Chapter 31:
Lessons and benefits

INTRODUCTION
Smallpox is the first disease to have been eradicated by concerted and determined action on a global scale. This was not achieved, however, until more than 175 years after Edward Jenner’s demonstration of the use of cowpox as a vaccine and his assertion that it was capable of eliminating smallpox from the earth. The vaccine virus had been promptly and widely distributed in the world, and vaccination was eagerly taken up as a protection against a universally feared disease. However, smallpox continued to spread as sustained control efforts were beyond the capacity of many government and health structures and vaccinations were frequently unsuccessful, especially in warm climates. Through the nineteenth century and the early part of the twentieth, tens of millions of persons were affected, of whom one-fifth or more died; no country was entirely spared. A heat-stable vaccine perfected in the 1920s helped to increase the efficacy of vaccination in the tropics, but it was difficult to produce and was not widely used.
As health systems improved and more extensive vaccination could be undertaken, the industrialized countries became free of endemic smallpox by the 1950s but frequent introductions of the disease from less fortunate countries obliged them to maintain costly national vaccination programmes and to endeavour, not wholly successfully, to protect themselves by compelling all travellers to be vaccinated. In most developing countries, few people were successfully vaccinated and smallpox was essentially uncontrolled.
A change in the approach to smallpox control was proposed in 1958 at the Eleventh World Health Assembly by a delegate of the USSR, who advocated that all countries should collaborate in a global eradication programme. This was unanimously approved by the Health Assembly the following year. At the time, 60% of the world’s population lived in areas in which smallpox was endemic.
The next 7 years saw some improvement in the quality of vaccine and some countries did become free of smallpox, but the disease continued to be widely prevalent and epidemics were frequent.
In 1966, the government delegates to the Nineteenth World Health Assembly decided that increased resources were required and allocated special funds for the Intensified Smallpox Eradication Programme that was to begin on 1 January 1967. They proposed a goal of 10 years for the achievement of eradication. This was an optimistic goal, given that some 10-15 million cases were then occurring annually in 31 endemic countries or territories with a total population of more than 1000 million; that a century and a half of vaccination had yielded only modest results; that programmes would have to be conducted in most of the world’s least developed countries ;and that civil strife, famine and floods could be expected as recurring problems. Nevertheless, the last endemic case of smallpox occurred just 10 years, 9 months and 26 days after this programme began.
The rapidity with which smallpox was finally eradicated after so long a history of persistent transmission suggests that lessons may be derived from the experience of the Intensified Programme to benefit other initiatives in health and development. Most significant is the extraordinary achievement which was possible when countries throughout the world collaborated in the pursuit of a common aim, making use of the structures of an international organization and acting under its auspices. This made it possible for the necessary resources to be mobilized and applied to better effect, for improved methods of management and epidemiology to be introduced and widely applied, for vital modifications in strategy to be communicated quickly, and for new and often very simple techniques suited to a country’s capacities and characteristics to be introduced promptly. In consequence, international confidence and accord were strengthened and a foundation was laid for other community-wide health programmes.
The smallpox eradication programme, however, cannot serve as a template for other disease control or eradication campaigns. Every disease has its own epidemiological characteristics and methods for its control which require strategies and tactics specific to it. Also, the approach taken to the eradication of smallpox differed considerably from country to country and was continually modified to capitalize on an evolving understanding of smallpox epidemiology and to deal with different local conditions. It is important also to note that smallpox had a number of features which greatly facilitated eradication. Most important is the fact that its severity and ability to spread in any part of the world commanded both the attention and the concern of health authorities everywhere. It had no known animal reservoir; there were no long-term carriers of the virus; and a single attack of the disease conferred essentially life-long immunity. The detection of cases was comparatively simple because the rash was so characteristic and persons with subclinical infections did not transmit the disease. Finally, a highly effective, easily administered and surprisingly heat-stable vaccine, conferring long-term protection, was available by the time the Intensified Programme started. Taken together, these characteristics are unique in relation to human infections. Indeed, when the goal of eradication from all countries of the world was decided upon, its feasibility in most of the industrialized countries and some of the developing ones had already been demonstrated.
The earliest successes of the Intensified Programme were recorded in western and central Africa, where it was quickly shown that smallpox spread less rapidly and less easily than most people had thought and that the prompt detection and immediate containment of outbreaks were vitally important- facts that were to have a profound influence elsewhere. Although the 21 countries concerned included some of the world’s poorest and most heavily infected, 17 of them became free of smallpox within 2 years of the start of the programme in January 1967 and the last cases were discovered in June 1970. In Brazil, too, surprisingly rapid progress was made and endemic smallpox was eradicated from the Western Hemisphere in April 1971.
The provision of adequate supplies of potent freeze-dried vaccine and the introduc- tion of the simple bifurcated needle had a remarkable impact on the incidence of smallpox in most countries, even those in which it was not possible to mount fully satisfactory programmes. This was especially notable in eastern and southern Africa where, by the end of 1971, smallpox had been eliminated from all but 3 countries. Meanwhile, well-executed programmes, in which the detection and containment of outbreaks were an important feature, stopped transmission in East Pakistan (now Bangladesh) in 1970 and in Indonesia and Afghanistan in 1972.

Plate 31.1. The Headquarters of the World Health Organization in Geneva, Switzerland.
Plate 31.2. First-day cover issued by the United Nations, commemorates the global eradication of smallpox. Variola virus virions as they appear under the electron microscope are shown on the stamps. A replica of the Winged Victory of Samothrace (on the left of the envelope) was presented to WHO when it received the Albert J. Lasker Special Award for Public Service from the Albert and Mary Lasker Foundation in recognition of the role the Organization played in eradicating smallpox.
Serious setbacks to the global programme occurred or were first confirmed in 1972. That year Bangladesh became reinfected with the return of vast numbers of refugees immediately after the civil war that had led to its independence; Botswana was swept by an epidemic as a result of introductions of the disease from South Africa; and it became known with certainty that Iran had become endemic in 1970 and Iraq in 1971. By late 1973, however, special campaigns had succeeded in eliminating smallpox from all the reinfected countries except Bangladesh.
In September 1973, greatly intensified campaigns began in the 5 remaining endemic countries: 4 in Asia (Bangladesh, India, Nepal and Pakistan) and 1 in Africa (Ethiopia). In the densely populated areas of Asia, new methods and extra resources were required to cope with smallpox among people who moved much about their country and among the large groups of persons displaced by natural disasters or civil strife. The employment of tens of thousands of health staff in ingeniously devised, well-supervised search and containment programmes made it possible to stop transmission in Pakistan in 1974 and in the other 3 countries in 1975.
Late in 1975, personnel and additional resources were shifted to Ethiopia, then the only country in which smallpox remained endemic. There, the milder form, variola minor, spread tenaciously across a vast and sparsely settled area in which civil strife was widespread and there were few roads or health services. Using many local volunteers and helicopters in yet another type of campaign, the smallpox eradication staff contained the last outbreak, in the Ogaden desert, in August 1976. However, civil war and the exodus of many refugees brought about a reintroduction of the disease into Somalia. Experienced staff and resources from many countries were mobilized to deal with this emergency, and the world’s last naturally occurring outbreak took place on 26 October 1977.
Endemic smallpox had been eradicated but the health authorities of the world had to be completely confident of this fact if they were to forego the security—and the expense—of vaccination. Close surveillance and special searches had therefore to be conducted in many countries for at least 2 years after the last known case had occurred before international commissions appointed by WHO could be asked independently to verify the absence of smallpox. Finally, a WHO Global Commission undertook a variety of studies to satisfy itself that eradication had been achieved throughout the world, its conclusions being endorsed by the Thirty-third World Health Assembly in May 1980.
No two national eradication programmes were exactly alike, and all changed as they evolved, different elements and approaches contributing to the ultimate success. In this chapter, we try to identify the most important principles and lessons which appear to have a bearing on other community—wide health activities. Many of the conclusions are shared by other authors (Dutta et al .,1975; Foster, 1977; Sharma, 1980; Yekutiel, 1981; Hopkins, 1985; Jarrett, 1985), but differences are also apparent as each author has approached the question with a different experience and from a different point of view. Finally, we attempt the difficult task of assessing the costs and the benefits of the eradication of smallpox.
Plate 31.3. Dr Karan Singh, the Indian Minister of Health and Family Planning, presented the World Health Organization with this bronze statue of Nataraj on 15 August 1975, celebrating at once India’s Independence Day and her freedom from smallpox. The statue is now in the Executive Board lounge at WHO Headquarters
PRINCIPLES AND LESSONS
Political Commitment, Coordination and Implementation
For a worldwide programme against a disease to be successfully undertaken, all countries must agree to it and there must be a mechanism for coordinating and monitoring the work. The World Health Assembly provides the necessary and, indeed, the only forum in which global health policies can be agreed upon; and the World Health Organization alone has the requisite channels of communication with the national authorities through which their several programmes can be coordinated, with the support of the international scientific expertise upon which the Organization can draw. Both the Health Assembly and the World Health Organization were essential to the success of smallpox eradication.
The policy decision by the Twelfth World Health Assembly (1959) to undertake the global eradication of smallpox represented an important first step. Through the 1950s, most national governments and colonial administrations had conducted smallpox control programmes, some of which were very effective. If any disease were to be eradicated by such a widespread although uncoordinated effort, smallpox was the most likely one, given the threat it posed to all countries and the availability of an effective vaccine. However, the interest of national authorities in smallpox control waxed and waned with the varying incidence of the disease and as they became temporarily free of it or, on the contrary, were reinfected from abroad. A concerted and sustained initiative, supported by one or more bilateral assistance agencies, might have succeeded in eliminating smallpox from many countries but it is unlikely that it could have achieved world-wide eradication. Moreover, a scheme to certify that eradication had been accomplished would have carried little conviction without the credit and authority of an international agency which could mobilize respected scientists from throughout the world.
Some countries were encouraged by the decision in 1959 to begin or to intensify their own special programmes and some bilateral support was found, but 3 factors compromised the effort. The first was that the World Health Assembly did not back up its decision by the allocation of special funds, and WHO provided very few staff to coordinate or assist the national efforts and very few funds to help their work. In the majority of countries little action was taken and eradication was assigned a low degree of priority. Second was the fact that in Brazil, South Africa and some countries of eastern Africa, the prevalent form of smallpox was variola minor, which caused only mild illness and few deaths and therefore ranked low among the many other health problems. The third factor was that several large countries were not then Members of WHO. For them, the resolution of the Health Assembly had no direct bearing on their national policies and few of them provided information about the incidence of smallpox or the nature of their activities to control it.
The allocation by the Nineteenth World Health Assembly (1966) of special funds for smallpox eradication signalled a change in priorities. It served to stimulate national commitment to the idea of eradication and encouraged the backing of bilateral assistance agencies; it permitted the recruitment of additional WHO staff; and it provided additional resources for national programmes. The annual allocation of US$2.4 million was not large when compared to the overall need, and minuscule compared to the amounts being expended for the prevention of smallpox in the industrialized countries, but it was an important stimulus without which eradication could not have been achieved.
National support for global smallpox eradication, expressed as unanimous approval of the programme in the World Health Assembly, did not quickly take the form of effective national action, often owing to inertia though sometimes for lack of resources. WHO could not compel a Member State to meet the responsibilities to which it had pledged itself, but by the exercise of moral suasion it was eventually able to overcome reluctance on the part of national authorities. This required WHO staff to play an active role in advocating that eradication programmes should be started and sometimes meant a direct approach to heads of state or other senior national figures when officials at lower levels failed to respond. This encouragement of national programmes and the subsequent support of their work would not have been possible without a technical staff in WHO of sufficient size. From 1959 through 1966, there were at most 1 WHO medical officer in WHO Headquarters and 4 or 5 with field projects who were engaged specifically in smallpox eradication—too few, and with insufficient funds at their disposal, to have any significant impact. In theory, the WHO representatives who were resident in most countries in which smallpox was endemic might have stimulated the development of eradication programmes, but each was responsible for coordinating all the WHO supported activities in a country and served as a technical resource for other health projects. Few had any particular experience of smallpox eradication or the time to devote to it. As additional funds became available, the number of WHO smallpox eradication programme staff the world over increased to 50 in 1967 and eventually to more than 100. Their professional expertise was to prove essential.
At first, many senior WHO and national staff had believed that management skills only were required. The needs, as they perceived them, were simple and straightforward: to procure sufficient vaccine and to organize vaccination programmes. They believed that generalist managers, rather than epidemiologists or other specialists, were sufficient for this task. It was apparent from the beginning, however, that the challenge was far greater than the straightforward application of vaccine. It was necessary to adapt vaccination programmes to different administrative, socio-cultural and geographical situations and to devise mechanisms to monitor and assess the work, in terms not only of the numbers of vaccinations performed but but also of their effect on the incidence of smallpox. A better understanding of smallpox epidemiology was required in order to refine the strategies and tactics. Better methods for vaccine production were needed, as were improved instruments for vaccination. It was also important to determine with certainty that there was no natural reservoir of smallpox and to demonstrate that the clinically similar and virologically related disease, human monkeypox, was not a serious threat to the programme. Complementing the staff of physicians was a cadre of non-medical staff, termed “operations officers”, who proved to be invaluable in dealing imaginatively with the complex logistics of programme implementation. This network of professional WHO staff, although small in number compared to the tens of thousands of national staff, facilitated the rapid communication of new information throughout the world and assisted in adapting and applying it to national programmes.
In summary, the commitment of the World Health Assembly to a programme of global smallpox eradication provided encouragement to national health authorities to undertake programmes in their countries, an encouragement strengthened by the demonstration in previous years and in a number of developing countries that eradication was practically feasible. However, more was required than good intent and expectation. Meaningful levels of national and international support were essential, as well as mechanisms to harmonize the many different ideas and plans of multilateral, bilateral and national organizations.
The Importance of a Special Programme
Smallpox eradication was conducted through a specifically targeted and time-limited special programme with funds allotted specially for it both in the WHO budget and in most national budgets, and with full-time technical staff assigned responsibility for its supervision. In this respect it may be regarded as the type of categorical programme the conduct of which remains a contentious issue of health policy, especially in developing countries (Vittachi, 1985). Yet, it made important contributions to the development of health services because, far from being separately or autonomously administered, it worked with and through the existing national health service structures and had to coordinate its activities with those of other programmes. The basic health services network, for in- stance, constituted the foundation of the disease-reporting structure, and in all countries this had to be greatly improved by training and supervision in order to become effective and to provide quickly the accurate information on which the containment of smallpox depended. Immunization programmes were strengthened in many countries as smallpox eradication teams undertook to provide other vaccines, such as BCG, measles, yellow fever and DPT, and assisted with the transport of personnel and supplies for other programmes. Some participation of the existing health staff in vaccination and in search and containment activities was required everywhere because of the small numbers engaged full-time in smallpox eradication. In consequence, many thousands of health staff received training in the execution of vaccination programmes and in field epidemiology; in many cases the only field supervision they received was provided in the course of their smallpox eradication work . A substantial number who now occupy senior positions in national and international organizations are successfully applying methods used for smallpox eradication in programmes against other diseases. These methods include the use of surveillance systems for management and assessment, sample survey techniques to measure performance, and the use of disease-recognition cards to help in case detection.
Experience in the programme demonstrates 3 principles of importance to health policy decisions: (1) the provision of disease control services which reach all persons in the community requires strategies and systems of management for which traditional health care delivery systems are ill-equipped; (2) special programmes to deal with health problems of general concern offer the advantage of attracting both resources and community support; and (3) the significant improvement in efficiency and supervision that can often be realized in special programmes may well offset the additional costs they sometimes entail.
The delivery of community-wide services
Health officials in most countries have recognized that traditional health care systems-comprising a network of medical practitioners, health centres, and hospitals-have been designed fundamentally to provide therapeutic services for those who seek help and are ill-equipped to deliver preventive and other services which must reach all or most persons in a community. The limitation of traditional health care systems has been that only a proportion of the population, usually the better-educated, has taken the initiative to seek its services and only some of them have benefited from what preventive services have been offered. Few in the health care system have had the training that would enable them to design or implement programmes for the delivery of services to the whole of the population. Just as, in the 1950s and 1960s, most endemic countries assigned special teams to provide smallpox vaccination, so did they have special teams and programmes to deal with tuberculosis, yaws and malaria, for vector control, for family planning and so on.
The experience in national smallpox eradication programmes confirmed that the existing health care structures were inadequate to deal with community-wide programmes of disease control. Health centres, for example, were customarily directed by physicians or others whose training and preoccupation were with curative medicine, whose management skills were limited, who rarely left the health centres and whose work was seldom supervised. Few centres gave vaccinations of any type and, when they did, often used vaccine that was not properly stored or handled. The cases of smallpox that were seen were only occasionally reported and then usually with great delay; outbreaks were rarely contained. The hospitals performed even more poorly, the inadequacy or lack of isolation procedures actually serving in many instances to augment the transmission of smallpox; even the hospital personnel themselves were often unvaccinated. Travelling teams of smallpox eradication staff endeavoured to alter practices and procedures but only when the personnel of health centres and hospitals were trained and regularly supervised by smallpox eradication programme staff did the performance improve significantly.
It became apparent that in all countries there was a need for a specially dedicated and trained professional staff at all levels to decide and coordinate the strategy and tactics of the smallpox eradication programme and to modify these according to local needs, to develop reporting and surveillance systems, to undertake case detection and containment measures, and to train local health staff in vaccination procedures and the proper preservation of vaccine. There was a need, too, to seek the support of village leaders and, through them, the acceptance and participation of the population. Such activities were alien to most traditional health care units.
The necessity of providing far more than curative care in order to meet the health needs of the community was recognized at the International Conference on Primary Health Care, held at Alma-Ata, USSR, in 1978. It identified primary health care as the key to this goal, being composed of a group of activities encompassing promotive, curative and rehabilitative services for all in the community.
Primary health care is often discussed as though all its activities could be pursued in a like manner, and indeed the skeletal structure of the traditional health care system can sometimes serve as the base for both preventive and curative services. As was apparent in the smallpox eradication programme, however, a different orientation and training of personnel are required for community—based programmes whose objectives are more broadly defined in terms of preventive and other disease control activities intended to reach all in the community. If directed by physicians with traditional training, the standards of the traditional service for the delivery of health care will usually be assessed by the level of training and skill of its practitioners, the quality and sophistication of its facilities and the numbers treated. In contrast, community-wide programmes whether preventive (such as those for immunization or family planning), curative (such as those for oral rehydration or for the therapy of yaws or malaria), or a combination of the two- require that the standards of performance be assessed in terms of success in dealing with health problems in the community. Such programmes require active outreach through public education and persuasion to ensure their acceptance, the provision of services at a site and time convenient to their clients as well as methods, such as surveillance, to measure the degree of success. Based on the experience in smallpox eradication, few traditional health care systems have been designed or their personnel equipped to handle both types of activity, and thus curative medicine has remained their dominant concern.
Attraction of resources and community support
Special-purpose programmes to achieve certain clear and specific objectives, usually within a finite period of time, have usually been better supported and financed by politicians and the public alike than have programmes, however laudable, whose health goals have been less explicitly defined. Thus, a programme to eradicate smallpox or to prevent poliomyelitis has had more appeal than one to develop the basic health services ; indeed, almost without exception, public service organizations deal with particular diseases (e. g., poliomyelitis, tuberculosis or cystic fibrosis) or groups of diseases (e . g., cancer or lung diseases). Such programmes can serve broader objectives in the development of the health services, as did smallpox eradication, but support for health programmes that have lacked a categorical focus has often proved difficult to obtain.
Such special-purpose programmes are particularly important in public health because it is always more difficult to obtain a political commitment to and financial support for public health programmes than for those involving curative medical services. There are several reasons for this. First, political leaders are more readily persuaded to provide funds for curative services which, with their hospitals and health centres, are more tangible than a community-based programme. Secondly, the physicians who are most likely to be consulted regarding needs and priorities in health care are clinicians, who are more numerous and usually more influential than public health physicians; lacking a public health perspective, they tend to favour the development of clinical facilities which they will use. Thirdly, those who are the most disadvantaged and have the greatest need for community-based health services are usually the least influential politically. Thus, special- purpose public health programmes which can command attention provide an important balance to the traditional biases in allocation of health resources.
Special-purpose programmes are also associated with intensive publicity, which provides an opportunity to educate the population regarding the desirability of selected health interventions. For example, comparatively few people will voluntarily seek to be vaccinated, but more than 80% can usually be reached during the course of a well-publicized and well-executed mass campaign. As Jamison (1985) has pointed out, China’s remarkable improvements in health over the past 30 years can be attributed in substantial measure to its special health campaigns, of which there have been 4 or 5 each year.
On a global scale, there is no better recent illustration of the potential for heightened support for community-based health programmes with specific objectives than WHO’s Expanded Programme on Immunization, whose goal, established by the Thirtieth World Health Assembly in 1977 (resolution WHA30 .53), is to provide 6 vaccine antigens to children throughout the world by 1990. This effort was augmented by UNICEF’s Child Survival and Development Revolution and was subsequently endorsed in the United Nations (Mandl, 1985). International support of unprecendented magnitude was mobilized, national governments responded with special programmes and, as a result, levels of immuni- zation coverage significantly increased in many countries.
Efficiency and supervision
Special programmes which involve the large-scale delivery of services permit economies to be realized and can facilitate better management of supplies and equipment than is possible when services are provided only in established health centres or practitioners’ offices. Immunization programmes are a case in point. The cost of a dose of vaccine in multiple-dose containers is far less than that of the same dose individually packaged. To take full advantage of this, however, all or most of the contents of the larger container must be used at once, because vaccines deteriorate rapidly after the vial is opened ; this is most easily accomplished in a large-scale campaign in which large numbers of people are vaccinated each day. Another but more difficult approach is to assemble large numbers of children at clinics on special vaccination days.
The efficient use of vaccine is also more readily achieved when a few vaccinators perform many vaccinations than when many health centre staff each perform a few. Throughout the course of the smallpox eradication programme, there were recurring problems in ensuring proper vaccination technique and the proper sterilization of instruments by hospitals and health centres. Despite frequent visits by supervisory smallpox staff, many health centres in all countries regularly stored reconstituted vaccine far longer than the 1 day that was prescribed and ignored or were unable to cope with refrigeration failures. Although similar problems affected vaccination teams, it proved far easier to supervise, say, 10-25 vaccination teams than 100-250 health centres.
Definition of Objectives and Goals
From 1967, the most important difference between the Intensified Smallpox Eradica- tion Programme and the previous efforts was that the strategy and tactics were decided in terms of a clear ultimate objective-a nil incidence of smallpox. Although this objective is implicit in any eradication programme, progress before 1967 had been measured primarily by the numbers of vaccinations performed ; the reporting of cases was considered so deficient as to be meaningless (WHO Expert Committee on Smallpox, 1964) but nothing had been done to improve its quality . Focusing on the objective of a nil incidence meant that the reporting of cases had to be improved and surveillance systems and field epidemiology developed. New methods were devised for discovering cases and containing outbreaks; resources were allocated in such a way as to provide for particularly intensive efforts where the incidence was highest, at times when transmission was most susceptible to interruption and in places where the risk of spread was greatest. In effect, this approach served to blend management with epidemiology.
Logic suggests that any disease control programme should provide continuous measurements of its impact on incidence and that these in turn should dictate changes in strategy and tactics. In fact, this is seldom the case even today. Most authorities ignore such information or dismiss efforts to obtain the data as being too difficult. Instead, progress is assessed in terms of activity, such as the numbers of vaccinations performed or of patients treated. Several countries in the early
1960s reported with satisfaction that they had vaccinated half or more of their population against smallpox each year, yet the incidence remained high owing to the use of poor vaccine and to lack of supervision. This clear indication that something was amiss with the management of the programme or the efficacy of the vaccine was ignored, however.
Although progress in the Intensified Programme was gauged primarily by the reduction of smallpox incidence, subordinate programme goals were also established in each country and area. They closely followed the principles for good management enunciated by Austin (1979), being specific, measurable, realistic and dynamic. For ex- ample, mass vaccination campaigns were expected to result in more than 80% of the population in each area having a vaccination scar. Assessment teams could easily determine the proportion of the population with a scar and, as experience showed, this goal could readily be achieved with a reasonably effective campaign. As programmes improved, this target was made more rigorous, it being required that 80% of those under 15 years old and sometimes 80% of those under 5 should have a vaccination scar. Although more difficult, these standards were not beyond attainment. For successful primary vaccination, take-rates of 95% or more were established as the standard, one which could be readily measured and was tolerant of error since rates of 99% and more were customary under optimal conditions.
From 1974, standards were also established for surveillance and containment. They established as goals that 75 % of outbreaks should be discovered within 2 weeks of the onset of the first case, that containment of the outbreak should begin within 48 hours of its discovery and that no new cases should occur more than 17 days after containment had begun. As the incidence of smallpox decreased or ceased, other standards for the measurement of performance were developed which related to the population’s knowledge of a reward for reporting cases and the completeness of reporting of other diseases, such as chickenpox.
The various standards were of the greatest value when the data were promptly collected, analysed and used as management guides for programme action. The knowledge by those collecting the information that their data were being promptly put to use contributed greatly to the development of the system and to better performance. There was a limit, however, to the number of standards that could be effectively employed. This became evident during the concluding phases of global eradication as more standards were adopted and their stringency was increased : a growing volume of data accumulated, only a portion of which could be satisfactorily analysed and interpreted for use. It was apparent that a few indicators of overall performance, closely followed, were more valuable than a broad spectrum of indicators expressing the measure of many different aspects of programme execution.
Quality Control
Methods to ensure that smallpox vaccine was potent at the time of its use, that vaccination coverage met the expected goals, and that progress was being made in diminishing smallpox incidence all represented forms of quality control. Before 1967, their application was infrequent. In both industrialized and developing countries, vaccines, even at the time of manufacture, often failed to meet the accepted international standards ; few independent national testing centres monitored vaccine quality ; and few health service staff examined the vaccinated after one week to determine whether their vaccina- tions had been successful. In many countries, large numbers of vaccinations were regularly reported but seldom was there confirmation of this by sample survey to check vaccination scars. It was known that the cases of smallpox that were reported represented only a fraction of the total but even these data were seldom reviewed to determine epidemiological trends or patterns of incidence.
The evident disinterest in quality control which characterized smallpox control programmes before 1967 is difficult to understand, but in fact it typifies large segments of current public health and medical practice . In many countries, for example, biological and pharmaceutical products are accepted and used with little assurance of their potency or purity and with little confidence that they have been properly refrigerated. Even the most elementary measurement systems, such as the enumeration of deaths by cause and the incidence of important diseases, are manifestly deficient. Where systems exist for the routine collection of information, the data,
more often than not, are consigned to statistical reports. The fact that the concept of surveillance, although simple in principle, proved so difficult to apply, reflected the lack of experience with measurement throughout the health field and, indeed, the lack of programme goals which would encourage such measurement.
Programme Management
Multinational, cooperative health pro- grammes are inevitably difficult to manage, given the realities of national sovereignty and the intrinsic problems of international organizations. The smallpox eradication programme could not operate as a monolithic structure, like a military command ; rather, it was obliged to function in a collegial structure of many independent national programmes, each with its own administrative traditions and socio-cultural patterns, and utilizing resources from many different sources. It was a programme in which WHO, the coordinating organization, provided only a small proportion of the resources and had no authority with respect to national programmes other than that of moral suasion . Authority and responsibility within WHO itself were highly decentralized, each of its 6 regional offices enjoying a substantial degree of autonomy. With its functions and its structures at the time, the Organization was better suited to the implementation of local or regional programmes than to the execution of a world-wide programme which required international mobilization and the selective allocation and re-allocation of resources on a global basis.
Other global health programmes are confronted with similar challenges today. An effort is therefore made here to identify factors in management which contributed to the eradication of smallpox and which might facilitate more effective and better coordinated programmes of other types .
The network of professional staff
Because a hierarchical structure of international and national staff was not possible, other mechanisms had to be found to coordinate planning and to ensure continuity in the execution of the work, to control the quality of vaccines and of performance alike, and to assess and redirect the programme as it evolved. Within WHO itself, the successful accomplishment of these tasks depended primarily on the recruitment of capable professional staff who could be given substantial latitude to make decisions, who could be assured of the funds, manpower and administrative support they needed, and who could be provided with leadership by example and exhortation rather than by directive . In the broader reaches of the programme much depended on the extent to which continuing close communication could be maintained between the national and the international staff, on their degree of mutual respect, and on the level of their common understanding of problems and needs.
A unit at WHO Headquarters with overall responsibility and accountability for all activities related to the programme proved to be essential. At first, the responsibility for a number of activities directly pertaining to smallpox eradication was scattered among a variety of units. The testing of smallpox vaccine and the development of its production were the concern of one small unit which had to deal with the entire field of biological products; notifications of smallpox cases were received by the units concerned with the application of the International Health Regulations and with the compilation of international health statistics ; and yet another unit, concerned with virus diseases, dealt with smallpox research. The Smallpox Eradication unit gradually assumed the responsibility for all the activities that concerned the programme and they subsequently became more effective and more responsive to the programme’s needs.
More rapid progress might have been possible if, from the beginning, there had been special staff to handle two other activities-public information and soliciting contributions from donors. There was a need to publicize widely what was being done, and where and how, in order to encourage national authorities and the participating staff and to recruit support from donors. WHO’s public information office did what it could but was unable adequately to meet this need as it was small and had to serve the Organization’s many other interests and programmes. Use of the Weekly epidemiological record to publish a full and candid account of progress and problems in the programme at intervals of 2 or 3 weeks served well to inform the public health community, but it was not especially helpful in stimulating coverage by the mass media for the information of a broader public. A marked change occurred in 1977, when a full-time public information officer joined the small- pox eradication programme. His efforts proved vital to fostering public confidence that eradication had been achieved and that vaccination could be stopped. There were no professional staff in WHO, however, whose full-time responsibility it was to solicit voluntary contributions even though two-thirds of all international funds for the programme were expected to be provided from this source. The staff of the smallpox eradication programme undertook to raise these funds as best they could but they lacked the expertise, the necessary political contacts and the time, and their success was limited.
The Smallpox Eradication unit at WHO Headquarters provided a central point of contact for those outside the programme, whether scientists in research or vaccine production laboratories, potential donors, possible candidates for service, or the media. Because the unit needed to keep abreast of the latest developments to disseminate current technical information about the programme as widely as possible, frequent and regular communication between the scientific and public health communities and the staff of the unit was encouraged. This facilitated the rapid application in practice of new developments and benefited other operations as well.
A counterpart professional group of at least 2 or 3 persons in each of the 4 WHO regions in which smallpox was endemic would have been invaluable, particularly because of WHO’s decentralized structure, but, although this was strongly encouraged, it was implemented in only 1 region. Consequently functions that might more logically have devolved upon the regional offices of WHO often had to be undertaken from Headquarters ; national programmes were not always adequately supported or monitored ; and the global coordination of activities was less satisfactory than it might have been.
For national programmes, an accountable and responsible professional person, preferably appointed to deal exclusively with smallpox eradication, was considered essential by WHO as a locus of contact and for the planning and implementation of the programmes. Each country was therefore requested to designate a specific person to be responsible for smallpox eradication rather than simply an office or a section of the health ministry. This proved effective except in countries where officials were frequently transferred. However, 3 functions which were customarily the responsibility of parts of the ministry not directly concerned with disease control often presented special problems : case reporting, quality control of vaccine, and public education.
The national notification of cases was often the responsibility of a statistical unit which mechanically recorded such data as were received, showed little concern with the completeness of notifications and was not responsible for initiating action based on the reports received or compiled. Such systems seldom improved unless the smallpox eradication officer assumed the responsibility for the notifications of smallpox cases and used the data for monitoring the programme and allocating resources. This assumption of re- sponsibility, however, often did not occur until many months or years after programmes began.
The quality control of smallpox vaccine was a problem in most countries which produced their own vaccine. Usually they had no national control laboratories and the production laboratories themselves were the ultimate arbiters of quality. Although it was WHO policy to have a WHO collaborating centre test all vaccines used in the programme, the laboratory directors often opposed this and sometimes refused to submit samples. The national smallpox eradication programme officers had no authority to enforce the policy and so it was frequently necessary for senior WHO staff to intervene with higher-level government officials. Compliance, however, was seldom easily achieved, and in a few countries substandard vaccines continued to be used even though the problem was known and recognized.
Responsibility for health education was usually assigned to a special unit in the ministry of health, but such units were seldom either adequately staffed or especially able or imaginative. Few contributed significantly to smallpox eradication campaigns, most educa- tional efforts being mounted by regional and local smallpox programme personnel who pragmatically developed materials as required.
Overall, the basically collegial management of the programme functioned surprisingly well, its principal handicap being the lack of adequate numbers of senior staff at WHO Headquarters and in the regional offices, in national programme offices and in states or provinces. Paradoxically, national governments were reluctant to provide one or a few additional senior supervisory staff, even when available, although they were almost always prepared to add tens, hundreds or even thousands of vaccinators. In one of the largest countries, for instance, the national programme directorate consisted until 1972 of only 1 professional person, and in one of WHO’s regional offices smallpox eradication was the part-time responsibility of a medical officer who had to deal with all communicable diseases.
Personnel recruitment and training
The competence, motivation and experience of the staff ultimately govern the success of all programmes and this was unquestionably the case with smallpox eradication. Within WHO, considerable time was required to assemble the professional staff that was needed. Except for staff at Headquarters, recruitment was the de facto responsibility of the regional offices. Other factors of selection sometimes outweighed those of professional competence and motivation, and the smallpox eradication staff at Headquarters were, at first, seldom consulted by the regional offices about personnel decisions. Performance was not always closely monitored and contracts were sometimes renewed irrespective of performance, or personnel who proved unsatisfactory in one post might be transferred to another that could be as crucial to the programme as their previous position. However, increasing numbers of competent staff were recruited to WHO as special efforts were made by Headquarters to identify qualified candidates through personal contacts with an informal network of reputable epidemiologists, and applications were encouraged from staff who had performed well in national programmes.
The quality of national programme leadership was initially no less uneven; as the programme progresssed, however, and eradication appeared more attainable, national officials increasingly assigned direction to their more able staff, many of whom had previously demonstrated their competence in field operations. Contrary to a widely held view, most countries had more than enough competent staff who could assume positions of leadership, even if many of them lacked practical experience in management because their supervisors had been unwilling or unable to delegate authority and accountability.
A common understanding by all the senior national and international staff of the principles underlying the programme, of its essential components, and of the more important measures of progress was as crucial to success as the quality of the staff, for on it depended the ability of the programme directors to introduce effective innovations and to adapt their programmes to the prevailing circumstances. The Handbook for Smallpox Eradication Programmes in Endemic Areas(SE/67.5 Rev.1), surveillance reports, national and inter country meetings, and personal visits all helped to accomplish this. The experience in the programme in western and central Africa suggests that special training programmes of perhaps 2-4 weeks’ duration for all newly assigned international and senior national staff would have been equally useful elsewhere. However, a lack of appreciation by the regional offices of the need for such courses and a dearth of senior personnel to conduct them precluded their development until 1974. At that time, the intensification of the programmes in India and Bangladesh brought in sufficient additional WHO staff and consultants and specially recruited national epidemiologists to permit training programmes to be conducted in each of the remaining endemic countries.
National smallpox eradication programmes were usually staffed by persons already engaged in smallpox control and others who were reassigned from other programmes. Most countries had many more health staff than programmes with the resources to support them and their work. Given 1-2 weeks of practical field training for smallpox eradication, a steady flow of the supplies and equipment they needed and good field supervision, most performed competently and with dedication. The quality and the nature of the supervision they received were of vital importance. The best results were obtained where WHO, national, and state or provincial supervisory staff travelled frequently into the field to review activities, to resolve problems and to work with the field staff on the solution of their problems. Monthly or fortnightly meetings at which the field staff and supervisors from different areas met to discuss progress and problems and to compare results also proved valuable.
Not only was smallpox a disease with which the ordinary villager was familiar and that he could easily recognize, though he might confuse it with chickenpox, but it also became evident early in the programme that the villagers and their leaders, if properly approached, were usually willing—indeed, eager-to cooperate in organizing vaccination programmes and in detecting cases. From 1973, when programmes in the remaining endemic countries were intensified, many of them were recruited and trained for part-time work in these activities. Their performance, as that of other field staff, was directly proportional to the clarity of the direction provided and the quality of the supervision they received.
In brief, it was clear that comparatively few, strongly motivated and knowledgeable professionals could organize and effectively mobilize large numbers of persons and that in most countries they could count on the eager support of the health staff and the general population alike. The limiting factor was the inadequate number of motivated and knowledgeable leaders, largely because too few were recruited, trained and assigned to responsible positions.
Financial and other resources
A deficiency of resources was a continual problem, which seriously jeopardized the international effort. Despite the importance of global smallpox eradication for all countries, support for the programme was barely adequate to sustain it, even during the last months before transmission was stopped. In large part, this was due to scepticism during the early years of the programme about the feasibility of eradicating a disease. Global malaria eradication had required and received substantial resources, but it was increasingly recognized to be unattainable. In consequence, disappointed bilateral donors and organizations of the United Nations system gradually withdrew support and many declined to provide more than token help for yet another eradication campaign. Such efforts as were made to inform potential donors of the progress being made in smallpox eradication and of the programme’s needs proved inade- quate until 1974. An intensified, well-publicized campaign had by then begun to stop transmission in the 5 remaining endemic countries as quickly as possible, before natural or man-made catastrophes could thwart the effort. When it became evident that additional resources were indispensable, special funds were made available by WHO and large contributions were received from Sweden and later from several other donors. These made possible the successful, large—scale programmes in Asia, but until 1976 they were insufficient to strengthen adequately the programmes in Ethiopia and Somalia. After the last case occurred in 1977, but long before the necessary work of certifying that eradication had been achieved was completed, support for the programme waned again.
Plate 31.4. Even Snoopy, the well-known cartoon character, supported smallpox eradication. He was never vaccinated, however. (Drawn by Charles Schulz, 1976.)
Obtaining sufficient resources in the endemic countries often proved as difficult as obtaining international contributions. Although few countries had to provide significantly more money for smallpox eradication than for their previous smallpox control work, their health budgets were small and competing needs were many. To obtain adequate resources, special appeals to national leaders were frequently required. When a nil incidence was reached and the immediate threat of smallpox was removed, however, there was a strong incentive to allocate the men, money and materials to the control of other diseases; consequently, support diminished rapidly and resources to permit certification activities were seldom more than barely adequate.
Several requirements need to be borne in mind when there is a considerable dependence on voluntary donations of money or materials from different sources: (1) quality control of donated items; (2) standardization of supplies; and (3) availability of discretionary funds.
Donations in kind to the smallpox eradication programme were primarily gifts of vaccine, which was tested by WHO collaborating laboratories to be certain that it met the accepted international standards. Although it had originally been thought that vaccine from well-established laboratories in industrialized countries would not need to be tested, it was soon discovered that some of it did not meet the standards.
It was found that many governments licensed producers to distribute vaccine which had been found acceptable only by tests conducted by the producer’s own laboratory, and that the least competent producers were the least conscientious in vaccine testing and sometimes certified sub—standard batches. As a result of these findings, a number of countries were prompted to establish national vaccine control laboratories for the first time. The quality of vaccine subsequently improved significantly, but even then occasional batches of substandard vaccine were submitted for donation.
Standardization of equipment and supplies was especially important for items that required spare parts or knowledgeable mechanics for their maintenance. For vehicles and motor cycles, the most commonly provided articles, it was best to provide models already in general use in a country. The provision of unfamiliar products meant that stockpiles of spare parts had to be created and mechanics had to be specially trained. This could be done reasonably economically on the scale that obtained in the larger countries, but it gave rise to considerable problems in smaller countries. In all countries, however, the provision of only a few vehicles or motor cycles of unfamiliar manufacture usually proved to be more of a problem than a benefit. Standardization with regard to vaccine was also important. At first, vials from different manufacturers contained amounts ranging from 15 to 500 doses (0.15-5.00 ml) of vaccine, but this complicated programme planning and confused the vaccinators; efforts were therefore made to standardize all vials of vaccine so that they contained 0.25 ml when reconstituted. Package inserts (printed forms detailing uses and contraindications) accompanying the vaccine also proved to be a problem because each country had its own policies regarding the age for and contraindications to vaccination. Eventually, however, all producers were persuaded to use a specially prepared WHO package insert which corresponded to global vaccination policies.
Finally, it is important to note that, for a programme financed principally by voluntary contributions, it was essential to have some unrestricted funds which could be used for any necessary purpose and in any country. Most donations were restricted for use in a single country or were received as contributions in kind; only a small proportion of them were received in cash and without limitations on their use. Fortunately, funds were available under the WHO regular budget to meet programme needs for which provision was not otherwise made. In western and central Africa, for example, the USA provided for all except what were known as “local costs” (costs of petrol, vehicle repair and per diem allowances for the teams), which its national policy prevented it from meeting ; these costs were covered by WHO. There and elsewhere the sums required were small in comparison with the totals involved, but without discretionary funds most of the programmes would not have been able to operate. Likewise, although almost all the vaccine not produced locally was provided as contributions in kind, discretionary funds were needed for the purchase of vaccination instruments and for the printing of package inserts.
Logistics
Whether a programme functioned or failed depended upon the availability of vaccines, vaccination instruments, vehicles and other supplies. Without them, programmes stopped, the momentum was lost, smallpox spread, and morale fell quickly. It was not always easy to ensure that these items were available as needed, since the demand for them fluctuated as a result of natural and man-made emergencies, unexpected epidemics and a host of other factors. The WHO smallpox eradication programme took an active part in dealing with such problems, acting in an operational capacity rather than restricting itself to the advisory technical role that was more customary in many international programmes. This proved helpful in countless circumstances. Being in frequent contact with national and WHO programme staff, the Smallpox Eradication unit could sometimes anticipate problems and take preparatory action and was able to evaluate requests and to respond quickly. An emergency reserve of vaccine and vaccination instruments was created which permitted these to be distributed within 48 hours of a request being received ;supplies and equipment could occasionally be diverted from one country to another; and special funds were sometimes provided for emergency procurement of equipment or to pay for special consultants.
The most intractable problem, and one that was never fully solved, was the supply of vehicles. Most health ministries were short of roadworthy transport and were usually unable to provide for emergency requirements. For vehicles of foreign manufacture there was usually a delay of 12-18 months between the submission of a purchase order and their delivery but it was often impossible to gauge the need for them more than 3-6 months in advance. The difficulty was resolved in some countries by purchasing locally manufactured or assembled vehicles and in others by the local purchase of already-imported vehicles, although this was usually more costly ; in some instances, special workshops were established to repair and maintain the often large fleet of unroadworthy vehicles. Better results would have been obtained if it had been possible to procure a reserve fleet of new vehicles which could be dispatched quickly when needed, and if more efforts and re- sources had been directed to the development or improvement of national vehicle maintenance and repair facilities.
The dispensing of and accounting for funds and the uses to which they could be put were a constant, often formidable administrative problem. In many endemic countries, small per diem allowances and long delays in payment all but precluded travel by the national field staff; allowances for petrol often permitted only a few days of vehicle operation each month ; budgets for vehicle maintenance and repair were small ; and there was often no provision for the disbursement of funds for exceptional needs such as the establishment of facilities for the isolation of patients or the payment of a reward for reporting cases. These and similar fiscal problems were largely resolved by the use of WHO funds to meet the “local costs” mentioned above. Their use was facilitated by establishing imprest accounts, which were an advance made to WHO advisers and senior national staff, for which they had to account before a further advance was made. The availability of ready cash in this way permitted action to be taken expeditiously and eased the work in the field. Implementation of the system was not with- out problems, however. For example, in many areas illiteracy made it difficult to obtain the receipts which a proper accounting called for, and in all programmes there were a host of questions as to what constituted proper expenditure. The propriety might be questioned, for instance, of making small payments to smallpox-afflicted beggar families in India to ensure that they remained in isolation. Without the sympathetic and flexible administrative support provided by WHO, satisfactory solutions would seldom have been found.
Operational tactics and strategy
An important principle underlying the operation of the smallpox eradication programme as a whole was that the administrative structure and pattern of operations of each national programme should be integrated as well as possible into the health and socio- cultural setting of the country concerned. This differed from the operational strategy in malaria eradication, which called for a separate malaria service and laid down detailed administrative responsibilities and functions for personnel at every level. For smallpox eradication, the operational objective was broadly identified:the ultimate goal was a nil incidence of smallpox, to be confirmed by an adequate surveillance programme. To achieve this, a two-part programme was stipulated. First, a vaccination campaign was recommended to ensure a level of immunity among the population as a whole high enough to reduce the incidence of smallpox substantially ; secondly, a surveillance programme was to be established to ensure prompt reporting of cases from all health facilities, to permit the investigation and containment of outbreaks and to analyse patterns of occurrence of smallpox so that corrective measures could be taken in both vaccination and surveillance activities.
Programmes were expected to be designed locally by the national staff and their WHO counterparts working in collaboration and to evolve and change with time in the light of experience. Consequently, programmes differed greatly from country to country and from time to time. The role of the WHO staff assigned to the countries likewise differed somewhat from one country to another . The most effective were those who served as working counterparts and took an active role in field operations. Those who assumed the more traditional role of passive technical advisers and rarely travelled outside the capital city were encouraged to leave the programme. As working counterparts, WHO staff with prior experience in other smallpox eradication programmes transmitted confidence in the feasibility of eradication and were better able to introduce new methods ; they frequently served to provide continuity and sustain momentum in programmes when the national leadership changed ; and it was sometimes easier for them than for their national counterparts to approach the more senior health officials in the country to seek additional support or changes in policy.
Given this operational strategy, the WHO smallpox eradication staff in Geneva viewed as their first priority a duty to anticipate and to be fully responsive to national programme needs and to provide all possible support to them. An immediate response to requests for resources or advice, continuing communication regarding progress and developments, and frequent contact through visits and meetings were essential elements. In consequence, those who served with the smallpox eradication programme, whether as national officials or as WHO staff or consultants, identified as much with international as with national goals; they related closely to each other; and they sustained a remarkably high level of morale despite incredibly arduous working conditions. Although a pattern of programme management such as this would appear only logical, surprisingly few multinational health programmes currently operate with this philosophy.
Global strategy and priorities were regularly discussed and decided at meetings with regional and national advisers and national programme staff. Forums such as these were valuable as it was in the course of executing national programmes that the most important observations were made, as a result of which significant changes in strategy and tactics were introduced. These international meetings provided opportunities for critical discussion of the experiences communicated, for a comparison of observations, and for the charting of new directions.
The target of a nil incidence of smallpox- the completion of a finite task-undoubtedly played a role in motivating staff and sustaining interest. There are few health programmes which have such a clearly definable end-point. However, comparable levels of achievement, interest and morale in other programmes should be possible where specific goals are clearly identified, where progress is regularly monitored and where the programme staff are fully supported and encouraged in their efforts.
Research
The importance of the problem-oriented applied and basic research that was conducted throughout the course of the smallpox eradication programme cannot be too emphatically stated. The nature and extent of the research agenda could not at first be fully elaborated or foreseen. The most explicit question when the programme began was whether there was a natural reservoir of variola virus which could thwart the objective of eradication. Beyond this, there was the belief that studies conducted during the execution of programmes could do much to elucidate the epidemiology of the disease and to benefit programme implementation. There was, moreover, the belief that the potential of the tools and methods already available could be further developed to permit the task to be achieved faster and more efficiently.
What was not anticipated at the inception of the programme was the extent to which changes would occur in programme strategy and tactics and in the understanding of the epidemiology and virology of smallpox and other poxviruses. Contributions to these changes were made in a range of disciplines, extending from basic molecular biology to applied technology and the social sciences. The research agenda did not, however, unfold spontaneously. Smallpox eradication programme staff and consultants met regularly to discuss developments and needs. Many staff had to be encouraged and sometimes prodded to explore important questions. Substantial time and effort were expended in editing and preparing for publication many of the papers which were eventually distributed.
The fact that most research was undertaken during and in the context of the field work in order to answer practical questions or to resolve apparent paradoxes provided an unusual impetus to the research effort. Moreover, the interaction of research and programme execution permitted the prompt practical application of many of the findings.
The lesson for other disease control programmes seems evident. However, even today, despite countless discussions about the importance of research for smallpox eradication, other problems of importance to the developing countries receive little research support. Research in applied technology and the social sciences is notably neglected and the potential offered by modern molecular biology has barely begun to be realized. For health programmes in the developing countries, research is neither an academic luxury nor merely an interesting intellectual exercise, as has sometimes been suggested. It is a necessity for the successful prosecution of disease control and was inherent in the achievement of smallpox eradication.
Certification
A feature peculiar to smallpox eradication was that, once it had been achieved, health officials throughout the world-and the general public all had to be sufficiently confident of the fact that the disease had been eradicated everywhere for them to abandon the practice of vaccination. To in still the necessary conviction, special certification activities were required; they are not without relevance to other situations in which one country’s policy is shaped by the health conditions in other countries.
Fostering the required confidence presented difficulties at many levels. National authorities everywhere recognized that the reporting of infectious diseases was deficient in all countries and that in certain circumstances some governments suppressed information about known cases of smallpox (see Chapters 22 and 23). Within countries, smallpox vaccination, one of the oldest public health measures, was a well-established practice, not lightly to be discarded by those responsible for their country’s health. The general population of the endemic countries readily recognized smallpox, and in many cultures it was so familiar as to be considered an inevitable occurrence of normal life. Continual efforts were made by the smallpox eradication programme to publicize widely and in detail, both in the scientific and the general press, what was being accomplished and how. Accounts of the work appeared in WHO’s Weekly epidemiological record; comprehensive summaries were prepared each year for the World Health Assembly and the Executive Board of WHO; numerous scientific papers were published; and coverage in the public media was actively solicited. These efforts intensified as the goal of eradication approached and was finally reached. Although they were partly successful in convincing many persons that the programme had been well conducted and that WHO and national officials spoke with justified confidence of the accomplishment, more was required.
In 1971, the decision was made to appoint independent international commissions of recognized scientists to visit each country in the endemic areas 2 years or more after the occurrence of the last known case so that they might satisfy themselves that the measures taken by the programme would have detected smallpox had it been present. If they were not satisfied, they were directed to recommend additional measures which should be taken. Such visits were arranged only when WHO and national staff were themselves confident that smallpox had been eradicated from an area and that the fact could be documented. Confidence in the process was enhanced when most countries followed a precedent set by Indonesia during the visit of the second of the commissions (early in 1974), when the members of the commission were informed that they could go anywhere they wished, that they could have access to any records they wanted and that they could question anyone about any matter pertaining to smallpox and the eradication programme (see Chapter 13). The first of the international commissions was convened in 1973; altogether, 22 commissions visited 63 different countries (see Chapters 24-27).
There were a number of salutary features of this approach which deserve mention. First, it required each country to prepare a special report setting forth the activities and the evidence which documented the absence of smallpox; this requirement stimulated national officials to support smallpox surveillance programmes after the last case had occurred and when the inclination was strong to divert resources prematurely to other needs. Secondly, wider knowledge of the nature of the programme and confidence in its success were gained by involving in the commissions scientists of many different nationalities, including those who were most sceptical. Thirdly, when each commission reached a decision that eradication had been achieved, important opportunities were presented to publicize the fact nationally and internationally.
A global commission, composed of 22 scientists from 20 countries and assisted by 9 advisers from 7 countries, surveyed the status of the programme from a world-wide perspective and recommended other activities which they believed were needed for them to be confident that eradication had been achieved. Although some activities involved special studies in areas and countries to which access by international staff had been limited, all were completed or satisfactory alternative measures devised and conducted.
Certification of smallpox eradication was valuable and necessary in giving the world community confidence in the achievement. Like the eradication programme itself, it was designed specifically to meet this need and cannot serve as a template to be applied to other questions in which mutual confidence among nations is essential for deciding sound policy. However, problems arising from national doubts about the status of conditions in other countries have arisen in the past and can be expected in the future. Such problems have included those pertaining to the acquired immunodeficiency syndrome (AIDS) and cholera, as well as natural and man-made environmental contamination involving chemicals and nuclear materials. In such circumstances, certain of the principles of the certification programme have applicability—specifically, assessment of the problem in question under the auspices of an international organization, the use of respected scientists of different nationalities who are requested to be critical in judgement, and open publication of their observations and conclusions.
COSTS AND BENEFITS
The eradication of smallpox marked the end of the pain and suffering of its victims who, as recently as 1967, are estimated to have numbered 10-15 million each year and among whom probably 1.5-2 million died. It marked the end of the severe disfigurement, blindness and other disabling conditions among those who survived. It meant that all countries could utilize their smallpox hospitals and wards for other health purposes, that they could stop vaccination programmes and that travellers would no longer need to present vaccination certificates attesting that they had been successfully vaccinated.
The existence of smallpox had important financial implications for all countries. In 1967, all countries were expending substantial funds either to control smallpox and to care for its victims, as was the case in the endemic countries, or to vaccinate and operate quarantine programmes to prevent the disease from being imported, as was the case in countries which were free of endemic smallpox. The expenditure of considerably greater sums for further therapeutic or quarantine services would have accomplished little. However, modest additional expenditures for the prevention of smallpox made a dramatic difference. For the entire global smallpox eradication programme, the annual costs, on average, amounted to only US$23 million over the 13-year period, 1967-1979, a sum which includes both national costs and international contributions.
The benefits to all countries of eradicating smallpox would appear so great and so clear that it is difficult to understand why there were problems in obtaining the requisite resources and political commitment. In part, this reflects the fact that governments tend to be more immediately and generously responsive in providing for the immediate needs of those who are ill. As a practical reality, patients express gratitude for the services received and political support for those pro- viding them. Preventive services are less appealing, the results being reflected in impersonal statistics which indicate that there are fewer or perhaps no patients. An equally important problem is the fact that measures for disease prevention usually require a long period of sustained support and attention before results become apparent. Unfortunately, government officials and donor organizations customarily conceive of plans and budgets in blocks of 3-5 years. Longer-term commitments are uncommon, and with changes in leadership different initiatives are pursued. Even for smallpox eradication, which required comparatively small resources, it proved difficult in most countries to sustain the interest of both national governments and international agencies much beyond 5-6 years.
The Cost to the Developing Countries
For the endemic countries, data regarding the cost of smallpox control programmes are few, and estimates of the expenditure on the care of patients and of the economic losses in productivity due to death or illness are available only for India. No known data document the cost of rehabilitation for those who were left blind or otherwise handicapped.
In 1967, the cost of smallpox control programmes consisted primarily of expenditure on vaccination, ie,., the cost of vaccine, personnel and transport. For the developing countries, this amounted to about US$0.10 per vaccination performed (World Health Organization, 1966b). From national programme reports, it is estimated that a number equivalent to about 20% of the 2500 million residents of the developing countries was being vaccinated each year. This would suggest that about US$50 million were being expended annually for vaccination (Table 31.1).
The costs of care for those who developed smallpox were computed in a study in India by Ramaiah (1976a), who calculated an average expenditure of US$2.85 per patient. Assuming, as he does (Ramaiah, 1976b), that about 2% of all cases were being reported in India in 1967, the total cost of patient care for that year in India alone would have been US$12 million. Given the fact that India, in 1967, accounted for 64% of all reported cases in the world, it would seem reasonable to estimate the cost of patient care globally at more than US$20 million.
Losses due to diminished economic productivity as a result of death must also be considered. For India, during 1967, they are calculated to have been about US$700 million.
The calculation is based on Ramaiah’s analysis (1976a), which employs a life-table approach and defines economic productivity in terms of expected excess of income over consumption during the individual’s lifetime. However approximate the calculation, the average loss in economic productivity of about US$825 per death would appear conservative. Extrapolated globally for perhaps 1.5 million deaths which were estimated to have occurred in 1967, it would seem reasonable to assign a value of at least US$1000 million.
Loss of productivity due to the 3-4 weeks of incapacitation associated with illness must also be considered although in India this was found to be small (Ramaiah, 1976a), mainly because a large proportion of cases were in children for whom no loss in productivity was assumed, and, in part, owing to the low productivity of the average worker.
From these data, sketchy as they are, the cost of smallpox to the developing countries in 1967 was substantial indeed, being not less than US$1000 million (Table 31.1).
Table 31.1: Estimated cost of smallpox to the developing countries, 1967 (millions of US$) a
 a Because the most comprehensive data are from India (Ramalah, I976a, b; Basu et al., 1979), these are given separately, the figures for all developing countries being extrapolated from those for India. Among a total population of 1079 million persons in the endemic countries in 1967, 513 million (48%) lived in India.
a Because the most comprehensive data are from India (Ramalah, I976a, b; Basu et al., 1979), these are given separately, the figures for all developing countries being extrapolated from those for India. Among a total population of 1079 million persons in the endemic countries in 1967, 513 million (48%) lived in India.
The Cost to the Industrialized Countries
Almost all industrialized countries spent substantial sums of money for the routine vaccination of their own populations so that, if smallpox was introduced, the disease would not spread widely; international travellers were required to present certificates of vaccination; and at least two countries maintained special hospitals for use should smallpox be introduced.
Only one comprehensive study of the costs of smallpox prevention in an industrialized country has been reported, a study conducted in the USA in 1968 (Sencer & Axnick, 1973). The cost that year to the USA of providing 5 .6 million primary vaccinations and 8.6 million revaccinations was calculated to be US$92.8 million—about US$6.50 per vaccination (Table 31.2). Among those vaccinated, 8024 had complications requiring medical attention, 238 were hospitalized, 9 died and 4 were permanently disabled. Other costs were associate with absences from work due to vaccination and vaccination reactions, quarantine services and time lost by the maritime industry in waiting for clearance of vessels. The average annual cost of US$150 million amounted to about US$0.75 per capita for 1968. These data do not permit accurate global estimates of the expenditure by all industrialized countries but, if a cost as low as US$0.25 per capita is assumed for those other than the USA, the annual cost, for 1967, would have been US$350 million.
Table 31.2: Costs associated with smallpox protection in the USA, 1968 (millions of US$)a
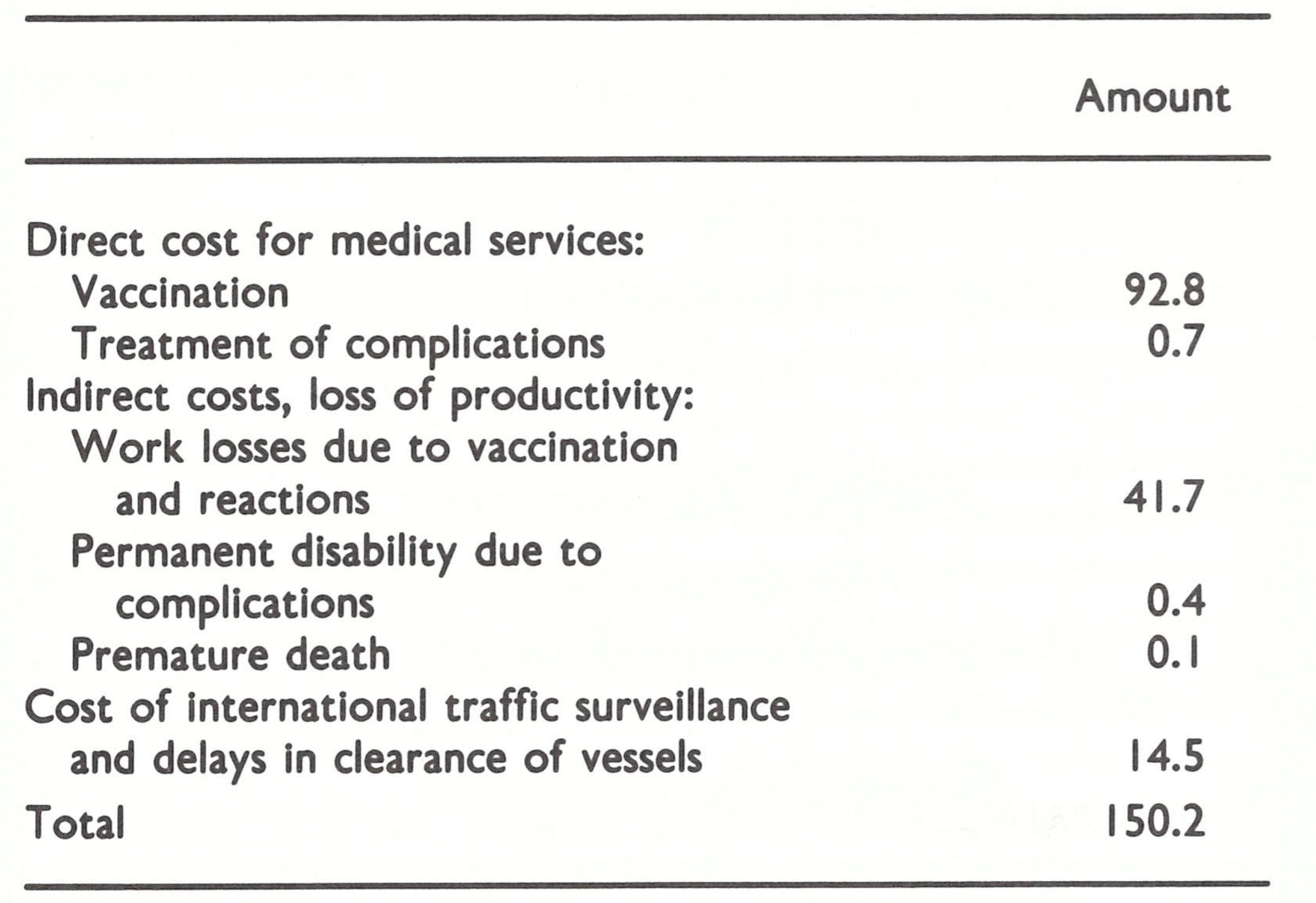 a From Sencer & Axnlck (1973).
a From Sencer & Axnlck (1973).
Expenditure
Compared to the annual cost of smallpox to the world which, in 1967, was more than US$1350 million, the anticipated expenditures for a 10-year global eradication programme were modest indeed. The Director-General of WHO, in 1966, estimated a need for international assistance of US$4.85 million per year over a 10-year period. He requested that US$2.4 million be appropriated for this purpose in WHO’s 1967 budget, although this was accepted by the World Health Assembly by only the narrowest of margins (see Chapter 9).
Ultimately, the costs of the programme were greater than had been anticipated (Table 31.3). International expenditure amounted to US$98 million, about twice what had been foreseen. The endemic countries are believed to have spent no more than twice this amount, about US$200 million.
For all countries, the economic benefits of the programme were substantial as it became possible to stop all preventive measures and to close treatment facilities. The USA, although the largest donor, is estimated to realize in savings the total of all its contributions to the programme every 26 days (Brilliant, 1985).
Table 31.3: Expenditure on smallpox eradication, 1967-1979 (US$)a
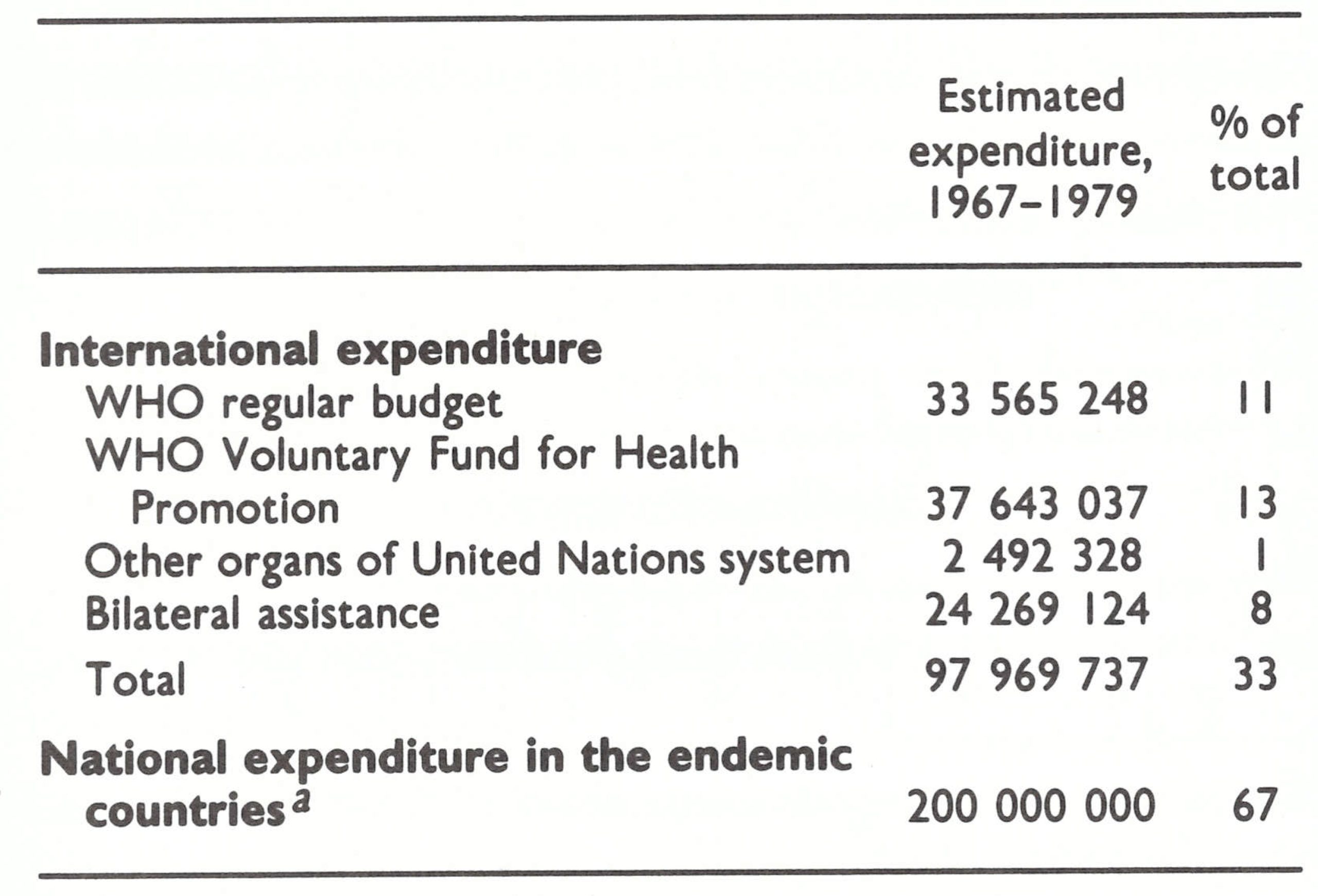 a Based on analysis of financial data from Bangladesh, Ethiopia, India and Indonesia and less complete data from other countries which had endemic smallpox In 1967.
a Based on analysis of financial data from Bangladesh, Ethiopia, India and Indonesia and less complete data from other countries which had endemic smallpox In 1967.
IMPLICATIONS FOR THE FUTURE
The achievement of smallpox eradication demonstrated the potential of WHO as an organization within which all countries, whatever their beliefs and politics, could cooperate successfully in the pursuit of a common global objective. It encourages the hope that other challenges might likewise be addressed. By demonstrating how cost-effective a population-wide programme for disease prevention could be, it directed attention to other preventive measures and health programmes which could effectively utilize community-wide strategies. Previously endemic countries, having become aware of the considerable capacity of their own health services when given proper direction and supervision, looked toward new goals. Thus, an important impetus was provided for new initiatives in, for example, immunization, diarrhoea) disease control and the prevention of blindness. This was by far the most significant contribution of smallpox eradication to the shaping of future strategies for the provision of health care.
Global smallpox eradication came at a time when conventional wisdom increasingly held that human pathogens were ecologically so well adapted that the concept of eradication was untenable (Dubos, 1965). However, the demonstration that the eradication of a dis- ease was feasible led a number of scientists to conclude that this very feasibility was the most important lesson to be learned from the programme and to advocate that a similar approach should be taken to other diseases (Stuart-Harris et al., 1982). A number of diseases have been proposed as candidates, and efforts have, in fact, begun to eliminate dracunculiasis (guinea-worm infection) globally and to eradicate poliomyelitis from the Western Hemisphere.
Disease eradication is unquestionably an attractive goal, but the difficulty of its achievement should not be underestimated. It must be borne in mind that when the smallpox eradication programme began, the prospects for its success were more favourable than for any other disease eradication programme that might be envisaged today. The technical feasibility of interrupting the transmission of the smallpox virus had already been demonstrated both in the industrialized countries and in many developing ones; an inexpensive, highly effective vaccine was available; and there was a substantial political commitment to the achievement of the goal that had been set. Nevertheless, however favourable the circumstances, success was by no means a certainty even during the concluding years or even the final months of the programme. Indeed, the gap between success and failure in a number of national programmes was a narrow one, and the issue was often favourably decided by fortuitous and unpredictable political developments and with only marginally adequate resources. It is difficult to conceive of other disease eradication programmes experiencing fewer problems; and if they were technically more difficult or less adequately and universally supported, their success would appear to be doubtful indeed.
The consequences of the failure of an eradication programme must also be weighed. Some have argued that such special efforts as would be required would result, at worst, in better control of the disease. However, the repercussions which followed upon the failure of malaria eradication cannot be ignored. Not only was the judgement and credibility of national and international leadership called into question but a number of assistance agencies decided, as a matter of policy, not to provide resources for another eradication effort. Some agencies, in fact, questioned the desirability of supporting any categorical disease programmes. These views prevailed throughout the smallpox eradication programme, often to its detriment.
Eradication of Other Diseases
The possible eradication of a number of diseases has been considered recently (Stuart- Harris et al., 1982) although, in the enthusiasm and interest, the proper definition of eradication has been deplorably corrupted (see Chapter 9). Some have used the term to refer to the control of a disease to the point at which it is no longer an important public health problem and some have mistakenly applied the term to programmes intended to prevent hunger or to control accidents and injuries. Here, we refer only to the feasibility of interrupting the transmission of an infectious agent over a geographical area of sufficient size so that control measures may be stopped or greatly reduced, i.e.,eradication on a regional or global scale.
The candidate diseases of greatest interest are those in which man is the only host of the pathogen and the pathogens themselves do not survive for long periods in nature or man. The prospects for eradicating diseases which have an animal reservoir-such as yellow fever, rabies or plague-are nil given present technology. Equally problematic are cholera, the vibrio of which can persist for a long time in brackish, polluted waters, and diseases such as tuberculosis and leprosy, of which the mycobacteria can remain latent in man for many decades.
Another important consideration which must be weighed in considering a disease for eradication is obtaining a sufficiently broad and sustained political commitment. Those who decide policy and the allocation of funds must perceive the disease problem to be serious enough to warrant expending additional funds; but, no less, the populations which are most affected must be sufficiently motivated to cooperate. The time required is important as well because, as was noted above, it proved difficult in all countries to sustain an interest in smallpox eradication for longer than about 6 years.
The preventive measures required for eradicating the disease in question must be inexpensive, considering the fact that international support for health programmes has never been substantial and that most developing countries are already hard-pressed to meet the needs of their existing health activities. The smallpox eradication experience must be borne in mind as, despite the relatively small budget it called for and the implications which success had for all countries, the difficulty of having adequate funds available was a major constraint.
Finally, the methods to be used for the eradication of a disease should be comparatively simple to apply and should not require frequent, repeated contacts with individuals in the population. Skilled management in the developing countries is not plentiful, and programmes that require complicated procedures or considerable discretionary judgement are less likely to succeed than simpler ones. Problems can also be anticipated if it is necessary to contact the population on repeated occasions, as would be the case if individual subjects had to be given a drug each day or each week for a period of weeks or months. The cost and discipline required to execute such programmes make them prohibitive in most areas.
The prospects at present for the global eradication of most human diseases are not good. Epidemiological characteristics preclude many from consideration, while the nature and cost of the available technologies rule out others. However, with a growing international interest in prevention programmes and the emergence of new and better vaccines and other technological developments, there is hope that other global eradication programmes may eventually be successfully mounted. During recent years, 4 diseases have been seriously advanced as candidates for global eradication within the foreseeable future: measles (Hopkins et al.,1982; Katz et al.,1983), poliomyelitis (Horstmann et al., 1984), dracunculiasis (Hopkins, 1983b), and yaws (Hopkins, 1976; Burke et al.,1985). In 1985, the Pan American Health Organization approved a regional poliomyelitis eradication programme, the objective of which is the interruption of poliovirus transmission in the Western Hemisphere by 1990. In 1986, a programme for the global elimination of dracunculiasis was approved by the Thirty-ninth World Health Assembly (resolution WHA39.21) although no time limit was established for its accomplishment. The prospects for each of these initiatives are briefly reviewed below.
Measles
The possibility of measles eradication is suggested by the fact that man is the only host of the virus and that a single dose of an inexpensive vaccine provides long-lasting immunity in 90-95% of vaccinated persons. In developing countries, measles is a sufficiently serious disease to warrant an eradication programme. In the industrialized countries, however, complications and deaths associated with measles are so much less frequent that many countries do not now conduct effective control programmes. The wisdom of this policy has to be questioned but, certainly, there is not yet universal interest in the control of the disease, let alone in its eradication. There are other impediments as well. The measles virus is much more readily transmitted from person to person than was that of smallpox. Not surprisingly, the disease spreads rapidly and widely, and a high proportion of children in developing countries experience measles before they reach 3 years of age. Because the virus spreads so easily and the diagnosis may present difficulties, surveillance-containment measures such as were used in smallpox eradication have not proved to be feasible or effective. To interrupt transmission, it has been calculated (Anderson & May, 1983) that an immunity level greater than 90% will be necessary, a level which is all the more difficult to achieve because vaccination is not possible before the age of 6-12 months, when the child loses its maternal antibody. If there were a vaccine which could be administered at or shortly after birth, the prospects would certainly be better.
Practical evidence that an eradication campaign is premature is provided by the experience in the USA. There, the incidence of measles has been reduced almost to nil but, despite a commitment to interrupt transmission by 1982 and the provision of considerable resources to that end, the measles virus continues to spread.
Poliomyelitis
The feasibility of eradicating poliomyelitis appears greater than that of eradicating measles. Poliomyelitis is more universally accepted as being of sufficient importance to warrant an eradication programme. Man is the only host of the virus and good protection is usually provided by both the inactivated vaccine and the attenuated live vaccine. Many industrialized countries and some developing countries have, in fact, already been successful in interrupting poliovirus transmission, mostly through use of the oral, attenuated vaccine. Some industrialized countries which have used the inactivated vaccine have also been successful.
The decision by the Pan American Health Organization to begin a regional poliomyelitis eradication campaign was preceded by national vaccination campaigns in the Americas in which the inexpensive and easily administered oral vaccine was used. In the early 1970s continuing circulation of polio-virus ceased in North America, and by 1985 the number of reported cases in the Western Hemisphere had diminished to fewer than 1000 a year.
The eradication of poliomyelitis, however, presents a number of special problems. First, the oral vaccine is so thermolabile that refrigeration is required almost to the point of administration, and at least 3 doses are necessary for protection. Vaccination campaigns that must depend upon such a vaccine are inevitably more complex and more difficult than those in which a single dose of thermostable vaccine can be used, as was the case with smallpox. Another matter of concern is the fact that several studies suggest that the oral vaccine is less efficacious in some tropical areas than in temperate climates, although the reasons for this remain unclear. The inactivated vaccine has been suggested as an alternative but it is more costly and requires 2 doses to be given by syringe and needle, a more cumbersome method. A secondset of problems concerns the development of surveillance methods by which to detect the presence of circulating poliovirus. Only 1 person among 1000 or more who are infected with the virus manifests paralytic disease, and such cases require confirmation by laboratory examination. The occurrence of paralytic cases signifies that poliovirus is present in an area, but their absence does not necessarily indicate the contrary because it is known that poliovirus can spread over large areas and for an unknown period of time without causing paralytic illness. Confirmation that poliovirus transmission has been interrupted is therefore difficult. A surveillance system for paralytic illness is being developed in the Americas which involves laboratory confirmation of suspected cases and community-wide containment vaccination. The efficacy of this approach in reducing the transmission of the virus and its sensitivity in detecting circulating virus remain to be determined. The experience acquired in the Western Hemisphere will determine the feasibility of eradication in other areas.
Dracunculiasis (guinea-worm infection)
The elimination of dracunculiasis, a parasitic infection, was agreed upon by the Thirty-ninth World Health Assembly, in 1986, as a campaign to be conducted in association with programmes of the International Drinking Water Supply and Sanitation Decade; although the Health Assembly’s resolution (WHA39.21) speaks of “elimination”, it is difficult to distinguish the intent of this from that of “eradication”. The parasite, Dracunculus medinensis, a nematode worm that measures 35-100 cm in length when adult, lives in the skin of man, the female emerges in a painful abscess to discharges tiny larvae when the infected part of the body is immersed in water. The larvae are ingested by a minute fresh-water crustacean, Cyclops, that serves as an intermediate host, in which they mature and infect man when he swallows water contaminated by the Cyclops organisms. Interruption of guinea-worm transmission is reasonably easily and rapidly achieved either by destroying the larval form of the parasite in the water tanks and ponds where people are infected, by filtering or boiling water before drinking it or by preventing patients with infection from entering such bodies of water.
Favouring eradication is the fact that comparatively simple measures have produced a dramatic reduction in incidence and the elimination of infection in many villages and larger areas of Africa and Asia. Moreover, the population at risk is estimated to be no more than 50 million persons, almost all of whom now live in rural areas in a regional belt extending across the middle of Africa and in western India and eastern Pakistan. Finally, the disease itself is a painful, disabling one of concern to the afflicted population, and for surveillance purposes the adult worm is easy to identify.
The principal problems that can be foreseen are those of interesting donor agencies in providing support for the elimination of a tropical disease which is so little known outside the affected countries and of mobilizing national interest and support for the elimination of a disease rarely seen outside rural and often remote areas.
Yaws
Yaws is a treponemal infection, transmitted from person to person, against which widespread control and eradication campaigns were mounted during the 1950s and 1960s (see Chapter 9). A single dose of penicillin effected a rapid cure and these earlier campaigns succeeded in dramatically reducing the incidence of the disease. Initially, it appeared that eradication could be easily and rapidly accomplished, but persistent low-level infections which were difficult to detect resulted in the continuation of transmission. A more concerted effort involving repeated visits to inspect all persons in the afflicted areas was required but, as cases diminished in number, so, too, did both the national and international interest and commitment.
During recent years, there has been a resurgence of yaws in many countries of Africa and some in Asia (Wkly epidem. rec., 1986a) and renewed campaigns have begun in a number of them. Although the eradication of yaws has been proposed as a possible goal, recognition of the extent and magnitude of the problem, of the practical difficulties and of the cost of implementing successful programmes has effectively muted discussion of eradication for the time being.
Conclusion
It is apparent that the successful eradication of smallpox has had important ramifications into other areas of health work, while it also provides illuminating evidence of the need for caution in deciding upon other eradication programmes. Those who were directly engaged in smallpox eradication, and many other health staff as well, gained an understanding of the impact a community-based programme, especially one in prevention, could have, of its remarkable cost-benefit implications and of the considerable human and financial resources which could be mobilized for such an effort. Many of these persons, both in developing and in industrialized countries, are now applying that understanding in public health practice. The establishment of specific, measurable, practical goals and their use in management have begun to be introduced into national health programme objectives and into community-based health initiatives. Surveillance and sample survey techniques elaborated in the course of smallpox eradication have begun to be employed increasingly in health programme management. Throughout the world, more emphasis is being placed on programmes for disease prevention and health promotion, in respect of both communicable and non-communicable diseases, although the need for such programmes is still vastly greater than the effort that is being expended upon them.
WHO, whose role in smallpox eradication was so vital, offers a unique, although as yet not fully realized potential, for promoting these new and growing efforts. It is an organization which demonstrably can catalyse achievements far out of proportion to the financial resources it commands. The extent to which it is successful will depend upon the confidence which its Member States place upon it, on its effectiveness in enunciating clear and measurable objectives and in mobilizing support for their realization, on the number and competence of its professional staff, and on its ability to set aside extraneous political questions. Its ability to respond appropriately to challenges old and new will be decisive in its task of helping all the people of the world to the attainment of the highest possible level of health.