Chapter 23:
Smallpox in non-endemic countries

INTRODUCTION
In the preceding 11 chapters we have systematically reviewed the elimination of smallpox from the 31 countries in which it was endemic in 1967 and 2 other countries (Botswana and the Sudan) in which endemicity was re-established after 1967. Because smallpox was endemic in many parts of the world in the 1960s and early 1970s, cases continued to be imported into smallpox-free countries. The annual numbers of smallpox cases in most of the larger countries between 1920 and 1958 are tabulated in Chapter 8. The year in which smallpox was last endemic in each of these countries is indicated in the tables; cases occurring after that year were due to importations. This chapter is concerned with a more detailed description and analysis of outbreaks of smallpox that occurred in industrialized non-endemic countries after 1958, and in non-endemic countries of Africa, South America and Asia after 1966, when reasonably complete information first began to be compiled.
In the industrialized countries a total of 37 outbreaks due to importations from endemic areas were reported between 1959 and 1974: 34 occurred in 13 countries of Europe, 1 in Canada, and 2 in Japan (Table 23.1). In addition to importations by infected persons, there were 3 laboratory-associated outbreaks in the United Kingdom between 1966 and 1978. These are comparable to importations from endemic countries in that they were introductions of smallpox infection into a smallpox-free country ; they are described in the last section of this chapter.
Table 23.1: Annul numbers of importaintons of smallpox into industrialized countries, 1958-1979
 a Thirteen countries; see table 23.2.
a Thirteen countries; see table 23.2.
b One outbreak in the Federal Republic of Germany started in 1958 but continued into 1959.
A notable feature of this period, compared with earlier times (see Chapters 5 and 8), was the absence of transfers of smallpox between the Eastern and Western Hemispheres, and the rarity of intercontinental importations other than from the Indian subcontinent to Europe (Fig. 23.1). This is surprising, in view of the vast volume of international traffic (4 million air passengers in 1948, 46 million in 1966, and over 400 million in 1975) and the much greater speed of travel by air than by sea.
As the Intensified Smallpox Eradication Programme proceeded, more detailed information was collected about cases throughout Africa, South America and Asia, and as a result of this effort, many outbreaks were recognized which were due to transfers across national boundaries in each of those continents. Most of these importations were contained, but some had serious consequences, leading to the re-establishment of endemic smallpox in the Sudan (1968), Botswana (1971), Bangladesh (1972) and Somalia (1976). An importation from Afghanistan into Iran in 1970 led to a large epidemic which was not terminated until 1972, and spread from Iran to Iraq, then to the Syrian Arab Republic, and from Iraq to Yugoslavia.
Excluding the laboratory-associated incidents, the 34 outbreaks in Europe produced 573 cases, of which 90 were fatal. Although the number of cases was extremely small compared with the number occurring in the endemic countries (perhaps some 50 million cases annually in the mid-l950s), health officers and the general public in the industrialized countries feared smallpox more than any other of the diseases then primarily indigenous to the developing countries.
Importations into Europe and Japan did not cease until 1974, when smallpox had been eliminated from most countries of Africa, from Indonesia, and from large areas of India and Pakistan, including most of the larger cities.
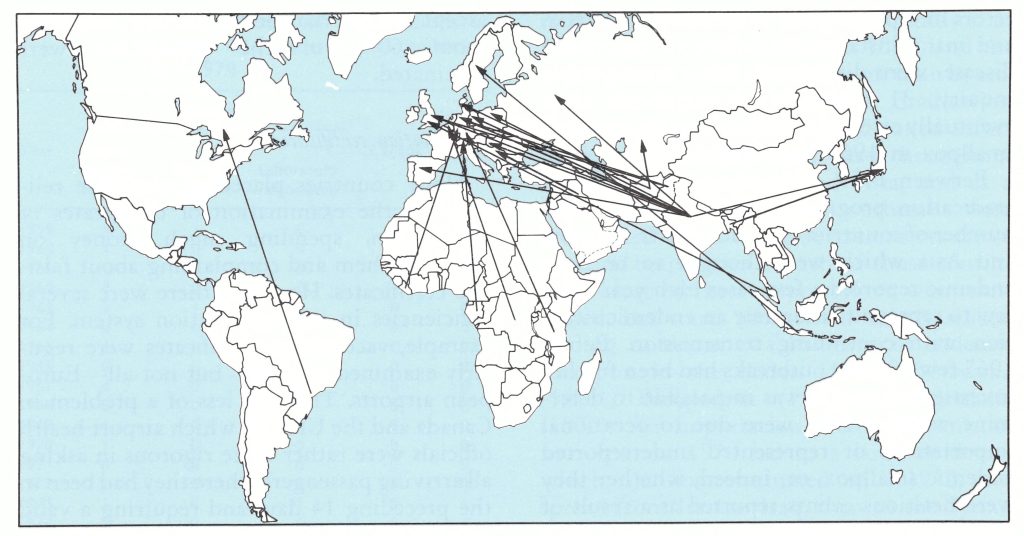
Fig. 23.1. International transfers of smallpox from Africa and Asia to Europe and Japan, 1959-1974. and from Brazil to Canada in 1962. In several cases one arrow represents several transfers, e.g., between India and the Federal Republic of Germany and between Pakistan and the United Kingdom.
CRITERIA FOR DEFINING NON-ENDEMIC COUNTRIES
Apart from the industrialized countries, in which importations had been recognized as such from the 1940s or earlier, few efforts were made until 1967 to classify countries as having endemic smallpox or as being smallpox-free. All countries, by international convention, were supposed to report the occurrence of cases of smallpox promptly to WHO, but not all did so, nor were the reports that were received investigated to determine their validity. With the establishment of the Intensified Smallpox Eradication Programme, a deliberate attempt was made to distinguish countries in which smallpox was endemic from those that were free of the disease. Many errors in reporting the existence of smallpox, and many instances of failure to report the disease, were discovered. After considerable inquiry, 31 countries or territories were eventually categorized as harbouring endemic smallpox in 1967 (see Chapter 10).
Between 1959, when the global smallpox eradication programme began, and 1967, a number of countries of Africa, South America and Asia which were thought to be nonendemic reported a few cases each year—too few to represent accurately an endemic situation with continuing transmission. Before 1967 few of these outbreaks had been further investigated, and it was impossible to determine whether they were due to occasional importations or represented underreported endemic smallpox, or, indeed, whether they were fictitious events reported as a result of clerical or diagnostic error.
Because of uncertainty as to whether countries in Africa, South America and Asia were indeed free of smallpox, and because reporting had been unsatisfactory and importations had rarely been fully documented, discussion of importations into these countries will be brief, and restricted, for the most part, to the period after 1967.
THE SIGNIFICANCE OF SMALLPOX IN NON-ENDEMIC COUNTRIES
Two aspects of smallpox in non-endemic countries were relevant to the global strategy of smallpox eradication: the actions taken by the countries themselves and those taken by WHO.
Actions Taken by the Non-endemic Countries
Before about 1970, almost all industrialized countries regularly vaccinated a large proportion o€ their population and enforced the requirement stipulated in the International Health Regulations that international travellers should hold valid certificates of vaccination. These measures were pursued with varying degrees of diligence in different countries. In the USA, for example, most children were required to show evidence of vaccination at school entry and the vaccination rate in the population as a whole exceeded 95%. In the United Kingdom vaccination was encouraged but not enforced, except for international travellers, and only about 60% of the population were vaccinated.
Vaccination certificates
Many countries placed considerable reliance on the examination of certificates of vaccination, spending much money on checking them and complaining about falsified certificates. However, there were several deficiencies in the certification system. For example, vaccination certificates were regularly examined at most—but not all—European airports. This was less of a problem in Canada and the USA, in which airport health officials were rather more rigorous in asking all arriving passengers where they had been in the preceding 14 days and requiring a valid vaccination certificate from all those who had been in a smallpox-endemic country during this period.
With regard to vaccination certificates, there was much discussion of the need to examine the results of vaccinations 7-9 days later to confirm whether these had been successful, and to require a repeat vaccination if they had not. Few appreciated that much of the vaccine used, especially in endemic countries, was of low potency, and that the failure of a first attempt often resulted in a second vaccination with equally poor vaccine. However, certificates did not require that the results of a second primary vaccination should be examined.
The principal value of vaccination certificates probably lay in encouraging most travellers to be vaccinated before they left their own country. Most intercontinental travellers were from non-endemic countries, and although they were in fact responsible for the majority of importations into European countries (see the next section), the number of incidents might have been much higher had there been no requirement for vaccination certificates.
Control of outbreaks
In accordance with the philosophy of smallpox control then prevalent (see Chapter 9), industrialized countries in the 1950s and early 1960s usually responded to the discovery of an importation of smallpox by mounting a large vaccination campaign, in parallel with efforts to identify contacts and vaccinate and isolate them. For example, in the outbreak which followed an importation into Stockholm, Sweden, in 1963 and caused 27 cases of smallpox and 4 deaths, some 300 000 persons were vaccinated in a period of a few weeks, with 1076 reported complications, of which 77 were serious (Strom & Zetterberg, 1966).
In the late 1960s and 1970s, when surveillance and containment were accepted as the best method of smallpox control, mass vaccination campaigns were rarely undertaken. One exception was the mass vaccination programme undertaken during the large outbreak in Yugoslavia in 1972. Earlier, in 1970, the Federal Republic of Germany had considered mass vaccination when an outbreak occurred at Meschede Hospital, but had been persuaded by WHO not to implement this operation, on the grounds that it was unnecessary and would be costly and likely to result in many complications.
The two countries in Europe with the most importations, the Federal Republic of Germany and the United Kingdom (see Table 23.2), maintained special hospitals for the isolation of smallpox patients, which were held on stand-by in case of a possible outbreak of the disease. The last of these hospitals in the United Kingdom, the Catherine-de-Barnes Isolation Hospital near Birmingham, was not closed until 1985. At the 1976 Winter Olympic Games in Austria, a special building with 8 beds was set aside for use as a smallpox hospital in the event of an outbreak and was identified as such.
Clearly, the health authorities of the industrialized countries remained highly apprehensive of the danger of smallpox, a view shared by the general public. This was evident in the Meschede outbreak, during which motor vehicles bearing a Meschede numberplate sometimes had difficulty in obtaining petrol from garages in other parts of the Federal Republic. As late as 1978, after the laboratory-associated outbreak in Birmingham, England, health authorities in 8 countries demanded valid vaccination certificates for a period of many weeks from all passengers arriving from the United Kingdom, and the authorities in another 6 countries required them from passengers who had been in Birmingham in the previous 14 days.
The attitude to importations in developing countries was not so rigorous, except in those in which a recent campaign had led to the eradication of the disease and thus to a heightened sense of the risk of importation. In the developing countries, many importations resulted in substantial outbreaks and on several occasions to the re-establishment of endemicity.
Actions Taken by WHO
Although the health authorities of the industrialized countries were responsible for controlling any importations, after the establishment of the Intensified Smallpox Eradication Programme WHO took several steps to assist them. An emergency supply of vaccine was held in Geneva, and the health authorities of all countries were notified that members of the WHO Smallpox Eradication unit were prepared to travel at short notice to any country requesting assistance. This rarely proved necessary, but the Smallpox Eradication unit maintained close telephone contact with the relevant health authorities until the emergency was over. However, Henderson and a WHO consultant, Dr Paul Wehrle, assisted in the investigation of the unusual outbreak at Meschede (see Chapter 4); vaccine and WHO technical assistance were supplied to Yugoslavia in 1972; and in 1978 Dr Joel Breman, then a member of the unit, visited the United Kingdom to take part in the inquiry into the laboratory-associated outbreak in Birmingham.
Assistance was also provided by WHO after importations of smallpox into Bangladesh, Botswana, the Gulf states, and the Sudan. Finally, reports of smallpox in non-endemic countries which reached WHO through the reporting system were always investigated to ascertain whether or not they were due to misdiagnosis or to clerical error. Such investigations had been conducted throughout the programme and even after eradication, during the operation of the international rumour register (see Chapter 28).
The Weekly epidemiological record was a very useful means for the prompt dissemination of information about smallpox (see Chapter 10); it was widely distributed by WHO to Member States, particularly to their epidemiologists and port and airport health services. In 1968, a large number of reprints of an article by Dumbell (1968), “Laboratory aids to the control of smallpox in countries where the disease is not endemic”, was given special distribution to Member States. Also in 1968, the Smallpox Eradication unit invited Dr Thomas hl. Mack, then an epidemiologist at the United States Communicable Disease Center, to WHO Headquarters, where he reviewed importations of smallpox into Europe; his paper, “Smallpox in Europe, 1951-1971”(Mack, 1972), was the first comprehensive analysis of the epidemiological pattern of smallpox importations into nonendemic countries.
SMALLPOX IN EUROPE, 1959-1978
Over a period of 20 years, from 1959 to 1978,13 European countries—about half the larger countries of the continent—reported the occurrence of cases of smallpox. Excluding laboratory-associated outbreaks, which are discussed at the end of this chapter, there were 34 importations from endemic countries, and on 4 occasions the disease spread to neighbouring countries (Table 23.2).
Outbreaks occurred in Europe each year from 1959 to 1973, except 1964, 1966 and 1971, with the largest numbers in 1961,1962 and 1963. In all, 573 cases were recorded, including the imported (index) cases. The largest outbreaks consisted of 175 cases in Yugoslavia and an associated case in the Federal Republic of Germany (1972), 99 cases in Poland and an associated case in the German Democratic Republic (1963), 47 cases in the United Kingdom (1962), and 46 cases in the USSR (1959-1 960). The other 30 introductions caused single-case outbreaks on 14 occasions and outbreaks of 2-33 cases on 16 occasions. Although two-thirds of the outbreaks led to no more than 5 cases, their impact on the communities in which they occurred was out of proportion to the real risk; cases always made the headlines in the newspapers, many persons sought vaccination, and in the larger outbreaks mass vaccination campaigns were urged or undertaken.
The Federal Republic of Germany and the United Kingdom, which together accounted for 19 of the importations from the endemic countries during this period, were the most frequently affected, in part because of the more frequent travel between them and the Indian subcontinent.
Sources of Importations
Asian countries were the source of infection for 28 of the 34 introductions from outside Europe; in only 5 instances was infection brought from Africa, once each from Gabon, Liberia and the United Republic of Tanzania, and twice from Zaire. The Indian subcontinent was the principal source of importations, 14 coming from India and 8 from Pakistan.
As the smallpox eradication programmes progressed in the endemic countries, introductions of smallpox into Europe became less and less frequent—23 in 1959-963, 7 in 1964-1968 and 4 in 1969-1973—in spite of the increase in the volume of air travel over this period.
Twenty-seven of the 29 importations from overseas for which data are available were associated with air travel, but none resulted from transmission on an aeroplane; all the infected persons were in the incubation period or the prodromal phase of the disease, when virus was not transmitted. The 2 outbreaks in 1962 in which the index case travelled by ship were recognized during the voyage or when the ship docked, as the patients arrived with fully developed signs and symptoms. On one occasion only (No. 33 in Table 23.2) was the index case known to have travelled by bus, and the prodromal symptoms of smallpox, which were taken to be due to fatigue from the long journey, did not develop until after the arrival of the person concerned in Yugoslavia.
In 4 instances, cases were imported from one European country into another. A single case that occurred in Schaffhausen in Switzerland in January 1962 was probably infected in Dusseldorf, in the Federal Republic of Germany, at the end of December 1961 (No. 12 in Table 23.2). In 1970, a case in Tromso in Norway had been exposed to one in Denmark (No.32), and a case occurred in the Federal Republic of Germany in a man who had been exposed during the epidemic in Yugoslavia in 1972 (No.33). The large outbreak in Poland in 1963 (No. 22) was probably responsible for a single case in the German Democratic Republic later that year.
Table 22.2: Importations of smallpox into Europe by travellers, 1959-1974
 a One case in Switzerland.
a One case in Switzerland.
b One case in in the German Democratic Republic.
c One case in Norway.
d One case in the Federal Republic of Germany.
Nature of Index Cases
The index case in importation No. 4 (Table 23.2) was said to have been infected with virus transmitted from Afghanistan on a carpet, but little additional information is available ; all other outbreaks were known to be due to the entry of infected persons. Of the other 31 importations into Europe (details are lacking for No. 2 and No. ll), 20 of the index cases occurred in Europeans who had recently visited smallpox-endemic areas. Their occupations varied; among them were 4 physicians and 4 engineers or electricians. Only 11 index cases (7 adults and 4 children) were nationals of an endemic country: 7 were Pakistanis and 4 were Indians and all of them were visiting relatives or friends in the United Kingdom, except for an Indian visiting the Federal Republic of Germany.
Among those importing smallpox, the proportion of males to females was 26 to 5. Twenty-four were adults; the youngest was a 6-month-old baby infected in Zaire (No. 30 in Table 23.2) and the oldest a Swiss nurse aged 70 years who was infected in Gabon (No. 23).
Only one-third of the index cases gave histories of apparently satisfactory smallpox vaccination. In spite of the availability of potent vaccine and the concern of health officers in European countries regarding importations of smallpox, case histories revealed that most of the Europeans responsible for importations were not well protected when visiting endemic countries. It was estimated that about 70% of the importations resulted from unsatisfactory revaccinations, for which poorly kept liquid vaccine seemed mainly responsible. Throughout the global eradication programme health officials expressed great concern about forged vaccination certificates and focused much of their attention on this matter, but it probably played a fairly marginal role, only a few migrants from the Indian subcontinent being implicated.
Of 28 index cases who arrived from abroad by plane, only 5 had signs of disease on arrival, including an acne-like rash and lesions on the lips. Six arrived in the prodromal, influenza like stage and the remaining 16 landed apparently healthy; it was impossible to identify any of these cases on arrival. One third of those who were incubating smallpox fell ill within 3 days of their arrival and the other two-thirds by the end of the first or the second word after arrival. Recognition of the disease and its notification were often delayed, since the doctor who saw the cases of the did not suspect smallpox and were usually unfamiliar with its clinical picture.

Plate 23.1. The WHO smallpox recognition card was abundantly used by the Somali search teams inquiring about possible cases of smallpox.
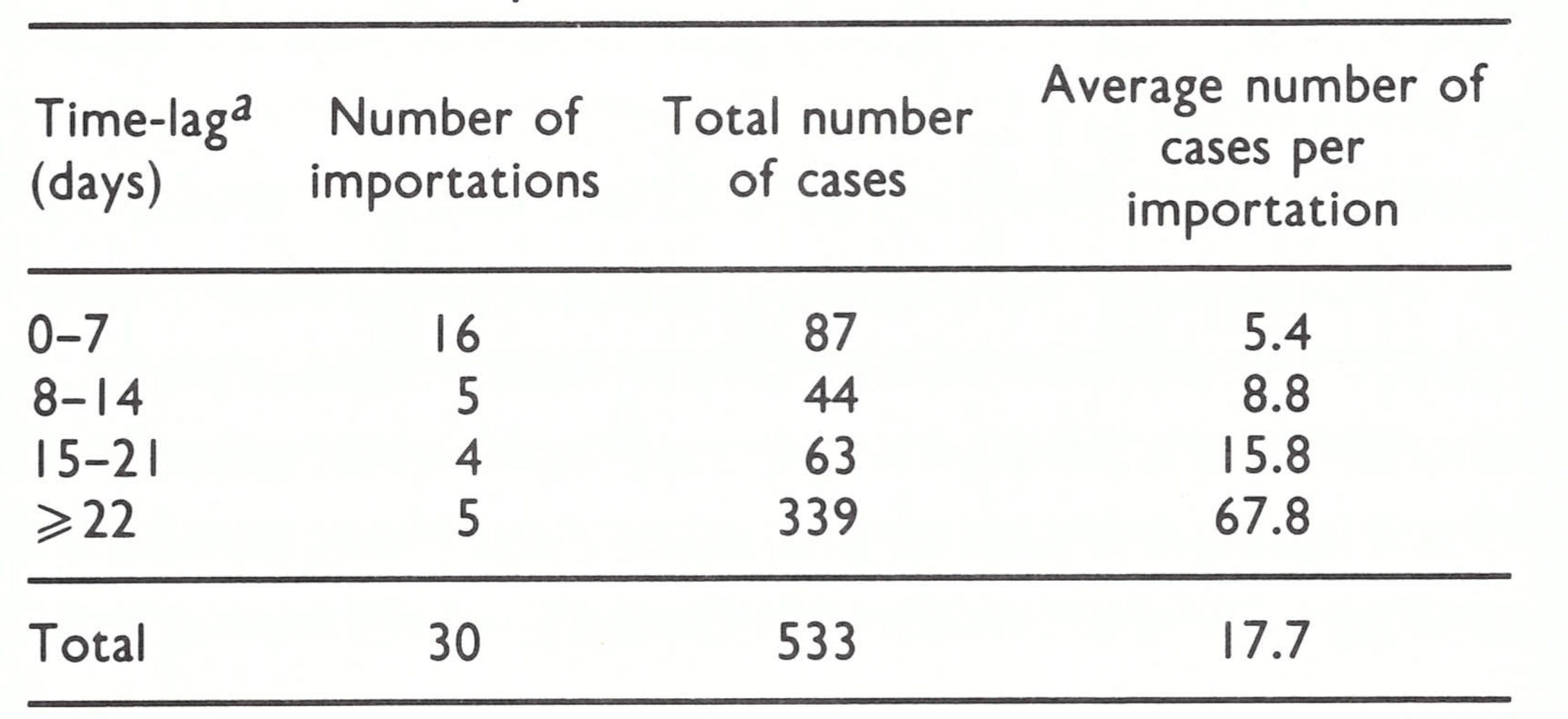
Delays in Notification
Of 30 importations for which data are available, 21 were recognized as smallpox withiT? ?. weeks of the arrival of the index cases. indicating that the importations were discovered within one incubation period of generation of the cases (Table 23.3). on 5 occasions (No.12, No.13, No.21, N0.22 and No.33 in Table 23.2), delays of more than 3 weeks (range, 22-42 days) occurred before the recognition of smallpox. All these outbreaks resulted in serial transmission for 3 or more generations (see Table 23.4). Clearly, the longer the delay in discovery, the greater was the number of cases that occurred. Sometimes, however, the index case was promptly recognized but a first generation case was missed, as in importation No. 18, in Cardiff, Wales, in which the index case was correctly diagnosed within 4 days of the onset of fever, but a female first-generation patient was not discovered for 20 days; 47 cases occurred in this outbreak, despite early detection of the index case.
Transmission from Imported Cases
In 14 of the 34 importations into Europe there were no secondary cases (Table 23.4). Of 20 importations in which transmission occurred, 12 resulted in 1 or 2 indigenous generations and 5 in 3 or 4 generations; in only 3 importations were there more than 5 generations of transmission. Except for the last-mentioned outbreaks, containment measures were successful in interrupting transmission within about 2 months.
Seasonal effects
Although importations occurred at all times of the year, they were more numerous in the winter and spring (Table 23.5), the usual periods of seasonal increase in smallpox incidence in the endemic areas of the Northern Hemisphere from which most importations originated. The importations at this time of the year usually caused considerably larger outbreaks than those in the summer and autumn, showing that the temperate countries of Europe were also subject to seasonal influences.
Cases infected in Europe
Of the 573 known cases, 35 were index cases infected outside Europe, including 3 cases on board ship in outbreak No.19. Of the 537 indigenous cases, 277 (52%) were infected in health establishments or during the course of medical or nursing duties (Table 23.4); 57 (21%) of them were fatal. The other 261 cases resulted from intimate contact with cases in affected households or from casual contacts in institutions such as schools or factories. Although most cases in Europe were cared for in well-equipped hospitals, these institutions played an important role in the further dissemination of smallpox and posed a real risk for other patients as well as staff. The routine vaccination of hospital staff was recommended in Europe and North America, but it was rarely carried out satisfactorily. Most cases occurred among young medical professionals, nearly 20% of whom had never been successfully vaccinated. In contrast, cases among hospital patients and visitors occurred most frequently in young children and aged persons. A few cases were reported in seamen and port employees, as in outbreak No. 19. A Czechoslovak Airlines navigator who contracted smallpox (No. 26) was infected during his stay in Bombay, not on his plane.
Case-fatality rates
There had been several importations of variola minor into Europe during the first half of the 20th century, but all importations after 1959 were of variola major. The overall case-fatality rate of 16% (see Table 23.2) was of about the same magnitude as that in endemic countries, the deaths occurring primarily in unvaccinated infants, in persons with contraindications to routine vaccination, and in older patients who had been vaccinated many years earlier.
Table 23.3: Delays in notification and the extent of spread of smallpox in 30 outbreaks in Europe, 1959- I973
 a Interval between the date of onset of fever in the first case and date of notification to the health service.
a Interval between the date of onset of fever in the first case and date of notification to the health service.
Table 23.4: Europe: smallpox outbreaks by generation
 a Infection sald to have been transmitted on a carpet.
a Infection sald to have been transmitted on a carpet.
Table 23.5: Europe: seasonal influence on the numbers of importations of smallpox and the size of outbreaks following importations
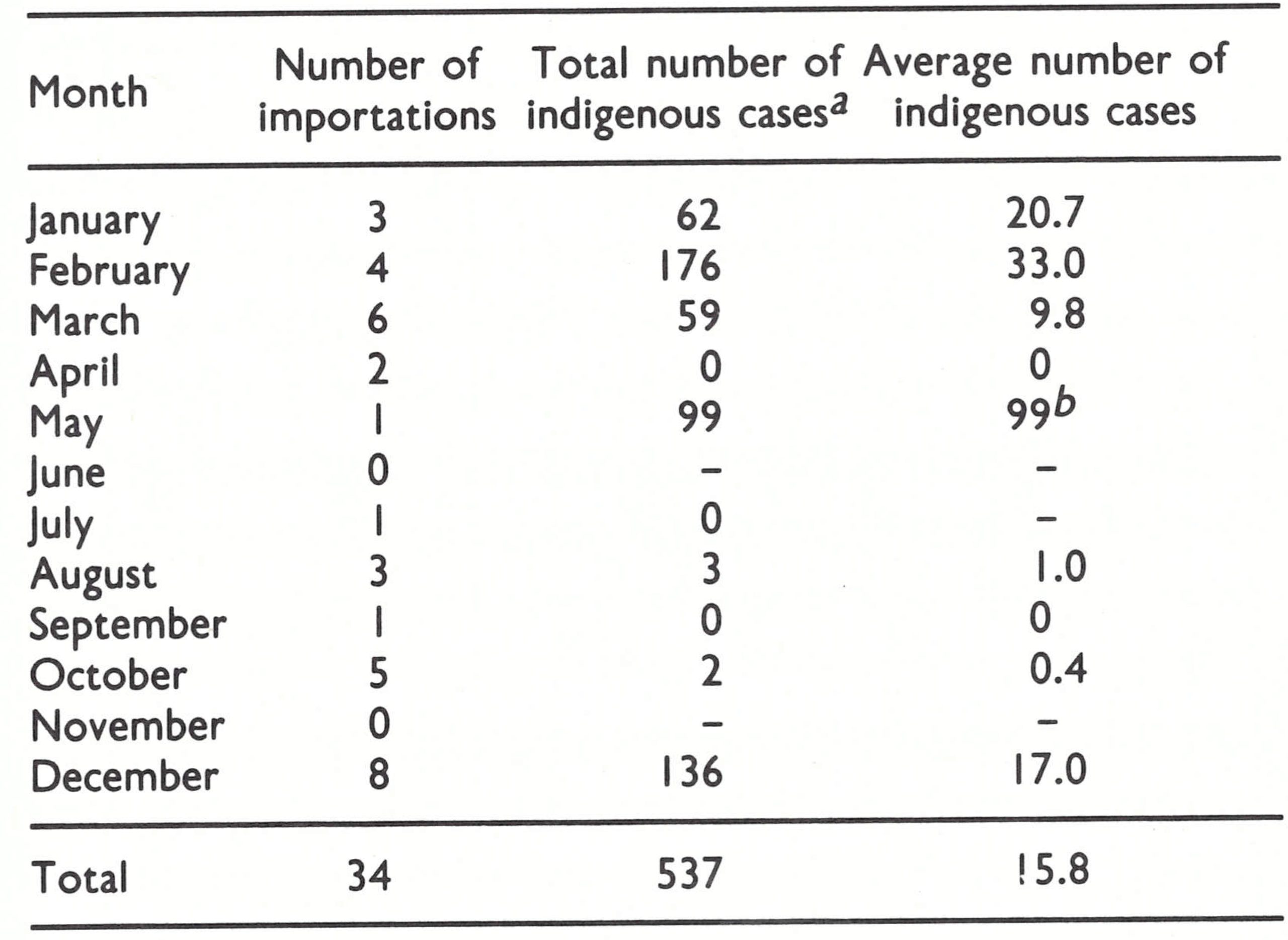 a All cases are attributed to the month in which the index case occurred.
a All cases are attributed to the month in which the index case occurred.
b Outbreak No.22: one exceptionally large outbreak occurred at the end of the epidemic season.
The extent of individual outbreaks in Europe
Except for a few outbreaks, smallpox importations into Europe did not produce large numbers of cases, reaching double figures in only 11 outbreaks, even though some outbreaks were not discovered for as long as 3 weeks after the onset of illness in the first case (Table 23.3). Forty per cent of the importations caused no further transmission. After 1963, only 2 outbreaks occurred in which there were more than 2 cases, and both were associated with unusual circumstances: severe cough and the aerosol spread of virus in outbreak No. 31 (Meschede), and spread in Yugoslavia in one of the country’s least developed areas, involving an unrecognized case in a man who was moved from hospital to hospital (No. 33). The fact that there was not greater spread can be attributed in part to the prompt isolation of patients at home or in hospital and to the generally rapid and effective application of control measures.
Especially after 1967, however, smallpox importations into Europe received extensive press, radio and television coverage. Despite the prompt measures usually taken by the public health authorities, the deep-rooted if sometimes unfounded fears of the population were difficult to quell. Several countries suffered considerably in consequence. For example, in the first few days after the recognition of the large outbreak in Yugoslavia, the country was in turmoil: people were afraid to visit public places until they and their families had been protected by vaccination; trucks carrying market products from affected areas were turned back; tourist bookings were cancelled ; and some countries closed their borders and advised their nationals not to visit Yugoslavia. Only after a steady flow of epidemiological information and surveillance data had reassured neighbouring countries were the last of the restrictions on trade and travel dropped, some 12 weeks after the beginning of the outbreak.
Case Studies of Importations into Europe
Detailed accounts of 2 outbreaks following importations into Europe are given elsewhere: outbreak No.31 in Chapter 4, as an example of the airborne transmission of smallpox, and outbreak No. 33 later in this chapter, as part of the epidemic that spread across south-western Asia into Europe in 1970-1972.
Two other examples illustrate different aspects of smallpox outbreaks after importations into Europe: an outbreak (No.16) in Bradford, England in 1961, in which transmission occurred in 3 hospitals; and an episode (No.32) in Denmark and Norway in 1970 that led to only 1 further case despite the original patient’s having had numerous contacts.
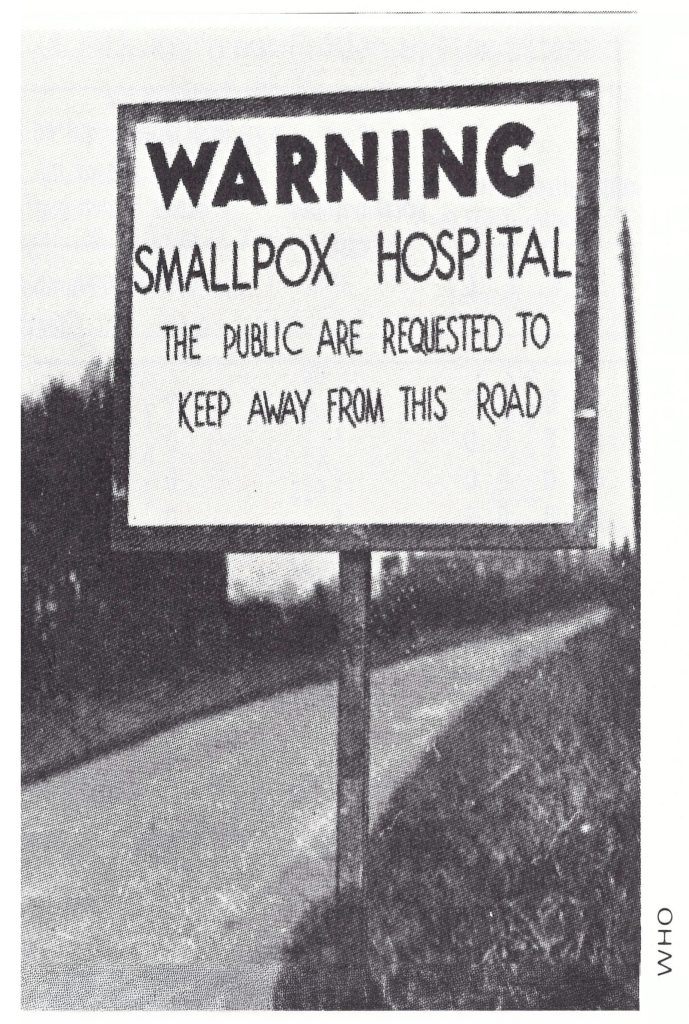
Plate 22.2. Some non-endemic countries kept special hospitals ready for the isolation of patients in case smallpox was imported. Sign on a public road in Yorkshire, England, during an outbreak of smallpox in 1953.
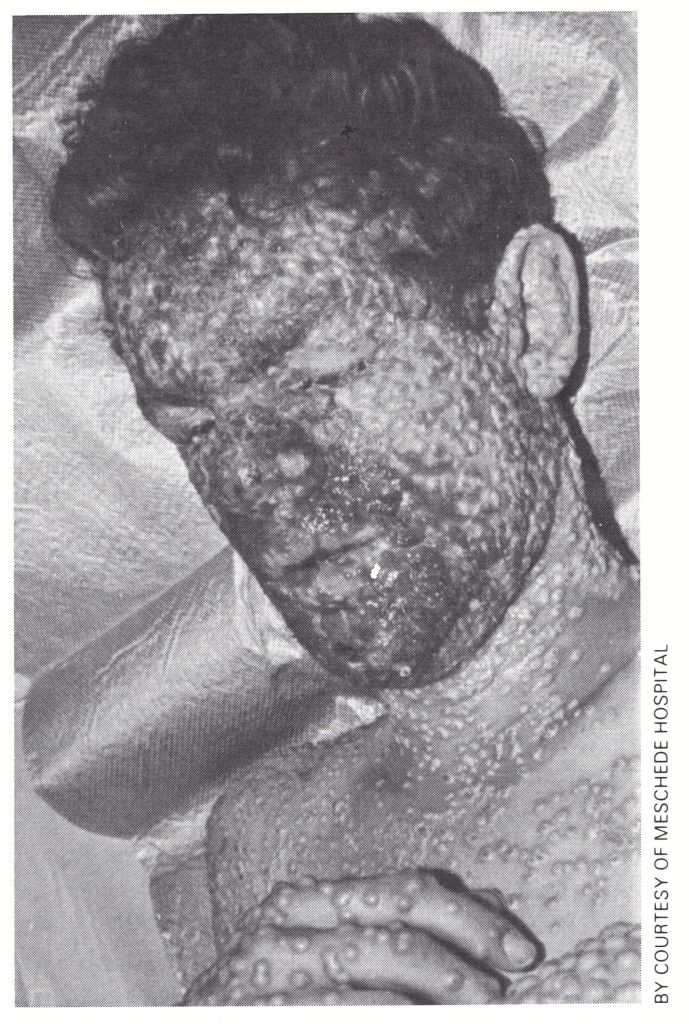
Plate 22.3. The airborne spread of virus from this 20-year-old electrician, infected in Pakistan, caused smallpox in 17 other patients in the 1970 outbreak in Meschede Hospital, Federal Republic of Germany, described in Chapter 4. He had had no direct contact with any of them.
The Bradford outbreak
The outbreak in Bradford started with a 9-year-old Pakistani girl, who developed smallpox in December 1961. She had travelled with her family from Karachi to London by air on 16 December 1961, and then by train to Bradford on 17 December (England and Wales, Ministry of Health, 1963). On 5 December, she had been vaccinated against smallpox and issued with an international certificate of vaccination. On 23 December she was admitted to Bradford Children’s Hospital with symptoms of malaria, and the presence of Plasmodium vivax was confirmed by blood examination. She responded to antimalarial drugs and was afebrile from 24 to 26 December. On 27 December she developed a low-grade fever and became apathetic and listless. Two days later her temperature rose to 40°C. On 30 December she developed petechiae on her face and neck and died. A post-mortem examination on 1 January 1962 attributed death to staphylococcal septicaemia and malaria. She was flown to Pakistan to be buried. Smallpox was not suspected; even the physical evidence of recent vaccination was not noted.
Between 11 and 13 January 1962,lO first generation cases of smallpox were discovered in the Bradford area (Fig. 23.2) and virologically confirmed. All were unvaccinated before this episode, except case No.2, in a 40-year-old visitor to an affected ward at Bradford Children’s Hospital—a man who had been vaccinated while a member of the armed services during the Second World War—and case No.3, a resident cook at the Bradford Children’s Hospital, who became ill on 6 January. The cook was admitted on 11 January to the Leeds Road Hospital, where a diagnosis of smallpox was made; she died the next day. The other cases were in 6 unvaccinated child inpatients (cases No.4-No.9), an 18-year old nurse (case No.10), and the 37- year-old pathologist (case No. 11) who had performed the post-mortem on the index case; 5 died.
The patients were promptly isolated and vaccinated; only 3 second-generation cases were recognized. The first 2 of these were in elderly male patients (cases No.12 and No.13) in the ward of another hospital (St Luke’s) to which case No.2 had been admitted just prior to his death. The third was a boy (case No.14) who had been in contact with case No.6, a child who had been transferred to the Wharfedale Children’s Hospital. All 3 second-generation cases were confirmed virologically; 2 recovered and 1 died, apparently from a heart attack.
To sum up, the Bradford outbreak comprised 14 cases; 7 of the patients died, 6 of them from smallpox. All the indigenous infections were contracted in hospital, and 4 hospitals were involved, with transmission in 3 of them. The outbreak was already rather large by the time it was recognized as being caused by smallpox, and there had been numerous opportunities for transmission, both within hospitals and in the general community. The task of identifying, tracing and vaccinating more than 1400 contacts and keeping them under surveillance was expensive, difficult and time-consuming. Although mass vaccination was never contemplated, vaccination clinics were opened because so many people had been already exposed by the time the outbreak was recognized. Practically the whole of the town’s population of 250 000 was vaccinated within 5 days (Douglas & Edgar, 1962).
This episode illustrates the unpreparedness of hospitals in the United Kingdom to cope with an outbreak of smallpox at that time, given the large proportion of unvaccinated professional and domestic staff, the difficulty of recognizing haemorrhagic-type smallpox and the risks thereby incurred, and the problems encountered in effectively containing the outbreak once it had been recognized. The response to the provision of vaccination clinics demonstrated the existence of considerable public fear and apprehension about smallpox.
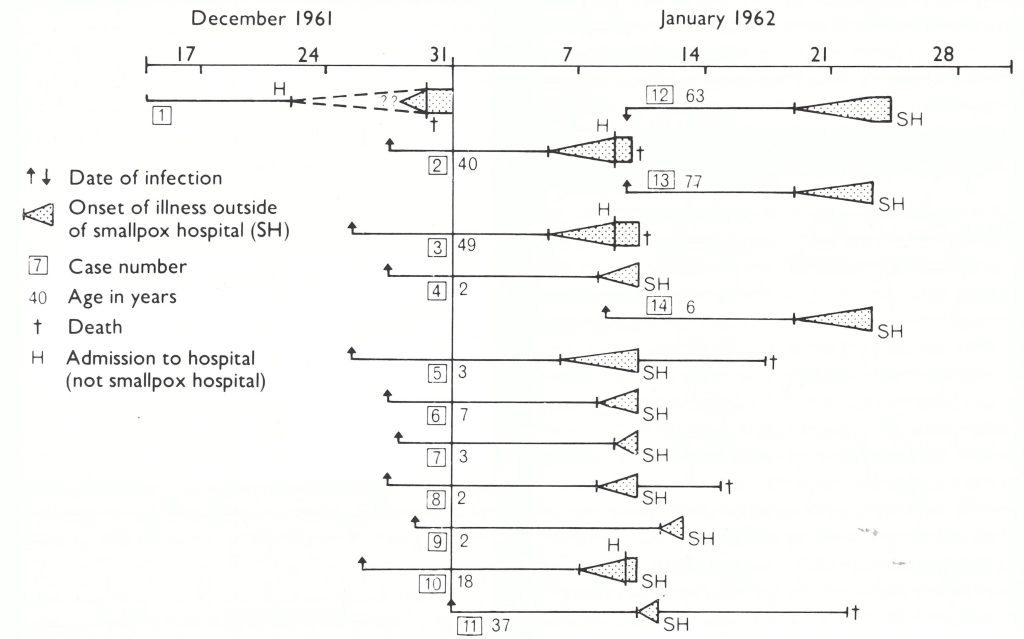
Fig. 22.3. Outbreak of smallpox in Bradford, England, in December 1961 -January 1962. All cases were hospital associated. The index case was a Pakistani girl who was admitted to the Bradford Children’s Hospital and died of unrecognized haemorrhagic smallpox. Cases No. 4-9 were patients at that hospital, case No. 2 a hospital visitor, and cases No. 3.10, and II a resident cook, a nurse and the pathologist, respectively. The three second generation cases occurred at another hospital to which case No. 2 had been admitted, and case No. 14 at a third hospital to which case No. 4 had been admitted before it was realized that he had smallpox. (Based on England and Wales, Ministry of Health, 1963.)
Outbreak in Skodsborg, Denmark, and Tromso, Norway
In August 1970 smallpox was imported into Denmark by a 22-year-old Danish medical student who had returned to Copenhagen after a curtailed holiday in Afghanistan. He had been successfully vaccinated in 1956 in Norway and revaccinated with liquid vaccine in May 1970, but the result had not been checked and he said later that the revaccination had been unsuccessful. He arrived in Kabul early in August, and was admitted to hospital on the 14th, suffering from severe gastroenteritis. Because cholera was suspected, he was transferred to the infectious diseases ward, where he was exposed to cases of smallpox between 17 and 19 August. On 26 August he returned to Copenhagen, feeling reasonably well and with a normal temperature.
On 28 August, when he was living in the staff quarters of the Skodsborg Hospital, near Copenhagen, he became feverish and was treated with penicillin. The next day he developed a rash, which was attributed to the penicillin. On 31 August he was admitted to the infectious diseases ward of the Blegdam Hospital with a diagnosis of pneumonia and dysentery. On 2 September, smallpox was suspected and he was placed in isolation. The State Serum Institute in Copenhagen confirmed the diagnosis by laboratory examination a day later. On 4 September the rash became confluent and haemorrhagic, and secondary infection occurred, with severe pneumonia. He later developed renal symptoms and died.
Some 400 direct or indirect contacts of the patient were identified, traced, vaccinated and put into quarantine at the Blegdam Hospital. They were mainly persons who had lived with the medical student in the dormitory at the Skodsborg Hospital and personnel at the Blegdam Hospital who had cared for the patient or had had contact with his clothing and bed-linen.
The Danish health authorities at no time contemplated mass vaccination, but maintained an alert for potential secondary cases until mid-October, because there might have been a missed case which would be detected only if the infection were transmitted to others. However, the only subsequent case that did occur was recognized in Norway.
Smallpox infection was carried to Tromso, in the far north of Norway, by a 25-year-old Norwegian medical student who had been living in the staff quarters of the Skodsborg Hospital in a room next to that of the Danish student. On 28 August, after they had talked briefly, the Norwegian student had left for Norway, travelling by car with another young Norwegian.
At the beginning of September, when the case in Denmark was confirmed as smallpox, the Norwegian medical student was identified by the Danish national health service as being a close contact. The Norwegian health authorities were notified, and on 4 September he was traced, vaccinated and kept under surveillance. Five days after vaccination he developed an accelerated reaction on the vaccination site. On 5 September, 9 days after contact, he developed low back pain and a rash suggestive of smallpox. Paired sera were sent to Oslo for serological tests, the results of which indicated smallpox. The person who had driven with him from Skodsborg to Norway and 33 other possible contacts were traced, vaccinated and isolated, but no further case occurred. This pattern, with good surveillance and minimal or no secondary spread, occurred in about half of the recognized importations into Europe during the period 1959-1 973.
IMPORTATIONS INTO NORTH AMERICA AFTER 1959
The transmission of smallpox had been interrupted in the USA and its territories in 1949. In that year the last known outbreak, resulting in 8 cases and 1 death, occurred in Texas and was probably due to an importation from Mexico, in which the last case of smallpox occurred in 1951. Reports of smallpox during the 1950s turned out on further investigation to have been cases of chickenpox. In Canada, endemic smallpox was eliminated in 1943, but there were 7 imported cases in 1945 and 1946.
As international air traffic increased in the 1960s and 1970s, and many more people travelled from Canada and the USA to Africa, South America and Asia, in which smallpox was still endemic, there was a constant and increasing risk of importing smallpox into North America. In contrast to Europe, there were no introductions of variola major from the Indian subcontinent into North America, despite the fact that Americans were the most numerous short-term travellers to the subcontinent. For example, Mack (1972) estimated that there were over 3 times as many travellers to India from the USA as from the Federal Republic of Germany (in 1969, 50 000 Americans compared with 14 000 Germans). However, after 1958, there were 5 importations from India into the Federal Republic of Germany but none into the USA. Only 1 importation of smallpox into North America was reported—a single case of variola minor imported from Brazil into Canada via the USA.
Sixteen years after Canada’s last case of smallpox, the disease was brought back to Toronto from Brazil in 1962 by a 15-year-old Canadian boy, who had lived for several years in Parana State, Brazil. At the end of July 1962 he had been in contact with 4 children who were said to be suffering from chickenpox. On 10 August he and his family left Brazil by air and arrived in New York City on 11 August. Just before his departure from Brazil, the boy had developed fever and malaise which were diagnosed as influenza. On arrival in New York he had presented a smallpox vaccination certificate dated 22 July 1962 (Wkly epidem. rec., 1962), but in fact he had not been vaccinated for approximately 6 years (Best & Davis, 1965).
The family remained in New York for some 6 hours before boarding a train to Toronto. Soon after his arrival there on 12 August, the boy developed a rash, which 2 days later had spread widely over the body, showing a typical centrifugal distribution. He was admitted to hospital in Toronto on 18 August. The clinical diagnosis of smallpox was confirmed on 20 August by the isolation of variola virus. Passengers on the plane on which he had travelled from Brazil to New York were identified, vaccinated and placed under surveillance, as were the members of his family and other known close contacts in Toronto. Persons who had travelled on the train from New York or had had possible contact in the railway stations were requested through the mass media to report for vaccination, and those who did so were also placed under surveillance. No additional cases were reported.
IMPORTATIONS INTO JAPAN

Plate 22.4. The Japanese government official who was infected in Dhaka in 1973 worked in this conference room of the parliament building in Tokyo while suffering the prodromal symptoms of smallpox. which was diagnosed a few days later. Health officials disinfected the room.
Japan, the only large industrialized country in eastern Asia, had been free of smallpox since 1951. There were a few imported cases each year until 1955; then, after an absence of smallpox for 18 years, 2 importations occurred, in 1973 and 1974, at a time when the number of travellers from Japan to the Indian subcontinent had increased substantially. The first case was in a 33-year-old Japanese traveller, who had stayed in Dhaka, Bangladesh, from February to mid-March 1973, when Dhaka and its surrounding areas were experiencing an extensive epidemic of smallpox (see Chapter 16). The patient, who was reported to have been vaccinated in midJanuary, returned to Tokyo via Bangkok on 18 March, became ill on 23 March and was hospitalized on 26 March. On 31 March he was isolated in the Tokyo Metropolitan Infectious Diseases Hospital and a diagnosis of smallpox was virologically confirmed a day later. Close contacts were identified and placed under surveillance, but no secondary cases occurred (Wkly epidem. rec.,1973a).
The second importation into Japan occurred in January 1974 (Wkly epidem. rec.,1974). The index case was a Japanese Buddhist pilgrim, who was exposed to smallpox while travelling through northern India. He had no record of vaccination in childhood, and the result of his vaccination in Japan on 7 December 1973 was interpreted to be a “reaction of immunity”. He developed symptoms on 22 January 1974, 5 days after his return to Japan. Control measures, initiated on 28 January, when smallpox was suspected, included the isolation of the patient and his family, and the vaccination and surveillance of some 270 persons considered to be close contacts, including 19 pilgrims who had accompanied the patient to India. No secondary cases occurred.
IMPORTATIONS INTO RECENTLY ENDEMIC COUNTRIES, 1959-1976
Besides the countries of Europe, North and Central America, Oceania and eastern Asia in which smallpox was not endemic in 1959 (see Chapter 9, Fig. 9.3), there were a number of countries in Africa, South America, southeastern Asia and south-western Asia in which smallpox had been endemic in the 1950s but had been eliminated during the next decade, and which were thereafter exposed to the risk of importations from neighbouring endemic areas. Importations also occurred across the borders of countries that continued to harbour foci of endemic smallpox (see, for example, Chapter 15, which discusses importations from India into Nepal). Data on importations into non-endemic countries of South America are reasonably complete from 1959 onwards, but data from Africa and Asia were very scanty prior to the establishment of the Intensified Smallpox Eradication Programme in 1967. Even after 1967, not much information is available on importations into African countries. Comments on importations into these continents are therefore limited to tabulations of importations from one country into another within each continent, from 1959 for South America, and from 1967 for Africa and Asia. However, a connected series of outbreaks in Iran, Iraq and the Syrian Arab Republic in 1970-1972 will be described in greater detail.
Africa
By 1958, 13 of the 47 countries of Africa appeared to have become free of endemic smallpox. In the period 1959-1966, when WHO encouraged the remaining African States to institute national smallpox eradication programmes, 17 countries (5 of them reinfected) are believed to have succeeded in interrupting smallpox transmission (Table 23.6). When the WHO Intensified Smallpox Eradication Programme began in Africa in 1967, smallpox was endemic in 23 countries, and between 1968 and 1976 endemicity was re-established in 3 countries.
Between 1967 and 1976, over 70 importations of smallpox from neighbouring endemic countries into non-endemic countries were reported (Table 23.7). International boundaries in Africa, most of them drawn during the 19th century by the European colonial powers, bore little relationship to ethnic or tribal distribution, so that many of them were crossed and recrossed as frequently as were state or district boundaries in a country such as India. The transfer of smallpox across these boundaries occurred repeatedly, and the figures for importations in the late 1960s, when smallpox was becoming much less common and surveillance was improving, are not complete. It is known that in several instances (indicated by the symbol “+” in Table 23.7) there were more importations than those reported; it is also clear that importations from Ethiopia into neighbouring countries were at least as numerous before 1971 as after that year, when effective surveillance began.
In most cases the disease did not persist long after importation, as, for example, after the numerous transfers from Ethiopia to Djibouti and Somalia between 1971 and 1975. However, importations into the Sudan (1967), Botswana (1971) and Somalia (1976) led to the re-establishment of endemicity in the recipient countries and had a considerable impact on the global eradication programme. In each country, transmission persisted until a full-scale eradication programme had been set up and the local health staff had grasped the concept of surveillance and containment, which enabled them finally to interrupt transmission. Of more than 17 importations into non-endemic countries of western Africa that were recorded after 1966, at least 10 originated in Nigeria. Ethiopia was an even more important source country: all but 7 out of more than 47 importations reported anywhere in Africa between 1971 and 1976 originated there.
Table 23.6: Africa: last year of smallpox endemicity in individual countries or territories
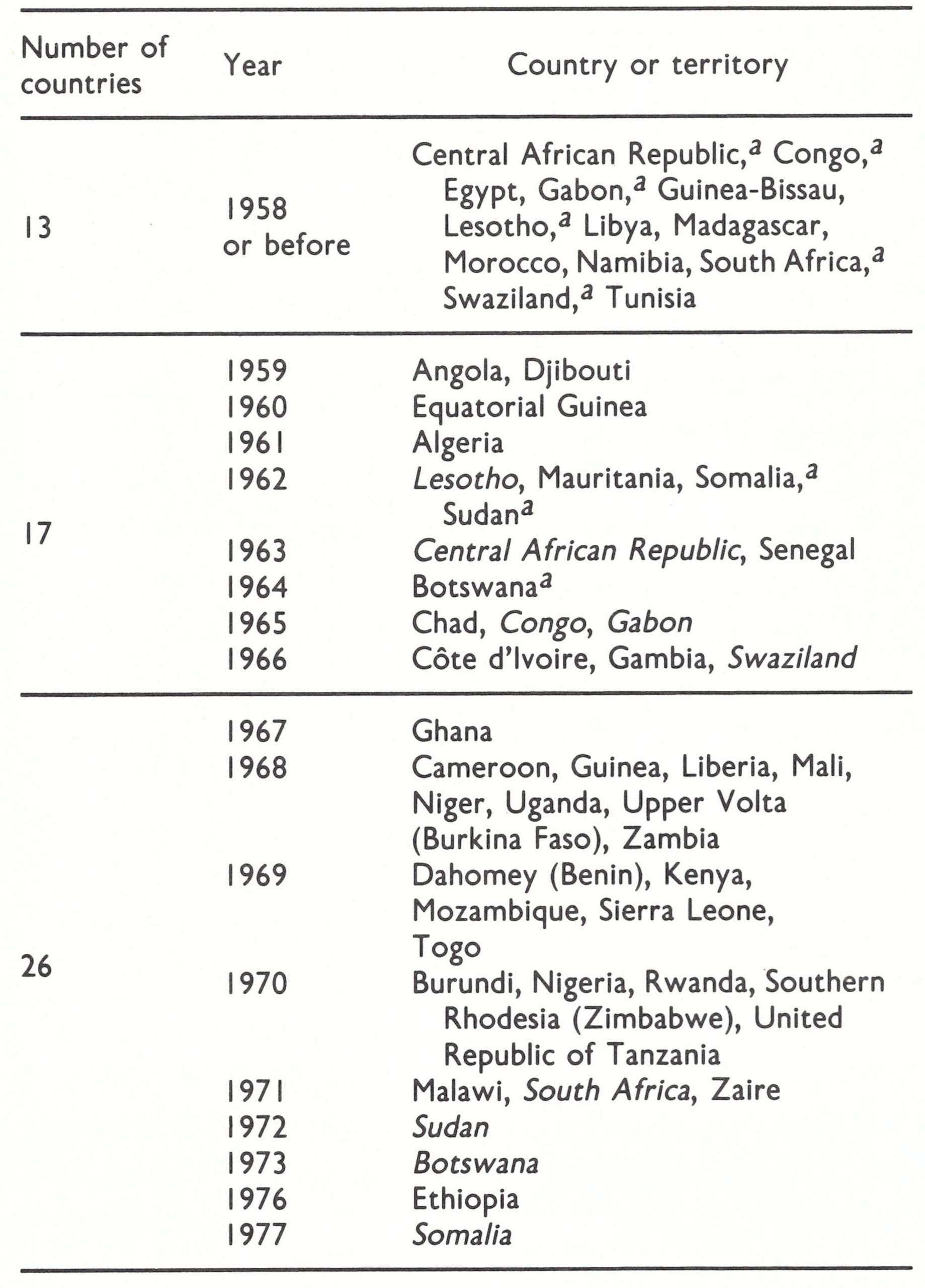 a Endemic smallpox re-established later, and subsequently eliminated, in the year indicated by the italicizing of the country's name.
a Endemic smallpox re-established later, and subsequently eliminated, in the year indicated by the italicizing of the country's name.
Table 23.7: Africa: non-endemic countries experiencing importations, 1967-1976, by regions
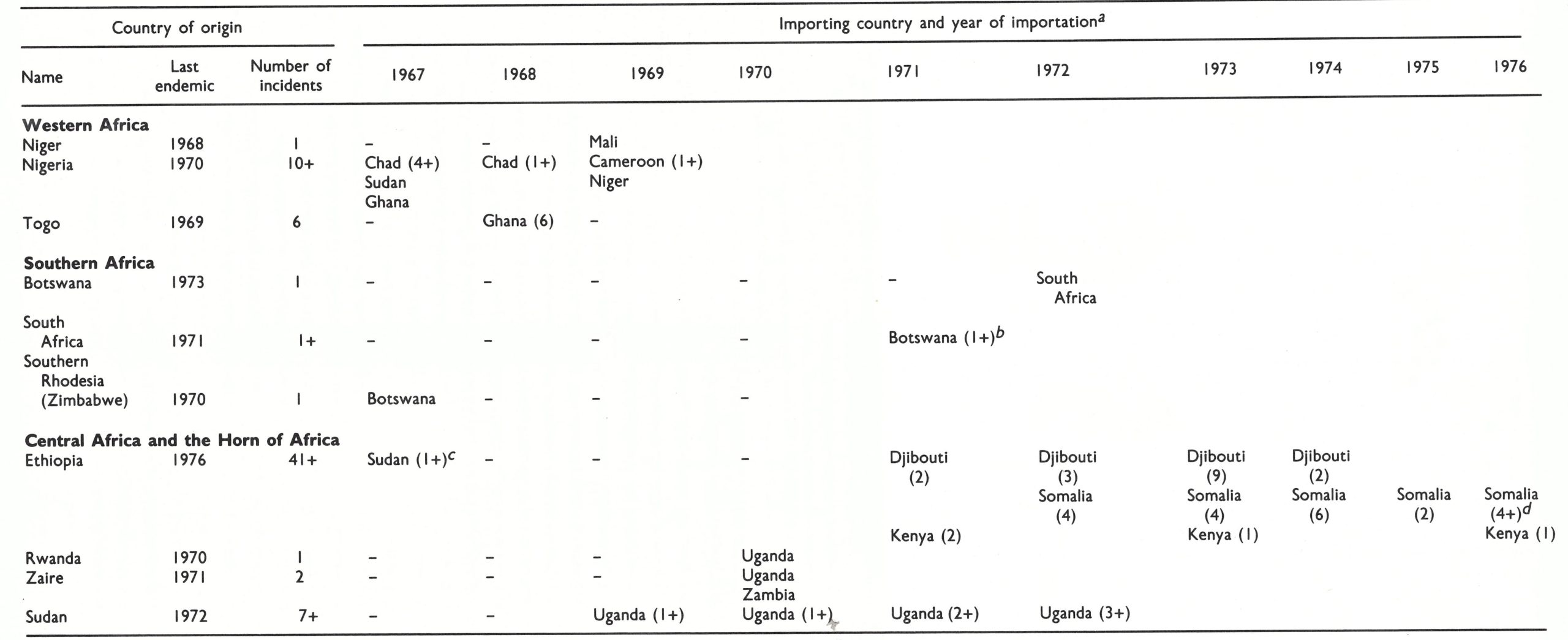 a Numbers in brackets indicate number of separate importations in the year indicated.
a Numbers in brackets indicate number of separate importations in the year indicated.
b This importation led to the re-establishment of endemic smallpox in Botswana (see Chapter 20).
c This importation led to the re-establishment of endemic smallpox in the Sudan (see Chapter 18).
d The last of these importations led to the re-establishment of endemic smallpox in Somalia (see Chapter 22).
South America
By 1959 smallpox transmission had been interrupted in Chile, Peru, Uruguay and Venezuela. In the 8-year period from 1959 to 1966 another 5 countries became smallpox free: Argentina, Bolivia, Colombia, Ecuador and Paraguay. Except in Peru, importations during the period 1959-1970 did not result in large numbers of cases. However, in Peru in 1963, following its introduction from Brazil, variola minor became endemic and remained so until 1966. From 1964 onwards, Brazil was the only known source from which smallpox was exported to other countries in the subcontinent (Table 23.8).
Southern Asia
Apart from importations into countries of south-eastern Asia that had long been smallpox-free (see Chapter 8), information on importations into the non-endemic non-industrialized countries in Asia is fragmentary before 1967 and still incomplete after that date. What is known can be most effectively discussed in respect of 2 regions: countries adjacent to India, and southwestern Asia.
Countries adjacent to India
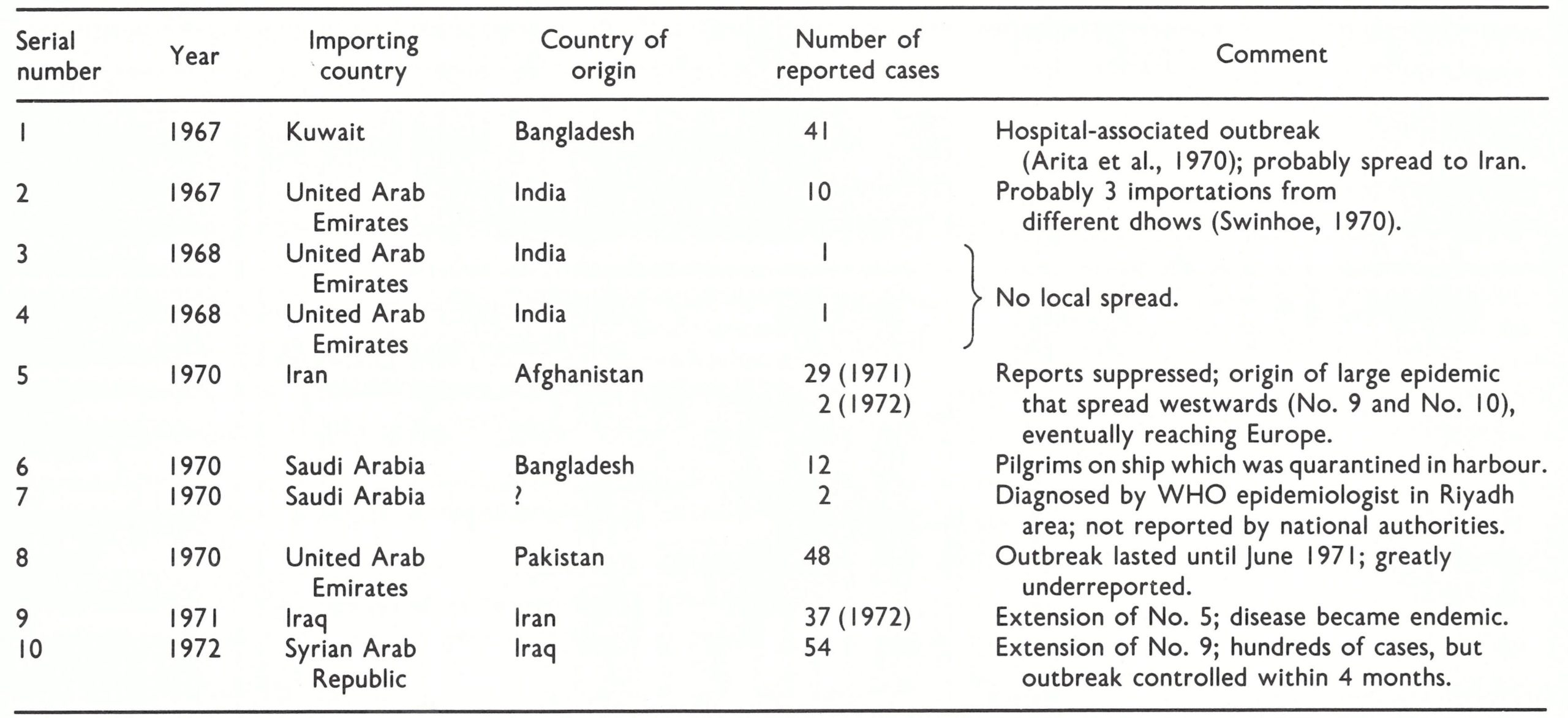
Reported importations into non-endemic countries near India during the period 1967-1974 are shown in Table 23.9. The 12 outbreaks fall into 5 groups: importations into Sri Lanka, Afghanistan, Bangladesh, Bhutan and Burma.
Importations into Sri Lanka (outbreaks No.2 and No.6) and Afghanistan (3 outbreaks, grouped together as No.7) were effectively contained. Sri Lanka had been free of endemic smallpox since 1951 and was vigilant in its efforts to maintain that status. The 2 reported cases were contained without local spread, vaccination being carried out on a large scale in Kandy (outbreak No.2) and Colombo (outbreak No.6) respectively. Three importations into Afghanistan occurred in 1973, the year after smallpox had been eliminated; they were discovered promptly and the containment methods used during the eradication programme limited spread.
The importation of smallpox into Bangladesh early in 1972, following the return from India of millions of refugees, led to the re-establishment of endemic smallpox and to many thousands of cases. Eradication was not achieved until October 1975.
Table 23.8: South America: reported importations of smallpox into non-endemic countries, 1959- 1970a
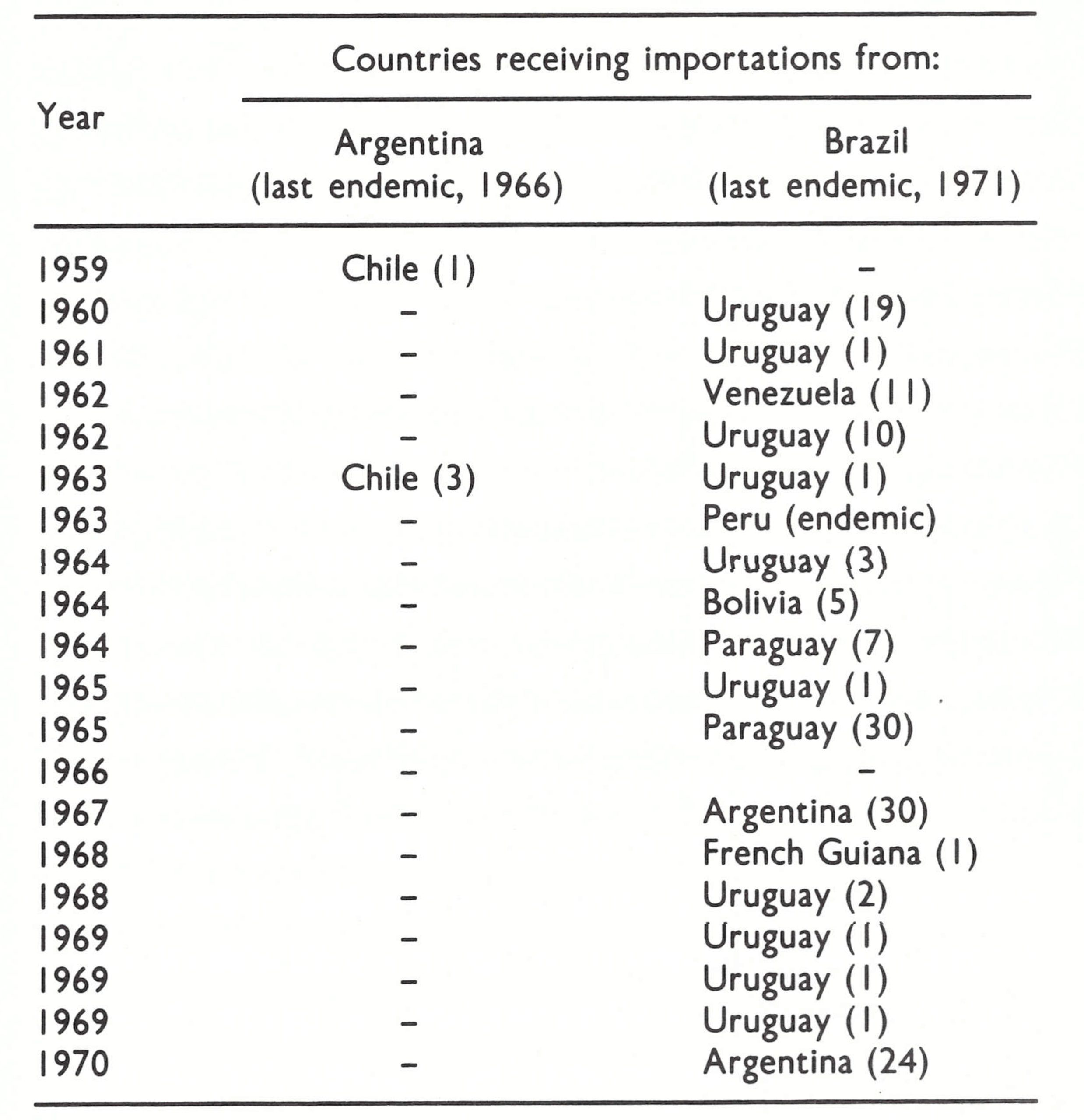 a Numbers in brackets indicate the number of reported cases associated with each importation.
a Numbers in brackets indicate the number of reported cases associated with each importation.
Table 23.9: Importations of smallpox into non-endemic countries adjacent to India, 1967- I974

From an epidemiological standpoint, Bhutan is equivalent to an Indian state, so that it is not surprising that smallpox spread across the border from Assam (outbreaks No. 1, No.8, and No.9). Because of the small and sparse population the disease did not persist. In Burma, on the other hand, introductions from Chittagong, East Pakistan (Bangladesh), in 1968 and 1969, shortly after smallpox had been eliminated (outbreaks No.3 and No.4), spread without control for several months, because it was very difficult for the health services to operate in the area, in which there were many insurgents.
Southwestern Asia
This region (Fig. 23.3) consists of Iran (now the Islamic Republic of Iran) and Iraq to the north, Israel, Jordan, Lebanon and the Syrian Arab Republic to the west, and the Arabian peninsula, comprising Democratic Yemen, Saudi Arabia, Yemen, and the 5 Gulf states of Bahrain, Kuwait, Oman, Qatar and the United Arab Emirates. The Arabian Peninsula is mostly desert and the majority of the population is concentrated in a few cities. However, this area was the crossroads of smallpox transmission, since between 1 and 2 million pilgrims came to Mecca by sea, land and air every year, many from the endemic countries of Africa and Asia. Even more important were the numerous migrant workers in the Gulf states, mostly from Pakistan and India.
By 1963, all countries in south-western Asia, except Yemen, appeared to have interrupted smallpox transmission, but frequent importations, particularly from the Indian subcontinent, and deficiencies in the notification of cases to WHO (including the occasional suppression of reports) made it very difficult to know precisely when these countries became non-endemic and to judge the magnitude of outbreaks following importations (Table 23.10). Smallpox was poorly reported, not only because of inadequate health services, but also because of national pride and the fear that the presence of the disease might lead to restrictions on travel or the imposition of an economic embargo by neighbouring countries. In Saudi Arabia, it was believed that reports of the presence of smallpox would inhibit visits by pilgrims. The reliance of some countries in this area on their own capacity to control outbreaks of smallpox occasionally resulted in large numbers of cases and the spread of the disease for up to 2 years. In some of these countries, moreover, clinical and laboratory diagnoses were unreliable, so that the health services could not be certain whether the cases that they recorded were indeed smallpox. They hesitated to request WHO’S assistance in improving laboratory diagnosis, because the rendering of such support might lead to international disclosure of the suppression of information about outbreaks.
Between 1967 and 1972, Iran, Iraq, Kuwait, Saudi Arabia, the Syrian Arab Republic, or the United Arab Emirates continued to report cases of imported smallpox every year except 1969. Brief comments on these outbreaks are provided in Table 23.10. The 1970-1972 outbreak, which originated in Afghanistan and spread through 4 countries—Iran, Iraq, the Syrian Arab Republic and Yugoslavia—was of particular interest and importance, because of its extent, the degree of underreporting, and its occurrence at a time when the Intensified Smallpox Eradication Programme was in full swing.
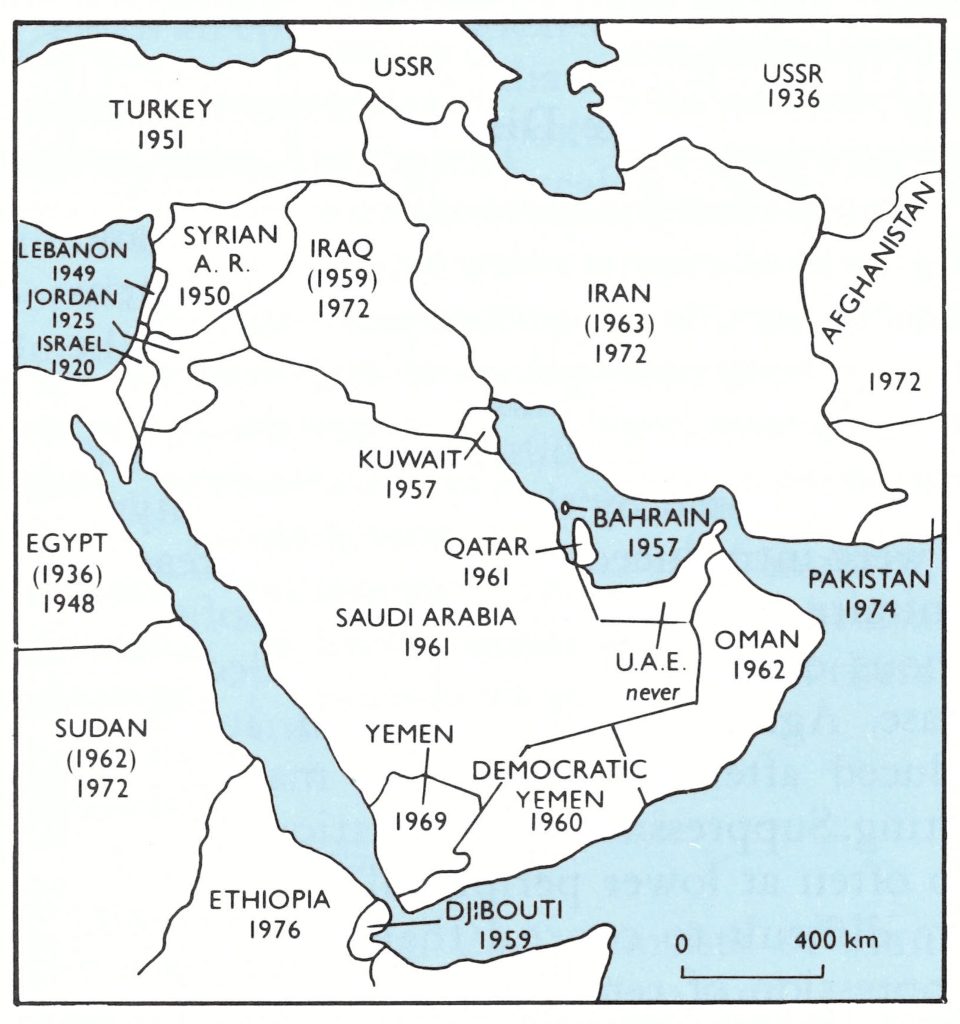
Fig. 22.3. South-western Asia: years in which smallpox ceased to be endemic in each country, before the 1970-1972 epidemic in Iran, Iraq and the Syrian Arab Republic.
Table 23.10: Importations of smallpox into non-endemic countries of south-western Asia, 1967- I972
THE 1970-1972 OUTBREAK IN SOUTH-WESTERN ASIA AND EUROPE
Iran officially reported 29 cases in 1971 and 2 in 1972; Iraq reported 37 cases and the Syrian Arab Republic 54 cases in 1972 (Table 23.10). However, it was known that the actual numbers of cases were much greater, especially in Iran, and it was feared that the epidemic in these countries would cause a substantial set-back to the global eradication programme.
Epidemic spread began in Iran towards the end of 1970, but reports of cases were suppressed. Iran had eliminated smallpox in 1963 by a well-organized mass vaccination campaign; one additional outbreak is known to have occurred in Khorramshahr in 1967, but it was not reported. Apart from this experience and the excessive measures recently taken against countries which had reported cholera, the authorities in Iran had also to take into account the forthcoming major celebrations commemorating the 2500th anniversary of the Persian Empire, which they did not wish to jeopardize ;the major function was to be held in Persepolis, in Fars Province, on 12 October 1971, and the heads of state and dignitaries from more than 100 countries were to attend it.
However, extensive outbreaks of smallpox could not long go undetected in a large, cosmopolitan country such as Iran. Acting on information received through the United States Center for Disease Control, WHO sent a cable to Iran on 13 January 1971: “Informed presence smallpox cases 46, deaths 8, Tabriz, E. Azerbaijan province . . . appreciate any additional information.” About a month later Iran cabled that 9 cases had, indeed, occurred, saying that 3 infected Afghans in Mashhad had led to 4 more cases there and 2 in Tabriz. No epidemiological details were given and no further cases were reported.
Suppression of Information on Quarantinable Diseases
Suppression of the reporting of diseases of international importance has been —and remains —a common practice in many countries, both developing and developed. So far as the countries of south-western Asia are concerned, the failure to report smallpox can be ascribed in part to recent experience with cholera. This disease, which had been absent from the area for many years, was reintroduced in the mid-1 960s. Governments were unfamiliar with it, and although the outbreaks were caused by the milder eltor biotype, there were many deaths. A variety of measures were introduced to control the spread of cholera, including the imposition of a cordon sanitaire, prohibition of the import of goods and widespread vaccination. These had a serious economic impact, which led some governments to suppress reports of the disease. Against this background, it is not surprising that when smallpox was reintroduced after an absence of many years, governments sometimes responded by not reporting. Suppression of information occurred not only at the central national level, but also often at lower peripheral levels within countries. Smallpox, however, was rather more difficult to conceal than cholera.
WHO actively sought to discourage the suppression of reports of smallpox. Several approaches were used. Endemic countries were encouraged to report fully, and when this led to an apparent increase in the recorded incidence the governments were congratulated on their improved surveillance. As the numbers of smallpox cases declined, WHO encouraged countries to offer a reward for reporting cases to both health personnel and the public, to make it clear that government officials appreciated receiving this information. Finally, when rumours of smallpox in what was thought to be a smallpox-free country were reported by such persons as visitors or foreign officials, governments were asked to institute inquiries.
During the following months, reports of smallpox in Iran from various sources grew more and more numerous until finally, on 17 November 1971, the Surgeon General of the United States Public Health Service cabled the following message to the Director General of WHO: “Reliable reports of smallpox in Shiraz and Abadan, Iran. Can you inquire as to the validity of the report? Until matter resolved U.S. will require valid [vaccination] certificates of arrivals from Iran.” It should be noted that the USA had discontinued routine vaccination in 1971 and naturally a smallpox epidemic in a country with which the USA was in close contact was of great concern. Iran’s cabled response to an inquiry from WHO, 11 days later, was that 20 cases had occurred between 28 August and 3 October 1971 but none since then, making a total of 29 acknowledged and reported cases in 1971.
Nothing further was heard until 6 March 1972, when Iran, without prompting, notified WHO that 2 cases had occurred on 16 January on its “eastern border”. Following a request by WHO for more information, the Ministry of Health stated that the reported cases had occurred in the children of a Baluchi mother who normally lived in Quetta, Pakistan. No information was given as to their recent whereabouts in Pakistan, and at that time active surveillance had revealed no cases in the Quetta area.
At this point it became clear that an epidemic, which could no longer be concealed, was occurring-and not merely in Iran. On 5 March 1972, Iraq reported to WHO by cable that sporadic cases had occurred on its border with Iran and requested 500 000 doses of vaccine. On 17 March, Yugoslavia reported the presence of smallpox to WHO; on 25 March, the Syrian Arab Republic reported the discovery of 15 cases; and on 28 March, the Federal Republic of Germany notified a case in Hanover, in a man who had come from Yugoslavia. In the face of this evidence, the resistance of all the countries of south-western Asia to reporting the disease weakened, but it did not collapse.
Iran
Iran (population in 1972, 30.3 million) officially reported 31 cases of smallpox in 1971-1972. The suspicion that there had been many more cases was confirmed following a visit to Iran by Henderson from 2 to 13 August 1972. He reported that over 2000 cases had been hospitalized and that 6000-8000 cases had probably occurred. Subsequently, a confidential government report supplied to the Global Commission for the Certification of Smallpox Eradication in December 1978 gave details of 1996 cases in 400 widespread outbreaks between November 1970 and September 1972 (Fig. 23.4). Of these cases, 1349 had been confirmed by laboratory tests.
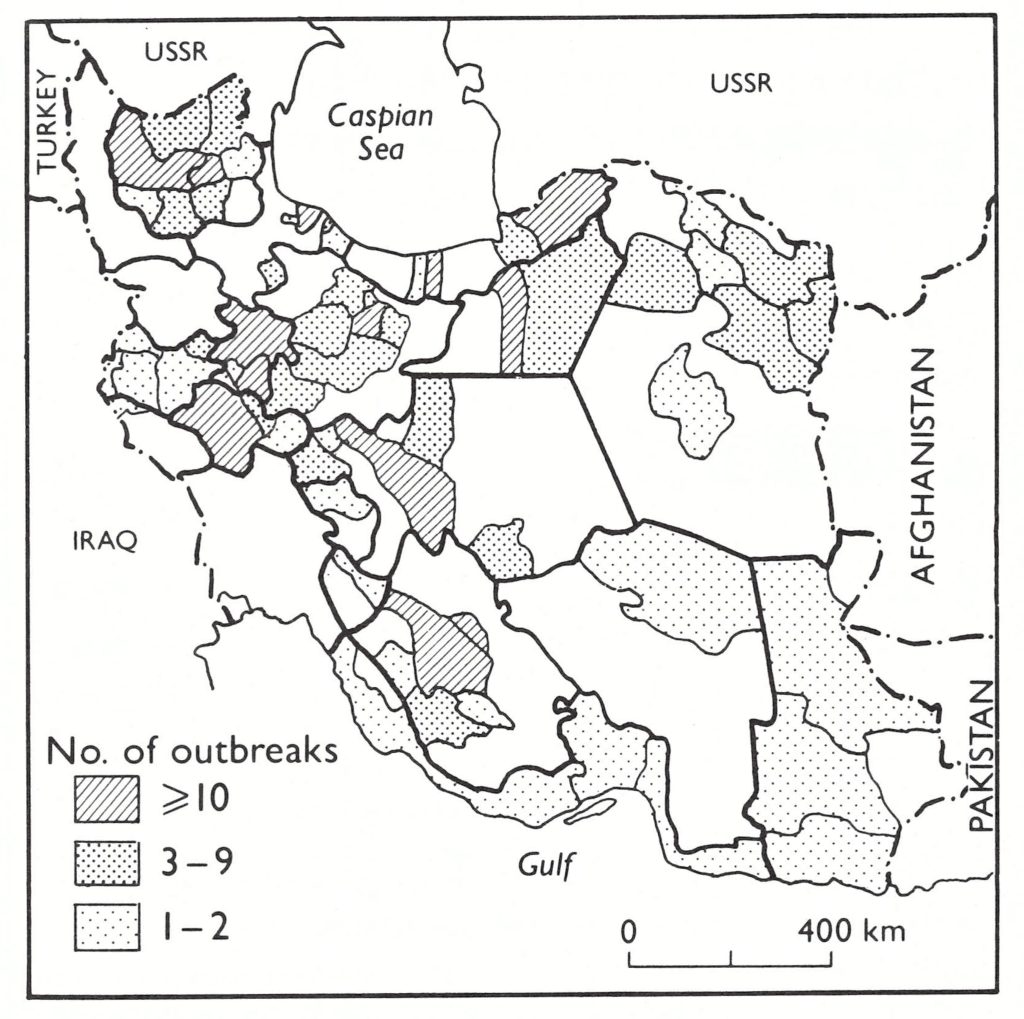
Fig. 23.4. Iran: distribution by district of 400 smallpox outbreaks with some 2000 locally reported cases over the period between November 1970 and September 1972.
The epidemic seems to have started when an Afghan family of 6 left their village near Kabul on 16 October 1970 and began a pilgrimage through the smallpox-endemic areas of Afghanistan to the holy city of Mashhad, in Khorasan Province in northeastern Iran, where several thousand pilgrims congregate daily during the hadj. The family arrived in Mashhad on 20 October. One of the children developed a rash on 3 November and 2 others were similarly afflicted 6 weeks later. Although the first imported case was apparently promptly diagnosed by a local health worker, the disease had already been transmitted to many other pilgrims.
The primary wave of smallpox spread to another 6 provinces in the north (Fig. 23.5), which were to be the most severely affected and for the longest time. Once smallpox reached Teheran it was amplified by hospital-associated spread, and became a typical urban outbreak affecting slum areas and semi-urban districts around the city. Teheran and the original foci in the northern provinces became the principal sources of infection for another 12 provinces in the west-central part of the country during 1971, from which 2 more in the southern part were affected in 1972. Subsequent review suggested that the confidential report, which had noted that 73% of the cases occurred in cities, seriously underreported the numbers of cases occurring in the rural areas.
The strategy adopted by the health authorities was containment by mass vaccination, with only a rudimentary surveillance component. The little freeze-dried vaccine available was below standard; liquid vaccine was used for most vaccinations. Primary take rates were reported to be no more than 65%. Many persons who claimed to have been vaccinated subsequently developed the disease. Although it was reported that 12.5 million vaccinations had been performed in 1970 and 19.8 million in 1971, smallpox continued to spread throughout Iran. There were major outbreaks in Shiraz, which was the largest city near Persepolis, where the celebrations were to be staged. The health authorities conducted repeated mass vaccination campaigns in Shiraz itself, but partly because liquid vaccine of low potency was being used, transmission was not interrupted. The authorities were in a quandary ; they recognized that the vaccine was of low potency, but could not apply to WHO for potent vaccine because of instructions issued at a higher level of government. Eventually, in November 1971, freeze-dried vaccine was sent to Iran by WHO Headquarters: 2 million doses in 1971, followed by 11 million in 1972. A second round of mass vaccination was performed and during 1972 more than 20.6 million people were vaccinated. The last case of smallpox in Iran was reported from Fars Province, with onset of rash in September 1972. The epidemic in Iran lasted for 22 months, and at least 400 outbreaks occurred in 70 out of the 162 districts in the country. Iraq Once the Iranian outbreak had begun in Mashhad in November 1970, smallpox moved relatively quickly along the main road to Teheran and Kermanshah, which is the principal route to Baghdad, the capital of Iraq (population in 1972, 10 million). It seems likely that smallpox arrived in Baghdad at the end of 1971 and then spread north and south along the principal roads running parallel to the Tigris and Euphrates rivers (see Fig. 23.5). An estimated 800 cases of smallpox probably occurred in the country, the last case being in Baghdad in June 1972.
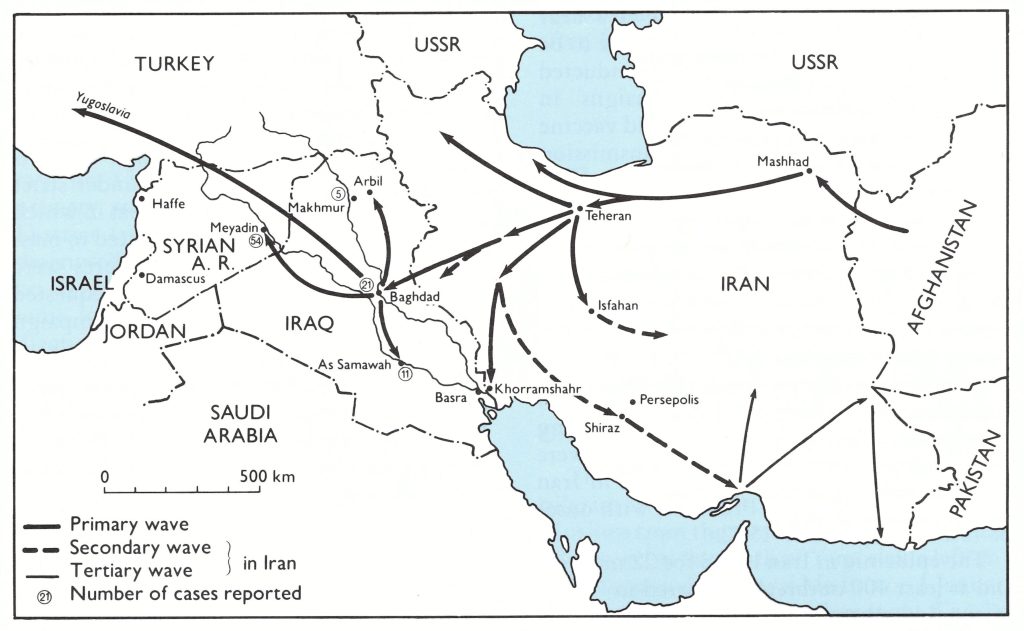
Fig. 23.5. Spread of smallpox in Iran, Iraq and the Syrian Arab Republic, 1970-1972. The disease was introduced from Afghanistan into Mashhad, Iran, in October 1970. There were three waves of dispersion through Iran, which lasted over a period of 22 months. By the end of 1971 smallpox had crossed into Iraq, where it spread north to Arbil and south to As Samawah. Transmission in Iraq was interrupted by June 1972. In February 1972. smallpox spread from Baghdad in Iraq to Meyadin in the Syrian Arab Republic, where a smaller outbreak occurred that was contained by June 1972.
The presence of smallpox in Iraq first came to the attention of WHO when a cable was received on 5 March 1972 reporting the presence of smallpox cases on its northern border with Iran and requesting 500000 doses of vaccine. The Smallpox Eradication unit received further information on the outbreak on 8 March, during the debriefing of Dr N. Maltseva, who had been touring vaccine production facilities in Iraq, Iran and the Syrian Arab Republic in January and February. She reported that there had been cases of smallpox in Baghdad in January. On 18 March, Iraq informed WHO that 20 cases had occurred in widely separated areas: in Arbil in the north-east, in Baghdad, and in As Samawah in the south. A letter dated 19 March from the Ministry of Health mentioned 2 more cases and stated that the infection had spread from Arbil to Baghdad and from there to As Samawah. It was reported that all known cases had been isolated in fever hospitals and that contacts had been vaccinated and placed under strict surveillance. The population of areas in which cases had been notified were subjected to mass vaccination and surveillance measures were instituted. All provinces had been requested to intensify the mass vaccination campaign begun in December 1971. Subsequently, it was reported that over 2.3 million vaccinations were performed in 1971, followed by 8.2 million in 1972 and 1.2 million in 1973.
Three more cases were reported in Baghdad in June and 1 in July 1972. In August Dr Ehsan Shafa, of the Smallpox Eradication unit, visited Iraq. He was presented with records of only 37 cases, with 5 deaths, in 3 provinces, for none of which could the source of infection be determined. However, the pilgrim responsible for the outbreak in Yugoslavia (see below) had been infected between 3 and 6 February 1972, before the onset of any of the reported cases. In addition to Dr Maltseva’s report, an oral statement by a WHO nurse indicated that cases had occurred in a province for which data had not been provided. Furthermore, cases from Iraq had given rise to outbreaks in both Yugoslavia and the Syrian Arab Republic, and long experience with smallpox had shown that such exports to other countries usually indicated the presence of an outbreak of considerable size in the exporting country.
When Dr Shafa reviewed the data with a special technical committee in Iraq, the meeting agreed that a number of cases had been “overlooked” or “misdiagnosed”. A more realistic estimate put the total number of cases at a minimum of 800. Nevertheless, the measures taken by the health authorities were found to have interrupted transmission in June 1972. Slow transmission might still have been going on undetected only to flare up later, but continued surveillance in the latter part of 1972 and in 1973 indicated that transmission did not continue after June 1972.
Syrian Arab Republic
On 25 March 1972, the Syrian health authorities notified WHO that cases of smallpox had been discovered in the Syrian Arab Republic (population in 1972, 6.7 million). The index case was reported to be a 9-year-old boy who had visited Baghdad with his mother for a religious festival between 28 February and 5 March. He developed fever on 9 March, 4 days after his return from Iraq, and rash on 15 March. He was a pupil at the primary school in a village near Meyadin District (see Fig. 23.5). His condition was diagnosed at a dispensary as chickenpox, but on 21 March another schoolchild from the same locality, with a severe skin rash, was diagnosed by a physician in Meyadin as having smallpox. Simultaneously, a physician in another town diagnosed smallpox in 2 other schoolchildren with skin rashes. The disease spread through school contacts to the other villages in the area. A total of 54 cases and 2 deaths were reported, the date of onset of illness in the last case being 27 April 1972.
To control the outbreak, an isolation camp was established in Meyadin and the affected villages were cordoned OK Vaccination of everyone in the Syrian Arab Republic was made compulsory, starting with the affected region. WHO provided more than a million doses of freeze-dried vaccine and a supply of bifurcated needles in March 1972. Health centres and dispensaries were reported to have performed 75 748 vaccinations in 1971, 897 828 in 1972, and 106 176 in 1973.
There were inconsistencies in the data reported. The onset of illness in the index case occurred only a few days before the onset in those reported as secondary cases, an event which suggests multiple introductions or an earlier start to the outbreak. Nevertheless, the government had acted promptly in reporting to WHO and appeared to have done reasonably well in containing further spread.
However, pockmark surveys conducted in 1978 during the preparation of a report for the Global Commission for the Certification of Smallpox Eradication confirmed that far more cases had occurred in the Meyadin area in 1972 than had been reported (see Chapter 26). In fact, one case with pockmarks dating back to 1971 was found in Haffe District, on the other side of the country. Evidence of facial scarring, indicating the occurrence of cases in 1966-1967, which had not been reported, was also found. It was not clear in this instance whether the reporting of cases had been suppressed or whether cases had gone unnotified or had been misdiagnosed as chickenpox. However, the International Commission that visited the country in 1978 found that no smallpox had occurred there after 1972.
Yugoslavia
The reappearance of smallpox in Yugoslavia in 1972 (population in that year, 20.8 million), after more than 45 years without a case, was totally unexpected and caused great concern throughout the world. The epidemic has been described by Stojkovic et al. (1974) and, more briefly, by Litvinjenko et al. (WHO/SE/73.57).
Origin of the epidemic
The outbreak began with an infected pilgrim returning from Iraq. A bus-load of 25 Muslims from the semi-autonomous province of Kosovo in the south of Yugoslavia left on a pilgrimage to Mecca and Medina on 1 January 1972. On their way home they spent 3 nights in Baghdad and visited religious sites between Basra and Baghdad from 3 to 6 February, before leaving for Yugoslavia. The index case, a 38-year old Muslim priest, returned to his village of Danjane (population, 750), 20 kilometres north-east of Djakovica (Fig. 23.6), on 15 February 1972. The next day he fell ill with symptoms of fatigue, shivering and fever, which he thought were due to the strenuous bus journey of several thousand kilometres. He denied ever having had a rash and a month later no evidence of skin lesions could be seen on his face or body. Although he had been vaccinated on 5 December 1971, no vaccination scar had developed. No one else on the bus contracted smallpox.

Fig. 23.6. Spread of smallpox in Yugoslavia in 1972. The index case arrived from Iraq on 15 February; the last 2 cases in Yugoslavia became ill in Kosovo and Belgrade on 11 April. The case in Hanover, Federal Republic of Germany, occurred on 22 March.
Spread of smallpox in Kosovo Province
A few days after his return, the index case was visited by many of his close relatives, friends and acquaintances, 11 of whom contracted smallpox. Nine cases occurred in Kosovo Province, 1 in Novi Pazar, 160 kilometres to the north (in Serbia), and 1 in a village north of Novi Pazar. These 11 cases were first generation cases, with onsets between 1 and 7 March (Fig. 23.7). None of them was suspected to be smallpox.
It was not until the evening of 14 March that smallpox was recognized by a doctor in the infectious diseases ward of the hospital in Prizren, in the district adjacent to Djakovica, who notified the federal health authorities of suspected smallpox in 4 patients coming from Danjane. The same day 4 other patients admitted to the hospital in Djakovica were recognized as having smallpox.
On 17 March the Yugoslav federal health authorities cabled to WHO that 8 cases of suspected smallpox had been detected. The clinical diagnosis was confirmed by laboratory tests on lesion material at the Institute of Immunology and Virology in Belgrade, confirmation being sent to WHO on 20 March. On 21 March, the WHO Regional Office for Europe informed Member States of the situation and a day later Dr R. Lindner, an Austrian epidemiologist who had previously worked in the Indonesian smallpox eradication programme, was sent to Yugoslavia as a WHO consultant to assist with the investigations.
Between 15 and 31 March, 100 additional cases of smallpox occurred among the immediate family members and relatives of known cases and among the patients of hospitals in Djakovica and Prizren, who had come into contact with cases before the correct diagnosis had been made (Fig. 23.7). This group formed the second generation of cases in Kosovo. Between 1 and 11 April, 14 more cases were recorded in Kosovo. With this third generation of cases the epidemic in Kosovo itself came to an end. It had affected 124 persons, of whom 26 died.
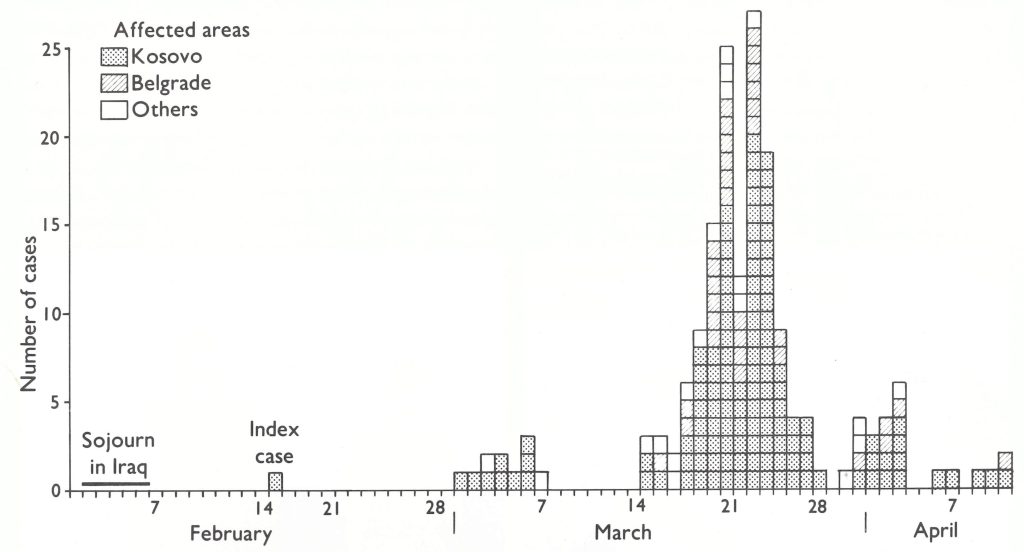
Fig. 23.7. Yugoslavia: number of cases of smallpox, by date of onset and locality, 1972. The first generation of cases occurred in Kosovo province and adjacent areas; the large second generation in Kosovo, Belgrade and some other places.
Spread of the disease outside Kosovo
A tragic and unusual chain of events led to considerable spread outside Kosovo. It started when a 30-year old teacher (Lj. M.), from a village near Novi Pazar, went to Djakovica on 21 February to enrol at the Higher Institute of Education. He came into contact with the index case, became feverish on 3 March after his return and developed a rash on 5 March, when he went to the local medical centre at Novi Pazar and was treated with penicillin. On 7 March he wen: by bus with his brother to the hospital in CaEak. After spending 8 March in the Dermatology and Venereal Diseases ward in catak, he was transferred by ambulance to the Belgrade Dermatology and Venereal Diseases Department on 9 March, because his condition was deteriorating. There he was shown to students and staff as a case demonstrating an unusual drug reaction to penicillin. With the development of severe haemorrhagic complications, the patient was taken, on 10 March, to the Surgical Clinic, where he died during the night. No one in any of the 4 medical establishments through which he had passed had had any suspicion that he might be suffering from smallpox. The brother of the deceased accompanied the body back to Novi Pazar, where it was buried on 12 March. The brother developed a rash on 20 March, and since the Yugoslav medical personnel were by then alerted to the disease, smallpox was diagnosed on 21 March. Only at this point was it realized that Lj. M. had died from haemorrhagic-type smallpox.
Retrospective epidemiological investigation showed that the patient had infected a total of 38 persons, 8 of whom-died; 2 were infected in Novi Pazar, 9 in the Catak hospital (8 patients and a nurse), and 27 in the Belgrade hospitals (20 patients and 7 hospital staff, including 2 physicians and a nurse). In view of the time that had elapsed before the diagnosis was made and of the difficulty of tracing the thousands of contacts of the patient, it was decided to undertake mass vaccination throughout Serbia. A few other cases occurred in additional foci outside Kosovo Province, and 1 case in a Yugoslav migrant worker, who became ill in Hanover, Federal Republic of Germany.
Control measures
On 15 March, a team of epidemiologists and infectious diseases specialists from Belgrade went to Kosovo and joined local health staff in clinical examinations and epidemiological investigations.
The Province of Kosovo, bordering on Albania, was then a rural, relatively undeveloped area, whose Albanian-speaking inhabitants regarded outsiders with suspicion. The population was composed of large extended families, whose members constantly visited one another, and the men frequently travelled long distances to look for work. Most of the epidemiologists carrying out the field investigations had to communicate through an interpreter with a rather uncooperative population, and this caused them some difficulties. The index case, for instance, never admitted to having had a rash and it was some time before circumstantial epidemiological and serological evidence confirmed the diagnosis of smallpox. The reticence of the man concerned was understandable. He belonged to the semi-secret Bektachi religious sect and was most reluctant to have his illness associated with the pilgrimage or to discredit his religion thereby. Indeed, had he been identified as the source of an infection which had killed several members of his village and of surrounding villages, his life might have been in danger.
Vaccination of the population in the initial foci in Kosovo began on 16 March and was extended in concentric rings, until by the end of the month almost all the population in the affected province had been vaccinated. There were problems, however, with coverage and unsuccessful vaccination owing to the use of liquid vaccine. It was not until the end of April that 95% successful coverage was achieved. By the third generation of the outbreak, most cases were occurring among persons who had been unsuccessfully vaccinated.
Containment measures in the 25 localities in villages and towns in which cases of smallpox had been detected included the strict isolation of patients, quarantine of their contacts in facilities specially established in hospitals, hotels, pensions etc., and vaccination of the population. In households in which more than one family member had been infected, their home was turned into a quarantine centre. Where necessary, whole villages were put under surveillance, the inhabitants’ temperatures were taken and the skin of patients was inspected regularly. Population movement to affected areas was restricted and public meetings were prohibited.
In Kosovo, extensive vaccination of hospital staff and the general population was begun as soon as the diagnosis of smallpox had been confirmed, and the same procedure was It is interesting to note that there was an unusually high proportion of haemorrhagic-type cases: 10%, as opposed to the usual 1%. Hospital transmission accounted for 48% of the infections. A high rate of transmission (an average of 12.8 new infections per case) during the second generation of cases was assumed to be associated with inadequate protection from vaccination, 37% of these cases having occurred among previously vaccinated persons. While the number of deaths among previously vaccinated persons was half that among the unvaccinated, the overall case-fatality rate was 20%. The age distribution of cases corresponded with that of the population affected, and the sex ratio was 57%;) males to 43%, females.
The unusual magnitude of the outbreak was considered to be due to the sizeable proportion of susceptible individuals in the population, delayed diagnosis, hospital transmission, the initially large number of unsuccessful revaccinations, communication problems in the tracing of contacts, and an atypical haemorrhagic-type case, which gave rise to the extraordinarily high number of 38 secondary infections.
The spread of smallpox in south-western Asia in 1970-1972 and its importation into Yugoslavia and the Federal Republic of Germany embarrassed several of the countries involved and retarded the progress of the global eradication programme. However, they did help to mobilize support for the programme and to reinforce surveillance efforts in all the countries of south-western Asia.
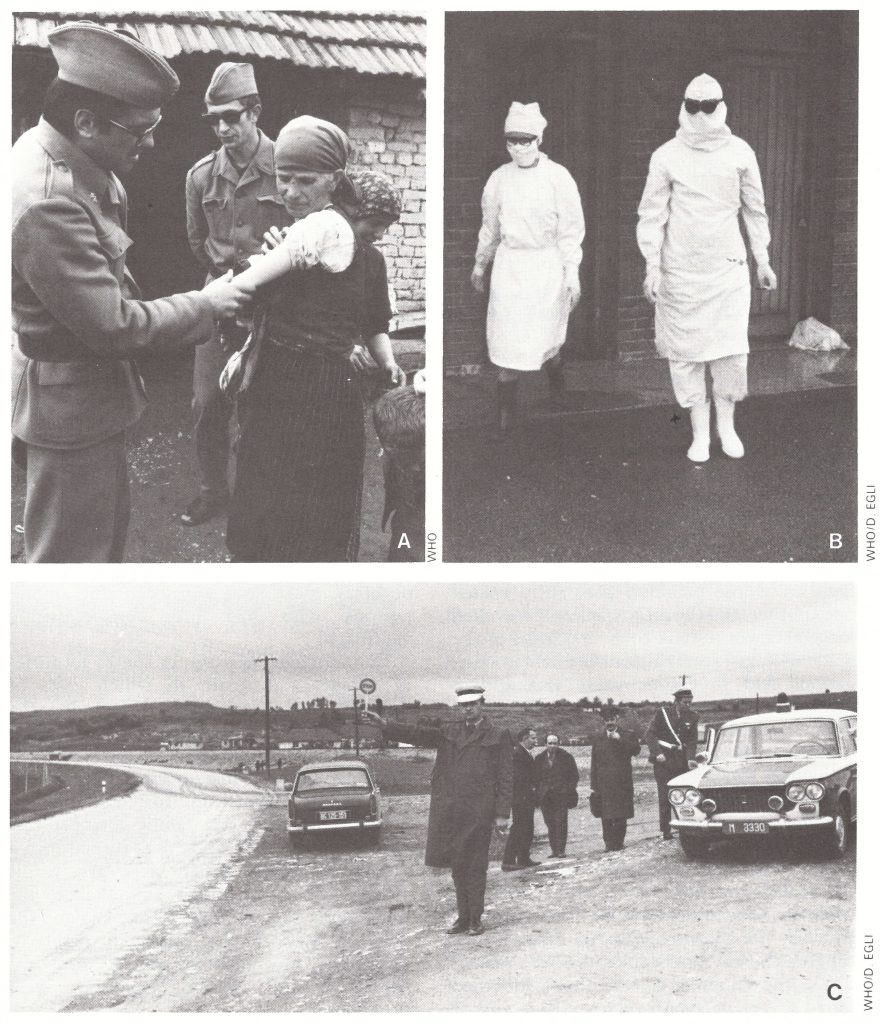
Plate 22.5. Control measures taken during the 1972 outbreak in Yugoslavia. A: More than 300 health teams, some of them army medical units, took part in the vaccination campaign. B: Protective clothing worn by medical personnel in emergency smallpox hospitals. C: Check-points were established a t hundreds of places along the main roads to check vaccination certificates.
LABORATORY -ASSOCIATED OUTBREAKS IN THE UNITED KINGDOM
Microbiological laboratory space inevitably becomes contaminated with the bacteria or viruses in use, the more easily if safety measures are not taken (see Chapter 30). Smallpox laboratories were no exception. However, the regular x7accination and revaccination of persons in any way associated with these laboratories provided good protection against their infection with variola virus.
In countries that still had endemic transmission of smallpox, it was only when cases occurred among laboratory workers that it was possible to ascribe them with any certainty to an infection acquired in a laboratory. Although laboratory-associated outbreaks of smallpox may have occurred in various countries of the Americas, Asia and Europe when the disease was endemic in them, only 3 known laboratory-associated outbreaks and 1 suspected outbreak have been recognized; they all occurred in the United Kingdom after smallpox had ceased to be endemic there (Table 23.11). Only 2 of these were fully documented: one in London (1973), the other in Birmingham (1978). A single-case outbreak in Liverpool, in 1949, involved a laboratory worker who was accidentally infected with variola virus while handling contaminated materials (A. W. Downie, personal communication, 1980). An outbreak of variola minor in the Midlands and Wales in 1966 was later associated with infection acquired from a laboratory. The 2 confirmed outbreaks will be described first.
The London Outbreak, 1973
This outbreak followed the last importation of smallpox into the United Kingdom, which occurred in February 1973, when an Anglo-Indian infected during a holiday in Calcutta became ill after his return to London at the end of February (No. 34, Table 23.2). There were no contact infections.
The laboratory-associated outbreak occurred in March and April 1973, during which another 4 cases of smallpox were reported in the United Kingdom (Cox, 1974). On 11 March 1973 a 23-year-old female laboratory assistant in the Mycological Reference Laboratory at the London School of Hygiene and Tropical Medicine became ill with influenza-like symptoms-headache, backache and high fever. She had been vaccinated as a child and revaccinated in 1972, but did not recall noting any reaction at that time. On 13 March she visited her doctor, who assumed that she had influenza and treated her with oxytetracycline. On 15 March she developed a slight rash and a day later was admitted to St Mary’s Hospital, London, with a provisional diagnosis of glandular fever, and placed in a general ward. A drug rash due to oxytetracycline was suspected and later, because she worked in a mycological laboratory, the possibility of fungal infection was considered.
On 22 March she was visited by a friend working in the mycology laboratory, who, at the request of the head of the laboratory, took scrapings from the patient’s skin lesions, which were investigated the same afternoon. To the surprise of all, brick-shaped poxvirus particles characteristic of variola virus were seen with the electron microscope. An investigation of the patient’s movements before the onset of fever revealed that on 28 February she had entered the poxvirus laboratory (located in the same building as the mycology laboratory) and had watched the chorioallantoic membranes of eggs inoculated with variola virus being harvested on the open bench.
The poxviruses being studied in the laboratory at that time included variola major virus (Harvey strain) and two strains of “whitepox” virus (see Chapter 30). Subsequent investigations showed that it was the Harvey strain of variola virus with which the technician had been infected (Dumbell, 1974).
The patient was taken to Long Reach Isolation Hospital in Dartford, Kent, and the diagnosis of smallpox was confirmed. As many identifiable contacts as possible were traced, vaccinated and placed under surveillance. Unfortunately this group did not include a woman who had occupied the bed next to the laboratory technician’s until 20 March, at St Mary’s Hospital, nor her son and daughter-in-law, who had often visited her in the general ward. On 30 March the 34-yearold son and his 29-year-old wife fell ill with a headache, back pain and nausea. On 2 April their condition deteriorated and they were admitted to an isolation ward of the West Hendon Hospital with a provisional diagnosis of viral gastroenteritis. A skin rash developed on 3 April and became vesicular a day later, when smallpox was suspected and confirmed by laboratory examination. On the 1974). same day both patients were transferred to the Long Reach Isolation Hospital and died, the wife from haemorrhagic-type smallpox and the husband from confluent ordinary-type smallpox.
On 24 April another case, diagnosed as variola sine eruptione, was notified in a nurse, successfully vaccinated on 4 April, who had tended the couple with smallpox in the West Hendon Hospital. A week later, she had fever accompanied by headache, backache and shivering, with a papular rash on her hands. She was transferred to Long Reach, where a diagnosis was made on the basis of the clinical history.
Thus, the “escape” of variola virus from the London poxvirus laboratory resulted in 4 cases, of which 2 were fatal. The British government set up a committee of inquiry, whose report (Cox, 1974) concluded that the technician had probably been infected by the respiratory route while watching the harvesting of chorioallantoic membranes from eggs on 28 February, and that the other 2 patients had been infected on 17 March, when visiting the hospital.
The important feature of the report, in the light of later actions about methods of handling variola virus in laboratories, is the description of the laboratory facilities used at that time. The report noted that the laboratory was of an old-fashioned design, grossly overcrowded and poorly equipped. Work with variola virus was done on an open bench and a deep-freeze for storing variola virus stood in the corridor. But, as Dr K. R. Dumbell of St Mary’s Hospital Medical School testified, the conditions which prevailed there were comparable with those in other teaching hospitals and medical schools in London. Even as recently as 1973, then, scientists working with variola virus did not handle it as a highly dangerous agent but relied on good microbiological techniques and on the regular vaccination of all personnel involved in the laboratories rather than on physical safety facilities. This did not apply to laboratories specially built for handling dangerous microbial pathogens, such as the Microbiological Research Establishment at Porton Down, Wiltshire, in which elaborate physical facilities were provided for the safe handling of dangerous viruses and bacteria. The report concluded with a recommended Code of Practice for Safety in Laboratories Handling Variola Virus (see Chapter 30).
The Birmingham Outbreak, 1978
Ten months after the last case of endemic smallpox in the world had been detected in Somalia in 1977, the British health authorities reported to WHO that on 27 August 1978, a 40-year-old Englishwoman had been confirmed to be suffering from smallpox. The patient, Mrs Janet Parker, a medical photographer in the Anatomy Department of the Medical School of the University of Birmingham, became ill with fever, headache and muscular pains on 11 August and developed a rash on 15 August. This was at first thought to be a drug rash. She remained at her own home until 21 August, when she was transferred to her parents’ house. On 24 August the appearance of vesicles led to a suspicion of smallpox, the patient was admitted to the East Birmingham Hospital and when a diagnosis of smallpox was confirmed by electron microscopy, she was placed in the Catherine-de-Barnes Isolation Hospital. Variola major virus was isolated from vesicle fluid on 27 August. Her condition, complicated by renal involvement, deteriorated rapidly and she died on 11 September. Mrs Parker had last been vaccinated in 1966. She had not travelled abroad in the recent past and to the best of her knowledge had had no contact with any persons recently returned from abroad. Indeed, endemic variola major had not been present anywhere in the world since October 1975. In order to investigate the matter, a Source of Infection Committee composed of 5 experts was established by the University of Birmingham on 28 August 1978. One of the members was Professor Henry S. Bedson, Head of the Department of Medical Microbiology of the Medical School of the University of Birmingham, in which the smallpox laboratory functioned as the regional diagnostic smallpox laboratory. Bedson was an active participant in WHO’S coordinated laboratory investigations of variola and “whitepox” viruses (see Chapter 30). The committee suspected that the smallpox laboratory was the probable source of infection. Meanwhile the health authorities had identified about 290 persons who might have had contact with the patient during her illness. These included the immediate members of her family and other relatives, patients of the East Birmingham Hospital, and colleagues at the Medical School. All were vaccinated and placed under surveillance at home. Four of them were hospitalized with different illnesses, none of which was smallpox. Three were discharged from hospital, while the fourth person—the 77-yearold father of the deceased patient—developed fever on 1 September, 12 days after his daughter had been brought to his house in his car in the vesicular stage of her illness. He did not develop a rash but died suddenly on 5 September from a heart attack. The tragedy was not over. On 2 September the 49-year-old Professor Bedson was found severely ill after an apparent suicide attempt and died 5 days later. On 7 September Mrs Parker’s mother, aged 70, became ill while in quarantine at home and on 8 September developed a sparse macular rash, which was confirmed by laboratory examination as being due to smallpox. She recovered and was discharged from isolation on 22 September.
Table 23.11: Laboratory-associated outbreaks of smallpox in the United Kingdom
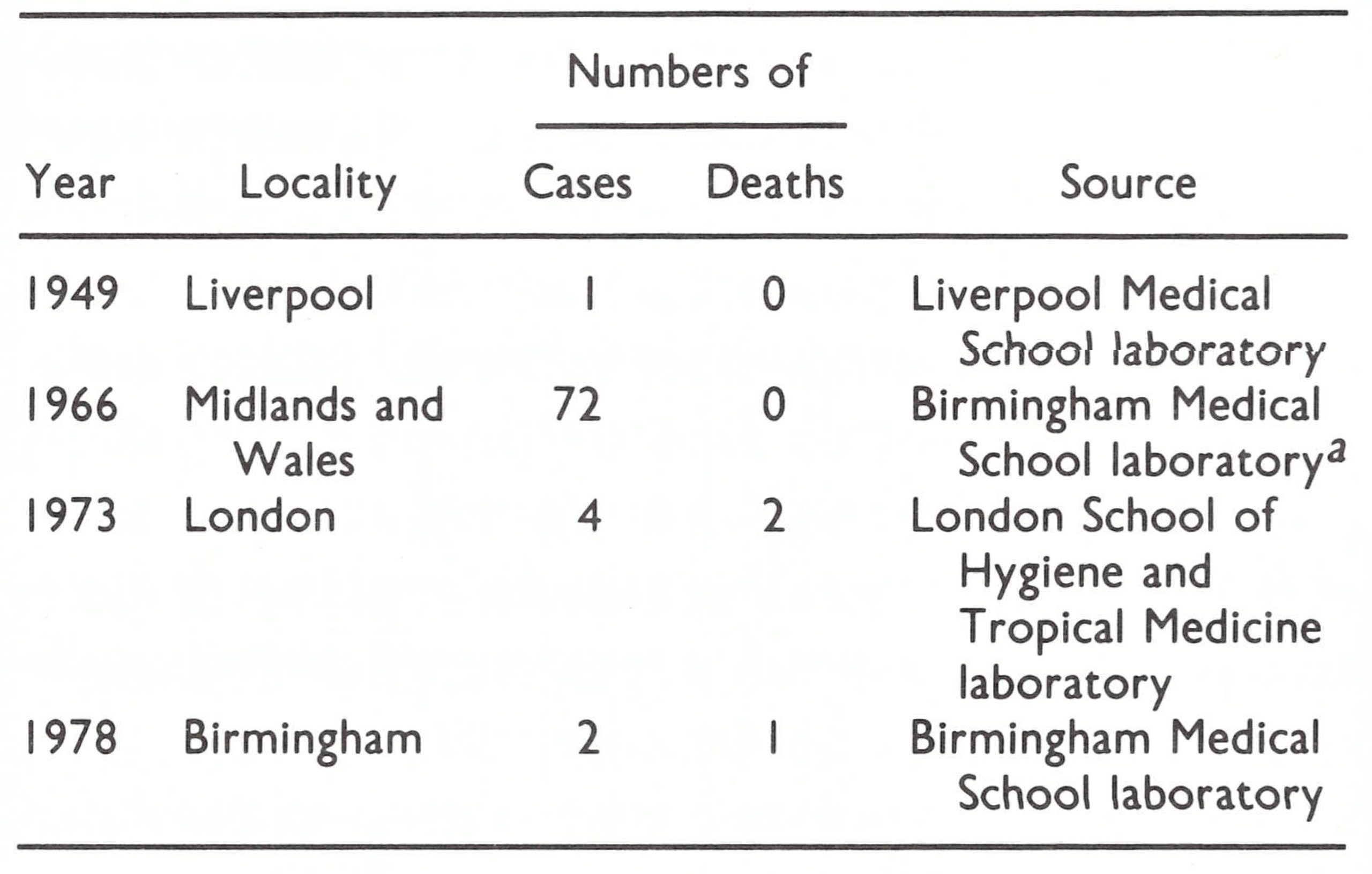 a Suspected.
a Suspected.
In view of the mildness of the illness which the second patient developed, as well as the vigorous surveillance and control measures, a further community-wide spread of smallpox was judged to be very unlikely. Priority vaccination was restricted to contacts, persons who worked or lived in nearby foci and persons who needed vaccination to travel.
On 30 August 1978, the Secretary of State for Social Services requested Professor R. A. Shooter to conduct an official investigation, the results of which were published in July 1980 (Shooter, 1980). Dr Joel Breman, from the WHO Smallpox Eradication unit, participated as an observer in the first 3 meetings of this investigation. As in the episode in London in 1973, the index case was in a person not directly connected with work in the smallpox laboratory. hlrs Parker was a medical photographer who worked in another department of the medical school, though in rooms on the floor immediately above the smallpox laboratory (Plate 23.6).
The team of investigators inspected the premises thoroughly, carried out tests on air movement between the laboratory and the photographer’s room and made exhaustive inquiries to determine whether there might have been personal contact between Mrs Parker and any worker in the virus laboratory during the last week of July.
It concluded that hZrs Parker had been infected with a strain of smallpox virus used in the smallpox laboratory, probably during the last week of July 1978, but how the virus was transferred to hlrs Parker was less certain.
“The evidence points to two possible routes by which smallpox virus was transmitted from the pox laboratory to hfrs. Parker: by the airborne route, either through the duct in the ‘telephone room’ or while visiting the Medical Microbiology corridor; or by the personal contact route, transfer being by the visitor from the Xedical hficrobiology Department who regularly entered the animal pox room. We are unable to say with certainty which of these two routes might have led to hlrs. Parker contracting smallpox. Both are possible though neither seems capable of delivering a large dose of virus unless an accident occurred involving the liberation of virus, which was not recognised or recalled. Kevertheless, from what we know small doses of virus could have been liberated from time to time which could have been responsible for hfrs. Parker’s infection. We believe that the airborne route through the duct to the ‘telephone room’ is the most probable way by which Mrs. Parker was infected because this seems to be the one route that could hare selecti\yely affected her.” (Shooter, 1980.)
This episode constituted the last known outbreak of smallpox in the world, and Mrs Parker’s mother the last known case of smallpox in the world. It is ironic that when cases of variola major had occurred again, they had emanated not from a remote source in Africa or Asia, but from a well-equipped laboratory in one of England’s largest cities. As a consequence of this episode, much attention was paid to the problem of variola virus stocks in laboratories, a matter which actively interested many Member States at the Thirty-second and Thirty-third World Health Assemblies in 1979 and 1980 respectively (see Chapter 30).
Impact of the Birmingham Outbreak
In July 1978 there was a growing belief that the last case of smallpox in the world had occurred in Somalia in October 1977. It was not surprising, therefore, that the Birmingham incident led to a great deal of publicity in the media and caused considerable concern in the medical community throughout the world. Health administrators in the developing countries of Africa, in particular, renewed their calls for the cessation of laboratory studies of variola virus and the destruction of all stocks of the virus.
Because of the publicity, WHO received inquiries from the press and from health administrators in many countries concerning proposals for reducing the risk of another escape of variola virus from a laboratory. Information officers were recruited by the Smallpox Eradication unit to handle the inquiries, and Arita, as chief of the unit, developed plans to deal with the situation. Two meetings were convened: a meeting of experts in February 1979 to evaluate the justification for retaining variola virus stocks in laboratories, and a conference in April with the directors of 9 laboratories which were then retaining the virus, together with representatives of the governments concerned, to discuss control measures and future actions.
The plans were debated at a special open meeting held during the sixty-third session of the Executive Board in January 1979, which was attended by a large number of journalists, and the meetings took place as scheduled. Thus, the Birmingham laboratory-associated outbreak, though an unfortunate incident, hastened a recognition of the risk of holding variola virus stocks and led to an immediate reduction in the number of laboratories retaining the virus, from 13 in 1978 to 7 in 1979 (see Chapter 30, Table 30.7).
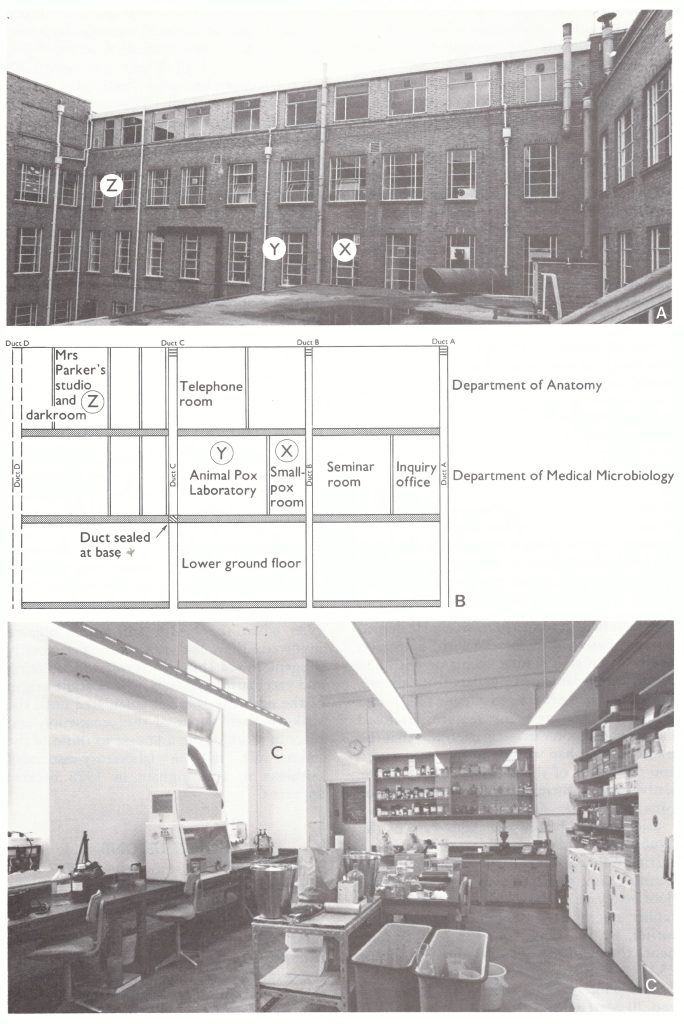
Plate 22.6. Departments of Anatomy and Medical Microbiology at the Medical School, University of Birmingham. A: From the east courtyard. X = smallpox room; Y = animal poxvirus laboratory; Z = photographic studio. B: Diagram showing location of these rooms and the service ducts running through them. C: Photograph of the animal pox laboratory looking towards duct C, which is marked by the letter C. (From Shooter, 1980, with permission from the Controller of Her Majesty’s Stationery Office, United Kingdom.)
Outbreak of Variola Minor in the Midlands and Wales, 1966
During the official inquiry into the Birmingham outbreak, the similarity of the apparent origin of an outbreak of variola minor in England and Wales in 1966 was brought to the attention of the team of investigators. The first case in this earlier outbreak to be identified and reported to WHO, on 2 May 1966, was in an unvaccinated 17-year-old girl who had developed an influenza-like illness on 16 April. Four days later a rash appeared, and she was admitted on 25 April to the Moxley lnfectious Diseases Hospital, Walsall, Lancashire, as a case of chickenpox. Four days after that, smallpox was suspected and the girl was admitted to a smallpox hospital on 29 April. The diagnosis was confirmed by the isolation of variola minor virus.
Investigation of the girl’s family and associates led to the discovery of an additional 71 cases of variola minor in the Midlands and Wales between February and August 1966. Detailed inquiries held in 1966 had failed to establish the source of infection. However, 12 years later, the team of investigators headed by Professor R. A. Shooter carried out a retrospective examination of all available reports and correspondence concerning the 1966 outbreak (Shooter, 1980). The earliest case identified was in an unvaccinated 23- year-old photographer employed at the Medical School of the University of Birmingham. He had become ill on 18 February with fever, headache and backache and had developed a generalized rash 4 days later. During the first week of illness he had remained at home and when the rash had appeared he had returned to work. He denied having had any contact with a person exhibiting a rash similar to his or with any recent immigrants or travellers from abroad. He himself had never been outside the United Kingdom. The relevant feature disclosed during the Shooter investigation was that the photographer had worked in the same studio and darkroom of the Medical School of the University of Birmingham as those used by Mrs Parker. Eleven days before the index case of the 1966 outbreak became ill, work was being carried out with variola minor virus in the Birmingham smallpox laboratory, on the floor below (see Plate 23.6). Thus the photographer might have been infected, 12 years earlier, by the same route as Mrs Parker; hence the inclusion of this outbreak in Table 23.11 as “suspected” laboratory-associated.
The photographer became ill between 4 and 20 March 1966 ; his fiancke, his parents and a schoolteacher were infected at a folkdance evening, and a 72-year-old man during a visit to a public house. These secondary cases gave rise to 2 main chains of transmission. The first spread from the photographer’s fiancke to members of a youth club in her town and from them to their families and associates. The other chain stemmed from the 72-year old man, who infected 2 of his grandchildren, who in turn infected their friends and families. The spread continued, and at least 25 persons had been infected before 29 April, when the diagnosis of smallpox was made in the 17-year-old girl mentioned earlier. By June, 47 smallpox cases had been reported in the heavily populated West Midlands. Subsequently, new foci of infection appeared in Wales and Lancashire, although no connection could be established between these outbreaks and those in the Midlands, probably because of missed cases wrongly diagnosed as chickenpox.
The last known case occurred in Salford, Lancashire, with onset on 9 July 1966. The patient concerned was discharged from the isolation hospital on 1 August, but in compliance with the International Sanitary Regulations England and Wales were not declared free of smallpox until 18 August of that year. The reaction of the public and the health authorities to this outbreak differed greatly from the response, described earlier, to importations of variola major into European countries. Many cases in the 1966 outbreak had been misdiagnosed as chickenpox, and even when the health authorities became involved, they had not been particularly diligent in searching for cases and isolating and vaccinating contacts. The possible origin of the outbreak was not elucidated until the striking resemblance of the occupation and place of work of the first case to those of the index case in the laboratory-associated outbreak in Birmingham in 1978 became apparent.
CONCLUSIONS
Smallpox importations into European countries emphasized the risk of infection to which professional staff and patients in hospitals and other medical institutions were exposed. Over half of all cases associated with importations were found in this group, whose protection by regular vaccination with potent vaccine could have reduced the number of cases very substantially. Nevertheless, the majority of the outbreaks were effectively controlled by surveillance and containment, and smallpox importations caused few disastrous events in Europe.
The review of importations into southwestern Asia, especially the epidemic in 1970-1972 that spread from Afghanistan into Iran, Iraq and the Syrian Arab Republic and eventually into Europe, demonstrates that poor surveillance, and especially the deliberate suppression of reports of the disease, had extremely serious consequences both for the countries concerned and for their neighbours.
For most of the period after 1950, the Indian subcontinent was the major source from which smallpox was occasionally transferred to the countries of Europe, especially the United Kingdom and the Federal Republic of Germany, and to non-endemic countries in Asia. The majority of importations into Europe were due to Europeans returning home after travelling in the Indian subcontinent. In spite of the large volume of air traffic between the Indian subcontinent and the USA during this period, there were no importations into the latter country, possibly because of the better vaccination status and stricter enforcement of health regulations in the USA than in Europe.
As countries in Africa and South America became free of smallpox, they experienced importations mainly from one country in each of these continents with a large population and extensive endemic foci, which became the major exporter of smallpox to its neighbours—namely, Ethiopia in Africa and Brazil in South America.
The number of diagnosed laboratoryassociated outbreaks was remarkably small, probably because of the high level of vaccination among laboratory staff. However, the last tragic incident in Birmingham emphasized the need for close supervision of variola virus stocks during the period following eradication.
Robertbor
July 3, 2025Хотите собрать данные о человеке ? Этот бот предоставит полный профиль в режиме реального времени . Используйте продвинутые инструменты для анализа публичных записей в открытых источниках. Узнайте место работы или интересы через систему мониторинга с верификацией результатов. настоящий глаз бога Система функционирует в рамках закона , используя только открытые данные . Получите детализированную выжимку с историей аккаунтов и списком связей. Доверьтесь проверенному решению для digital-расследований — результаты вас удивят !
KennethLobre
July 5, 2025Выгребная яма — это подземная ёмкость , предназначенная для первичной обработки сточных вод . Принцип действия заключается в том, что жидкость из дома поступает в бак , где твердые частицы оседают , а жиры и масла собираются в верхнем слое. В конструкцию входят входная труба, герметичный бак , соединительный канал и почвенный фильтр для доочистки стоков. https://sklad-slabov.ru/forum/user/22171/ Плюсы использования: низкие затраты , долговечность и экологичность при соблюдении норм. Однако важно не перегружать систему , иначе частично очищенная вода попадут в грунт, вызывая загрязнение. Материалы изготовления: бетонные блоки, полиэтиленовые резервуары и композитные баки для индивидуальных нужд.
Jaimenip
July 12, 2025Доставка грузов из Китая в Россию проводится через железнодорожные каналы, с проверкой документов на в портах назначения. Таможенные пошлины составляют в диапазоне 15–20%, в зависимости от типа продукции — например, сельхозпродукты облагаются по максимальной ставке. Чтобы сократить сроки используют серые каналы доставки , которые быстрее стандартных методов , но связаны с дополнительными затратами. Доставка грузов из Китая При официальном оформлении требуется предоставить паспорта на товар и акты инспекции, особенно для сложных грузов . Сроки доставки варьируются от одной недели до двух недель , в зависимости от удалённости пункта назначения и эффективности таможни . Стоимость услуг включает транспортные расходы, налоги и комиссии за оформление , что влияет на рентабельность поставок.
JerryOxirm
July 12, 2025Back then, I believed following instructions was enough. Doctors give you pills — you nod, take it, and move on. It felt official. But that illusion broke slowly. First came the fatigue. I blamed stress. And deep down, I knew something was off. I read the label. No one had warned me about interactions. suhagra I started seeing: one dose doesn’t fit all. Two people can take the same pill and walk away with different futures. Damage accumulates. Still we trust too easily. Now I question more. Not because I don’t trust science. I take health personally now. But I don’t care. This is survival, not stubbornness. The lesson that stuck most, it would be keyword.
DuaneWiz
July 12, 2025Данный портал предлагает актуальные новостные материалы со всего мира. Здесь можно найти события из жизни, технологиях и разных направлениях. Контент пополняется ежедневно, что позволяет всегда быть в курсе. Понятная навигация облегчает восприятие. https://egomoda.ru Каждая статья оформлены качественно. Редакция придерживается информативности. Оставайтесь с нами, чтобы быть в курсе самых главных событий.
KevinLer
July 14, 2025Хотите найти данные о пользователе? Наш сервис предоставит полный профиль мгновенно. Используйте продвинутые инструменты для анализа публичных записей в соцсетях . Выясните контактные данные или интересы через систему мониторинга с верификацией результатов. глаз бога телега Бот работает в рамках закона , обрабатывая общедоступную информацию. Получите расширенный отчет с историей аккаунтов и графиками активности . Попробуйте проверенному решению для исследований — результаты вас удивят !
rolex-submariner-shop.ru
July 14, 2025Модель Submariner от выпущенная в 1954 году стала первыми водонепроницаемыми часами , выдерживающими глубину до 100 метров . Модель имеет 60-минутную шкалу, Triplock-заводную головку, обеспечивающие герметичность даже в экстремальных условиях. Конструкция включает хромалитовый циферблат , черный керамический безель , подчеркивающие функциональность . Хронометры Rolex Submariner отзывы Механизм с запасом хода до 3 суток сочетается с перманентной работой, что делает их идеальным выбором для активного образа жизни. За десятилетия Submariner стал символом часового искусства, оцениваемым как коллекционеры .
Harlanzes
July 19, 2025La montre connectée Garmin fēnix® Chronos représente un summum de luxe avec un design élégant et capteurs multisports. Adaptée aux activités variées, elle propose une polyvalence et durabilité extrême, idéale pour les aventures en extérieur grâce à ses outils de navigation . Grâce à son autonomie allant jusqu’à plusieurs jours selon l’usage, cette montre reste opérationnelle dans des conditions extrêmes, même lors de activités exigeantes. garmin venu Les outils de suivi incluent la fréquence cardiaque en temps réel , accompagnées de conseils d’entraînement personnalisés, pour les amateurs de fitness . Facile à personnaliser , elle s’intègre à votre quotidien , avec une interface tactile réactive et compatibilité avec les apps mobiles .
DavidHam
July 20, 2025Эта платформа размещает интересные новостные материалы в одном месте. Здесь доступны события из жизни, бизнесе и других областях. Информация обновляется регулярно, что позволяет всегда быть в курсе. Минималистичный дизайн ускоряет поиск. https://ladiesblog.ru Каждое сообщение оформлены качественно. Мы стремимся к честной подачи. Следите за обновлениями, чтобы быть в центре внимания.
JosephForia
July 23, 2025Responsible gaming involves implementing measures to minimize risks, including age verification and encouraging mindful participation. Setting clear boundaries for money wagered helps avoid excessive losses, while tools like self-exclusion options empower informed decisions . Training staff ensures early identification of problematic behavior , fostering a supportive environment . betpawa phone number Offering resources such as counseling services and self-assessment tools enables players to seek help effectively. Adhering to regulations like ID checks and fair gameplay policies builds trust within the community. Aim to build a balanced ecosystem where entertainment coexists with financial prudence , ensuring sustainable play.
Walterlof
August 1, 2025Татуировки — это уникальное искусство , где каждая линия несёт глубокий смысл и отражает характер человека. Для многих тату — вечный символ , который напоминает о преодолённых трудностях и дополняет жизненный опыт. Сам акт нанесения — это ритуал доверия между мастером и клиентом , где тело становится живым холстом . запчасти для машинок Разные направления, от акварельных рисунков до традиционных орнаментов , позволяют воплотить любую идею в изысканной форме . Эстетика нательного искусства в способности расти вместе с человеком, превращая эмоции в живой символ внутреннего мира. Выбирая узор , люди раскрывают душу через формы, создавая личное произведение, которое радует глаз каждый день.
DavidHam
August 2, 2025Данный портал собирает интересные новостные материалы на любые темы. Здесь доступны новости о политике, науке и многом другом. Контент пополняется регулярно, что позволяет всегда быть в курсе. Удобная структура делает использование комфортным. https://modavgorode.ru Каждое сообщение проходят проверку. Целью сайта является честной подачи. Оставайтесь с нами, чтобы быть всегда информированными.
RichardJof
August 4, 2025This iconic Rainbow Daytona showcases high-end craftsmanship with its colorful ceramic chapter ring. Featuring 18k white gold , it blends precision timing features with dazzling visual appeal . Available in exclusive editions , this timepiece attracts discerning collectors worldwide. Rolex Cosmograph Daytona Rainbow videos The meticulously set gems on the bezel creates a spectrum that catches the light . Powered by Rolex’s precision-engineered automatic mechanism, it ensures reliable performance for enduring legacy. An investment piece, the Daytona Rainbow reflects Swiss watchmaking heritage in its entirety .
Thomasunums
August 12, 2025Les devices Garmin intègrent des outils performantes en fitness . Avec écran AMOLED ainsi que de analyse de stress, ces montres s’adaptent à tous niveaux. L’autonomie peut aller jusqu’à une longue durée en utilisation normale , adaptée aux activités intenses . livraison rapide depuis Paris Les métriques analysent les étapes et aussi les calories, offrant global . Simples en personnaliser, elles s’intègrent facilement dans votre vie, avec une interface ergonomique. Opter pour Garmin garantit accéder à une technologie fiable pour améliorer votre quotidien.
Ernestbindy
August 14, 2025Sorumlulukla casino oynamak , riskleri azaltır. Oyun bütçenizi dikkatli planlamak, sorunları önlemeye yardımcı olur . Katılımınızı hariç tutma araçlarını kullanmak, riskleri minimize etmenize katkıda bulunur. Alev Online Casino Bahislerin risklerinin farkında olmak, uzun süreli keyif temin eder . İhtiyaç halinde profesyonel destek danışmak, keyfi artırmaya yardımcı olur. Bu önlemler, sorunsuz keyifli bahis süreci keyfini maksimize eder.
Ernestbindy
August 17, 2025Bilinçli kumar oynamak , deneyiminizi güvenceye alır . Oyun bütçenizi dikkatli planlamak, sorunları önlemeye katkı sağlar . Kendinizi hariç tutma araçlarını kullanmak, sorunları engellemenize destek olur . Alev Casino TR Kumarın etkilerinin farkında olmak, dengeli katılım mümkün kılar. Zorlandığınızda yardım grubu başvurmak, dengeyi çözmeye yardımcı olur . Bu önlemler, sorunsuz keyifli casino katılımı deneyimi zenginleştirir .
RobertTeels
August 22, 2025Goods delivery from China is dependable and swift. Our company provides custom solutions for enterprises of any capacity. We handle all shipping processes to make your operations uninterrupted. air delivery china With scheduled shipments, we ensure timely delivery of your orders. Clients trust our skilled team and affordable rates. Choosing us means certainty in every shipment.
RobertTeels
August 24, 2025Goods delivery from China is reliable and efficient. Our company provides custom solutions for enterprises of any size. We take care of all transportation processes to make your workflow smooth. air express shipping from china With scheduled shipments, we guarantee timely delivery of your packages. Clients trust our professional team and competitive rates. Choosing us means confidence in every delivery.
Kevinsar
August 25, 2025Современные системы отслеживания рабочего времени способствуют улучшению эффективности . Точность фиксации минимизирует неточности в отчётности . Руководителям легче контролировать проектные задачи с детализацией. https://pennavenuearts.org/finance/how-to-predict-employee-burnout/ Персонал получают прозрачный доступ для отслеживания . Использование цифровых решений значительно ускоряет внутренние операции без лишних затрат . Это гарантирует доверие между отделами , повышая лояльность сотрудников.
RobertTeels
August 27, 2025Goods delivery from China is reliable and efficient. Our company offers tailored solutions for enterprises of any capacity. We manage all transportation processes to make your operations seamless. air freight cost from china With direct shipments, we guarantee timely delivery of your packages. Clients trust our skilled team and competitive rates. Choosing us means confidence in every delivery.
Carlosteado
August 29, 2025В мессенджере Telegram появилась новая функция — внутренние звёзды. Они служат для мотивации создателей. Любой пользователь может отправлять звёзды чатам. купить звезды телкграм дешево Звёзды конвертируются в реальные деньги. Это удобный способ выразить благодарность. Оцените опцию уже немедленно.
EdgarGlink
August 29, 2025В приложении Telegram появилась функция звезд. Теперь люди могут помечать важные сообщения. Это позволяет быстро открывать нужную заметку. звезды купить Функция комфортна для деловых задач. С её помощью легко зафиксировать ключевые фразы. Такой инструмент сохраняет ресурсы и делает общение эффективнее.
EdgarGlink
August 31, 2025В приложении Telegram появилась функция звёзд. Теперь пользователи могут помечать важные месседжи. Это помогает быстро открывать нужную заметку. как купить звезды в россии Функция комфортна для деловых задач. Благодаря этому легко оставить ключевые заметки. Такой инструмент экономит ресурсы и делает общение эффективнее.
CharlesThert
September 2, 2025On our website you can discover a lot of valuable information. It is made to support you with different topics. You will find simple explanations and real examples. The content is frequently improved to stay relevant. https://indianastars.us It’s a great resource for learning. Every visitor can take advantage of the materials here. Start reading the site today.
EdgarGlink
September 2, 2025В Telegram появилась функция звёзд. Теперь пользователи могут выделять важные месседжи. Это помогает быстро открывать нужную переписку. можно ли купить звезды телеграмм Функция полезна для деловых задач. Благодаря этому легко оставить ключевые моменты. Такой инструмент бережёт ресурсы и делает общение эффективнее.
Davidram
September 4, 2025Crash mechanics games are online games with a interactive experience. They include a rising multiplier that players can track in real time. The goal is to act before the bar crashes. best csgo crash site Such games are popular for their simplicity and intensity. They are often used to improve reaction speed. Plenty of platforms host crash games with different designs and features. You can check out these games now for a fun experience.
Patrickfarve
September 10, 2025Заказ автозапчастей онлайн становится всё более востребованной среди водителей. Онлайн-платформы предлагают широкий выбор комплектующих для любых моделей автомобилей. Стоимость в сайтах часто доступнее, чем в обычных магазинах. Покупатели могут анализировать предложения разных поставщиков без лишних затрат времени. Запчасти для грузовиков Кроме того, простая система отправки позволяет забрать заказ без задержек. Комментарии других пользователей дают возможность выбрать подходящие автозапчасти. Многие сервисы дают защиту на товары, что усиливает доверие покупателей. Таким образом, покупка через интернет автозапчастей экономит время и деньги.
Daviddig
September 11, 2025This website contains a large amount of helpful insights about male and female intimate life. Visitors can discover different subjects that support them enhance their connections. Articles on the site describe positive dialogue between people. You will also come across advice on building shared trust. Content here is created by experts in the field of personal well-being. https://ra-be.info/love/the-evolution-of-amateur-porn-in-the-digital-era/ Many of the articles are clear and practical and beneficial for daily life. Visitors can adapt this knowledge to improve their connections. In short, this resource provides a comprehensive collection of trusted information about intimate topics for all adults.
Jamespycle
September 12, 2025Il gioco equilibrato nell’i-gaming consiste nel fare decisioni attente mentre ci si intrattiene alle piattaforme interattive. Esso sostiene abitudini sani e aiuta i partecipanti a stabilire limiti chiari. Principi del gioco responsabile comprendono il gestire tempo e spese in modo sensato. I giocatori sono invitati a mantenere un approccio positivo e a osservare il proprio comportamento. Contenuti informativi sul gioco responsabile guidano le persone a capire i propri abitudini. plinko gratis demo Molte servizi offrono strumenti e opzioni per monitoraggio. Praticare il gioco responsabile permette a tutti di apprezzare l’i-gaming in modo consapevole. In sintesi, il gioco responsabile nell’i-gaming riguarda la autocontrollo e il seguire azioni che favoriscono il proprio benessere.
bokep
September 19, 2025Hi it's me, I am also visiting this website on a regular basis, this web page is truly good and the people are really sharing fastidious thoughts.
AlvinKah
September 23, 2025Приобретение профессиональной техники — серьёзный этап в развитии красоты. Для начала стоит понять цели и процедуры, которые вы планируете оказывать. Необходимо оценить сертификаты и производителя выбранного оборудования. Комментарии прошлых пользователей помогут сделать осознанный подбор. beautyinstrument.ru Также нужно обратить внимание на функциональность и эргономику работы. Начальная демонстрация оборудования помогает понять эффективность работы. Стоит также проанализировать стоимость и поддержку производителя. Правильный выбор техники поможет усилить качество процедур.
AlvinKah
September 28, 2025Приобретение косметологического оборудования — ответственный шаг в развитии салона. Прежде всего стоит уточнить задачи и услуги, которые собираетесь проводить. Необходимо оценить разрешения и надёжность выбранного аппарата. Комментарии опытных клиентов помогут принять уверенный подбор. Бьюти Инструмент Также нужно обратить внимание на функциональность и простоту работы. Тестовая демонстрация оборудования позволяет понять комфорт работы. Важно проанализировать стоимость и сервисное обслуживание. Правильный выбор аппарата позволит улучшить качество процедур.
RogerDuets
September 29, 2025Самостоятельные девушки — это выразительные личности, которые берегут свою автономию. Они выбирают к вдумчивому подходу в взаимодействии. Такие девушки повсеместно обладают сильным характером и четкими жизненными целями. Они не стесняются показывать свои позиции. https://donetsk.spaxam.net/ Общение с ними обычно получается насыщенным. Они умеют воспринимать собеседника и строить честные отношения. Такие девушки мотивируют окружающих своей естественностью. Они следуют своим курсом, не подстраиваясь под навязанные ожидания.
RogerDuets
September 30, 2025Независимые девушки — это неповторимые личности, которые берегут свою автономию. Они предпочитают к вдумчивому подходу в общении. Такие девушки повсеместно обладают уверенным характером и четкими жизненными установками. Они открыто артикулировать свои взгляды. https://lugansk.spaxam.net/ Разговор с ними всегда получается осмысленным. Они способны понимать собеседника и создавать честные отношения. Такие девушки мотивируют окружающих своей подлинностью. Они стремятся своим курсом, не подстраиваясь под навязанные ожидания.
MichaelSpisa
October 3, 2025Современное медоборудование играет ключевую часть в диагностике и поддержке пациентов. Больницы всё чаще используют инновационную аппаратуру. Это обеспечивает врачам ставить точные заключения. Новые приборы гарантируют комфорт и для пациентов, и для медиков. http://www.tombru.com/mushing/index.php?topic=1681.new#new Внедрение высоких технологий помогает качественное восстановление. Многие устройства имеют функции для точного контроля состояния здоровья. Врачи могут своевременно реагировать, основываясь на показателях аппаратуры. Таким образом, инновационное медицинское оборудование повышает эффективность здравоохранения.
LeonardMoG
October 8, 2025Creative photography often focuses on expressing the beauty of the body lines. It is about light rather than surface. Experienced photographers use natural tones to create emotion. Such images emphasize artistry and personality. https://xnudes.ai/ Each photo aims to tell a story through movement. The goal is to show inner grace in an respectful way. Viewers often value such work for its emotional power. This style of photography unites art and aesthetics into something truly expressive.
Michaeltut
October 24, 2025Нейросетевые поисковые системы для мониторинга источников становятся всё более популярными. Они позволяют собирать публичные данные из социальных сетей. Такие боты используются для аналитики. Они умеют оперативно систематизировать большие объёмы данных. глаз бога официальный телеграм Это способствует получить более полную картину событий. Некоторые системы также включают функции визуализации. Такие платформы активно применяются среди исследователей. Эволюция технологий превращает поиск информации более точным и удобным.
Michaeltut
October 30, 2025Современные боты для анализа данных становятся всё более удобными. Они помогают собирать доступные данные из интернета. Такие решения подходят для журналистики. Они могут оперативно анализировать большие объёмы информации. глаз бога телеграмм официальный Это помогает создать более полную картину событий. Отдельные системы также включают инструменты фильтрации. Такие сервисы широко используются среди аналитиков. Эволюция технологий позволяет сделать поиск информации более точным и наглядным.
Дизельное топливо
November 1, 2025Дизельное топливо — это важный компонент энергетики, который нашёл применение в промышленности. Посредством своей плотности энергии дизельное топливо гарантирует надёжную эксплуатацию двигателей. Соответствующее стандартам топливо способствует бесперебойность работоспособности систем. Существенное влияние имеет химический баланс топлива, ведь низкосортные добавки могут негативно повлиять. Поставщики дизельного топлива стараются соблюдать нормы безопасности. Новые методы позволяют улучшать его характеристики. При выборе дизельного топлива важно проверять поставщика. Доставка и содержание топлива также определяют на его свойства. Низкосортное ДТ может привести к увеличению расхода. Поэтому использование проверенных поставщиков — необходимое условие. В настоящее время представлено множество вариантов дизельного топлива, отличающихся по назначению. Морозостойкие виды дизельного топлива позволяют эксплуатацию двигателей даже при экстремальных условиях. Благодаря развитию новых технологий качество топлива улучшается. Ответственный подход в вопросе использования дизельного топлива помогают повышение производительности. Таким образом, надёжный источник энергии является основой эффективной работы любого транспортного средства.
NathanLauby
November 10, 2025The site provides a lot of engaging and informative information. Here, you can learn about different articles that help you learn new things. Readers will value the content shared here. Every category is well-structured, making it simple to use. The materials are easy to understand. You can find recommendations on various fields. Whether you’re looking for inspiration, this site has everything you need. Overall, this resource is a reliable place for curious minds. https://rublevo.info/
Floydcop
November 11, 2025This website features a lot of captivating and useful information. On the website, you can discover a wide range of subjects that provide insights. Visitors will benefit from the resources shared on this site. Every page is well-structured, making it comfortable to use. The materials are easy to understand. The site includes recommendations on numerous themes. Whether you’re looking for educational content, this site has something for everyone. To sum up, this site is a valuable hub for those who love learning. https://borny.info/
Floydcop
November 12, 2025This online platform features a lot of engaging and valuable information. On this platform, you can find many topics that provide insights. Users will appreciate the information shared through this platform. Each section is easy to navigate, making it comfortable to use. The content are written clearly. It’s possible to find information on numerous themes. If you want to find useful facts, this site has everything you need. All in all, this site is a reliable place for curious minds. https://xevanio.de/
AustralianGameShowsObeld
November 19, 2025Word games identifying famous faces from clues, price guessing competitions for consumer goods, celebrity panel shows testing knowledge - experience experimental formats from Australian television's creative era. https://australiangameshows.top/
GratiaVitaeObeld
November 21, 2025Обучение без стресса — как выбрать формат, который подходит именно вам https://gratiavitae.ru/
PerplexityKupitObeld
November 22, 2025perplexity max купить подписку https://uniqueartworks.ru/perplexity-kupit.html
MetabolicFreedomObeld
November 25, 2025Reconnect with your body's wisdom and unlock metabolic health through practical daily actions. https://metabolicfreedom.top/ metabolic freedom book free download
WallyRam
November 28, 2025Своевременное выполнение уроков играет значимую роль в обучении школьников. Оно помогает закреплять материал и повышать успеваемость. Большинство школьников осознают, что внеурочные упражнения формируют самостоятельность. Регулярная практика позволяет повысить концентрацию. https://aforisimo.ru/uchoba/32471.html Преподаватели нередко говорят, что домашняя подготовка помогает глубже понимать темы. Кроме того, домашняя работа формирует организованность. Школьники, которые делают уроки, обычно добиваются лучших результатов. Таким образом, выполнение домашних заданий остаётся ключевым фактором успеха для любого ученика.
kuhni-v-ivanovo.ru
December 3, 2025Национальные награды занимают значимое место в жизни общества. Они подчёркивают вклад людей, которые проявили себя в развитие страны. Подобные отличия помогают усиливать уважение гражданского подвига. Кроме того, они вдохновляют людей на повышение личных результатов. изготовление наград Официальное признание нередко повышает уважение к человеку в профессиональной среде. Необходимо осознавать, что награждение — это больше, чем символ, а выражение благодарности. Она отражает важность усилий, который был проделан человеком. В итоге, государственные награды остаются ключевым инструментом поощрения в государственной системе.
TimothyGligh
December 7, 2025Envision the intricate web of well-being, where experts frequently spot a pattern of sticking to everyday routines without much thought. It unfolds like a well-rehearsed story: detect an imbalance in your system, adhere to standard recommendations, and cross your fingers for restoration. This structure subtly assures us of an uncomplicated path forward. Consider vitality as a beautifully crafted puzzle, with every element distinct and irreplaceable. People often report subtle signals of discomfort that don't fit neatly into standard explanations. A broad range of experiences unfolds, some invigorating and empowering, while others provoke deeper contemplation. Immersing yourself in the practice of tuning into your body's whispers and signals. frequently brings to light overlooked synergies and natural rhythms. This profound realization ignites a fresh era in comprehensive health awareness. Even when two journeys appear similar on the surface, their outcomes can diverge in remarkable and unexpected ways. It forms a vibrant, ever-unfolding fabric rich with purpose. Opening yourself to new potentials isn't just beneficial—it's a gateway to profound freedom. We motivate those on the path to become collaborative storytellers in their own tales of vitality. Strengthen your foundation with rich veins of knowledge and perspective. Ready to expand your horizons on this vital topic? Click through for more on cenforce 200 sildenafil
NathanLauby
December 8, 2025На этом сайте представлено много ценной информации. Пользователи отмечают, что ресурс удобен для поиска информации. Контент постоянно пополняется, что делает сайт удобным для изучения. Многие считают, что структура сайта хорошо продумана и позволяет сэкономить время. Широкий выбор материалов делает ресурс интересным для разных категорий пользователей. Также отмечается, что материалы оформлены аккуратно и понятны даже новичкам. Сайт помогает получать новые сведения благодаря подробным статьям. Таким образом, этот ресурс можно назвать удобным местом для изучения важных тем для каждого посетителя. https://icolog.ru
LasMujeresPDFObeld
December 8, 2025¿Temes que si pones límites te dejará? Lee esto urgentemente https://lasmujeresqueamandemasiadopdf.cyou/ las mujeres que aman demasiado pdf descargar
общество экспертов России по недропользованию
January 7, 2026Сфера недропользования — это комплекс работ, связанный с разработкой подземных богатств. Оно включает поиск минерального сырья и их дальнейшую переработку. Эта отрасль регулируется установленными правилами, направленными на охрану окружающей среды. Ответственное ведение работ в недропользовании способствует экономическому росту. оэрн
Бейт-Шемеш mdash; работа на военной базе
January 24, 2026This is a very good tip especially to those fresh to the blogosphere. Short but very precise info… Thanks for sharing this one. A must read article!
twistedlovepdfObeld
February 3, 2026If you love a hero who grovels when he messes up, you will appreciate the ending of this book. Alex has to earn Ava back. The Twisted Love PDF is often sought after for this specific sequence. The redemption arc is well-handled. It is a story that satisfies the desire for justice and love in equal measure. https://twistedlovepdf.site/ Twisted Love Read Pdf Online
twistedlovepdfObeld
February 3, 2026Ultimately, Twisted Love is about two people finding their missing piece. It is a satisfying, complete narrative. The Twisted Love PDF is your ticket to this emotional fulfillment. The story of Alex and Ava is a testament to the enduring power of the romance genre. It is a book that will make you believe in love. https://twistedlovepdf.site/ Ex A Twisted Love Story Epub Free Download
twistedlovepdfObeld
February 3, 2026The raw emotion in the scenes where Alex opens up to Ava is palpable. It is a breakthrough moment for his character. Readers often highlight these parts in the Twisted Love PDF. The book is about the bravery it takes to show your true self to another person. It is a beautiful, moving story of vulnerability. https://twistedlovepdf.site/ Twisted Love Pdf Free
twistedlovepdfObeld
February 4, 2026The "sunshine and the grump" dynamic is taken to the extreme in this popular novel. Alex is cold, dismissing emotions as a weakness, while Ava embraces the beauty of the world around her. If you are curious about the hype, finding a Twisted Love PDF can introduce you to this addictive universe. The book does not shy away from the uglier sides of their personalities, making the characters feel real and flawed. Their journey toward a happily ever after is fraught with obstacles, but that only makes the destination more satisfying. It is a modern classic in the New Adult genre for a very good reason. https://twistedlovepdf.site/ Twisted Love Epub Free
Twisted Love Pdf En Español Como Descargar
February 4, 2026The world-building in the Twisted series starts here, establishing a network of friends and rivals that will span multiple books. Alex and Ava are the anchors of this world. Finding a Twisted Love PDF is the first step into a larger universe of interconnected stories. The prose is elegant and descriptive, immersing you in the setting. It is a book that offers an escape from reality, transporting you to a world of glamour, danger, and intense romance.
Twisted Love Epub Free
February 5, 2026What makes this book stand out in a crowded market is the depth of the backstory given to both protagonists. They are not just falling in love; they are solving the mysteries of their own lives. A search for the Twisted Love PDF reveals a story that is as much a thriller as it is a romance. Alex's cold calculation meets Ava's warm spontaneity, creating a chemical reaction that drives the plot forward. The supporting characters are also well-drawn, setting up future books in the series while adding flavor to this one. It is a comprehensive, immersive reading experience.
Marvinnon
February 10, 2026https://ultimelestiri.md/social/cum-o-companie-rusa-a-organizat-un-atac-cibernetic-asupra-unei-firme-din-r-moldova/#google_vignette
LymanCox
February 11, 2026Опрятный вид формирует сильное мнение о вас. Ваш образ влияет на оценку вас окружающими мгновенно. Уверенность в подобранном луке повышает вашу самооценку. Этот подход подчеркивает высокий стандарт ответственности и уважение к мелочам. https://r3.balmain1.ru/redirect.php?id=MzIVhXwqSKSY Посредством гардероб вы можете проявить свою индивидуальность и вкус. Окружающие неосознанно воспринимают стильных индивидов как более компетентных. Поэтому, инвестиции в свой образ — это вклад в ваше будущее.
LymanCox
February 13, 2026Стильный внешний вид создает первое мнение о вас. Он работает на оценку вас окружающими сразу. Хорошее самочувствие в своем луке укрепляет вашу уверенность. Он демонстрирует высокий стандарт ответственности и уважение к мелочам. https://b4.chenews.ru/redirect.php?id=UEH6IzEjySRN Посредством гардероб вы можете выразить свою личность и стиль. Люди неосознанно воспринимают стильных индивидов как более успешных. Поэтому, инвестиции в собственный стиль — это вклад в свое успешное будущее.
Edwardrag
February 17, 2026I consider, that you are not right. Let's discuss it. Write to me in PM, we will communicate. --------- https://avenue17.ru/
PeterDug
February 19, 2026I am sorry, that has interfered... I understand this question. Let's discuss. Write here or in PM. --------- https://avenue18.ru/
jJthrl
February 19, 2026166330 757624light bulbs are excellent for lighting the home but stay away from incandescent lamps because they create so significantly heat;; 555643