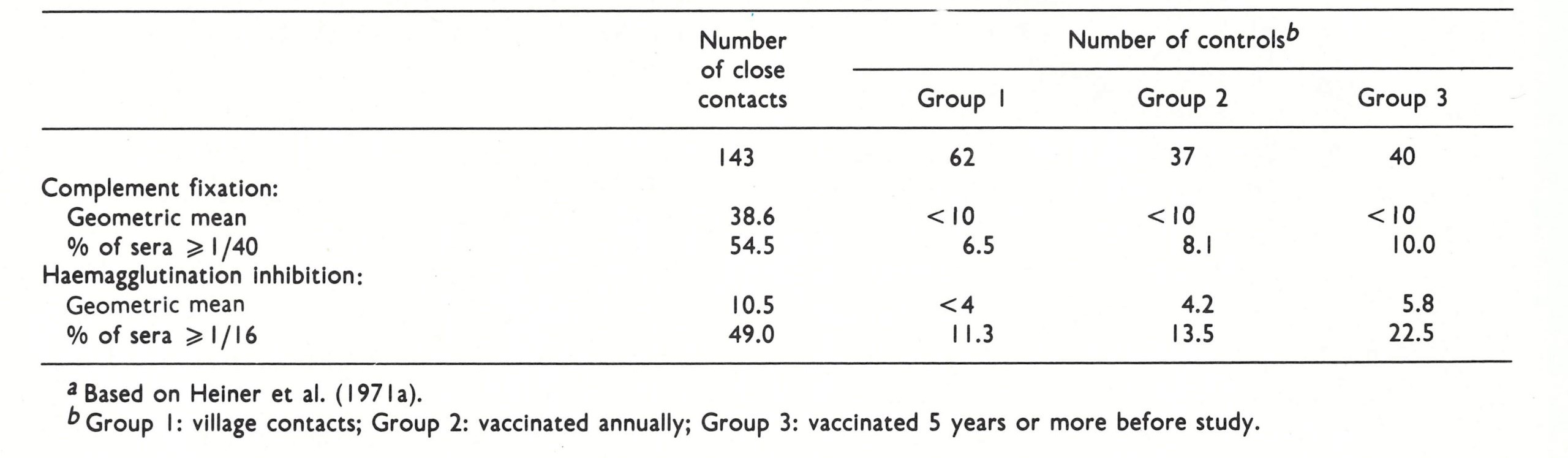
Two groups of people were studied. “Healthy contacts” were individuals who had not contracted overt smallpox but had been household or compound contacts of a recent case of smallpox and had not been vaccinated within 9 months of the study. The principal control group (Group 1 of Table 1.5) consisted of similar subjects who lived in the same villages but had not been in such close contact with smallpox cases. Two subsidiary control groups were used to determine the persistence of antibodies after vaccination; members of one group (Group 2 of Table 1 .5) had been vaccinated annually but not within 9 months of the study, and members of the other group (Group 3 of Table 1 .5) had last been vaccinated 5 years or more before the study. The highly significant differences between the close contacts and controls revealed by these tests were supported by similar results using other serological tests (neutralization, passive haemagglutination-inhibition and immunodiffusion). The frequency distribution of positive titres among the controls was unimodal, the majority being negative or having very low titres (Fig. 1.2). The titres of the contact group had a bimodal distribution, about half being negative or very low and the other half positive. This serological evidence indicates that subclinical infection that was accompanied by enough replication of virus to stimulate the production of complement fixing, and haemagglutinin-inhibiting antibodies occurred in many of the vaccinated close contacts of cases of variola major. Rao et al. (1970) came to a similar conclusion, using agel-precipitation test with both variola and vaccinia antigens. There was also suggestive but inconclusive evidence that inapparent infection occurred among subjects who had recovered from smallpox years before, a result that has parallels in measles (Ueda et al., 1969).
Table 1.5: Comparison of Titres of Complement-Fixing and Haemagglutinin-Inhibiting Antibodies Among Vaccinated Close Contacts of Cases of Variola Major and Vaccinated Controlsa
FLAT-TYPE SMALLPOX
Flat-type smallpox was so called because the lesions remained more or less flush with the skin at the time when raised vesicles formed in ordinary-type smallpox (Plate 1.21). This manifestation of the disease was seldom encountered (6.7% of cases in unvaccinated subjects in Rao’s series), and the majority of cases (72%) occurred in children. It was very rare in successfully vaccinated subjects. The prognosis was always grave, and most cases were fatal (see Table 1.2).
The pre-eruptive stage lasted 3-4 days, with the usual constitutional symptoms, which were severe and continued after the appearance of the rash. The fever remained elevated throughout and the patient had severe toxaemic symptoms.
The Rash
The enanthem on the tongue and palate was usually extensive and sometimes confluent. Occasionally a severe enanthem occurred on the rectal mucous membrane. The characteristic feature of flat-type smallpox was the nature of the skin lesions. Unlike the regular evolution seen in ordinary-type smallpox, the focal lesions in the skin matured very slowly, and at the papulovesicular stage, about 6 days after the onset of fever, a small depression was visible. By the 7th or 8th day the lesions were flat and appeared to be buried in the skin (Plate 1 .21). Most lesions had haemorrhages into their base, the central flattened portions appeared black or dark purple, and they were surrounded by an erythematous areola. The lesions differed from those of ordinary type smallpox in that the vesicles contained very little fluid, they were not multilocular, and they did not show umbilication. In contrast to the “shotty” feel of the lesions in ordinary type smallpox, they were soft and velvety to the touch. No further evolution of the lesions occurred, and frank pustules were rarely seen, although occasionally a few lesions, especially on the dorsum of the feet and hands, became pustular, while elsewhere on the body they remained as flat vesicles. Because of their superficial nature, the skin over the lesions peeled off after slight trauma, sometimes leaving extensive raw areas. Often the skin lesions did not conform to the classical “centrifugal” distribution.
Clinical Course
Throughout the course of the disease the patient was toxic and febrile. Respiratory complications, including oedema of the lung and sometimes frank pneumonia, set in by the 7th or the 8th day after the onset of fever. Rao noted that unvaccinated children sometimes developed an acute dilatation of the stomach 24-48 hours before death, which usually occurred between the 8th and the 12th day. A day or two before death, the colour of the lesions changed to an ashen grey, which, along with acute dilatation of the stomach, was a bad prognostic sign. In cases with a confluent enanthem on the tongue and palate, the mucous membrane sloughed, leaving large raw areas. Some patients passed blood d mucus in the early stages of the disease, indicating the extensive involvement of the rectal mucous membrane, and in such cases, Just before death, the rectal mucous membrane was sometimes sloughed off.
Among the few who survived, scabbing usually began on about the 13th-16th day after the onset of fever and was complete by about the 21st day. The scabs were thin and superficial and separated rapidly, leaving very superficial scars. Because of the bleeding into the base of the lesions, the scabs, before they dried, were purplish in colour.
Flat-type smallpox was probably due to the infection of particularly susceptible subjects with virulent strains of, the variola virus; it never occurred in, variola minor. The appearance of the lesions suggested a deficient cellular immune response in these patients, but no relevant studies were ever reported.
HAEMORRHAGIC-TYPE SMALLPOX
General Features
Considering its comparative rarity (only 200 cases in Rao’s series of 6942 hospitalized patients in Madras), a great deal has been written about haemorrhagic-type smallpox. No doubt this preoccupation was partly due to the rarity of the syndrome, its great severity and the difficult problem that it presented in differential diagnosis. This was particularly true in countries in which smallpox was no longer endemic; there were many instances in which outbreaks, or their extension could be traced to an unrecognized importation of haemorrhagic-type smallpox (see, for example, Benn, 1963; Stojkovic et al.,1974).
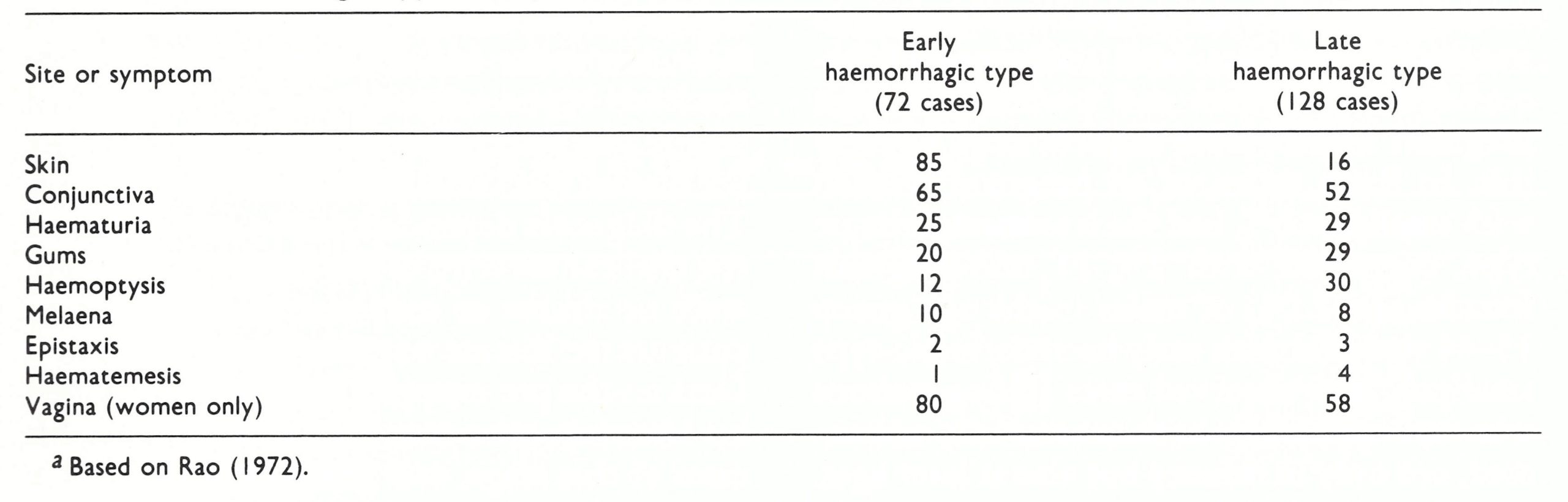
Histopathological studies (Bras, 1952a) support the clinical distinction of two varieties of haemorrhagic-type smallpox—what Curschmann (1875) and Immermann (1895) called ”purpura variolosa” and ”variola pustulosa haemorrhagica.” We shall follow Rao (1972) in calling them early and late haemorrhagic-type smallpox respectively. Early haemorrhagic-type smallpox was characterized by haemorrhages into the skin and/or mucous membranes early in the course of the illness. Subconjunctival haemorrhages were the most common, and bleeding from the gums, epistaxis, haematemesis, haemoptysis, haematuria, as well as vaginal bleeding in women, occurred at any time in the course of the illness.
In late haemorrhagic-type smallpox haemorrhages into the skin and mucous membranes often occurred, and usually also into the bases of the de,1eloping skin lesions. Some of these cases could equally well have been considered as cases of flat-type or confluent ordinary-type smallpox, associated with haemorrhages as a complication. However, all classifications contain an arbitrary element.
Haemorrhagic-type smallpox, of both subtypes, had two unusual epidemiological features: it occurred mostly in adults (Calcutta: Guha Mazumder et al., 1975; Madras: Rao, 1972) and in some extensive series (the Calcutta and Madras series) it was as common in vaccinated as in unvaccinated subjects (see Table 1.2). On the other hand, Sarkar et al. (1972), in a series of 170 cases observed in Calcutta during the years 1963-1969, recorded no cases of haemorrhagic-type smallpox among 81 patients who had been vaccinated but did note 32 cases among 89 unvaccinated subjects.



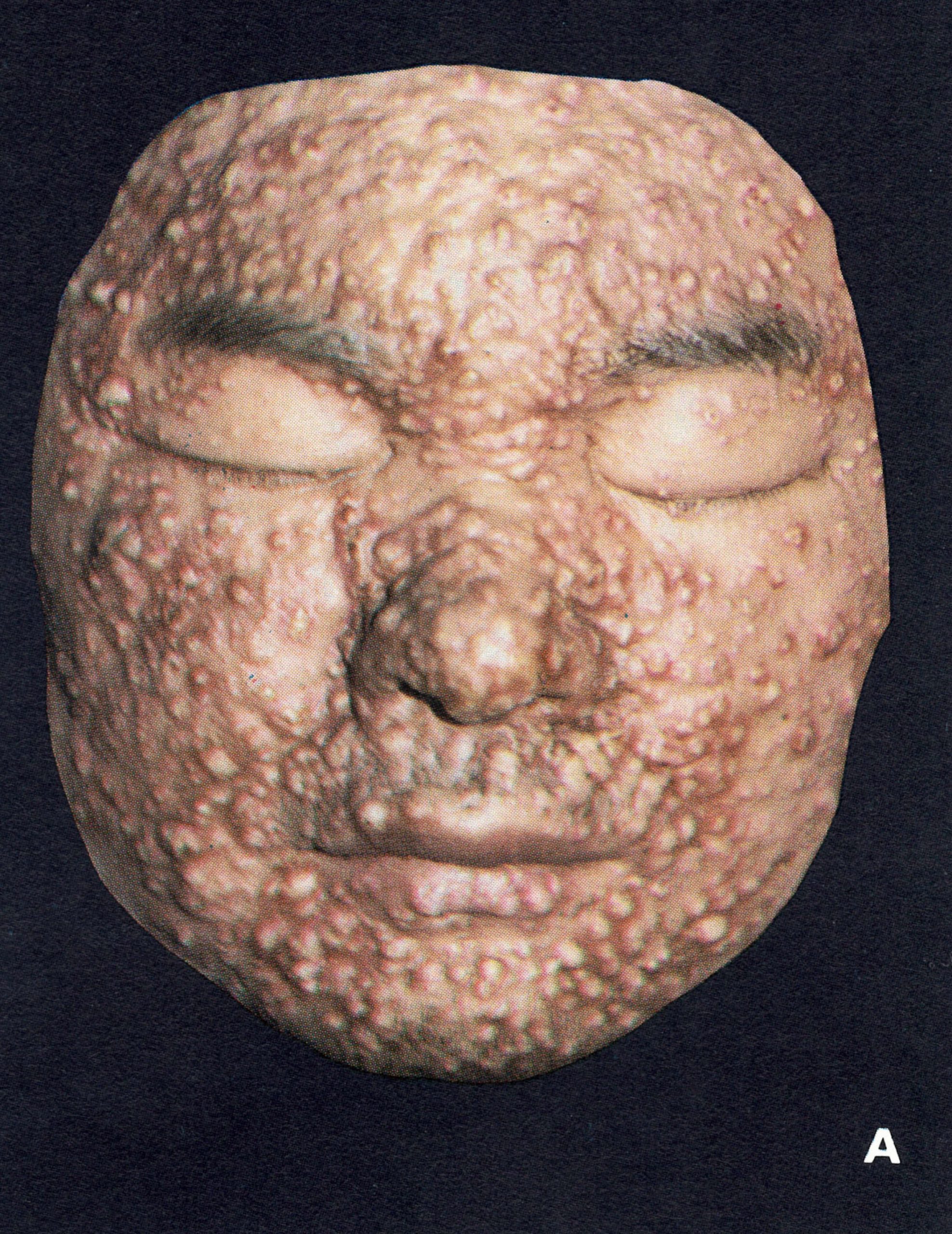
Plate 1.21. Flat-type smallpox. A: Adult Indian man. B and C: Unvaccinated young woman from Madras, India, on the 6th day of rash; she died 3 days later. Note severe toxaemia and extensive flat pustules in both cases. (A from Herrlich et al ., 1967.)

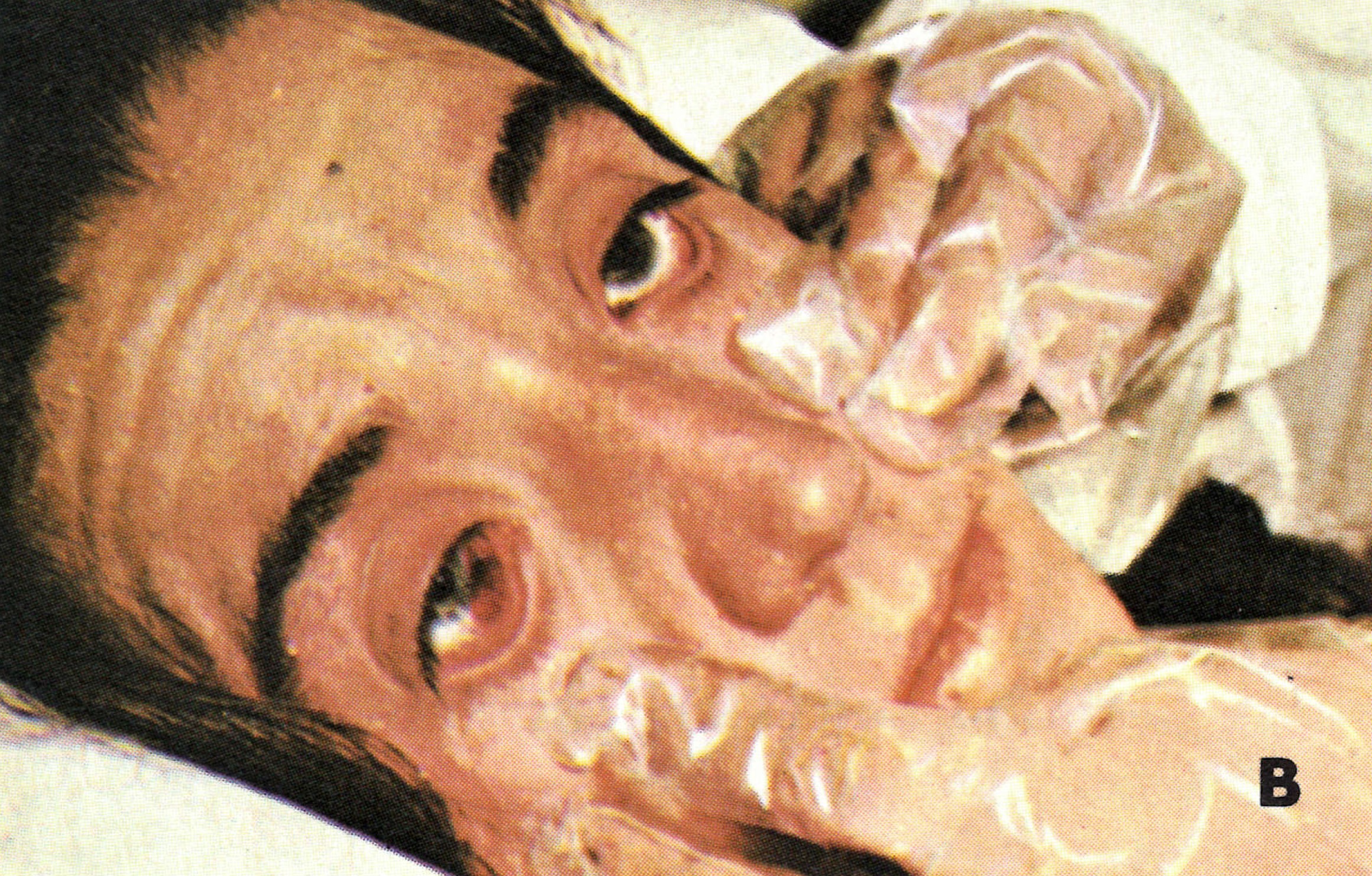

Plate 1.22. Early haemorrhagic-type smallpox. A: In an unvaccinated 60-year-old woman, who died on the 4th day of illness. Besides the rash illustrated she bled from many other sites, with subconjunctival haemorrhages, a bloody enanthem, epistaxis, haematuria, blood in the faeces and metrorrhagia. B: Subconjunctival haemorrhage. C: Fully developed haemorrhagic diathesis and death. (A from Stojkovic et al ., 1974: B and C from Herrlich et al ., 1967.)


Plate 1.23. Contrast between early and late haemorrhagic-type smallpox. A and B: Early haemorrhagic-type smallpox in a pregnant 18-year-old woman, showing severe toxaemia, petechial exanthem and bleeding from body openings; I hour before death. C: Late haemorrhagic-type smallpox in young woman, showing bleeding in base of pustules and development of a general haemorrhagic diathesis late in the disease. (From Herrlich et al ., 1967.)
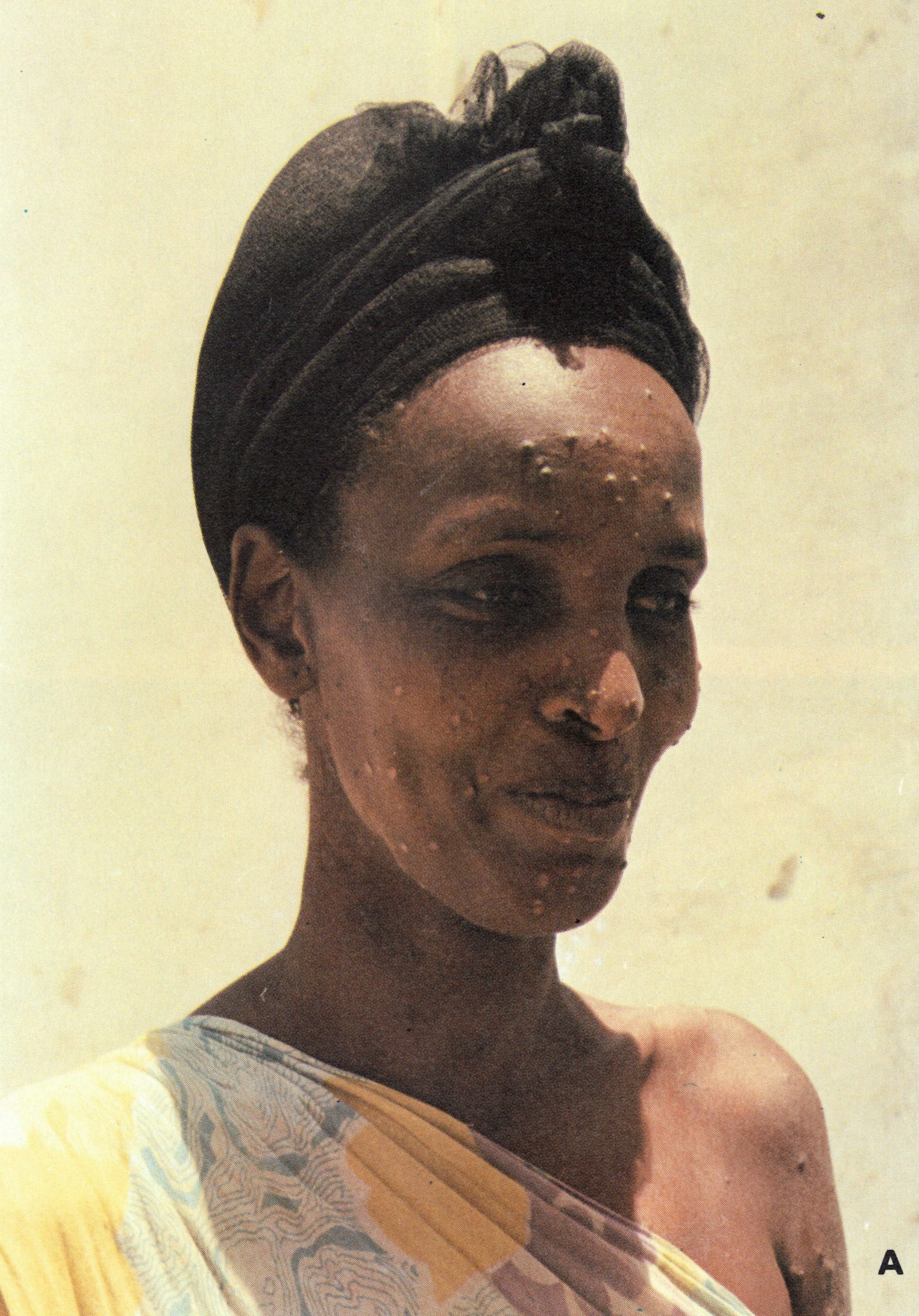

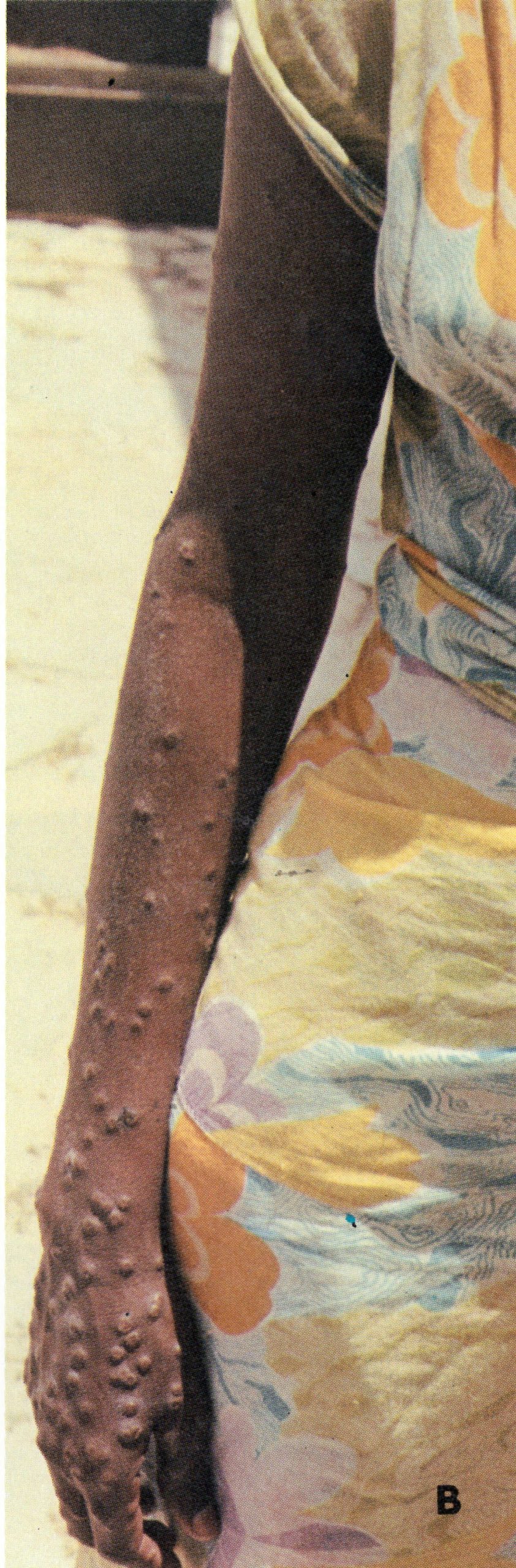
Plate 1.24. Variola minor in a 30-year-old unvaccinated Somali woman, 12 days after the onset of rash. The patient was not very sick and was ambulant throughout the disease. The lesions on the face were sparse (A) and evolved more rapidly than those on the arms and legs (B and C).
Early Haemorrhagic-Type Smallpox
With minor changes, descriptions of early and late haemorrhagic-type smallpox, and statistical data relating to them, are taken from Rao (1972). There is no point in trying to distinguish a “pre-eruptive” stage in this subtype, since death usually occurred before the focal rash had time to develop. The onset was sudden, and the high fever was accompanied by severe headache and backache which often persisted until the patient died. Patients looked very sick and were restless, anxious and pale. On the 2nd day of fever, the whole body was suffused with a generalized erythema, and petechiae and areas of ecchymosis appeared (Plate 1.22A and C). Subconjunctival haemorrhage was the most common (Plate 1.22B), but haemorrhages occurred from many sites (Table 1.6). On the 3rd day of the disease, the whole skin exhibited a finely textured matted surface and was velvety to the touch (Plate 1.23A and B), and 24 hours later it resembled dark-purple velvet, a feature seen most clearly in fair-skinned patients.
Patients showed signs of severe toxaemia, and became restless, breathless, and complained of heaviness and pain in the chest. Ricketts (1908) described and illustrated a characteristic expression of the face, with the features immobile, the lines of expression obliterated, the cheeks relaxed, the lips full and parted and the eyelids drooping-an expression of profound prostration. He also spoke of a fetid odour of the breath that was common to the toxaemic state in most cases of very severe smallpox, whether they were haemorrhagic, flat or confluent ordinary in type. Death occurred rather suddenly on about the 6th day of fever, patients usually remaining conscious until the end. Clinical observation and postmortem studies (Bras, 1952a) revealed that these patients did not die of haemorrhage, but they showed evidence of heart failure and sometimes oedema of the lungs. If the patient survived a few days longer, the superficial layers of the skin became raised and fluid collected underneath, forming large blebs containing serous or serosanguinous fluid, which ruptured after slight trauma, leaving extensive raw areas.
As was true for haemorrhagic-type smallpox in general, the early haemorrhagic subtype was more common in adults, 88% of all cases in Rao’s series being in persons over 14 years of age. Two-thirds of his cases were in women, pregnant women being especially susceptible. Of all the smallpox cases occurring in pregnant women in the Madras series, 16% were of this subtype, compared with only 0.9% among non-pregnant females and 0.8% among males in the age group 15-44 years. If a vaccinated person contracted hemorrhagic-type smallpox the outcome was not influenced by the prior vaccination; indeed, Rao (1972) states that a few cases of fatal early haemorrhagic-type smallpox occurred even among persons who had recently been successfully revaccinated.
Table 1.6: Frequency of haemorrhages (percentages of cases) in different anatomical sites in early and late haemorrhagic-type smallpox
Late Haemorrhagic-Type Smallpox
This form was differentiated from early haemorrhagic-type smallpox by the occurrence of haemorrhages after the appearance of the rash. The pre-eruptive stage lasted for 3-4 days, the temperature being about 40°C, with severe toxaemic symptoms like those described for early haemorrhagic-type smallpox, which continued unabated even after the appearance of the rash. The lesions, which started as macules, soon became papules but thereafter matured very slowly. They sometimes showed haemorrhages into their bases, which gave them a “flat” appearance (Plate 1.23C). Bras (1952a) noted that sections of such lesions showed that often the bleeding actually occurred in the corium beneath the pustules rather than in the pustules themselves.
Bleeding occurred in various mucous membranes although somewhat less frequently than in early haemorrhagic-type smallpox (Table 1.6). If the haemorrhagic focal lesions were “flat”, they did not evolve beyond the vesicular stage but then flattened out and became black. In about 15% of Rao’s cases, they matured into pustules, which followed the same course as in ordinary-type smallpox. In these cases, there were no haemorrhages into the lesions, but only into mucous membranes.
The majority of cases of late haemorrhagic type smallpox were fatal (see Table 1 .2), death occurring between the 8th and the 10th day. Cases with flat lesions had a higher fatality rate than those with raised pustular lesions. Among the patients who survived, the haemorrhages gradually resolved during a prolonged convalescence. However, in the few survivors among cases with the flat type of lesions, scabs usually formed sooner, resulting in only superficial scarring.
Of cases in the Madras series, 80% occurred in persons over 14 years old. Unlike the situation with early haemorrhagic-type smallpox, there was little difference in frequency between men and women, although pregnant women were slightly more susceptible. In Rao’s series, of all pregnant women with smallpox, 6 % had the late haemorrhagic type, compared with 2% of non-pregnant females and 2.1 %° of males in the age group 15-44 years. As with early haemorrhagic type smallpox, Rao observed cases among persons who had apparently been successfully vaccinated, not only in infancy but also at later ages.
Haemorrhagic-type smallpox was primarily due to defects in the response to infection by individual patients. It was very rare in variola minor (see below), but epidemiological evidence suggested that viral strains of unusual virulence were not the main cause of haemorrhagic-type smallpox. For example, Rao (1972) noted that there had not been a single haemorrhagic-type case among the contacts of 385 cases of haemorrhagic-type smallpox in Madras, although many of these contacts had contracted other forms of smallpox; this was an even longer series than that analysed in Table 1.2. Postmortem studies (Bras, 1952a) excluded concomitant bacterial infection as a precipitating factor. As will be shown in a later section, these cases were characterized by high and sustained viraemia, severe depletion of platelets and a poorly developed humoral immune response.
VARIOLA MINOR
This variety of smallpox differed greatly from variola major in its spectrum of severity and in its case-fatality rates—about 1 compared with about 20%.
Clinical Course
The most comprehensive account of the symptomatology of this disease was provided by Marsden (1936). His observations were based on 13 686 cases (most of which he examined personally) that occurred in London between 1928 and 1934. The description which follows is drawn largely from that source, supplemented by the accounts of MacCallum & Moody (1921), Jong (1956) and Noble et al. (1970), and the extensive field experience of epidemiologists working in Brazil, Ethiopia and Somalia during the smallpox eradication programmes in those countries.
Almost all cases of variola minor would have been classified as discrete ordinary- or modified-type smallpox, but in any individual case, it was impossible to determine whether the disease was variola major or variola minor. The diagnosis depended on the assessment of the clinical severity of the outbreak; if there were no deaths or only one among 50 or so patients the disease was usually variola minor. Data on the pre-eruptive stage were provided by Marsden, who saw only about 1 % of his cases at this stage, and MacCallum & Moody (1921), who saw many of the 2333 cases in their Jamaican series during the early stages of the disease. The onset was sudden, with a fever of 40°C, severe headache and backache and sometimes vomiting. Marsden recorded the occurrence of pre-eruptive rashes in 48 of the cases he saw during this stage; there were typical erythematous prodromal rashes in 37 cases. MacCallum & Moody recorded no such rashes in their mainly dark-skinned patients. The constitutional symptoms of the established disease were usually much less severe than those in cases of variola major with a comparable rash (Plate 1 .24). The toxaemia so evident in variola major rarely occurred, and patients with extensive skin rashes were often ambulant. The individual lesions were smaller than those of variola major, so that Marsden was able to count more than 500 lesions on the faces of 295 of his patients without this producing confluence, as would have been expected in variola major. Both MacCallum & Moody and Jong noted that the early vesicles and early pustules were unilocular and were not umbilicated, a clinical finding that was supported by histological examination of biopsy material. The sequence of appearance, the distribution and the nature of the skin lesions were similar to those described earlier for variola major, but their evolution was often more rapid. The eruption became vesicular on the 3rd day after the appearance of the first papules, and within 24 hours had become pustular. Early crusting was established on the 6th or 7th day of rash.
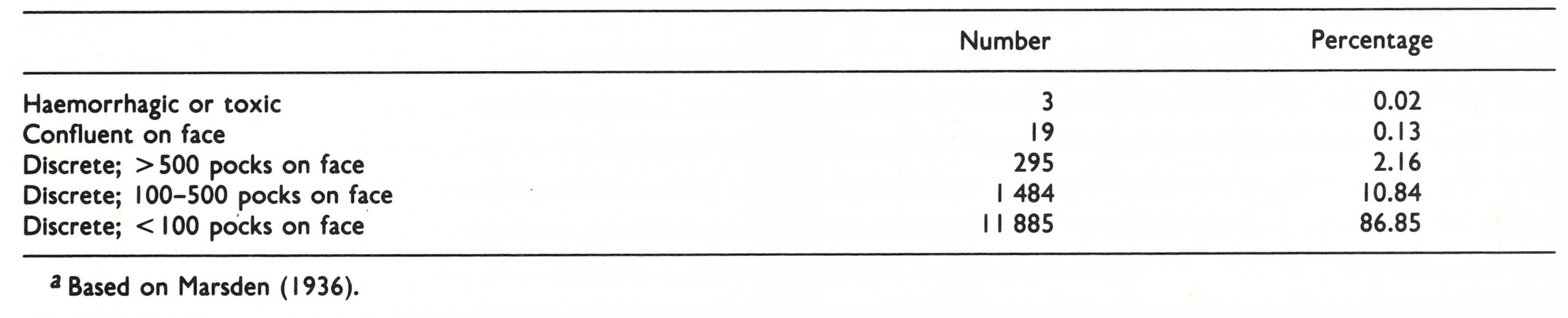
Cases of variola minor could not be classified according to Rao’s scheme (see Table 1 .1) because of the smaller size and more rapid evolution of the skin lesions. Indeed, the vast majority would have been classified as “modified- type smallpox”, which would clearly be a misnomer. Marsden grouped his cases according to the criteria formulated by Ricketts (1893) (Table 1.7). He noted that many of those classified as “discrete” would have been confluent in variola major; none was described as flat-type smallpox.
In keeping with the reduced severity and the more rapid evolution of the rash, secondary fever was rare, occurring in most of the more severe cases but, in Marsden’s experience, in only 0.13% of those with fewer than 100 lesions on the face, a group which included 87% of the cases in his series. Both MacCallum & Moody and Jong noted the absence in variola minor of the characteristic fetid odour of variola major.
Haemorrhagic-type cases did occur in variola minor, but they were extremely rare. Marsden recorded 3 cases, one of which recovered; Tigre et al. (1973) describe a fatal case in a 4-year-old boy infected in Argentina in 1970 and refer to 4 others observed in Brazil; Rodrigues-da-Silva et al. (1963) recorded 1 case which survived, and Moody (1922) recorded 2 fatal cases, both in pregnant women, among 2912 cases of variola minor in an epidemic in Jamaica in 1920-1921 .
There were 150 pregnant women in Marsden’s series but he commented only on the effects on the fetus, described below, and not on the severity of disease in the mother. The mortality in the Jamaica outbreak described by MacCallum & Moody (1921) was 0.4%, but of the 5 women who died 4 were 6 or 7 months pregnant and all of them displayed a “marked tendency to haemorrhage”.
Plate 1.25. James Pickford Marsden (1900-1977). Formerly Deputy Medical Superintendent, River Hospitals (London County Council), Dartford, Kent, England. He described a series of 13 686 cases of variola minor in outbreaks in London between 1928 and 1934.
Variola Sine Eruptione and Subclinical Infection
In a susceptible population the host resistance to any infection has a Gaussian distribution. The data on variola major (see Table 1.2) suggest that there would be few cases of variola sine eruptione and subclinical infection in unvaccinated persons exposed to this infection; however, many more such cases might be expected to occur in variola minor (Table 1.7). Data on the occurrence of such infections are difficult to find, but observations made in Brazil during the 1960s support this view. Positive titres of complement fixing antibody were found in 6 asymptomatic contacts of children with overt variola minor; most of the contacts had not been vaccinated more recently than 20 years before (Rodrigues-da-Silva et al., 1963). In a carefully studied ward outbreak, Salles-Gomes et al. (1965) observed positive complement-fixing and sometimes haemagglutinin-inhibiting antibody responses among 13 contacts exposed to overt variola minor. Four of these cases occurred in previously fully susceptible patients who had never had variola or been vaccinated.
Table 1.7: Classification of clinical type of cases of variola minors
SMALLPOX ACQUIRED BY UNUSUAL ROUTES OF INFECTIONS
Inoculation Variola and Variolation
Under unusual conditions, smallpox could be accidentally acquired through inoculation. Such cases sometimes occurred among nursing mothers and among those engaged in postmortem work (Lyons & Dixon, 1953), and cutaneous infections were recorded in an outbreak among lace-workers (Boobbyer, 1894). Marsden (1936) recorded 50 cases of accidental smallpox inoculation in variola minor and noted that the lesions of inoculation were usually recognized by their larger size and more advanced development than the other elements of the focal rash.
Much more common, however, was the practice of deliberately inoculating variola virus into the skin, practised since ancient times in Africa and India and in China (where, however, infection was usually produced by nasal insulation) and on a large scale in some parts of Europe and North America during the 18th century (see Chapter 6). Variolation continued to be practised in many parts of Africa and in Afghanistan and Pakistan until quite recent times, and the spread from variolated individuals was an important source of smallpox in Afghanistan and Ethiopia up to the time of eradication in 1973 and 1976 respectively.
The technique of cutaneous variolation has varied at different times and in different places. Detailed descriptions of the methods used during the 18th century in France and other countries of Europe and in North America can be found in Miller (1957) and Razzell (1977b); methods used more recently in Africa and Asia are described in Chapters 14 and 21.
the methods used during the 18th century in France and other countries of Europe and in North America can be found in Miller (1957) and Razzell (1977b); methods used more recently in Africa and Asia are described in Chapters 14 and 21.
Clinical picture
The clinical picture of inoculation smallpox was influenced by several factors. Inoculation carried out after the manner of modern vaccination produced a local skin lesion that first appeared as a small papule on the 3rd day after the operation. It grew in size and became vesicular by the 5th day, and by the 8th or 9th day there was a large pustular lesion with much surrounding erythema and oedema (see Chapter 6, Plates 6.1-6.3). Fever and constitutional symptoms corresponding to the pre-eruptive stage of ordinary-type smallpox began on the 8th day and often lasted for only 2 or 3 days (Fig. 1.3). There were usually a number of secondary lesions around the primary lesion (see Plates 6.1-6.3), and the generalized rash began on the 9th day on the face, often consisting of very scanty macules, which rapidly became vesicular. Subsequent lesions sometimes appeared over the next 3 or 4 days and evolved more rapidly than in smallpox acquired by the respiratory route. Even in the few cases that had a large number of secondary pustules (which in inoculation smallpox amounted to as many as 300-1000), the lesions matured more rapidly than in ordinary-type smallpox, so that scabbing occurred 3 or 4 days earlier and the lesions, being more superficial, gave rise to less scarring. By the 18th or 19th day most of the scabs, except for the lesions on the palms of the hands and the soles of the feet, had been shed.
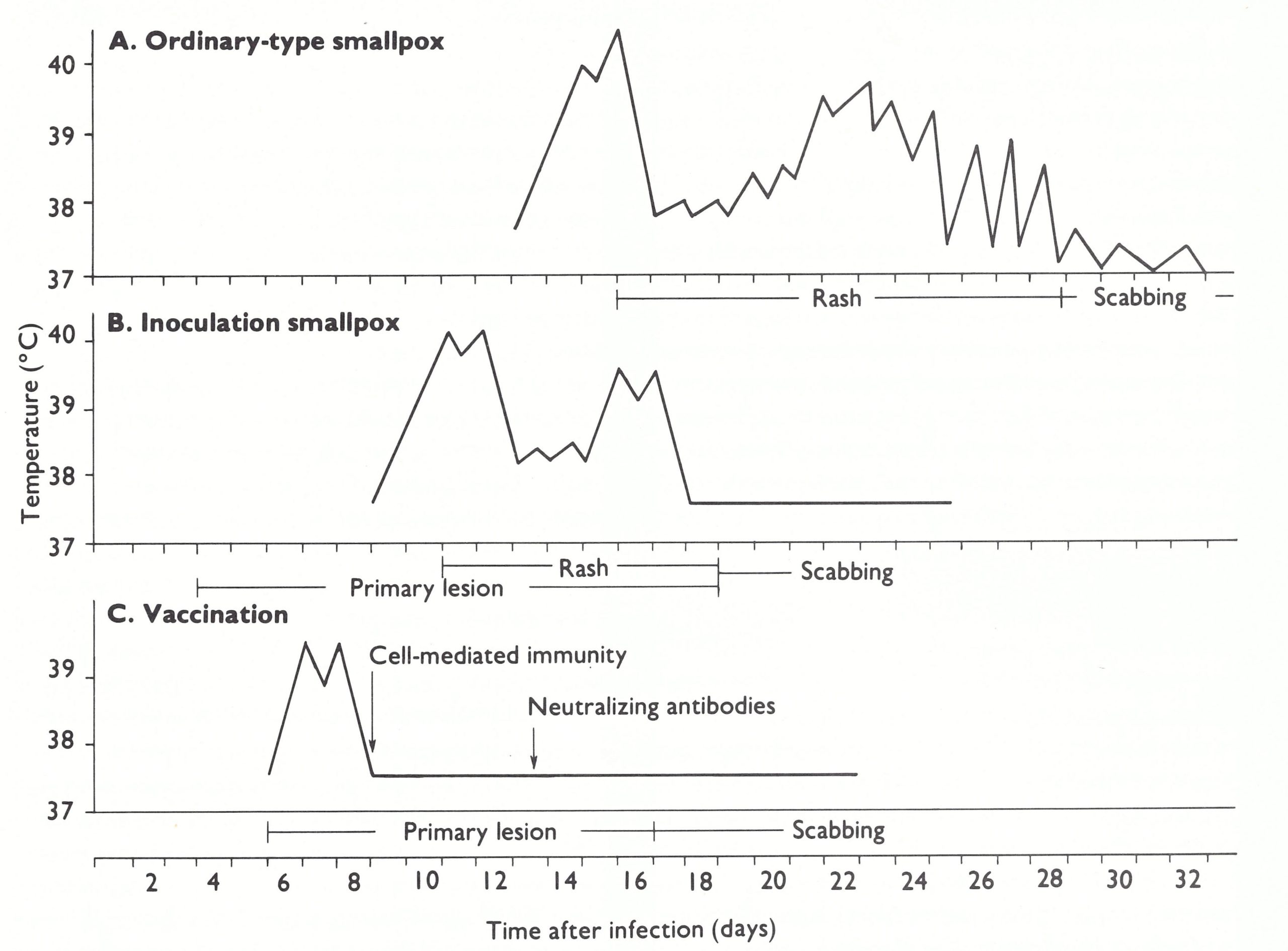
Fig 1.3. Percentages of positive antibody titres obtained at various times after the onset of ordinary type variola major, by 4 types of serological test, in 151 subjects of whom 127 had been vaccinated, usually many years before. (From Downie et al ., 1969a.)
Neither haemorrhagic- nor flat-type smallpox seems to have been recorded as a sequel to variolation, at least in European and North American practice. This may have been due to the professional interests of the inoculators and their concern to be exempt from any possible blame for deaths that occurred; but, in any event, it was the practice to avoid inoculating, especially susceptible persons—pregnant women, children under 2 years of age and the aged and infirm.
Apart from the primary skin lesion, most cases, like those of naturally acquired inoculation smallpox, appeared to fall into the category of modified-type smallpox. Cases with only a primary skin lesion, 1 or 2 days of fever and no rash—variola sine eruptione—were said to be not uncommon. Rao himself suffered from such an infection (Rao, 1972).
Because of the smaller number of lesions and their more rapid maturation, cases of inoculation smallpox were less infectious and were infectious for shorter periods, than those of smallpox acquired by the respiratory route. Nevertheless, they often did initiate smallpox in unvaccinated (and unvariolated) contacts, both in 18th-century practice in Europe and North America and in recent times in Afghanistan and Ethiopia. Such contact cases were no different from those associated with other epidemics due to whatever strain happened to have been used for variolation.
Because of the smaller number of lesions and their more rapid maturation, cases of inoculation smallpox were less infectious, and were infectious for shorter periods, than those of smallpox acquired by the respiratory route. Nevertheless, they often did initiate smallpox in unvaccinated (and unvariolated) contacts, both in 18th century practice in Europe and North America and in recent times in Afghanistan and Ethiopia. Such contact cases were no different from those associated with other epidemics due to whatever strain happened to have been used for variolation.
Severity
In the hands of some of the famous British practitioners of variolation (e.g., the Suttons—see Razzell, 1977b) the severity of smallpox due to variolation appears to have been low and the mortality less than 2%.
In their day only variola major virus was circulating in Great Britain and some contact cases acquired severe and sometimes fatal smallpox; the explanation for the mild nature of smallpox after variolation lay with the age and health of the inoculated subjects, the route of inoculation and the small dose usually employed.
In Ethiopia, where variolation was practised until 1976, the virus used during the last few decades was variola minor and inoculation smallpox was correspondingly mild; nevertheless, it was an important source of outbreaks during the latter part of the eradication campaign in that country (see Chapter 21).
Congenital Smallpox
The effects of pregnancy on the clinical course of smallpox in the mother are discussed later in this chapter. Infection of the fetus depended on the growth of the virus in the placenta and its subsequent release into the cord blood. Its frequency was uncertain, since most pregnant women suffering from variola major aborted during the pre-eruptive fever. Occasionally babies born of mothers suffering from smallpox developed symptoms after birth; Rao (1972) records 10 such cases among 116 live births. In these babies, all of whom died, the fever-to-fever interval was 9-12 days. Among the offspring of 84 women who suffered from haemorrhagic-type smallpox (all with intense and sustained viraemia) none of the 21 children born alive developed clinically recognizable congenital smallpox, but 17 of them died in less than 72 hours too soon for a diagnosis to be made.
The baby was infected in half of 34 pregnancies in which the mother was infected with variola minor during late pregnancy (Marsden & Greenfield, 1934). Usually the infection was acquired in utero, at the time of the mother’s viraemia; the incubation period then appeared to be 8-9 days, as in inoculation smallpox. If the fetus escaped infection during that time the infant might become infected at birth or later in the neonatal period, especially if the mother’s rash was then at an early stage of development. If the mother carried the fetus to term, the newborn infant was usually temporarily immune from smallpox because of maternal antibodies.
Fetal variola was a rare occurrence, reported only in variola minor. In some cases (MacCallum & Moody, 1921; Ribeiro et al., 1965) the fetus sustained an attack of smallpox in utero and was subsequently born alive, having been infected at the time the mother had the disease 2 or 3 months before birth. More often (for example in 8 of the 20 pregnant women in the series described by MacCallum & Moody (1921)) abortion occurred and the macerated fetus was marked with scars from an attack of variola minor sustained in utero.
Nowhere in the scientific literature is there a reliable reference to the occurrence of congenital defects caused by smallpox or vaccination in a pregnant woman. Since the usual viral causes of congenital defects are non-cytocidal viruses, whereas variola and vaccinia viruses are both cytocidal, this is not unexpected.
EFFECTS OF VACCINATION ON THE CLINICAL COURSE OF SMALLPOX
The most important effect of vaccination was the protection of the subject from smallpox, but prior vaccination, even many years before, usually influenced the course of the disease in persons who did show symptoms. The situation in individual subjects depended on a variety of factors, some relating to the host: genetic resistance, physiological state, and interval since vaccination or revaccination; some to the vaccine and its mode of delivery: the strain of vaccinia virus used, the potency of the vaccine and the inoculation procedure employed; and, finally, of course, whether the infection was due to variola major or variola minor virus. Further, it was the general practice to vaccinate or revaccinate contacts; some of these individuals were incubating smallpox at the time of vaccination.
Successful vaccination within 5 years of exposure provided a high level of protection against smallpox. When vaccination had been performed more than 20 years before exposure there was sometimes no residual immunity and the course of the disease was similar to that seen in unvaccinated subjects, although even then the outcome, examined statistically, was modified (Hanna, 1913).
Although its most important effect was the prevention of infection, vaccination also influenced the frequency of different clinical types of smallpox among persons who did contract the disease (see Table 1.2). Not only was modified-type smallpox much more common among vaccinated patients (25.3% compared with 2.1%. in Rao’s series), but a larger proportion of ordinary-type cases was classified as discrete (83.5% compared with 47.4%) and flat-type cases were less common (1.3% compared with 6.7%). However, Rao (1972) and Guha Mazumder et al. (1975) reported that, among those who got smallpox, haemorrhagic-type smallpox was slightly more common among vaccinated than among unvaccinated subjects (see Table 1 .2 and below). Not all investigators agreed with this view; for example, Sarkar et al. (1972) reported that in a series of 170 cases, no cases of haemorrhagic-type smallpox occurred among vaccinated persons, but 32 cases occurred in unvaccinated subjects. Except in modified-type smallpox, which was hardly ever fatal, and haemorrhagic-type, which was almost always fatal, the case-fatality rates were lower in vaccinated than in unvaccinated patients (see Table 1.2).
Vaccination resulted in the modification of three aspects: the toxaemia (and correspondingly the case-fatality rate), the number of lesions, and the character and evolution of the rash. The waning of vaccine protection against these manifestations did not occur uniformly.
Effects of Vaccination on Toxaemia
The initial constitutional symptoms of smallpox were associated with the replication of variola virus during the incubation period, the end of which was marked by the sudden onset of fever and headache that accompanied the secondary viraemia. In some cases vaccine protection had little apparent effect on symptoms of fever and headache at the end of the incubation period, but no skin lesions developed; the patient was said to have suffered from variola sine eruptione, which was occasionally associated with pneumonitis. Sometimes the pre-eruptive stage in vaccinated subjects was accompanied by a fleeting erythematous rash that particularly affected the flexures.
The more toxic forms of smallpox, except for the haemorrhagic-type, were much less common in vaccinated than in unvaccinated subjects (see Table 1.2).
Effects of Vaccination on Toxaemia
The initial constitutional symptoms of smallpox were associated with the replication of variola virus during the incubation period, the end of which was marked by the sudden onset of fever and headache that accompanied the secondary viraemia. In some cases, vaccine protection had little apparent effect on symptoms of fever and headache at the end of the incubation period, but no skin lesions developed; the patient was said to have suffered from variola sine eruptione, which was occasionally associated with pneumonitis. Sometimes the pre-eruptive stage in vaccinated subjects was accompanied by a fleeting erythematous rash that particularly affected the flexures.
The more toxic forms of smallpox, except for the haemorrhagic type, were much less common in vaccinated than in unvaccinated subjects (see Table 1.2).
Effects of Vaccination on the Number of Lesions
The skin lesions were initiated by the infection of dermal capillaries by virus released into the circulation during the secondary viraemia (see Chapter 3). Prior vaccination usually reduced the level of viraemia and thus the opportunity for skin lesions to develop; variola sine eruptione occurred mainly in vaccinated persons, and confluent lesions were much less common among vaccinated subjects. In Rao’s series 16.5% of vaccinated patients who had ordinary-type smallpox were classified as confluent or semiconfluent, compared with 52.6% of unvaccinated patients.
Effects of Vaccination on the Character and Evolution of the Rash
In some cases of smallpox in vaccinated subjects the character and rate of evolution of the rash differed from the usual pattern, presumably because of the anamnestic response initiated by infection with variola virus in the vaccinated subject. The individual lesions were more superficial and hence did not have the “shotty” feel, and their edges were often irregular. Umbilication and loculation were not found in these superficial lesions, which resembled those of chickenpox. Often the modified lesions were very small, but they could vary quite considerably in size in any particular area of skin (Plate 1 .19C). In fair-skinned subjects the red areola around the pustules was often more pronounced presumably an allergic manifestation. In many vaccinated subjects the rash also evolved more rapidly so that the lesions passed through the stages of macule, vesicle and pustule in 3 or 4 days instead of 7 or 8. On the other hand, many field workers found no such differences in symptomatology, apart from a greater frequency of cases of ordinary-type smallpox with few skin lesions. Smallpox in vaccinated subjects who did contract the disease was no different in other respects from that found in unvaccinated patients. Mack et al. (1970), in cases with similar lesion density, found no differences that could be related to vaccination status in the length of the pre-eruptive stage, the rate of maturation of skin lesions, the occurrence of corneal lesions, the case fatality rate or the prevalence of residual pockmarks.
Effects of Vaccination in Variola Minor
In Marsden’s series, variola minor occurred in 1756 patients who showed evidence of having been successfully vaccinated, out of a total of 13 686 cases. In only 2 of these was there evidence of vaccination within the previous 5 years and in only 7 within the previous 10 years; the great majority had been vaccinated 20 or more years earlier. In an epidemic in the Netherlands, Jong (1956) found no cases in persons vaccinated less than 30 years before, and, in Brazil, Suzart de Carvalho Filho et al. (1970) found a vaccine efficacy ratio of 94%, regardless of the interval since previous vaccination (see Chapter 12). Vaccination thus provided very good protection against variola minor, a conclusion which is in keeping with the experience of epidemiologists working in Ethiopia and Somalia during the global smallpox eradication programme.
LABORATORY FINDINGS
Laboratory observations on cases of smallpox will be described in Chapter 3, as part of an attempt to build up a coherent picture of the pathogenesis of the disease. However, it is useful to examine some of the results here in the context of the symptomatology of smallpox.
Virological Observations
The principal value of the laboratory, without which it would have been impossible confidently to certify global smallpox eradication, was the demonstration of the presence or absence of variola virus in vesicle fluid and ‘crusts from suspected cases of smallpox (see below). This section reviews virological findings made on cases of smallpox which may help to explain the clinical signs and symptoms.
Viraemia
According to the model for the pathogenesis of variola developed in Chapter 3, there was an early transient viraemia soon after infection. The virus then replicated in the lymph nodes, spleen and bone marrow until just before the onset of symptoms, which was associated with secondary viraemia. All the reported observations of viraemia in smallpox relate to this “secondary” viraemia.
Precise observations were never made on the distribution of variola virions among the various components of the blood (plasma, leukocytes and erythrocytes); by analogy with other poxvirus infections viraemia would have been expected to be primarily cell-associated (see Chapter 3). However, most observations that were made on the blood of smallpox patients utilized either serum or lysed whole blood, the material being inoculated either into monkeys (Kyrle & Morawetz, 1915) or on the chorioallantois membrane of chick embryos (Downie et al., 1950, 1953, 1969b; Mitra et al., 1966). In haemorrhagic-type smallpox both serum and lysed blood gave positive results; it is possible that viraemia might have been detected more readily in cases of ordinary-type smallpox if separated leukocytes had been examined.
However, the general pattern appears to have been consistent. Although viraemia must always have occurred, virus was only rarely recovered from the blood or serum from cases of ordinary-type smallpox. Downie et al. (1950, 1953) and Mitra et al. (1966) recorded one or two positive results out of many attempts in such cases and then only in the early days of the disease. The picture in haemorrhagic-type smallpox was quite different. Virus was readily recovered from the blood of all cases, the titres were usually high, as determined by titration on the chorioallantoic membrane of chick embryos (Downie et al ., 1953, 1969b; Mitra et al ., 1966; Sarkar et al., 1969), and viraemia usually persisted until the patient died. Downie et al. (1969b) noted that viraemia was consistently much higher in cases of early than of late haemorrhagic-type smallpox. Patients with haemorrhagic-type smallpox usually also had soluble antigens in their bloodstream (antigenemia), the level of which was roughly correlated with the level of the viraemia. Although few opportunities occurred for its practical use, the demonstration of antigen in the serum provided a useful and rapid laboratory diagnostic test for haemorrhagic-type smallpox, a disease in which the differential diagnosis was extremely difficult, especially in non-endemic countries, in which it would rarely have been suspected.
Thus haemorrhagic-type smallpox appears to have been associated with overwhelming infection and the continued release of virus from infected cells into the bloodstream; in other cases, demonstrable viraemia was usually restricted to the pre-eruptive and early eruptive stages of the disease.
Skin
Variola virus could be readily demonstrated in the skin lesions of all cases of smallpox, from the earliest stages of the rash until the scabs separated. The large amount of virus in the vesicle fluid was eventually included within the scabs. However, because virus in the scabs was associated with large flakes of inspissated material it appeared to be relatively unimportant as a source of infectivity for contacts, compared with virus in the oropharyngeal secretions (see Chapter 4). In spite of the absence of vesicles or pustules, the skin of cases of haemorrhagic-type smallpox contained very large numbers of virions.
Oral and pharyngeal mucous membranes
The earliest focal lesions in smallpox occurred in the oropharynx, and instead of forming papules and vesicles, as in the skin, these lesions soon ulcerated and thus liberated large amounts of virus into the saliva. This was the major source of infectious virus as far as the transmission of smallpox was concerned (see Chapter 4).
Conjunctiva
Patients with smallpox sometimes had conjunctivitis. Virus could be readily recovered from the conjunctival swabs of patients in whom conjunctivitis developed early in the course of the disease, but usually not from convalescent patients who developed conjunctivitis (Dekking et al.,1967; Kempe et al.,1969; Sarkar et al.,1973a). The occasional appearance of variolous conjunctivitis at or before the onset of fever suggested to Kempe et al. (1969) that the conjunctiva may have been the portal of entry in these cases.
Virological Observations
The principal value of the laboratory, without which it would have been impossible confidently to certify global smallpox eradication, was the demonstration of the presence or absence of variola virus in vesicle fluid and ‘crusts from suspected cases of smallpox (see below). This section reviews virological findings made on cases of smallpox which may help to explain the clinical signs and symptoms.
Urine
The interpretation of the results of testing urine for virus was difficult, since patients often had pustules on the skin near the urethral orifice, and catheterization, had it been possible to do this aseptically, was not ethically justifiable. However, viruria was recorded by all investigators who tested the urine from cases of variola major. Positive results were recorded by Downie et al. (1 965a) in 17 out of 34 specimens, and by Sarkar et al. (1973a) in 21 out of 39. The viruria was greater in degree and more persistent in severe cases (haemorrhagic-type smallpox and those with a confluent rash) than in milder cases. No virus was detected in the urine of some cases whose severity was comparable to that of cases with viruria.
Serological Observation
The immune response in generalized orthopoxvirus infections (including smallpox) is described in Chapter 3; this section summarizes information on the correlation between various serological responses and the clinical severity of smallpox, to the extent that such information is available. Unfortunately, there is an almost complete lack of data on cell-mediated immunity in smallpox, an immune response that was probably of critical importance in the pathogenesis and immunopathology of the disease.
The most comprehensive studies on the serological responses in cases of smallpox are those reported by Downie et al . (1969a,b) on ordinary-type and haemorrhagic-type smallpox, using haemagglutination-inhibition, complement-fixation, gel-precipitation and neutralization tests. In most cases of non-fatal ordinary-type smallpox, antibody was detected by haemagglutination-inhibition and neutralization tests between the 6th and 8th days after the onset; by complement fixation and gel precipitation about 2 days later (Fig.1.4). The antibody response was slower and the titres were lower in early haemorrhagic type smallpox than in other cases (Sarkar et al.,1967, 1969), but Downie et al. (1969b) found haemagglutinin-inhibiting antibodies in most cases of haemorrhagic-type smallpox, although both neutralizing and complement-fixing antibodies were at much lower levels or absent in such cases.
As might be expected, antibodies usually appeared earlier and reached higher levels in vaccinated than in unvaccinated patients (Downie & McCarthy, 1958).
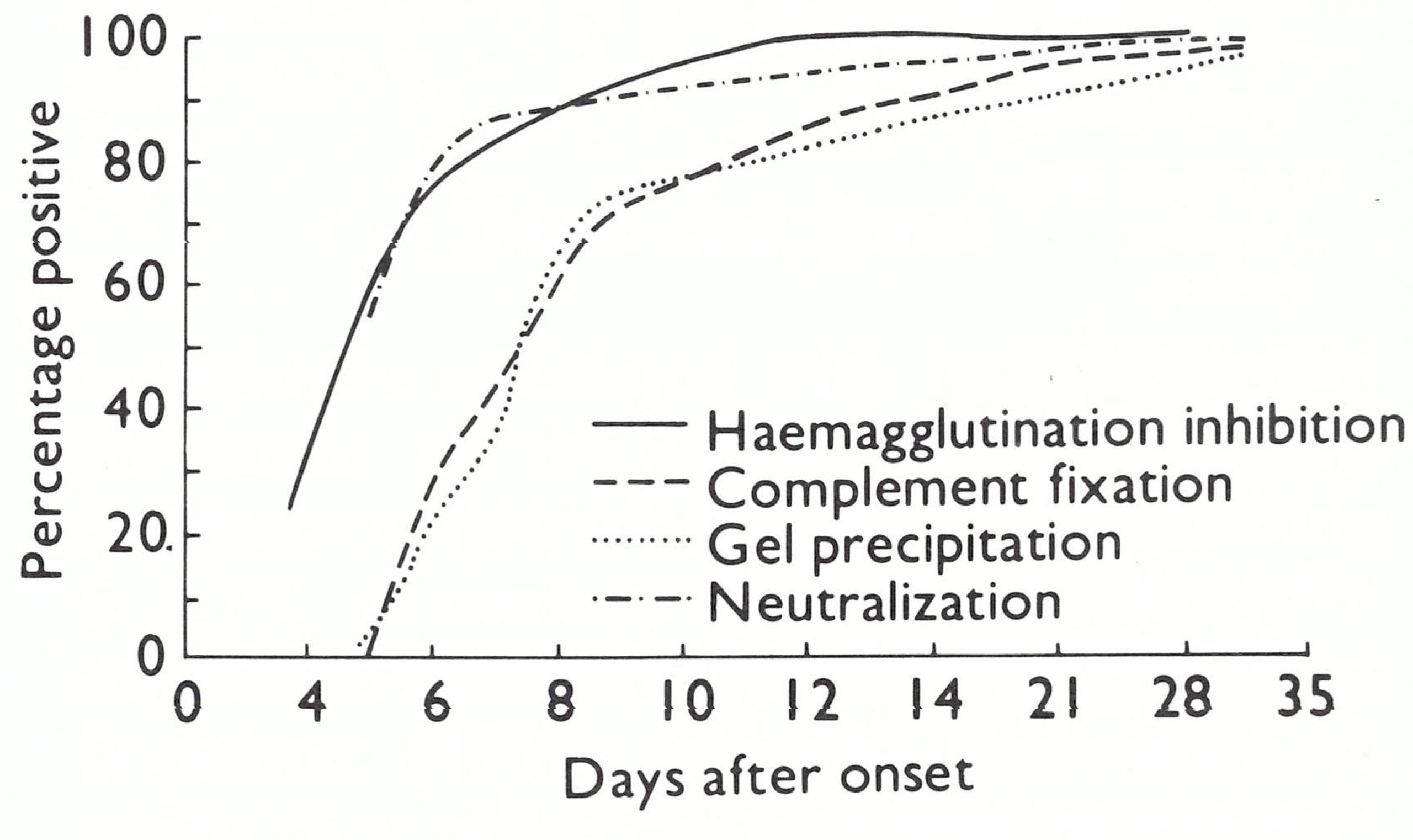
Fig 1.4. Percentages of positive antibody titres obtained at various times after the onset of ordinary type variola major, by 4 types of serological test, in 151 subjects of whom 127 had been vaccinated, usually many years before. (From Downie et al.,1969a.)
Virological Observations
The blood picture in smallpox varied according to the nature of the case and the stage of the disease. In most cases there was little change in the red blood cell count, but during the eruptive stage the numbers of granular leukocytes usually fell and a relative and absolute increase in the numbers of lymphocytes occurred. The granulocytopenia was often reversed during the late pustular stage, perhaps because of secondary infection of the skin lesions in some cases.
In early hemorrhagic-type smallpox, there was often a striking change in the blood picture, which Ikeda (1925) considered to be of diagnostic value. Pathological forms of normoblasts with basophil stippling or polychromatophilia were common; the total leukocyte count was increased by 30-40%, with a marked augmentation in the numbers of lymphocytes and monocytes; and the presence of myelocytes and myeloblasts suggested an intense stimulation of the bone marrow. In contrast to the rise in the number of platelets found after the vesicular stage in many other cases of smallpox, Ikeda discovered that there was a marked and progressive thrombocytopenia in haernorrhagic-type smallpox, the number of circulating platelets often falling to a very low level.
Sarkar et al.(1968) compared the concentrations of various serum proteins in 28 sera from cases of smallpox of different clinical severity with those of an equal number of normal subjects. The total proteins were unchanged, but albumin was diminished and globulin increased, the increase being associated with fractions a2 and γ. There was no correlation between the concentrations of any of these proteins and the level of haemagglutinin- inhibiting antibodies.
More detailed studies of the pathophysiology of bleeding were carried out on patients in Madras and reported by McKenzie et al. (1965) and Roberts et al. (1965). Their findings in relation to vascular integrity, platelet function and blood coagulation are summarized in Table 1.8, which illustrates the generality of impaired functions in haemorrhagic-smallpox, especially. evident in the early type. In contrast to Ikeda (1925), these investigators found that many patients with smallpox but with no clinical evidence of haemorrhage had moderate to severe thrombocytopenia but usually no other coagulation defect. Patients with late haemorrhagic-type smallpox had severe thrombocytopenia and some had a mild to moderate decrease in prothrombin and a moderate decrease in accelerator globulin. As expected, the cases of early haemorrhagic-type smallpox were characterized by multiple defects, with significant and specific coagulation defects in addition to severe thrombocytopenia. All had an elevated thrombin time and a total absence of accelerator globulin, which the authors ascribed to disseminated intravascular coagulation. At autopsy, such cases showed disseminated intravascular thrombosis involving small vessels in many organs.
COMPLICATIONS
Complications of two kinds occurred in smallpox. One group was due either directly or indirectly to viral activity in an unusual site, the other to secondary bacterial infection.
The Skin
As noted earlier, pustulation was part of the natural sequence of development of the skin lesions in smallpox. However, in most countries in the days before antibiotics were available and, even recently, in those in which hygiene was poor and such treatment not obtainable, secondary bacterial infection of the skin lesions often occurred, sometimes to an extent that Ricketts (1908) described as “thousands of boils”. In pre-antibiotic days septic complications also occurred in variola minor; Marsden (1936) recorded the presence of boils in 3.65% and of septic dermatitis in 2.3% of his series of cases. Even higher percentages of these complications were seen in the Ogaden desert during the late stages of the eradication programme in Somalia (Ježek et al.,1981).
Ocular System
As noted earlier, pustulation was part of the natural sequence of development of the skin lesions in smallpox. However, in most countries in the days before antibiotics were available and, even recently, in those in which hygiene was poor and such treatment not obtainable, secondary bacterial infection of the skin lesions often occurred, sometimes to an extent that Ricketts (1908) described as “thousands of boils”. In pre-antibiotic days septic complications also occurred in variola minor; Marsden (1936) recorded the presence of boils in 3.65% and of septic dermatitis in 2.3% of his series of cases. Even higher percentages of these complications were seen in the Ogaden desert during the late stages of the eradication programme in Somalia (Ježek et al.,1981).
Mild conjunctivitis, occurring early in the course of the disease, or at the time of the eruption if there were lesions on the eyelids, was essentially part of the acute disease and not a complication. Sometimes it was the only symptom (Dekking et al.,1967). Pocks often occurred on the margins of the eyelids but not on the avascular cornea. Often there was much swelling of the eyelids (see Plate 1.13), which made it difficult to open the eyes. Dixon (1962) suggests that it was this swelling, rather than keratitis or corneal ulceration, that accounted for the frequent references in the old non-technical literature that a person was “blind with smallpox”. Corneal ulceration and sometimes keratitis did occur in smallpox. These complications were common in haemorrhagic-type smallpox but were of relatively minor importance because such patients soon died. In ordinary-type smallpox corneal ulceration occurred at about the end of the 2nd week of illness, beginning at the corneal margin. Sometimes the ulcers healed rapidly and there was only a trivial opacity; on other occasions, there was severe corneal scarring. Both Dixon (1962) and Rao (1972) note that keratitis and corneal ulceration were far more common in malnourished children than in the well-nourished; for this reason, these conditions continued to be more important complications in developing countries than in the more prosperous industrialized countries. Mack et al. (1970) reported that 28 out of 405 patients examined within 6 weeks of onset in a rural setting in Pakistani Punjab had corneal lesions, which occurred mostly in patients with confluent or semiconfluent rashes. Three out of 11 patients seen a year later had permanent ocular lesions, and 4 other instances of permanent lesions were observed in 148 cases in whom lesions had not originally been seen. The overall rate of residual corneal opacity in those surviving smallpox was 4.4%. Corneal ulcers occurred in 1% of cases in Rao’s series (excluding haemorrhagic-type smallpox) and keratitis in about 0.25%.
Joints and Bones
Arthritis, associated with involvement of the bones of the joints, was a relatively common complication of smallpox, occurring in 1.7% of cases in Rao’s series, usually in children. Cockshott & MacGregor (1958) and Cockshott (1965) reviewed the condition, which they called “osteomyelitis variolosa”, and described a series of cases observed in Nigeria. More recently, Gupta & Srivasta (1973) reviewed the X-ray features of 20 cases observed in India. The elbow was the most commonly affected joint and symmetrical bilateral joint involvement was frequent (Plate 1.26). Although secondary bacterial infection sometimes occurred, the disease was primarily due to viral infection of the meta-physes of growing bones. The primary bone lesion was probably a proliferating arteritis, which led to fibrosis, necrosis and bone resorption (Eeckels et al.,1964).
This complication usually occurred late in the course of the disease, after the 15th day, and was accompanied by a brief recurrence of fever during the scabbing stage. Because of the severity of smallpox itself, and the insidious nature of the bone and joint involvement, cases were often missed during the attack, and only recognized as probably having been due to smallpox years afterwards because of a variety of bone defects for which there were no other explanations (Gupta & Srivasta, 1973).
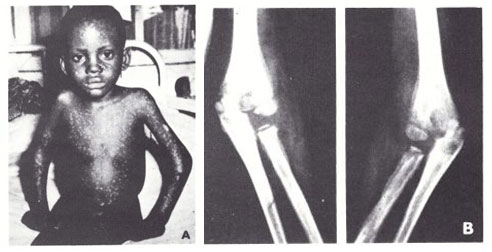
Plate1.26. Osteomyelitis variolosa in an unvaccinated Nigerian child. joint symptoms appeared I week after the onset of rash and affected both elbows. A: External appearance, showing hypopigmented spots of healed exanthem and swollen elbows. B: X-ray appearances. (From Cockshott & MacGregor, 1958.)
Respiratory System
Rao (1972) regarded respiratory complications as common in severe smallpox, especially in the unvaccinated. However, the symptoms he describes, bronchitis and pneumonitis, are better regarded as part of the normal disease syndrome than as complications. Pulmonary oedema was fairly common in haemorrhagic-and flat-type smallpox. Bronchopneumonia due to secondary bacterial infection sometimes occurred and could be serious in debilitated patients. In his long series of cases of variola minor, Marsden (1936) recorded only 7 cases of bronchopneumonia.
Although sometimes responsible for death, pulmonary complications were usually followed by complete recovery. However, coughing could have serious epidemiological consequences, if it occurred during the 1st week of disease, when the oral secretions were most highly infectious (see Chapter 4). A.R. Rao (personal communication, 1981) regarded cough associated with the sticky mucus of bronchitis as a relatively common symptom, especially in unvaccinated individuals. However, its epidemiological consequences were reduced if, as in the majority of cases, it did not become evident before about the 10th day of the disease. Epidemiologists engaged in the global smallpox eradication programme regarded cough as a rare symptom in smallpox.
Gastrointestinal System
Apart from vomiting and, less commonly, diarrhea during the pre-eruptive stage, gastrointestinal symptoms were rare. Diarrhea sometimes occurred in the 2nd week and acute dilatation of the stomach was observed, especially in infants, though only rarely (Rao, 1972). Extensive viral infection of the intestinal mucous membrane occurred in some severe cases, especially in flat-type smallpox. In such cases, which were usually fatal, portions of the mucous membrane were passed as a tubular cast.
Genitourinary System
Orchitis was uncommon (0.1% in Rao’s series) and usually unilateral. This observation casts doubt on the suggestion of Phadke et al. (1973) that smallpox was the single most important etiological factor in obstructive azoospermia in India. In haemorrhagic-type smallpox, bleeding into the pelvis of the kidney sometimes produced haematuria (see Table 1.6).
Central Nervous System
Encephalitis was a relatively common complication of smallpox (about 1 in 500 cases in variola major (Rao, 1972) and 1 in 2000 cases in variola minor (Marsden, 1936)). It usually appeared between the 6th and the 10th day, when the rash was in the papular or vesicular stage. Encephalitis contributed little to the case-fatality rate of variola major but was an important factor in the few deaths which occurred in variola minor. Recovery, although sometimes slow, was usually complete.
According to a detailed review by Marsden & Hurst (1932), the symptomatology and the pathological findings in fatal cases of encephalitis associated with variola minor were indistinguishable from those of the encephalomyelitis which occasionally occurs after vaccination or in the late stages of measles. Clinical details are described in Chapter 7, for although it was a much rarer complication (in Madras, for example, 1 in 500 cases of smallpox and 1 in 100 000 cases of primary vaccination (Rao, 1972)), postinfection encephalitis was a much more significant feature of vaccination than of smallpox, since it was then the result of medical intervention in an otherwise healthy subject rather than a rare complication of a severe disease.
SEQUELAE
In order of their frequency the sequelae seen in persons who recovered from smallpox were facial pockmarks, blindness, and limb deformities.
Pockmarks
During the first few months after recovery from smallpox the sites of the scabs were abnormally pigmented, hypopigmented in dark-skinned persons and red or hyperpigmented in fair-skinned subjects (Plate 1.27A and B). As the skin regained its normal pigmentation, most cases of variola major, but few of variola minor, were seen to have pitted scars, called pockmarks, in the sites of some of the pustular skin lesions. These were depressed scars 2 mm or more in diameter, usually circular and varying in number from one (which would be difficult to ascribe to smallpox) to several hundred (Plate 1.27C and D). They resulted from fibrosis in the dermis and were much more common on the face because of the greater frequency of large sebaceous glands in the skin of the face (Bras, 1952b). Although the rash occurred on the scalp as well, relatively few pockmarks were seen there. In ordinary type variola major the rash affected the sebaceous glands severely (Bras, 1952b) and permanent facial pockmarks occurred in 65-80% of survivors (Mack et al.,1970; Ježek et al.,1978d). The sebaceous glands were not affected in flat type smallpox and the few patients who survived this type of infection were rarely severely pockmarked.
When secondary bacterial infection of the pustules occurred, the resulting scarring was often more severe and the scars more irregular in shape than after an uncomplicated rash.
In variola minor the rash, though sometimes profuse, comprised shallow lesions that were usually restricted to the epidermis and only rarely involved the sebaceous glands—hence pockmarks were much less common in such cases. For example, Marsden (1936) recorded depressed scars in only 0.7% of his series of cases, although hyperpigmentation was present in about 11% of these fair-skinned subjects at the time of their discharge from hospital. Among persons with more deeply pigmented skins, hypopigmented spots sometimes occurred on the face or elsewhere for several months after recovery (Ježek & Hardjotanojo, 1980) but eventually disappeared.
The observation of facial pockmarks was an important epidemiological tool in smallpox eradication programmes in countries in which the disease was due to variola major, but in those in which variola minor prevailed pockmarking was too infrequent for such surveys to be of epidemiological value (see Chapters 4 and 24).
Blindness
Corneal scarring with consequent blindness sometimes followed the keratitis or corneal ulceration which was a rare complication of smallpox (though less uncommon in malnourished individuals). As Dixon (1962) commented, “Every writer on smallpox over the last 150 years has pointed out that in his experience the amount of blindness due to smallpox was much less than that quoted by previous authors”. The explanation is probably that the authors quoted were almost always writing of conditions in Europe. During the last 150 years the level of nourishment and hygiene rose steadily among those who formed the subject of these publications, and as remarked earlier, keratitis, corneal ulceration and corneal scarring rarely occurred in well-nourished patients. Blindness following smallpox remained a serious although uncommon complication in poorer countries (Plate 1 .27C and D). Rao (1972) noted 60 patients with keratitis and/or corneal ulcer, of whom 24 had loss of vision in one eye and 1 in both eyes—an incidence of blindness of 0.45% among 5459 survivors. In Bangladesh, Hughes (WHO/SE/78.101) found blindness in 0.9°% and corneal opacities in an additional 2.1% of patients examined 1- 2 years after recovery from smallpox. All 4 cases of blindness and 7 of the 9 cases of corneal scarring occurred in unvaccinated subjects
Limb Deformities
As has been described earlier, osteomyelitis and arthritis were not uncommon complications of smallpox. Many cases resolved without permanent deformity. Because of the severity of the disease itself and the mild symptoms of joint involvement, skeletal manifestations were often missed during the acute infection and recognized years later in the form of bone shortening, flail joints, subluxations and gross bone deformities (Gupta & Srivasta, 1973).
PROGNOSIS OF VARIOLA MAJOR
The prognosis of a case of smallpox had to be evaluated in terms of the likelihood of death and the possibilities of serious sequelae. In both respects, the prognosis of variola minor was almost invariably good; the vast majority of patients recovered and even facial pockmarks were an uncommon sequel. It is therefore necessary to consider the prognosis only in terms of variola major. As will be further elaborated in Chapter 2, there were geographical variations in the virulence of variola major virus, in terms of the usual case fatality rates in different parts of the world, which during the period of the Intensified Smallpox Eradication Programme (see Chapter 10) seemed to be uniformly high in the Indian subcontinent and adjacent parts of western Asia and rather lower in Indonesia and western, central and eastern Africa.
Calculation of Case-Fatality Rates
How representative were hospital-based data?
The calculation of the case-fatality rate in smallpox was not a straightforward matter. Most data (e.g., Rao, 1972; Guha Mazumder et al ., 1975) were based on series of cases treated in hospitals; the question arises of how representative of the total spectrum of cases were those admitted to hospital. Rao’s (1972) series was probably representative of cases in Madras; in a personal communication (1981) this author states that between 1961 and 1969, 80-90°,0 of all cases in Madras were admitted to the city’s Infectious Diseases Hospital, the proportion between 1965 and 1969 being almost 100%.
This was not true of other areas, especially where rural populations were involved. Koplan et al . (1978) investigated this problem in Bangladesh, from which smallpox had been eliminated in 1970 only to be reintroduced by refugees returning from India in 1972. Table 1.9 compares the age- and sex-specific case-fatality rates pertaining to 346 cases admitted to the Dhaka Infectious Diseases Hospital during the period March 1972 to April 1973 with those of 502 non-hospitalized cases diagnosed by specially trained surveillance teams in a rural area in the Noakhali District in south-central Bangladesh during the period July 1972 to February 1973. The age and sex distributions of the two sets of data are very similar; when the rates were applied to a standard Bengali population the overall case fatality rates were only changed from 51 % to 52% for the hospitalized patients and from 21 % to 23% for the village patients, a highly significant difference between the two sets of data.
The explanation is complex and lies in a number of factors which would probably differ in importance in different places, but which must always be borne in mind when considering case-fatality rates based on hospitalized series of cases in countries in which smallpox was endemic. In Bangladesh, hospital admission reflected a high proportion of patients who were too ill to travel back to their villages or too sick to hide their illness within the community, whereas the village data essentially referred to every case in the community.
Table 1.9: Age- and sex-specific case-fatality rates of 346 hospitalized smallpox patients and 502 nonhospitalized rural smallpox cases in Bangladesha
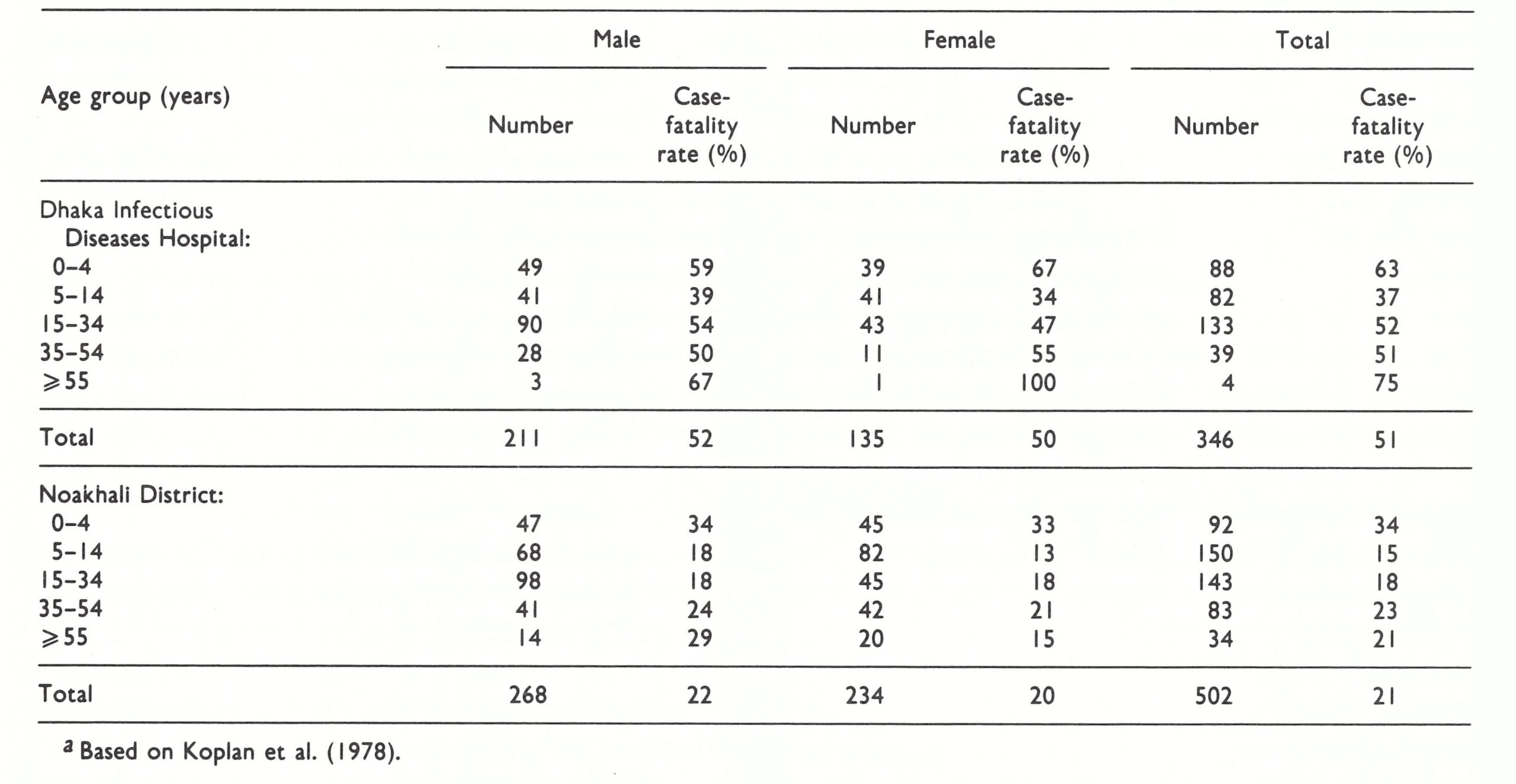
Effects of Immunity
Immunity after an attack of smallpox
A person who had recovered from smallpox had a high degree of immunity to reinfection, which usually lasted throughout life, but second attacks did occasionally occur. Rao (1972) noted about 1 repeat attack per 1000 cases, the average interval between the attacks being 15-20 years. This refers to clinical disease, confirmed by laboratory investigation, in pockmarked persons. Serological examination of exposed contacts would probably have revealed that second subclinical infections were much more common; subclinical infection was not uncommon in vaccinated contacts (Heiner et al., 1971a). However, subclinical infections were of little epidemiological importance, except as boosters of immunity, since subjects with such infections did not transmit them.
Another measure of the persistence of resistance following smallpox was provided by determining the response of persons known to have had smallpox to challenge vaccination with vaccinia virus. Interpretation of the results (Table 1.10) is complicated by the fact that many of those who had had variola major had also been vaccinated, a procedure which enhanced immunity to challenge vaccination (Zikmund et al.,1978). A substantial proportion of persons exhibited a major response to vaccination as early as 1 year after recovery from variola minor, and even after variola major resistance to challenge vaccination was low in half the subjects tested 6-11 years after recovery from the disease. In variola major immunity to challenge vaccination persisted for much longer in those who had had a severe attack of smallpox than in those who had suffered only a mild attack (Vichniakov, 1968). As far as heterologous immunity is concerned, it appears that vaccination protected against naturally transmitted smallpox (see below and Chapter 7) rather more effectively than smallpox modified the response to vaccination. This may have been mainly due to the dose of virus and the manner of its implantation: a large dose introduced into the skin in vaccination and a small dose implanted on the respiratory mucosa in smallpox.
Table 1.10: Protection against challenge vaccination with vaccinia virus among persons who had recovered from smallpoxa
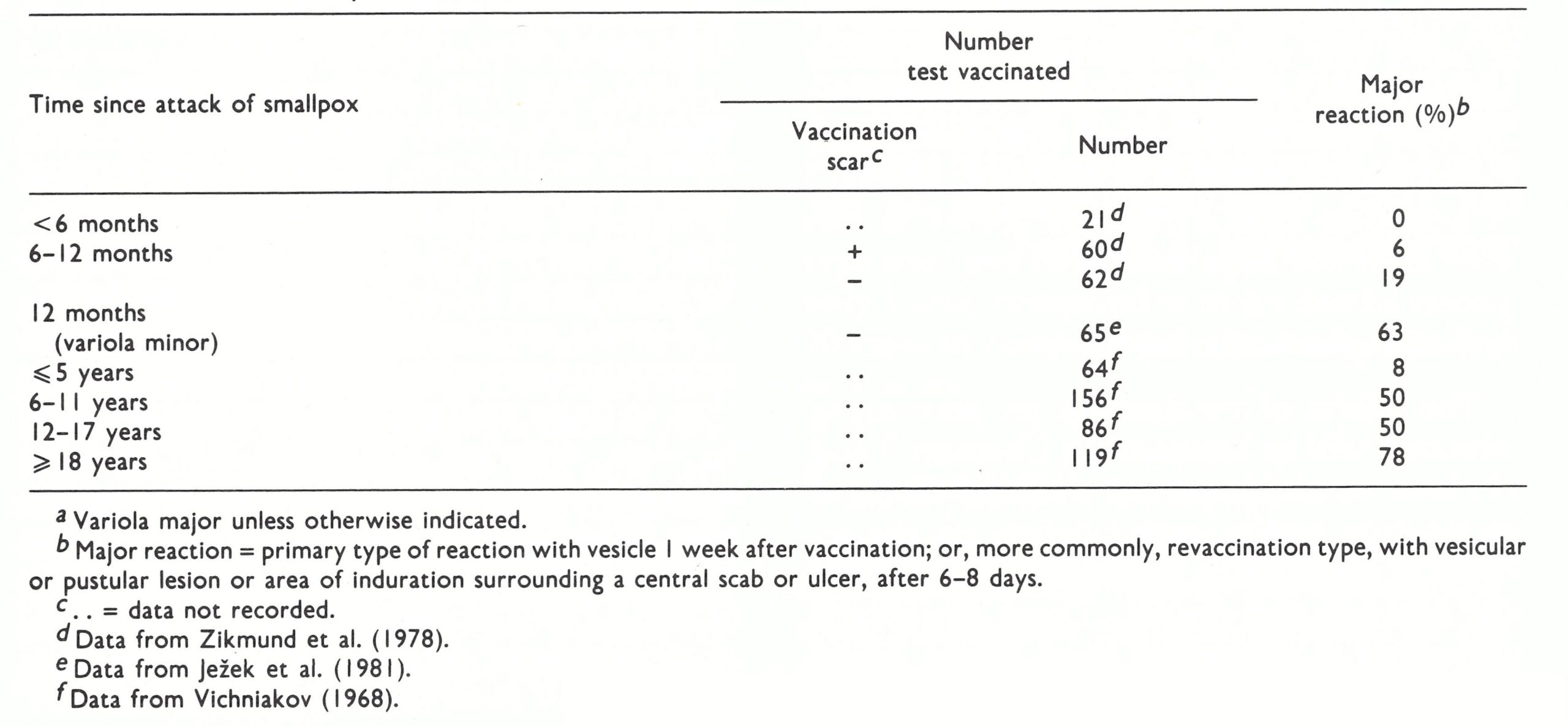
Immunity after vaccination
The effects of vaccination on preventing infection will be discussed in Chapters 7 and 11; here we are concerned with the effects of vaccination and/or revaccination on the severity of smallpox in vaccinated persons who did contract the disease. There are several difficulties in evaluating these effects. There were some patients who said that they had been vaccinated (or revaccinated) but had no scar; Rao (1972) classed these as “unsuccessfully vaccinated”. However, even in Madras some of these persons may have been successfully vaccinated, with vaccine of low potency applied over a small area of skin, leaving no scar; such misdiagnoses of vaccination status may account for the difference in prognosis between the “unvaccinated” and the “unsuccessfully vaccinated” in Rao’s data (case fatality rates in ordinary-type smallpox of 36.9% and 27.2% respectively). Among those with a vaccination scar there were other problems. First, did the scar really result from the replication of vaccinia virus in the skin? Secondary infection without viral replication could cause scars, especially when the rotary lancet was used with an unsatisfactory liquid vaccine. Secondly, how long ago did the last successful vaccination (or revaccination) occur? These questions could not always be accurately answered, but it is important to bear them in mind when considering the effects of vaccination on the prognosis of smallpox. Finally, the studies of Heiner et al. (1971a) showed that in endemic areas subclinical infection with variola virus occurred rather frequently among vaccinated persons, thus boosting their immunity.
Data published by Hanna (1913) from an outbreak of variola major in Liverpool, England, in 1902-1903, illustrate clearly the ameliorating effect of childhood vaccination on the severity of smallpox (Table 1.11). There was a striking difference between vaccinated and unvaccinated patients in all age groups, both in the spectrum of severity and in case-fatality rates. Protection waned with age—i.e., with increasing intervals since vaccination but was substantial even in those aged more than 50 years.
Rao’s data (see Table 1.2) confirm the extent of the protection against death provided by vaccination; the overall case-fatality rates in vaccinated and unvaccinated (including “unsuccessfully vaccinated”) persons in his series were 6.3% and 35.5% respectively.
Hanna’s conclusions on the duration of protection against death provided by vaccination, in those who got smallpox, is confirmed by data collected by Mack (1972), who analysed 680 cases of variola major occurring after importations of the disease into Europe and Canada during the period 1950-1971 (Table 1 .12). The case-fatality rate was 52% in unvaccinated persons, 1 .4% in those vaccinated 0-10 years before exposure, and only 11 0 o in those vaccinated over 20 years before exposure. The contrast is even more striking if only the age group 10-49 years is considered a case-fatality rate of 49% in the unvaccinated and one of 4.3% in those vaccinated over 20 years earlier.
Before 1967 it was a common practice in India, as it had earlier been in Great Britain and elsewhere, to make several insertions of vaccinia virus at adjacent sites. Early in the Intensified Smallpox Eradication Programme it was decided that vaccination should routinely be carried out on one site only (see Chapter 11), but some older data suggested that there was a correlation between protection and scar area (allowing for changes in the area with growth) and/or the number of insertions. For example, Hanna (1913) reported that the mildest attacks of smallpox occurred in those with the largest scar areas, while at all ages the average scar areas of vaccinated contacts who did not get smallpox was substantially larger than in those who did. Likewise, Rao (1972) reported a case-fatality rate of 16.4% among 79 cases of ordinary-type smallpox in persons aged 0-9 years with only 1 scar, compared with no deaths among 70 cases in comparable individuals with 2, 3 or 4 scars.
Table 1.11: Effect of vaccination in infancy on the severity and case-fatality rates in variola major, according to age groupsa
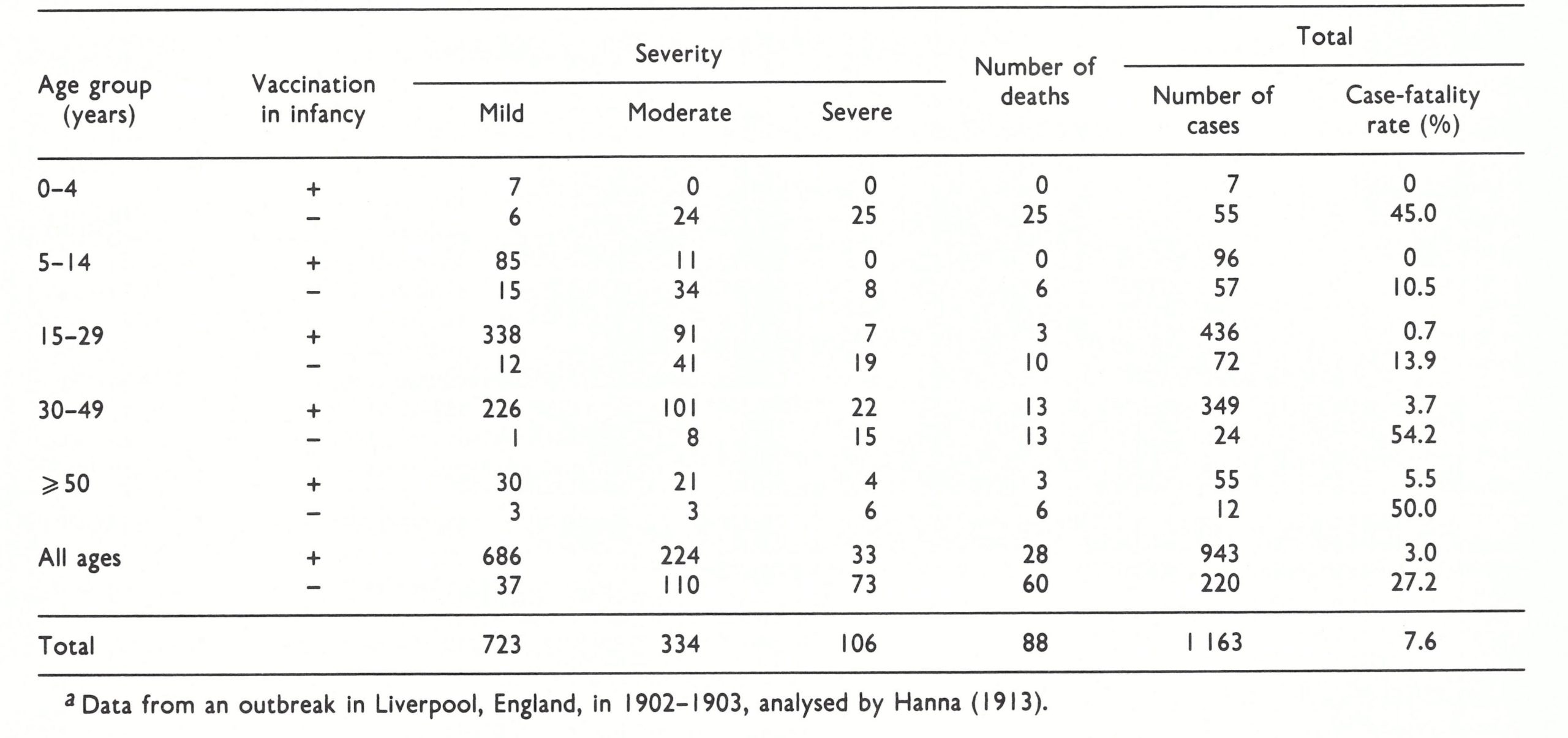
Table 1.12: Age and vaccination status of cases of variola major occurring after importations into western
countries during the period 1950-1971a
Passive immunity
Apart from reports of the deliberate use of anti-orthopoxvirus serum for serotherapy, some information has been gathered on the effects of passive immunity resulting from the vaccination of pregnant women during the incubation period of smallpox on the resistance of the fetus and the newborn child. Pregnant women were particularly susceptible to the effects of smallpox (see below), and abortion often occurred. Nevertheless, it was found that some women who had been vaccinated during the incubation period of their attack went to term and bore live babies who were usually resistant to smallpox, presumably because of passive immunization.
Table 1.13: Age-specific case-fatality rates of smallpox in unvaccinated persons in India
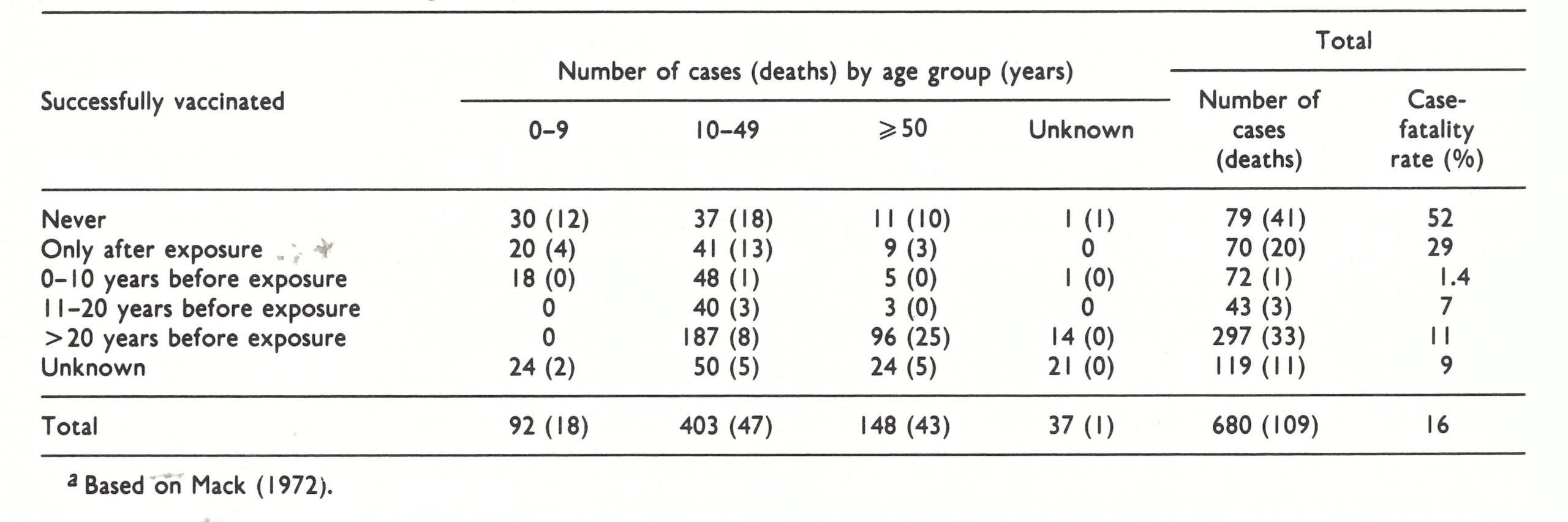
Effects of Age
Smallpox affected persons of all ages; the age incidence of the disease in endemic countries reflected the particular epidemiological characteristics of the population at the time (see Chapter 4). Some relevant data on the relation of age to prognosis in cases of variola major occurring in unvaccinated subjects are provided in Tables 1.9 and 1.11; additional statistics from India are shown in Table 1.13 and data for Pakistan are given by Mack et al. (1970). All these figures accord with the general impressions of most epidemiologists with extensive experience of smallpox and are consistent with the usual pattern of age-related susceptibility to death from acute infectious diseases (Burnet, 1952). Mortality was very high (usually over 40%) in infants, fell to its lowest level in children, and then rose with increasing age. The low case-fatality rate in unvaccinated children is significant in that the famous variolators in Great Britain during the 18th century, such as the Suttons, selected healthy children for this procedure (Razzell, 1977b), which may partly account for the low mortality it caused.
Such deaths as did occur in variola minor were predominantly in very young children. Suzart de Carvalho Filho et al. (1970) recorded an overall case-fatality rate of 0.8% in Brazil in 1968—1969, but the rate was 16.7% among patients aged less than 3 months and 2% in the age group 3—12 months (see Chapter 12, Table 12.16).
Effects of Pregnancy
It is universally agreed that smallpox was more severe in pregnant women than in nonpregnant women or in men, irrespective of vaccination status. Table 1.14 sets forth the distribution of clinical types of smallpox in Rao’s series, in pregnant and non-pregnant women and in men in the age group 15-44 years, according to vaccination status. Although pregnant women constituted only 11.6% of the series, 50% of the cases of haemorrhagic-type smallpox occurred among them, mostly in women who had been vaccinated in infancy; indeed, almost one-quarter of all cases of smallpox in pregnant women were of the haemorrhagic type. Flat-type smallpox was over twice as common among pregnant women (3.4% compared with 1.5%) whereas modified-type smallpox was less than half as frequent (9.4% with 21.2%).
The effects of smallpox on the fetus or the newborn infant were also severe (Table 1.15) but congenital smallpox was not often diagnosed among those born alive. Ten cases were recognized among the live births in Rao’s series, but because their mothers had died many infants also died within a few days of birth and it was not determined whether they had smallpox or not. Smallpox caused premature termination of the pregnancy in 75% of women who got the disease during the early weeks of pregnancy and in 60% of those who contracted it after the fetus had become viable but before it had reached full term.
Table 1.14: Distribution of principal clinical types of smallpox in pregnant and non-pregnant women and in men in the age-group 15—44 years, as related to vaccination statusa
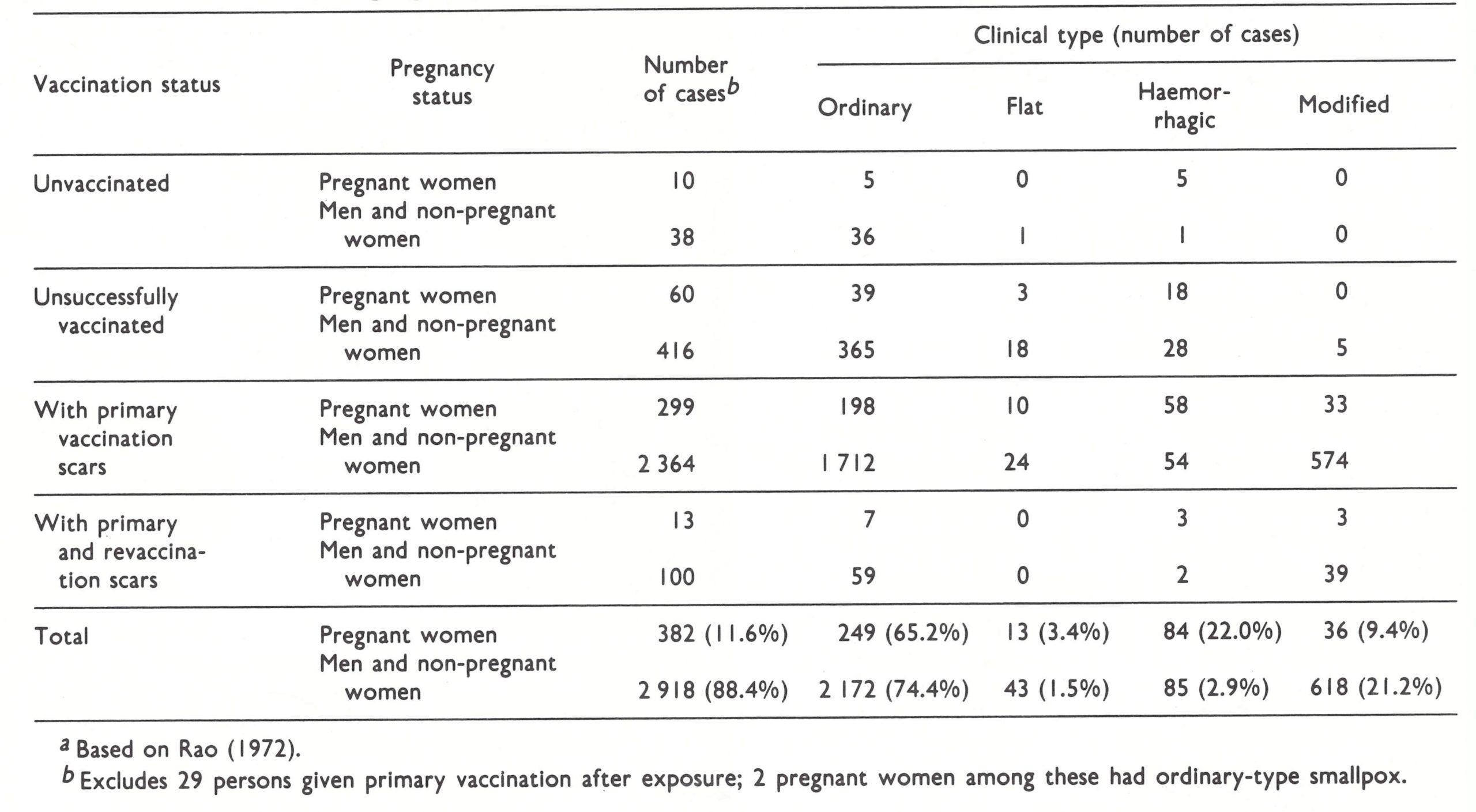
Table 1.15: The effect of smallpox on the outcome of pregnancya
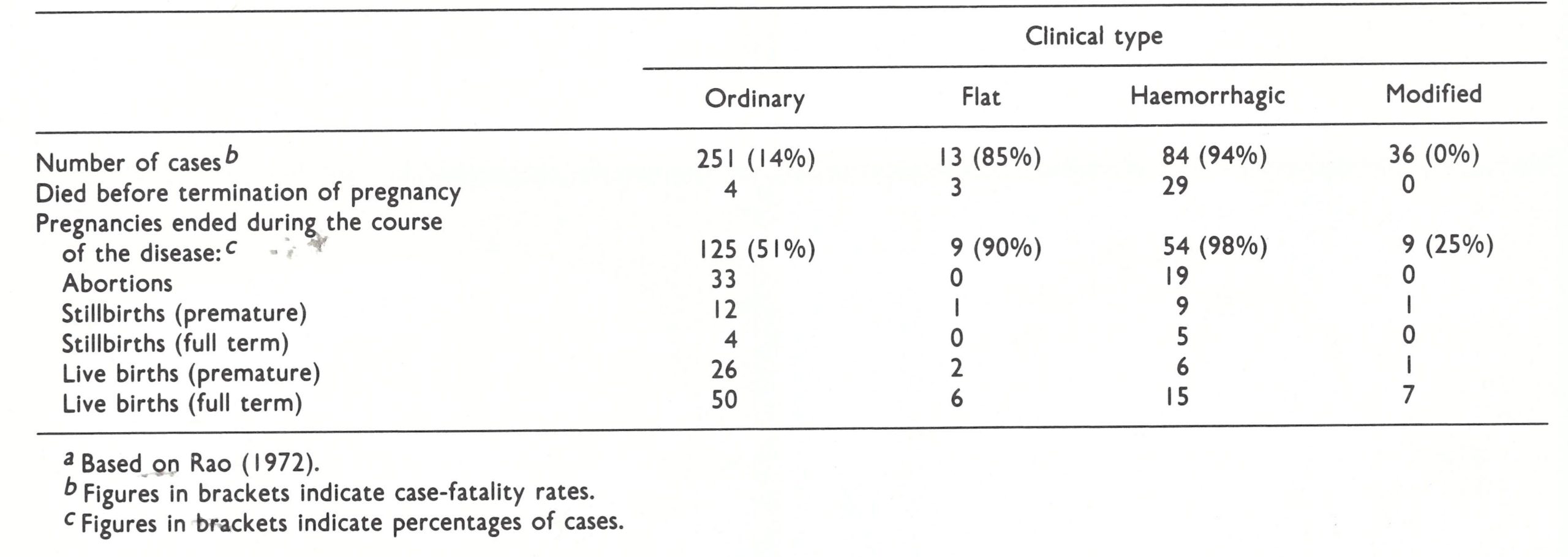
Clinical Type of Disease
Whether flat-or haemorrhagic-type smallpox developed in particular persons depended to some extent on the physiological factors just discussed, but clinical type provided much the best basis for the prognosis of individual cases. Haemorrhagic- and flat-type smallpox were almost always fatal and among cases of ordinary-type smallpox, the extent of the rash (confluent, semiconfluent or discrete) was of prognostic value. Modified-type smallpox was very rarely fatal.
DIFFERENTIAL DIAGNOSIS
The problems involved in the diagnosis of smallpox during an epidemic or in a situation in which the disease was endemic were of a different nature from those in suspected importations into non-endemic countries or regions. There were three elements in the diagnosis: clinical, epidemiological, and laboratory. No one diagnostic approach was always sufficient in itself. The clinical diagnosis of ordinary-type smallpox after the rash had developed was not difficult, and most cases were of this kind. But there were often patients in whom an accurate diagnosis could not be made on clinical grounds alone, at any rate at the first examination, early in the course of the disease. In such cases the epidemiological circumstances of the suspected case often provided a valuable lead. Nor was it wise to trust implicitly a positive report from the laboratory, if it ran counter to clinical and epidemiological evidence. Like everyone else, laboratory workers sometimes made mistakes, and clerical errors were always a possibility.
The clinical diagnosis of the great majority of cases of smallpox rested on the characteristic features of the pre-eruptive fever, the order of appearance of the rash (first on the face, then on the forearms, trunk and lower limbs), the evolution of the individual lesions, from macule to vesicle and pustule, and the appearance and feel of the vesicle and pustule. Furthermore, the lesions on any particular part of the body were all at more or less the same stage of development. The distribution of the skin lesions was also of great diagnostic value, with relatively few lesions on the trunk but many on the face and arms (more on the extensor than the flexor surfaces) and on the lower limbs, and on the palms of the hands and the soles of the feet. The major difficulties in differential diagnosis of ordinary-type smallpox arose in cases modified by vaccination, in which the lesions were often sparse and abnormal in appearance and underwent an accelerated course of evolution.
The diagnosis of flat-type smallpox was also relatively straightforward, but haemorrhagic-type smallpox, especially the early subtype and both forms in the early stages, was usually impossible to diagnose without laboratory assistance, and the diagnosis was often missed in non-endemic situations in which smallpox was not thought of by the attendant physician.
Diagnosis of smallpox in the pre-eruptive stage was impossible on clinical grounds alone, although it would have been suspected if epidemiological considerations (exposure to a known case, lack of vaccination) had been suggestive. The differential diagnosis of smallpox at this stage of the disease will therefore not be discussed here.
Ordinary-and Flat-Type Smallpox
The diseases involved in the differential diagnosis of ordinary-and flat-type smallpox were essentially those causing fever with rash.
Human monkeypox
Although a rare disease, human monkeypox ranks first among the diseases that might be confused with smallpox, because differential diagnosis was impossible on clinical grounds alone, although gross lymphadenopathy was found in most cases of monkeypox and not in smallpox (see Chapter 29). In the field, diagnosis depended on the occurrence of a disease indistinguishable from ordinary-type smallpox in the appropriate epidemiological situation: a particular geographical area (western and central Africa), no endemic smallpox, and the appropriate environmental surroundings (a small village in a tropical rain forest). Laboratory confirmation was essential, either by recovery of the virus from lesion material or retrospectively by appropriate serological tests.
Chicken monkeypox
This disease of world-wide occurrence was the single most important infection to be considered in the differential diagnosis and was particularly important in three circumstances: in countries in which variola minor was endemic, in vaccinated individuals, and in situations in which chickenpox occurred rather frequently in adults, often as a severe disease, as in several parts of India. For example, in post-eradication searches in India in 1976, 63% of the “suspected smallpox” cases were in fact cases of chickenpox (Je2ek et al.,1978e).
In the usual case of chickenpox, the nature, distribution and evolution of the rash are quite distinctive (Plate 1.28). The skin lesions in chickenpox are much more superficial than they were in smallpox. They appear in “crops” so that at any time lesions of various ages may be found on the same part of the body and their distribution is “centripetal” (denser on the trunk than the face and extremities) rather than “centrifugal”, as in smallpox.
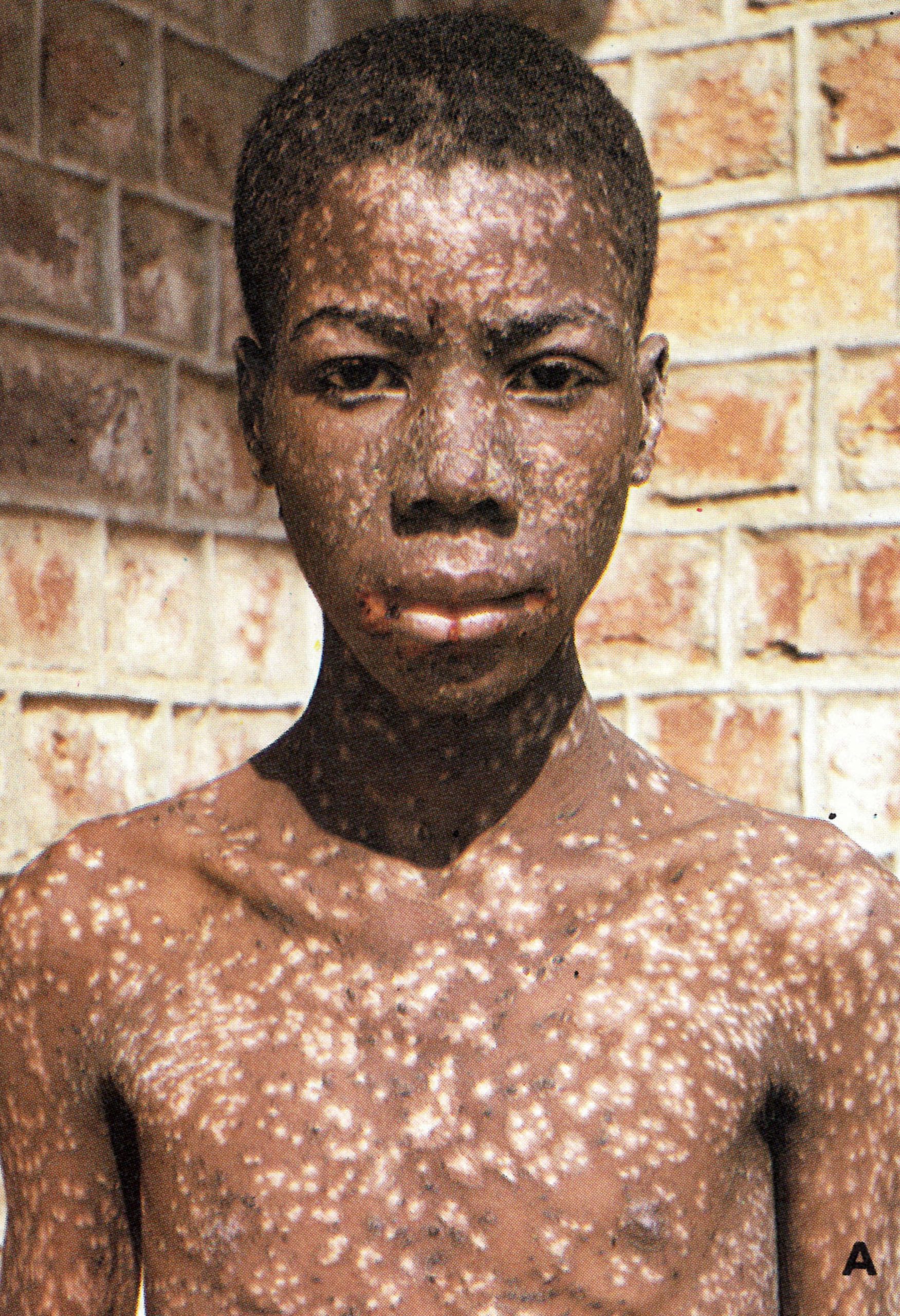



Plate1.27. Sequelae of smallpox. Shortly after recovery, the sites of pustules are usually depigmented in dark-skinned subjects (A) or red in fair-skinned subjects (B). Most cases of variola major leave facial pockmarks, which may be deeply pigmented (C); blindness is a rare complication (C and D). (B from Herrlich et al .,196.)
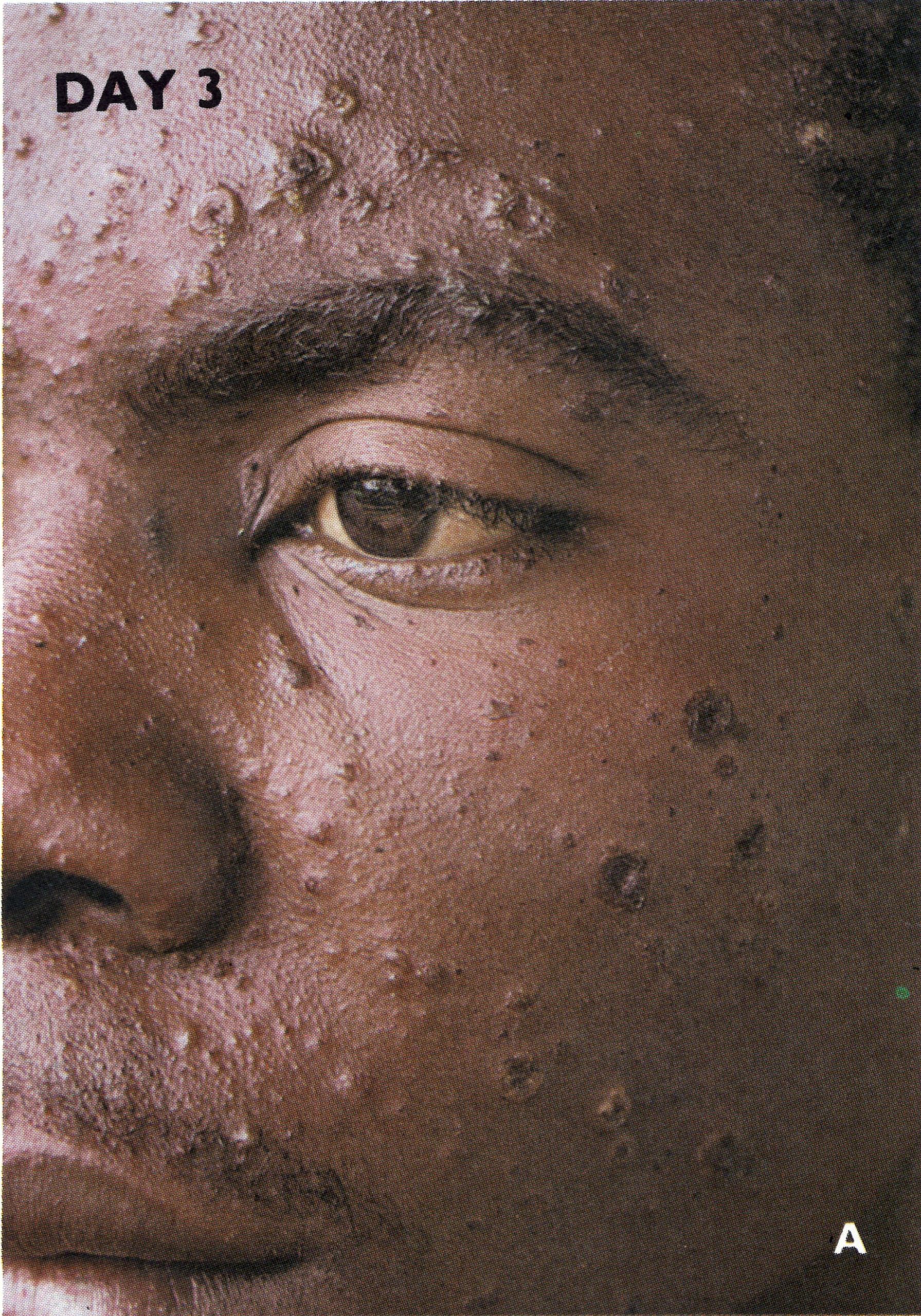

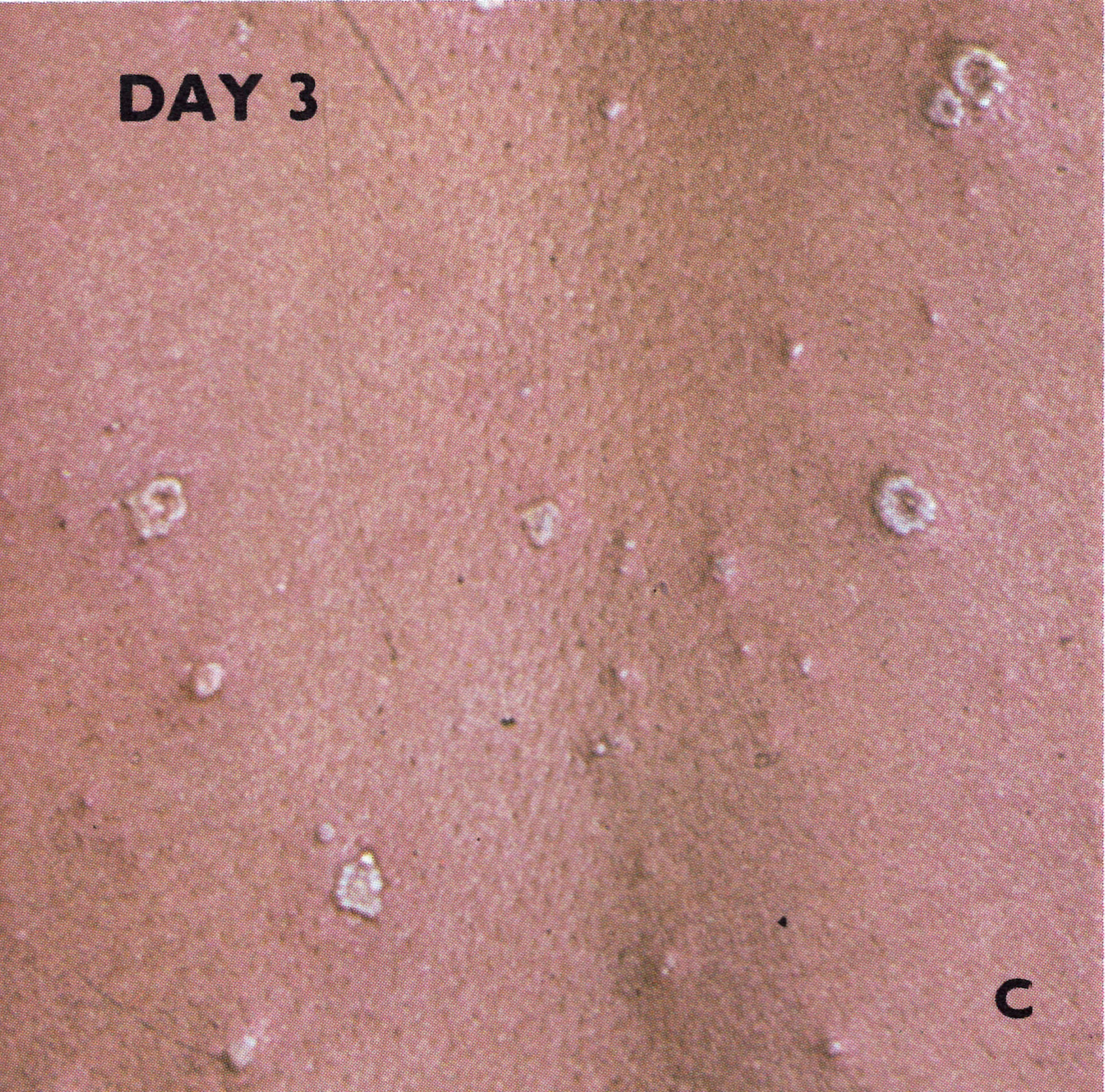
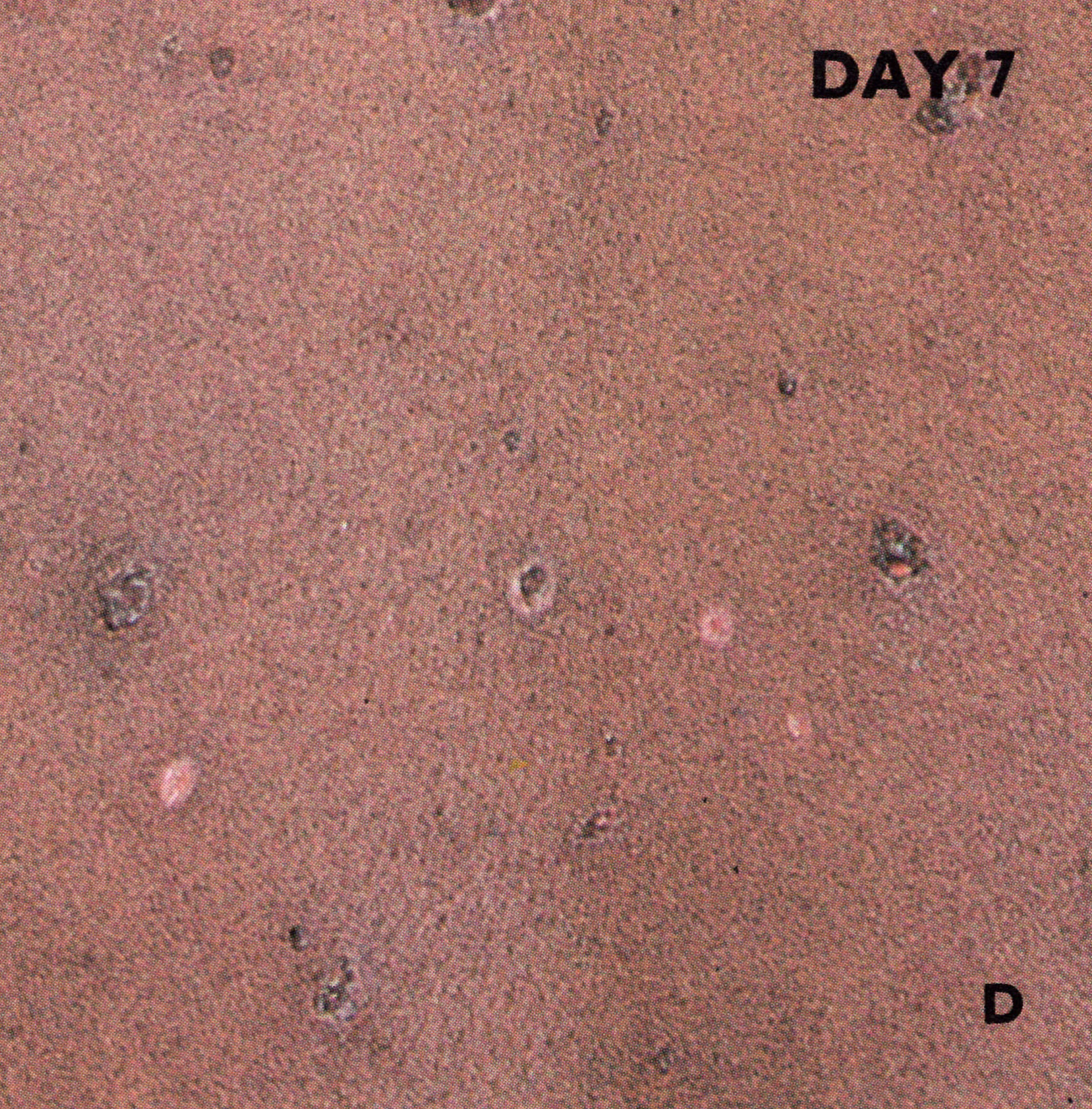
Plate1.28. Chickenpox. On the 3rd day of rash (A, B, and C) pocks are at different stages of development: papules, vesicles, pustules, and scabs. On the 7th day of rash (D) all pocks are scabbed. There are many lesions on the trunk (B) and few on the limbs.
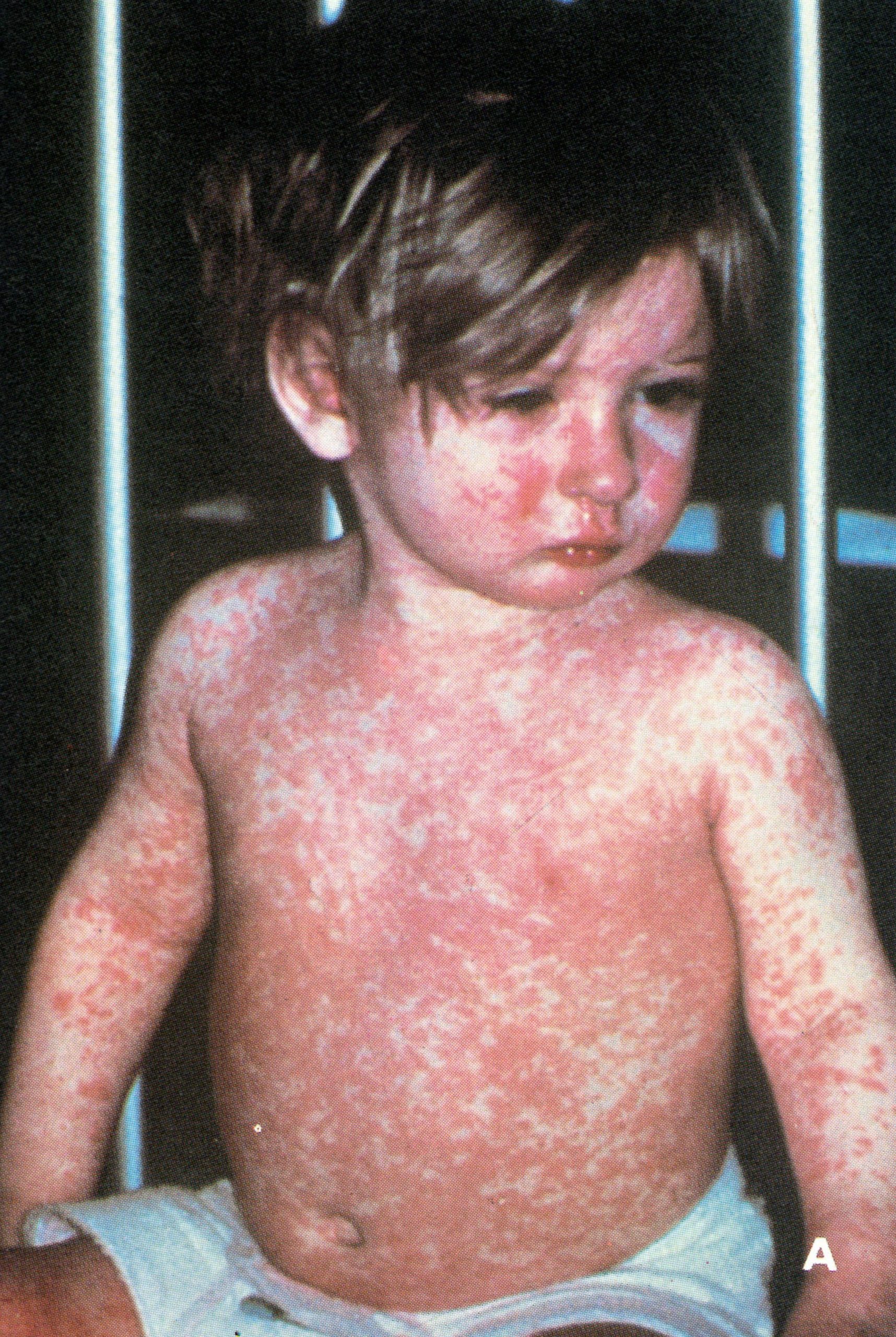

Plate1.29. A: Measles. There is a blotchy generalized rash, as well as a runny nose and sore eyes. B: Secondary syphilis. The rash had a different distribution from that of smallpox, did not feel “shotty” and did not progress to pustules and scabs as in smallpox. (From Lambert & Farrar, 1982). C: Erythema multiforme. (B from Herrlich et al .,196.)



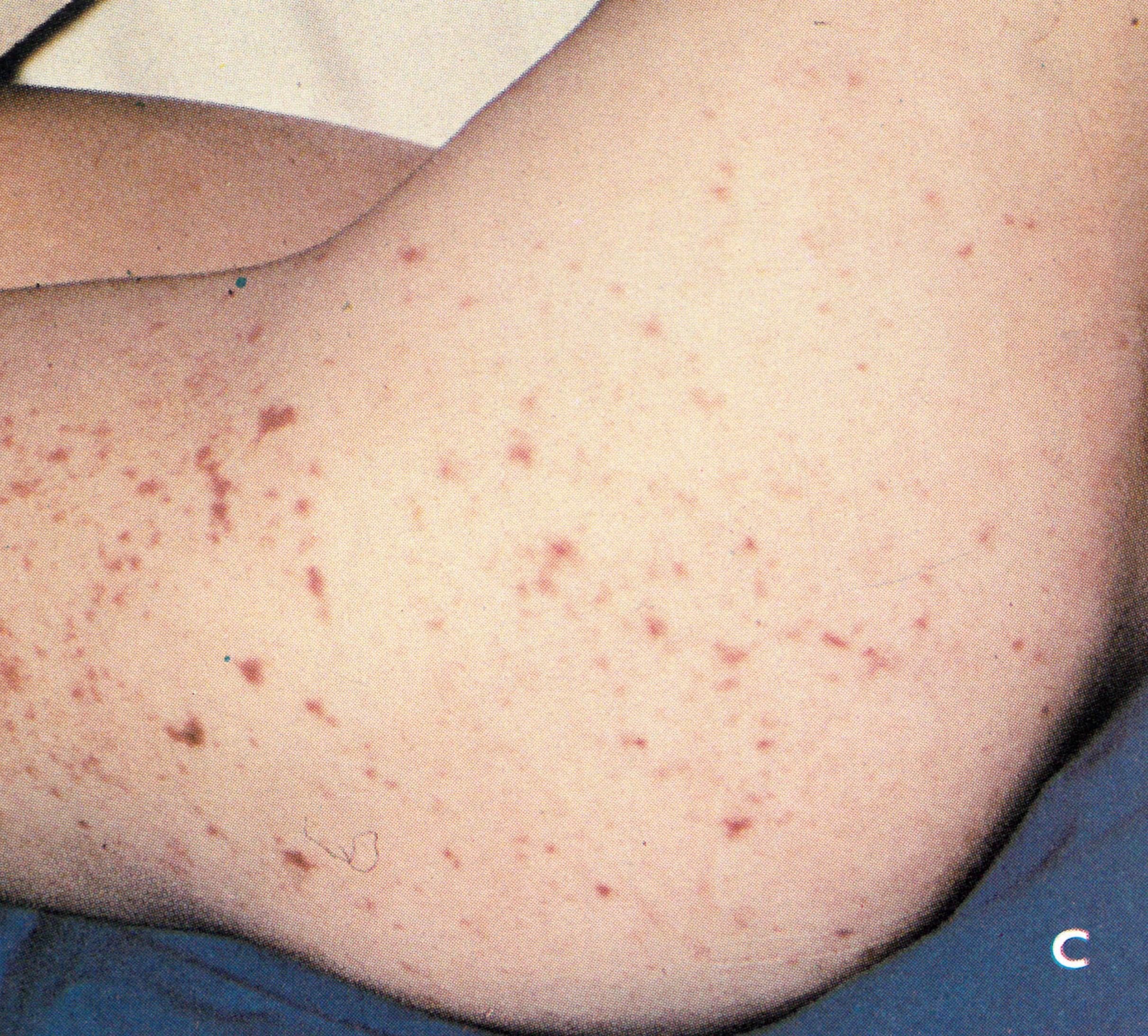

Plate 1.30. A and B: Drug eruptions, which sometimes occurred in patients with smallpox. C and D: Meningococcal septicaemia, which could be difficult to differentiate from early haemorrhagic-type smallpox. (B, C, D from Lambert & Farrar, 1982.)
Difficulties arose with severe chickenpox in adults (White, 1978), a disease found especially in some parts of India (Kerala, Tamil Nadu (formerly Madras State), and West Bengal). Indeed, some severe cases of chickenpox in adults were associated with such an extensive rash, including lesions on the palms and soles, that it was impossible to be certain at any stage of the disease as to whether it was chickenpox or smallpox. During the eradication programme, all such cases were regarded as smallpox and appropriate control measures were undertaken. Sometimes the lesions in this type of chickenpox were haemorrhagic, and it was in these cases that the rate of development of the rash and its distribution were important diagnostic features.
Such severe cases of chickenpox have always been rare. Diagnostic problems occurred more frequently between attacks of chickenpox of ordinary severity and mild, particularly vaccine-modified, attacks of smallpox. In vaccine-modified smallpox the lesions were often superficial, not “shotty”; they dried up quickly with a small scab and left scars very little different from those of chickenpox. Differential diagnosis was often impossible on clinical grounds alone; laboratory confirmation was essential.
Since they had the same seasonal incidence, smallpox and chickenpox might sometimes have been expected to occur concurrently in the same patient. Sarkar et al. (1976) report 3 such cases from a refugee camp near Calcutta in 1972, in males aged 15, 30 and 60 years respectively, all with vaccination scars. All the patients survived, the clinical course of each disease being unaffected by the other. The diagnosis of smallpox was confirmed in every case by the examination of material from variola-like lesions, and varicella virus was detected by electron microscopy in vesicle fluid from a chickenpox-like lesion in the one case that was examined by this technique.
Tamapox
This poxvirus disease occurs as a zoonosis in parts of Kenya and Zaire, and probably elsewhere in Africa (see Chapter 29). The lesions are usually single, and few in number if they are multiple. They are nodular rather than pustular and evolve much more slowly than the lesions of smallpox. However, when first seen, such lesions could be confused with those of mild smallpox in a vaccinated subject. The slow course and absence of pustulation would subsequently clarify the diagnosis. Electron microscopic examination of lesion material reveals virions similar to those of variola virus. However, tanapox cannot be cultivated on the chorioallantoic membrane.
Measles
In the first 2 days of the rash, before vesicles developed, the most likely cause of confusion was measles (Plate 1.29A), and this difficulty could persist for several more days in flat-type smallpox, although the severity of this disease was much greater than that of measles. The presence of Koplik’s spots was, of course, diagnostic of measles, and in any case the difficulty disappeared as the rash evolved. Historically, measles did not present a problem in countries with endemic smallpox, but in non-endemic countries an early case of smallpox was sometimes diagnosed as measles, with possibly serious consequences in terms of secondary cases. On the other hand, in countries in which smallpox was endemic, physicians were often prone to diagnose all outbreaks of rash associated with deaths as smallpox and to report them as such to the health authorities. Some of these outbreaks later proved to be due to measles.
Syphilis
Earlier writers, e.g., Councilman (1907) and Ricketts (1908), paid considerable attention to syphilitic rashes as presenting a problem in differential diagnosis. With the advent of penicillin and the consequent reduction in the incidence of syphilis especially of secondary syphilis-in the developed countries, the disease has ceased even to be mentioned by writers, such as Christie (1980), dealing with the general domain of infectious diseases. However, in African countries and India secondary syphilis remained a disease to be considered in the differential diagnosis of smallpox, up to the time of eradication. The roseolar and papular syphilitic rashes (Plate 1.29B) varied in size and distribution and felt different from those of smallpox. The individual lesions were sometimes hard, but they could not be rolled between the thumb and forefinger, to give the “shotty” feel characteristic of the smallpox vesicle. Neither could they be “split” by passing a needle horizontally through the lesion, as could the vesicles of smallpox. The distribution was also different; if there were a profuse rash on the face, there would also be an equally dense rash on the chest and abdomen and the toxaemia would have been too slight for a case of smallpox with such a rash. Finally, the diagnosis would be clinched by the fact that the papules of syphilis did not evolve further, to vesicles and pustules, like those of smallpox.
Erythema multiforme
This disease (Plate 1.29C) could cause difficulties at any stage of the rash; the distribution of lesions is sometimes very like that of smallpox. In both diseases the patient could be quite ill and have a profuse vesicular eruption particularly affecting the extremities. However, the history is completely unlike that of smallpox: the onset of symptoms and rash tend to coincide, and the rash evolves very rapidly to the vesicular stage. Further, erythema multiforme is almost always accompanied by stomatitis, and often by conjunctivitis and urethritis.
In severe cases there could be confusion with flat-type smallpox, since the vesicles were occasionally soft, superficial and flat, individually resembling those of flat-type smallpox. They sometimes coalesced and produced large bullae, also seen in some cases of severe smallpox. The degree of malaise was usually not like that seen in flat-type smallpox, where the patient at this stage had only about 48 hours to live, but the most important difference was in the speed of evolution of the rash in the two diseases. In smallpox with this skin picture, the patient would have been ill and getting progressively worse for at least 10 days and the vesicular eruption would have only just fully emerged; in erythema multiforme the rash develops with the onset of constitutional symptoms and evolves rapidly to the vesicular stage.
Lesions due to vaccination
Generalized vaccinia, described in Chapter 7 (see Plate 7.7), rarely caused confusion; the history of vaccination and the nature and distribution of the rash differed substantially from what was found in smallpox. However, problems of precise diagnosis sometimes arose in smallpox contacts who had been vaccinated during what turned out to be the incubation period of smallpox. They usually showed a positive take at the vaccination site and often a modified rash, which could have been caused by variola or vaccinia virus. Operationally, all such cases were regarded as smallpox from the point of view of management. Precise diagnosis could be made by the culture of virus from several of the vesicles or pustules.
Drug eruptions
Although less important in countries in which smallpox was still endemic, drug eruptions (Plate 1 .30A and B) were an important diagnostic problem in countries in which smallpox had been eradicated years before and doctors rarely considered the possibility of the disease. Many instances exist in which the rash of an imported case of smallpox, and sometimes the rashes of second-generation cases deriving from it, were diagnosed as drug rashes, since the sick patients had customarily been treated with some kind of drug for the pre-eruptive fever. The diagnosis usually became quite clear with the passage of time and the evolution of the rash, but vaccine-modified smallpox could continue to mislead the physician if he had never considered smallpox as a possible diagnosis.
In endemic countries in recent years, since a wide variety of drugs have become available, cases of smallpox and drug eruption sometimes occurred coincidently. Rao (1972) described a case in which the drug rash completely obscured that due to smallpox and the diagnosis was only made when variola virus was recovered from some “seeds” extracted from the palms of the hands.
Rashes due to other causes
There are few diseases characterized by a rash that did not at some time suggest a diagnosis of smallpox, occasionally with dramatic effect in non-endemic countries. Acne, scabies and insect bites may be mentioned as examples. Coxsackievirus infections could pose a problem (Mukherjee et al.,1976), and in countries in which both diseases were endemic, dengue haemorrhagic fever and other arbovirus infections associated with a rash were sometimes initially diagnosed as smallpox.
Haemorrhagic-Type Smallpox
Haemorrhagic-type and flat-type smallpox were sometimes associated with a severe shock-like condition, loss of muscle tone and a peculiar state of apprehension and mental alertness that were said to be unlike the manifestations of any other infectious disease. The occurrence of a petechial rash, especially in the groin and along the flanks to the axillae, was regarded as diagnostic of smallpox, since other forms of febrile purpura, due to meningococci or other organisms, did not have such a localized and symmetrical distribution; but an accurate diagnosis was impossible without laboratory aid. The literature on outbreaks following the importation of smallpox into non-endemic countries (see Chapter 23) is replete with instances in which the index case or sometimes a first-generation case, presenting as an acutely fatal case of haemorrhagic-type smallpox, was almost always misdiagnosed as meningococcal septicaemia (Plate 1.30C and D) or acute leukaemia. However, meningococcal bacteraemia is usually more rapidly lethal than was haemorrhagic- type smallpox; acute leukaemia is less rapid.
Erythematous rashes on the face and later on the arms and trunk sometimes suggested the diagnosis of toxic scarlet fever, but the early rash in haemorrhagic-type smallpox was a diffuse not a punctate erythema, the temperature was lower than in severe scarlet fever and the tongue and fauces were practically normal.
Even in endemic areas, and at times when variola major was a common disease, it was very difficult to diagnose very severe smallpox, whether of the haemorrhagic or of the flat type, in its early stages. It can be readily understood why the diagnosis was so often missed in non-endemic countries.
Table 1.16: Alternative diagnoses is suspected but unfonfirmed cases of smallpox
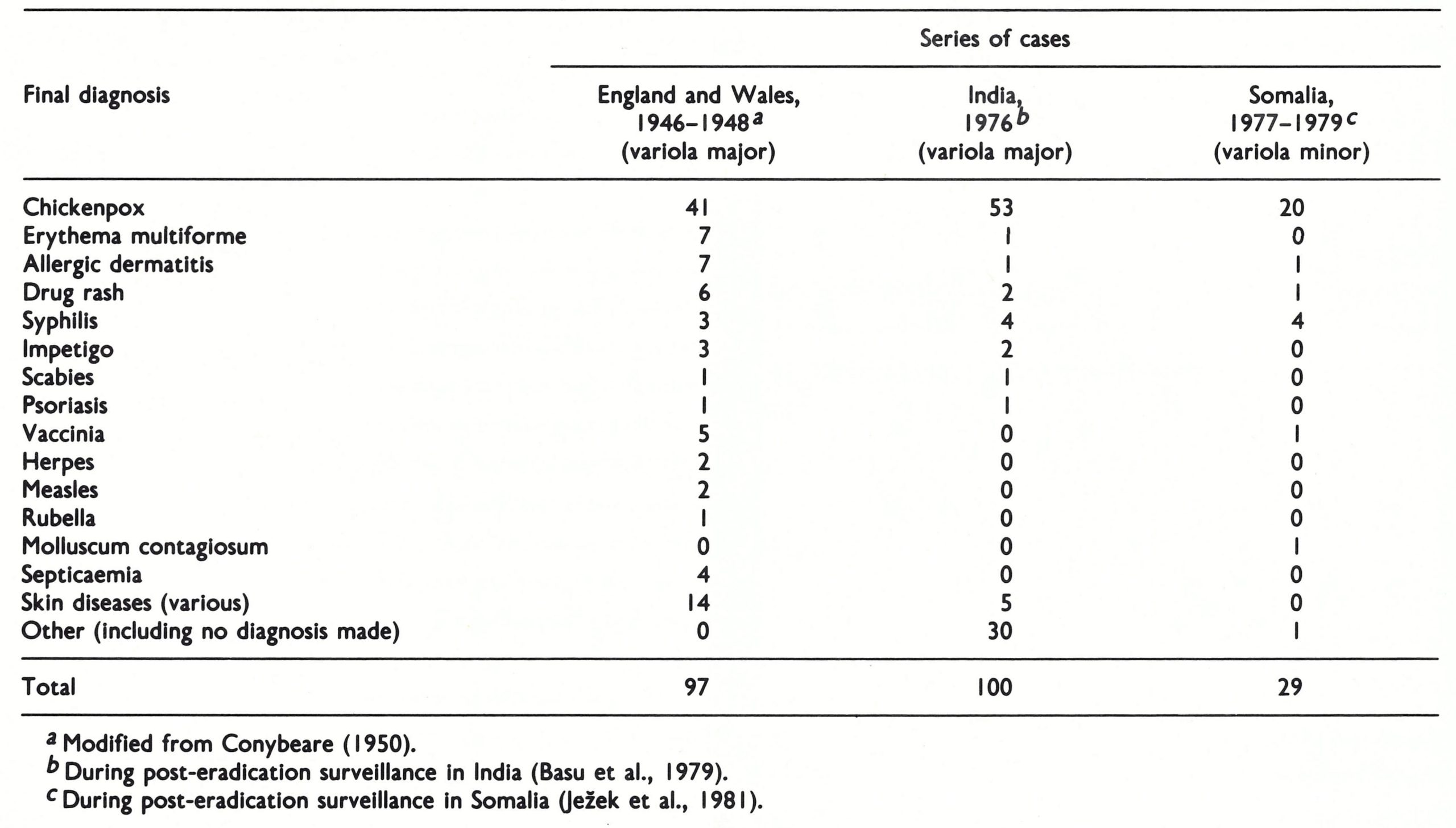
Effects of Prior Vaccination on Symptomatology
From the diagnostic point of view, it was important for physicians to appreciate that there was great individual variation in the extent to which vaccine immunity persisted. The person presenting with symptoms suggestive of flat-type smallpox, who had had a successful primary vaccination within 5 years, was unlikely to be suffering from this disease; the probability of another diagnosis should therefore have been seriously considered. On the other hand, the presence of signs or symptoms suggestive of a very mild attack of smallpox should not have led the doctor to discount the diagnosis even in the face of an apparently successful vaccination within a year. It was also important to remember that exceedingly mild smallpox, even variola sine eruptione, could occur in persons who had no evidence of ever having been successfully vaccinated.
Alternative Diagnoses
Several authors have summarized alternative diagnoses that have been made in suspected but unconfirmed cases of smallpox. Table 1.16 lists final diagnoses made in cases of suspected smallpox in situations in which variola major was the expected form of the disease (England and Wales, 1946-1948; India, 1976) and in those in which the endemic disease was variola minor (Somalia, 1977-1979). The overriding importance of chickenpox is apparent in all series. Marsden (1936) also reported that chickenpox was by far the commonest disease to be initially mistaken for variola minor in England (31 of 994 cases of suspected but unconfirmed smallpox). Other conditions suspected to be smallpox included almost all diseases that produced a rash.
LABORATORY CONFIRMATION OF SMALLPOX DIAGNOSIS
Laboratory methods played a crucial role in the global smallpox eradication programme; indeed, eradication could not have been confidently certified to have been achieved without their use. A detailed historical description of the laboratory methods used for the diagnosis of smallpox is presented in Chapter 2 and an account of the development of laboratory support for the Intensified Smallpox Eradication Programme is given in Chapter 10.
As well as being of critical importance in the global smallpox eradication programme, laboratory methods were also useful for the confirmation of clinical diagnoses. Indeed, although laboratory workers could make mistakes, the recovery of variola virus from a skin lesion was usually regarded as conclusive evidence that a particular patient was or had been suffering from smallpox. Such confirmation was rarely sought in endemic countries when smallpox was a common disease. Any doubtful case was always regarded as smallpox; containment and vaccination procedures operated independently of and were initiated before laboratory confirmation. However, laboratory confirmation or refutation of suspected smallpox was a valuable procedure in non-endemic countries and in smallpox-free regions of the endemic countries as eradication approached.
If an electron microscope was available, the examination of material from vesicles, pustules or scabs, examined by the negative staining technique, could give a rapid presumptive diagnosis of poxvirus, or sometimes herpesvirus, infection. Definitive diagnosis depended on the isolation of the causative virus on the chorioallantoic membrane of the developing chick embryo and its further characterization, if necessary, by biological tests. Usually, the character of the pocks produced on the chorioallantoic membrane was distinctive enough for the diagnosis of variola, vaccinia, monkeypox or herpesvirus infection to be made (see Chapter 2).
In the period before the Intensified Smallpox Eradication Programme was launched, gel-precipitation tests were employed extensively in some national programmes (e.g., in India; Basu et al.,1979), and by laboratories that did not have an electron microscope. With adequate amounts of recently collected vesicle fluid it was an accurate and rapid test (World Health Organization, 1969a; A.W. Downie, personal communication, 1981), and when anti-varicella serum was employed in parallel tests it could be used to differentiate smallpox from chickenpox (Brunell et al.,1971; A.R. Rao, personal communication, 1981).
TREATMENT: PROPHYLACTIC AND CURATIVE
No disease better illustrated the adage “Prevention is better than cure” than smallpox. Nevertheless, until 1975 millions of persons were infected with variola major virus and, as the foregoing description of its clinical features bears witness, it was a horrible disease with a high case-fatality rate. Any treatment that would ameliorate the severity of the disease in those who were infected would have been welcomed.
In this section, treatment administered after exposure and thus during the incubation period is called “prophylactic” and treatment given after the development of symptoms is “curative”. Three procedures were used or investigated: vaccination after exposure, immunoprophylaxis and immunotherapy, and chemoprophylaxis and chemotherapy.
Vaccination during the Incubation Period
The sheet anchor of smallpox control during the Intensified Smallpox Eradication Programme was surveillance and containment (see Chapter 10). Containment was possible because vaccination provided protection against infection for those who had not already been infected with variola virus. However, vaccination must also be discussed as a form of prophylactic treatment, for it also modified the progress of the disease in persons vaccinated during the first few days of the incubation period. The precedent for this concept was Pasteur’s demonstration of protection against rabies by vaccination during the incubation period. The different timescales of the pathogenesis of vaccinia and variola (see Fig. 1.3 and Fig. 3.1 of Chapter 3) provided hope that such prophylactic treatment, if carried out during the first week of the incubation period of smallpox, might ameliorate or sometimes abort the disease. Precise data were difficult to obtain, because it was rarely known whether or when a contact had actually been infected with variola virus. Unless sophisticated serological tests had been carried out (and this was never done) it would have been impossible to differentiate between a person sustaining only vaccination and one who had also been incubating smallpox but in whom that infection had produced no symptoms. However, all observers agree that persons in whom smallpox developed a week or more after primary vaccination often had a modified attack. Dixon (1962) summarized his review of the older literature by saying that “at least 50 % of cases where successful primary vaccination had occurred during the first week [of the incubation period] will get some vaccine-modification and reduction of severity, whereas when done at a later period the number showing such modification is not likely to be over 20%”. In fact, on theoretical grounds the degree of modification might be expected to be highly dependent on the exact timing of infection with variola virus and vaccination; the more nearly these corresponded, the greater was the degree of protection. Without distinguishing the timing of primary vaccination, Rao (1972) observed a frequency of modified-type smallpox of 8.8% among those given primary vaccination after exposure, compared with 1.0% among unvaccinated patients.
Successful revaccination would have been expected to be even more effective, because of the accelerated immune response.
Immunoprophylaxis and Immunotherapy
Although the procedure was rendered superfluous by the development of effective measles vaccines, measles could be aborted or ameliorated by the administration of immune gamma-globulin during the first 7 days of the incubation period (Janeway, 1944). During the 1960s some experimental work was carried out in animals (see Chapter 3), and a few trials were made in human beings, to determine whether immunoprophylaxis or immunotherapy might be useful in smallpox .
The most comprehensive trials were carried out in Madras (Kempe et al.,1956, 1961). Immune gamma-globulin, prepared from the serum of recently vaccinated adults (not smallpox convalescents) was administered to close contacts of smallpox cases, most of whom were also vaccinated or revaccinated at the same time. The results of these and other trials (Marennikova, 1962), summarized in Table 1.17, indicate that if given during the incubation period vaccinia-immune gamma globulin provided protection additional to that expected from vaccination at that time. The greater potency against variola virus of homologous antiserum from smallpox convalescents (Downie & McCarthy, 1958; Downie et al.,1961 b) might have been expected to give even better results, but no trials were ever made with such sera. In any case vaccinia immune or variola-immune gamma-globulin were available in such small quantities that they could only have been used in unusual situations. However, vaccinia-immune gamma-globulin did appear to have a place in the prevention and treatment of vaccination complications in some especially susceptible individuals (see Chapters 7 and 11).
Table 1.17: Alternative diagnoses is suspected but unfonfirmed cases of smallpox

Chemoprophylaxis and Chemotherapy
It is not surprising that orthopoxviruses, being the largest and most complex viruses, were among the first for which antiviral agents were developed that were effective in inhibiting viral replication in cells (see Chapter 2). Some of these drugs also had activity against orthopoxvirus infections in mice and they were subsequently tested for the treatment and chemoprophylaxis of smallpox. The results were disappointing, in that none was effective in treatment, and chemoprophylaxis was of marginal value only and did not compare in effectiveness with the vaccination of contacts.
A Comment on Chemoprophylaxis in Smallpox
"The major drawback to routine use of the drug [metisazone] is the frequency of often severe nausea and vomiting which occurs in not less than 25% and more often in two thirds or more. In presently endemic countries, use of the drug is wholly impractical, not only in terms of acceptance on the part of the population, but because of the logistics involved in giving it. It has been difficult enough to persuade health administrators of the need for immediate investigation and control of all outbreaks and even more difficult to establish the mechanics for doing this properly. Use of methisazone would require not only administration of the drug but repeat visits to determine whether vomiting had occurred and, if necessary, repeat administration of the drug. This cannot be considered.
"In the non-endemic developed countries, one could more easily cope with the logistics of administration. It is noted, however, that vaccinia immune globulin has been shown to have a protective efficacy of the same order of magnitude as methisazone but without the associated toxic side effects." (D.A. Henderson, unpublished report, December 1970.)
My infection seems to have been a case of 'contact fever', a condition which had been recognized as occurring in fully vaccinated individuals many years ago. One of the sisters and the physician attending this patient developed a similar illness also, in spite of vaccination immediately after the diagnosis was made."
Thiosemicarbazones for chemotherapy
The effectiveness of certain thiosemicarbazones in the treatment of tuberculosis led to the demonstration by Hamre et al.(1950) that some thiosemicarbazones reduced the mortality of mice inoculated with vaccinia virus. This led to the testing by pharmaceutical companies of many different thiosemicarbazones, two of which (N-methylisatin β- thiosemicarbazone (metisazone (methisazone)) and 4-bromo-3-methylisothiazole-5- carboxaldehyde thiosemicarbazone (M & B 7714)) appeared to be particularly effective against variola in mice (Bauer & Sadler, 1960; Rao et al.,1965). Clinical trials for the treatment and prophylaxis of smallpox were carried out in Madras (see reviews by Bauer (1972) and Rao (1972)).
Both drugs were only slightly soluble and were given as tablets or as a micronized preparation in syrup. The main side effects were nausea and vomiting, which were sometimes severe. Rao et al. (1966a, 1969b) carried out double-blind trials of both thiosemicarbazones (Table 1.18). The only apparent differences between the treated and control groups were small reductions in the already low case fatality rates in vaccinated subjects. However, analysed, there were no significant differences in case-fatality rates between the unvaccinated treated subjects and the controls; nor were there any significant differences in symptomatology among the small number of cases of ordinary-type smallpox whom it was possible to treat as early as the 5th day of disease (2nd day of rash).
Thiosemicarbazones for chemoprophylaxis
Clearly, these thiosemicarbazones were useless for the treatment of smallpox. However, Bauer et al. (1963) had claimed impressive results in chemoprophylaxis with metisazone in a trial in Madras. Most of the case contacts had been vaccinated during infancy and again shortly after detection of the index cases. Among 1100 subjects treated with metisazone there were 3 cases of smallpox and no deaths. Of 1126 controls not given the drug, 78 developed smallpox and 12 died. The result was hailed enthusiastically:”…if further experience of this substance leads to equally favourable conclusions, the work… will perhaps rank as the most significant advance in smallpox control since the days of Jenner” (Lancet, 1963). Such a comment was perhaps pardonable in Great Britain at a time when there were rather frequent importations of variola major from the Indian subcontinent. Statements in the Indian press, such as “at last a drug has come to replace the much-dreaded vaccination” (quoted by Rao, 1972), were more serious in their implications for the control and eradication of smallpox.
There were major defects in the design of this trial: treatment and control groups were not allocated at random, contacts were not visited daily, and assessment of the taking of the drug (which caused nausea and vomiting) was made by questioning at a second visit 2 weeks after supplies of it had been distributed. Further trials with metisazone gave variable but mostly favourable results, which are summarized in Table 1.19. Rao et al. (1966b) reported a less favourable but still significant result with unvaccinated contacts given M&B 7714 as a chemoprophylactic drug.
The overall conclusion is that given prophylactically, metisazone did exert some protective effect, but its administration was often associated with severe nausea and vomiting. Health administrators considered its use in countries in which smallpox was still endemic in the late 1960s and early 1970s as “wholly impractical” (see box) in terms of acceptability by the populations concerned and the logistics of administering it. In non-endemic countries, these difficulties would be less serious but in these situations’ vaccinia-immune globulin, which had a protective effect of the same magnitude as metisazone, without toxic side effects, was available. Prompt vaccination or revaccination of contacts remained the sheet anchor of prophylaxis until smallpox was finally eradicated.
Thiosemicarbazones for chemotherapy
The effectiveness of certain thiosemicarbazones in the treatment of tuberculosis led to the demonstration by Hamre et al. (1950) that some thiosemicarbazones reduced the mortality of mice inoculated with vaccinia virus. This led to the testing by pharmaceutical companies of many different thiosemicarbazones, two of which (N-methylisatin β-thiosemicarbazone (metisazone (methisazone)) and 4-bromo-3-methylisothiazole-5- carboxaldehyde thiosemicarbazone (M & B 7714)) appeared to be particularly effective against variola in mice (Bauer & Sadler, 1960; Rao et al., 1965). Clinical trials for the treatment and prophylaxis of smallpox were carried out in Madras (see reviews by Bauer (1972) and Rao (1972)).
Both drugs were only slightly soluble and were given as tablets or as a micronized preparation in syrup. The main side effects were nausea and vomiting, which were sometimes severe. Rao et al. (1966a, 1969b) carried out double-blind trials of both thiosemicarbazones (Table 1.18). The only apparent differences between the treated and control groups were small reductions in the already low case fatality rates in vaccinated subjects. However, analysed, there were no significant differences in case-fatality rates between the unvaccinated treated subjects and the controls; nor were there any significant differences in symptomatology among the small number of cases of ordinary-type smallpox whom it was possible to treat as early as the 5th day of disease (2nd day of rash).
Cytosine arabinoside
In an uncontrolled trial in Bangladesh, Hossain et al. (1972) reported promising results with cytosine arabinoside in the treatment of variola major. However, subsequent controlled studies in both variola major (Monsur et al.,1975) and variola minor (Dennis et al.,1974) provided no evidence of any effect on either the mortality (in variola major) or the clinical progression of the disease. Nor was the related drug, adenine arabinoside, of any use (Koplan et al .,1975).
Table 1.18: Case-fatality rates in patients treated with either of two thiosemicarbazones and placebos
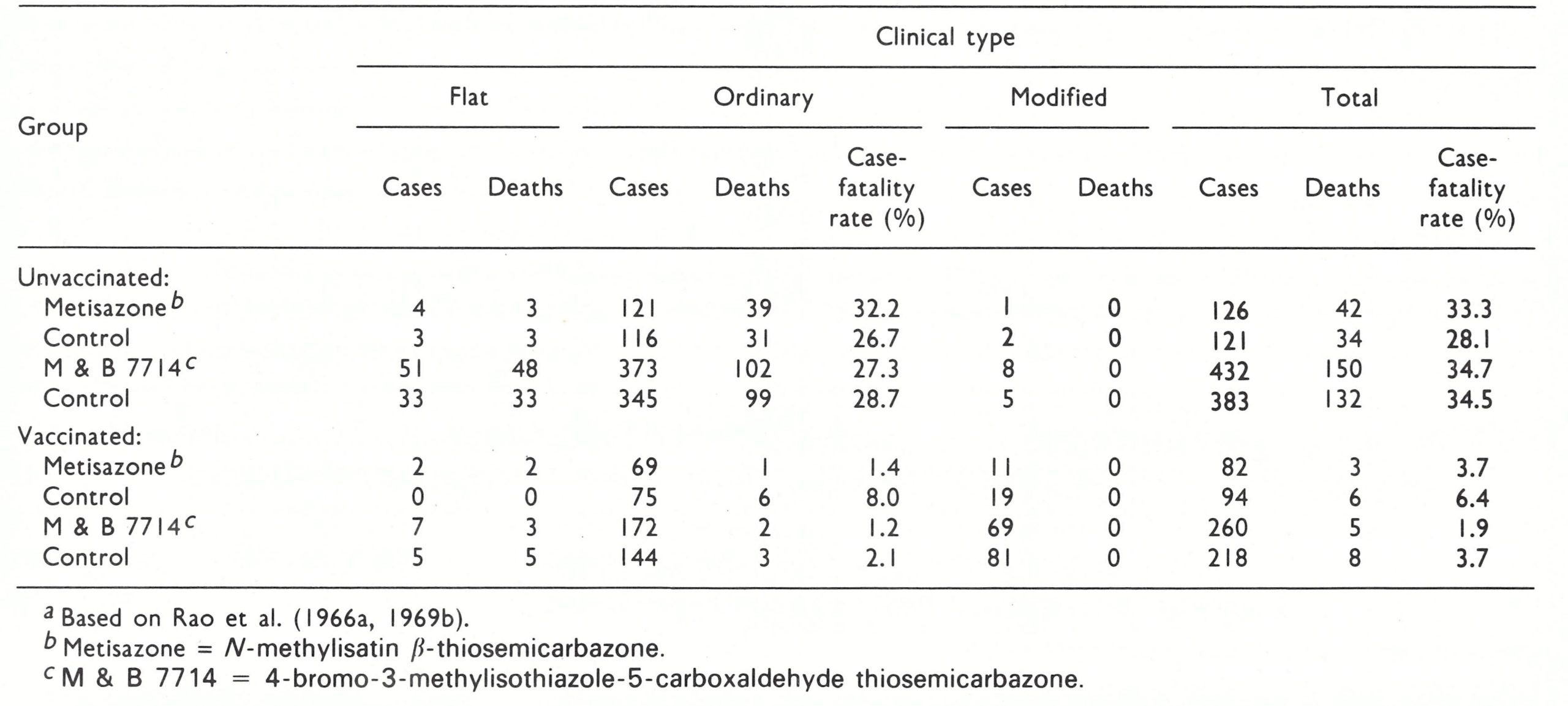
Table 1.19: Summary of results of thiosemicarbazone prophylaxis in smallpox
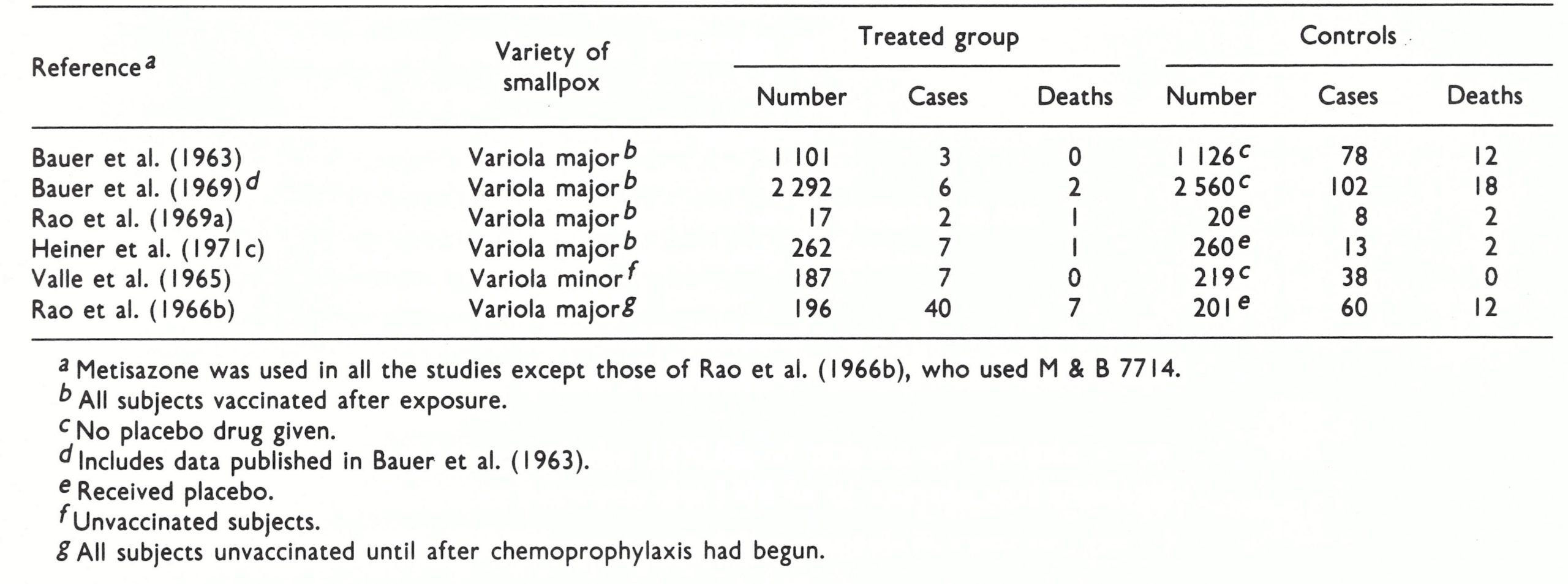
Symptomatic Treatment
In the absence of any effective therapy for established cases of smallpox, treatment was symptomatic and demanded above all good nursing care, which put great demands on the devotion and skill of the nursing staff. ln the crowded smallpox hospitals in endemic countries most nursing care was in fact provided by members of the patient’s family, who often came to stay in the hospital.
In endemic countries, in which hospital facilities were often poor, patients were usually better looked after at home in their village surroundings. Koplan et al. (1978) showed that the case-fatality rate was substantially higher in hospitals than in village surroundings, mainly because only the more severe cases, often in persons without local family support, were admitted to hospital, and devoted family care was better than the nursing provided in grossly overcrowded hospitals. Another reason for encouraging treatment at home during the Intensified Smallpox Eradication Programme was the frequency with which smallpox was transmitted to other patients in hospitals, which often left much to be desired in terms of their overall administration and management of other patients, visitors and staff.
xmwpgyyrwi
November 20, 2025fqzeoqzsyuyyilgwiyxhzshfpgptir
boyarka
January 16, 2026It's fantastic that you are getting thoughts from this post as well as from our argument maee here. http://boyarka-inform.com/
Порно с анальным сексом
January 29, 2026Где смотреть порно, исПорно с анальным сексомледуя надежные платформы в Интернете. Изучите надежные порнохабы для приватного просмотра.