Chapter 27:
The completion of global certification: the Horn of Africa and China

INTRODUCTION
As the eradication of smallpox was certified, country by country and region by region, global certification activities finally focused on the Horn of Africa and China (Fig. 27.1). For very different reasons, these were the last regions of the world to provide the detailed information required before the global eradication of smallpox could be certified by the Global Commission in December 1979.
The Horn of Africa comprises 3 contiguous countries, Ethiopia, Somalia, and Djibouti (Fig. 27.2), in the first 2 of which smallpox had remained endemic after it had been eliminated from every other country in the world. The eradication programme in these countries had been hindered by warfare and civil disturbances (see Chapters 21 and 22), which continued into the period of precertification surveillance and of certification itself. The last known case of endemic small- pox in the world had occurred in Merca, Somalia, in October 1977. In Kenya, smallpox was related epidemiologically to outbreaks in Ethiopia and Somalia because of the common borders with those countries, and the 4 countries were therefore grouped together for certification purposes. Furthermore, because of the movements of nomads and refugees between them, it was essential that all 4 countries should be prepared for certification and visited by international commissions simultaneously. A symbolic target date was established for the final certification, 26 October 1979—exactly 2 years after the onset of rash in the last case in Somalia.
In China, it was believed that the last case had occurred many years earlier, but WHO had not been involved in either the eradication campaign or any follow-up activities, nor did WHO officials have access to China before 1972. Even then, it proved very difficult to obtain a satisfactory description of how and when smallpox had been eradicated until a visit by a WHO team was arranged by the Smallpox Eradication unit in July 1979. Because of the vast population and size of China, the Global Commission believed that the smallpox situation there should be properly documented before its smallpox-free status could be certified.
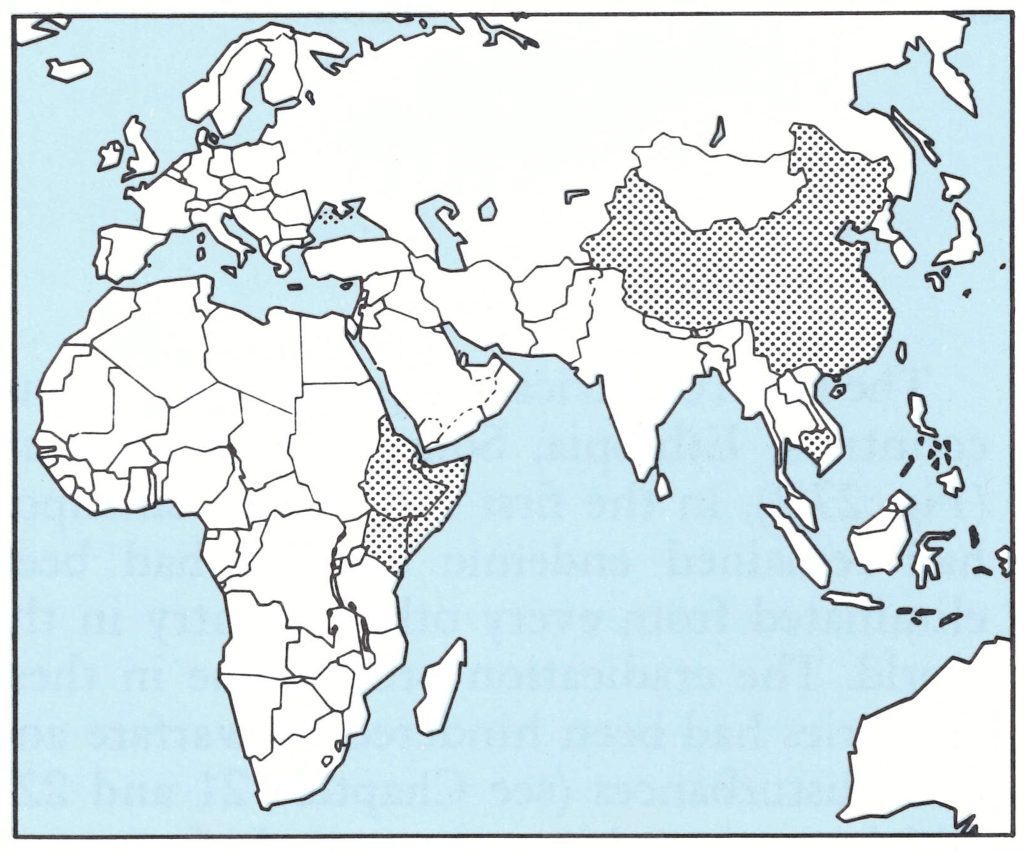
Fig. 27.1. The Horn of Africa, China and Democratic Kampuchea (see Chapter 26), the last areas in the world to be certified free of smallpox .
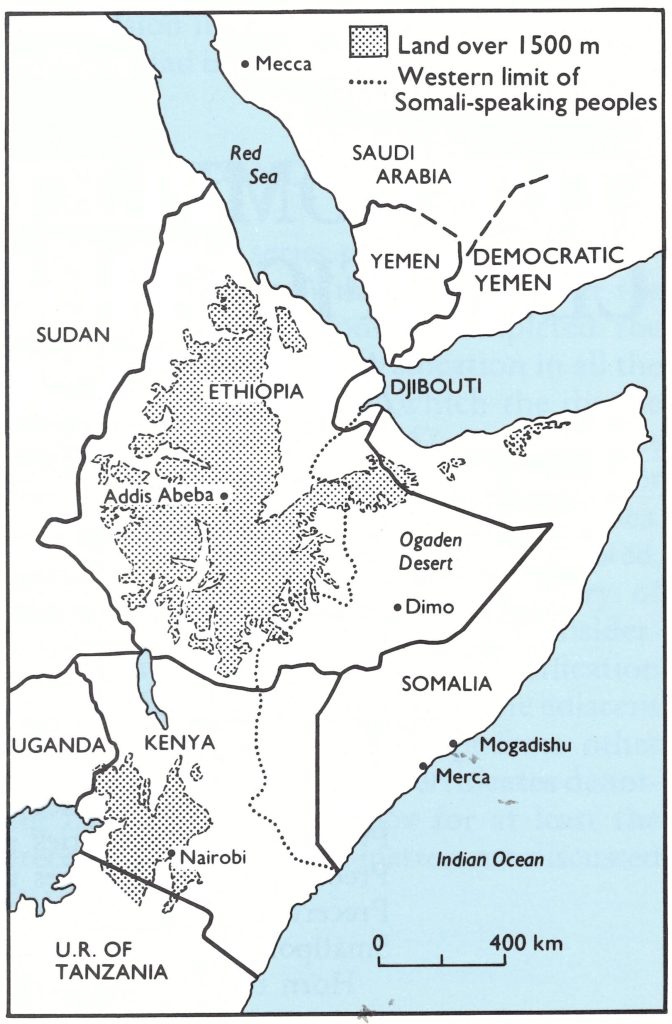
Fig. 27.2. The countries of the Horn of Africa and neighbouring parts of Africa and south-western Asia, showing land above 1500 metres. Dimo was the site of the last case of smallpox in Ethiopia, Merca that of the last case in Somalia.
PREPARATIONS FOR THE CERTIFICATION OF SMALLPOX ERADICATION IN THE HORN OF AFRICA
With the global eradication of variola major in October 1975 and the imminen eradication of variola minor during 1977, there was pressure to complete certification of the global eradication of smallpox as quickly as possible, because of its implications with respect to the discontinuation of routine vaccination and the abandonment of the requirement of vaccination certificates for international travellers. Because Ethiopia and Somalia were the last countries in the world in which smallpox had been endemic, it was possible to focus all available WHO resources on this effort, and from 1977 onwards much larger international resources were directed to these countries than had ever been made available to the other countries of Africa.
The problem of certification in the Horn of Africa was further compounded by the fact that the prevalent variety of smallpox had been variola minor, and studies in the area had shown that less than 10% of patients bore persistent facial scars after recovery. Thus pockmark surveys to determine whether smallpox had recently been present were of little use, and identifying cases of chickenpox, which might have been confused with variola minor, and obtaining specimens from them for laboratory testing, therefore became of great importance.
Coordination of Arrangements for Certification
In order to coordinate activities in the 4 countries and ensure that border areas were properly covered, the Smallpox Eradication unit organized a series of 3 coordination meetings. The first, in March 1977, was largely concerned with the completion of the eradication programme in Somalia and is described in Chapter 22; the second (September 1977) and third (April 1978) were devoted primarily to preparations for certification. Arita and Dr W. Koinange of Kenya undertook the laborious task of persuading sometimes reluctant governments to participate in these coordination activities.
Second coordination meeting, Nairobi, September 1977
In response to the emergency measures then in operation in Somalia (see Chapter 22), a second coordination meeting was held in Nairobi from 26 to 28 September 1977, 6 months after the first meeting, at a time when, as is now known, the interruption of transmission in Somalia was only a month away. It was attended by national smallpox eradication programme staff from Djibouti, Ethiopia, Kenya, Somalia, and the Sudan, together with WHO staff from the Smallpox Eradication unit and the WHO Regional Office for Africa. Despite the fact that, at the time, the Ethiopian Ogaden was occupied by the Somali army and the Western Somalia Liberation Front, a delegation from Ethiopia attended the meeting, exchanged information on surveillance activities with the participants from other countries and contributed greatly to the success of the meeting.
Discussions at the meeting were focused on how rapidly Somalia could eradicate smallpox and how the countries in the Horn of Africa could further strengthen their surveillance measures so as to prevent any further setbacks of the kind that had occurred in Somalia—namely, the establishment of new endemic foci following importations into smallpox-free areas. Important recommendations were made, among them the following
“Smallpox surveillance activities, including specimen collection, should be increased in all priority areas of the participating countries for the next 12 months and, during this period, special attention should be paid to the possible presence of smallpox foci in both displaced populations and remote areas where search activities might have been incomplete or improperly conducted and vaccination coverage might be low.
“Special measures should be taken by all the participating countries to ensure appropriate vaccination and control of persons who travel abroad, especially those going to Saudi Arabia for the forthcoming pilgrimage. Somali medical teams going to Saudi Arabia for medical service of their pilgrims should be accompanied by experienced smallpox surveillance officers so that smallpox surveillance can be exercised during the pilgrimage period.”
Third coordination meeting, Nairobi, April 1978
Since smallpox had not been reported from Somalia or elsewhere since October 1977, a third coordination meeting was held in Nairobi from 17 to 19 April 1978, specifically to discuss preparations for the certification of the Horn of Africa. It was planned that the meeting would be attended by programme staff from Democratic Yemen, Djibouti, Ethiopia, Kenya and Somalia, although at the last moment the delegates from Somalia were unable to attend owing to confusion about visas. Because of their proximity to Somalia, just across the Red Sea, it was originally intended that Yemen should also send repre- sentatives to this meeting. However, Democratic Yemen and Yemen were visited by international commissions and certified in June 1979, separately from the Horn of Africa (see Chapter 26).
The meeting decided that surveillance should continue at least until October 1979, in order to make sure that the Merca case had, in fact, been the world’s last case of endemic smallpox. It was agreed that complete documentation on eradication programmes and precertification activities in the countries of the Horn of Africa should be submitted to the meeting of the Global Commission in December 1979, so as to allow it fully to appraise the progress of the programme and report its findings to the Thirty-third World Health Assembly in May 1980.
The meeting also requested WHO to offer a special reward to the first person to report an active case of smallpox anywhere in the world.
Two weeks after the Nairobi meeting, the Thirty-first World Health Assembly did establish such a reward, the amount offered being US$1000 (see Chapter 24).
Message from the Director-General of WHO
The historical significance of the third coordination meeting in the context of the global programme was well expressed by the message of the Director-General of WHO to the meeting:
"It is now almost six months since the last case of onset of rash was recorded in the Somali smallpox eradication programme. Since that date, 26 October 1977, no further case of smallpox infection has been detected in the Horn of Africa, or anywhere in the world. This date, therefore, appears to mark the turning point in the global smallpox eradication campaign. Until then, the major objective had been to eliminate all smallpox foci. But now the situation has changed. Now it is our task to demonstrate whether we have broken the chain of smallpox transmission which has continued amongst the peoples of the world for thousands of years.
"In this respect, this meeting has a special place in the history of smallpox eradication. Proving the absence of the disease is likely to be no less difficult than containing outbreaks. There will naturally be a certain degree of doubt, since the event has never happened before in the history of medicine.
"I believe this meeting will tackle the problem of scientific credibility fully and squarely. But one point is already made clear. Surveillance, once established on a sound technical basis, should continue throughout two years following the detection of the last case. This is the only way to ensure that the international criteria of public safety have been fully met.
"One of the most heartening aspects of the global eradication campaign is the way the countries concerned have worked together to achieve the enormous progress made to date. Your participation in this meeting again demonstrates that sense of international solidarity, and the desire of the six countries you represent to contribute to the goal of worldwide global eradication. The most critical programmes are those in your areas . The next two years' surveillance will mark the crucial phase in the final confirmation of this worldwide achievement."
Precertification activities
Intensive precertification programmes were undertaken in all 4 countries in preparation for visits by 4 separate international commissions in October 1979. The situation in each country was different. In Ethiopia and Somalia, the personnel and organization of the national eradication programmes were retained but shifted their target from the elimination of endemic foci to an active search for unreported cases. However, the ease with which these operations were accomplished differed greatly in the 2 countries. At the time, the whole of Somalia was under government control and the intensive surveillance activities developed during the eradication programme continued throughout the next 2 years. In the much larger country of Ethiopia, although active surveillance could, with some difficulty, be carried out in most of the country, the Ogaden desert, which included portions of the 3 provinces of
Bale, Hararge and Sidamo, was the scene of active warfare, with armed forces moving from Somalia into Ethiopia. These disturbances greatly increased the difficulties of active surveillance. The Ogaden was clearly an area of special concern, requiring particularly intensive surveillance because, as epidemiological studies there had shown, the transmission of variola minor could be sustained for many months among comparatively small population groups (see Chapter 22).
Endemic smallpox had been eliminated from Kenya in 1969, but some importations had occurred thereafter, most recently in December 1976, in a rural area adjacent to Somalia, so that a special surveillance pro- gramme in that part of the country had had to be organized. Similarly, Djibouti had had to organize special surveillance in 1977 because of its proximity to the Ogaden, whence refugees were flowing into the country.

Plate 27.1. Participants at the third coordination meeting in Nairobi, 17 – 19 April 1978. Left to right, front row: Z. Islam (WHO), Yemane Tekeste (Ethiopia), 1. Arita (WHO), C. L. Khamis (Kenya), B. O’Keefe (Kenya), D.W.O. Alima (Kenya); middle row: H.B. Lundbeck (Sweden), K. R. Dumbell (United Kingdom), S.O. Foster (WHO), V. Radke (WHO), W.M. Jaffer (Democratic Yemen), Girma Teshome (Ethiopia); back row: P. R . Arbani (WHO), I.P. Mwatete (Kenya), M. N. El Naggar (WHO), J. F. Wickett (WHO), R.C. Steinglass (WHO).
Precertification Activities in Ethiopia
The Ethiopian smallpox eradication programme was conducted successfully during a period of considerable political disturbance (see Chapter 21), which continued and indeed became more serious during the preparations for certification. Both the eradication campaign and the subsequent precertification operations are described in detail by Tekeste et al. (1984).
The last known case in Ethiopia occurred in August 1976 in Dimo village, El Kere awraja, in the Ogaden. There were then 25 WHO epidemiologists, 15 national coordinators and about 1000 Ethiopian staff in the smallpox eradication programme, using some 90 vehicles. From the end of 1976 onwards, Ato Yemane Tekeste served as the project manager of the Ethiopian smallpox eradication programme. He was assisted by 3 WHO epidemiologists (Dr Lev Khodakevich as senior adviser, Dr Claudio do Amaral and Dr Poerwokoesoemo R. Arbani) and a WHO finance officer (Mr Omar S. Ismail). Under Ato Tekeste’s direction, 9 assessment officers supervised 15 programme coordinators, each responsible for one of the 15 regions, in the management, training and supervision of field staff as well as in the assessment of the programme. These coordinators employed a number of surveillance agents and intermediate supervisory staff, totalling about 1000.
With these changed staffing arrangements, the precertification activities were started early in 1977. During 1977, 1978 and 1979, when extensive searches for possible hidden foci were carried out, Eritrea as well as a number of other areas in the north and the Ogaden in the south were often partly or completely inaccessible because of civil disturbances and warfare. Accordingly, search operations were conducted or stopped as the areas became accessible or inaccessible. In border areas which became inaccessible to Ethiopian staff, rumours were investigated, wherever possible, from bases in Djibouti, northern Kenya and Somalia. This necessitated extensive coordination between the 4 countries through the exchange of reports on smallpox rumours, which was achieved by close contact between national programme directors and Arita, who frequently visited Ethiopia and the neighbouring countries.
Political events in the Ogaden
Because of military activities, precertification operations in areas under the control of the Ethiopian government were conducted differently from those in areas in which the government then had little control—namely Eritrea and the Ogaden (shown in Fig. 27.3 as a stippled area). Although the areas of limited access were geographically extensive, the majority of the population lived in the more accessible central highland areas. The last case of smallpox in Eritrea occurred late in 1972. Intensive searches in 1973-1974, before the activities of the separatist movement limited access to the rural areas, failed to reveal any evidence of further cases. The Ogaden desert, on the other hand, was the route by which smallpox had spread to Somalia in 1976 and was thus an area of great importance for surveillance.
Fig. 27.4 illustrates the changing fortunes of war in the Ogaden. Politically, the period of the smallpox epidemic in southern Somalia was marked at first by guerrilla activities in the Ogaden by the Western Somalia Liberation Front and then by the occupation of this area by the Somali army in July 1977. Eight months later the Ethiopian army recaptured the major towns, but continuing guerrilla activity prevented the resumption of normal surveillance elsewhere. By 1979 the situation had stabilized to the point where searches could be made along the western limits of the Ogaden.
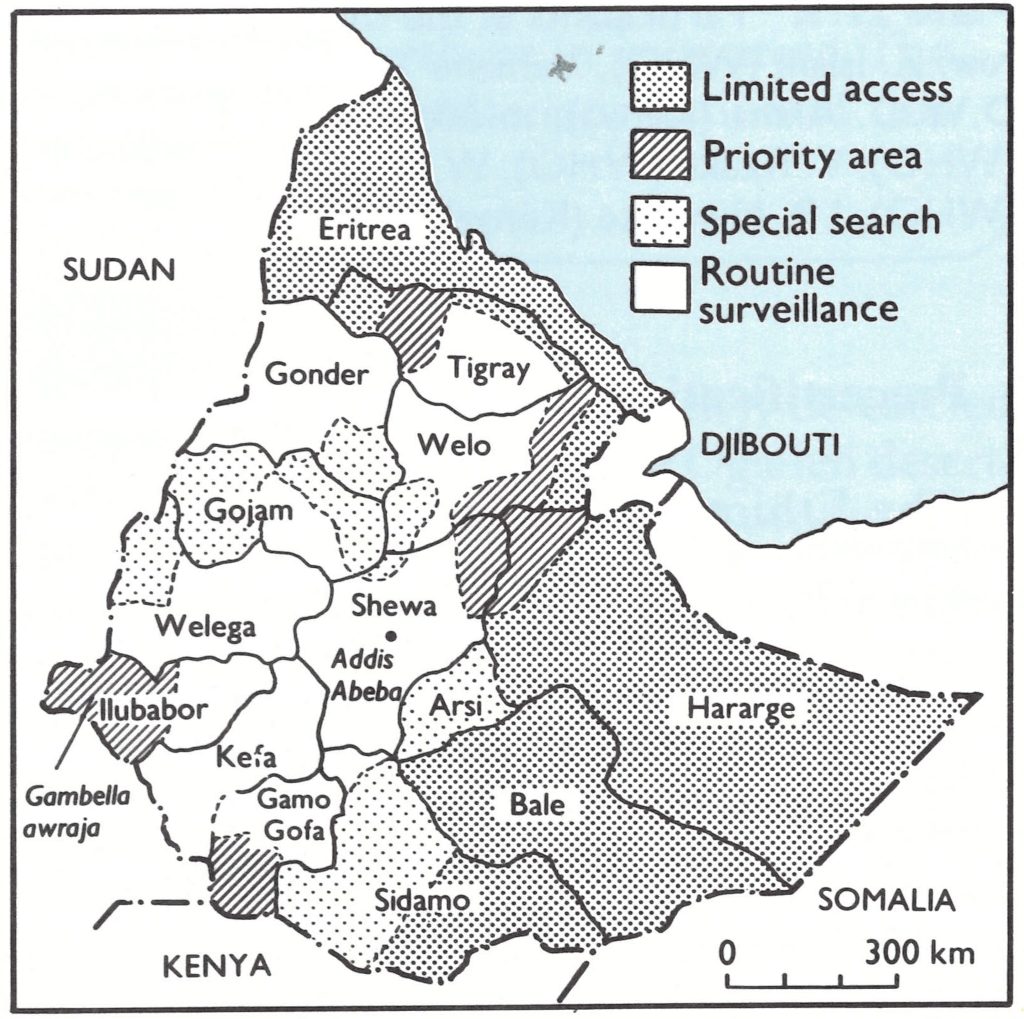
Plate 27.3. Ethiopia: status of surveillance at the end of 1977. Throughout the programme, civil disturbances were occurring in various parts of the country so that smallpox staff were excluded from certain areas. Priority areas were defined as those difficult to reach, but where there was sometimes a calm period of a few weeks during which an intensive search could be carried out. Special searches were organized in areas which were in principle accessible, but where a satisfactory routine surveillance system could not be established. Routine surveillance was based on regular contacts with the 20000 Farmers’ Associations, whose membership accounted for two thirds of the population of Ethiopia. For details of the search carried out in Gambella, llubabor, see box.
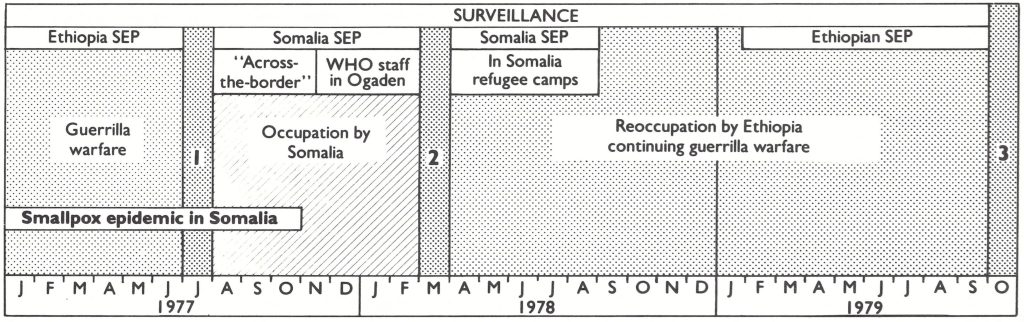
Fig. 27.4. Interplay between the changing fortunes of war in the Ogaden and smallpox surveillance activities. In July 1977 the Western Somalia Liberation Front overran the Ogaden and the Somali army established control (I). In March 1978, Ethiopian troops retook the Ogaden (2). Surveillance in varying degrees was maintained from both until eradication was certified in October 1979 (3). SEP = smallpox eradication programme.
Search in Gambella Awraja, Ilubabor Region
In Ethiopia, there were a few remote and inaccessible areas in which logistically it was extremely difficult to organize a search operation, Gambella awraja being one of them. This remote area (see Fig. 27.3) was inhabited mainly by primitive tribal groups. No smallpox had been reported there since the start of the eradication programme in 1971, but until 1978 the only search conducted was by a team consisting of an Ethiopian surveillance agent and a United States Peace Corps volunteer, who in April-May 1972 travelled by foot for about 290 kilometres along the Gilo river towards the Sudanese border to vaccinate and search for smallpox.
In March-April 1978, a well-planned search was conducted among the 140 000 inhabitants of this area. About 60 surveillance staff worked under the supervision of 2 Ethiopian coordinators and a WHO epidemiologist, Dr Claudio do Amaral, using helicopters and river transport. About two-thirds of all the houses in the awraja were visited by the team; the remainder had been abandoned because the people had moved close to the river, but the team visited them by walking along the riverbank. In all, 36 suspected cases were investigated, and 30 specimens were collected, but no smallpox was found.
Precertification activities in the accessible areas
Different parts of the politically accessible portion of Ethiopia presented somewhat different problems. Over most of the area routine surveillance was carried out through the newly established farmers’ associations (see below) in the rural areas and urban dwellers’ associations in the towns. In other areas special searches were organized. Certain areas were considered to be at high risk because the last cases had occurred there, access to them was difficult, or good routine surveillance had not been possible. In others, travel was safe only during a few weeks of calm between outbreaks of civil strife. Finally, there were some remote, sparsely populated areas which had been infrequently searched and which could not be reached without special logistic arrangements or transport by helicopters.
Searches in rural areas. The population of Ethiopia is predominantly rural, with only 11 living in towns or villages with 2000 or more inhabitants. The search for evidence of recent smallpox in most rural areas was based on the farmers’ associations, which were cooperatives comprising some 500-1000 persons. There were about 20 000 of them in Ethiopia in 1977. Because of the close contact between members of these associations and their chairmen, it was possible to acquaint them with the need for reporting smallpox cases, and during the active search operations each association became a basic unit for the collection of information on smallpox.
During 1977, local surveillance teams were supposed to visit all the farmers’ associations in their assigned areas 4 times a year. However, it soon became clear that coverage was erratic, 86 % of the farmers’ associations being visited at some time but some only once and many on several occasions. In 1978 this system was abandoned and a search for cases of smallpox was undertaken which covered some 50% of all houses in rural Ethiopia. Every month about one-fifth of all farmers’ associations were visited by the surveillance workers. In this way, 20 322 out of the 20 828 farmers’ associations were visited by surveillance workers between November 1978 and April 1979. The population thus contacted, either direct or through their neighbours, amounted to about 20 million—two-thirds of the total population of Ethiopia.
During the search the supervisors of the surveillance workers investigated 7260 cases of fever with rash and collected 929 specimens. A large number of cases of chickenpox and measles were seen, but no cases of smallpox.
Searches in urban areas. In addition to the searches in rural areas, the surveillance agents also searched urban areas during 1978 and 1979 ; thus 760 of the 929 towns, with a total population of 3.8 million, were searched, about 2500 cases of fever with rash being investigated and 189 specimens collected. Once again, no smallpox cases were found.
Second visits to the sites of the last outbreaks. During the period 1971-1976, smallpox had occurred in 99 of the 102 awrajas in Ethiopia. Between November 1978 and March 1979 the sites of the last outbreaks in 64 of these 99 awrajas were revisited by surveillance teams (Fig. 27.5). In the other 35 awrajas, mainly in Eritrea and the Ogaden, no such follow-up visits could be arranged because of civil strife and the resettlement of the rural population. During the visits to these 64 awrajas, 2 additional outbreaks were identified which had occurred before August 1976, but there were no signs of transmission after the last recorded case.

Fig. 27.5. Ethiopia: Location of the last outbreaks of smallpox in 64 accessible awrajas that were reinvestigated during 1979.
Laboratory investigations. The variety of smallpox occurring in Ethiopia in the 1970s was variola minor, which elsewhere had been found to leave facial pockmarks in less than 10% of cases. As an alternative to pockmark surveys as a way of detecting missed cases of smallpox, special attention was devoted to the surveillance of chickenpox. Large-scale collections of specimens for laboratory investigation were made from cases of chickenpox or fever with rash, 2886 specimens being examined between 1977 and 1979 (Table 27.1). Fig. 27.6 shows the distribution, by awraja, of specimens collected during 1977 and 1978.
Variola virus was not found, but herpesvirus particles were seen in about 25 of the specimens and vaccinia virus on 9 occasions. The latter resulted from contamination, since specimens were sometimes collected while vaccinations were being performed.
Table 27.1: Ethiopia: results of laboratory examinations of specimens submitted to WHO collaborating centers, 1977-1979
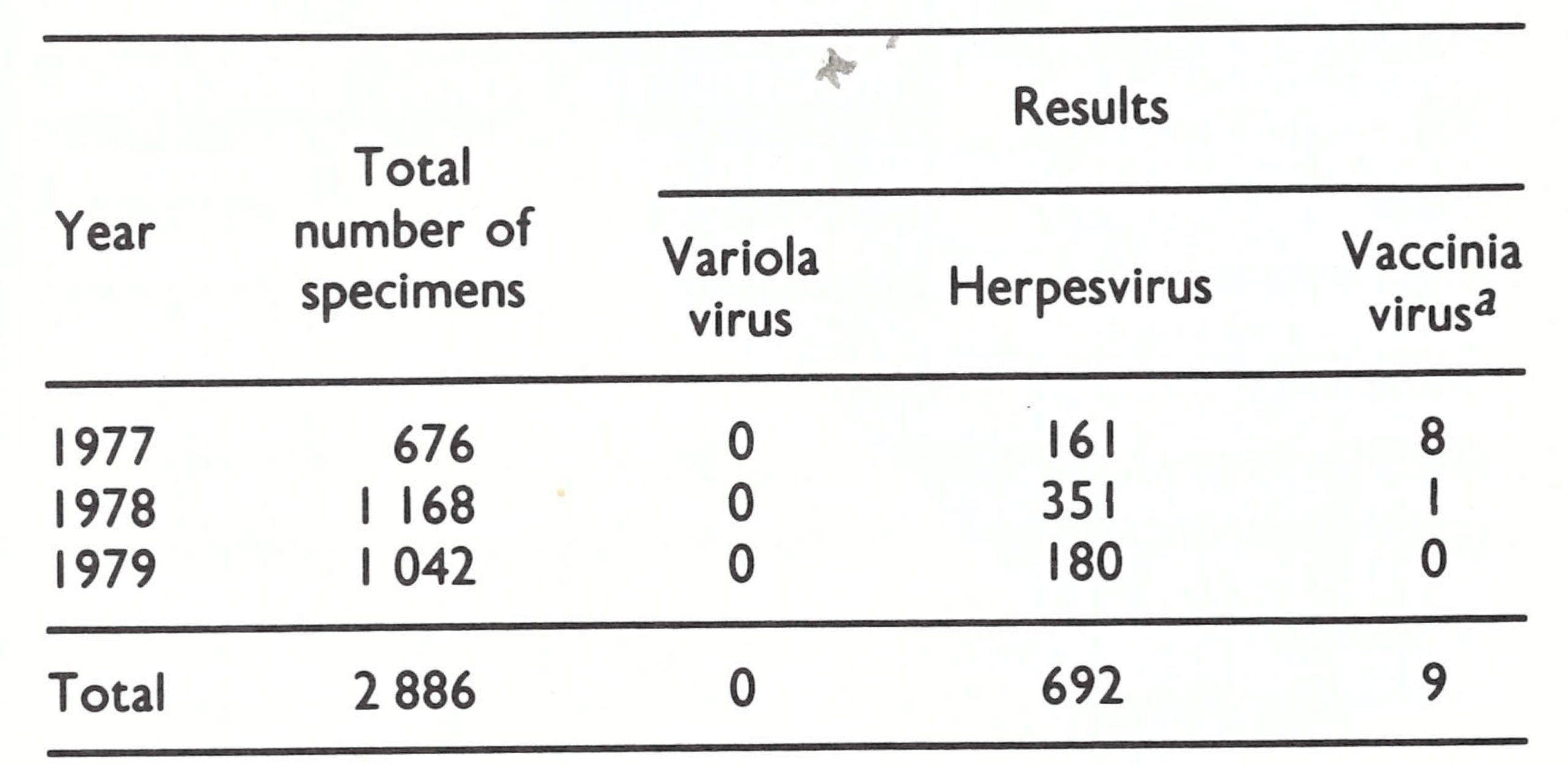 a Present as a result of contamination.
a Present as a result of contamination.
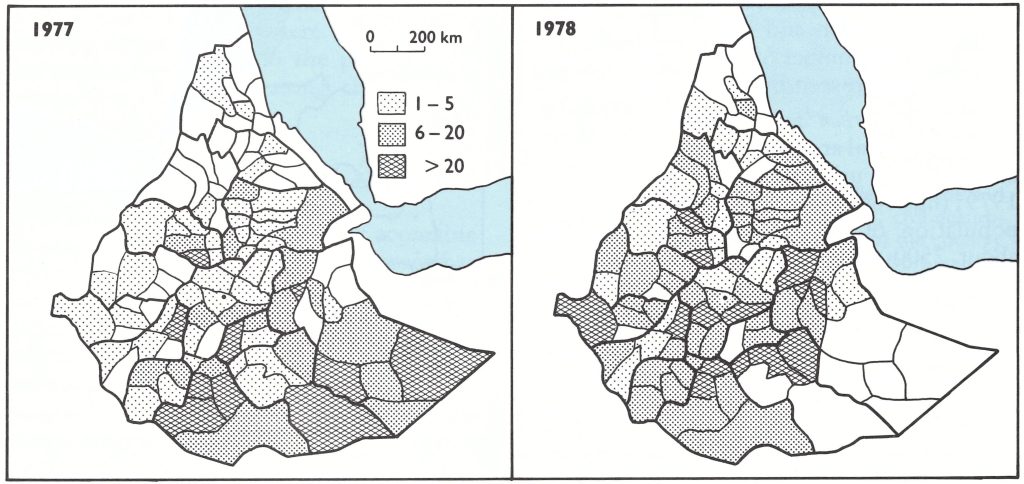
Fig. 27.6. Ethiopia: Numbers of specimens collected for laboratory examination in 1977 and 1978 by awroja.
Precertification activities in the Ogaden desert
The Ogaden desert, which traverses the major portion of the regions of Hararge, Bale and Sidamo (see Fig. 27.3), comprises 10 awrajas with a total population of about 1.4 million, most of whom are Somali-speaking nomads. It lies on a plateau bordered to the north and west by the Ethiopian highlands and to the south and east by Somalia, and by a small corner of Kenya in the extreme south-west. At its widest the desert extends 800 kilometres from east to west and 400 kilometres from north to south; it covers an area of about 200 000 square kilometres (Fig. 27.7). From the autumn of 1976 onwards the increasing guerrilla activities in the Ogaden made it more and more difficult for both WHO and Ethiopian programme staff to carry out surveillance; smallpox programme activities conducted by Ethiopian staff were finally halted in July 1977, when the Somali army invaded the area, but were resumed in March 1978, when the Ethiopian army regained possession.
Arrangements for surveillance. To cope with this situation, Arita went to Addis Abeba in mid-1977 to discuss with local WHO and Ethiopian national programme staff how best to maintain active surveillance in the Ogaden. This was of the utmost importance, because the Western Somalia Liberation Front had overrun the area, so that it was inaccessible to the Ethiopian smallpox eradication programme staff. Moreover, at that time smallpox was still endemic in southern Somalia. There was therefore a real risk that endemic smallpox might be re-established in Ethiopia, and it was essential that this should be prevented.
Two major actions were therefore taken, one in Ethiopia and one in Somalia. First, in Ethiopia a “belt” area was established between the highland areas adjacent to the Ogaden, which were under Ethiopian control, and the Ogaden desert, stretching from Djibouti to the border with Kenya (Fig. 27.7). An intensive surveillance and vaccination programme was carried out here between September and December 1977. On average, 55% of all farmers’ associations were visited each month and by the end of the 4-month campaign, virtually all had been visited by a worker from the Ethiopian smallpox eradication programme. Altogether 348 suspected cases were investigated and 272 specimens collected, but no evidence of smallpox was found.
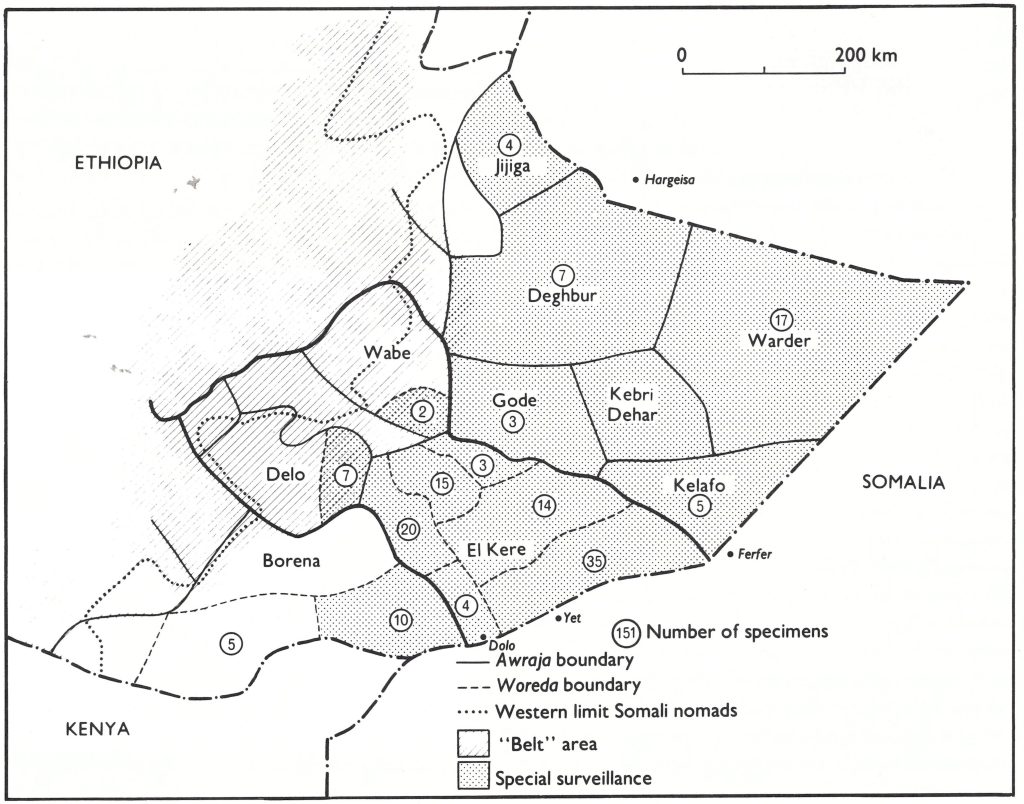
Fig. 27.7. Ethiopia: Areas of the Ogaden desert under special surveillance, showing awrajas in Hararge, Bale and Sidamo Regions, the western limits of the seasonal migrations of the Somali nomads, and the “belt” area where a special vaccination campaign was conducted in September-December 1977. The numbers of specimens collected for laboratory examination between July 1977 and April 1978 are shown by awraja and woreda.
Secondly, an attempt was made to conduct an active search from the Somali side. Efforts to achieve this by collaboration with the International Committee of the Red Cross, which was doing relief work for wounded soldiers in the Somali-occupied areas of the Ogaden, were unsuccessful, but other arrangements succeeded.
Early in September 1977, Arita organized a private meeting in Mogadishu of senior WHO and Somali staff who had extensive experience of surveillance and knew the geography of the Ogaden. It was decided to seek the agreement of the Western Somalia Liberation Front to enter the Ogaden and to employ 5 WHO epidemiologists, Dr Mohamed El Naggar, Dr Bert van Ramshorst, Dr Jean-Paul Ryst, Dr Jay S. Weisfeld and Mr Carl Hasselblad, to carry out across-the-border searches. Operational border posts were established in Hargeisa, Ferfer, Yet and Dolo (see Fig. 27.7). Many of the workers who had been employed in this area under the aegis of the Ethiopian smallpox eradication programme were recruited, because most had remained in the area after it had been occupied and were happy to return to duty. As the WHO epidemiologists could not cross the border into the area, which was under the control of the Somali army and the Western Somalia Liberation Front, experienced local workers supervised the searchers and verified rumours.
During these surveillance activities, 143 searchers visited 599 villages and 383 watering-places; 219 rumours were inves- tigated. Posters giving information on the reward offered were displayed in each of the villages and at Koranic schools and watering places. The number of rumoured cases of smallpox was almost certainly exaggerated, as former Ethiopian staff had not been paid since the cessation of their programme in the area; by providing reports of possible cases of smallpox they assured their continued employment. In spite of the many suspected cases reported, experienced national epidemiologists found no evidence of continuing transmission.
In November 1977, Arita was informed by messenger that the Western Somalia Liberation Front had agreed that WHO staff could work in the Ogaden. Dr El Naggar, accompanied by a Somali counterpart, entered the Ogaden from Somalia to supervise surveillance personally and to check rumours. Because he was known to the local population, they cooperated closely with him. Borena and El Kere awrajas were chosen for the initial searches because they shared long borders with areas of southern Somalia in which smallpox had persisted until October 1977; furthermore, 11 of the 12 rumours of smallpox which had not been investigated by a WHO epidemiologist had originated in this area. Dr El Naggar supervised 20 searchers, who visited 33 000 houses and 300 Koranic schools. Independent assessment revealed that 94.6% of the houses had been visited by the searchers and that 51 % of households knew of the reward of 200 Somali shillings (US$32). No smallpox was found.
In January 1978, Dr Rabie A. L. Khattab succeeded Dr El Naggar as the WHO epidemiologist responsible for surveillance in the Ogaden. He continued the programmes in Borena and El Kere awrajas and extended his activities to the adjacent awrajas of Delo and Wabe. With the aid of 79 searchers, 20 000 houses and 700 Koranic schools were visited, but no evidence of smallpox was found. Surveillance from the Somali side was terminated early in March 1978, when Ethiopian forces reoccupied the Ogaden, but was then resumed under Ethiopian auspices.
Search in Gambella Awraja, Ilubabor Region
Early in 1977, the Ethiopian national smallpox eradication programme tried to strengthen surveillance by the assignment of 4 WHO epidemiologists (Dr do Amaral, Dr Arbani, Dr El Naggar and Dr Gromyko) and national coordinators . However, because of increasing unrest in the Ogaden, their activities were limited in scope outside the capital towns of the awrajasof Kebri Dehar, Deghbur, Warder, Kelafo, Gode and El Kere in the Ogaden desert (Fig . 27.7).
In April, Mr William Waugh, one of the helicopter pilots working for the Ethiopian smallpox eradication programme, was kidnapped at gunpoint and held for ransom near Gode. In May, Dr do Amaral was held for 2 days in Somalia when he came too close to the border while checking a rumour in Warder awraja. Again, in June, he was kidnapped by guerrillas in Warderawraja but a week later turned up in Hargeisa in northern Somalia.
In June, immediately after this incident, WHO received a cable from the United Nations Economic Commission for Africa (ECA), Addis Abeba, stating that WHO epidemiologists were taking unacceptable risks. Arita flew to Addis Abeba to attend a meeting with ECA security officials to discuss the matter. It was agreed that the withdrawal of WHO epidemiologists would in fact mean the discontinuation of precertification activities, which would be a set-back not only for the eradication campaign in the Horn of Africa, but also for the global programme as a whole. The participants agreed that minimal activities should be continued by WHO and national staff in the Ogaden, but formulated a plan for emergency evacuation, should this prove necessary.
During the last 2 weeks of July, however, the Somali army invaded and overran the entire area, forcing the withdrawal of all the WHO staff. Thus, the surveillance of smallpox by the Ethiopian smallpox eradication programme ceased in these areas until March 1978, when the Ethiopian army resumed control.
Laboratory investigations. During special surveillance activities in the Ogaden between July 1977 and March 1978, 151 specimens were collected from cases of chickenpox or fever with rash and tested by WHO collaborating centres. The geographical distribution of the cases from which these specimens were collected is shown in Fig. 27.7. All the important areas in which smallpox importation or transmission was suspected were covered. Half the specimens were collected in El Kere awraja, the area in which the last known smallpox case in Ethiopia had occurred. Four of the 151 specimens were reported to contain small numbers of pox virions, as revealed by electron microscopy. Vaccinia virus was cultured from 2 of them, while the other 2 were negative. It was found that surveillance workers were using bifurcated needles that had been used for vaccination, to dislodge scabs, so that the positive results were presumably due to contamination with vaccinia virus. The source of 1 of the 2 specimens which was negative on culture was investigated by a WHO epidemiologist, who reported that, on clinical and epidemiological grounds, the case was definitely not smallpox. It was not possible to reinvestigate the patient from whom the fourth specimen had been taken. It was collected in July 1977 in El Kere awraja, but intensive and continuous search between August 1977 and March 1978 failed to find any smallpox in this area.
Plate 27.2. Mohamed Noureldin El Naggar (b. 1938), Egyptian epidemiologist, joined the programme as a consultant in March 1975 in Bangladesh. After 6 months he was transferred to Ethiopia. He played a very important role in precertification activities in the Ogaden.
Precertification Activities in Somalia
When the last known case occurred in Merca, southern Somalia, in October 1977,19 WHO epidemiologists, 27 national epidemiologists, and about 1600 other personnel, using 65 vehicles, were engaged in surveillance and containment measures for the smallpox eradication campaign. Dr Abdullahi Deria, director of the national campaign, and Jezek, WHO coordinator, assisted by Mr Rodney J. Hatfield, WHO administrator, directed the campaign. This impressive force continued active search operations during 1978 and 1979, as required for certification, although the number of WHO epidemiologists was reduced to 10 by the end of 1977 as activities became better organized. The eradication campaign and subsequent precertification activities have been described in detail by Jezek et al. (1981).
Development of reporting systems
Apart from one person who was infected in southern Somalia in July 1977, but moved to a military camp in the north during the incubation period, all cases in the Somali epidemic had occurred in southern Somalia. The surveillance and containment programme had therefore been focused on that part of the country. With the conversion of the programme into post-eradication active search operations, routine reporting systems were developed throughout the country. To achieve this, a smallpox office was established in each of the 16 regions and 83 districts (Fig. 27.8).
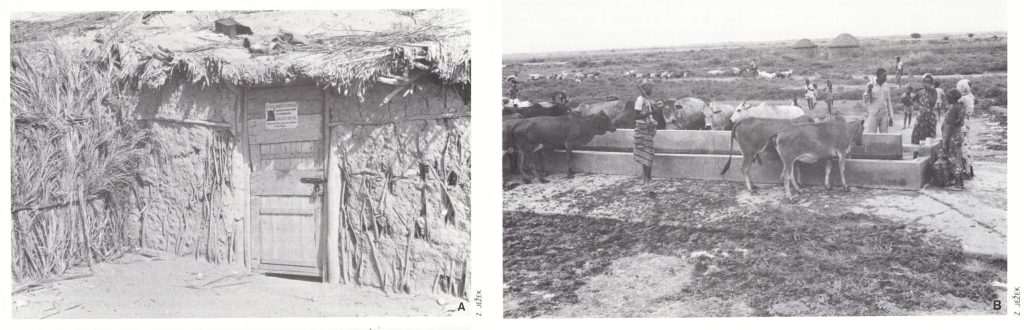
Plate 27.3. Precertification activities in Somalia. A: During periodic searches, a reward poster or written message was left on the door of the hut if no one was home. B: Watering points were natural gathering places for pastoral people and were an important source of information about nomadic groups.
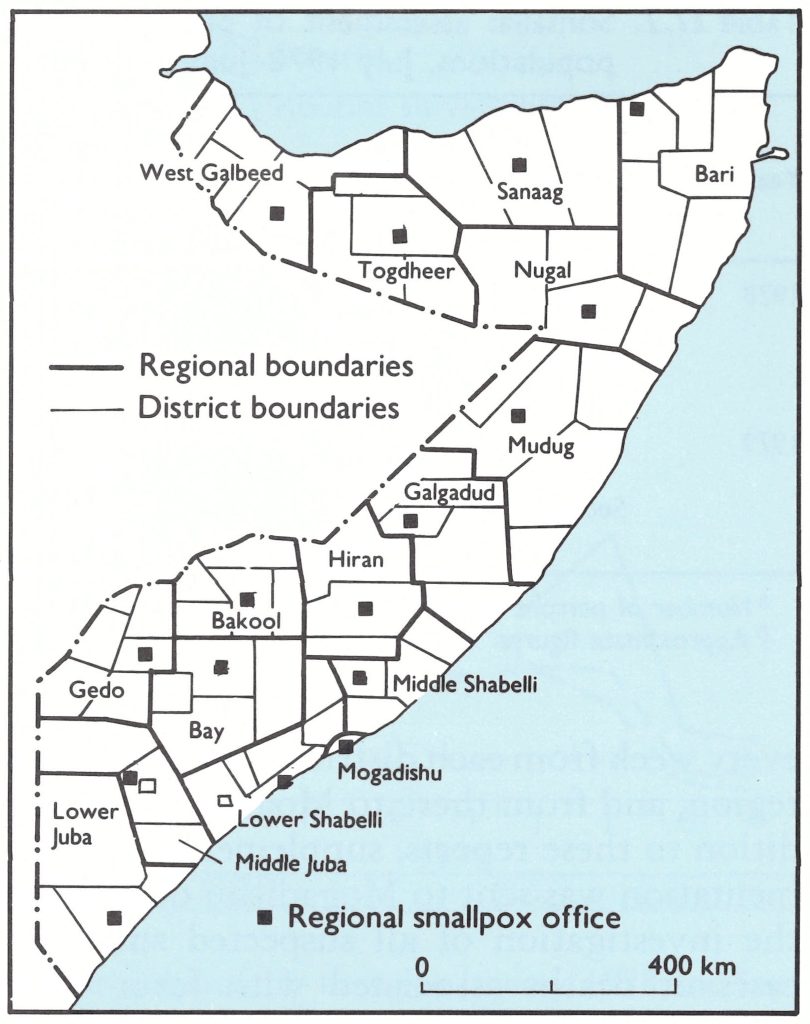
Fig. 27.8. Regions (named) and districts in Somalia. A smallpox office was established in each region and district during the period 1978-1979.
The regional smallpox offices were staffed by WHO or national epidemiologists and the district offices by local staff. They served to intensify the routine reporting of suspected cases of smallpox and other cases of fever with rash. A cable reporting findings was sent every week from each district to its respective region, and from there to Mogadishu. In addition to these reports, supplementary documentation was sent to Mogadishu describing the investigation of all suspected smallpox cases or deaths associated with fever with rash.
Although new to Somalia, this reporting system proved to be most effective, almost complete returns being received from all the smallpox offices. Regional and district offices gathered comprehensive demographic data including maps showing localities, households, population, etc., which were also used for other health programmes. These had to be updated frequently as the nomadic population moved from one part of the country to another.
Search for cases of fever with rash
The search for cases of fever with rash which had been developed during the smallpox epidemic in 1977 (see Chapter 22) was continued throughout 1978 and 1979. Six country-wide searches were conducted in 1978 and 3 in 1979. Except in the searches carried out during the first 3 months of 1978, all districts were covered (Fig. 27.9).
Following the pattern that had been developed in India, every search was assessed by national assessment teams, which found coverage to be very good (Fig. 27.10); over 70% of the general public reported that they had seen searchers with recognition cards and knew about the reward and where to report a case of suspected smallpox if they found one (Table 27.2). The high level of awareness among the nomadic population was impressive, since these people were rarely in contact with the established health services.
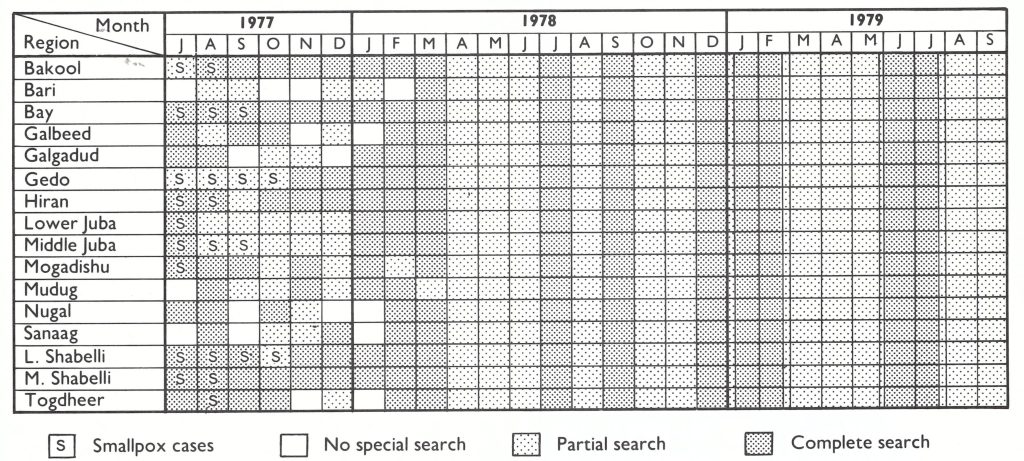
Fig. 27.9. Somalia: Frequency of search operations for cases of fever with rash, by region. Partial searches were carried out by regional surveillance teams at hospitals and markets, and in high-risk areas. Most parts of the country were searched 6 times in 1978 and twice in 1979. In 1978 the full search procedure usually lasted a month but in 1979 less frequent searches allowed greater attention to detail and more thorough independent assessment of performance.
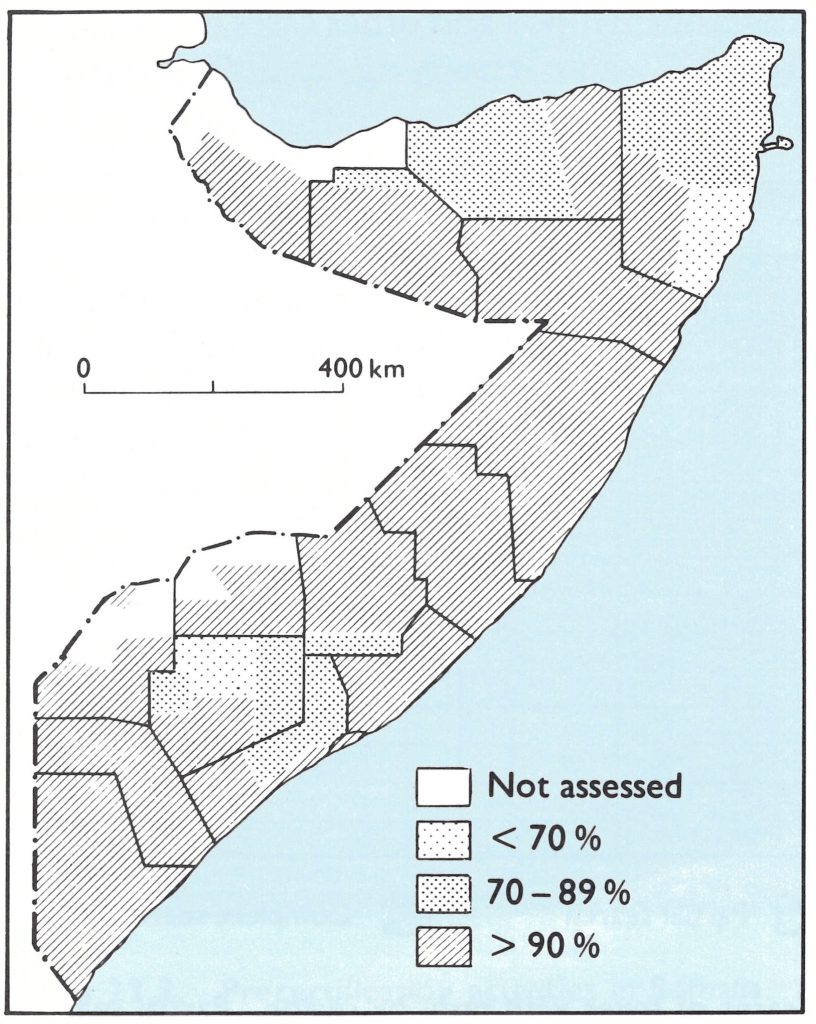
Fig. 27.10. Somalia national assessment of March 1979: percentages of localities found to have been searched in each district.
Table 27.2: Somalia: results of laboratory examinations of specimens submitted to WHO collaborating centres, 1977-1979
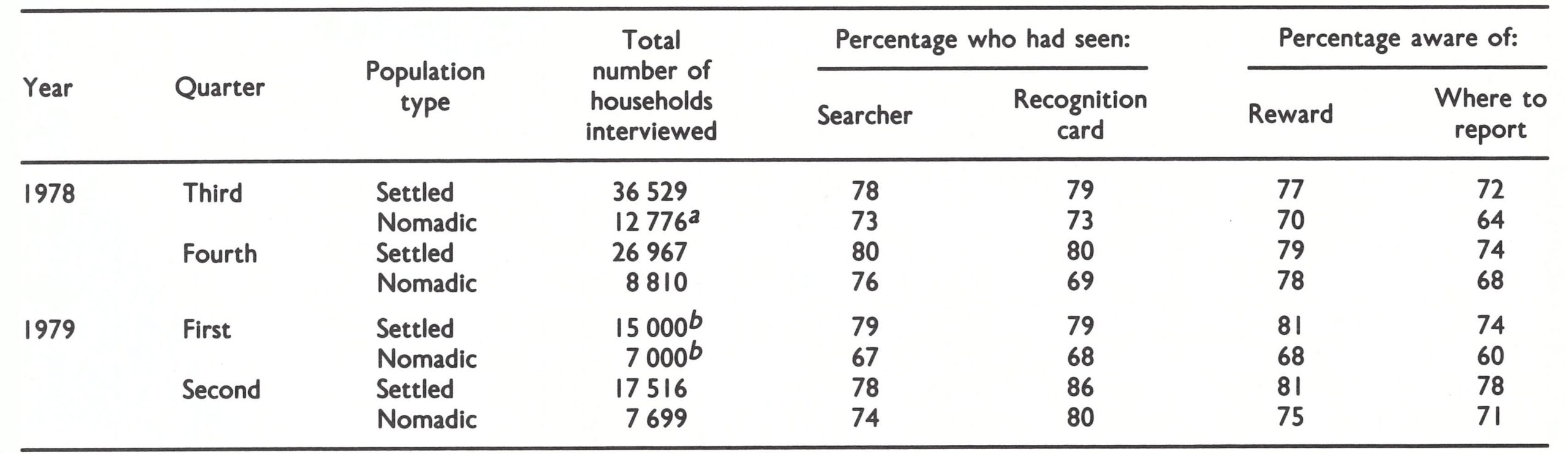 a Number of persons interviewed.
a Number of persons interviewed.
b Approximate figures.
In all, 19 623 cases of fever with rash were investigated in 1978 and 11 576 cases during the first 9 months of 1979 (Fig . 27.11). The diseases seen included chickenpox, measles and various other diseases associated with a rash;none proved to be smallpox.
Laboratory investigations
Laboratory specimens were collected from patients with clinically suspected smallpox and chickenpox, especially from those who had not been vaccinated, as well as from individuals affected in outbreaks of fever with rash in which a death had occurred.
Altogether 1646 specimens were collected in 1978 and 1074 in 1979, all of which were negative for variola virus (Table 27.3). Speci- mens were collected from all over Somalia, especially from the south (Fig. 27.12). The absence of variola virus in any of the specmens gave staff confidence that variola minor had not been misdiagnosed as chickenpox.
Precertification Activities in Kenya
Despite strenuous efforts, Kenyan and WHO epidemiologists had not been able to identify the geographical source of the outbreak of smallpox in Mandera District, northern Kenya, which occurred between December 1976 and February 1977, but it was thought to have been the result of importation from Somalia (see Chapter 19). During 1978 and 1979, searches in Kenya were conducted by staff recruited within the districts to be searched, and supervised by local health workers and senior health officers from the Division of Disease Control of the Ministry of Health, Nairobi. Dr W. Koinange, a Kenyan member of the Global Commission, Dr Ziaul Islam and Mr Vincent Radke contributed to the development of the Kenyan certification work. The Ministry of Health offered a reward of 200 Kenya shillings (US$25) for any confirmed smallpox case, and the radio and press publicized the search operations and the need to report promptly any cases of fever with rash to the staff of the nearest health unit or to other government officials.
Special searches
High-risk areas were designated, essentially those bordering on Ethiopia and Somalia (Fig. 27:13), and special searches conducted in them. Searches were supervised at three levels: (1) by the public health technician (daily supervision); (2) by senior supervisors from the district headquarters; and (3) by independent assessment teams consisting of both national staff and their WHO counterparts working in the Division of Disease Control.
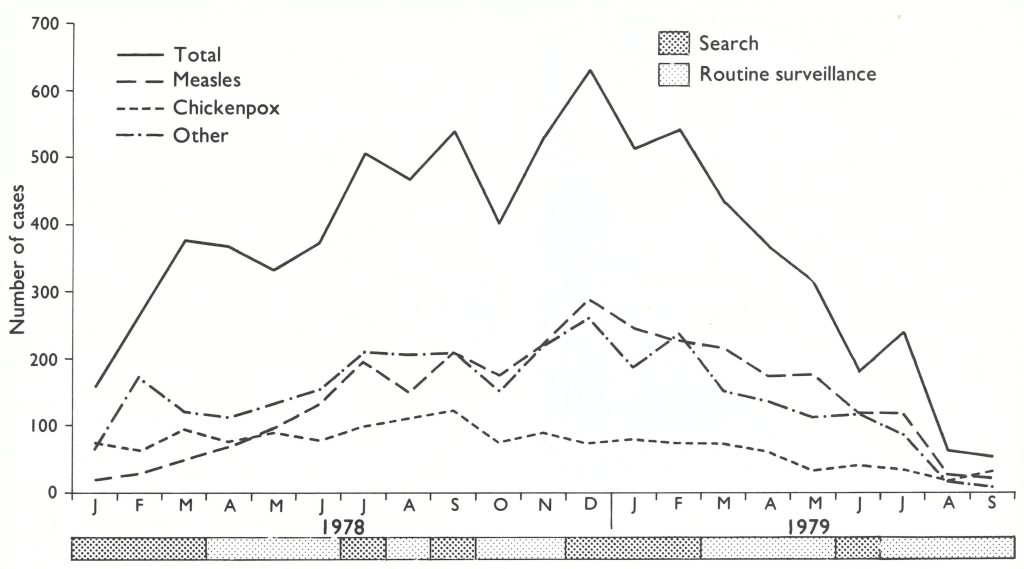
Fig. 27.11. Somalia: Number of cases of fever with rash reported monthly between January 1978 and September 1979.
Table 27.3: Somalia: results of laboratory examinations of specimens submitted to WHO collaborating centres, 1977-1979
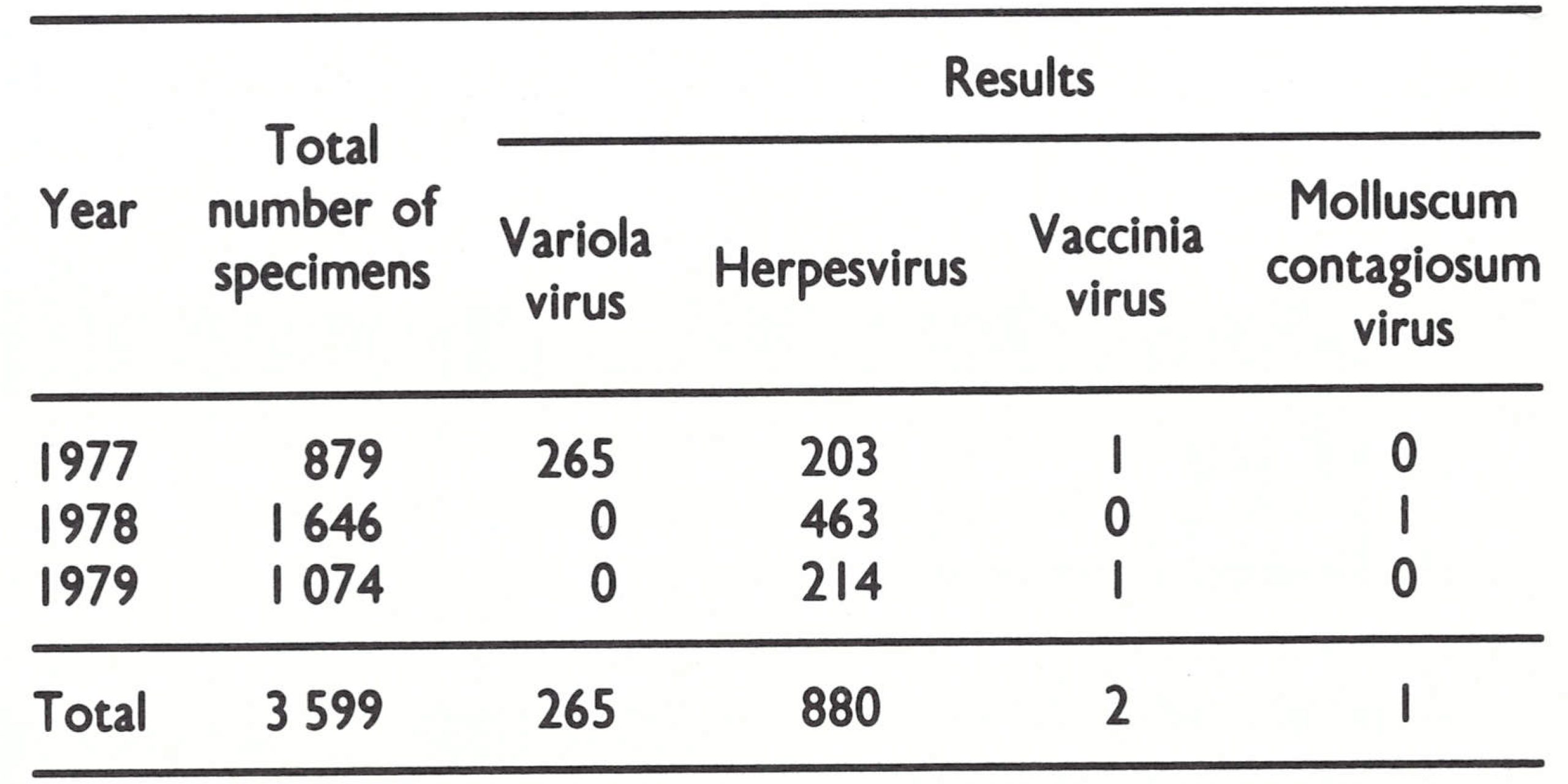
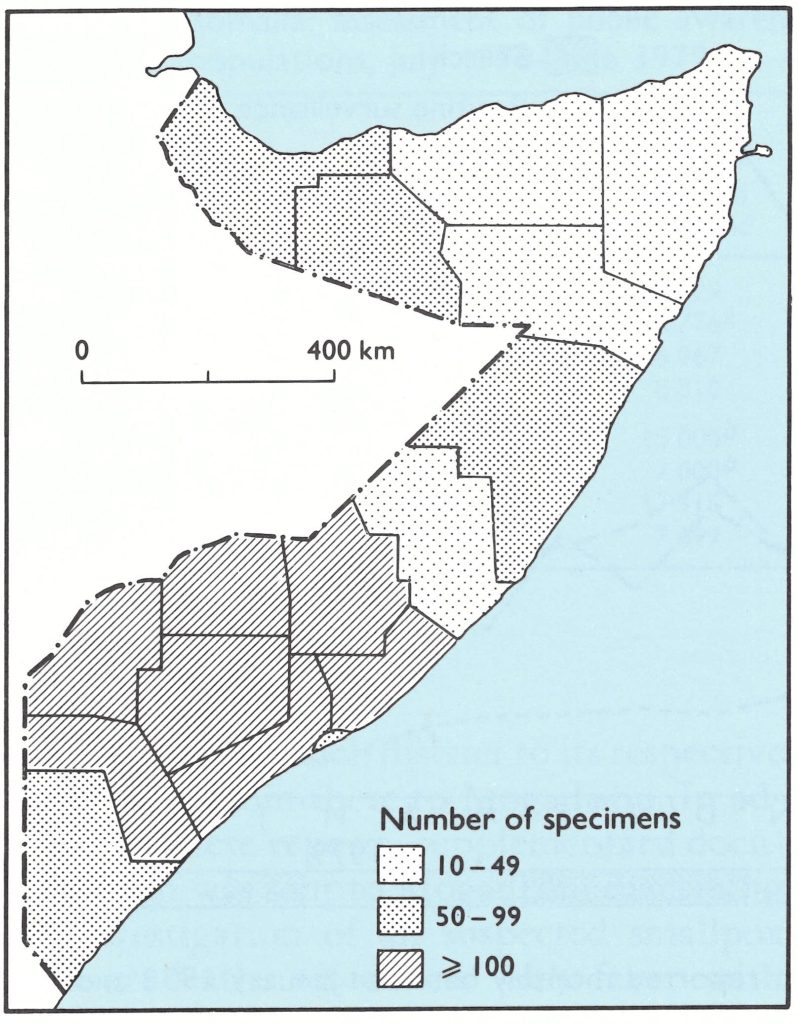
Fig. 27.12. Somalia: Number of specimens collected for laboratory examination from cases of fever with rash during 1978, by region.
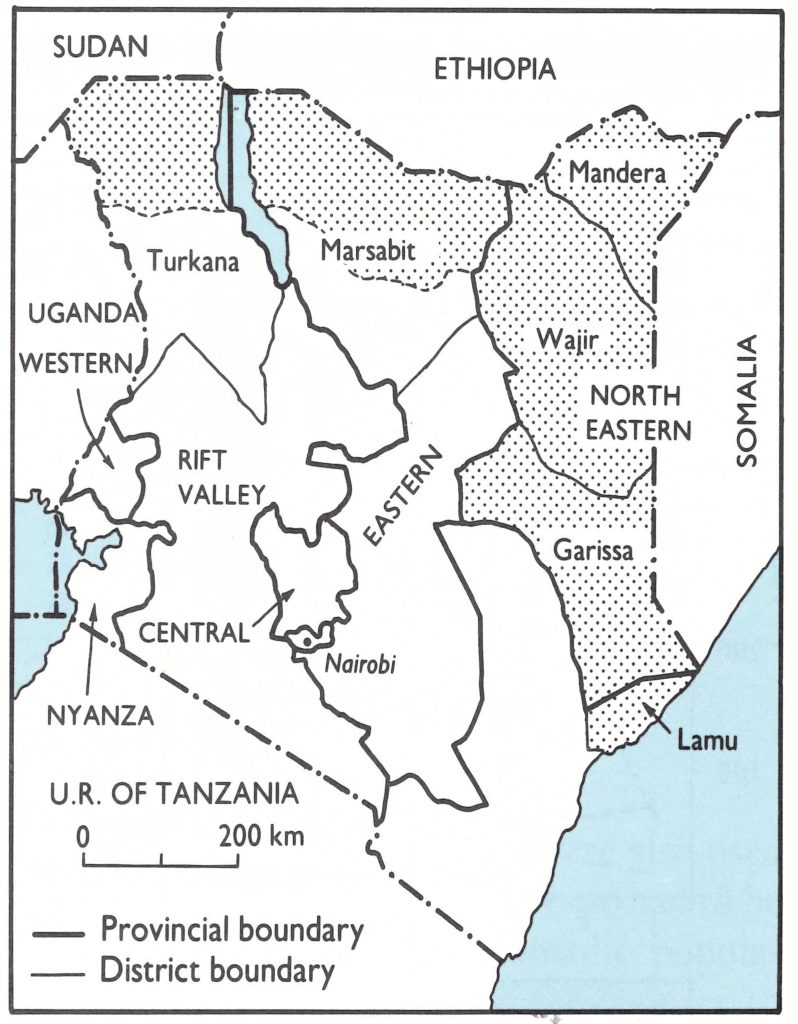
Fig. 27.13. Kenya: Areas of high priority for active search operations in 6 northern districts.
The searches in the high-risk districts of Mandera, Wajir, Garissa and Marsabit were conducted between September 1977 and March 1978,189 searchers and 43 supervisors, with 16 vehicles, being employed (Table 27.4). They covered over 440 000 persons in an area of 200 000 square kilometres.
In Mandera District, 6 searches were conducted, although occasionally some areas were not accessible to the local searchers and supervisory staff because of bad weather or for security reasons. Out of 134 rumours received only 2 could not be checked immediately because of security problems, but were checked later when the areas were visited.
In Wajir District, areas bordering on Ethiopia and Somalia were given priority in surveillance and vaccination activities . At the time, a large number of people had crossed from Ethiopia into northern Kenya to escape the conflict in the Ogaden and in search of water and grazing land. As rumours of smallpox from the Ethiopian side of the border came to the attention of Kenyan teams, they crossed the border to investigate whenever the security situation permitted. Five searches were conducted in the district and 35 rumours of possible cases were recorded. Only 3 rumours, all from the Ethiopian side of the border, could not be investigated because of security problems. However, cross-notifications were made to the Ethiopian health authorities through WHO in Geneva. Although Garissa District was not as important epidemiologically as Mandera and Wajir Districts, 4 searches were conducted there and I search in the northern area of Marsabit District.
A cluster sampling technique was used in assessing the search operations, 118 out of 120 localities sampled being assessed (98.3%) and 905 people interviewed. Of the latter, 72% reported that they had seen the searchers, and 75% had a smallpox vaccination scar.
Laboratory investigations
In 1978 and 1979, 1599 specimens were collected in high-risk areas and tested by WHO collaborating centres, with negative results.
Table 27.4: Kenya: results of active search operations, September 1977-March 1978, by district
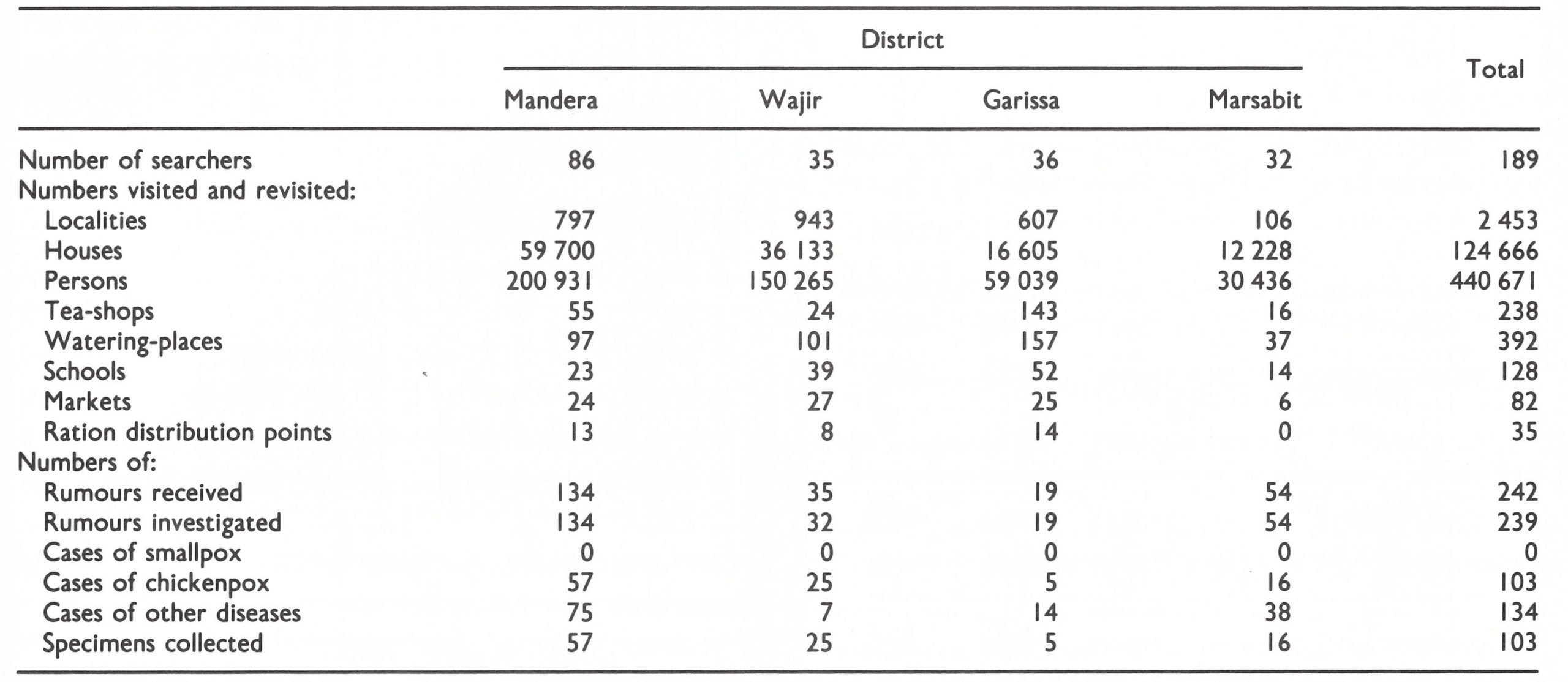
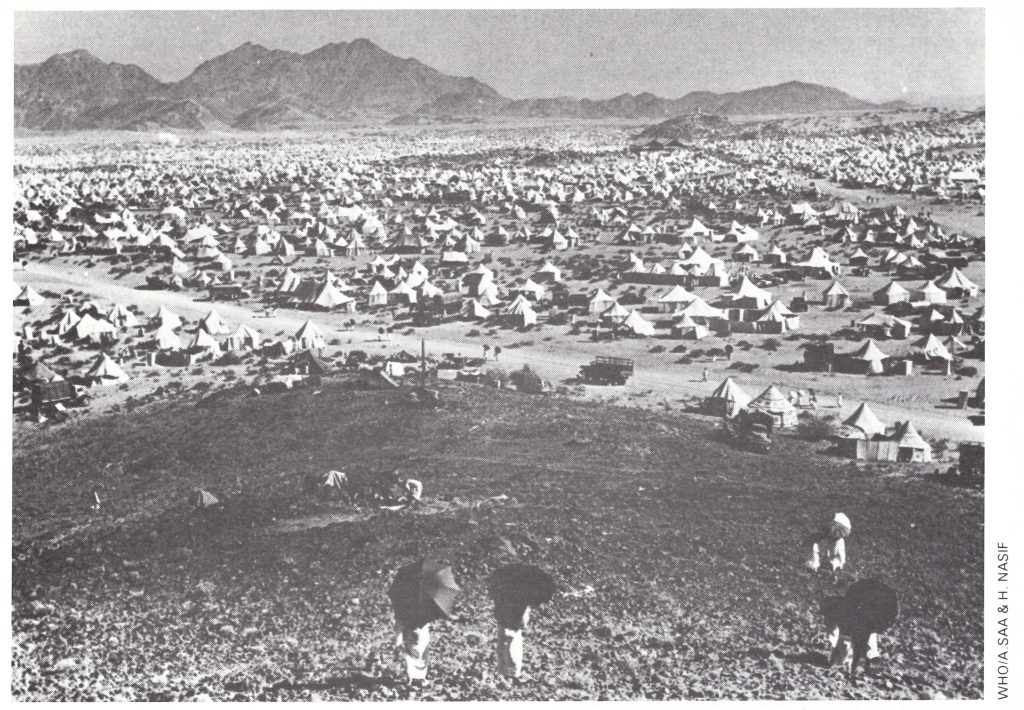
Plate 27.4. Pilgrims’ tents near Mecca in Saudi Arabia. The annual influx of people from the Muslim world provided an explosive potential for the spread of smallpox.
Precertification Activities in Djibouti
Whenever famine or political unrest occurred in the Ogaden desert, many refugees fled to Djibouti. Between June and December 1977, when Somali troops invaded the Ethiopian Ogaden, some 10 000-20 000 refugees crossed into Djibouti, camping mainly in Djibouti City, Dikhil and Tadjoura.
On his return from the second Nairobi coordination meeting in September 1977, the representative of Djibouti, Dr A. A. Warsama, began work aimed at strengthening the local vaccination programme as well as surveillance for the detection of imported cases of smallpox. In November-December 1977, Dr Nicole Grasset visited Djibouti to work with the programme in conducting a special search for smallpox among the refugees. Dr Jean- Paul Ryst assisted the programme from September 1978 to October 1979 and Dr Arnaud Trebucq between May and December 1979.
The 1977 vaccination campaign reached 94 289 persons in Djibouti City, out of an estimated total population of 150 000. In December 1977, a vaccination scar survey of 1517 persons found 90% or more with scars in each age group.
Active search operations
Active search operations were planned in November 1977. The smallpox eradication programme activities were widely publicized, in particular the reward of 5000 Djibouti francs (US$28) which would be given to anyone reporting a case of smallpox. An appeal from the President of the Republic to the population to collaborate actively with the programme and announcing the reward was published in the local press and read over the radio in Afar, Somali, Arabic and French. Any cases of fever with rash found during the search were to be reported to the supervisor or the Chief of the Department of Hygiene and Epidemiology on the same day. Refugees were vaccinated if they did not have a vaccination scar.
Full coverage of this small country was achieved in the course of 2 search operations, the first between December 1977 and January 1978 and the second between February and April 1978. In the second search, 20 chickenpox cases were found but no case of smallpox. Altogether 142 specimens were collected during 1978 and 1979 and tested by WHO collaborating centres; none contained variola virus.
Plate 27.5. Members of the preliminary international commission that visited Ethiopia in April 1979 listening to the report being made by their chairman (Dr J.. Kostrzewski) and rapporteur (Dr K. R. Dumbell) to Wogayehu Sahlu, permanent secretary of the Ministry of Health, Ethiopia. Left to right, front row: Taddesse Alemu (Ethiopia), Fekade Tsegaye (Ethiopia), L. N. Khodakevich (WHO), Wogayehu Sahlu (Ethiopia), T. Olakowski (WHO); middle Row: N. A. Ward (United Kingdom), R. N. Basu (India), Z.M. Dlamini (Swaziland), H. B. Lundbeck (Sweden), C. do Amaral (WHO); back row: O. S. Ismail (WHO), Haile Miriam Kahssay (Ethiopia), A.I. Gromyko (WHO), Unidentified participant, Assefa Gobeze (Ethiopia).
Smallpox Surveillance among Muslim Pilgrims from the Horn of Africa
The pilgrimage season, during which over a million Muslims from about 40 countries visit the holy towns of Mecca and Medina, occurs in November-December. Even before the season starts, the number of international travellers to Saudi Arabia increases.
In 1977, the Saudi Arabian health authorities set up smallpox surveillance centres in Jeddah, Medina, Mecca, Mona and Arafat. A circular was sent to all medical groups concerned with the health problems of the pilgrims, indicating that any suspected case of smallpox should be promptly reported and investigated.
The Saudi Arabian health service checked all pilgrims on their arrival at ports of entry to ascertain whether they had an appropriate certificate of smallpox vaccination. Pilgrims from Djibouti, Ethiopia, Kenya and Somalia were examined to see whether they had vaccination scars. Pilgrims from Ethiopia and Somalia also had to submit particulars of their itinerary, intended address, the name of their guide, the name of the regions from which they came and whether they knew of any smallpox cases in their villages during the previous 3 months. Somali pilgrims were all vaccinated on arrival, regardless of their vaccination history, and the Somali government sent smallpox surveillance teams to accompany the Somali pilgrims during their trip, to deal promptly with an outbreak should it occur. Foreign medical missions collaborated fully in these surveillance activities, making regular inquiries about cases of fever with rash. Saudi Arabian medical officers at Jeddah, Mecca and Medina visited Ethiopian and Somali camps at least twice a week. No case of smallpox was found. A total of 22 specimens collected from patients suffering from fever with rash were all negative. These activities were supervised by Dr Ehsan Shafa from the Smallpox Eradication unit, who worked in Saudi Arabia between 3 November and 9 December 1977.
CERTIFICATION OF SMALLPOX ERADICATION IN THE HORN OF AFRICA
Since endemic smallpox had persisted in the Horn of Africa for many months after it had been eradicated from all other parts of the world, the certification of smallpox eradication in the countries concerned had important implications in terms of vaccination requirements throughout the world. The Smallpox Eradication unit therefore went to considerable trouble to organize certification activities and, believing that the last endemic countries could be certified by the commissions, prepared to publicize the event. Arrangements were made for all 4 countries to be visited simultaneously in October 1979 by separate international commissions, which would then meet in Nairobi to discuss their respective findings and announce the certification of smallpox eradication for the Horn of Africa as a whole on 26 October 1979, exactly 2 years after the recognition in Somalia of the world’s last case of endemic smallpox. Arrangements were made in advance with representatives of the world media in order to ensure public recognition of the global eradication of smallpox.
By September 1979 each of the 4 countries concerned had prepared a comprehensive report on its national eradication programme and precertification activities. These reports were submitted in advance to the members of the respective international commissions before their visits. In order to coordinate arrangements, the chairmen of the 4 international commissions met at WHO Headquarters in Geneva and discussed the strategy of their activities in each country and at the combined meeting in Nairobi. Prior to this, however, preliminary visits were made to Ethiopia.
Preliminary Visits to Ethiopia
Two preliminary visits to Ethiopia by some Commission members were arranged, from 31 May to 15 June 1978 and from 3 to 18 April 1979, because Ethiopian certification involved some areas that were not fully under government control, and many high-priority areas were situated in regions in which travel was extremely difficult. The first visit, by Dr Keith Dumbell and Dr P. N. Shrestha, led to a joint decision by the Ethiopian government and WHO to carry out a single thorough search, instead of a multiplicity of searches, which were always incomplete and in fact beyond the capacity of the programme staff available.
In the second visit in April 1979, 7 commission members, of whom only Dr Jan Kostrzewski (chairman) and Dr Dumbell (rapporteur) also served on the final Ethiopian International Commission in October (see Chapter 24, Annex 24.1), went to Ethiopia. The group visited all the regions and 70 of the 102 awrajas, mainly in the highland areas, so that in October 1979 the final visit by the International Commission would be able to concentrate on critical areas in the Ogaden (Fig. 27.14).
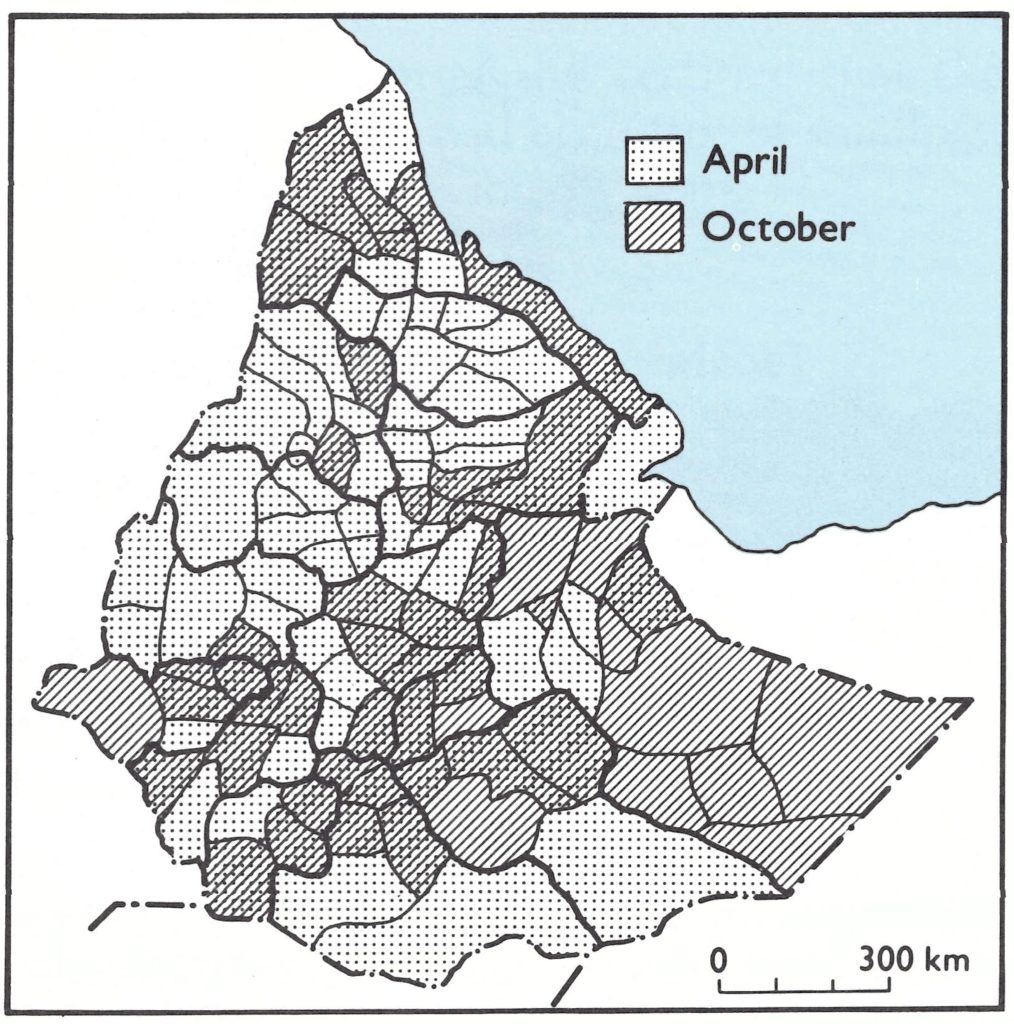
Fig. 27.14. Ethiopia: Awrajas viwas sited by the members of the International Commission for the Certification of Smallpox Eradication in Ethiopia on a preliminary visit 5-16 April, on the final visit by the Commission 4-14 October 1979, and on both occasions.
Visits by the International Commissions
Separate international commissions visited the individual countries of the Horn of Africa during the first 3 weeks of October 1979, as follows:
| Country | Date | Commission Chairman |
|---|---|---|
| Djibouti | 9-18 October 1979 | Dr R. Netter |
| Ethiopia | 1-17 October 1979 | Dr J. Kostrzewski |
| Kenya | 1-19 October 1979 | Dr R. N. Basu |
| Somalia | 1-21 October 1979 | Dr H. Lundbeck |
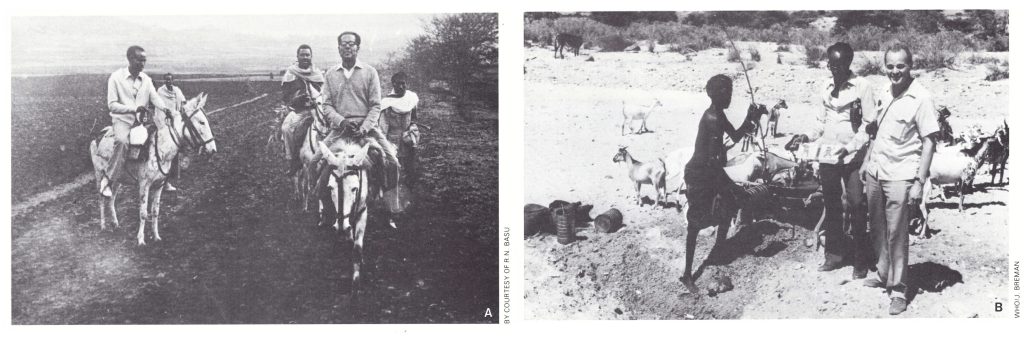
Plate 27.6. Field visits by members of international commissions. A: R. N. Basu, a member of the preliminary international commission which visited Ethiopia in April 1979, riding by mule between villages in a remote part of the country. B: R. Netter, chairman of the international commission in Djibouti, on a field visit.
The 20 members of the 4 international commissions travelled extensively in their respective countries. In Ethiopia, because of the difficult terrain, a fixed-wing aircraft and helicopters were placed at the disposal of commission members, who used them to travel extensively throughout the country and to visit areas not accessible by overland travel. Since variola minor had been prevalent in these areas, the commissions paid special attention to the laboratory investigation of 6671 specimens collected from cases of fever with rash in the 4 countries during 1978 and 1979; all proved to be negative for smallpox (Table 27.5).
In each country, the commission members were satisfied with the data presented on past surveillance activities and certified that the country concerned had been free of smallpox for at least the previous 2 years.
Table 27.5: Horn of Africa: numbers of specimens tested by WHO collaborating centres during 1978 and 1979a
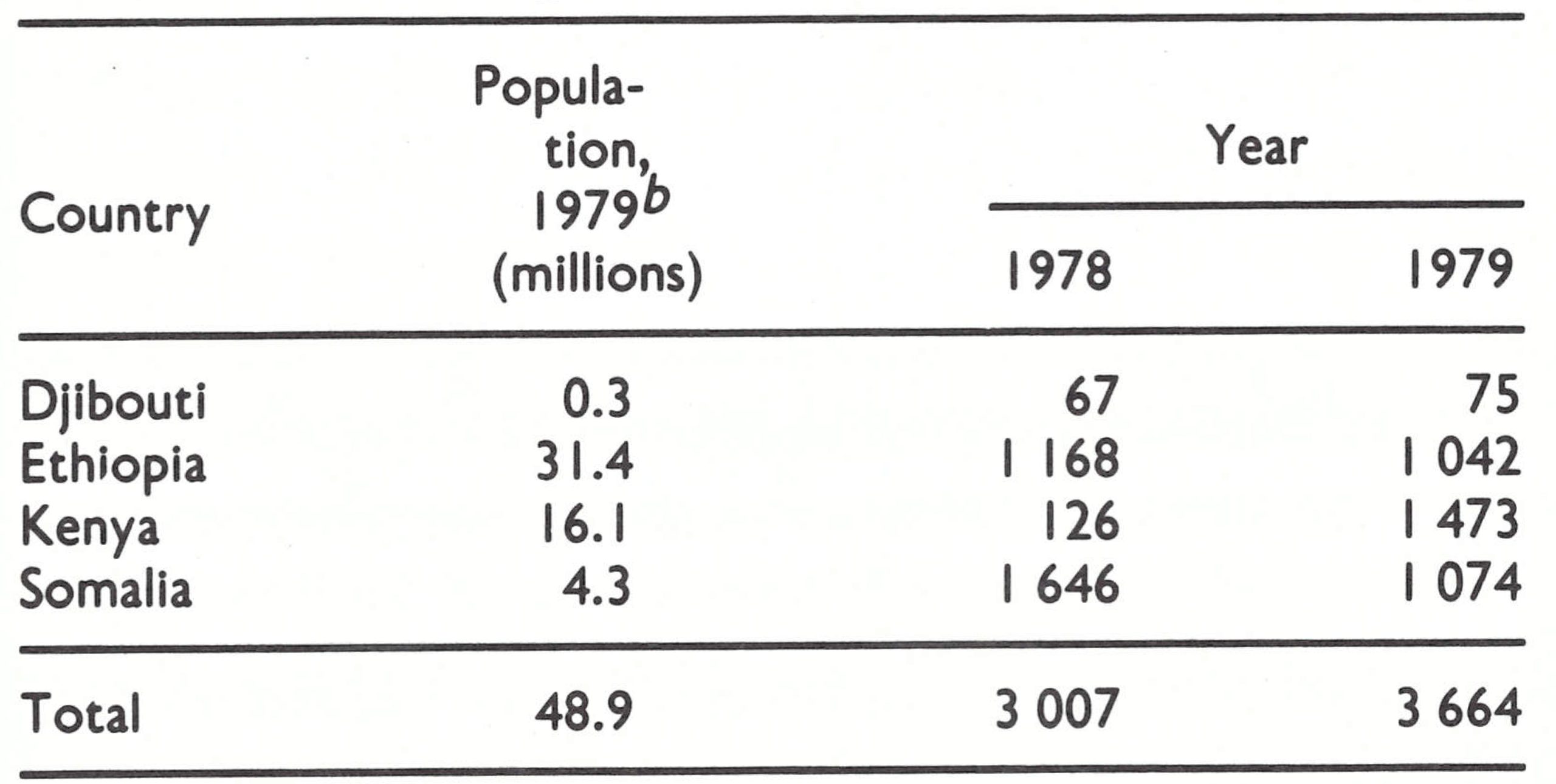 a All were negative for variola virus.
a All were negative for variola virus.
b Population data from United Nations (1985).
Plate 27.7. International Commission for the Certification of Smallpox Eradication in Somalia with programme staff, October 1979. Left to right, front row: V. Zikmund (WHO), B. Kr’ii (WHO), A. Deria (Somalia), Z. Jezek (WHO), F. Partow (WHO), T.J. Geffen (United Kingdom), P.N. Shrestha (Nepal), M. Rabile Good (Somalia), H.B. Lundbeck (Sweden),). M. Aashi (Saudi Arabia), Z.M. Dlamini (Swaziland), J.D. Millar (USA), 1. Arita (WHO), Z. Ali Henry (Somalia); middle row: A. L. Khattab (WHO), D. Shire (Somalia), M. A. Gure (Somalia), M. T.A. Gaafar (Egypt), M.N. El Naggar (WHO), M. Adan Abdulle (Somalia), 1 .0. Awad (Somalia), A. A. Beira (Somalia), M. S. Mohamed (Somalia). W. Hardjotanojo (WHO), M. A. Jama (Somalia). back row: R. J. Hatfield (WHO), A. A. Farah (Somalia), A. S. Hassan (Somalia), A.M. Ahmed (Somalia), M. Yusuf (Somalia), H. Alaso (Somalia), J.M. Jussuf (Somalia). The names of the Commission members are in bold type.
Joint Meeting in Nairobi
After the certification of the individual countries had been completed, all members of the 4 international commissions and a number of others involved in the smallpox eradication programme, including 12 members of the Global Commission, some of whom had not been members of the international commissions, met in Nairobi, where the chairmen of the 4 commissions presented their respective reports. Having agreed that endemic smallpox no longer occurred in the Horn of Africa, and taking into consideration the recommendations presented in the reports of the 4 commissions, the joint meeting made the following recommendations:
- Smallpox vaccination should be terminated throughout Djibouti, Ethiopia, Kenya and Somalia.
- Vaccination certificates for smallpox should no longer be required of any travellers coming to, or leaving, the 4 countries.
- Experience from previously certified countries indicated that smallpox rumours would continue to occur even after certification. All such rumours were to be reported promptly to national authorities and thoroughly investigated by competent personnel, and the findings transmitted to WHO, so as to minimize unnecessary national and international concern. Specimens should be collected if necessary and sent through WHO, Geneva, to the WHO collaborating centres.
On 26 October 1979 a conference organized by the Smallpox Eradication unit was held in the Kenyatta Hall, Nairobi, in the presence of the Director-General of WHO, Dr Halfdan Mahler, the Regional Director for Africa, Dr Comlan A. A. Quenum, and the Regional Director for the Eastern Mediterranean, Dr Abdul H. Taba. Dr Kostrzewski, as the chairman of the joint meeting of the individual commissions, reported to Dr Mahler the commissions’ conclusion that smallpox had been eradicated in the Horn of Africa. Immediately after this meeting, Dr Mahler sent the following message by cable or telex to all Member States and to international organizations:
“The Director-General of the World Health Organization presents his compliments and has the honour to…inform you that International Commission today certified smallpox eradication in Horn of Africa which was last stronghold of disease Stop I personally believe smallpox has now been eradicated throughout world and am confident that Global Commission for Certification of Smallpox Eradication will confirm this in December 1979 Stop I shall then present final report to World Health Assembly in May 1980 Stop World Health Organization has accomplished this mission with support and participation of all Member States”
On the same date, 26 October 1979, in the Weekly epidemiological record, health officials throughout the world were informed of the successful certification of smallpox eradication in the Horn of Africa (Plate 27.8).
The certification of the Horn of Africa meant that all countries in Africa had been certified. However, neither the Global Commission nor WHO was yet able to make a definitive statement on global eradication, since smallpox eradication in China had not yet been certified.
Plate 27.8. Cover of the Weekly Epidemiological Record for 26 October 1979, the day on which certification of the Horn of Africa was completed in Nairobi. The illustration shows Ali Maow Maalin, who was diagnosed as having variola minor on 26 October 1977 and was the last case in the world of endemic smallpox.
CERTIFICATION OF SMALLPOX ERADICATION IN CHINA
After the Second World War, civil war broke out in the Republic of China. In October 1949, after the defeat of the Kuo- mintang government, the government of the People’s Republic of China was established and controlled the whole of mainland China. However, the Kuomintang government, which controlled only Taiwan, was until 1971 recognized by the United Nations as having the right to represent the entire country. Obviously, the Kuomintang government was unable to provide WHO with data about smallpox on the mainland. WHO was there- fore not in a position to receive information on mainland China until 1972, when it followed the policy of the United Nations and recognized the government of the People’s Republic of China as the only government having the right to represent China.
Lack of Information on Smallpox Eradication
Although mainland China was in theory accessible to WHO representatives from 1972 onwards, for several years it was very difficult to obtain information on health matters. From the outset of the global eradication programme, the Organization was understandably concerned about the smallpox situation in the most populous country in the world. Discussions in Geneva with Dr Chang Wei-hsun, an Assistant Director-General of WHO, who was a paediatrician from Beijing, elicited the information that he had not seen a case of smallpox since 1957 and was unaware of cases anywhere in China after about 1960.
In the absence of better ways of obtaining information, two other approaches were adopted. Whenever possible, Henderson and Arita met individuals or delegations planning to visit China and told them that the Smallpox Eradication unit wished to obtain more definite information about smallpox in China. They were asked to look for facial pockmarks wherever they went and to estimate the age of any person with such pockmarks. About 15 reports were received on facial pockmarks seen in China, but without exception the persons concerned were adults—no pockmarked children were seen.
Another approach was to examine refugees from China after they had crossed the border into Hong Kong and Nepal. Arita visited Hong Kong in 1970 to request the local authorities to conduct a pockmark survey. However, although the Hong Kong health authorities originally agreed to do so, they subsequently declined, feeling that it was a politically sensitive matter. In 1975, Dr P. N. Shrestha, director of the national smallpox eradication programme in Nepal, conducted pockmark surveys among Tibetan refugees in that country, and found that 43 out of 2350 of them (1.8%) had facial pockmarks. Although they could not remember exactly when they had had smallpox, none of these people recollected that it had been contracted later than 1961 and none was less than 14 years old in 1975. The results suggested that smallpox had been eradicated in Tibet early in the 1960s.
The Consultation on the Worldwide Certification of Smallpox Eradication, held in October 1977, devoted some time to discussing the smallpox situation in China. It considered that, although according to the information available it seemed unlikely that smallpox was still endemic there, China’s vast size and population—one-quarter of the world’s total—justified a more detailed study. For this purpose, the Commission recommended that during 1978 China should be visited by an international commission, WHO consultants or WHO staff, to verify and document its history of smallpox eradication. This was eventually achieved in July 1979.
The problem was one of effective communications. Chinese officials, on the one hand, felt that additional documentation and a visit by Commission members were unnecessary, as transmission had been interrupted many years earlier; the Commission, on the other hand, believed that the available documentation from China was not sufficient to convince the world community of the reality of this achievement.
Because of the difficulty of obtaining the requisite information, China was (with Democratic Kampuchea, see Chapter 26) the last country to be certified by the Global Commission as being free of endemic smallpox, on 9 December 1979.
Development of Effective Contacts with China
Initial efforts, 1973-1976
At the Twenty-sixth World Health Assembly, in May 1973, the delegate from China reported that smallpox eradication had been achieved in practice by 1959 through a country-wide vaccination campaign initiated following Liberation (World Health Organization, 1973b). Extensive use had been made of part-time vaccinators and health auxiliaries in order to cover remote areas adequately. Once vaccination of the population had been completed, smallpox control had been integrated into the general health services and everyone was routinely vaccinated and revaccinated every 6 years . This had been reinforced by the recent growth of health cooperatives and the “barefoot doctor” system. No other details were given. Information on the health system in China began to emerge with the WHO study visits in 1973 and 1974, but none of these provided any specific details about smallpox, nor was there any assurance that importations from endemic neighbours to the south (Bhutan, India and Nepal) would be quickly detected and contained.
1977: Increasing urgency of better contacts
In January 1977 WHO was still no better informed about the eradication of smallpox in China and was beginning to consider seriously how to approach the problem of certification. A representative of China was invited to serve on the International Commission for the Certification of Smallpox Eradication in Bangladesh and Burma in November-December 1977, in the expectation that the Chinese authorities might be interested in determining whether China’s southern neighbours were free of smallpox. However, an invitation sent in May 1977 was declined on the grounds of “busy working arrangements”. A separate invitation to participate in the October 1977 Consultation on Worldwide Certification was also refused, despite the personal attention of Dr Ch’en Wen-chieh, the Chinese Assistant Director-General of WHO who had succeeded Dr Chang Wei-hsun.
Following a request from the Smallpox Eradication unit, the WHO Regional Office for the Western Pacific cabled Beijing on 26 September 1977 and requested a brief summary statement covering the date of the last case, ongoing surveillance activities, vaccination policy and information on laboratory stocks of variola virus. The reply sent on 24 October 1977 was, if anything, briefer than the statement made by the Chinese delegation at the World Health Assembly in 1973, except that the information was given that variola virus was being held by specific institutions designated by the government. The reaction of the Chinese seemed to be one of indifference to the opinion of the rest of the world. They seemed to feel that no one need doubt their word that smallpox had been eliminated from China many years earlier.
Predictably, the Consultation in October 1977 recommended that WHO should obtain more information from China and that a visit should be arranged for a group which would include members of the Global Commission.
1978: Further informal contacts
On 4 January 1978, a letter was sent from the Regional Office for the Western Pacific proposing that 3 international experts and 3 WHO medical officers should visit China for 3 weeks during July-August 1978, and pointing out that “smallpox eradication in China appears to have been uniquely successful in terms of the vast geographical areas and methods employed. Detailed information on these activities would be of considerable value when worldwide eradication is reported to all Member States of WHO at the World Health Assembly”…In order to make the proposal more readily acceptable a list of 6 experts and 5 WHO epidemiologists was attached to the letter, to enable the Chinese government to make a choice.
On 28 February 1978, following the adoption by the Executive Board of a resolution requesting the Director-General to establish the Global Commission for the Certification of Smallpox Eradication, the Chinese government was invited to nominate a member of the Commission. In their reply of 29 April, the Chinese authorities again declined to become involved in the certification process. At the same time a brief reply was received to the letter of 4 January from the Regional Office for the Western Pacific reiterating what had been stated previously concerning smallpox and adding:
“It is based on the principle of responsibility for the health of the Chinese people and the people of the world and on the conscientious and careful conclusion reached after long years of thorough investigation and scientific surveillance that the Chinese Government has declared smallpox eradicated. As to the proposed visit to China by a group including members of the Global Commission with a purpose to ‘certify’ whether or not China has really achieved smallpox eradication
It was obvious that more effective communications were required between China and WHO on the philosophy of the certification programme. During the Thirty-first World Health Assembly, in May 1978, informal discussions were held between Dr Hsueh Kung-cho and other members of the Chinese delegation and WHO officials, including Arita, Chief of the Smallpox Eradication unit, at which it was agreed that the proposed visit should be postponed and that China would prepare a country report for the Global Commission before any further steps were taken. There followed a prolonged series of informal contacts aimed at convincing the Chinese authorities that the requests by WHO for more information and the invitations to participate in the certification commissions did not imply that WHO doubted their word that smallpox eradication had been achieved, but rather that it was a matter of compiling formal documentation which would convince health authorities all over the world so that it would be possible to discontinue smallpox vaccination everywhere.
Informal approaches were made during the visits to China by Dr William Foege, Director of the Center for Disease Control, Atlanta, USA, in June 1978 and by Mr Paul Lawton, Division of Coordination, WHO, in October 1978. No concrete results were obtained, but the impression was gained that the Chinese authorities were becoming more open and responsive.
Time Schedules for Certification
"Dr Hsueh Kung-cho first explained the smallpox situation in China. In 1950, special regulations to deal with the smallpox problem were set up and an eradication programme started. In 1959 the last case was recorded and to date there have been no further smallpox cases detected. Notably during the last ten years, national health programmes have been further strengthened, establishing close communication at province, country and town levels.
"I [Arita] explained the following points: Although I personally believed that smallpox had been eradicated in China, data to support this achievement were not sufficient. In the context of certification activities for global smallpox eradication, there are still a considerable number of health personnel as well as the press community who express uncertainty regarding smallpox in China. It is most desirable therefore for China to show their achievement to the world.
"In reply to this, Dr Hsueh Kung-cho indicated that a country report on surveillance activities for smallpox eradication would be prepared by China and submitted to WHO and all other necessary action required would be further reviewed when this report was prepared. In the circumstances, it was agreed that the initial proposal from WHO for Global Commission members to visit China during July-August 1978 should be postponed.
"The timing of the certification activities was discussed. The first Global Commission meeting would take place in December 1978 and the final meeting was expected to take place in October or November 1979, so that preparation of the report had to be started as soon as possible. It was agreed that the Smallpox Eradication unit would submit items to be included for special documentation during the next few days."
On 27 November 1978 WHO received a 2-page document entitled A General Introduction on the Eradication of Smallpox in the People’s Republic of China, from Dr Chiang Yi-chen, Minister of Public Health. The only new information was that the last case had occurred in March 1960 in Yunnan Province and that variola virus was held by the National Institute for the Control of Drugs and Biological Products in Beijing.
During the meeting of the Global Commission in December 1978, Arita organized a special subcommittee to discuss this report and future plans for the certification of China, the participants being Fenner, Chairman of the Global Commission; Dr Foege, who had recently visited China; Henderson, former Chief of the Smallpox Eradication unit; Dr Kostrzewski, who had been Chairman of the International Commission for the Certification of Smallpox Eradication in India; and Dr Shrestha, who had organized the pockmark survey of Tibetan refugees in Nepal. The unanimous opinion of the sub-committee was that it was highly likely that smallpox had been eradicated in China, in view of the structure of the health and social services in the country, but that evidence was lacking; that high-level negotiations between China and WHO or influential WHO Member States on behalf of WHO would be required to obtain data; and that technically the minimum data requirement would include the results of surveys for facial pockmarks and vaccinations scars on a province-by-province basis. Dr Kostrzewski stressed the desirability of oral negotiations at the stage that had been reached; continued written requests might be perceived as intimidating. The subcommittee drafted a statement which was approved by the plenary meeting of the Global Commission and included in the Commission’s report for 1978:
“Considering the extensive health service network in China and its capability for effective surveillance, the Commission expressed confidence that smallpox transmission had been interrupted. However, it was believed that more substantial documentation would be of considerable importance to provide persuasive evidence of this fact to the world community. A more complete country report should be sought with information presented, if possible, on a province-by-province basis. Useful information would include documentation of the last cases, an account of past smallpox activities in individual provinces and current epidemiological surveillance activities indicating how suspected cases would be detected. Certification of freedom from smallpox was deferred pending receipt of additional information.”
During 1978, the Global Commission certified a number of countries, including Namibia, Southern Rhodesia (Zimbabwe), and Thailand, but deferred certification of China, Democratic Kampuchea, Iraq, Madagascar and South Africa because of insufficient evidence.

Plate 27.9. The WHO team of J. Breman and F. Fenner, in Kunming, Yunnan Province, China, with Fu Guichen, Jiang Yutu, Jiang Weizhang and Zuo Kejia. Jiang Yutu accompanied the WHO team; the other Chinese were health officials of Yunnan Province.
The Improvement of Health Services in China
Immediately after the Liberation, one of the first acts of Mao Zedong's government was to eliminate smallpox from China by mass vaccination campaigns. This was achieved by enlisting community support and using all available health personnel for intensive vaccination campaigns (see Chapter 8). Later, routine vaccination was incorporated into primary health care. Although there had been undeniable improvements since 1949, in the early 1960s health services were still not being provided to many of the 85% of the population living in the rural areas. Mao Zedong's directive of 26 June 1965 prescribed that, in health and medical work, the stress should be put on the rural areas. The changes made were: (1) the establishment of mobile medical teams formed out of existing health manpower to work in the rural areas; (2) the discontinuation of formal medical education pending its complete reform; (3) the genuine unification of traditional and western medicine; and (4) the massive training of "barefoot doctors" and health auxiliaries for the delivery of health services to the rural population.
The Ministry of Health was reorganized and responsibility for the delivery of health services delegated to the provincial, regional or municipal level. At the same time, five-sixths of the state bureaucracy in Peking was disbanded. As a consequence of this radical decentralization, emphasis was given to the rural areas and by 1974 satisfactory coverage of the entire population had been achieved. This, however, also had the result that there was little or no epidemiological information on a country-wide basis at national level. On the other hand, comprehensive information was available at provincial and commune level.
Awareness of the need to report communicable diseases was highly developed and coverage in terms of surveillance very extensive, as even in production teams—the basic units of community organization—one person was made responsible for disease notification.
1979: A visit by a WHO team is arranged
The next initiative in what had become rather delicate negotiations was undertaken, at WHO’s request, by Sir Gustav Nossal, Chairman of the WHO Western Pacific Advisory Committee for Medical Research, who visited China in April 1979. He engaged in informal discussions to find out under what conditions the Chinese would accept a visit by Fenner (a fellow Australian who was Chairman of the Global Commission), accompanied by a WHO staff member. The response was encouraging. He detected a positive and flexible attitude on the part of the Chinese, who showed far less sensitivity to the issue than he had expected. The proposed visit appeared to be welcome. During the Thirty-second World Health Assembly, in May 1979, information was provided informally to the effect that the Chinese would agree to a visit by Fenner in July.
Visit of the WHO team to China
The result of these protracted negotiations was that a WHO team consisting of Fenner and Dr Joel Breman, of the Smallpox Eradication unit, visited China from 14 to 30 July 1979. They found that a country report had already been prepared by Professor Jiang Yutu, Professor Li Heming and Dr Zhao Kai, three scientists who had participated in a meeting of officials from laboratories retain- ing variola virus and the national control authorities concerned, which had been held in Geneva from 23 to 24 April 1979. As others had predicted, once discussions had been established on a person-to-person basis, matters went very smoothly. The WHO team reviewed the report with the authorities as well as a special detailed report on the last outbreaks in Yunnan Province. This report also included the results of a vaccination scar and pockmark survey of 73 820 persons in the border areas of Yunnan carried out in March-May 1979. Their only real concern at the time was that, while there was comprehensive information concerning the last cases reported from Yunnan in 1960, cases had also been reported in Xizang Autonomous Region (Tibet) in 1960, about which there were no details. It was impracticable for the WHO team to visit Xizang, but the Chinese authorities promised to carry out investigations comparable to those described for Yunnan.
The WHO team, accompanied by Dr Jiang Yutu, examined the communicable disease surveillance system in three areas: Beijing municipality, Shanghai municipality and Yunnan Province, from which the last endemic case in China has been reported in 1961 (Fig. 27.15). In all areas, visits were made to provincial, municipal and district epidemic prevention sections, commune hospitals, health centres, and village primary schools. The team was impressed by the detailed records available at provincial and municipal level about smallpox outbreaks and vaccination campaigns which had been conducted well over 20 years previously. Fenner and Dr Breman felt confident that the system for the surveillance of communicable diseases operating in the country would have detected outbreaks of smallpox if they had occurred after 1960.
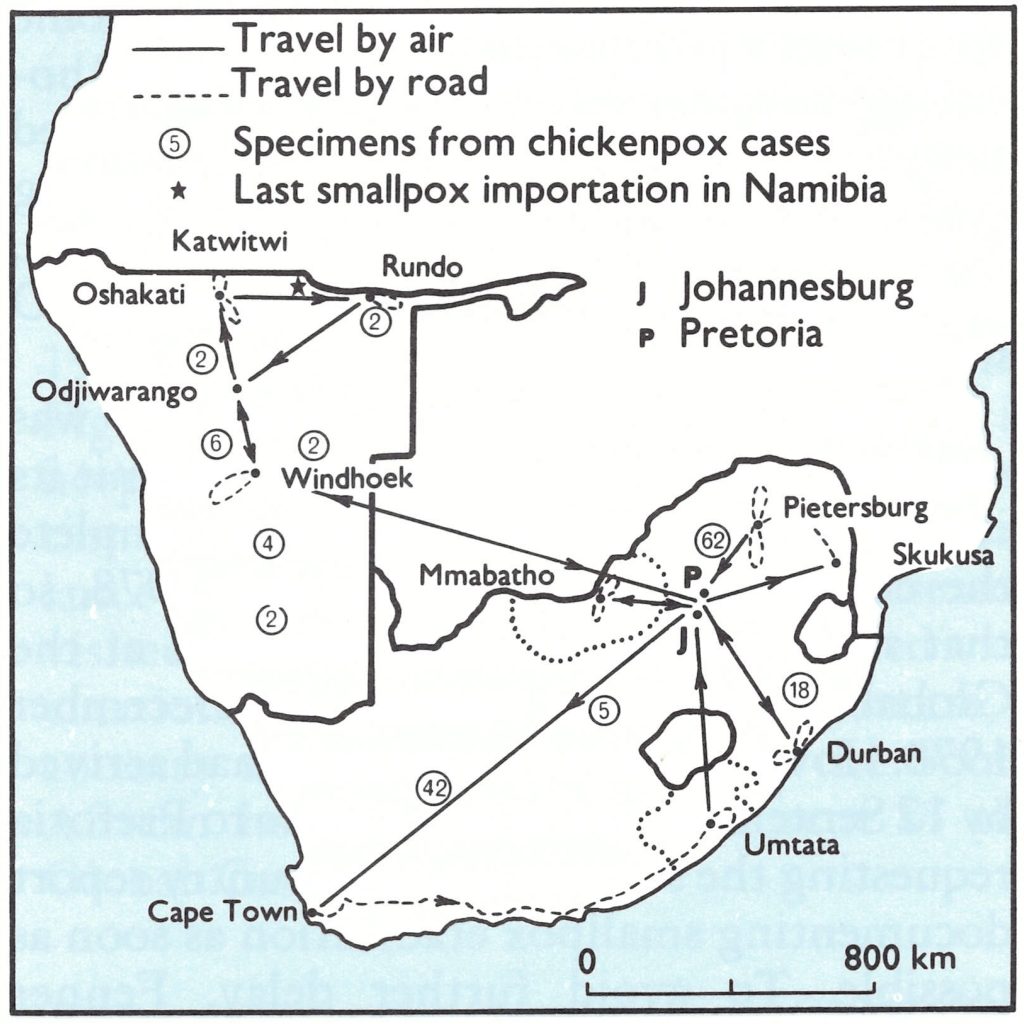
Fig. 27.15. China and neighbouring countries, in relation to certification activities, showing travel by the WHO team in July 1979 and the areas for which special reports were prepared (Provinces of Yunnan and Taiwan; Xizang Autonomous Region [Tibet]). Places where the last cases of endemic smallpox were reported in Xizang in 1960 and in Yunnan in 1961, the site of imported cases in Xizang in 1962 and 1964, and the locations of outbreaks following variolation in northern Yunnan in 1958 and in Nei Monggol Autonomous Region and Shanxi Province in 1962-1965 are also shown.
It was also agreed that 2 representatives from China would participate in the December meeting of the Global Commission in 1979, one of whom would be a member of the Global Commission and the other an epidemiologist familiar with the details of the eradication of smallpox in China.
The WHO team’s visit as well as communications between China and WHO resulted in several documents becoming available on smallpox eradication in China, containing a great deal of data completely unknown to WHO and to the world scientific community before 1978 (WHO/SE/79.142 Rev.1; WHO/SE/79.151; SME/79.10; SME/79.11, Fenner & Breman). Subsequently, Xu & Jiang (1981) described the elimination of smallpox from Shanghai, and Jiang Yutu published an account of smallpox in China in a Chinese medical encyclopaedia (Jiang, 1985). The description of the eradication of smallpox in China given in Chapter 8 is based on the relevant information in these reports. Threematters of particular importance for the certification programme are described below : smallpox in Yunnan Province and in Xizang Autonomous Region (Tibet), and the location of laboratory stocks of variola virus. Also included in the present chapter is an account of outbreaks of smallpox in northern China in 1962-1965, which did not come to the attention of WHO until the 1980s. The data are shown in Table 27.6.
Table 27.6: Horn of Africa: numbers of specimens tested by WHO collaborating centres during 1978 and 1979a
 a Data for all provinces, autonomous regions and municipalities over the period 1950-1965 are shown In Chapter 8, Table 8 .13. No cases were reported after 1956 in the administrative units not listed. No cases were reported anywhere in China after 1965.
a Data for all provinces, autonomous regions and municipalities over the period 1950-1965 are shown In Chapter 8, Table 8 .13. No cases were reported after 1956 in the administrative units not listed. No cases were reported anywhere in China after 1965.
b Associated with variolation.
c Importations from Nepal.
Smallpox in Yunnan Province
Yunnan, with a population of about 30 million, is situated in south-western China and borders on Burma, the Lao People’s Democratic Republic and Viet Nam (Fig. 27.16). Although the reported incidence of smallpox had been reduced to zero throughout most of China by the late 1950s (see Chapter 8, Table 8.13), cases continued to occur in Yunnan until 1961 (Table 27.7). Scattered cases were reported from counties in many parts of Yunnan up to 1959, but after that year 5 out of the 6 outbreaks reported occurred in counties adjacent to Burma (Fig. 27.16). The villages in these counties were inhabited by ethnic minorities having strong ties with Burma and there was frequent communication with villages across the border. At the time, communications between these areas and Kunming, the provincial capital, were very poor, and elements of the Kuomintang, by preventing adequate vaccination coverage, had increased the difficulty of eliminating smallpox. Up to 1960, smallpox outbreaks repeatedly occurred on the Burmese side of the border and the disease then passed over into China as the inhabitants carried it across. For example, in 73 of the 461 cases (16%) reported in 1959 from Cangyuan county, the disease had been contracted in Burma. It was estimated that at this time between 30% and 60% of the villagers on the Chinese side of the border were vaccinated. After a delayed but intensive vaccination campaign in Cangyuan and neighbouring counties in 1959, which was said to have reached 98.8% of the population, the out-breaks subsided. Seven cases were reported from 3 counties in 1960 and 28 cases in 1961, 5 from Lancang county, 21 from Monghai county, and finally 2 from Monglian county—the last endemic cases in China.
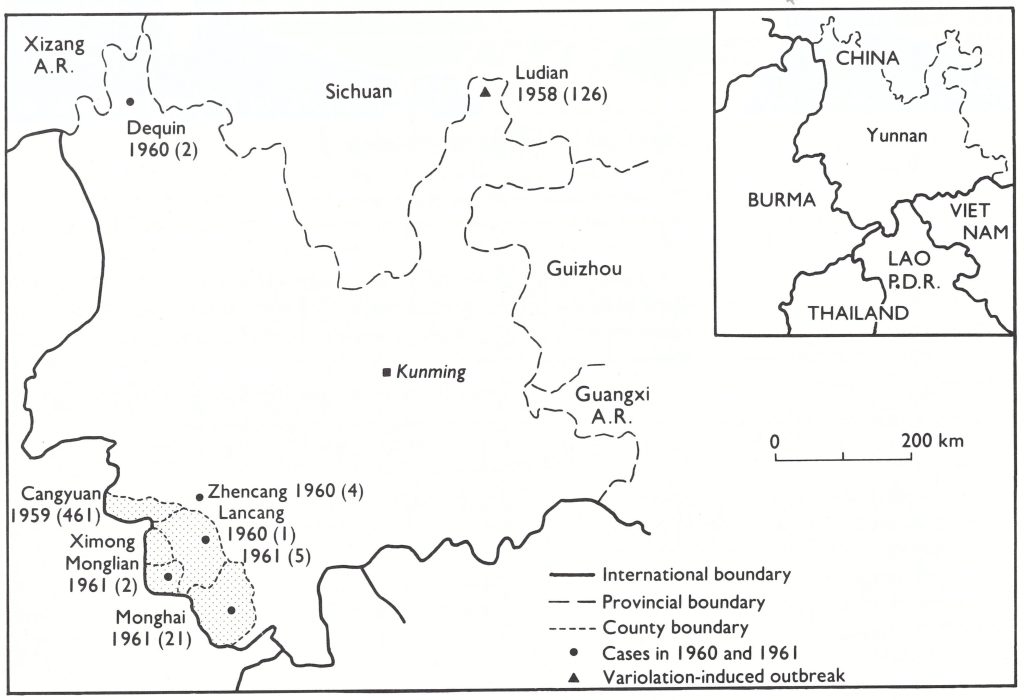
Fig. 27.16. Yunnan Province, showing sites of smallpox outbreaks in 1960-1961 and counties near the Burmese border where vaccination scar and facial pockmark surveys were conducted in 1979. An outbreak of 461 cases occurred in Cangyuan county in 1959 and a variolation-induced outbreak of 126 cases occurred in Ludian county in northern Yunnan in 1958. Numbers next to locations indicate the year in which the number of cases (in parentheses) occurred.
Table 27.7: Yunnan Province: numbers of reported cases of smallpox, 1958-1962, by countya
 a Data from Dr Jiang Yutu (personal communication, 1985).
a Data from Dr Jiang Yutu (personal communication, 1985).
b Outbreak caused by variolation given by nasal Insufflation.
c The last cases of endemic smallpox In China.
In the border districts in which the last smallpox outbreaks had occurred, vaccination scar and pockmark surveys were conducted in March-May 1979, in preparation for the visit to Kunming by the WHO team. The overall vaccination rate among 44 771 persons examined in the rural districts was 90.4%, compared with 94.0% for Kunming municipality (Table 27.8). In both areas, the rate was also satisfactory for the age group 0-4 years. The overall frequency of pockmarks in persons in these districts was 6.0%, compared with 0.3 in Kunming municipality (Table 27.9), but the age distribution (Table 27.10) revealed that in Monglian county, in which, as has already been mentioned, the last reported cases occurred in 1961, no person under 22 years of age had facial pockmarks, nor were any pockmarked persons under 20 found elsewhere in Yunnan.
The evidence provided to the Global Commission showed that endemic smallpox had persisted in these remote border areas of Yunnan for several years after it had been eliminated from the rest of China (except Xizang Autonomous Region ; see below). However, the pockmark and vaccination scar surveys conducted in 1979 in the counties in which smallpox was last endemic provided reassurance that transmission had been interrupted in the early 1960s and that no further outbreaks had occurred.
Table 27.9: Yunnan Province: results of facial pockmark survey in counties near the border with Burma, and Kunming municipality, March-May 1979
 a Cangyuan, Monghai, Monglian and Ximong counties.
a Cangyuan, Monghai, Monglian and Ximong counties.
b Kunming municipality.
Table 27.9: Yunnan Province: results of facial pockmark survey in counties near the border with Burma, and Kunming municipality, March-May 1979

Table 27.10: Yunnan Province: age distribution of 1020 pockmarked persons, May 1979
 a None of whom had had smallpox after 1960
a None of whom had had smallpox after 1960
Smallpox in Xizang Autonomous Region (Tibet)
Xizang Autonomous Region (Fig. 27.17) is separated from the neighbouring countries of Bhutan, India and Nepal by the Himalayan mountain chain. Its 1.8 million inhabitants are spread over 1.2 million square kilometres, giving a population density of only 1.5 per square kilometre. Xizang therefore appears to have been a rather unfavourable place for maintaining smallpox transmission, although it was periodically subject to epidemics of great severity. In all, 23 cases were reported in 1955 and 4 in 1956, followed by 16 in 1960. This led to a request from the WHO team for a special report, which was forwarded to WHO in November 1979. No further details of the cases in 1960 were available except that 5 of them occurred in Changdu subregion and 11 in Lhasa subregion.
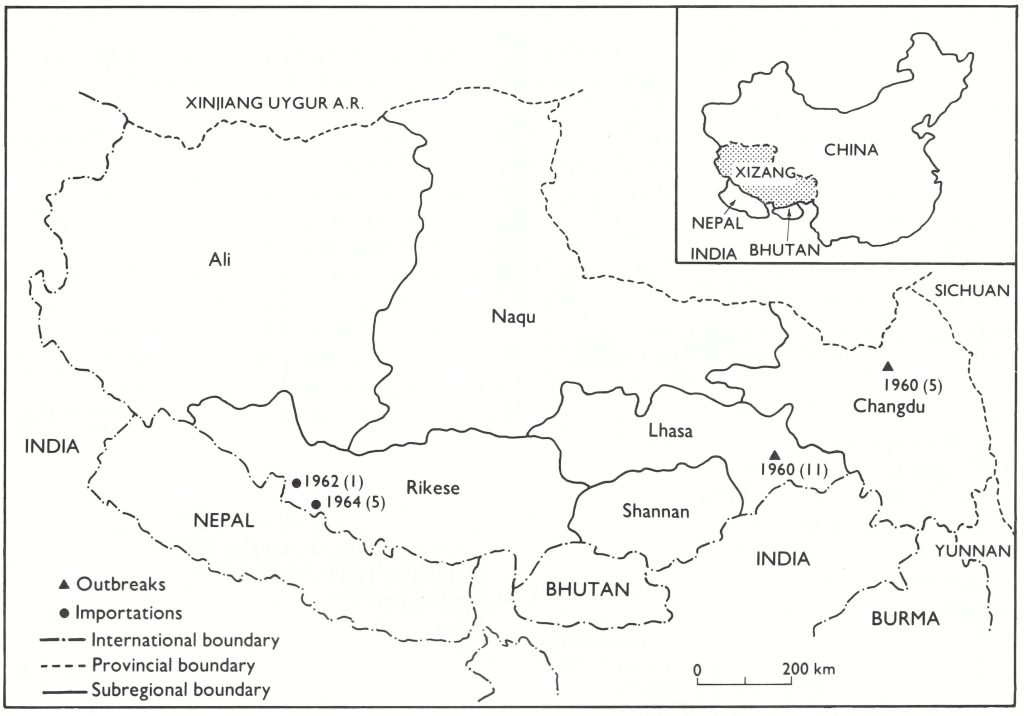
Fig. 27.17. Xizang Autonomous Region (Tibet), showing subregional, provincial and international boundaries, and the sites where the last endemic cases occurred in 1960: 5 cases in Changdu county (Changdu subregion) and II cases in Linzki county (Lhasa subregion) . There was I case in 1962 and 5 cases in 1964 in Nielamu county (Rikese subregion), associated with importations from Nepal. Numbers next to locations indicate the year in which the number of cases (in parentheses) occurred.
The special report provided details of subsequent vaccination coverage, information on suspected cases of smallpox, and the results of vaccination scar and facial pockmark surveys conducted in August 1979. Between 1960 and 1979, 39 cases of suspected smallpox were investigated in the 3 years 1963, 1965 and 1970. All turned out to be cases of chickenpox. At the time of the Global Commission meeting, the Chinese authorities reported rumours of 4 importations from Nepal into Xizang in the early 1960s, with 1 secondary case. Subsequently Dr Jiang Yutu (personal communications, 1984, 1985) confirmed that, following importations from Nepal, 1 case had occurred in Nielamu county (Rikeze subregion) in 1962 and 5 cases in 1964.
In addition to routine vaccination, for which freeze-dried vaccine was used from 1965 onwards, mass vaccination campaigns were carried out in 1964 and 1975 to increase the immunity level of the population in areas bordering on India and Nepal. Limited data showed that the take rate in persons undergoing primary vaccination varied between 86% and 95%.
The vaccination scar and facial pockmark surveys in August 1979 covered 15 661 persons in Shannan and Rikeze subregions and Lhasa City (Table 27.11). Vaccination rates were high (91%) among those over 4 years of age but only 57.5% in those below that age. No persons with facial pockmarks were found in Shannan subregion but about 1 % of over 12 000 persons examined in Lhasa City and Rikeze subregion, all of them over the age of 20 years, were pockmarked. This evidence reinforced the data from the pock- mark survey on Tibetan refugees provided to WHO earlier.
Table 27.11: Xizang Autonomous Region (Tibet):a age-specific vaccination scar and facial pockmark rates, August 1979
a Shannan and Rikeze subregions and Lhasa City.
Province of Taiwan
In 1972, WHO decided to follow the United Nations in recognizing the Beijing government as representing China, consider- ing Taiwan as one of its provinces and referring to the island as “China (Province of Taiwan)”.
Unlike mainland China, Taiwan had been an active member of WHO from 1948, when the Organization was established, until 1972, when it was excluded following the above- mentioned decision. In 1978, Taiwan had a population of 17.9 million (7.5 million in 1950) and a comprehensive health services infrastructure. The last big epidemic of smallpox had occurred in 1946-1947: 6754 cases with 2040 deaths. Mass vaccination campaigns with the annual primary vaccination of infants and vaccination of the entire population eliminated endemic smallpox in 1954, after which no cases had been found. The country report, endorsed by the Director-General of Health Services, together with a signed “Declaration of Smallpox free Status”, was judged to be satisfactory by the Global Commission on 8 December 1978, but for purposes of formal certification Taiwan could, of course, only be considered together with China as a whole.
Variolation in China after 1950
Variolation, initially by insufflation and later by scarification, had been practised in China since about the 10th century (see Chapter 6), and was practised almost as widely as vaccination during the early years of the 20th century. It continued to be used for over a decade after the Liberation in remote rural areas that were at the time served almost exclusively by practitioners of traditional medicine. The Global Commission was told of an outbreak of 126 cases in 1958 in Ludian county in the north-east corner of Yunnan Province (see Fig. 27.16) which followed variolation by nasal insufflation, 5 years after the last case of endemic smallpox in that county but only a year after the last outbreaks in other counties in northern Yunnan. Some years after the last meeting of the Global Commission, information was provided by Dr Jiang Yutu (1985; and personal communications, 1984, 1987) about other variolation-induced outbreaks in northern China in the mid-1960s (Fig. 27.18), in Nei Monggol Autonomous Region (1 case in 1962, 255 cases in 1963 and 30 cases in 1964) and 2 nearby counties of Shanxi Province (28 cases in 1963 and 4 in 1965).
Fig. 27.18. Sites of the outbreaks in northern China, 1962-1965, following variolation. Figures beneath place names indicate the year of the outbreak and the number of cases (in parentheses). (From Jiang Yutu, 1985; and personal communications, 1984, 1987.)
These incidents have been explained by Dr Jiang Yutu (personal communications, 1984, 1987) as follows. Throughout the whole of continental China between 1959 and 1962, almost everything, including smallpox vaccine, was in short supply. In 1963, just after the country had recovered from this situation, people demanded that their children should be vaccinated but supplies of potent vaccine were not sufficient to ensure the coverage of all areas, especially the mountainous and remote ones. In Nei Monggol and Shanxi, as a result, the inhabitants turned to their local traditional doctors, some of whom had been variolators, maintaining virus in sealed jars containing honey. After smallpox had disappeared from their region in the 1950s (see Chapter 8, Table 8.13), they had continued to maintain the viability of the virus by the annual inocula- tion of their own children. Thus, when supplies of vaccine failed in the early 1960s, these variolators still had active variola virus, and with the cessation of vaccination many more children became susceptible and many more were inoculated with the virus. The outbreaks which then occurred were investigated by Dr Zhao Kai, of the National Vaccine and Serum Institute, Beijing, who recovered variola virus both from cases and from the variolation material. Stringent measures were taken to eliminate the practice and supplies of potent freeze-dried vaccine were provided to remove any need for recourse to variolation. As has been pointed out earlier, a massive reorganization of the health services in China in 1965 greatly improved the quality of health care in the rural areas. No cases of smallpox occurred after 1965, either in these areas or elsewhere in China.
Variola Virus Stocks
Inquiries made by the Chinese Ministry of Health in 1961-1962, 1966 and again in 1978 established that the only variola virus stocks held in laboratories were located in the National Institute for the Control of Biological Products in Beijing. The virus had last been used in 1967, as a positive control during laboratory investigations of material from a suspected case of smallpox. The WHO team noted
“The laboratory does not conform to WHO standards for facilities storing variola virus. As a depository only, the physical and administrative arrangements seem adequate for the particular situation, but the building housing the virus stocks, and the cabinet itself, would not offer maximum security against a determined saboteur.”
In January 1981 these stocks were destroyed by the Chinese government .
Review by the Global Commission
WHO’s efforts to collect additional information on smallpox in China had eventually resulted in a visit of a team of experts to the country in July 1979 and the accumulation of substantial data that lent support to the view that smallpox had been eradicated. However, there was little time left for review and assessment of these data by the Global Com- mission, since the target date for global certification was the end of 1979. On 21 August 1979, Arita wrote to members of the Global Commission and submitted to them all the data then available: the country report by the Ministry of Health (WHO/SE/79.142 Rev.1); a provincial report by the Health Department of Yunnan Province, in which the last endemic case had occurred (SME/79.10); a report on the visit to China by Fenner and Breman (SME/79.11); and a report on smallpox eradication in Taiwan Province. Information on Xizang (Tibet) and vaccine production arrangements did not become available to WHO until November 1979. In the letter, Arita noted that the WHO team believed, from the evidence that it had been able to collect on its visit, that smallpox had been eliminated from China, and specifically requested an answer to the following 3 questions
- Do you think that the Global Commission should now approve certification of smallpox eradication in China?; or
- Do you as an individual member of the Global Commission approve certification of smallpox eradication in China, but feel that its final eradication should not be declared until all the Commission members meet again from 6 to 9 December 1979? ; or
- Do you have any other comments or recommendations which do not fall into the above two categories?
The response of the members of the Global Commission was equivocal; 8 advocated immediate certification, 5 wished to discuss it at the December meeting, and 6 did not reply. Dr Holger Lundbeck, a Commission member from Sweden, expressed a widely held view by saying that, while he had no doubt that smallpox transmission had been interrupted long ago in China, in order to convince the world community, more information should be sought about Xizang for “there will always be people who doubt that eradication has been achieved, in particular in countries as big as China”.
Consideration of the certification of smallpox eradication in China was therefore deferred until the meeting of the Global Commission in Geneva in December 1979, which was attended by Dr Zhang Yi-hao from China as a member and Dr Jiang Yutu as an adviser. In addition to the reports previously circulated, 2 further reports were then available: (1) Supplementary Report about the Eradication of Smallpox in China, sent to WHO on 17 November 1979 by the Minister of Public Health, Dr Qian Xinzhong, which provided information on the production of smallpox vaccine, the health service structure, and the quarantine services ; and (2) a report
(WHO/SE/79/151) which included details of vaccination campaigns and coverage in Xizang, the last outbreaks there, and the results of a pockmark survey carried out in August 1979, which has already been described. Having considered all the data and heard reports from Dr Zhang Yi-hao and Dr Jiang Yutu, the Commission certified China to be free of smallpox on 9 December 1979.
Plate 27.10. Members of the Global Commission for the Certification of Smallpox Eradication, 9 December 1979. From left to right, front row: S. S. Marennikova (USSR), J. Azurin (Philippines), P.N. Burgasov (USSR), F. Fenner (Australia; Chairman), J. Kostrzewski (Poland; Vice-Chairman), D. A. Henderson (USA), W. Koinange (Kenya), Zhang Yihao (China); back row: P. F. Wehrle (USA; Rapporteur), R. N. Basu (India), J .M. Aashi (Saudi Arabia), H. B Lundbeck (Sweden), B. A . Rodrigues (Brazil), K. R . Dumbell (United Kingdom), R. Netter (France), I. Tagaya (Japan), J. S. Moeti (Botswana), Kalisa Ruti (Zaire), P. N. Shrestha (Nepal), A. Deria (Somalia).
CONCLUSIONS
In every health programme, success depends not only on the scientific technology but also on the managerial arrangements and political negotiations which pave the way for its implementation. The certification activities in the Horn of Africa and China illustrate how scientific technology and managerial and political arrangements were developed in parallel in order to accomplish a single task.
With the certification of the Horn of Africa and China, the chapter on the certification of the global eradication of smallpox, which had commenced in 1971 when Brazil recorded the last case on the South American continent, was closed. Activities had been greatly intensified since 1976 when it became apparent that global eradication was imminent. Four years of effort, from 1976 to 1979, had been successful in confirming that the world had become free of smallpox. This was the first time in history that human efforts had succeeded in eliminating a disease—and one which had been feared for thousands of years. Neither the vigorous operational campaign for the eradication of the disease nor the diligent certification programme was free from technical and human errors. Nevertheless, both were eventually successful.
The Global Commission met in Geneva from 6 to 9 December 1979. It had before it a draft final report which had already been reviewed and revised by 12 members of the Commission in Nairobi in October. The meeting concentrated its attention on the conclusions and recommendations (World Health Organization, 1980). After 4 days of intensive discussions, it accepted the following conclusions :
- Smallpox eradication had been achieved throughout the world.
- There was no evidence that smallpox would return as an endemic disease.
The 19 recommendations covered all aspects of operations relevant to Ortho poxviruses and the diseases that they cause in a world from which smallpox had been eradicated. The meeting closed on 9 December 1979 with a ceremony in which the members of the Global Commission signed a parchment declaring that the world was free of smallpox (see frontispiece).
The final report of the Global Commission, The Global Eradication of Smallpox (World Health Organization, 1980), was published in the 6 official languages of the World Health Organization and its conclusions and recommendations were accepted without change by the Thirty-third World Health Assembly on 8 May 1980.
Albertobleft
July 10, 2025Getting it status, like a merciful being would should So, how does Tencent’s AI benchmark work? Exceptional, an AI is foreordained a basic enterprise from a catalogue of closed 1,800 challenges, from hieroglyph materials visualisations and web apps to making interactive mini-games. Post-haste the AI generates the rules, ArtifactsBench gets to work. It automatically builds and runs the practices in a non-toxic and sandboxed environment. To devote to how the tenacity behaves, it captures a series of screenshots upwards time. This allows it to corroboration against things like animations, species changes after a button click, and other thought-provoking consumer feedback. In the end result, it hands atop of all this blurt into the open air – the by birth importune, the AI’s cryptogram, and the screenshots – to a Multimodal LLM (MLLM), to bill as a judge. This MLLM encounter isn’t no more than giving a inexplicit философема and a substitute alternatively uses a presumptive, per-task checklist to borders the show up to pass across ten lug ahead of a rescind metrics. Scoring includes functionality, psychedelic experiment appreciate affair, and the unvarying aesthetic quality. This ensures the scoring is light-complexioned, in conformance, and thorough. The efficacious subject is, does this automated beak in actuality caricature ownership of parentage taste? The results barrister it does. When the rankings from ArtifactsBench were compared to WebDev Arena, the gold-standard upholder procession where becoming humans философема on the excellent AI creations, they matched up with a 94.4% consistency. This is a monstrosity confined from older automated benchmarks, which not managed in all directions from 69.4% consistency. On bung of this, the framework’s judgments showed across 90% concord with gifted fallible developers. [url=https://www.artificialintelligence-news.com/]https://www.artificialintelligence-news.com/[/url]
Ernestbindy
August 16, 2025Bilinçli kumar oynamak , riskleri güvenceye alır . Zaman sınırlarınızı net tanımlamak , sorunları önlemeye katkı sağlar . Katılımınızı yönetim araçlarını kullanmak, kontrolü sağlamınıza destek olur . Alev Casino TR Oyunların etkilerinin farkında olmak, dengeli katılım mümkün kılar. Erken aşamada profesyonel destek danışmak, keyfi çözmeye yardımcı olur . Bu adımlar , eğlenceli dengeli bahis süreci keyfini maksimize eder.
RobertTeels
August 23, 2025Goods delivery from China is reliable and swift. Our company delivers flexible solutions for enterprises of any size. We manage all shipping processes to make your operations smooth. air express shipping from china With regular shipments, we guarantee timely arrival of your orders. Clients appreciate our professional team and competitive rates. Choosing us means assurance in every order.
RobertTeels
August 24, 2025Goods delivery from China is reliable and efficient. Our company offers flexible solutions for businesses of any scale. We take care of all transportation processes to make your workflow seamless. air shipping from china With direct shipments, we ensure timely delivery of your packages. Clients value our skilled team and reasonable rates. Choosing us means assurance in every shipment.
EdgarGlink
August 31, 2025В Telegram появилась функция звёзд. Теперь участники могут выделять важные чаты. Это помогает быстро находить нужную заметку. купить звезды дешево бот Функция комфортна для ежедневного общения. Благодаря этому легко зафиксировать ключевые моменты. Такой инструмент экономит нервы и делает общение проще.
RogerDuets
September 29, 2025Индивидуалки — это уникальные личности, которые отстаивают свою свободу. Они предпочитают к осознанному подходу в общении. Такие девушки обычно обладают независимым характером и четкими жизненными целями. Они смело демонстрировать свои мысли. https://spaxam.net/ Общение с ними нередко получается насыщенным. Они любят слышать собеседника и строить искренние отношения. Такие девушки вдохновляют окружающих своей аутентичностью. Они идут своим курсом, не подстраиваясь под сторонние ожидания.
RogerDuets
September 30, 2025Девушки-индивидуалки — это неповторимые личности, которые отстаивают свою свободу. Они склоняются к осознанному подходу в жизни. Такие девушки нередко обладают уверенным характером и сформированными жизненными ценностями. Они открыто демонстрировать свои убеждения. https://lugansk.spaxam.net/ Взаимодействие с ними нередко получается глубоким. Они способны слушать собеседника и строить искренние отношения. Такие девушки мотивируют окружающих своей неповторимостью. Они следуют своим путем, не подстраиваясь под внешние ожидания.
MichaelSpisa
October 5, 2025Новейшее медоборудование играет ключевую функцию в лечении и помощи пациентов. Клиники всё чаще используют передовую системы. Это позволяет специалистам делать точные заключения. Современные приборы гарантируют надёжность и для пациентов, и для врачей. http://www.oraerp.com/thread-421-post-302955.html#pid302955 Использование высоких технологий помогает результативное оздоровление. Большинство устройства содержат опции для детального наблюдения состояния здоровья. Врачи могут оперативно действовать, основываясь на данных аппаратуры. Таким образом, новейшее техническое оснащение усиливает уровень здравоохранения.
Floydcop
November 13, 2025This online platform offers a lot of interesting and valuable information. On this platform, you can discover various materials that expand knowledge. Readers will enjoy the resources shared here. Every category is organized clearly, making it comfortable to use. The content are relevant and engaging. You can find tips on various fields. If you want to find useful facts, this site has something for everyone. All in all, this website is a reliable place for curious minds. https://companysites.info/