Chapter 20:
Southern Africa

INTRODUCTION
In southern Africa, 10 countries or political jurisdictions lie south of Zaire and the United Republic of Tanzania, occupying an area of 6 million square kilometres (Fig. 20.1). This land mass consists principally of a great central plateau, primarily temperate to subtropical in climate; in 1970 its estimated population amounted to 54 million. The vast deserts of the Namib and Kalahari in the west encompass much of Namibia and Botswana, giving way to undulating plains and savanna to the east and eventually to detached groups of hills and mountains which extend from Malawi through western Mozambique and eastern Zimbabwe (called Southern Rhodesia prior to 1980).
In 1967, when the Intensified Smallpox Eradication Programme began, smallpox throughout southern Africa did not appear to be a major problem. Four areas-Angola, Botswana, Lesotho and Namibia-were believed to be non-endemic; 6 other areas recorded a total of only 534 cases in 1966 and 262 in 1967. Health services in most parts of southern Africa were generally more extensive than elsewhere in the continent and all had some type of organized programme of smallpox vaccination. Although smallpox was undoubtedly a greater problem than official data conveyed, it was thought to be not as widespread or of such high incidence as in neighbouring Zaire or the United Republic of Tanzania, for example.
Given the status of smallpox and the national resources available in many of the countries, prospects for the early interruption of smallpox transmission throughout this vast area might have appeared hopeful. However, political problems made it difficult for WHO to cooperate with the authorities in large parts of southern Africa, and these constraints inhibited the programme. Only 4 countries, with a total population of 10.4 million (in 1970), were Member States of WHO with full voting rights (Table 20.1). A fifth, Swaziland, became independent in 1968 and joined WHO a few years later. Official contact between the Organization and the health authorities of the other 5 political jurisdictions, which had a total population (in 1970) of 42.8 million, was difficult at best and in certain cases practically nonexistent. Angola and Mozambique, both Overseas Provinces of Portugal until 1975, were preoccupied with a protracted and costly civil war. Contact with their health authorities had to be made through the government in Lisbon, for which smallpox eradication was an issue of little significance compared with other problems. Namibia (South West Africa) was administered by South Africa, which, though still a WHO Member State, had been deprived of voting privileges and services by the Seventeenth World Health Assembly in 1964 and which had subsequently ceased to pay its annual contribution or to attend the World Health Assembly. Communications between WHO and South Africa all but ceased at this time, along with South Africa’s participation in the Organization’s activities. Until 1965, Southern Rhodesia had been an Associate Member of WHO, being represented by the United Kingdom in its international relations. When the government unilaterally declared independence, its rights were suspended on the initiative of the United Kingdom. Communications between WHO and Southern Rhodesia had officially to be conducted through the government in London, but there was little or no official contact between the United Kingdom and the new government of Southern Rhodesia.
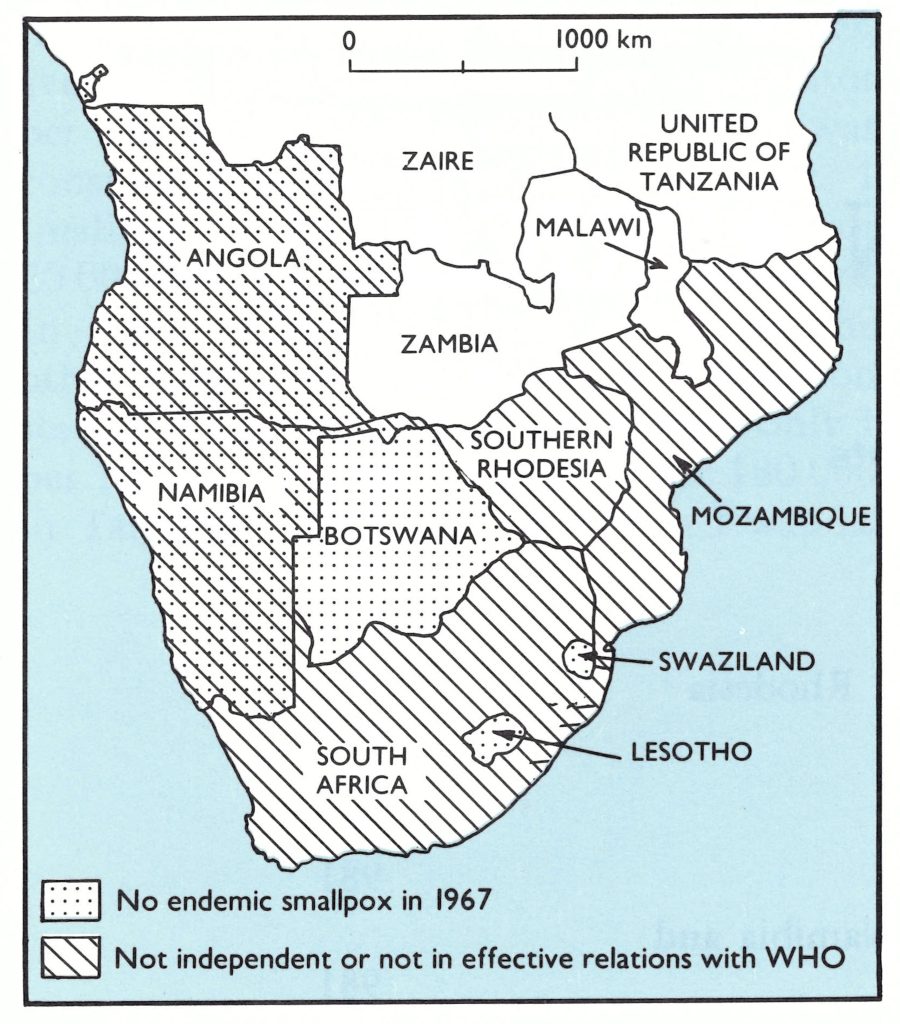
Fig. 20.1. Southern Africa: countries and territories, smallpox endemicity, and relationship with WHO, 1967. The endemicity shown reflects the situation in 1967 as determined later.
Table 20.1: Status of political jurisdictions in southern Africa, 1967-1975
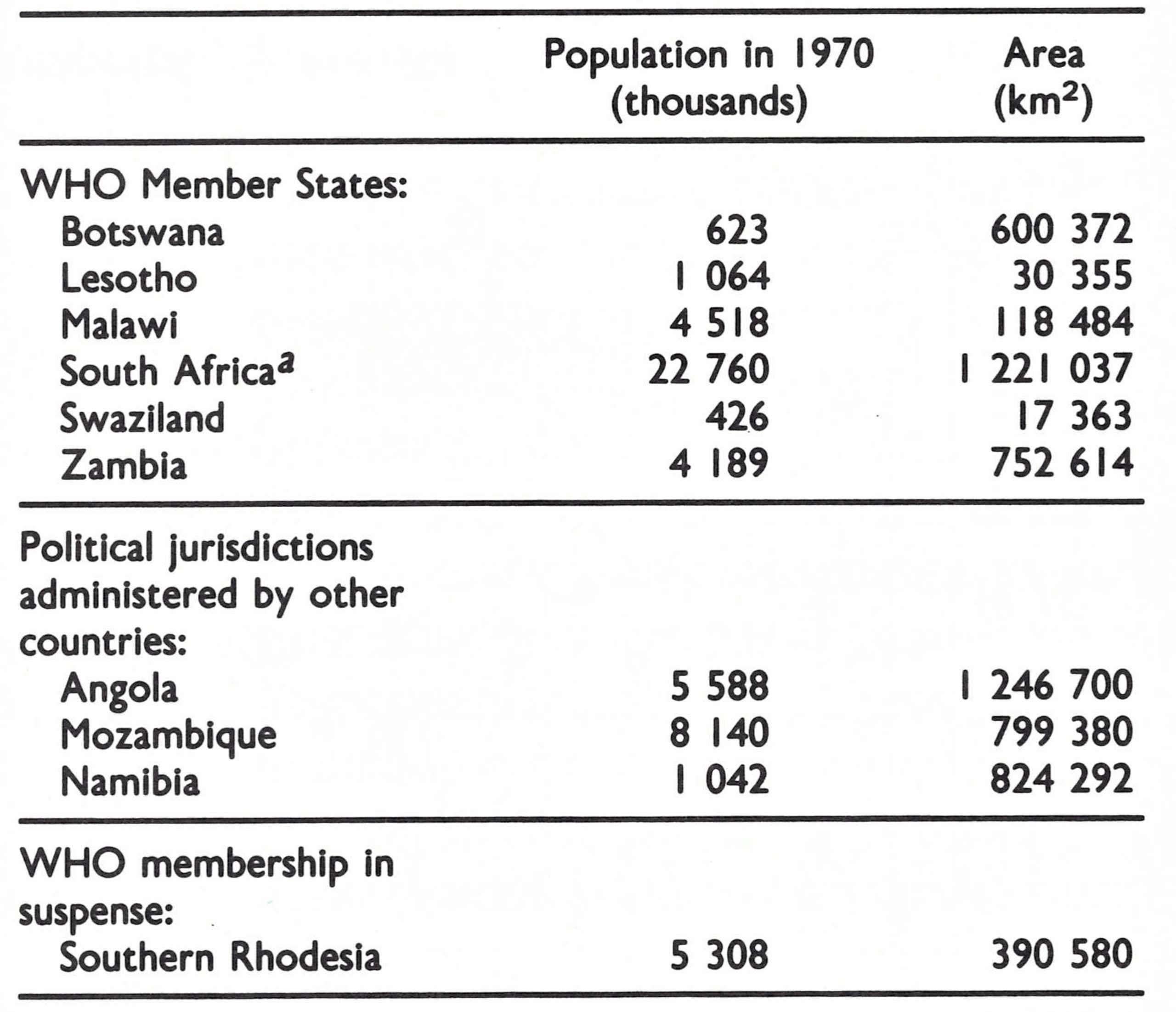
a Deprived of voting privvileges and services in 1964.
The only permissible contact between WHO and the 5 above-mentioned political jurisdictions was embodied in the provisions of the International Health Regulations, which required each to report weekly to WHO Headquarters the number of cases of smallpox, as well as other stipulated “quarantinable diseases”, and the areas that were affected. WHO Headquarters, in turn, could query reports and transmit information deemed to be of importance in the control of these diseases. Although many of the authorities concerned, like those of some other countries, were neither prompt nor comprehensive in their reporting, this contact, tenuous as it was, proved to be an important one.
A further difficulty lay in the fact that smallpox eradication held little interest for South Africa, in which an especially mild form of variola minor was prevalent, the severity of which was comparable to that of chickenpox.
In the circumstances, WHO could freely communicate with and provide assistance only to its “active” Member States, which together accounted for just 20% of the population of southern Africa. It was hoped that in the other endemic areas, programmes would eventually be conducted, if for no other reason than to avoid opprobrium in the eyes of independent African governments which had succeeded in eradicating smallpox.
It was therefore difficult to assess the extent of endemic smallpox in most countries of southern Africa between 1967 and 1971, not only because of problems of communication but also because the completeness of notification improved only slowly during this period. Few outbreaks in any country were investigated by appropriately trained staff or were confirmed by laboratory diagnosis. As a consequence, the extent of underreporting, the numbers of reported cases and outbreaks that represented importations from other countries, and the numbers of cases of chickenpox that might have been misdiagnosed as smallpox were, and remain, a matter of conjecture.
Mass vaccination campaigns, assisted by WHO, were conducted in Botswana, Malawi and Zambia; similar campaigns, assisted by WHO and UNICEF, were carried out in Lesotho and Swaziland. None, except the Botswana campaign, was particularly well executed. Nevertheless, transmission was interrupted in Zambia in 1968 and in Swaziland in 1966 or 1969, as is discussed later in this chapter. In Malawi, the disease disappeared in 1971. Lesotho’s last cases had occurred in 1962, 5 years before the beginning of the Intensified Programme.
Of the 5 political jurisdictions in southern Africa referred to earlier, Angola and Namibia remained smallpox-free, but endemic smallpox was present in 1967 in the other 3—Mozambique, South Africa and Southern Rhodesia. Because of political constraints, they received no help from WHO in their programmes. Mozambique conducted an extensive vaccination campaign in areas accessible to the health authorities, and in February 1969 the last cases were detected. Southern Rhodesia recorded small numbers of cases throughout 1970, all of them along its eastern border with Mozambique. The last known case occurred in December 1970, but whether it was the last in a continuing chain of endemic transmission or a result of importations from remote areas of Mozambique or Malawi remains unknown. South Africa began active eradication measures in 1970, conducting extensive systematic vaccination campaigns in northern parts of Transvaal Province, its only known endemic area. In 1971, it recorded its last indigenous case.
From February to August 1971, no cases of smallpox were reported to WHO from any country in southern Africa. Just when hope was growing that smallpox had been eliminated from this large area, cases began to be reported from Botswana, a hitherto smallpox-free country, adjacent to South Africa’s Transvaal Province. During the preceding 6 years, only a single imported case had been detected in Botswana. Vaccinial immunity throughout the country was low and smallpox began to spread. This was alarming. Not only might smallpox again become established in a country that had been free from it, but it was feared that it might spread through the populated areas in northwestern Botswana into areas of Angola which were inaccessible because of civil war. If smallpox were to become re-established there, the prospects for eradication would be significantly diminished. Effective measures to control the disease were greatly delayed but, by good fortune, it remained confined to Botswana, in which more than 1000 cases were recorded during 1972 and transmission persisted until November 1973.
On the basis of a retrospective review of data collected during the course of the programme and, subsequently, during activities leading to certification, it is probable that in 1967 there were not more than 5 comparatively small foci of smallpox (Fig. 20.2). One was in Zambia in areas adjacent to the then heavily endemic Katanga (Shaba) Province of Zaire. A second straddled the Mozambique-United Republic of Tanzania border, where a Mozambican independence movement was centred and where military forces associated with this movement, as well as refugees, moved into and out of the United Republic of Tanzania. A third lay in central Mozambique and southern Malawi, likewise an area in which security was a problem; a fourth was in rural mountainous areas of Southern Rhodesia and may or may not have extended into adjacent areas of Mozambique; the fifth was in Transvaal Province of South Africa. In all areas except South Africa, smallpox with a case-fatality rate of 5-15 prevailed; in South Africa, a very mild form of variola minor was present with a casefatality rate of less than 1%.
Fig. 20.2. Southern Africa: probable extent of endemic smallpox, 1967.
In this sparsely populated region of Africa, smallpox was readily interrupted with national or regional mass vaccination campaigns, few of which are believed to have achieved the high levels of vaccinial immunity attained in Zaire and western Africa. Moreover, except in Botswana, programmes of surveillance and containment were never well developed. However, the eradication programme served in some countries to develop reporting systems and to promote routine vaccination against this and other diseases in existing health facilities. It is apparent in retrospect, though, that eradication might have been achieved more readily and more rapidly if freeze-dried vaccine had been supplied to existing health programmes and if simple surveillance activities had been developed.
This chapter discusses first the activities in Zambia and then the programmes in Malawi, Mozambique and Southern Rhodesia. A third section deals with smallpox in the adjacent countries of South Africa, Botswana, Lesotho, Namibia and Swaziland. Lastly, activities in smallpox-free Angola are briefly described.
ZAMBIA
Zambia, a subtropical country consisting largely of wooded plateau, became independent in 1964. Its population of 3.8 million (in 1967) lived primarily in scattered villages, only 700 000 being resident in the 9 major towns. Its road system was comparatively extensive, as was its network of health facilities, which included 60 hospitals, 93 urban and specialized clinics and 323 rural clinics. Many of these were staffed by expatriates, there being at that time only 3 Zambian physicians and a dearth of Zambian paramedical staff. Few of these health units, however, provided vaccination against smallpox.
Smallpox, with a case-fatality rate of 5-15%, similar to the form existing in neighbouring Zaire, had been prevalent for many years (Table 20.2). Mass vaccination campaigns employing liquid vaccine were conducted during periodic outbreaks.
In 1963-1964, major epidemics began to occur in Zambia (Fig. 20.3), primarily along the Zairian border. The new government responded with a national mass smallpox vaccination campaign utilizing specially constituted mobile teams. The programme began in 1964 in each of 8 provinces under the supervision of provincial officials. One hundred and forty vaccinators were recruited and trained locally and discharged when the team had completed its work in a given area. They vaccinated at assembly points, using liquid vaccine. The intent was to vaccinate one-third of the population of each province each year. Vaccinations were performed during the dry season, from May to November . Despite a serious shortage of transport, limited supervision and inadequate refrigeration facilities, 1 .66 million vaccinations were reported to have been given during 1964 and 1.5 million in 1965. Take rates among primary vaccinees were found to be about 80%. This was lower than the take rates expected when freeze-dried vaccine was used but, considering the logistic problems in the country, it was a remarkably good result. The number of reported cases decreased sharply, from 2214 in 1964 to 528 in 1965.
Table 20.2: Zambia: number of reported cases of and deaths from smallpox and casefatality rates, 1956-1973, and number of vaccinations performed, 1964-1973
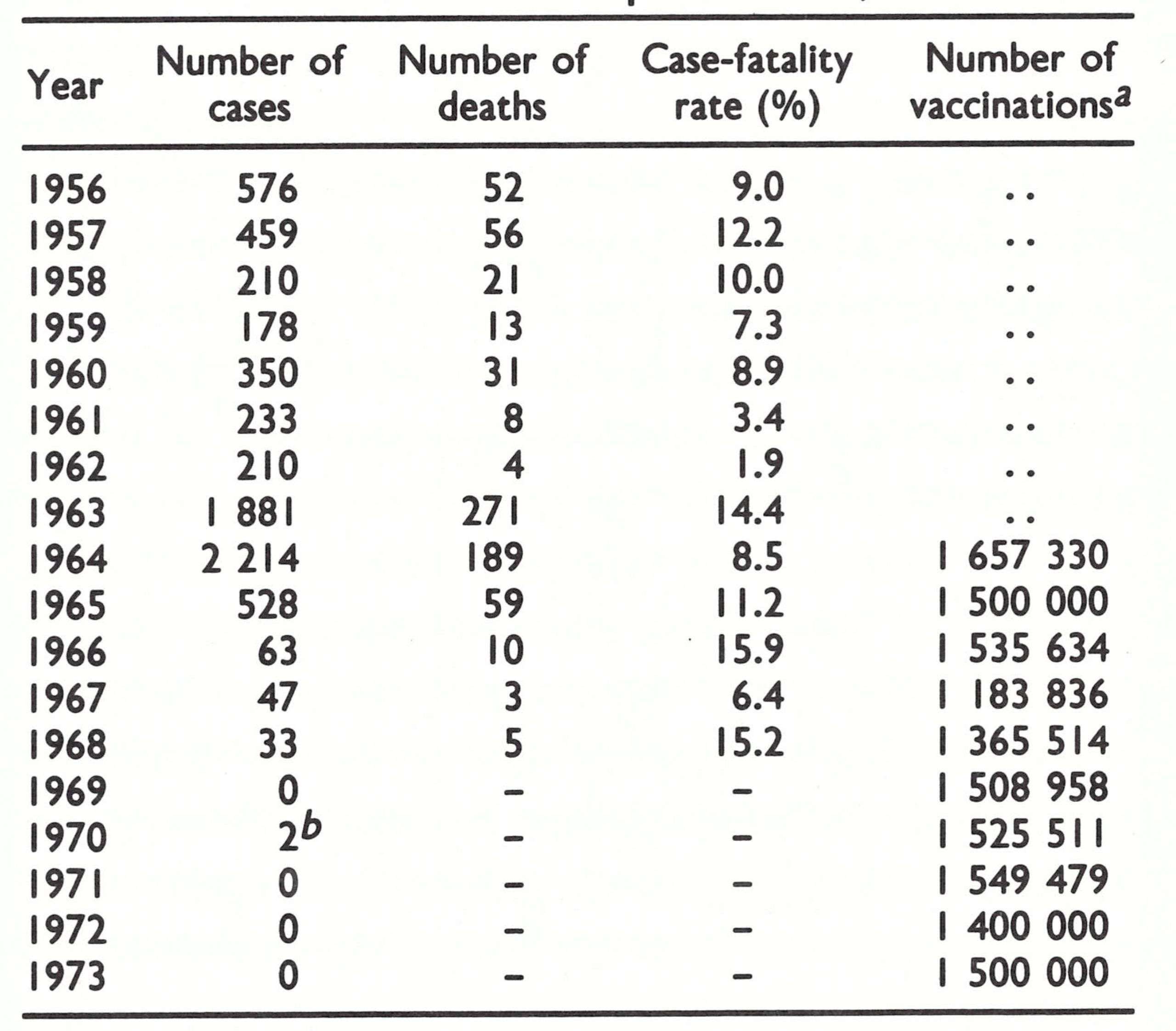
a..= data not recorded.
b Imported from Zaire.
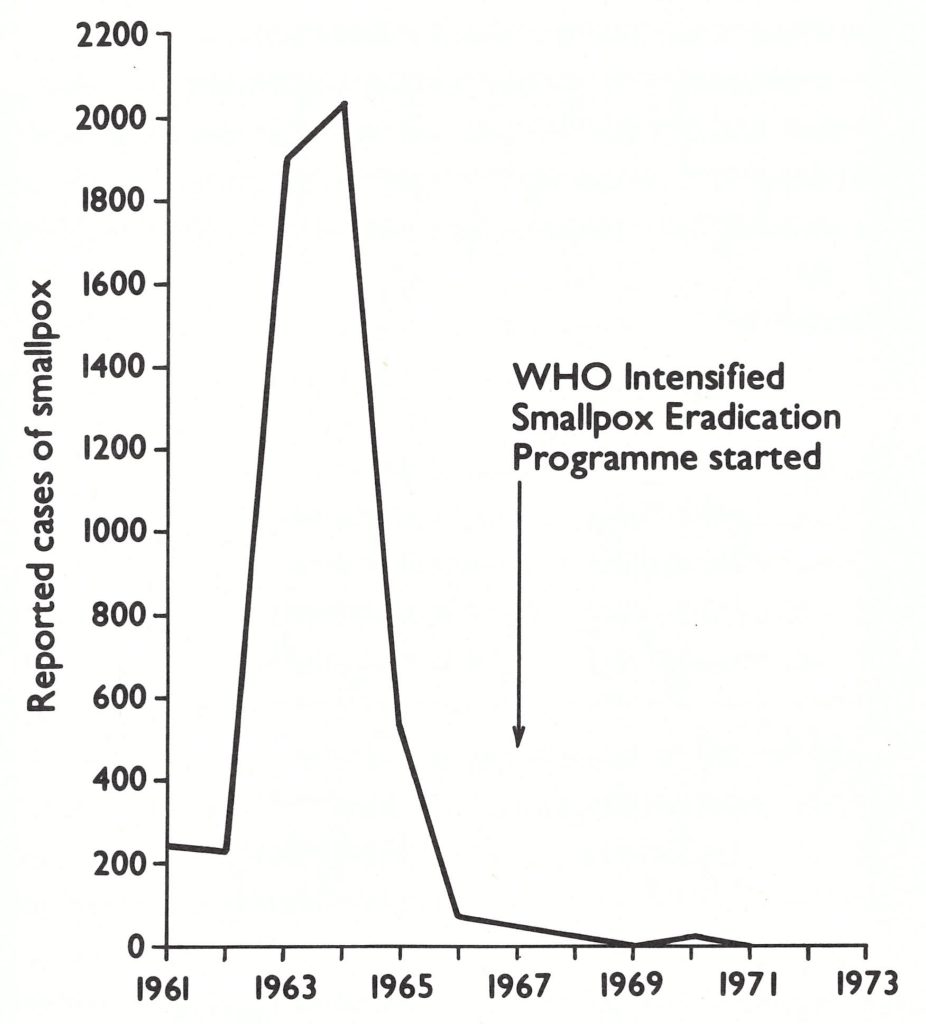
Fig. 20.3. Zambia: number of reported cases of smallpox, by year, 1961-1971.
In January 1966, freeze-dried vaccine, donated by the USSR, began to be employed. That year, another 1.54 million persons were vaccinated, and the number of cases decreased further to only 63 in 1966.
The government was committed to smallpox eradication and in March 1967 requested WHO to provide vehicles, refrigerators and other equipment as well as 4 advisers—a medical officer counterpart for the director and 3 operations officers to serve in supervisory roles, where needed, at provincial level. Between 1967 and 1973, WHO was to provide 10.6 million doses of vaccine and expend US$644 146, an outlay which included WHO salary payments. The WHO medical officer arrived in November 1967 and the 3 operations officers in 1968. Meanwhile, the government staff for the mass vaccination campaign was increased from 140 to 207.
Under the new WHO-assisted programme, BCG vaccine was given simultaneously to all schoolchildren and, in two of the provinces, to younger children as well. Between January 1966 and the end of 1968, the so-called “first phase” of the programme was completed—i.e., vaccination with freeze-dried vaccine throughout the country. The number vaccinated was roughly equivalent to the estimated population. In 1968, only 33 cases were reported and smallpox transmission appears to have been interrupted in December of that year.
During 1967-1968, the WHO-assisted programme changed little in character. Vaccination was conducted at assembly points; coverage and take rates were assessed only occasionally; little was done to improve the surveillance system. Indicative of the quality of surveillance is the fact that little is known about the last 10 cases reported in 1968, except that 2 were said to have been infected in Zaire.
Beginning in 1968, the established government health units were provided with stocks of vaccine and encouraged to vaccinate all who attended but, as was true in many countries, these units evinced little interest in undertaking even this most simple of preventive measures. Throughout the whole of 1969, they performed only 91 650 vaccinations and many of these were given by programme vaccinators who were assigned to clinics. Fully 3 additional years of concerted effort were required before the staff of the health units began to vaccinate significant numbers of persons.
Although a programme of vaccination had been completed throughout the country, the government decided in 1969 to repeat the national mass vaccination campaign, using special teams as before. Because smallpox was still endemic in neighbouring Zaire, the United Republic of Tanzania and Mozambique and because the existing health units were providing little help, government officials felt that this was the only way that they could ensure a sufficiently high level of vaccinial immunity to prevent spread should introductions occur.
The WHO operations officers were assigned to the provinces bordering on Zaire, and vaccination check-points were established at the principal border crossings to examine persons entering the country and to vaccinate anyone without a scar. In some areas, the coverage achieved was assessed by WHO operations officers after the teams had worked in an area. Throughout Zambia, however, supervision generally remained poor, which was reflected in the unsatisfactory performance of vaccinators, who averaged only 40 vaccinations per day.
The repeat mass vaccination campaign was costly but it did assure the movement throughout the countryside of vaccination teams which could detect any cases that existed. Between 1969 and 1971, an additional 4.6 million vaccinations were performed, the annual average being no more than had been achieved in 1964-1965, before the provision of WHO assistance.
During 1970, at the midpoint of this repeat round of mass vaccination, a cluster sample survey of the country was carried out by staff of the WHO Epidemiological Surveillance Centre in Nairobi, Kenya, to measure the level of vaccination coverage. In all, 17 927 persons were examined. The proportion with vaccination scars was found to range from 62% to 80 % in the different provinces, but in 5 of the 44 districts it was discovered that fewer than 60% of the people had ever been vaccinated. By any standard, the programme had not been notably successful.
The need to recruit at least one experienced team to encourage reporting and to investigate each suspected case had been stressed repeatedly by Ladnyi, the WHO intercountry smallpox adviser for eastern and southern Africa, but not until late 1969 was such a team formed and the first efforts made to ensure that each of the 429 health units provided a weekly report. Even then, the effort left much to be desired: as late as June 1970 the WHO medical adviser to the national programme commented that a report of a suspected case was usually followed by immediate investigation. The concept that every suspected case was important was not understood.
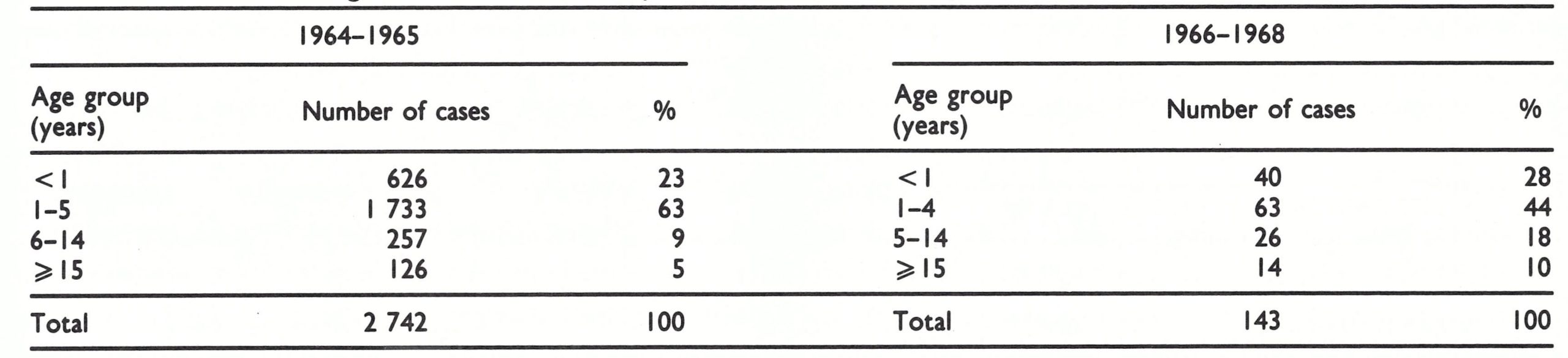
Meanwhile, in Zaire, mass vaccination throughout the neighbouring Shaba Province was completed during 1969, although a few cases of smallpox were reported each month in early 1971. Despite the continuing presence of endemic smallpox just across the border, only 2 imported cases were detected in Zambia, in April 1970. These cases actually spent less than a day in the country . The individuals concerned—a 4-year-old child and a 7-year-old child—were brought across the river from Zaire by their parents to be examined at a clinic. They were diagnosed as suffering from smallpox by the staff of the clinic and were promptly sent back to Zaire, Table 20.3. Zambia: age distribution of reported cases of smallpox, 1964-1965 and 1966-1968 but the incident was duly reported to the provincial health office. These were Zambia’s last known cases.
Not until the beginning of 1971, when the risk of importations seemed to have diminished almost to nil, was a comprehensive surveillance system finally established in northern Zambia, near the borders with Zaire and the United Republic of Tanzania. In these areas each village was visited twice monthly by a surveillance agent to detect cases with rash and fever which might be smallpox. Additional permanent vaccination posts were established along the frontiers and many suspected cases were investigated. Because the United Republic of Tanzania detected no cases in 1971 and Zaire found none after June of that year, it is not surprising that no further cases were discovered in the bordering areas of Zambia.
With the conclusion of the second round of mass vaccination, the number of staff was reduced and the number of WHO advisers decreased from 4 to 2. A maintenance programme was established whereby 15 mobile vaccination teams moved through the provinces vaccinating the more remote populations and encouraging vaccination in established health facilities. In all, 1.4 million persons were vaccinated in 1972 and 1.5 million in 1973, numbers comparable to those vaccinated by the much larger special vaccination campaign staff. In the mid-1970s, immunization against several diseases began to be offered by many of the established health units, and monthly reports giving the number of cases of disease and the number of vaccinations performed were received regularly from 96 hospitals and 689 health centres and subcentres.
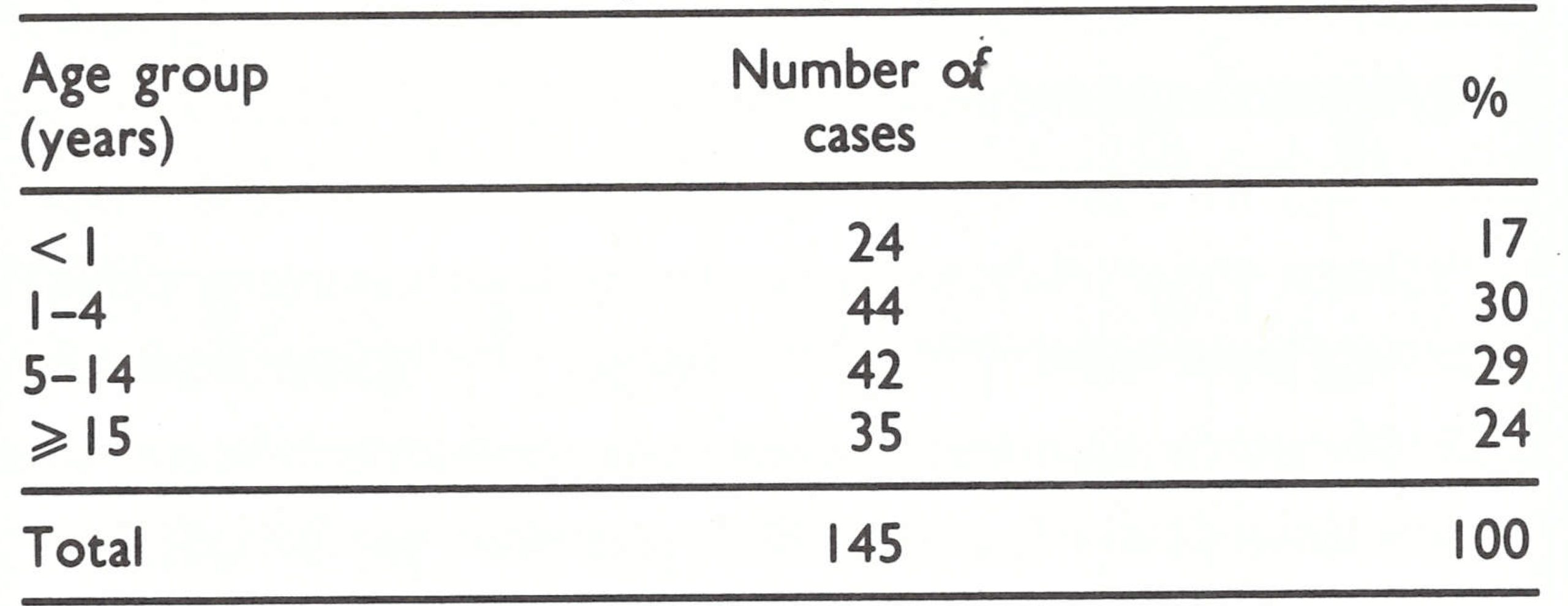
The age distribution of cases during 1964- 1965 was unusual in that 86% of those recorded were in individuals aged less than 6 years (Table 20.3). This was an unusually high proportion of cases among young children, for which there is no explanation other than that it may have been an artefact of reporting. Data for the 1966-1968 period show a more typical age distribution of cases.
Table 20.3: Zambia : age distribution of reported cases of smallpox, 1964-1965 and 1966-1968
MALAWI, MOZAMBIQUE AND SOUTHERN RHODESIA
Background
Malawi, Mozambique and Southern Rhodesia together had a population of 18 million (in 1970) and a reasonably extensive network of health centres and roads, Southern Rhodesia’s being the most fully developed. From 1963, the prevalent form of smallpox in these countries appears to have been variola major, with a case-fatality rate of 5-15%. During the early 1960s, smallpox had been of special concern to the health authorities, and all had organized mass vaccination campaigns employing mobile teams. Reasonably satisfactory control seems to have been achieved. In all, only 142 cases were reported in 1966 and 172 in 1967, although the true numbers were undoubtedly much greater because notifications in these countries, as elsewhere, were very incomplete.
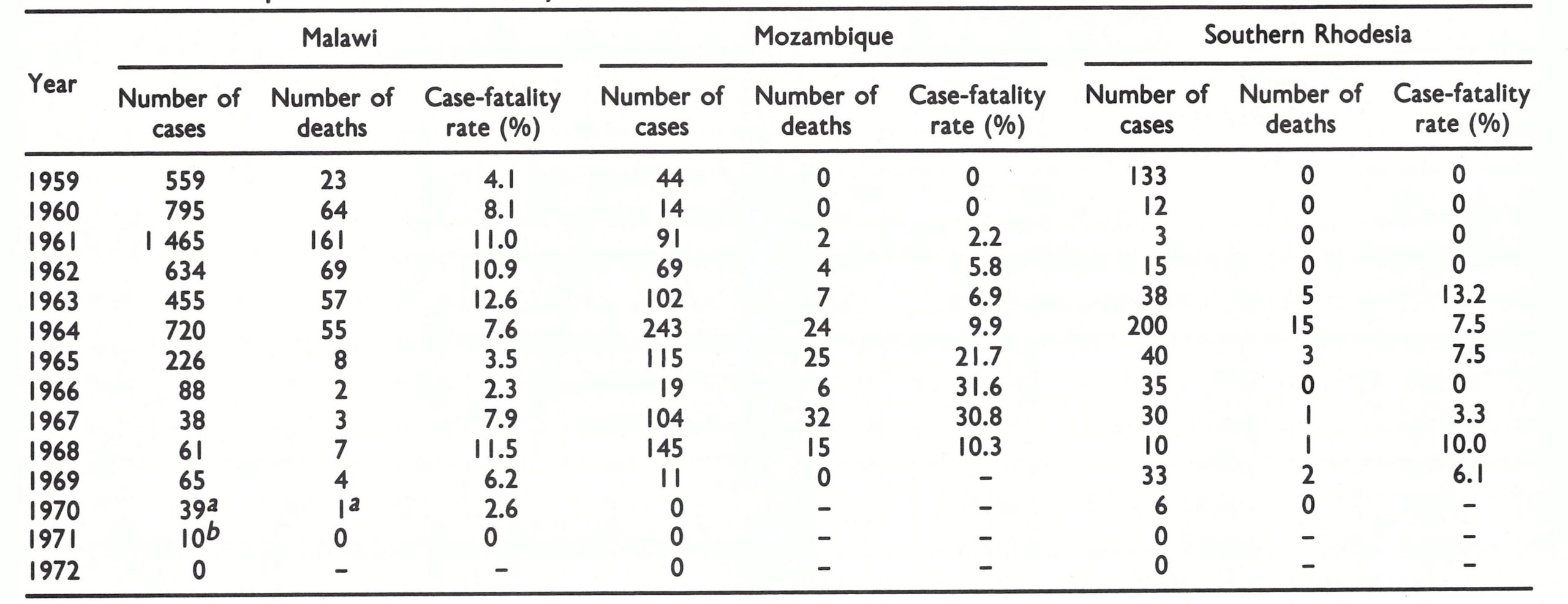
The recurrence of variola major was a recent development. Variola major had been prevalent before 1952, but in that year it was replaced by variola minor. From 1952 to 1958, for example, Malawi recorded 810 cases but only 8 deaths. In 1959, both the number of cases and the case-fatality rate began to increase and by 1961, 1465 cases with 161 deaths were reported (Table 20.4). The source of the strain which infected Malawi was in all likelihood either neighbouring Zambia or the United Republic of Tanzania. In Mozambique, a similar change in the prevalent smallpox strain took place in 1962-1964, at the time of civil conflict along its border with the United Republic of Tanzania. In 1963, fatal cases began to be observed in Southern Rhodesia, virtually all of them occurring in the eastern provinces bordering on Mozambique.
The civil war in Mozambique played a significant role in the persistence of smallpox in these countries. A national independence movement, which had been established in border areas in the south of the United Republic of Tanzania, moved into the 2 northern provinces of Mozambique in 1964. In addition to conducting guerrilla warfare, the independence movement established a political and administrative structure which, during the following decade, expanded into the central and north-western provinces. To combat this movement, the Mozambican government resettled many of the scattered rural population into villages which could be defended and in which health and educational services could be provided. Thus, village health units capable of reporting cases of smallpox existed throughout the country, but few activities were possible in the sparsely populated rural areas, including extensive tracts adjacent to the United Republic of Tanzania, Malawi and Southern Rhodesia.
Table 20.4: Malawi, Mozambique and Southern Rhodesia: number of reported cases of and deaths from smallpox and case-fatality rates, 1959-1972
 a Cases documented during survey in 1972.
a Cases documented during survey in 1972.
b Nine cases documented during 1972 survey and i during 1977 survey.
Vaccination Campaigns
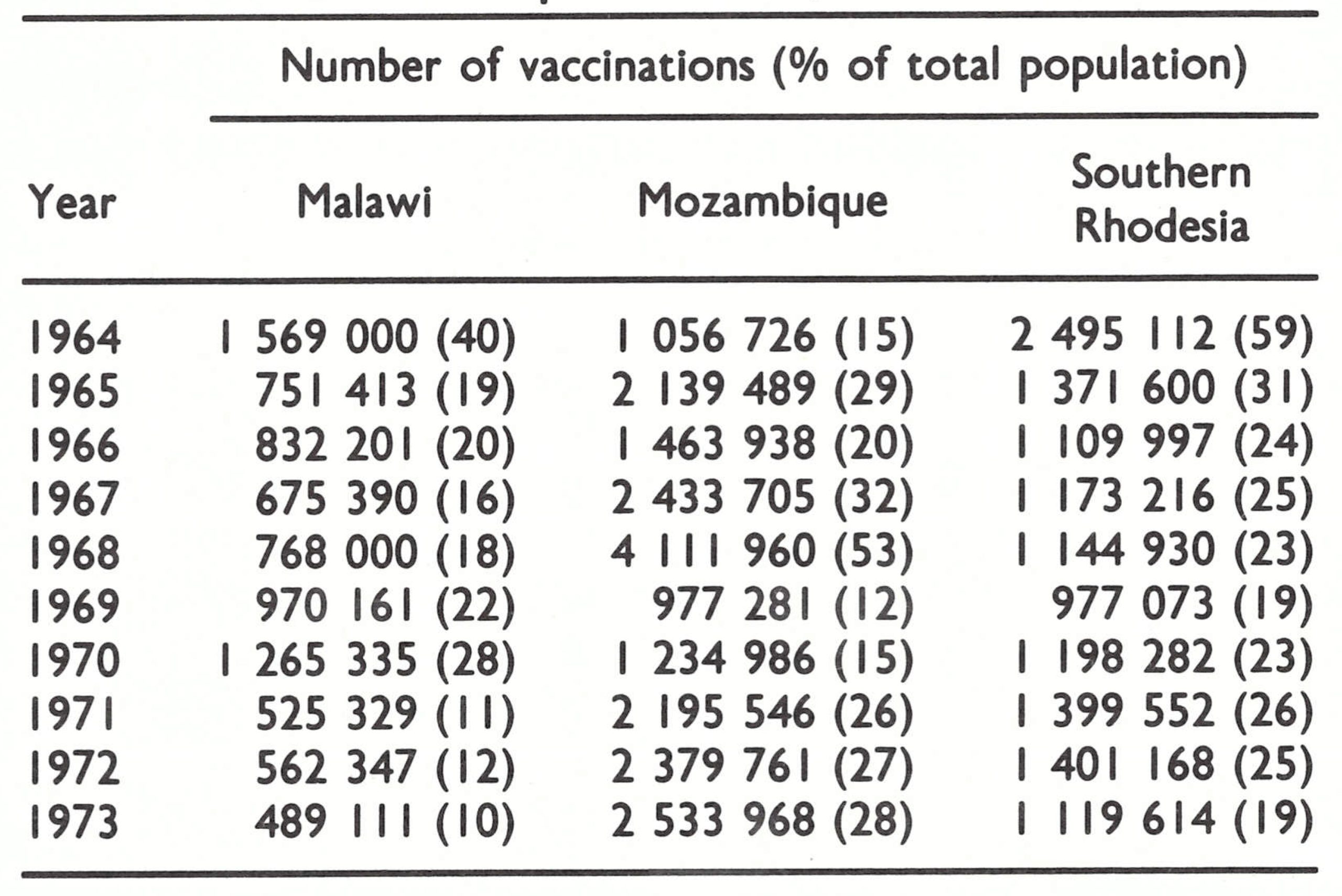
For a number of years prior to 1967, a considerable proportion of the population in each country was reported to have been vaccinated each year (Table 20.5), but none of the programmes incorporated a system for assessing the level of coverage achieved, and only in Southern Rhodesia were take rates regularly appraised.
Freeze-dried vaccine was used only in Mozambique, the vaccine having been produced at the Instituto de Investigacao in Lourenco Marques (now Maputo). Samples of this vaccine were tested by the International Reference Centre for Smallpox Vaccine in Bilthoven, Netherlands, in 1968 and 1972 and found to meet WHO standards. Vaccination in Mozambique was offered in hospitals as well as in health and first-aid posts and by mobile teams, each of 9 districts having 3 or 4 teams which sought to vaccinate one-third of the population each year. BCG vaccination was given simultaneously. During 1968, a special campaign was conducted which succeeded in vaccinating against smallpox half of the 8 million residents, although, because of security problems, 2 districts in the north, Niassa and Tete, could not be well covered. A repeat campaign was conducted in 1972, during which, because hostilities had subsided in Tete District, it was possible to vaccinate most of the people in this area. Although the coverage was not assessed, vaccinial immunity was probably reasonably good among accessible populations, considering that a large number of people had been vaccinated and freeze-dried vaccine had been used. However, immunity was undoubtedly much lower among the inhabitants of the large sparsely populated rural areas of the central and northern parts of the country.
In Southern Rhodesia, a similar type of programme was conducted, with vaccination being given by mobile teams and in existing health facilities. Poliomyelitis and BCG vaccines were administered simultaneously to children. Until 1970, liquid smallpox vaccine produced in South Africa had been employed. A continuing assessment of take rates among primary vaccinees was conducted by local health authorities, and these showed 75—90% successful vaccinations—rates which were lower than those obtained with freeze-dried vaccine, but higher than those in most countries that used liquid vaccine. The only available data regarding the prevalence of vaccinial immunity are from a 1978 government survey, which found that 74% of children aged 1-6 years and 92% of those aged 7-10 years had vaccination scars.
In Malawi, a permanent staff of 42 vaccinators regularly travelled by bicycle through their assigned regions, giving smallpox vaccine only; a 10-man mobile team was available for vaccination where outbreaks occurred. The mobile team worked primarily in the south, where, after 1965, almost all cases were found. Until 1966, liquid vaccine was employed; primary take rates, when measured in the field, were only 25-50%. The programme was not particularly successful, as was apparent from a survey in 1965, which showed that only 360 of 2566 schoolchildren (14%) in and around the capital city had vaccination scars. In January 1966, freezedried vaccine was made available by UNICEF and thereafter only this type of vaccine was employed. WHO staff visiting the country in 1966 and 1968 found that the supervision of vaccinators was poor, their productivity was low and the vaccinial immunity of the population was unsatisfactory. In one area of southern Malawi, in which United States Peace Corps volunteers assisted in mass vaccination in 1968, 50% of the inhabitants remained unvaccinated at the end of the campaign. Late in 1969, the government decided to request assistance from WHO in conducting a national smallpox eradication programme, but a better-organized vaccination campaign did not begin until April 1972. That programme included the administration of both BCG and smallpox vaccines. When the campaign was launched, surveys in different areas showed that 30—60% of children aged 0-4 years and 36—76% of those aged 5-14 years had vaccination scars. Only 5 months after the programme had begun, it was stopped by the government on account of the occurrence of abscesses due to BCG vaccination. It did not recommence until August 1973—almost a year later—but was halted once again, in December 1973, when cholera broke out and the teams were reassigned to perform cholera vaccination.
Finally, in 1974, an extensive vaccination campaign began, long after the last cases had been detected1. It concluded in 1976. WHO financial support throughout the course of the programme amounted to US$311 011; in addition, 7.8 million doses of vaccine were supplied.
Table 20.5: Malawi, Mozambique and Southern Rhodesia: number of reported cases of and deaths from smallpox and case-fatality rates, 1959-1972
The Smallpox Situation
In the 3 countries under review, information about smallpox, from 1967 until 1971, when the last known cases were detected, is sketchy. Undoubtedly, many cases occurred which were not reported and some which were reported may not have been smallpox. Health authorities at district or provincial level in each country usually performed areawide vaccination when cases were reported but rarely did they conduct investigations to detect additional cases or to identify the source of infection. Ladnyi, during visits to Malawi, tried to persuade the government to initiate a surveillance programme, but not until 1973 was a satisfactory programme established for the investigation of suspected cases of smallpox. Since there could be no direct official communication between WHO and the health authorities in Mozambique and Southern Rhodesia, a similar effort to encourage proper surveillance in these areas was greatly delayed. At the end of 1969, some WHO staff began corresponding personally with university faculty members in Salisbury, Southern Rhodesia, who soon thereafter undertook to examine specimens from many suspected cases although few epidemiological investigations were conducted. Not until the spring of 1972 did WHO and the countries concerned reach agreement to give Henderson special permission to visit Mozambique (as well as Angola and South Africa although not Southern Rhodesia) to assess the nature of their programmes and to discuss needed surveillance measures in areas then believed to be smallpox-free. Information about smallpox, even that pertaining to the last outbreaks, is thus fragmentary in all the countries concerned.
Mozambique detected 104 cases in 1967, 145 in 1968 and 11 in 1969 (the last occurring in February) (Fig. 20.4). Of the 145 cases in 1968, 142 were reported from parts of only 3 provinces, all in the north of the country (Fig. 20.5). Most of the outbreaks occurred in villages in Tete District, near the border with Malawi, and in Niassa District, which adjoined endemic areas in the United Republic of Tanzania. The 11 cases detected in 1969 were all in Niassa District. Because the guerrilla forces of the independence movement continued to travel between Niassa and the southern part of the United Republic of Tanzania, it is possible that these foci were related. This is speculation, however, since in neither country were outbreaks investigated to determine their sources. Few smallpox cases were reported in the south of the United Republic of Tanzania after 1969 but it later border areas of Malawi and Southern Rhodesia, at least until the end of 1970. In Mozambique, however, no further cases were detected after 1969. Because security in many of the border areas was problematic, cases may well have occurred but remained undetected.
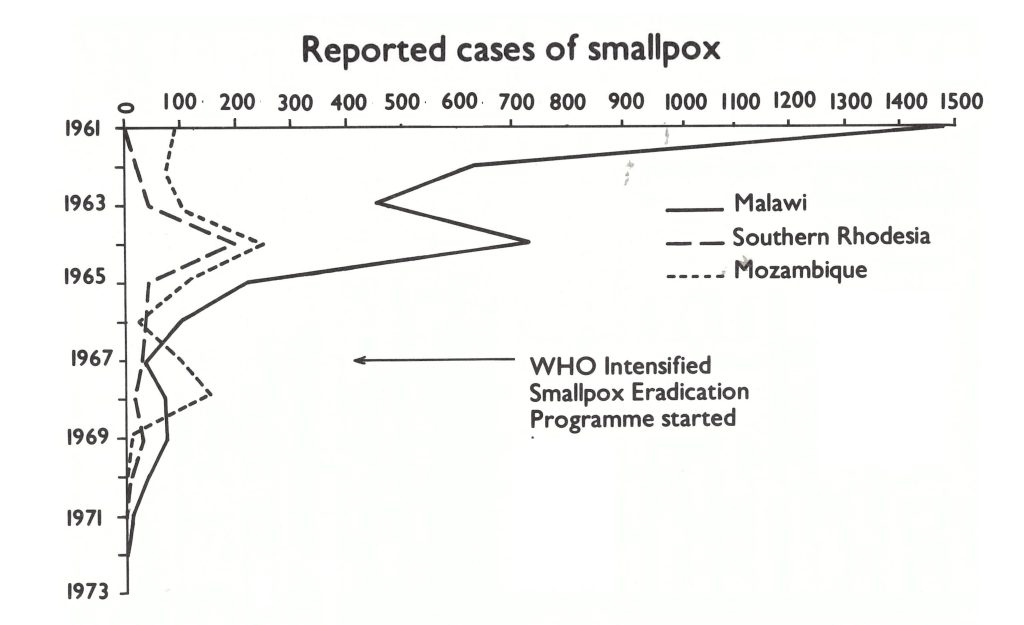
Fig. 20.4. Malawi, Mozambique, Southern Rhodesia: number of reported cases of smallpox, by year, 1961-1972.
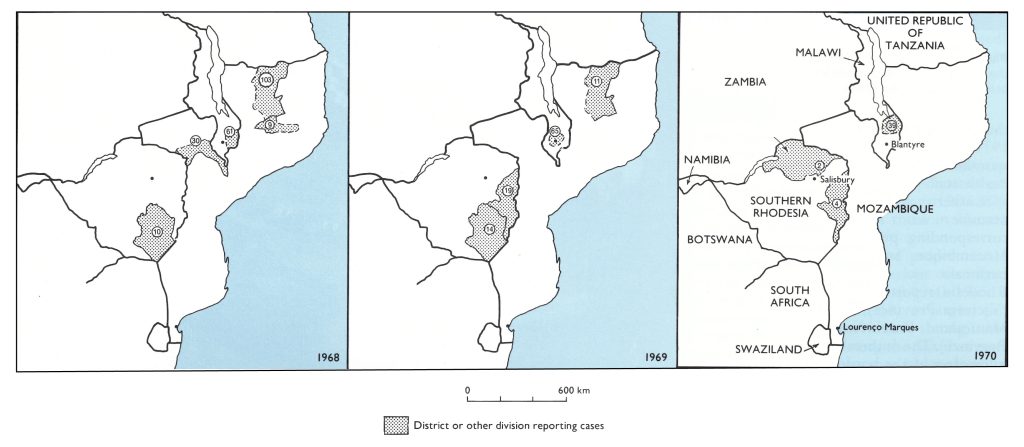
Fig. 20.5. Malawi, Mozambique, Southern Rhodesia: location of reported cases of smallpox, 1968-1970.
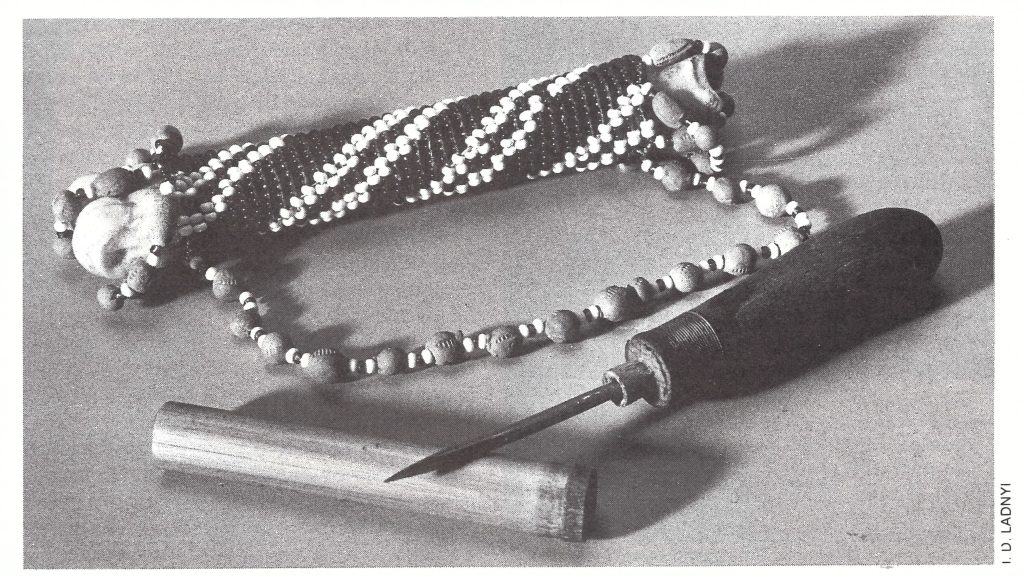
Plate 20.1. Important foci of smallpox in southern Africa were situated along the border between Mozambique and Malawi, which was frequently crossed by Mozambicans fleeing the civil war. They were stopped and vaccinated if they used the official crossing points, but most went along forest trails and so escaped vaccination.
In Malawi, all cases after 1966 were reported from the south of the country. Southern Malawi presented an especially difficult problem. Large numbers of refugees from Mozambique lived in the region, most of whom crossed into the country through forest areas rather than at official border crossings. As illegal immigrants, they sought to avoid any contact with government authorities and often fled into the jungle when teams came to vaccinate. In order to contain outbreaks, villages were sometimes surrounded by a police cordon to prevent villagers from leaving the area until all had been vaccinated. In addition, some outbreaks were discovered during which variolation had been performed, supposedly in order to quell the spread. Cases which were detected were frequently reported as occurring among refugees from Mozambique or residents who had been in contact with them. Whether the cases represented new importations or continuing transmission among immigrants is unknown. Malawi reported only 61 cases in 1968 and 65 cases in 1969. In December 1969, the last case was reported by the health services. No cases were notified during 1970-1971.
By early 1972, it appeared that smallpox transmission might have ceased in the Malawi-Mozambique area. More than a year had elapsed since the last cases had been detected in Malawi and nearly 3 years since the last case had been reported in Mozambique. However, neither country was believed to have adequate surveillance programmes and thus doubts persisted as to whether smallpox was really absent. WHO staff could not participate in confirmatory studies in Mozambique but they could do so in Malawi. In April 1972, Dr Ziaul Islam, who had replaced Ladnyi as the WHO intercountry smallpox adviser, undertook a village-byvillage field survey in areas of southern Malawi in which smallpox outbreaks had repeatedly occurred between 1966 and 1969. In 5 villages, he discovered 48 individuals with facial pockmarks who had developed smallpox in 1970 and 1971 (Table 20.6). The area was densely forested, populated with many refugees from Mozambique, including groups which, for religious reasons, refused vaccination. The first case that he could identify in the chain of transmission had become ill in April 1970, and the last in February 1971. The earliest source of infection could not be specifically linked to previous outbreaks in Malawi although outbreaks had occurred in the same area in the past. During a vaccination scar survey in the affected area, Dr Islam found that 61 % of children under 4 years of age, 84% of those aged 5-14 years, and 67% of persons aged 15 years and over had vaccination scars. Because of the proximity of the villages to Mozambique, the authorities there were notified. Mozambican teams subsequently undertook an extensive programme of vaccination and search throughout the adjoining area in Mozambique but found no cases. During 1977, WHO and Malawian staff undertook a more extensive survey of the entire affected area in Malawi. They confirmed Dr Islam’s earlier report but failed to detect further spread. They did, however, discover a pockmarked girl who was said to have become ill in September 1972, 19 months after the presumed last case in February 1971. Extensive investigation failed to reveal any other cases among family contacts and eventually it was concluded that the reported year of illness was erroneous. Malawi’s last known case is thus thought to have occurred in February 1971 in an outbreak which terminated spontaneously without being detected by health staff.
Table 20.5: Malawi, Mozambique and Southern Rhodesia: number of reported cases of and deaths from smallpox and case-fatality rates, 1959-1972
 a() = Cases by month of onset, discovered during 1972 and 1977 surveys.
a() = Cases by month of onset, discovered during 1972 and 1977 surveys.
Plate 20.2. Variolator’s kit obtained in 1966. Scabs and pustular material were carried in the bamboo stick; the awl was used for inoculation. Malawi was the only country in southern Africa where variolation was still being practised in the 1960s.
Southern Rhodesia’s surveillance programme was little better than the corresponding programmes in Malawi and Mozambique, and the origin of its last outbreaks no less mysterious. Southern Rhodesia reported only 10 cases in 1968 (Victoria Province) and 33 in 1969 (19 in Manicaland Province and 14 in Victoria Province). The outbreaks were all within 100 kilometres of the border with Mozambique. Mass vaccination was reported to have been performed in the area of each outbreak but only occasionally did provincial medical officers investigate outbreaks to ascertain the sources of infection. Indeed, as a review of records in 1978 was to show, none of the cases occurring in 1969 was investigated to determine the source of infection; a report of 10 cases was found which had been received by the provincial medical officer but had not been transmitted to the national authorities. (These cases do not appear in the official records and are not included in Table 20.4 or Table 20.6.)
In 1969, Dr Keith Dumbell from the WHO Collaborating Centre for Poxvirus Research in London and Henderson from Geneva began to correspond with Dr J. G. Cruickshank, a virologist at the University College in Salisbury, to encourage the taking of specimens from cases to confirm the diagnosis and to obtain virus strains for laboratory study. Subsequently, in March 1970, the Secretary of Health of Southern Rhodesia directed provincial medical officers to obtain such specimens, and Dr Cruickshank, employing electron microscopy and standard virus isolation techniques, began to process a flow of specimens (Swanepoel & Cruickshank, 1972). Throughout most of 1970, some of the specimens submitted showed herpes-varicella virus but none showed any poxviruses. No cases were reported to WHO from Southern Rhodesia during 1970 until 13 August, when a telex from the government was received in Geneva reporting a case of smallpox. Because the notification had been made under provisions of the International Health Regulations, official inquiry to Southern Rhodesia was permitted: “Would appreciate receiving urgently further particulars on source of infection of recent smallpox case and confirmation of diagnosis. No known smallpox in recent months in eastern Africa within 325 miles of Chipinga District [the location of the case].” The reply, telexed a week later, indicated that the case had not been confirmed because the patient had left the hospital before being questioned and was thought to have returned to Mozambique. The official weekly reports from Southern Rhodesia subsequently reflected no cases; only much later was the case added to the official records.
No other cases were notified until November 1970, when the government reported, by telex, 2 further cases. The existence of these cases implied that there was a persistent focus of endemic smallpox, and undoubtedly many more cases had occurred to sustain the chain of transmission. Letters and telegrams were exchanged, but to little avail. Southern Rhodesia was eventually to record officially 6 cases in late 1970. Four were reported from Chipinga Town, 25 kilometres from the Mozambican border; 2 of them were considered to have been possible importations from Mozambique but the information available was too vague to confirm this. The remaining 2 cases were reported from another province near the border and confirmed by electron microscopic examination. Their onset occurred in December 1970. It was reported that the patients had been in Mozambique 2 weeks earlier, but again the investigation was perfunctory.
Over the succeeding 5 years, Dr Cruickshank examined 17 specimens taken from suspected cases of smallpox and others from patients with chickenpox and other rash producing illnesses. None proved to be smallpox. During 1978, in preparation for certification, extensive pockmark surveys were conducted to detect cases that might have been missed. Only 1 case was found, which had occurred in mid-1970, some 6 months before the last 2 cases were recorded. (This case does not appear in the official records and is not included in Table 20.4 or Table 20.6)
In summary, only 6 cases of smallpox were officially reported by Southern Rhodesian health staff during 1970-1971. Later, another 49 cases were discovered during special surveys in Malawi and I further case in Southern Rhodesia. Such investigations as were carried out suggest that persistent transmission may have continued throughout 1970 and possibly during the early months of 1971 in border areas of Mozambique as well as in Malawi and Southern Rhodesia. At all events, the number of cases was undoubtedly substantially greater than the official records indicate.
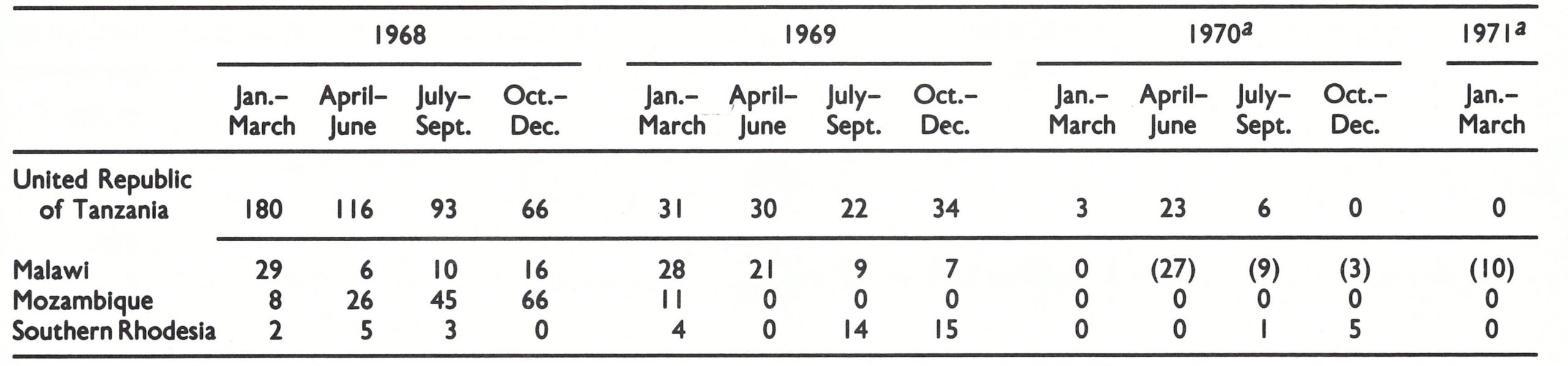
Table 20.6: United Republic of Tanzania, Malawi, Mozambique and Southern Rhodesia: number of cases of smallpox, by 3-month period, 1968-1971
a() = Cases by month of onset, discovered during 1972 and 1977 surveys.
Age Distribution of Cases
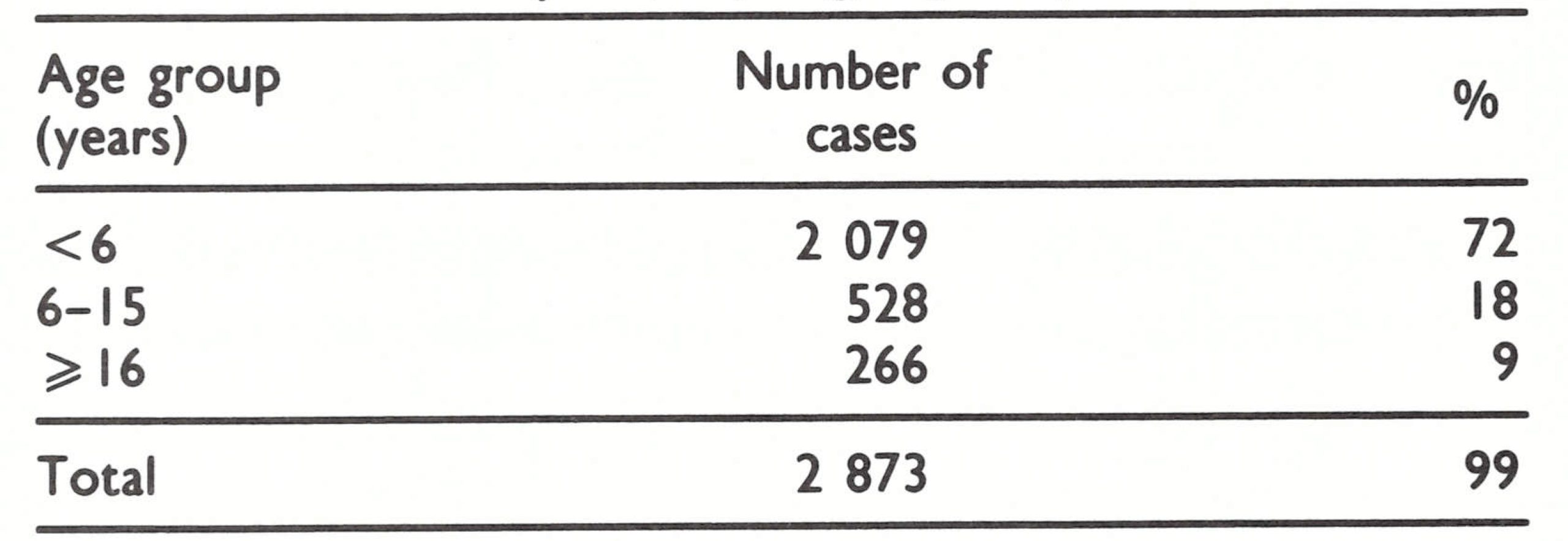
Information regarding the age distribution of cases is available for only a proportion of the cases from Malawi during 1960-1965 (Table 20.7) and for all of those in Mozambique in 1968 (Table 20.8).
Cases in Malawi occurred predominantly among children—a characteristic of endemic smallpox—during the period 1960-1965. In Mozambique during 1968, a larger proportion of cases was found among older persons, perhaps reflecting the fact that many cases occurred among more isolated groups living in sparsely settled areas. However, because reporting in both countries was incomplete, these data must be interpreted with caution.
Table 20.7: Malawi: number of reported cases of smallpox, by age group, 1960-1965a
 aData by age group not available for 1422 other cases reported during this period.
aData by age group not available for 1422 other cases reported during this period.
Table 20.8: Mozambique: number of reported cases of smallpox, by age group, 1968
SOUTH AFRICA, BOTSWANA, LESOTHO, NAMIBIA AND SWAZILAND
Background
South Africa, Botswana, Lesotho, Namibia and Swaziland are closely related geographically as well as by trade and commerce. South Africa is by far the largest of these countries, with a population of 22.8 million (in 1970).
The others had a combined population of only 3.2 million, many of whom were employed in South Africa, principally in mining, or travelled there regularly. An extensive, well-developed network of health services, roads and communication facilities extended throughout South Africa; the other countries had fewer resources of this kind.
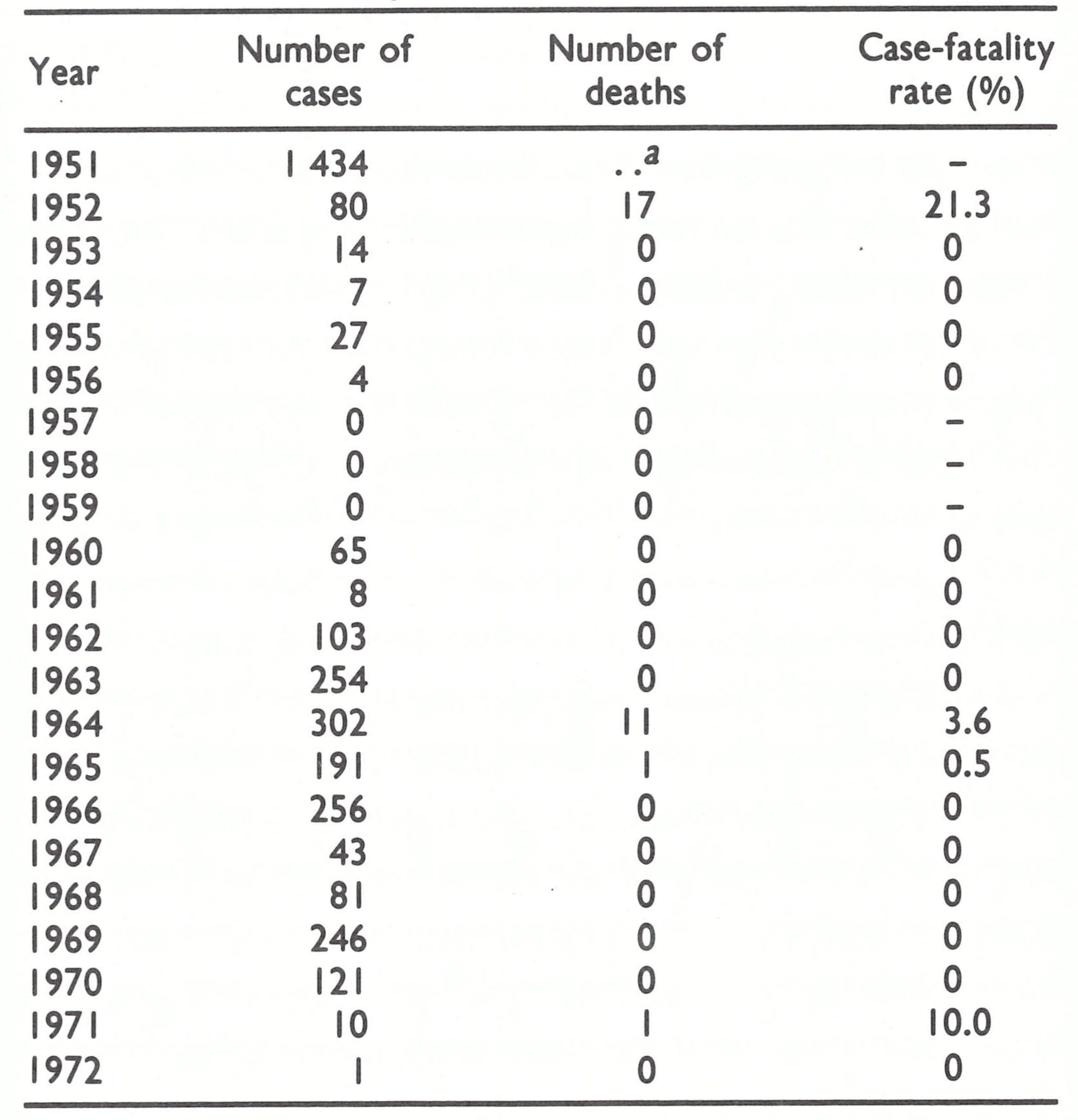
The persistence of endemic smallpox in this part of southern Africa can be attributed primarily to the fact that, for more than 50 years, the predominant type of smallpox had been a form of variola minor which was even less severe and with a lower case-fatality rate than that in the Americas. Described first in South Africa in the late 1800s, it was known as “amaas” or “kaffir-pox” (see Chapter 5). Its mild character is illustrated by the fact that from 1922 to 1944, 9122 cases were notified in South Africa but only 17 deaths were recorded. Between 1945 and 1952, however, case-fatality rates tended to approach those associated with variola major in African countries to the north. But after 1952, variola minor again displaced variola major. From 1953 to 1971, only 13 deaths attributed to smallpox were reported, of which 11 occurred in 1964 (Table 20 .9) during an outbreak of 54 cases in Port Elizabeth, Cape Province. This outbreak was attributed to an importation from Zambia. Evidence that the low casefatality rate was not an artefact due to incomplete recording of deaths was provided when variola minor spread from South Africa to Botswana in 1971. There, cases and deaths were much more carefully documented. Of 1122 patients, only 2 died.
Continuing vaccination campaigns employing liquid vaccine produced in South Africa had been in progress in each of the countries for many decades. The programmes were intended primarily to prevent largescale outbreaks of variola major should it be reintroduced rather than to control the relatively innocuous variola minor, against which the vaccine also provided protection.
Until 1972, little information regarding the epidemiology of smallpox and the control programme in South Africa was available to WHO. That which was available was gleaned from a monthly infectious diseases bulletin published by the government and occasional reports of outbreaks sent to WHO by the Secretary of Health, in partial conformity with the International Health Regulations. Information regarding the geographical distribution of cases would have been helpful but the reports listed cases only by month and by racial group.
Data from South Africa, such as they were, were regularly included in published reviews which appeared in the Weekly epidemiological record. As country after country in Africa became free of smallpox, South Africa’s dubious distinction as one of only a few endemic countries became politically intolerable to its authorities. Although the disease was not a public health problem, South Africa began to take an interest in smallpox in 1970 and commenced an intensive vaccination campaign in the endemic areas. Surveillance was incomplete, and it is therefore uncertain when transmission was actually interrupted. The last known endemic case occurred on 3 May 1971.
Only a few months later, neighbouring Botswana began to detect cases. Perfunctory control measures were taken but smallpox continued to spread. Not until May 1972, almost a year later, was an adequate programme begun. By then, the disease had spread widely across the country. Smallpox persisted in Botswana until November 1973.
Table 20.9: South Africa: number of reported cases of and deaths from smallpox and casefatality rates, 1951-1972
 a..= data not recorded.
a..= data not recorded.
Lesotho, Namibia and Swaziland
Events in South Africa and Botswana are described in greater detail later in this chapter. Smallpox occurrence and programme activities in Lesotho, Namibia and Swaziland may be briefly summarized. Namibia (population in 1970, 1.04 million) was one of the most sparsely inhabited countries in southern Africa; its last known case of smallpox was reported in 1956. Vaccination programmes employing mobile teams which administered poliomyelitis and BCG vaccines as well as smallpox vaccine were well established and had been operative for many years. Because smallpox transmission had been interrupted throughout western South Africa and Angola by 1960 and in Botswana in 1964, the risk of importations was small. Even the 1971-1973 epidemic in Botswana posed little threat because the outbreaks were concentrated in the eastern part of that country, separated from population centres in Namibia by hundreds of miles of desert. Consequently, no special activities were undertaken in Namibia during the Intensified Programme.
Swaziland was first visited by Ladnyi in 1968 and Lesotho in 1970 to assess the status of their activities and to offer such assistance from WHO as might be required. Lesotho (population in 1970, 1.06 million), after many years of freedom from smallpox, experienced an outbreak of 84 cases in 1961. The outbreak extended through June 1962, 52 cases being reported that year. No deaths occurred. In 1961, 700 000 persons were vaccinated in a 3-month mass campaign and, thereafter, mobile teams supported by UNICEF vaccinated between 50 000 and 150 000 people each year, administering liquid smallpox vaccine simultaneously with BCG vaccine. In 1970, WHO began to provide freeze-dried smallpox vaccine for the programme. No further cases were found. Swaziland (population in 1970, 426 000) began experiencing smallpox outbreaks in 1963, its first since 1950. From 1963 to the end of 1966, 182, 517, 85 and 73 cases were notified for the respective years, but only 9 deaths were reported during the entire period . How many of these were genuine cases of smallpox is unknown. Of a series of 73 cases diagnosed as smallpox by auxiliary health workers, 55 were sent to hospital but none was confirmed clinically as smallpox by the physicians who saw them. In areas in which outbreaks occurred, between 44 000 and 90 000 vaccinations were performed each year from 1963 to 1966, using liquid vaccine produced in South Africa. In September 1967, a UNICEF-assisted mass vaccination campaign began, employing BCG and freeze-dried smallpox vaccine. Between 1967 and 1972, when the mass campaign concluded, between 34 000 and 64 000 persons had been vaccinated each year. Thereafter, vaccination was performed by the health centres. A survey in 1970, 3 years after the programme had started, revealed that only 51% of persons under 15 years of age and 20% of those aged 15 and over had vaccination scars. The year in which smallpox transmission was interrupted in Swaziland is unknown. Twenty-five cases were reported to WHO in 1967, 20 in 1968, and 24 in 1969. Because of this, Swaziland was originally listed as an endemic country. However, government records reviewed during certification activities show no cases after 1966 and no one at that time could be found who knew anything about the cases that were said to have occurred between 1967 and 1969. Whether these cases represented clerical error or were indeed cases of smallpox could not be ascertained. As in most countries of southern Africa, smallpox transmission had ceased spontaneously during the course of an indifferently executed vaccination campaign. When surveillance programmes eventually began, no cases could be found.
South Africa
Richly endowed with natural resources and with a large and expanding industrial base, South Africa had many of the attributes of developed countries in temperate climates. Almost half of South Africa’s population of 22.8 million (in 1970) lived in urban areas. Preventive health services were administered by regional medical directors, 2 of whom were assigned to the 2 larger provinces (Cape and Transvaal) and 1 each to the 2 smaller (Orange Free State and Natal). They, in turn, oversaw the work of medical officers of health in each local authority. The pattern of vaccination activities differed somewhat from province to province but, in general, all provided vaccine through health centres and clinics, and supplemented this in rural areas by mobile teams which performed vaccinations at collecting points. Poliomyelitis, smallpox and BCG vaccines were administered to young children and smallpox vaccine to older children and adults. The smallpox vaccine, until 1970 a liquid vaccine, was produced at the State Vaccine Institute in Cape Town. Vaccination was also given to all children at school entry, and to the 100 000 or so men who came each year to work in the mines. From 1968 to 1975, between 600 000 and 900 000 persons received smallpox vaccine each year through government facilities. The number of vaccinations was small in proportion to the population, but the total did not include those, said to be many, that were provided by private physicians.
Reporting from the more than 10 000 health units which regularly saw patients was thought to be reasonably good, but because smallpox in South Africa was so mild, the government authorities believed that many persons with smallpox did not seek medical attention and so did not come to the attention of the health services. Teachers and heads of families were also supposed to report cases when they occurred but their level of compliance was uncertain, especially in areas in which religious sects objected to vaccination of any type.
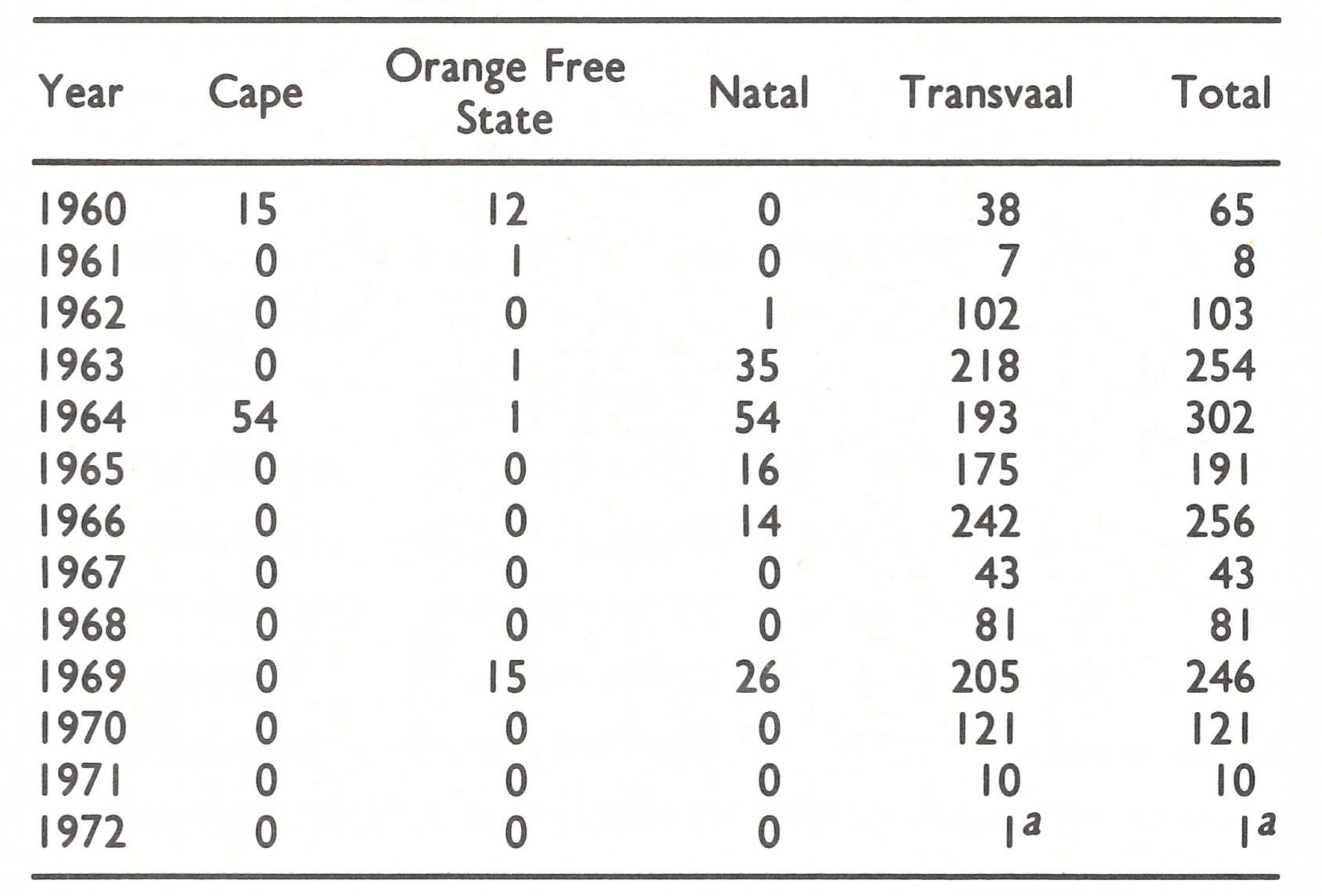
Information about smallpox was very incomplete for other reasons. Responsibility for health problems, as well as the investigation and control of outbreaks of smallpox and other diseases, was regarded as a provincial responsibility, and in the provinces, as mentioned above, this function was primarily discharged by local medical officers of health. Diligence in the investigation of cases and the conscientiousness with which notifications were forwarded varied from area to area. Since the mild variola minor caused the provincial health authorities little concern, not much time was devoted to the investigation or control of outbreaks. The problem was compounded by a national morbidity reporting system considered to be so unsatisfactory that in 1970 a complete restructuring of the system was begun. Pending completion of this effort, national morbidity reports ceased to be published in March 1970. Until 1978, further data regarding cases and their geographical location, as notified nationally, were not made available to WHO. When reviewed by WHO in 1978, reports revealed that the Transvaal accounted for most of the cases after 1960 and for all but 41 of the 502 cases reported after 1966 (Table 20.10).
Table 20.10: South Africa: number of reported cases of smallpox, by province, 1960-1972
 a Case imported from Botswana.
a Case imported from Botswana.
South Africa reported only 43 cases to WHO during 1967, and 81 cases in 1968 . Because so few cases were being reported in a country in which health services were so extensive, WHO had originally assumed that these cases must have occurred following importations and had provisionally classified South Africa as a non-endemic country.
In 1969, however, the number of reported cases increased (Fig. 20.6 ; Table 20.10). Because communication with South Africa through the usual official channels was not possible, Henderson addressed a personal letter to the Secretary for Health on 27 August, noting that as of that date: “South Africa now accounts for about 10% of all cases recorded in Africa this year” and asking for a fuller statement of the epidemiological situation as well as a description of the problems being encountered in controlling spread. By the end of that year, 246 cases had been reported to WHO.
A reply was not received until February 1970. In his letter addressed to Henderson at WHO, the Director of Medical Services showed a dismaying lack of understanding of the epidemiology of smallpox. He asserted that the cases were sporadic and explained that, with variola minor, “very mild undetected cases and subclinical cases, harbouring the virus in their tonsils, the lymph follicles of the tongue and pharynx are liable to spread the disease to every person not vaccinated against smallpox. Due to this mode of spread, a population with a successful vaccination rate of more than 80% is not protected.” He indicated that mass vaccination would continue in order to limit the spread of disease. In reply, Henderson pointed out that in Brazil, in which variola minor was also endemic, “smallpox is transmitted only by cases with definite lesions of smallpox and during the period . . . of rash . . . and that 80-90% of cases can be traced to personal contact in a house.” The favourable experience of other countries in investigating and containing each outbreak was noted and procedures for outbreak containment were described. What effect this correspondence had is unknown.
As it was later learned, the most important stimulus which precipitated a more vigorous programme in South Africa was the WHO Director-General’s report on smallpox eradication, prepared as a document (EB45/16 ; dated 1 December 1969 but never published in WHO’s Official Records) for the fortyfifth session of the Executive Board in January 1970 and obtained by South Africa. The report stated:
“Of the endemic countries in Africa, South Africa and Ethiopia are the only ones which have not yet initiated eradication programmes . The number of cases recorded this year by South Africa more than doubled [246 cases in 1969 compared with 81 cases in 1968] . . . However, little additional information is available . . . The continuing reservoir of smallpox in South Africa and Ethiopia is of increasing concern to neighbouring countries, most of which have become, or are rapidly becoming, smallpox free . . . With only three known exceptions, freeze-dried vaccine of satisfactory potency, stability and purity is now used in all endemic countries. However, in South Africa, liquid vaccine continues to be employed . . .”
South African health officials were angered by the report, considering it to be unfair for three reasons. The first was that the report and the tables of data referred to smallpox only generically, drawing no distinction between the severe variola major of Asia or many other countries of Africa and the mild form of variola minor present in South Africa. This, however, had been a policy followed by WHO since the inception of the programme because the mandate of the World Health Assembly was the eradication of smallpox of whatever variety. The second was the issue of whether or not South Africa could be said to have an eradication programme. As the health authorities viewed it, an effective vaccination campaign was being conducted throughout the country and local authorities were expected to control outbreaks when these occurred. In WHO’s view, however, an eradication programme had as its objective the complete interruption of smallpox transmission, an unrealistic aim as seen by the South African Director of Medical Services. The third reason was the emphasis on the use of freeze-dried vaccine-clearly of importance in tropical countries in which ambient temperatures were high and refrigerated storage was scarce. In South Africa, however, ambient temperatures were not so high and refrigerated storage for vaccine was not considered a problem. WHO’s emphasis on the need for freeze-dried vaccine in endemic areas was based on the recognition that even when refrigerated storage was adequate, health and medical personnel, even in industrialized countries, often failed to preserve vaccines properly.
Although highly sceptical that other African countries were making as much progress as was claimed, the South African health authorities decided early in 1970 to take additional measures to control smallpox and, by so doing, avoid the expected criticism of other independent African countries. A special programme was launched to produce large quantities of freeze-dried vaccine; by May, all mobile vaccination teams were using this. The vaccine was said to meet WHO standards although it was not examined by a WHO reference laboratory. By the end of 1970, liquid vaccine was being provided only to private practitioners.
In June 1970, an intensified systematic vaccination campaign was begun in the northern Transvaal, from which most smallpox cases were reported. It was termed a house-to-house campaign although, for convenience and efficiency, vaccinators usually assembled persons from a group of neighbouring houses. By the end of the year, more than 350 000 persons had been vaccinated. This represented only a small proportion of the 6.3 million people then resident in the province, although coverage in the infected but sparsely populated northern areas was said to be high.
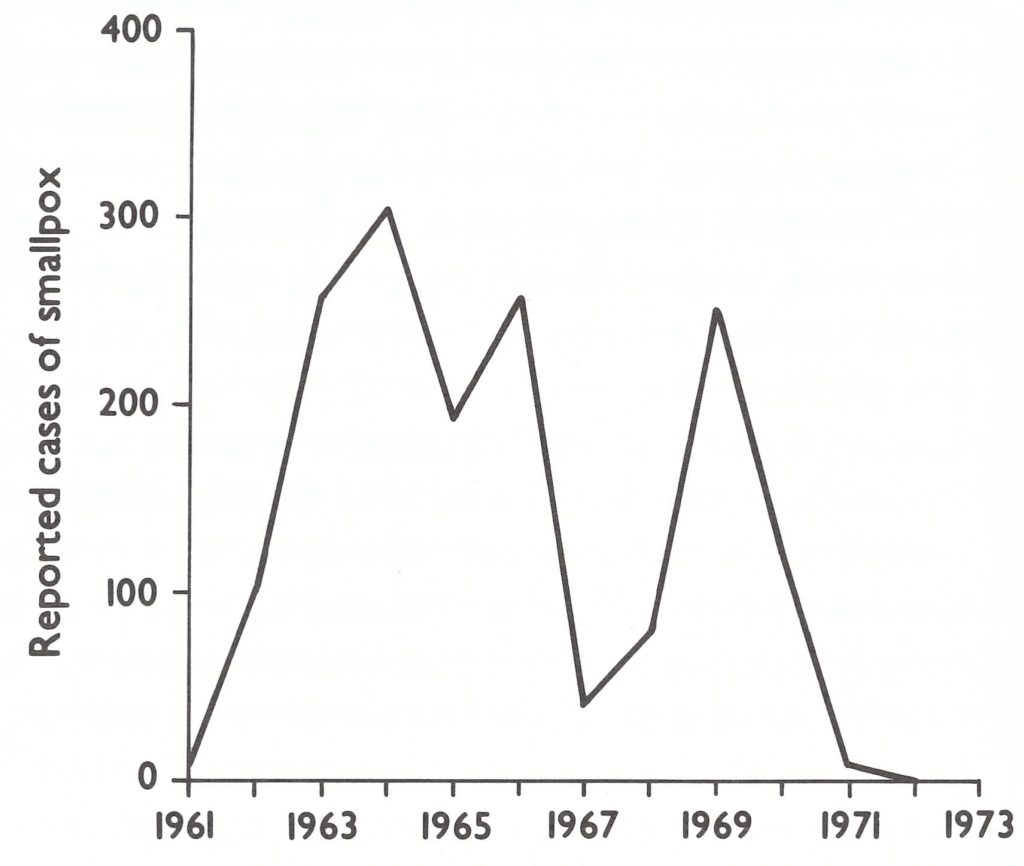
Fig. 20.6. South Africa: number of reported cases of smallpox, by year, 1961-1973.

Fig. 20.7. Southern Africa: areas known to have had endemic smallpox, 1970-1971.
By the end of June 1970,117 cases had been reported to WHO, but thereafter none was notified until December (4 cases) and again in January 1971 (7 cases). As was learned only much later by WHO, all were in the Transvaal, not far from the border with Botswana (Fig. 20.7). Reports from South Africa then ceased. Repeated inquiries were made by WHO officials and others in South Africa after January 1971, under the provisions of the International Health Regulations, asking for confirmation that no further cases had occurred, but there was no response. It was unclear whether there were indeed no cases or whether the government had decided not to report any more cases of smallpox to WHO.
In June 1971, Botswana reported a case of smallpox in Gaborone, the capital, but 2 weeks later asserted that the case had actually been chickenpox. In August, additional cases were reported and these were confirmed as smallpox by laboratory examination. The information was promptly relayed to South Africa and Southern Rhodesia, and teams from both countries immediately went to border areas to conduct intensive vaccination campaigns. The Botswana outbreak continued but only 1 case is known to have been reimported into South Africa-in a labourer who became ill on 14 February 1972.
The question of concern in the autumn of 1971 was how and where smallpox transmission was being sustained in the South AfricaBotswana area. As has been noted, South Africa had reported 11 cases during the 2-month period, December 1970 to January 1971, after 5 months during which no cases had been notified. Following this, 7 months had elapsed before cases were confirmed in Botswana. It was certain that many additional cases had occurred during these two intervals in order to sustain the chain of transmission. Discovery of the infected area was important. Botswana, whose surveillance system was poor, was a candidate area but, because of the letter from South Africa’s Secretary for Health, the programme in the latter country had to be regarded with suspicion. WHO Headquarters staff believed it imperative that a visit should be made to South Africa, as well as to Angola and Mozambique, to assess the situation. This was proposed on the grounds that such contact with South Africa was permissible under the terms of a resolution adopted by the WHO Executive Board (EB45.R20), endorsed by the Twenty-third World Health Assembly in resolution WHA23.46, which had requested the Director-General “to continue to take all necessary steps to assure the maximum co-ordination of national and international efforts”. This, it was felt, implied licence to visit South Africa. The proposal was discussed at length and eventually agreement was reached between WHO and the South African government that Henderson should visit South Africa, which he did in June 1972.
In the Transvaal, he found a well-organized vaccination campaign in progress, with attention being given to the detection and laboratory confirmation of suspected cases. During 1972, only a single importation from Botswana had been detected, but health officials were alert because they believed there would be more if not from Botswana, perhaps from Angola or Mozambique, which they believed continued to harbour endemic smallpox even though neither reported cases.
However, when Henderson endeavoured to obtain epidemiological data regarding the cases reported in 1971, it became apparent that there had been many more cases of smallpox than had been reported to the national authorities. Official records at that time showed only the 7 cases which had occurred in January 1971, in a hospital some 300 kilometres from the border with Botswana. On the other hand, -a review of records at the National Institute for Virology, Sandringham—the diagnostic reference centre—showed 10 poxvirus isolations during 1971, the last from a patient who became ill on 3 May 1971.
The laboratory itself, well equipped and well staffed, was in part inadvertently responsible for problems in smallpox control. It employed an unorthodox approach to the examination of specimens. Standard virological technique called for the isolation of virus on the membrane of fertile hens’ eggs. By visual examination of the pocks that grew, variola virus could readily be distinguished from vaccinia virus. At the Institute, the specimens were grown in tissue culture in which, if virus growth occurred, it was impossible to discriminate with certainty between variola virus and vaccinia virus. Accordingly, the laboratory reported only whether or not a virus of the “vacciniavariola virus group” had been isolated. The laboratory director’s view was that whoever sent the specimen should be able to make a clinical distinction between smallpox and disseminated vaccinia, and thus he saw no need to differentiate the viruses by laboratory study. Recipients of the reports, however, sometimes misinterpreted them and reclassified cases of smallpox as vaccinia.
Cases and outbreaks were notified to the regional medical directors by local health officials, who controlled any outbreaks that were found with varying levels of diligence. At neither the national nor the provincial level was there a health official responsible for ensuring that the outbreaks were properly investigated and contained. In no instance had an effort been made to trace the spread of smallpox or to define endemic areas. Reports of variola virus isolations by the reference laboratory were made known only to the persons submitting the specimens; provincial officials were not provided with copies of the reports.
Following Henderson’s visit in June 1972, health officials endeavoured to reconstruct the epidemiological pattern of spread of smallpox during 1971. This was important, for if it could be shown that the cases had been closely related and the outbreaks contained, there would be greater assurance that South Africa by 1972 was indeed free of smallpox. Conversely, if the cases had been scattered and unrelated to each other, widespread and perhaps continuing endemicity was implied.
The investigations eventually revealed that smallpox had indeed persisted in South Africa until at least May 1971, all the cases occurring after February having acquired the infection at a hospital about 100 kilometres north of Pretoria, in the Transvaal. As far as the outbreak could be reconstructed, 3 unvaccinated children from a village 30 kilometres distant were hospitalized with typical smallpox in January and February 1971 and the diagnosis was confirmed by virus isolation. The mother reported that her other 4 children, as well as a number of children in the vicinity, had been ill with a similar disease. Three additional children from the same village were admitted with smallpox during January and February, although no specimens were collected. On 26 March, a child hospitalized with tuberculous meningitis and receiving steroid therapy developed a rash at first thought to be druginduced. Specimens were taken and the National Institute for Virology reported the isolation of a virus of the vaccinia-variola group. The report was misinterpreted and it was concluded that the child had experienced disseminated vaccinia. The patient died on 3 April. Three additional cases occurred in previously hospitalized children on 12,14 and 19 April respectively, all of which were confirmed by virus isolation. The Regional Medical Director, who was asked to investigate, reported as follows:
“The suspected outbreak has occurred in the TB ward. One death [not officially notified] is attributed to the disease which had been diagnosed also in 3 other children who were examined . In addition, 3 cases of healing chickenpox were examined. According to my information, the latter disease has been “endemic” amongst children in this ward for many months. That is to say chickenpox has been diagnosed also amongst other children who have no visible lesions now and also in children who have been discharged already . . . Vaccination of patients and personnel . . . carried out 7 April did not give a satisfactory percentage of takes . . . The ward was placed in quarantine only this week. Therefore, a list was compiled of all inmates and also of all patients discharged . . . The homes of all will be visited by departmental field staff.”
A large hospital-based outbreak of smallpox and possibly of chickenpox had obviously been in progress for at least 2 months. Extensive vaccination campaigns were conducted subsequently in the many areas from which the hospital patients had Table 20.11. Botswana: number of reported cases come. Three additional cases were found, all of whom had been infected at the hospital: a child who had been hospitalized became ill on 3 May, and 2 labourers who had been seen in the outpatient department 2 weeks earlier became ill in March on a farm 100 kilometres distant . In all, 10 cases and 1 death appear on the official records for 1971 but, as is apparent from this account, there were at least 20 cases and possibly many more. Fortunately, the outbreak occurred at the end of the summer, the low point in seasonal transmission, so that despite greatly delayed containment measures, smallpox spread slowly and transmission was soon interrupted.
In South Africa, as in other countries of southern Africa, extensive vaccination rather than an organized surveillance-containment programme served to interrupt transmission. During the continuing vaccination campaign, no further cases were detected and none was reported by the 11 000 reporting units. Among 77 specimens submitted to the laboratory over the period 1972-1977, only 1 further isolation of the “vaccinia-variola group of viruses” was made, the specimen concerned being from the case (see above) that was imported from Botswana in 1972.
Botswana
Botswana, which became independent in 1966, is large but sparsely populated, the great Kalahari desert extending over the southwest portion of the country and occupying more than half the land area. Over 80% of its population of 623 000 (1970) lived along a strip of land in the south-east, not more than 200 kilometres wide, adjacent to the Transvaal Province of South Africa. Travel between Botswana and South Africa was frequent ; population movement within the country was extensive and followed an unusual pattern. A large proportion of the population maintained 3 dwellings: one in a village, a second at a cattle post and a third in a farming area. Family members spent time each year in the different locations, which were often widely separated. Moreover, an estimated one-third of the adult males left rural areas each year seeking employment in the country’s urban areas or in South Africa. Government health facilities were comparatively numerous; in 1966 there were 7 hospitals, 73 clinics and 65 health posts Several missionary groups also provided medical care.
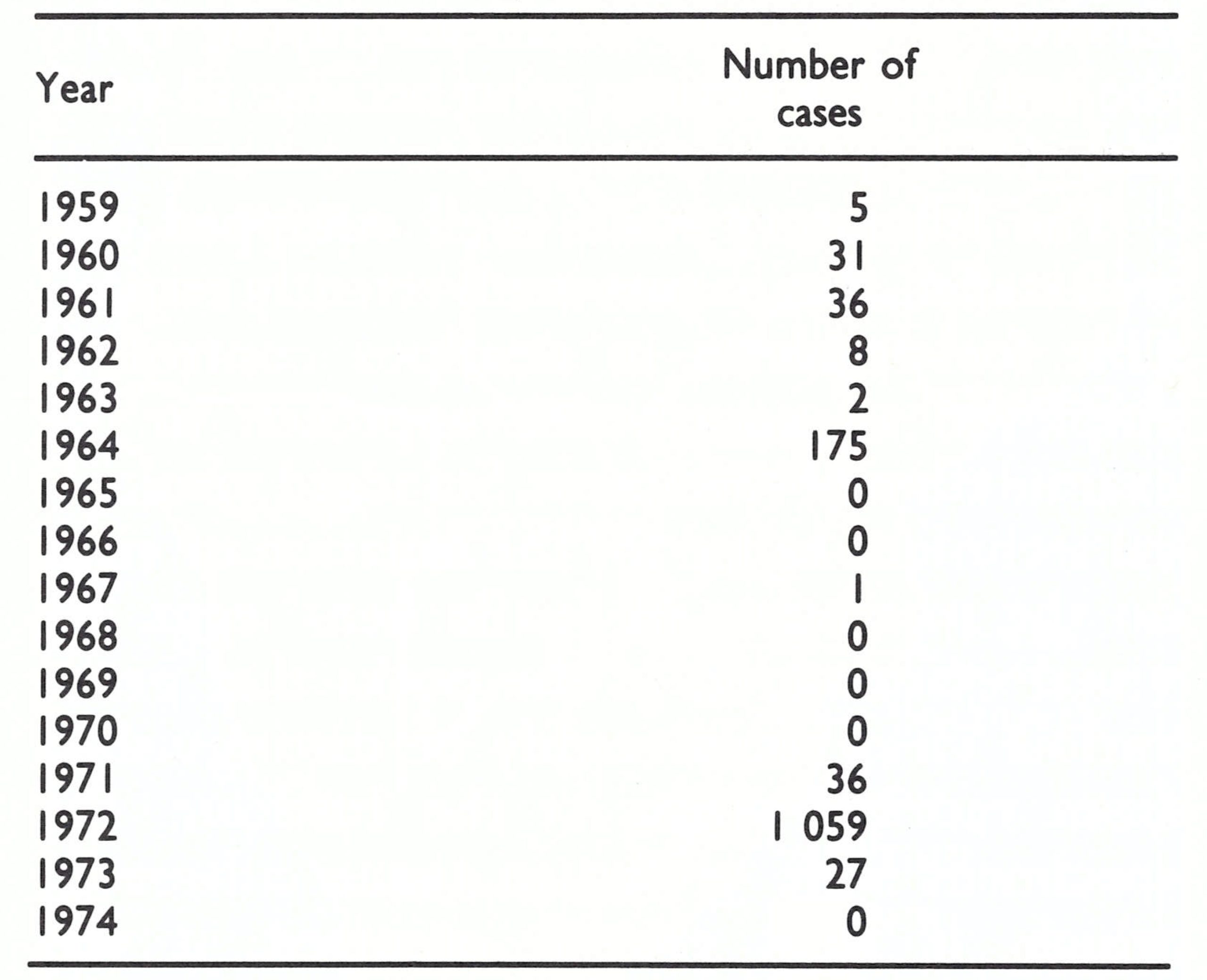
In this small and scattered but highly mobile population, smallpox was characterized by periodic outbreaks followed by long intervals with few or no cases. An outbreak of 175 reported cases and 34 deaths in 1964 was controlled by a mass vaccination campaign and during the following 6 years only 1 case was notified (Table 20.11).
Because Botswana was believed to be smallpox-free when the Intensified Smallpox Eradication Programme began and because adjacent countries were reporting few or no cases, the development of a special programme was not considered by WHO to be of high priority—if it was required at all. As time passed, the apparent need for a programme diminished. Neighbouring Namibia and Angola reported no cases and Zambia became smallpox-free in 1968. The only other adjacent countries notifying cases, South Africa and Southern Rhodesia, reported so few in 1967-1968 that WHO suspected that they were the result of importations rather than of endemic transmission. By the end of 1969, however, the number of reported cases in South Africa had increased so greatly that it seemed certain that endemic smallpox was present there. Although the government informed WHO that some of the cases were in Transvaal Province, their exact whereabouts were not revealed. Only in 1972 did it become known that virtually all the reported cases had occurred in the Transvaal, many near the border with Botswana.
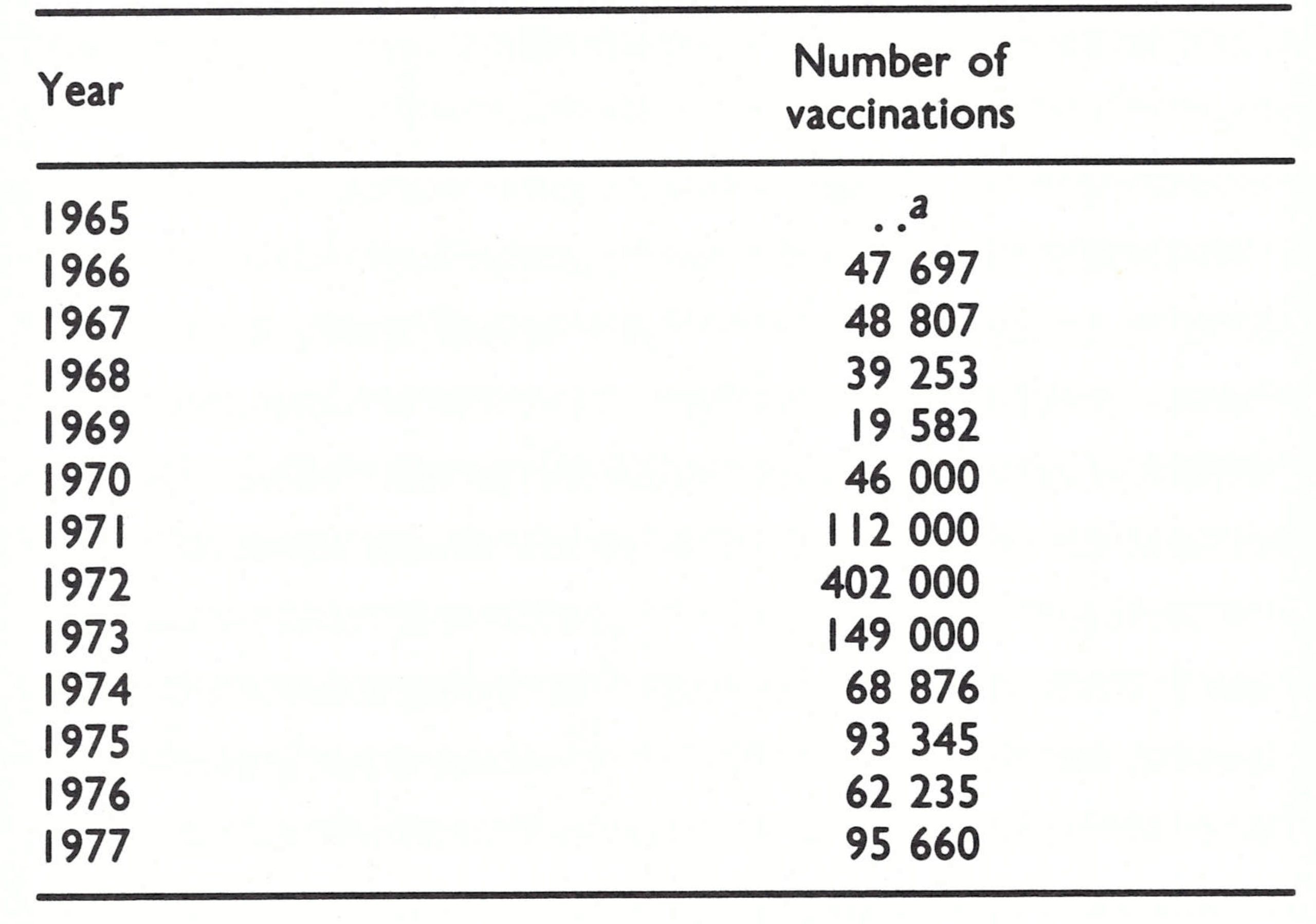
Ladnyi paid his first visit to Botswana in January 1971 to discuss the status of its vaccination campaign and the assistance that WHO might be able to offer. After Botswana’s mass vaccination campaign of 1964, some vaccination activities had continued (Table 20.12). Liquid vaccine from South Africa had been employed up to the end of 1969, and thereafter freeze-dried smallpox vaccine, also purchased from South Africa, was used. Vaccinations were given by mobile teams in 3 of the 6 health districts and offered by hospitals and clinics throughout the country. However, the health facilities for the most part vaccinated persons leaving for South Africa and Zambia, both of which countries required certificates of vaccination. The number vaccinated each year was equivalent to no more than 5-10% of the population. The proportion of successful vaccinations is unknown but was probably not high even when freeze-dried vaccine began to be used. The freeze-dried vaccine was provided in 100-dose containers and was normally used for 1-2 weeks after reconstitution, although its potency would have fallen to nil within 2-3 days.
Table 20.11: Botswana: number of reported cases of smallpox, 1959-1974
 a Case imported from Botswana.
a Case imported from Botswana.
Table 20.12: Botswana: number of smallpox vaccinations performed, 1965-1977
 a..=data not recorded.
a..=data not recorded.
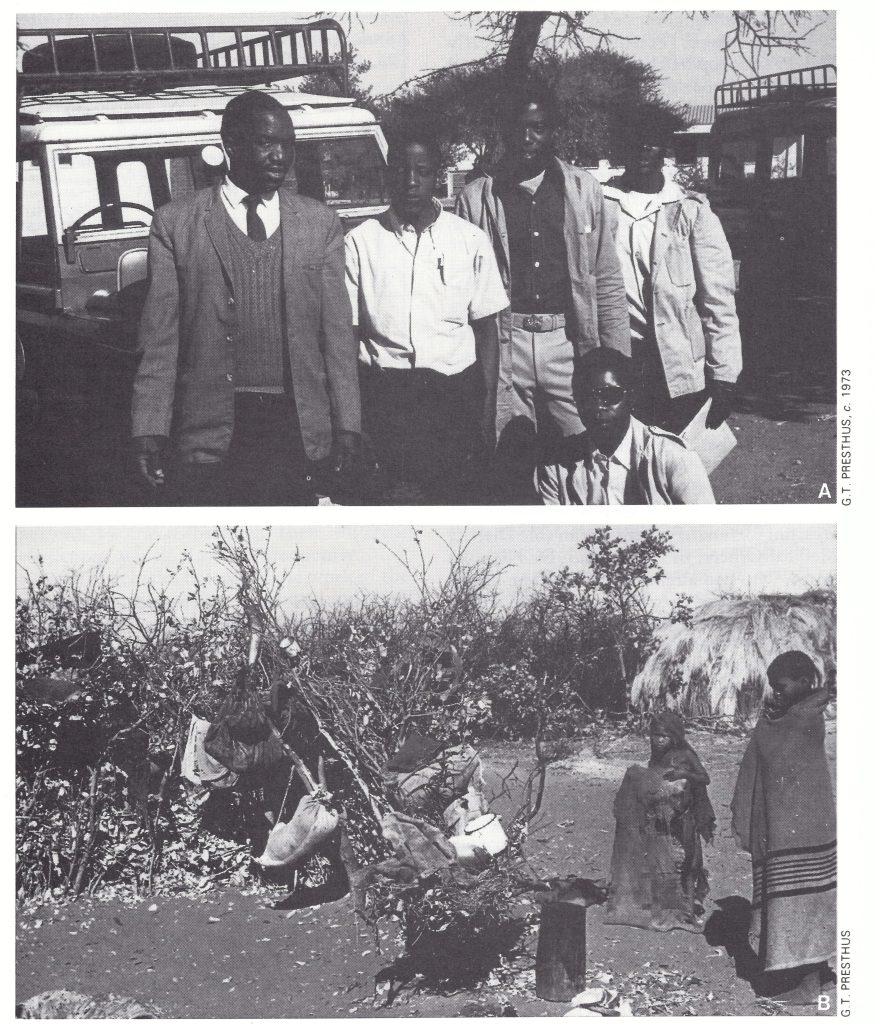
Plate 20.3. A: Joseph B. Sibiya (far left), Senior Health Inspector, with one of Botswana’s 4 surveillance teams. B: Many cases of smallpox were discovered in remote cattle posts in the Kalahari desert by the teams.
Ladnyi found that 80% of the pre-school children had no vaccination scar, and in a school near the capital whose pupils had recently been vaccinated by a mobile team, only 136 of 334 children (41%) had a vaccination scar. Better handling of the vaccine was obviously needed and he provided appropriate advice.
Ladnyi was concerned that smallpox might be imported, and his principal recommendation was that every suspected case of smallpox should be treated as an emergency and all necessary containment measures carried out with a minimum of delay. He recommended that a specimen should be taken from each 20. SOUTHERN AFRICA 98 9 suspected case and sent to WHO Headquarters for examination; meanwhile the suspected case should be dealt with as though it were smallpox. In a country in which vaccinial immunity was so low, there was a special need for prompt action. The government requested vehicles and vaccine in support of the programme, a request which was forwarded to the WHO Regional Office for Africa.
On 1 June 1971, only 5 months after Ladnyi’s visit, a cable was received in Geneva from Botswana reporting a case of smallpox. At that time, no cases had been reported from anywhere in southern Africa since January, although it was learned later that cases in South Africa continued to occur through May. Cables sent on 4 and 8 June from Botswana indicated that the case was in a patient already hospitalized in Gaborone, and that it had been confirmed virologically at South Africa’s National Institute for Virology.
Urgent action was indicated. However, permission for WHO Headquarters staff to visit a country required the prior agreement both of the WHO regional office concerned and of the country itself. Henderson immediately telephoned the regional office in Brazzaville to point out the urgency of rapid containment and of a thorough investigation and to propose that an experienced epidemiologist from Headquarters should visit Botswana immediately. The regional office contacted Botswana and, on 16 June, reported that a cable had been received from the government indicating that the situation was misunderstood, that the case had turned out to be chickenpox, and that no visit was required. A return telex from Geneva to Brazzaville again urged an early visit by a WHO adviser in view of the fact that the case was said to have been confirmed by laboratory investigation. The regional office replied that such a visit was not considered advisable.
On 27 August, additional cases of smallpox were reported from Botswana, and specimens were sent by the government direct to Geneva. By 6 September, the WHO Regional Reference Centre for Smallpox in Atlanta, USA, had confirmed the isolation of smallpox virus. This caused a flurry of telex messages and letters between Geneva and Brazzaville. Headquarters staff repeatedly urged an emergency visit by Arita, pointing, out that the Botswana focus presented a continuing threat to Botswana as well as neighbouring countries and noting that this was clearly as much an international as a national problem. The regional office requested more information from Botswana and asked whether WHO assistance was required.
On 7 September 1971, a letter was received in Geneva addressed to the Chief of the Smallpox Eradication unit from the Director of Medical Services of Botswana. Contrary to the cabled information received by the regional office, he reported that in May a 3-year-old child, hospitalized for tuberculosis, had developed smallpox and that a second case had been detected in a government employee in Gaborone on 16 August. Specimens from both had been confirmed as “vaccinia-variola type virus” by the South African National Institute for Virology. The second case had been vaccinated during a June vaccination campaign in Gaborone but showed no scar. The Director of Medical Services noted that ” . . . no source of infection has been identified. There must, however, be a focus of infection somewhere”.
On 20 September, Botswana requested a supply of freeze-dried vaccine which was immediately sent from Geneva and an operations officer to organize a vaccination campaign. However, as a new intercountry smallpox adviser, Dr Islam, had just replaced Ladnyi, whose current term of service in WHO had expired, he was sent instead. Unfortunately, despite his experience in the control of communicable diseases, he had not yet had direct experience with smallpox eradication and had not yet been briefed regarding techniques for surveillance and containment.
He arrived for a 15-day visit on 8 October by which time 3 additional smallpox cases had been detected and a fourth suspected case had been admitted to hospital. He was unable to trace the sources of these cases. The cases he did identify were in people who presented themselves at the hospital, and he indicated that “there is strong evidence that a smallpox focus exists . . . in the southern part of Central District . . . the investigations do not support the notion of recent importation”. A mass vaccination campaign was said to have been conducted but, in fact, only 38 600 vaccinations had been recorded between January and August 1971. In the area of the smallpox focus, he found that 80% of 1767 primaryschool children and 60% of 541 pre-school children had vaccination scars. In adjacent areas, however, only 20% of those aged 0-6 years had ever been vaccinated. He recommended a mass vaccination campaign in the primarily infected area, offered advice to the government regarding vaccine handling and vaccination technique and stressed the importance of surveillance. At this time, these were the only known cases of smallpox in the entire WHO African Region, the other countries in the African continent in which the disease was still endemic, Ethiopia and the Sudan, both then being in WHO’s Eastern Mediterranean Region.
Cases continued to be reported from Botswana and all specimens sent for examination to the WHO collaborating centres were confirmed as smallpox, but no information was provided by the government as to what was being done to control the spread of the disease. Faced by frequent and increasingly urgent requests from WHO Headquarters to respond to Botswana’s request for an operations officer, the regional office could only reply that no action could be taken unless it received an official application from the government.
In November 1971, an unexpected opportunity arose that permitted direct communication with Botswana. Mr John Phillips, the Resident Representative of the United Nations Development Programme in Botswana, stopped in Geneva on the way back to his duty station. After a full discussion of the problem with WHO staff, it was agreed that he would discuss it with government officials and ask them to submit a formal request to the regional office for the immediate assignment of an operations officer. The request was made forthwith, and Dr Pierre Ziegler, in charge of smallpox eradication in Zaire, was asked to make available his most experienced operations officer, Mr Garry Presthus (see Chapter 18, Plate 18.5). His transfer was not, however, arranged until the end of February 1972, nearly 9 months after Botswana had notified its first case.
On arrival, Mr Presthus, with his counterpart, Mr J. B. Sibiya, Senior Health Inspector for Botswana, rapidly set in motion a mass vaccination campaign and a programme which, unique among the programmes of southern Africa, emphasized the prompt detection of cases and their containment through vaccination. More than 18 months would elapse, however, before transmission could be interrupted.
Within a month of his arrival, Mr Presthus had met the director of the Botswana Red Cross, Ruth Seretse Khama, to explain the importance of smallpox eradication in Botswana and its significance for the global programme. In mid-April 1972, her husband, Sir Seretse Khama, the President of Botswana, had signed a special bill allocating US$25 000 from the government budget. Although not a large sum in comparison with funds provided in some other eradication programmes, this represented a substantial commitment for Botswana. funds provided in some other eradication programmes, this represented a substantial commitment for Botswana.
Using such vehicles as could be borrowed from other programmes, Mr Presthus and Mr Sibiya formed 4 teams to contain outbreaks in known foci and to encourage the network of health facilities to begin vaccinating both people attending clinics and the inhabitants of nearby villages (Presthus, 1974). By early May 1972, forms had been prepared to be used for weekly reports from each health unit. Volunteers of all types offered assistance.
Field investigations conducted during March documented 36 cases which had occurred during 1971, the first in March near the South African border. Mr Presthus believed that there had been many more cases, but with new cases being detected daily there was no time to document further the previous year’s experience.
In 1972, the number of reported cases increased to 63 in April and to 66 in May (Table 20.13). In that month, one of the cases was reported from Ngamiland, in the northwestern part of the country, an area of great concern because of the frequent movement of rebel forces between it and areas in southeastern Angola which were only partially accessible to the government of Angola. A surveillance team was hurriedly sent to the area, but fortunately there was an able District Medical Officer, in Ngamiland, Dr Nicholas Ward, who had already organized the health staff for extensive vaccination and search activities. Only 5 other cases were eventually detected in Ngamiland. A year later Dr Ward was recruited by WHO, which he served with distinction in smallpox eradication work in Bangladesh and India.
Table 20.13: Botswana: number of reported cases of smallpox, by month, 1971-1974
 a() = Cases shown by month of onset. Most of these cases were not discovered until many months later.
a() = Cases shown by month of onset. Most of these cases were not discovered until many months later.
Table 20.15: Botswana: results of vaccination scar surveys, by age group and district, January-March, 1973
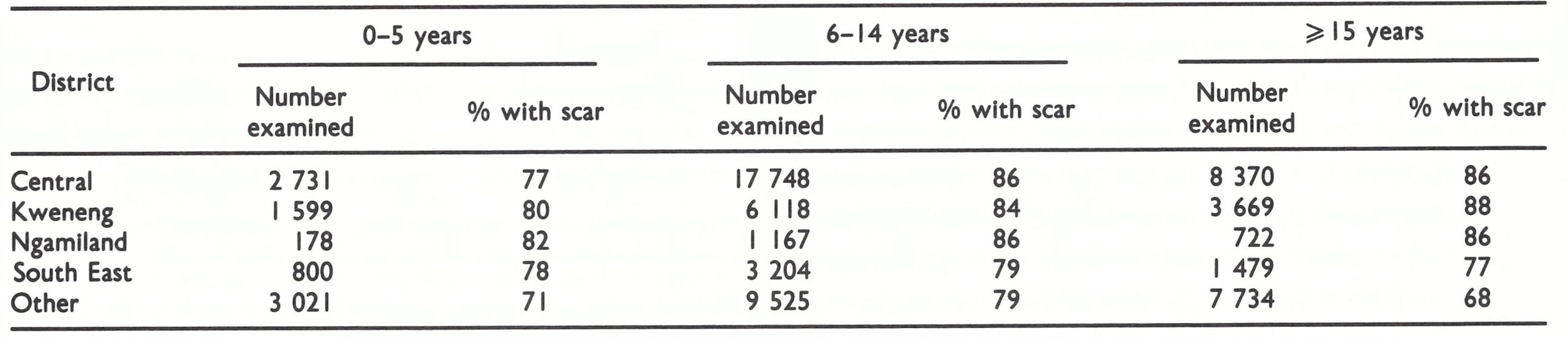
The increase in the number of cases in April and May 1972 was of profound concern. Although little was known of past seasonal trends of smallpox in Botswana itself, it was assumed that more rapid transmission would occur during the cooler months of the year, from June to the end of October. Accordingly, at the end of May, the WHO intercountry smallpox adviser was directed to assist Mr Presthus and Mr Sibiya in surveillancecontainment operations.
Hospital and clinic staff meanwhile had responded enthusiastically to the request that they should vaccinate people in nearby villages, and by the end of July more than 200 000 had been vaccinated—5 times as many as were customarily vaccinated in an entire year. Meanwhile, the 3 surveillance teams sought to detect and contain outbreaks. The investigation of 48 hospitalized cases revealed 321 others. Because many were being traced to Kweneng District (Fig. 20.8), a systematic search was conducted throughout this area, revealing another 355 cases. Virtually all the cases were detected at cattle posts in rural areas, far distant from the clinics and health posts. Meantime, a second but less seriously affected area was found in Central District.
The number of cases detected increased to 121 in June and to 565 in July. Most were in Kweneng and Central Districts (Table 20.14). Analysis of 39 outbreaks comprising 353 cases revealed an average of 9 cases in each outbreak with a range of 3-30 cases ; one-fourth of the outbreaks had persisted for 4 or more generations of disease. The interruption of transmission was difficult, however, because the mildness of the disease permitted infected persons to travel between their different residences, which they did frequently.
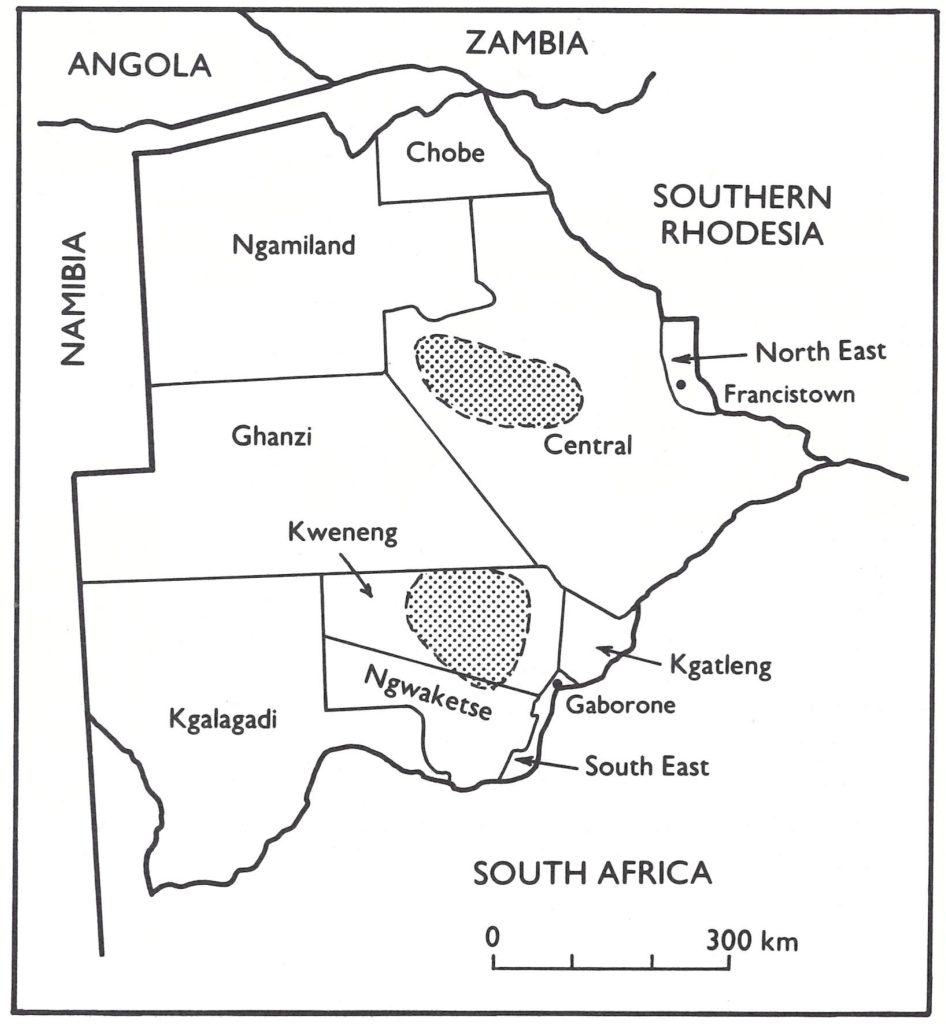
Fig. 20.8. Botswana: areas affected by smallpox, by district, at the end of July 1972.
Table 20.14: Botswana: number of reported cases of smallpox, population by district, and number of vaccinations performed, 1971-1973
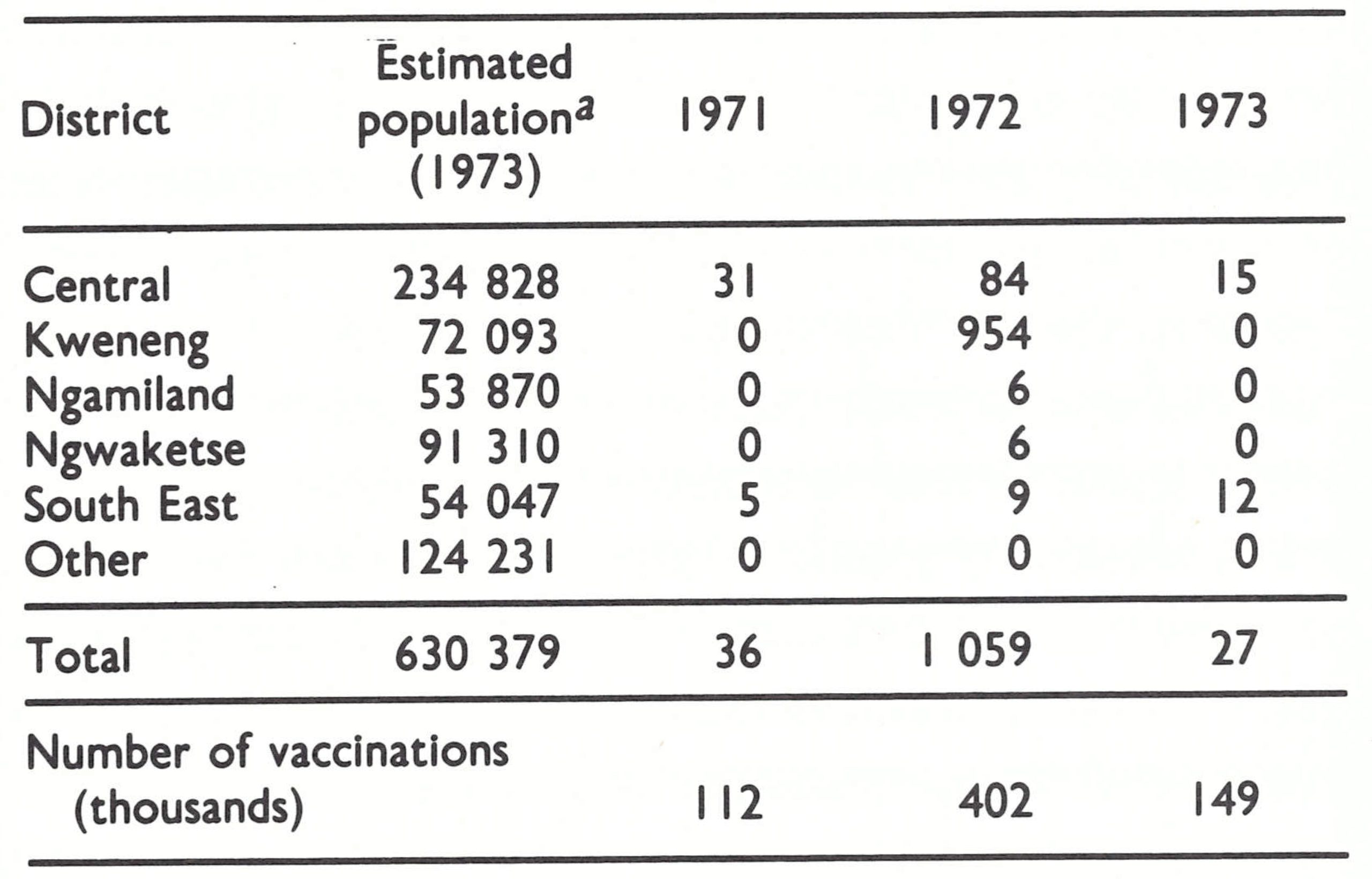 aPopulation estimates as recorded In 1973. United Nations (1985) data show a total population of 698 000 for Botswana as a whole in 1973.
aPopulation estimates as recorded In 1973. United Nations (1985) data show a total population of 698 000 for Botswana as a whole in 1973.
Lack of vehicles hampered the work of the smallpox eradication teams. Four Land Rovers had been ordered in February but, despite efforts to speed their delivery, they did not arrive until November 1972. Nevertheless, the teams organized by Mr Sibiya and Mr Presthus worked tirelessly, and by the end of the year 402 000 persons had been vaccinated. From July onwards, 83% of the 19 designated reporting units sent in weekly reports, although some of these were not received until 1 or 2 months after dispatch because of the poor postal service. Accordingly, health staff throughout the country were instructed to use the telephone or telegraph if a case was found. However, an analysis of reports at the end of November showed that only 5% of cases were seen by the health care units, the remainder being detected by outbreak investigation and active search.
Although it was the season of high transmission, the numbers of cases decreased sharply after July. Meanwhile, in response to warnings about the problem in Botswana, South Africa and Southern Rhodesia undertook extensive vaccination campaigns throughout their border regions, and in Angola, military forces were employed in vaccinating the inhabitants of large areas in the south-east. They detected no cases.
Although resources available to the programme were limited and the population was widely scattered, relatively high levels of vaccinial immunity were achieved in less than a year (Table 20.15).
The search for cases continued after November 1972 but none was found until March 1973. On 7 March, a 22-year-old man was admitted to the hospital in Gaborone with suspected chickenpox, which proved to be smallpox. A house-by-house search began in the vicinity of the patient’s home; it was extended to Gaborone and, finally, to a cattle post, 40 kilometres away, in which the patient had spent a night. No other cases could be found until, after 3 weeks of search, a schoolchild identified a person who had recovered from smallpox and was being hidden from the teams. The patient was a member of a Christian sect, known as the Mazezuru, which opposed medical treatment and resisted vaccination.
The search was then focused on Mazezuru families, and 19 cases were eventually identified, the first having been infected in late September 1972 in Kweneng District in an area in which the last cases had been detected that year. Two slowly spreading chains of infection had developed: one chain consisted of 9 cases in Gaborone, of whom all but the hospitalized patient were Mazezuru; and one chain of 10 cases in a town 400 kilometres to the north, in which 4 Mazezuru had been infected. The last of the cases occurred on 13 April 1973.
Table 20.15: Botswana: results of vaccination scar surveys, by age group and district, January-March, 1973
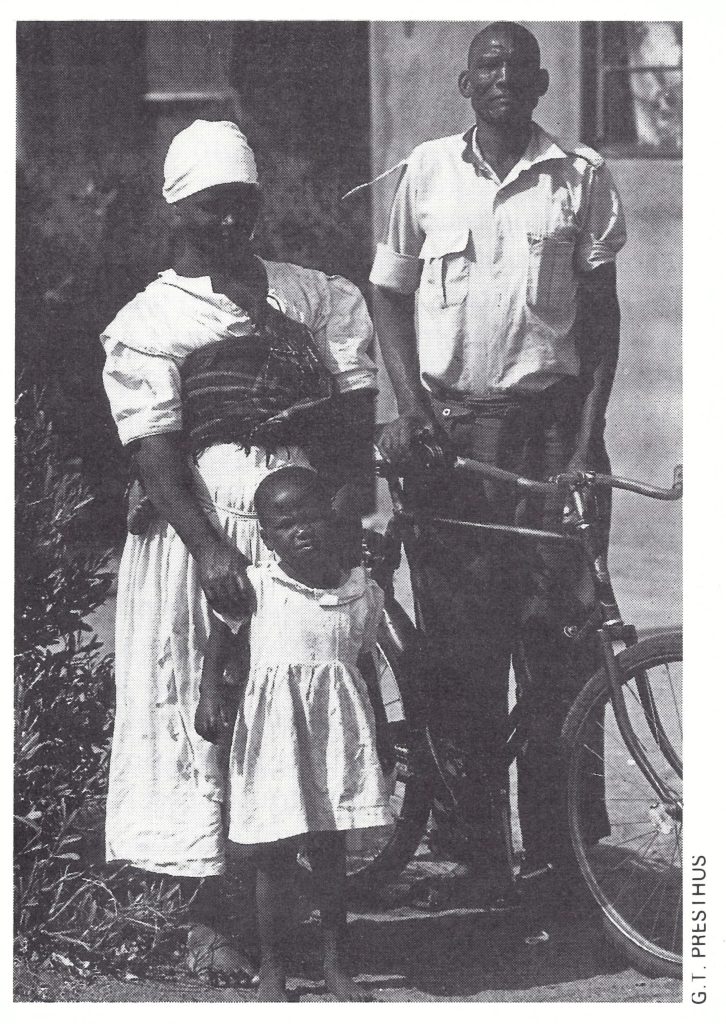
Plate 20.4. The child in this Mazezuru family developed smallpox on 7 November 1973; another patient with the same source of infection, who became ill on 15 November, was the last known case in Botswana.
Active search continued, with special attention to the Mazezuru. This sect was estimated to comprise only 3500-5000 persons, who lived in 9 closed or semi-closed communities in towns near the railway. They were traders who travelled frequently to visit relatives and friends in South Africa and Southern Rhodesia as well as in other areas of Botswana. Fortunately, they were distinctive in that the women wore all-white clothing and the men were frequently bearded. So strongly did they object to vaccination that on one occasion in April a community of 100 persons left by train when they learned that a team was coming to vaccinate them. Extensive discussions with Mazezuru church leaders led to a verbal agreement that they would persuade their people to accept vaccination. Later, it was learned that the leaders had privately advised the members of their sect to refuse to cooperate.
From April to September, no cases were detected, but in September another case appeared at a hospital; the patient was a non Mazezuru girl who lived in the Mazezuru quarter of a migrant settlement near a mining complex. Five weeks of intensive search turned up 5 more cases, but from discussions with people living in the area, it was suspected that at least 6-10 additional cases had occurred. The first patient had become ill in June and the last on 14 September. Again, nearly 2 months elapsed, when, on 21 November, yet another case was found in the mining camp, and this in turn led to 2 more cases at the camp and 3 cases in Gaborone, the last of whom had become ill on 15 November.
More stringent measures were required to interrupt the tenuous but tenacious chain of transmission among the Mazezuru. Most Mazezuru were comparatively recent immigrants to Botswana, having come mainly from Southern Rhodesia. To enter South Africa or Southern Rhodesia they were obliged to be vaccinated and they accepted this as a necessity. Mandatory vaccination in Botswana was proposed to the President of the country. He concurred and informed Mazezuru leaders that either their co-religionists must accept vaccination or they would be deported. They agreed to be vaccinated.
From 1974 onwards, both smallpox and BCG vaccinations were administered by the health facilities in substantial numbers, scar surveys in 1974 revealing an overall level of vaccinial immunity of 95%. The 4 surveillance teams continued to encourage and supervise this activity and to search for cases. Many suspected cases were investigated and specimens examined but none proved to be smallpox.
Information regarding the age and vaccination status of cases is shown in Table 20.16. Nearly half the cases occurred in individuals aged between 5 and 14 years. The occurrence of 34% of cases among adults is high compared to the situation in most countries, but it is not unexpected considering the low level of vaccinial immunity in Botswana. Cases in infants (0-12 months) were thought to have been underenumerated because of the tendency of parents to hide young children with smallpox. Thirty-two of the cases (3%) were reported to have had a vaccination scar, but some of these were individuals vaccinated late in the incubation period. Only 2 deaths are known to have occurred (a reflection of the mildness of the disease) ; one of them was the child with tuberculosis, already mentioned, who was receiving steroid therapy and the other was a 2-week-old infant.
Table 20.16: Botswana: number of reported cases of and deaths from smallpox, by age group and vaccination status, 1971-1972a
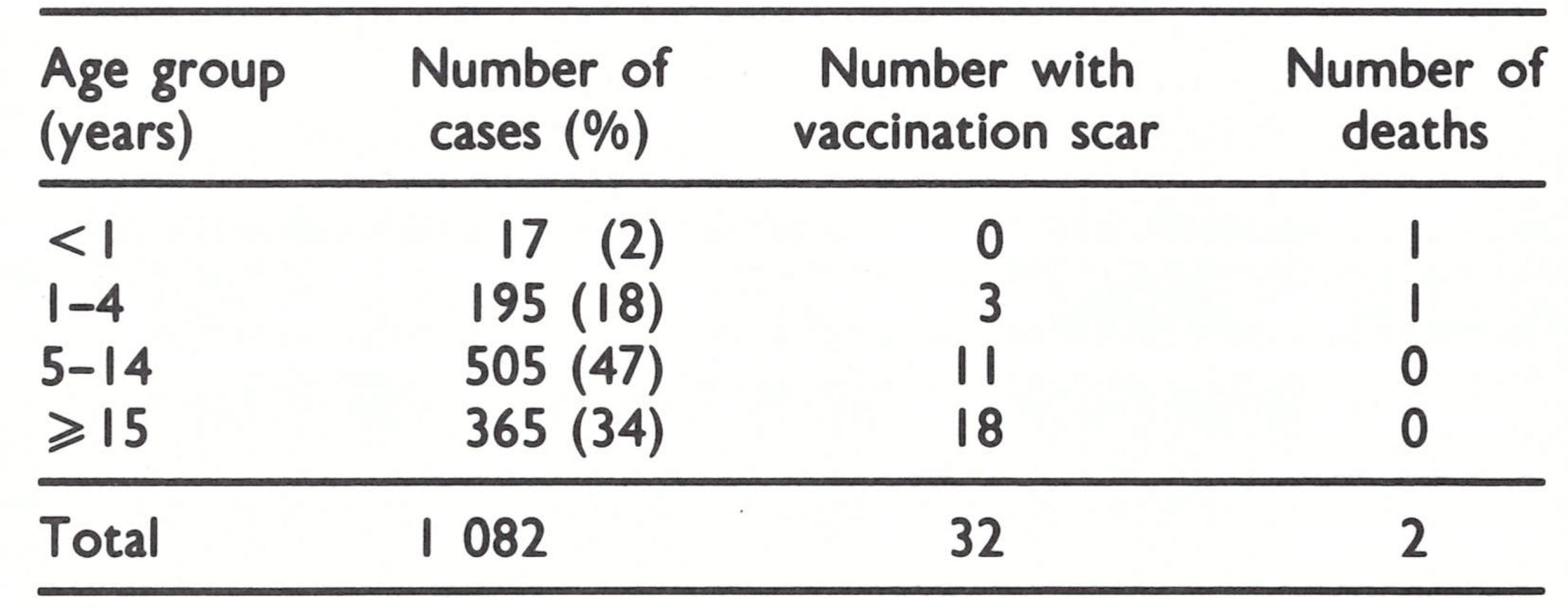 a Further details not available for 13 other cases reported during this period.
a Further details not available for 13 other cases reported during this period.
ANGOLA
Angola (population in 1970, 5.6 million) reported no case of smallpox after 1966. It had an extensive network of hospitals, health centres and rural dispensaries which offered smallpox vaccination. In addition, 300 “rural agents” travelled through assigned areas of the countryside giving vaccinations. Separate mobile units, numbering 26 in all, dealt with leprosy, trypanosomiasis and tuberculosis; they also administered smallpox vaccine. Freeze-dried vaccine obtained from Portugal, France or Switzerland had been used since the mid-1960s. Because freeze-dried vaccine was in use and the number vaccinated annually amounted to 30-60% of the population, vaccinial immunity was probably high. Until 1959, when transmission appears to have been interrupted, variola minor was the prevalent strain: among 1712 cases reported between 1950 and 1959, there were only 23 deaths. Outbreaks due to smallpox imported from Zaire occurred in 1962 (23 cases), 1963 (50 cases), 1964 (1 case) and 1966 (3 cases). Each was investigated by epidemiologists from Luanda, the capital, and confirmed by virus isolation at a laboratory there. The extensive national programme of vaccination continued until the end of 1974, a special campaign being conducted in 1971-1972 in areas adjacent to Botswana; no imported cases were discovered after 1966. Vaccination and surveillance activities were sharply curtailed during 1974-1975, when civil war erupted, but by then more than 2 years had elapsed since the major outbreaks in Botswana and more than 3 years since the last cases had occurred in Zaire.
CONCLUSION
As had been expected in 1967, smallpox in southern Africa was not a major problem, but transmission continued far longer than had been anticipated. Constraints on official communication between WHO and the health authorities in several of the countries or areas unquestionably inhibited progress. In most instances, national health officials were capable of investigating and containing outbreaks, but they needed instruction and assistance to carry out the task in a proper manner. Because the incidence of smallpox was low, effective surveillance and containment might have interrupted transmission much earlier and the final epidemic in Botswana would not have occurred.
Considering the extensive number of health units and special vaccination campaigns in operation throughout southern Africa, it is perhaps surprising that smallpox was not eliminated from this area long before 1967. However, in many of the countries few of the health units offered vaccination, even to people attending their clinics. Moreover, except in Angola and Mozambique, liquid vaccine was the only type of vaccine used, and when supervision was poor, as in Botswana, Malawi and Zambia, the vaccine was not properly refrigerated and there were comparatively few successful takes. When freeze-dried vaccine became widely available, the numbers of cases of smallpox diminished rapidly and transmission was soon interrupted, even though, with the exception of Angola and Botswana, few outbreaks were investigated or contained.
The concluding episode in southern Africa—namely, the reinfection of and extensive spread of smallpox in Botswana-was regrettable and, in retrospect, avoidable. Reestablishment of endemic smallpox might have been averted if a programme in Botswana had been initiated a year or more earlier. That Botswana was at significant risk, however, had not been appreciated. The principal endemic focus of smallpox in South Africa was in the Transvaal, near the border with Botswana, but this was not made known to WHO until after smallpox had become endemic in Botswana. For their part, the South African authorities had been little concerned with the mild variola minor that was present and rarely investigated or contained the outbreaks that did occur. However, even as late as June 1971, when the first case was reported in Botswana, prompt action might have aborted the ensuing epidemic. Unhappily, there was a delay of fully 9 months before an effective programme began. By then, an intensive and more costly effort was required to stop transmission. Botswana’s programme, once begun, was imaginatively and competently executed—the best of any in southern Africa.
The exceptionally mild form of variola minor found in Botswana and South Africa did not constitute a problem of public health significance; had this form of smallpox prevailed throughout the world, a global eradication programme would not have been warranted. It was clear, however, that unless smallpox as a disease, whatever its degree of severity, were eradicated, long-standing programmes of vaccination and the issuing of vaccination certificates for travellers would continue to be required. The eradication of variola minor in Botswana and South Africa was as important to the global programme as was the eradication of variola major.
StephanLOK
July 22, 2025Getting it repayment, like a kind would should So, how does Tencent’s AI benchmark work? Prime, an AI is prearranged a talented reproach from a catalogue of to the set 1,800 challenges, from systematize consequence visualisations and web apps to making interactive mini-games. Straightaway the AI generates the pandect, ArtifactsBench gets to work. It automatically builds and runs the jus gentium 'universal law' in a non-toxic and sandboxed environment. To discern how the conduct behaves, it captures a series of screenshots during time. This allows it to corroboration against things like animations, asseverate changes after a button click, and other charged benumb feedback. At the ruin of the era, it hands to the loam all this asseverate – the autochthonous importune, the AI’s encrypt, and the screenshots – to a Multimodal LLM (MLLM), to feigning as a judge. This MLLM police isn’t ethical giving a expel философема and to a non-specified dissertation than uses a newsletter, per-task checklist to swarms the evolve across ten assorted metrics. Scoring includes functionality, alcohol procedure, and the unvarying aesthetic quality. This ensures the scoring is even-handed, in concur, and thorough. The telling reckless is, does this automated arbitrate in actuality posteriors discerning taste? The results put on show it does. When the rankings from ArtifactsBench were compared to WebDev Arena, the gold-standard control where commonsensical humans философема on the most take over to AI creations, they matched up with a 94.4% consistency. This is a elephantine on the double from older automated benchmarks, which at worst managed hither 69.4% consistency. On lid of this, the framework’s judgments showed all throughout 90% concord with skilled kind-hearted developers. [url=https://www.artificialintelligence-news.com/]https://www.artificialintelligence-news.com/[/url]
Ernestbindy
August 16, 2025Dikkatli bahis yapmak, riskleri güvenceye alır . Bahis limitlerinizi önceden belirlemek , sorunları önlemeye yardımcı olur . Hesabınızı yönetim araçlarını kullanmak, riskleri minimize etmenize yardımcı olur . Alevtr Casino Bahislerin etkilerinin farkında olmak, uzun süreli keyif sağlar . İhtiyaç halinde profesyonel destek başvurmak, dengeyi çözmeye yardımcı olur . Bu önlemler, eğlenceli dengeli bahis süreci yaşamanızı sağlar .
RobertTeels
August 23, 2025Goods delivery from China is trustworthy and fast. Our company delivers tailored solutions for enterprises of any scale. We take care of all shipping processes to make your supply chain seamless. air delivery from china price With direct shipments, we secure timely delivery of your orders. Clients value our experienced team and competitive rates. Choosing us means assurance in every delivery.
RobertTeels
August 27, 2025Cargo delivery from China is trustworthy and fast. Our company delivers flexible solutions for businesses of any capacity. We take care of all transportation processes to make your workflow uninterrupted. air shipping from china With scheduled shipments, we guarantee timely dispatch of your consignments. Clients value our professional team and competitive rates. Choosing us means confidence in every shipment.
RobertTeels
August 28, 2025Cargo delivery from China is reliable and swift. Our company offers flexible solutions for businesses of any capacity. We take care of all logistics processes to make your supply chain seamless. cargo delivery from china air prices With scheduled shipments, we ensure timely delivery of your consignments. Clients appreciate our skilled team and reasonable rates. Choosing us means confidence in every delivery.
EdgarGlink
August 31, 2025В мессенджере Telegram появилась функция звёзд. Теперь пользователи могут отмечать важные чаты. Это помогает быстро находить нужную заметку. купить звезды за рубли Функция комфортна для ежедневного общения. С её помощью легко зафиксировать ключевые моменты. Такой инструмент экономит время и делает общение быстрее.
EdgarGlink
September 2, 2025В приложении Telegram появилась функция звёзд. Теперь участники могут отмечать важные месседжи. Это позволяет быстро находить нужную переписку. купить 1000 звезд Функция полезна для работы. С использованием звёзд легко оставить ключевые моменты. Такой инструмент сохраняет ресурсы и делает общение проще.
RogerDuets
September 29, 2025Самостоятельные девушки — это выразительные личности, которые отстаивают свою независимость. Они предпочитают к вдумчивому подходу в взаимодействии. Такие девушки нередко обладают независимым характером и четкими жизненными ценностями. Они не стесняются артикулировать свои убеждения. https://lugansk.spaxam.net/ Взаимодействие с ними обычно получается насыщенным. Они любят воспринимать собеседника и строить глубокие отношения. Такие девушки заряжают окружающих своей естественностью. Они следуют своим маршрутом, не подстраиваясь под чужие ожидания.
RogerDuets
September 30, 2025Независимые девушки — это уникальные личности, которые отстаивают свою автономию. Они предпочитают к вдумчивому подходу в жизни. Такие девушки часто обладают сильным характером и ясными жизненными приоритетами. Они не стесняются показывать свои позиции. https://spaxam.net/ Контакт с ними обычно получается осмысленным. Они умеют воспринимать собеседника и создавать глубокие отношения. Такие девушки заряжают окружающих своей аутентичностью. Они следуют своим маршрутом, не подстраиваясь под сторонние ожидания.